Embed Size (px)
Citation preview

94
ORIGINAL ARTICLE
Acta Medica Indonesiana - The Indonesian Journal of Internal Medicine
Effect of Allopurinol on Oxidative Stress and Hypoxic Adaptation Response During Surgical Correction of Tetralogy of Fallot
Fathema D. Rachmat1, Jusuf Rachmat1, Sudigdo Sastroasmoro2, Septelia I. Wanandi3
1 Department of Surgery, Faculty of Medicine, University of Indonesia-Cipto Mangunkusumo Hospital, Jakarta, Indonesia. 2 Department of Pediatric, Faculty of Medicine, University of Indonesia-Cipto Mangunkusumo Hospital, Jakarta, Indonesia. 3 Department of Biochemistry and Molecular Biology, Faculty of Medicine, University of Indonesia-Cipto Mangunkusumo Hospital, Jakarta, Indonesia.
Correspondence mail: Division of Thoracic and Cardiovascular Surgery, Department of Surgery, Faculty of Medicine, University of Indonesia-Cipto Mangunkusumo Hospital. Jl. Salemba 6 Jakarta 10430, Indonesia. email: [email protected].
ABSTRAKTujuan: menganalisis peran alopurinol dalam mengurangi cedera iskemia-reperfusi pada pembedahan
koreksi tetralogi falot (TF), serta mengevaluasi perubahan aktivitas ikat HIF-1 (hypoxia inducible factor)selama operasi koreksi TF. Metode: uji klinis acak tersamar ganda pada pasien yang menjalani operasi koreksi TF di Unit Pelayanan Jantung Terpadu, RS. Cipto Mangunkusumo periode September 2009-Mei 2010. Subyek penelitian secara acak dibagi menjadi dua kelompok. Kelompok pertama diberi alopurinol 10 mg/kg tiga kali sebelum operasi (n=13), kelompok kedua diberi plasebo (n=13). Spesimen jaringan ventrikel kanan diambil untuk pengukuran ekspresi reactive oxygen species (ROS), dan spesimen darah dari sinus koronarius diambil untuk pengukuran kadar TNF-α, superoxide dismutase (SOD), malondialdehyde (MDA), dan HIF-1α. Hasil: jumlah kardiomiosit pengekspresi ROS kelompok plasebo meningkat pada fase pre-iskemi, iskemi, dan reperfusi (41,37+29,29%; 42,61+22,82% dan 53,81+25,76%). Sedangkan pada kelompok alopurinol menurun (44,68+19,79%, 56,87+15,50 %, dan 47,98+22,52%). Konsentrasi TNF-α pada kelompok plasebo cenderung meningkat pada fase pre-iskemi, iskemi, reperfusi, dan pemulihan, tetapi secara statistik tidak signifikan. Sedangkan pada kelompok alopurinol kadar TNF-a cenderung menurun. Konsentrasi SOD meningkat pada kelompok alopurinol pada fase iskemia, sedangkan pada kelompok plasebo tidak ada peningkatan yang signifikan. Konsentrasi MDA pada kelompok plasebo meningkat tinggi (1,75 pmol/mg; 2,37 pmol/mg; 2,72 pmol/mg; 4,82 pmol/mg), sedangkan pada kelompok alopurinol tidak mengalami perubahan yang signifikan. Ekspresi HIF-1α pada kelompok plasebo mengalami penurunan yang signifikan (p=0,026) dari fase pre-iskemia ke fase iskemia, tetapi kembali meningkat saat fase reperfusi (0,95 OD/mg protein, 0,52 OD/mg protein, 0,9 OD/mg protein). Kesimpulan: pemberian alopurinol oral prabedah koreksi TF dapat mengurangi cedera iskemi reperfusi yang terlihat dari penurunan ekspresi ROS kardiomiosit, penurunan kadar TNF-α dan MDA dalam darah, serta meningkatkan konsentrasi SOD. Selain itu, terdapat penurunan ekspresi HIF-1α pada kardiomiosit ventrikel kanan selama fase iskemia.
Kata kunci: alopurinol, tetralogi falot, reactive oxygen species, superoxide dismutase, TNF-a, HIF-1.
ABSTRACTAim: to analyze the role of allopurinol in reducing the ischemia-reperfusion injury, and to confirm the HIF-1
binding activity changes during the surgical correction of tetralogy of fallot (TF). Methods: randomized, double-

Vol 45 • Number 2 • April 2013 Effect of allopurinol on oxidative stress and hypoxic adaptation response
95
blind experimental study on patients undergoing surgical correction of TF in the Integrated Cardiovascular Services, Cipto Mangunkusumo Hospital from September 2009-May 2010. Patients were randomly divided into two groups. The first group was given 10 mg/kg body weight of allopurinol 3 times before undergoing operation (n=13) and the other group was given placebo (n=13). Tissue specimen from right ventricular muscle were taken for measurement of reactive oxygen species (ROS) expression and blood specimens from intra-coronary sinus for measurement of TNF-α, superoxide dismutase (SOD), and malondialdehyde (MDA). Results: cardiomyocytes expressing ROS in placebo group increased (41.37+29.29%; 42.61+22.82% and 53.81+25.76%), while in allopurinol group decreased (44.68+19.79%, 56.87+15.50%, and 47.98+22.52%). Concentration of TNF-α tend to decrease in allopurinol group, while it tended to increase in the placebo goup. Concentration of SOD increased in the allopurinol group, while in the placebo group there were no significant changes. Concentration of MDA was highly increased in the placebo group (1.75 pmol/mg; 2.37 pmol/mg; 2.72 pmol/mg; 4.82 pmol/mg), but statistically it was not significant. On the other hand, there was no significant change of MDA concentration in the allopurinol group. Expression of HIF-1α in TF patients decreased significantly (p=0.026) from pre ischemic phase to ischemic phase, but it increased in the reperfusion phase (0.95 OD/mg protein, 0.52 OD/mg protein, 0.9 OD/mg protein). Conclusion: pre-surgical oral allopurinol treatment reduced ischemia-reperfusion injury during TF surgical correction, as indicated by the decrease in the number of cardiomyocytes expressing ROS, reducing TNF-α, SOD, and MDA concentration in blood. There was a decrease in HIF-1α concentration in cardiomyocytes of the right ventricle during ischemic phase.
Key words: allopurinol, tetralogy of fallot, reactive oxygen species, superoxide dismutase, TNF-a, HIF-1..
INTRODUCTIONCongenital heart disease (CHD) is an
inherited disease with the incidence of 35,000 to 40,000 cases each year in Indonesia. Cyanosis is commonly found with the incidence of 10-50% of all the cases of the tetralogy of fallot (TF).1-4
The new paradigm of early correction of the TF treatment is to avoid the rise of complications from history of the disease while avoiding the occurrence of postoperative problems. However, in Indonesia, many CHD patients presents the cardiac center with a condition that is too late to correct.1-4
Corrective action for CHD is generally done with an open heart surgery using the heart lung bypass machine or cardiopulmonary by pass (CPB), with the mortality of TF patients of 4-4.5%. The most important postoperative complication is oxidative stress due to ischemia-reperfusion injury and systemic inflammatory response syndrome that can lead to death.5,6
Ischemia-reperfusion injury resulting from the use of CPB leads to the formation of reactive oxygen species (ROS) which can destroy the nucleic acid, protein, carbohydrate, and lipid layer on the cell membrane. The destruction produces lipid radical peroxil and lipid peroxide,
or the formation of malondialdehyde (MDA). Some research about oxidative stress found that xanthine oxidase (XO) is the main source of ROS.7-11 Then, the body produces endogenous antioxidants, such as catalase, glutathione peroxidace, and superoxide dismutase (SOD) to counteract the ROS.7-8
Besides initiating the formation of the ROS, ischemia-reperfusion injury also triggers the inflammatory response by releasing the inflammatory mediators such as TNF-α. It is proven by the discovery of high TNF-α concentration after CPB procedure.9
In TF patient with chronic hypoxia and cyanosis, a transcription factor known as hypoxia-inducible factor (HIF)-1α is expressed. It encourages the expression of gene encoding proteins that play a role in cell adaptation.7,9,12-16
Research on various drugs to overcome reperfusion injury has been widely done.17-18 One of them is allopurinol. Allopurinol can act both as a non-competitive inhibitor and competitive inhibitor of xanthine oxidase.8,19 Das et al (1987) showed in their study that allopurinol and oxypurinol had radical scavenging and cardioprotection effects.17 However, the effect of allopurinol on ROS formation in surgical

Fathema D. Rachmat Acta Med Indones-Indones J Intern Med
96
correction of TF has not been confirmed yet.Therefore, in this study we aimed to analyze
the role of allopurinol in reducing the effect of oxidative stress due to ischemia-reperfusion injury. In addition, we would like to confirm the HIF-1 binding activity changes during the surgical correction of TF.
METHODSThis is an experimental randomized study
in patients undergoing surgical correction of TF by the same one senior cardiac surgeon during September 2009-May 2010 in the Integrated Cardiovascular Services, Cipto Mangunkusumo Hospital. Exclusion criteria included patients with hypersensitivity to allopurinol, and a single coronary artery.
Eligible patients were divided randomly into two groups. The first group (intervention group) received allopurinol 10 mg/kg body weight, 3 times before undergoing operation (twelve
hours, two hours, and just before induction of anesthesia). The second group (control group) was given placebo instead of allopurinol.
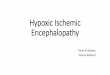
SamplesA resection of tissue sample was taken from
the right ventricular infundibular muscles and blood sample taken from intra coronary sinus (Figure 1). All specimens were immediately frozen after collection. Specimen analysis was performed in Biochemistry Laboratory, Faculty of Medicine, University of Indonesia.
MeasurementsCardiomyocytes and HIF-1 binding activity
measurement were performed on the resection of tissue samples. On the other hand, concentration of TNF-α, SOD, and MDA measurement were performed on the blood samples.
Measurement of ROS expression was performed on the single cell suspension obtained from the resection of tissue samples. The samples
Figure 1. Flow of collecting sample during surgery

Vol 45 • Number 2 • April 2013 Effect of allopurinol on oxidative stress and hypoxic adaptation response
97
were mixed with dichlorofluorescein diacetate (DCFH-DA) and incubated for 30 minutes, and then put on the flow cytometry to count the number of living cardiomyocytes expressing ROS.
The measurement HIF-1 binding activity was performed only on the control group. It was measured by transbinding HIF-1α assay through a two-stage: process the core protein extraction using nuclear extraction kit, and then the measurement of HIF-1 binding activity.
Concentration of TNF-α was measured by enzyme-linked immunosorbent assay (ELISA) technique, and concentration of SOD was measured through bio-chemical examination using a spectrophotometer (505 nanometers of wavelength).
Concentration of MDA was measured using thio-barbituric acid (TBA) technique and then performed on a spectrophotometry (530 nanometers of wavelength).
Ethics The protocol of this study had been approved
by the health research ethics committee of Faculty of Medicine, University of Indonesia. Written informed consents were obtained from all participants.
Statistical AnalysisData were presented as mean and standard
deviation (SD). Student t-test was used to compare those measurements between the placebo and allopurinol group.
RESULTSA total of 26 eligible patients were included
in this study, 13 patients were entered in the placebo group and 13 patients in the allopurinol group.
As shown in Table 1, it was found that both groups had comparable characteristics and could be assumed that both groups would have same prognostic factors. There was no mortality during the study.
Expression of ROSThe presence of living cardiomyocytes
expressing ROS was measured in three different phases (pre-ischemia, ischemia, and reperfusion) (Table 2).
There was a significant difference (p=0.008) of cardiomyocytes mean value of ROS expression between pre-ischemic and ischemic phase, while there was no significant difference between ischemic and reperfusion phase in allopurinol group. In contrast, mean value of cardiomyocytes in placebo group did not show any significant differences between phases.
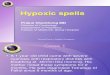
Expression of HIF-1αThe expression of HIF-1α was measured
only in the placebo group (control group). HIF-1α expression decreased significantly (p=0.026) from pre-ischemic to ischemic phase. Then it increased, but was not significant (p=0.241), in the reperfusion phase (Figure 2).
Table 1. Characteristics of patients undergoing surgical correction of TF in allopurinol group and placebo group
Variables Allopurinol (n=13) Placebo (n=13)
Gender (male) 8 11
Age-mean (SD) months 91.92 (72.20) 116.31(74.52)
Weight loss-mean (SD) kg 17.15 (7.61) 21.62 (12.78)
BSA-mean (SD) m2 0.75 (0.23) 0.85 (0.35)
SpO2-mean (SD) % 82.62 (11.75) 88.15 (7.19)
Leukocyte-mean (SD)/L 10.82 (4.08) 7.55(2.28)
Hb - mean (SD) g/dl 16.58 (2.95) 16.24 (3.92)
McGoon Ratio-mean (SD) 1.76 (0.36) 1.79 (0.38)
Nakata Index-mean (SD) 203.26 (74.48) 225.09 (28.84)
CPB-mean (SD) hrs 01:16:00 (00:19:14) 01:13:04 (0:15:34)
AoX-mean (SD) hrs 00:30:13 (00:05:01) 00:28:23 (00:03:31)
Notes: BSA=Body Surface Area; SpO2= Arterial Oxygen Saturation; Hb=Hemoglobin; CPB=Left Cardiac Pulmonary Bypass Time; AoX=Aortic Cross Clamp Time

Fathema D. Rachmat Acta Med Indones-Indones J Intern Med
98
Concentration of TNF-αConcentration of TNF-α in blood showed the
systemic inflammatory reaction due to the use of CPB in surgical correction of TF. It was measured in four different phases (pre-ischemia, ischemia, reperfusion, and recovery in ICU) (Table 3).
Statistically, there was no significant difference between phases in both groups (p>0.05). However, there was a clear tendency evident in each group. The concentration of TNF-α in the allopurinol group decreased during ischemia-reperfusion phase. In contrast, the concentration of TNF-α in the placebo group increased gradually.
Clinically, there were two patients in the allopurinol group with severe SIRS condition, where as in the placebo group, one patient had sepsis condition.
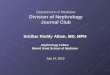
Concentration of SODSOD concentration in the placebo group
did not differ significantly in every interphase (Figure 3). In contrast, the SOD concentration in the allopurinol group increased significantly
(p=0.05) from pre-ischemic to ischemic phase. In the ischemic phase, SOD was found in the highest concentration in blood. Then, it decreased significantly (p=0.04) from ischemic to reperfusion phase.
Table 2. Precentage of right ventricular cardiomyocytes expressing ROS in 3 phases
Treatment Pre-ischemiaMean (SD)
IschemiaMean (SD)
ReperfusionMean (SD)
Allopurinol 44.68 (19.79)
56.87 (15.50)
47.98 (22.52)
Placebo 41.37 (29.29)
42.61 (22.82)
53.81 (25.76)
Figure 2. Mean value of HIF-1α binding activity in placebo group (OD/mg protein)
Table 3. Concentration of TNF-α in blood samples
Treatment Pre-ischemia (pg/ml)Mean (SD)
Ischemia (pg/ml)Mean (SD)
Reperfusion (pg/ml)Mean (SD)
Recovery (pg/ml)Mean (SD)
Allopurinol 19.36(15.06) 14.83(18.12) 14.53(13.45) 15.93(11.66)
Placebo 15.02(7.61) 26.38(57.35) 34.50(70.08) 47.39(73.54)
Figure 3. Mean value of SOD concentration (U/mg protein)
Figure 4. Mean value of MDA concentration (pmol/mg)
Concentration of MDAConcentration of MDA in both groups of
patients were measured in 4 different phases (pre-ischemia, ischemia, reperfusion, and recovery). Statistically, there was no significant difference of MDA concentration in both groups.
The MDA concentration in the allopurinol group increased from pre-ischemic to ischemic phase, but decreased in reperfusion and recovery phase. The lowest concentration of MDA in

Vol 45 • Number 2 • April 2013 Effect of allopurinol on oxidative stress and hypoxic adaptation response
99
allopurinol patient was found in the recovery phase.
Meanwhile, the MDA concentration in the placebo group increased from pre-ischemic to ischemic phase. Then it continued to increase until reaching its highest concentration in the recovery phase.
DISCUSSIONBased on the literature, allopurinol has an
inhibitory effect of XO activity.20 In this study, XO activity was limited only in the reperfusion phase, after the aortic cross-clamp was taken off. By using these assumptions, allopurinol was expected to have an effect only in the reperfusion phase. Therefore, variation in the values obtained in the pre-ischemic phase could be considered as a basic value of each independent variable.
The increase of ROS expression in the ischemic phase in both groups indicates a process that stimulates the paradoxically ROS expression. The process occurred through the formation of NO in low concentration (5-10% of normal concentration) and inhibition of cytochrome oxidase by nitric oxide leading to the formation of O2
- in low concentration of oxygen.21-23
The cardioprotection effects of allopurinol on myocardinal stunning in the reperfusion phase was confimed by the reduction of ROS expression in the allopurinol group while it continued to increase in placebo group.
The use of CPB in surgical correction of TF is one of the factors leading to systemic inflammation reaction. The effect of allopurinol on TNF-α concentration in blood was showed in the low concentration of TNF-α from the ischemic to recovery phase in allopurinol group compared to the placebo group (Table 3).
In hypoxic condition, ROS are formed due to the oxidation process. Thus, they have to be eliminated by antioxidant treatments.24 In this study, we found that allopurinol and SOD played an important role as antioxidants against ROS and oxidative stress. In the ischemic phase, SOD concentration was higher in patients with allopurinol than patients with placebo. Concentration of SOD in patients with placebo did not differ significantly in every phase (Figure
3). There have not been any studies about the association between allopurinol treatment and SOD concentration. However, from this study, we can conclude that allopurinnol treatment could reduce the ischemia-reperfusion injury and have synergic effect on expression and activity of SOD.
Concentration of MDA differed significantly between both groups in the recovery phase. Ischemia-reperfusion was found to increase MDA contents.24 Patients with allopurinol had lower concentration of MDA (Figure 4). Based on this result, allopurinol treatment was expected to reduce the destruction of lipid in the cell membrane. This result also supports previous studies that lipid peroxidation process in reperfusion phase could be prevented by ROS scavenging.25 Liu et al. (2008) found that MDA levels on ischemia-reperfusion injury in rat liver decreased when allopurinol or apocynin treatments were given.26
In surgical correction of TF, patients with chronic hypoxia will fall into acute ischemic hypoxia during the aortic cross clamp installation. However, we found that HIF-1 binding activity did not increase in the ischemic phase as we expected, but decreased. It supports the study of Reddy et al. (2006) that a maladaptation process occurred in cardiomyocytes of right ventricle of TF patients.3 This result of maladaptation process has changed the paradigm in TF patient treatment. The assumption that TF patients who adapted to the chronic hypoxia condition were able to overcome acute hypoxia was not true. Therefore, clinical finding caused by acute hypoxia, both in pre-surgery and post-surgery must be responded immediately to prevent morbidity and mortality.
On the other hand, in reperfusion phase, HIF-1 binding activity increased following the blood back to the coronary system. In that condition, ROS expression increased and led to stabilization of HIF-1α.
CONCLUSIONIt is concluded that pre-surgical oral
allopurinol treatment reduces the number of cardiomyocytes expressing ROS in reperfusion phase, reduces TNF-α concentration, increases

Fathema D. Rachmat Acta Med Indones-Indones J Intern Med
100
SOD concentration in blood, and stabilizes and reduces MDA concentration in blood.In addition, there was a decrease in HIF-1α concentration in cardiomyocytes of the right ventricle during ischemic phase.
REFERENCES1. Parry AJ, McElhinney DB, Kung GC, Reddy VM,
Brook M, Hanley FL. Elective primary repair of acyanotic tetralogy of Fallot in early infancy: Overall outcome and impact ono the pulmonary valve. J Am Coll Cardiol. 2000;36:2279-83.
2. Chang RKR, Chen AY. Factors associated with age at operation for children with congenital heart disease. Pediatrics. 2000;105:1073-81.
3. Reddy S, Osorio JC, Duque AM, Kaufman BD, Phillips AB, Chen JM. Failure of right ventricular adaptation in children with tetralogy of Fallot. Circulation. 2006;114(I):37-42.
4. Vohra HA, Adamson L, Haw MP. Is early primary repair for correction of tetralogy of Fallot comparable to surgery after 6 month of age? Interact Cardio Vasc Thorac Surg. 2008;7:698-701.
5. Giacomuzzi C, Mejak B, Shen I. Cardio-pulmonary bypass-overview: State of the art and future. Cardiopulmonary by pass-principles and practice. In: Gravlee GP, Stammers AH, Ungerleider RM, eds. Philadephia: Wolters Kluwer-Lippincott Williams & Wilkins; 2008. p. 685-99.
6. Paparellaa D, Yau TM, Young E. Cardiopulmonary by pass induced inflammation: Pathophysiology and treatment. An update. Europ J Cardio-thoracic Surg. 2002;21:232-44.
7. Saugstad OD. Role of xanthine oxidase and its inhibitor in hypoxia: Reoxugenation injury. Pediatrics. 1996;98:103-7.
8. MacGowan SW, Regan MC, Malone C, Sharkey O, Young L, Gorey TF. Supeoxide radical and xanthine oxidoreductase activity in the human heart during cardiac operations. Ann Thorac Surg. 1995;60:1289-93.
9. McCord JM. Oxygen-derived free radicals in post-ischemic tissue injury. N Engl J Med. 1985:312:159-63.
10. Klein HH, Pich S, Schuff-Werner P, Niedmann P, Blattmann U, Nebendahl K. The effects of trolox, a water soluble vitamin E analogue, in regionally ischemic, reperfused porcine hearts. Int J Cardiol. 1991;32:291-302.
11. Pacher P, Nivorozhkin A, Szabo C. Therapeutic effect of xanthine oxidase inhibitors: renaissance half a century after the discovery of allopurinol. Pharmacol Rev. 2006;58(1):87-114.
12. Essop MF. Cardiac metabolic adaptations in response to chronic hypoxia. J Physiol. 2007;584;715-26.
13. Ke Q, Costa M. Hypoxia-inducible factor-1 (HIF-1). Mol Pharmacol. 2006;70:1469-80.
14. Giordano FJ. Oxygen, oxidative stress, hypoxia, and heart failure. J Clin Invest. 2005;115:500-8.
15. McMichael M, Moore RM. Ischemia-reperfusion injury pathophysiology. Part I. J Veterinary Emerg & Crit Care. 2004;14(4): 231-41.
16. Dhalla N, Elmoselhi AB, Hata T, Makino N. Status of myocardial antioxidants in ischemia-reperfusion injury. Cardiovasc Res. 2000;477(3):446-56.
17. Das D, Engelman RM, Clement R, Otani H, Prasad MR, Rao PS. Role of xanthine oxidase inhibitor as free radical scavenger: A novel mechanism of action of allopurinol and oxypurinol in myocardial salvage. Biochem Biophy Res Commun. 1987;148:314-9.
18. Shernan SK. Perioperative myocardial ischemia-reperfusion injury. Anesthesiol Clin North Am. 2003;21:465-85.
19. Pacher P, Nivorozhkin A, Szabo C. Therapeutic effects of xanthine oxidase inhibitors: Renaissance half a century after the discovery of allopurinol. Pharmacol Reviews. 2006;58:87-114.
20. Zweier JL, Talukder MAH. The role of oxidants and free radicals in reperfusion injury. Cardiovasc Res. 2006;70:181-90.
21. Chandel NS, McClintock DS, Feliciano CE, Wood TM, Melendez JA, Rodriguez AM. Reactive oxygen species generated at mitochondrial complex III stabilize hypoxia-inducible factor-Ia during hypoxia. JBC. 2000;275:24130-8.
22. Young B, Lowe JS, Stevens A. Wheather’s functional history: A text and color atlas. Philadelphia: Elsevier; 2007.
23. Suyatna FD. Radikal bebas dan iskemia. Cermin Dunia Kedokt. 1989;57;258.
24. Dhalla NS, Elmoselhi AB, Hata T, Makino N. Status of myocardial antioxidants in ischemia-reperfusion injury. Cardiovasc Res. 2000;47:446-56.
25. Rashid MA, Wiliam-Olsson G. Influence of allopurinol on cardiac complications in open heart operations. Ann Thorac Surg. 1991;52:127-30.
26. Liu PG, He SQ, Zhang YH, Wu J. Protective effect of apocynin and allopurinol on ischemia/reperfusion-induced liver injury in mice. World J Gastroenterol. 2008;14(18):2832-7.