Embed Size (px)
Citation preview

Cas clinique
DOI of or1Cardiovas
Yokohama, Ja2Departme
Center, Yokoh
CorrespondYokohama CitKu, Yokohama
Ann Vasc Surhttp://dx.doi.or� Annals of V�Edit�e par ELS
Dysplasie fibromusculaire associ�ee �a ladissection spontan�ee simultan�ee de quatreart�eres p�eriph�eriques chez un homme de30 ans
Tadahisa Sugiura,1 Kiyotaka Imoto,1 Keiji Uchida,1 Hiromasa Yanagi,1 Daisuke Machida,1
Makoto Okiyama,1 Shota Yasuda,1 Shigeo Takebayashi,2 Yokohama, Japon
Un homme de 30 ans a eu un acc�es soudain de douleurs abdominales graves. Un scanner mon-trait des dissections des art�eres coeliaque, m�esent�erique sup�erieure, r�enale gauche, et iliaqueexterne droite ; une st�enose de l’art�ere r�enale droite ; et un infarctus du rein gauche. Apr�es�evaluation soigneuse, le diagnostic de dysplasie fibromusculaire (dysplasie m�ediale) �etait port�e,sur les r�esultats du scanner. Ce cas est extremement rare parce que la dysplasie fibromuscu-laire s’est produite en meme temps que des dissections spontan�ees simultan�ees de quatreart�eres p�eriph�eriques chez un jeune homme.
Fibromuscular dysplasia (FMD) is a noninflamma-
tory, nonatherosclerotic disorder that leads to arte-
rial stenosis. It most commonly affects the renal
and internal carotid arteries and is more common
among women than men. We report the case of a
30-year-old man who had FMD associated with
simultaneous spontaneous dissections of the celiac
artery, superior mesenteric artery, left renal artery,
and right external iliac artery.
CASE REPORT
A30-year-oldmanhad a sudden bout of severe abdominal
pain and was taken to a hospital. An enhanced computed
tomographic (CT) scan revealed dissections of the celiac
iginal article: 10.1016/j.avsg.2011.02.018.
cular Center, Yokohama City University Medical Center,pon.
nt of Radiology, Yokohama City University Medicalama, Japon.
ance : Tadahisa Sugiura, Cardiovascular Center,y University Medical Center, 4-57 Urafune-Cho, Minami-232-0024, Japon, E-mail: [email protected]
g 2011; 25: 838.e9-838.e11g/10.1016/j.acvfr.2012.07.021ascular Surgery Inc.EVIER MASSON SAS
artery (Fig. 1A), superior mesenteric artery, left renal
artery (Fig. 1B), and right external iliac artery (Fig 1C);
stenosis of the right renal artery; and left kidney infarction.
The patient was transferred to our hospital because his
condition did not improve 2 days after admission.
He was given a beta-blocker and a calcium antagonist
for hypertension. He was administered warfarin (target
international normalized ration: 2.0-2.5), and aspirin
(100 mg) for arterial stenosis owing to the dissections.
Laboratory tests gave the following findings: white cell
count, 15,660/mL; platelets, 7.4 � 104/mL, aspartate ami-
notransferase, 65 U/L; alanine aminotransferase, 63 U/L;
lactate dehydrogenase, 1,118 U/L; blood urea nitrogen,
18 mg/dL; serum creatinine, 2.11 mg/dL; and C-reactive
protein, 11.168 mg/dL. Vasculitis was initially suspected,
but was not supported by the results of laboratory tests.
Finally, FMD (medial dysplasia type) was diagnosed on
the basis of enhanced CT findings.
Headache and dizziness developed on the same day as
the abdominal pain. A brain CT scan showed a low-
density area in the left cerebellum. Although the finding
was not compatible with cerebellar infarction, the results
of follow-up CT indicated that the low-density area was a
small infarction. However, CT angiography showed no
dissection of the head or neck vessels.
Renal scintigraphy revealed glomerular filtration rate
(GFR) of 25.6 ml/min/1.73m2 (left kidney) and 6.7 ml/
min/1.73m2 (right kidney). We thought that the right
renal artery stenosis was the cause of decline of the right
894.e9

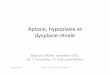
Fig. 1. (A) An enhanced computed tomographic (CT)
scan revealing dissection of the celiac artery (arrow). (B)
An enhanced CT scan revealing dissection of superior
mesenteric artery and left renal artery (arrow). (C) An
enhanced CT scan revealing dissection of right external
iliac artery (arrow).
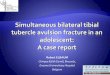
Fig. 2. Angiography of the right renal artery. The middle portion of the right renal artery was stenotic (A), and after
successful dilation with stent (B).
894.e10 Cas cliniques Annales de chirurgie vasculaire
renal GFR. Therefore, we performed percutaneous trans-
luminal right renal angioplasty (Fig. 2A, B). After this
procedure, renal function improved gradually; renal
scintigraphy showed GFR of 25.5 ml/min/1.73m2 (left)
and 21.6 ml/min/1.73m2 (right). Amylase and lipase
levels increased 4 days later, ischemic pancreatitis was
then diagnosed. The patient was discharged from the
hospital after 67 days. He is doing well 1 year after dis-
charge. He continued to take warfarin for 3 months and
will continue to take aspirin all his life.
DISCUSSION
The etiology of FMD remains unclear and is thought
to involve a variety of genetic, mechanical, and
hormonal factors. Among adults, FMD is more
common inwomen, with a 2-10 times higher preva-
lence than that in men.1 FMDmost often affects the
renal arteries, accounting for 60-75% of cases.2
Extracranial cerebrovascular arteries are involved in
25-30% of cases, and other miscellaneous arteries,
such as the mesenteric or brachial arteries and
coronary arteries, are involved in up to 30% of
cases. Approximately 25% of patients have invol-
vement of multiple arteries.2
The most commonly accepted classification of
FMD includes three major types: medial dysplasia,
intimal fibroplasia, and adventitial fibroplasia.3
Medial dysplasia is further divided into three
subgroups: medial fibroplasia, medial hyperplasia,

Vol. 25, No. 6, 2011 Cas cliniques 894.e11
and perimedial fibroplasia. Medial fibroplasia is
most common, accounting for 60-70%of all types of
FMD, and is characterized by a ‘‘string of beads’’
appearance on angiography.
Approximately one-half of all dissections
involving visceral arteries are asymptomatic. Occa-
sionally, patients present with intestinal angina or
hemorrhage.4,5 Various symptoms have been des-
cribed depending on the location of the lesions,
including jaundice in association with dissection of
the celiac and hepatic artery, or malabsorption with
involvement of the superior mesenteric artery.6,7
Glehen et al. reported a treatment strategy for the
acute phase of isolated symptomatic celiac artery
dissections.8 Surgery is indicated for management
of aneurysm, occlusive lesions jeopardizing the
lower intestine, arterial rupture, or liver ischemia.
They further suggest that conservative medical
treatment can be proposed for patients with limited
dissection in whom serial examinations have
demonstrated no evidence of rupture or expansion.
Therefore, the patient had conservative treatment in
this case.
Our patient had similar abdominal pain 1 year
before the present episode, but enhanced CT at
that time revealed no dissection, and he was asymp-
tomatic after that. The dissections of the four peri-
pheral arteries (celiac artery, superior mesenteric
artery, left renal artery, and right external iliac
artery)were therefore considered to have developed
spontaneously. To our knowledge, this is the first
documented case of FMD with these characteristics.
This case is extremely rare because FMD occurred
concurrently with spontaneous dissections of four
peripheral arteries in a young man.
REFERENCES
1. Estepa R, Gallego N, Orte L, Puras E, Aracil E, Ortuno J.
Renovascular hypertension in children. Scand J Urol Nephrol
2001;35:388-392.
2. Luscher TF, Keller HM, Imhof HG, et coll. Fibromuscular
hyperplasia: extension of a disease and therapeutic outcome.
Results of the University Hospital Zurich Cooperative Study
on Fibromuscular Hyperplasia. Nephron 1986;44(Suppl. 1):
109-114.
3. Harrison EG, McCormack LJ. Pathologic classification of renal
artery disease in renovascular hypertension. Mayo Clin Proc
1971;46:161-167.
4. Matsuo R, Ohta Y, Kitazono T, Irie H, Shikata T, Abe I,
Fujishima M. Isolated dissection of the celiac artery-a case
report. Angiology 2000;51:603-607.
5. Chaillou P, Moussu P, Noel SF, Sagan C, Pistorius MA,
Langlard JM, Patra P. Spontaneous dissection of the celiac
artery. Ann Vasc Surg 1997;11:413-415.
6. Bret PM, Partensky C, Bretagnolle M, Paliard P, Burke M.
Obstructive jaundice by a dissecting aneurysm of celiac axis
and hepatic artery. Dig Dis Sci 1987;32:1431-1434.
7. Clark F, Murray SM. Steatorrhoea due to dissecting aneurysm
of the superior mesenteric artery. Br Med J 1962;5310:
965-966.
8. Glehen O, Feugier P, Aleksic Y, Delannoy P, Chevalier JM.
Spontaneous dissection of the celiac artery. Ann Vasc Surg
2001;15:687-692.