Embed Size (px)
Citation preview

DUODENAL TUMOR OF UNUSUAL CHARACTERRICHARD T. SHACKELFORD, M.D., A. MURRAY FISHERi M.D.,
AND
WHITMER B. FIROR, M.D.BALTIMORE, MD.
THIS PAPER has been prepared for the purpose of recording a case whichshould be of particular interest to the internist, pathologist, radiologist, andsurgeon, for the following reasons:
I. It demonstrated an unusual cause for the presence of vague epigastricdistress associated with diarrhea, occult blood in the stool, anemia, and lossof weight.
2. The pathologico-anatomic lesion is of interest, and its origin provocativeof discussion.
3. The roentgenogram was deceptive, and of great interest.4. The case can be added to that increasing, but relatively small, number
in which a malignancy of the ampullary portion of the duodenum and adjacentpancreas has been successfully removed. So far as can be determined, it isthe only myosarcoma in the more than I25 cases reported in that series.
Case Report.-The patient, a married woman, age 6i, was first seen by one of us(A.M.F.), August 9, i94I, being referred by Dr. Wilbur Skillman. At this time hercomplaint was anemia for five years, and diarrhea for three months. The family historywas not important, her father and mother having both died in their 8o's. The patient hadhad a bad attack of rheumatic fever at i9, with no return of joint pains until an attackof arthritis four years ago, which involved all her jo«ints, with swelling and pain. Thesesymptoms finally cleared up after a tonsillectomy three and one-half years ago. Thepresent illness dates back five years, at which time she had symptoms of weakness,sore tongue, numbness of the hands and feet, and constipation. A diagnosis of perniciousanemia was made, and she was given I2 injections of liver extract intramuscularly,and liver and liver extract by mouth. An hemorrhoidectomy was performed at thistime because of bleeding. Four and one-half years ago a panhysterectomy was per-formed because of a diagnosis of myomata, one of which, however, proved, microscopi-cally, to be a myosarcoma (Fig. 7). Her recovery from this operation was uncomplicatedand except for the arthritis which was mentioned earlier, she remained well until May,I94I. This was three months before her examination, and she then developed rather markeddiarrhea which continued without interruption. The stools varied in number from4 to 8 in 24 hours. They were most apt to come early in the morning starting at 3 or 4o'clock, and again once or twice before breakfast. The stools were always bulky, butnever watery. At first they had a yellowish, curd-like character, later becoming grayishand at times foamy. They were always extremely foul-smelling, but never containedany blood. She had not suffered any severe abdominal pains but complained of some-soreness over the left lower quadrant of the abdomen of a colicky character, andoccasional discomfort in the epigastric region. There was no nausea or vomiting. Sore-ness of the tongue was not a symptom during this time, but she did notice that hergums were sore in places. She occasionally noticed numbness of the hands and to aless extent of the feet and had some unsteadiness when on her feet, which she interpretedas being due to weakness.
864

Volume 116 DUODENAL TUMORNumber 6
Physical Examination.-Temperature 99.4°F., pulse 96, blood pressure I08/65. Shewas much underweight, rather pale, and looked quite ill. The skin was smooth andsoft; there was no icterus and no skin lesions, but some large brown freckles over theforearms and backs of the hands. The eyes were deep-set and the lids very dark. Dentalplates were worn and there was no abnormality to be made out of the gums, mucousmembranes of the mouth or of the tongue, which was neither smooth nor red. Therewas no adenopathy. The lungs were entirely clear, and the heart was normal exceptfor the presence of numerous extrasystoles and a soft systolic murmur at the apex.Abdominal examination revealed nothing except a little tenderness in the left lowerquadrant and over the upper part of the abdomen, bilaterally, with a definite sensationof resistance in the epigastrium. Theliver edge was just palpable; it felt quitenormal. The spleen was not felt. Thefingernails were quite soft and thin. There -N6
was some swelling of the right leg asso-ciated with rather extensive varicoseveins. The neurologic examination re-vealed only some generalized muscleweakness, sluggish knee jerks, and someuncertainty of gait, apparently due toweakness; there was no spasticity. TheRomberg test was negative, and vibra-tory sense normal over hands, legs andspine.
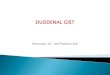
Laboratory Data.-The urine wasnormal except for a trace of albumin.The hemoglobin was 77 per cent (Sahli)R.B.C., 3,970,000; W.B.C. 6,200. Dif- DUODENUMferential: Polys, 64 per cent, L 22 per lcent, Mono. I4 per cent; the red blood STOMACHcells were normal in size and shape; noanisocytosis nor poikilocytosis; plateletswere rather scarce. The smear did notin the least resemble that of pernicious FIG. T.-Roentgenogram of stomach and duo-
denum after the ingestion of barium showing theanemia. filling defect in the duodenum caused by the
The preliminary impression was that tumor.the patient presented a history and a pic-ture suggesting nontropical sprue. It was felt that this would fit in with the formerdiagnosis of pernicious anemia, which evidently was not characteristic and did notrespond well to liver therapy. It was noted, however, that if she had had sprue atthat time it also should have shown a better response to liver. The second mostlikely diagnosis was thought to be carcinoma involving some part of the gastro-intestinal tract.
Stool specimens were examined and found to -be bulky, semiformed, and to containmuch undigested food. The first specimens did not show a definite increase in fat, asfar as could be determined by gross and microscopic examination. The benzidine testshowed a strong reaction for occult blood and the guaiac test showed a weak positive.In another examination following restriction of meat the benzidine test was againstrongly positive.
Gastric analysis following an Ewald test meal revealed no free acid, and IO per centof combined acid.
Roentgenologic examination of the gastro-intestinal tract, 8/I I/4I, by DoctorsWaters and Firor was reported as follows:
865

SHACKELFORD, FISHER AND FIROR Annals of SurgeryDecember. 19 42
"The stomach and duodenal cap are normal. A defect in the duodenum is observedextending from the distal portion of the cap into the descending portion of the duodenumapproximately to the region of the ampulla of Vater. This defect is sharply outlined,especially in its lower portion, and appears intrinsic rather than as the result of pressurefrom some extraduodenal mass. The barium mixture passes around the defect in a thinstream and discloses a normal mucosal pattern along the upper and lateral margin ofthe duodenum (Fig. i). Roentgenologic Diagnosis: The findings indicate a neoplasmin the duodenum the nature of which is indefinite. The vast majority of reported benignneoplasms of the duodenum have occurred in the duodenal cap, whereas the rare malig-nant lesions have been in the region occupied by this mass, but the sharply demarcatedcharacter of the defect in this case strongly favors benignity."
FIG. 2.-Drawing showing the sias the
tumor and the extent of the resection, as wellof the common duct.
Some improvement in her diarrhea followed the administration of dilute hydro-chloric acid, a low residue, low carbohydrate diet, but otherwise she did not improve.She was bothered a good deal with pain in the epigastrium and became increasinglyweak and pale. It was then felt that the lesion in the duodenum might well be amalignant one and that it might be responsible for many of her symptoms. On Septem-ber I7, I94I, an exploratory operation was performed by one of us (R.T.S.), at theUnion Memorial Hospital in Baltimore.
Preoperative Diagnosis: Benign polyp of the ampullary portion of the duodenum.Operation.-Under nitrous oxide, followed by drop-ether anethesia, the abdomen
was opened through an upper right rectus incision. On exploration, an intrinsic massthe size and shape of a lemon was felt within the descending portion of the duodenum,apparently attached to the posterior duodenal wall but not elsewhere. There were no
866

Volume 116 DUODENAL TUMORNumber 6
other masses seen or felt in the liver or other portions of the peritoneal cavity. Thegallbladder appeared normal. The anterior wall of the duodenum opposite the tumorwas opened longitudinally in order to inspect the lesion by direct vision. It was thenseen to be an coblong, reddish, firm, polypoid mass attached to the posterior wall of theduodenum throughout the length of the tumor by an indurated, sessile base extendingfrom about one-half inch below the pylorus to the ampulla of Vater. Its location madepreservation of the latter impossible if the former was to be removed. Resection of thatportion of the duodenum containing the tumor (Figs. 2 and 3) was decided upon.Accordingly, the duodenum was mobilized medially by incising its lateral peritonealattachments.
FIG. 3.-Drawing snowing tne appearance atter completion otthe resection of the ampullary portion of the duodenum and partof the head of the pancreas, with a Billroth-I gastroduodenostomy,ligation of the commoni duct and cholecystogastrostomy.
The duodenum was then transected between Stone anastomosis clamps at a pointone inch below the ampulla of Vater, which was at the lower border of the tumor.Both cut ends were carbolized. The common duct was positively identified by withdraw-ing bile from its lumen through a small hypodermic needle. It was then isolated andcut across about one inch from its entrance into the duodenal wall. Its cut proximalend was ligated with No. i chromic catgut reinforced by a second ligature of mediumblack silk. The stomach was sectioned one inch above the pylorus. This left the inter-vening segment of duodenum containing the tumor and ampulla attached to the pancreasalong its posterior wall. A small portion of the head of the pancreas was transected bysharp dissection at a sufficient distance to have a seemingly safe margin at the base of
867

SHACKELFORD, FISHER AND FIROR Annals of SurgerYDecember, 19 4 2
the tumor. The duodenum with its attached pancreas was then removed en masse.The cut surface of the pancreas was closed with interrupted silk sutures.
The unusual mobility of the remaining distal segment of duodenum made it possibleto perform a Billroth I, end-to-end gastroduodenostomy, which was accomplished bymeans of an inner continuous suture of the mucosal surfaces with No. o plain catgut anda serosal row of interrupted fine silk sutures.
Because the common duct could be implanted into the intestinal tract only undermarked tension, it was considered preferable to provide a pathway for bile by meansof a cholecystogastrostomy which could be done without any tension whatsoever. Thiswas accomplished in the usual way with two layers of sutures. The omentum wasplaced over both suture lines and the abdominal wound closed in layers using catgutfor the deeper sutures, silk for the skin and through and through stay sutures ofbraided silk. One Penrose drain was placed down to, but not into, the peritoneum andbrought out at the lower end of the incision.
During the procedure the patient received a transfusion of 500 cc. of citrated bloodplus IOOO Cc. of 5 per cent glucose intravenously.
The operation required two and one-half hours, and the patient returned to herroom in good condition, with pulse 126, blood pressure I38/90.
The postoperative period was a stormy one, being complicated by bilateral pulmonaryconsolidation, for which she received sulfathiazole; phlebitis of the great saphenous veinof the right leg; transitory jaundice, and generalized edema. This latter was thoughtto be mainly due to a very low serum protein level, which on September 20th, was 3.5grams per cent, and on September 23rd 4.1 grams per cent. Other laboratory studieswere reported as follows: Stool examination, on October gth, showed much gross fatwhich was stained with Sudan III. A specimen examined on October i6th showed littlefat. Blood chemical studies on September 20th were N.P.N. 29, blood chlorides 522;blood calcium 8.4; and blood phosphorous i.i. On September 23rd., N.P.N. 33, bloodchlorides 517; CO2 combining power 54 volumes per cent; and on October iith, bloodcalcium 9.2 milligrams per cent and blood phosphorous were 4 milligrams per cent.
On the I3th postoperative day the temperature which had been falling began to risein daily peaks, and on the i6th postoperative day signs of free fluid in the -abdomenappeared and the patient's condition became critical. That evening, under localanesthesia in her room, an opening was made in the healed incision and a clampinserted into the peritoneal cavity. There was an immediate gush of a large quantity(several hundred cubic centimeters) of grayish fluid containing particles of necroticmaterial. A Penrose drain was inserted, and the patient's condition immediately im-proved and continued to do so until her discharge from the hospital on her 37thpostoperative day. At the time of discharge she was ambulatory and consuming a
low fat diet, but one high in carbohydrate and protein, with liver two or three timeia week, and additional vitamins. The wound had healed except for a small sinusat its lower border which exuded a small amount of fluid. This healed two weeks laterand has remained healed.
On November 26th, she was found to be still improving and had gained three or
four pounds. She was still bothered by cramp-like abdominal pains, gas and eructationand was having an average of two stools a day, which were quite light in color butformed or semiformed. On January 5, i942, she looked definitely better but the
diarrhea, which has never entirely cleared up, was now worse again, and in spite of
a very good appetite, she was not gaining weight. The diarrhea was never watery,but the stools were bulky and at times foamy in character. Her hemoglobin was
then go per cent. It was felt that these symptoms were due mainly to lack of externalsecretion of the pancreas and pancreatin was then administered in doses of o.9 Gm.
three times daily, and is being continued.4 She was next seen February 26, I942, when she reported that she was feeling
868

Volume 116Number 6 DUODENAL TUMOR
a great deal better and gained four more pounds. Her diarrhea was much lessmarked but she still had two or three stools a day, which were quite bulky. She wasadvised to continue the same regimen of treatment.
On March i8, 1942, she reported great symptomatic improvement. She was havingalmost no symptoms and had gained weight and strength. Her color was much betterand her general appearance was one of quite good health. The following blood chem-ical studies were made, the results of which are all well within normal limits: Blood
FIG. 4.-Photograph of duodenal segment. Tumor-measures 3'/2X2V/2XI inches.Covered by mucosa and extending into muscular wall. Ampulla is situated at cornermargin of mass.
calcium 9.5 mg. per cent, blood phosphorous 3.9 mg. per cent;* total proteins 7.o6 percent; and fasting blood sugar 8i mg. per cent. The stool at this time was semiformed,yellowish-brown in color, and contained no gross fat. There was no occult blood bythe guaiac test.
The patient was progressing quite satisfactorily until May 30, 1942. At thistime, the stools were almost normal but she was having pain in the cervical spine.She had lost some weight and the hemoglobin had dropped to 7j5%. On June 9, 1942,she had much worse pain in the cervical spine and had developed flaccid paralysis of
869

SHACKELFORD, FISHER AND FIROR Annals of SurgeryDecember, 19 4 2
the left arm and some weakness of the left leg and of the face on that side. At thistime, she looked a great deal worse and it seemed obvious that she had metastaticcarcinoma involving the cervical spine and brain. From that time on she, went downhill rapidly with progressive increase in paralysis, coma, and death on June 25, 1942.An autopsy was not done but there can be no doubt that metastases from her originalcarcinoma were the cause of death.
Pathologic Examiniation-.-Gross: Dr. W. C. Merkel. Tlle specimen consists of a
FIG. 5. FIG. 7.
. ft.-O-v
FIG. 6. FIG. 8.
FIG. 5.-NO. 21777: Photomicrograph of section through duodenal tumor. Note regular muscularborder. Similar multinucleated giant cells and lack of cell patterns. (xIoo)
FIG. 6.-No. 21777: Higher magnification of section from duodenal tumor removed October, 1941.Note large multinucleated giant cells; loose vascular stroma; and pleomorphic cell morphology. (X200)
FIG. 7.-No. 13555: Photomicrograph of tumor removed (3-3-37). Uterine fibromyoma, withencapsulation. Note multinucleated cells, vascular spaces; and pleomorphic ce'll morphology. Theuterine wall forms a straight line of demarcation. (xIoo)
FIG. 8.-No. 13555: Higher magnification of section taken from uterine myoma (3-3-37). (X200)
segment of the duodenum, five inches in length, containing an oval-shaped, sessile polypon the pancreatic side of the duodenal wall. The polyp measured 3½2 inches in thelong diameter and 2½2 inches in the transverse diameter, and its depth was i½2 inchesThe surface is lobular, smooth and gives the impression of a thin layer of mucosa(Fig. 4). The cut surface is of a grayish white color forming no pattern and givingthe impression of being glandular tissue. The growth infiltrates the muscular wallbut the serosa is uninterrupted. Microscopically, the sections form a very sharp lineof demarcation. It appears as though the muscle were displaced by the growth.
870

Volume 116Number 6 DUODENAL TUMOR
The tumor is moderately vascular. There are many well-formed blood vessels whiclhwould indicate that these have not existed prior to the tumor invasion. There is markedvariation in the morphology and size of the cells. Multinucleated, huge giant cells arenumerous. The other cells which predominate have oval shaped nuclei. The cytoplasmis flocculent. Mitotic nuclei are numerous. There is no leukocytic infiltration, nor isthere any stroma formed by the tumor tissue which would give support. There is atotal absence of any cell pattern. There are areas of hemorrhage. The tissue adjacentin some areas is pancreas while most of the surrounding structures are muscle from thewall of the duodenum. Occasional lymphatics contain tumor cells, and the lymphoidstroma encountered is not infiltrated, nor does it show any evidence of resemblance totumor cells which would probably rule out an endotheliomatous type of sarcoma.Pathologic Diagnosis: Myosarcoma (comparing the growth with No. I3555 (Figs. 7and 8) which was a myosarcoma of the uterus, removed from the same patient in1937, indicates that this is probably metastatic).
There are several points about the above case which deserve furtherconsideration. One of great interest is whether the tumor represents ametastasis from the original myosarcoma of the uterus, removed four yearspreviously, or whether it is another primary tumor in a different location.Microscopically, the two lesions are identical, but the fact that the lesionoccurred in the duodenum, a rare, if not unique, site for such a metastasisplus the fact that, so far as could be determined, it is solitary, is very muchagainst the possibility of its having originated in the uterus. On the otherhand, myosarcomata of the duodenum as well as multiple myosarcomata inthe same patient have been reported, although a very cursory and in-complete survey of the literature has not revealed a similar distribution.Our opinion favors the view that the second lesion was primary in theduodenum.
Another point of interest is the fact that the patient suffered from asprue-type of diarrhea- previous to operation. This could be explained bypointing out that the pancreatic ducf traversed the tumor before joiningthe common duct and, hence, pancreatic secretions may have been blockedfrom entrance into the intestinal lumen. Jaundice was not present as thecommon duct entered the duodenum just below the tumor and in a directionwhich escaped impingement by the lesion.
The blood chemical findings are of considerable interest. In steatorrhea,whether of pancreatic origin-as we assume this to be-or due to sprue, it iscommon to find a low level of serum calcium and phosphorus. Theseabnormal values have been shown to be due to poor absorption from theintestinal tract, as is shown by excessive fecal excretion of these substanceswhile their urinary excretion is lowered. This decreased absorption is bestexplained, at least in the pancreatogenous type of steatorrhea, as being dueto two factors: (i) The excess of fat in the intestinal contents holds vitaminD in solution, thereby preventing its action in promoting calcium absorp-tion and causing more of it to be excreted in the feces; and (2) calciumforms insoluble soaps with excessive fatty acids and cannot be absorbednormally. Lowered serum proteins are also to be expected under thesecircumstances and may be related to an increased nitrogen excretion in the
871

SHACKELFORD, FISHER AND FIROR Annals of SurgeryDecember, 1942
feces, which does take place in the pancreatogenous-type of fatty diarrheain contradistinction to the sprue-type in which it is usually within normal limits.This was pointed out by Thaysen,3 who felt that the fecal nitrogen determina-tion was a good criterion in the differential diagnosis of steatorrhea. In ourpatient, it is well to remember, however, that these blood chemical studieswere made several days after the operation and were certainly modified tosome extent by the various factors that are known to alter their values underthose conditions.
The roentgenogram (Fig. i) was also of interest as the smooth outlineof the defect strongly suggested that the lesion was benign. The fact thatit proved to be malignant is worth serious consideration in the interpreta-tion of other films revealing a similar picture.
The operative attack upon these lesions was initiated by Dr. W. S. Hal-stead,1 who, in I898, first removed a carcinoma of the ampulla of Vater byremoving the duodenum, performing a Billroth-I gastroduodenostomy, andreimplanting the common and pancreatic ducts into the duodenum. At thesame time he performed a cholecystostomy. His patient succumbed sevenmonths later from a recurrence of the tumor. Since that time, other isolatedreports of similar procedures have appeared in the literature and have beensummarized by Hunt.' Recent interest has been stimulated by the writingsof Whipple, 5, 6, 8Sand his colleagues, who have had particular success withtheir modifications of the procedure, while the courage to attack this par-ticular case was derived to some degree from the recent success withwhich Dr. I. R. Trimble, of this city, performed a similar operation, whichhas been reported elsewhere.4 The articles by Whipple, Hunt and Trimblecan be recommended to those interested in the subject as in these will befound a thorough history of the methods of surgical attack, the results, anda tabulation of the cases reported in the literature.
In reviewing the above articles, one or two thoughts on the technic ofthe operation seem worthy of mention. It was pointed out by Whipple thata large proportion of these cases develop postoperative drainage for varyinglengths of time. Presumably, in most instances this has come from the cutsurface of the pancreas. In our case no provision was made for the drainageof this fluid which accumulated within the tightly closed abdomen and nearlycaused the death of the patient. The drainage was followed by prompt im-provement and recovery. In any future similar operation it is our plan toprovide such drainage at the time of operation.
Some writers emphasize the point that it is more satisfactory to reimplantt;he stump of the common duct into the duodenum, as contrasted with therestoration of biliary drainage by means of a cholecystogastrostomy. Thelatter was performed in this particular patient and, in our opinion, rightly so.The duct could have been reimplanted only under hazardous conditions oftension, while the gallbladder lay readily adjacent to the stomach. It is ourbelief that the most satisfactory operation is the one which technically is the
872

Volume 116Number 6 DUODENAL TUMOR
easiest to performii and at the samiie time accomplishes the purpose for whichit is planned.
SUMMARY
We have presented a case of a duodenal tumor which was of particularinterest for the following reasons:
i. The patient had a sprue-like diarrhea, associated with anemia and occultblood in the stools.
2. The smooth outline in the roentgenogram suggested a benign ratherthan a malignant lesion.
3. The tumor was a myosarcoma of the duodenum, in a patient who hadhad a myosarcoma of the uterus removed four years previously.
4. The lesion was successfully treated by removing the ampullary portionof the duodenum, with the adjacent portion of the head of the pancreas; andthen performing a cholecystogastrostomy and a Billroth-I gastroduodenostomy.
REFERENCESI Hunt, Verne C.: Surgical Management of Carcinoma of the Ampulla of Vater and of
the Periampullary Portion of the Duodenum. ANNALS OF SURGERY, 114, 570-602,October, I941.
2 Orr, Thomas G.: Resection of Duodenum and Head of Pancreas for Carcinoma of theAmpulla. Surg., Gynec. & Obst., 73, 240-243, August, I94I.
3 Thaysen, T. E. Hess: Ten Cases of Idiopathic Steatorrhea. Quar. Jour. Med., 4,359, I935.
4 Trimble, I. Ridgeway, Parsons, John W., and Sherman, Claude P.: A Otwe-StageOperation for the Cure of Carcinoma of the Ampulla of Vater and the Head ofthe Pancreas. Surg., Gynec. & Obst., 73, 7II-722, November, I941.
5Whipple, Allen O.: Surgical Treatment of Carcinoma of the Ampullary Region andHead of the Pancreas. Am. Jour. Surg., 40, 260-263, 1938.
6 Whipple, Allen O.: Personal communication.7 Whipple, Allen O., and Frantz, Virginia Kneeland: Adenoma of Islet Cells with Hyper-
insulinism. ANNALS OF SURGERY, 101, I299-1335, I935.8 Whipple, Allen O., Parson, William Barclay, and Mullins, Clinton R.: Treatnient of
Carcinoma of the Ampulla of Vater. ANNALS OF SURGERY, 102, 763-779, 1935.
873