Embed Size (px)
Citation preview

EMERGENCY MEDICINE Liverpool Hospital
The Weekly Probe23rd April 2013 Volume 17, Issue 10
Last Week’s Case – ChylothoraxPregabalin (Lyrica)Joke / Quote of the Week
LAST WEEK’S CASE – CHLYOTHORAX
A 65yo man presents with dyspnoea for 2 weeks following CABGs. He has no chest pain and is afebrile. On CXR he has a large left pleural effusion. Upon inserting a pleurocath, you note the drainage of a large amount of “salmon“ coloured fluid. What is this and how do you treat it?
The fluid is evidence of a chylothorax, which is caused by disruption or obstruction of the thoracic duct or its tributaries resulting in the leakage of chyle (lymphatic fluid of intestinal origin) into the pleural space.
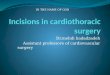
Where does it come from? A reminder for those of us who have not recently done their anatomy primary regarding the course of the thoracic duct. It functions to carry triglyceride filled chylomicrons, electrolytes, lymphocytes, fat soluble vitamins and immunoglobins from the gut back to the blood stream.

Note that there is some anatomic variability yet it commences from the cisterna chyli anterior to the L1 or 2 and passes through the aortic hiatus of the diaphragm into the chest. At ~ T5 it crosses over the vertebral column from the right behind the oesophagus to the left posterior mediastinum, running behind the arch. It then arches over the subclavian artery to empty into the region of the left jugular and subclavian veins. Below T 5, damage to the duct results in a right-sided effusion, above this results in a left-sided effusion. After receiving lymph from the lung and pleura + gut, the total flow through the duct is a pretty substantial 1500-2400ml per day.
Editor: Peter Wyllie

Why does it happen?o Traumatic
o Surgical – as in this case, it may occur from any cardiothoracic procedure + abdominal or neck operations.
o May also result from central lines, pacemaker insertion, and chest trauma. Has also been seen with iatrogenic infusion of TPN via central lines direct into thorax.
o Atraumatic o Malignancy – including lymphoma, pulmonary, mediastinal and metastatic cancerso Idiopathic ~ 6%o Miscellaneous including benign tumours, cirrhosis, thoracic aortic aneurysm, SLE,
TB, sarcoidosis, amyloidosis, venous thrombosis, heart failure
How do they present? Usually progressive dyspnoea – onset may be delayed 1-2 weeks. Chest pain and fever is uncommon, as the chyle does not produce a significant inflammatory response. Pleural effusion is unilateral in approximately 78 percent and involves the right hemithorax in 67 percent and left hemithorax in 33 percent.
What else could it be? The milky fluid suggests the presence of a may also be seen with a cholesterol pleural effusion, or an empyema. Cholesterol effusions are much less common than chylothoraces and contain a high concentration of cholesterol. These effusions typically occur in patients with thickened and sometimes calcified pleural surfaces in the setting of chronic pleural inflammation.However note that the appearance of fluid from a chylothorax may not always be milky. In a report reviewing 38 chylous pleural effusions as defined by the presence of chylomicrons, the pleural fluid was described as chylous (milky) in 47%, bloody in 26%, yellow turbid in 11%, green turbid 3%, and “other” in 13%. Thus consider in any patient with a persistent or recurrent pleural effusion of obscure aetiology that is turbid, bloody, or serosanguineous.
What do we test the fluid for? This depends on the clinical scenario. - The supernatant of the pleural fluid from a chylothorax typically fails to clear after
centrifugation, whereas “milky” appearing empyema fluid clears with centrifugation - White cells – usually > 80% lymphocytes- Triglycerides – strongly supported diagnosis if TG > 1.24mmol/L- Cholesterol level – usually low i.e. < 5.1 mmol/L- Other tests as dictated by the likely aetiology e.g. cytology, AFBs, culture
Treatment- Treat the underlying condition- Drain the pleura- Dietary control measures – something beyond the scope of the ED management but the aim
is to rest the thoracic duct. Fasting the patient or opting for a reduced fat diet especially long-chain triglycerides achieves this. This may be supplemented by TPN for more persistent cases.
- Pleurodesis- Thoracic duct ligation- Somatostatin or octretide- reduce flow of chyle- Pleuroperioneal or pleurvenous shunts - Thoracic duct embolisation
Refs: Up-to-date
PREGABALIN (LYRICA ®)
This is a medication that we are seeing and prescribing with increasing frequency and was recently reviewed in the most recent RADAR (Rational Assessment of Drugs and Research) publication. For the full version go to www.npsradar.org.au
Editor: Peter Wyllie

What is it? GABA analogue with analgesic, anticonvulsant, anxiolytic and sleep modifying activities
For who? As a treatment option for neuropathic pain which has not responded to other drugs. Note it is best used as part of a multifaceted, multidisciplinary, active approach. They add that the primary goal in most cases is to make the pain tolerable – not eliminate the pain. Consider other drugs first – couple of points regarding Lyrica
Superior to placebo for the treatment of neuropathic pain Limited evidence comparing pregabalin to amitrityline (Endep) & gabapentin (Neurontin)-
indirect comparisons suggest that it is non-inferior for efficacy and safety to amitrityline & gabapentin
Consider amitriptyline or nortriptyline as initial therapyo Established first line treatment for neuropathic pain yet TCAs are not approved by the
TGA for this indicationo Cheaper and easier to access o Can have adverse effects including anti-cholinergic effects (dry mouth, constipation,
retention) or CVS effects including postural hypotension, heart block and arrhythmias Gabapentin is an effective option yet it is not reimbursed by the PBS for this indication Consider pregabalin for neuropathic pain refractory to other drugs – dose dependent efficacy Consider combination therapy with 2 or more different drugs – yet may increase adverse
effects – e.g. COX 2 inhibitors Pain team review may be required
What’s the down side? Generally well tolerated with side effects in ~ 3% of patients (talking to those on the drug, I suspect the numbers are higher than this)
o Dizziness and drowsinesso Blurred vision, fatigue o Weight gaino Peripheral oedema, CCFo Depression and anxiety
Dosing – start 75mg bd increasing to 150mg bd after 3-7 days – note that it may take several weeks to achieve maximal effect. Dose reduction with renal impairment. Do not stop suddenly.
JOKE / QUOTE OF THE WEEK
FOR THOSE WHO LOVE THE PHILOSOPHY OF AMBIGUITY, AS WELL AS THE IDIOSYNCRASIES OF ENGLISH:
1. Don't sweat the petty things and don't pet the sweaty things.2. One tequila, two tequila, three tequila, floor.3. Atheism is a non-prophet organization.4. If man evolved from monkeys and apes, why do we still have monkeys and apes?5. The main reason that santa is so jolly is because he knows where all the bad girls live.6. I went to a bookstore and asked the saleswoman, "where's the self- help section?" she said if she told me, it would defeat the purpose.7. What if there were no hypothetical questions?8. If a deaf child signs swear words, does his mother wash his hands with soap?9. If someone with multiple personalities threatens to kill himself, is it considered a hostage situation?10. Is there another word for synonym?11. Where do forest rangers go to "get away from it all?" 12. What do you do when you see an endangered animal eating an endangered plant?13. If a parsley farmer is sued, can they garnish his wages?14. Would a fly without wings be called a walk?15. Why do they lock petrol station bathrooms? Are they afraid someone will clean them? 16. If a turtle doesn't have a shell, is he homeless or naked?
Editor: Peter Wyllie