-
7/30/2019 EMG Review Final Vandersluis
1/98
-
7/30/2019 EMG Review Final Vandersluis
2/98
Test question
Typical EMG findings in radiculopathy include
a) Low cmap and sensory responses; delayed / absent F wave,
and normal needle exam
b) Low cmap with normal sensory responses, delayed / absent
F
wave, and denervation in at least 2 related musclesc) Low cmap
with normal sensory responses, enlarged F wave,
and denervation in at least 2 related muscles
-
7/30/2019 EMG Review Final Vandersluis
3/98
-
7/30/2019 EMG Review Final Vandersluis
4/98
Components of an EMG
Left Median Motor
O
P
T
R
Wrist
O
P
T
R
Elbow
Left Median Sen Sensory
O
P
T R
2nd Digit
O
P
TR
3rd Digit
OP
T 4th Digit
O
P
T R
1st Digit
EMG - Left CervPara Mid
Nerve conduction studiesMotor nervesSensory nervesRepetitive
Stimulation
ElectromyographyQualitativeQuantitative
-
7/30/2019 EMG Review Final Vandersluis
5/98
Nerve Conduction Studies
Peripheral nerves are stimulated with a controlled
electrical stimulus
Responses are recorded Compound motor action potential
(CMAP)
Sensory nerve action potential (SNAP)
F wave
H reflex
-
7/30/2019 EMG Review Final Vandersluis
6/98
Left Median Motor
O
P
T
R
Wrist
O
P
T
R
Elbow
-
7/30/2019 EMG Review Final Vandersluis
7/98
Motor NCS Parameters Distal Latency
determined by conduction velocity of the nerve,
neuromuscular
junction & muscle
Amplitude
determined by number of muscle fibersactivated
Proximal conduction velocity
determined by conduction velocity of the fastest fibers
-
7/30/2019 EMG Review Final Vandersluis
8/98
Normal Median Motor Study
DL CV Amp
(msec) (m/s) (mV)
Wrist-APB 3.2 15.0
Elbow-Wrist 55 14.8
-
7/30/2019 EMG Review Final Vandersluis
9/98
-
7/30/2019 EMG Review Final Vandersluis
10/98
Sensory NCS Parameters
Onset and peak latencies
Conduction velocity
determined by velocity of a very few fast fibers
Amplitude determined by the number of large sensory fibers
activated
-
7/30/2019 EMG Review Final Vandersluis
11/98
Normal Median Sensory Study
1 msec/div
Latency CV Amp
(msec) (m/s) (uV)
Wrist-D2 2.2 58 44.1
-
7/30/2019 EMG Review Final Vandersluis
12/98
CASE 1
29 y.o. male
Acute right foot drop 4 weeks earlier
No trauma, no hx DM
EXAM: MRC 2/5 rt dorsiflex toes
4/5 rt ankle DF and eversion
Decr pp dorsum foot
Reflexes sym.
No tinel
s at fib head
-
7/30/2019 EMG Review Final Vandersluis
13/98
Where is lesion
Character (axonal, demyelinating)
prognosis
-
7/30/2019 EMG Review Final Vandersluis
14/98
.
-
7/30/2019 EMG Review Final Vandersluis
15/98
-
7/30/2019 EMG Review Final Vandersluis
16/98
-
7/30/2019 EMG Review Final Vandersluis
17/98
CASE 2
67 y.o. male
buttock pain to lat thigh, exac with ambulation
Few wks later rt foot drop
Exam: 4/5 rt foot df, eversion, pf 5-/5
Trace ankle reflexes
Decr sens on dorsum foot
SLR neg
-
7/30/2019 EMG Review Final Vandersluis
18/98
-
7/30/2019 EMG Review Final Vandersluis
19/98
F-wave study
small late response from a short duration supramaximal
stimulation.
It initiates an ant idromicmotorresponse to the spinal cord
followedby an or thodromicmotorresponse to the recording
electrode.
5% CMAP height
The configuration and latency change with each stimulation.
This is due to a polysynaptic response in the spinal cord,
whereRenshaw cells (R) inhibit impulses from traveling the same
path each
time.
-
7/30/2019 EMG Review Final Vandersluis
20/98
F Waves
Useful to assess proximal nerve to spinal cord
Helpful in the evaluation of:
Radiculopathy
Guillian-Barre Syndrome
Peripheral neuropathy
Other demyelinating neuropathies
-
7/30/2019 EMG Review Final Vandersluis
21/98
F Waves: Normal Median
-
7/30/2019 EMG Review Final Vandersluis
22/98
H- reflex study late response equivalent to achilles reflex.
Stimulate tibial
at popliteal fossa, pickup over soleus muscle
initiated with a submax stimulus at a long duration (0.51.0
ms).
preferentially activates the IA afferent nerve fibers(muscle
spindle sensory)
causing an or thodromicsensoryresponse to the spinalcord, and
then an or thodromicmotorresponse back tothe recording
electrode.
The morphology of wave pattern and latency remainsconstant
-
7/30/2019 EMG Review Final Vandersluis
23/98
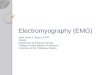
Muscle SpindleIa - responsive to the rate of change in muscle
length,
as well to change in velocity
http://en.wikipedia.org/wiki/File:MuscleSpindle.svg
-
7/30/2019 EMG Review Final Vandersluis
24/98
H Reflexes
Useful to assess proximal nerve conduction
Criteria: 50% diff in
amplitude)
Helpful in the evaluation of: Polyneuropathy
S1 radiculopathy
Upper Motor Neuron lesions
-
7/30/2019 EMG Review Final Vandersluis
25/98
Nerve Conduction Studies:Late Responses
F Wave Latency Retrograde rebound motor impulse
Travels full length of motor axon and back
Information about proximal segments
Limited sensitivity/specificity
H Reflex Afferent Path: Sensory axons (group Ia fibers)
Efferent Path: Motor Axons (alpha motor neurons)
Follows muscle stretch reflex arc
Side to side latency most valuable
-
7/30/2019 EMG Review Final Vandersluis
26/98
-
7/30/2019 EMG Review Final Vandersluis
27/98
DDX Small peroneal motor CMAPs normal sensory
No conduction block
Deep peroneal (spares sensory) vs L5
Absent peroneal F points proximal
Normal tibial CMAP + normal sural sensory
Eliminates tibial, sciatic or plexus
Some S1 involvement suggested
H reflex absent with normal M response
-
7/30/2019 EMG Review Final Vandersluis
28/98
-
7/30/2019 EMG Review Final Vandersluis
29/98
-
7/30/2019 EMG Review Final Vandersluis
30/98
Radiculopathy(Neuro-foraminal Stenosis from L-5 Disc
Herniation)
-
7/30/2019 EMG Review Final Vandersluis
31/98
-
7/30/2019 EMG Review Final Vandersluis
32/98
Radiculopathy(Electrodiagnostic Features)
Normal or low amplitude CMAP in corresponding
dermatome
Normal SNAP in corresponding dermatome Denervation in a
segmental myotomal distribution
(at least 2 muscles innervated by the same root
via more than one peripheral nerve) with or
without denervation of paraspinals
-
7/30/2019 EMG Review Final Vandersluis
33/98
http://www.google.com/url?sa=i&rct=j&q=dorsal%20root%20ganglia&source=images&cd=&cad=rja&docid=QaVeUXsDVfAwBM&tbnid=5LmCVD1eXWYH1M:&ved=0CAUQjRw&url=http://otah2o.wikispaces.com/09+Nervous+System&ei=ID8NUdbjAseH0QHWnYDYBw&bvm=bv.41867550,d.dmQ&psig=AFQjCNFV3yniGkFw633fCeXH2bdUvsA_5Q&ust=1359909020796331
-
7/30/2019 EMG Review Final Vandersluis
34/98
Needle Electromyography
Needle electrode is inserted into the muscle
Needle is disposable, single use
Multiple muscles are accessible for examination
Combination of muscles tested
Dependent upon clinical question
Level of discomfort is mild
-
7/30/2019 EMG Review Final Vandersluis
35/98
Needle Electromyography
Muscle is studied at rest and at different levels ofsustained,
voluntary contraction.
At rest, the muscle should be silent--any spontaneous
activity may signal a nerve or muscle abnormality.
During activity, the
electrical shape and
pattern of the responsecan distinguish
between nerve and
muscle disease.
-
7/30/2019 EMG Review Final Vandersluis
36/98
http://www.google.com/url?sa=i&rct=j&q=motor+unit+diagram&source=images&cd=&cad=rja&docid=_3l8DoY7wp_G0M&tbnid=Ia2LpycbobgtqM:&ved=0CAUQjRw&url=http://www.sciencedirect.com/science/article/pii/S1047965107000897&ei=2ZYNUdzIIpKF0QHmjYGgDw&bvm=bv.41867550,d.dmQ&psig=AFQjCNH_MwRz198zFlmDmaNyLSWYCDgxHA&ust=1359931410578948
-
7/30/2019 EMG Review Final Vandersluis
37/98
EMG - Motor Units
Evaluated during early recruitment
Morphologic parameters studied
Amplitude
Duration Phases
Rule of 5s: as increase effort each unit comes in at ~5hz,
and next added when previous firing ~10hz
-
7/30/2019 EMG Review Final Vandersluis
38/98
-
7/30/2019 EMG Review Final Vandersluis
39/98
Case 3
53 fem, progressive weak distal L hand No neck pain, numb, loss
of bowel, bladder
PHx: dm x 8years, smoker, htn; no sig fhx
Exam: atrophy intrinsics LH
Brisk reflexes UE, and rt babinski present
Normal sens, cerebellar, gait
Init inv: mri c/s mild disk bulging. Emg lt c7-t1 radic.
EMG IS REPEATED AT 7M
-
7/30/2019 EMG Review Final Vandersluis
40/98
-
7/30/2019 EMG Review Final Vandersluis
41/98
-
7/30/2019 EMG Review Final Vandersluis
42/98
EMG - Denervation Recruitment is the pattern of motor unit
firing when a
muscle contracts
Reduced - less motor units to draw upon
Configuration size and shape:
Large Amplitude more that normal # nerve fibers
Large Duration nerve fibers timing is variable
-
7/30/2019 EMG Review Final Vandersluis
43/98
Needle Electromyography:Neurogenic Motor Unit
EMG - Left VastusLat
This unit demonstrates:
Reduced recruitment
Increased amplitude Increased duration
Polyphasia
-
7/30/2019 EMG Review Final Vandersluis
44/98
-
7/30/2019 EMG Review Final Vandersluis
45/98
Reinnervation collateral
sprouting
-
7/30/2019 EMG Review Final Vandersluis
46/98
-
7/30/2019 EMG Review Final Vandersluis
47/98
Needle Electromyography:Muscle at rest
Insertional Activity
Burst of electrical activity as needle is inserted into
muscle
Due to disruption of muscle fiber membranes Prolonged with
denervation, some muscle diseases
Spontaneous Activity
Fibrillations, positive sharp waves, fasciculations
Hallmark of denervation, muscle membrane irritation
-
7/30/2019 EMG Review Final Vandersluis
48/98
Needle Electromyography:Grading of Spontaneous Activity
100 V 10 ms
EMG - Left AntTibialis
0 No Fibs/PSWs
+/- Fibs/PSWs that are not persistent
1+ Persistent Fibs/PSWs in at least 2 areas
2+ Persistent Fibs/PSWs of moderate #s in three or more
areas
3+ Persistent Fibs/PSWs of large #s but not obscuring
baseline
4+ Baseline obliterated in all areas examined
1+ 2+ 3+ 4+
-
7/30/2019 EMG Review Final Vandersluis
49/98
Spontaneous Muscle Electrical Activity
Examples:
Fibrillation potential/positive waves
indicates loss of muscle-nerve connection
provides information about the chronicity of the problem
Fasciculation
spontaneous motor unit potential, may indicate irritability in
the motor
nerve cell
-
7/30/2019 EMG Review Final Vandersluis
50/98
-
7/30/2019 EMG Review Final Vandersluis
51/98
Fasciculation
-
7/30/2019 EMG Review Final Vandersluis
52/98
-
7/30/2019 EMG Review Final Vandersluis
53/98
-
7/30/2019 EMG Review Final Vandersluis
54/98
Case 4
76 healthy female, progressive LE numb / wk 1 year
Imbalance cane walker
Recent involvement of hands
Exam: Motor: grip 4+, hip flex 4, dorsiflex 4-
Sens: marked loss vib and proprioception feet
Areflexic
Gait wide-based; pos Romberg
-
7/30/2019 EMG Review Final Vandersluis
55/98
-
7/30/2019 EMG Review Final Vandersluis
56/98
-
7/30/2019 EMG Review Final Vandersluis
57/98
-
7/30/2019 EMG Review Final Vandersluis
58/98
-
7/30/2019 EMG Review Final Vandersluis
59/98
Needle 19
-
7/30/2019 EMG Review Final Vandersluis
60/98
Summary
Sensorimotor polyneuropathy
Cmap loss >> denervation
Conduction blocks
Sig slowing
Few fibrillation potentials, some larger unit ->
predominately chronic
-
7/30/2019 EMG Review Final Vandersluis
61/98
DDX Chronic acquired demyelinating
neuropathy CIDP +/- early HIV
Multifocal motor NP with conduction block
Anti MAG, monoclonal gammopathy,
MGUS, osteosclerotic myeloma (POEMS syn)
Multiple myeloma, Waldenstroms
Castelmans
Amyloidosis
-
7/30/2019 EMG Review Final Vandersluis
62/98
Electrodiagnosis provides
Confirmation of neuropathy
Eg vib loss in np vs post cord
Fiber type sens, motor, both
Pathology demyel vs axonal
Chronicity and activity
-
7/30/2019 EMG Review Final Vandersluis
63/98
Test question
Typical EMG findings in radiculopathy include
a) Low cmap and sensory responses; delayed / absent F wave,
and normal needle exam
b) Low cmap with normal sensory responses, delayed / absent
F
wave, and denervation in at least 2 related musclesc) Low cmap
with normal sensory responses, enlarged F wave,
and denervation in at least 2 related muscles
-
7/30/2019 EMG Review Final Vandersluis
64/98
The End
-
7/30/2019 EMG Review Final Vandersluis
65/98
-
7/30/2019 EMG Review Final Vandersluis
66/98
Limitations of NCSs/EMG
Generally not helpful in the evaluation/diagnosis of:
Pain from joint disease
Fibromyalgia or myofascial pain syndromes
Central nervous system disorders
Disorders that do not arise from the neuromuscular system
-
7/30/2019 EMG Review Final Vandersluis
67/98
What to Expect From an
EMG Report
A clinically and physiologically
relevantinterpretation/diagnosis
An outline of the localization, severity, and acuity of the
process Notation of other diagnoses that are
detected/excluded
Explanation of any technical problems
-
7/30/2019 EMG Review Final Vandersluis
68/98
What to Expect From an
EMG Report
The reason for the referral is addressed
Pertinent information that may affect management is
provided Need for re-evaluation in the future
Urgent need for medical intervention
-
7/30/2019 EMG Review Final Vandersluis
69/98
What to Expect From an
EMG Report
Data obtained during the study: (NCS)
Amplitude
Distal latency
Distance
Conduction velocity
Normal (Reference) data
Side-to-side comparison (when appropriate)
Limb temperature during the study
-
7/30/2019 EMG Review Final Vandersluis
70/98
-
7/30/2019 EMG Review Final Vandersluis
71/98
What to Expect From an
EMG Report
Data obtained during the study: (EMG)
Presence & type of abnormal spontaneous activity
Motor unit recruitment
Motor unit morphology
-
7/30/2019 EMG Review Final Vandersluis
72/98
EMG Pearls
Electrodiagnostic studies are a supplement to, and not
areplacement, for the history and physical examination
Electrodiagnostic results are often time-dependent
Electrodiagnostic studies are not standardized
investigations and may be modified by the practitioner toanswer
the diagnostic question
-
7/30/2019 EMG Review Final Vandersluis
73/98
-
7/30/2019 EMG Review Final Vandersluis
74/98
Specialized EDX Testing
Interference pattern analysis
Quantitative motor unit analysis
Single fiber analysis
Segmentation studies
Cranial nerve testing
Brainstem and somatosensory evoked potentials
Pelvic floor and respiratory muscles
-
7/30/2019 EMG Review Final Vandersluis
75/98
Outline
What conditions are commonly evaluated/diagnosed byNCSs/EMG?
What are the technical details of these studies?
What are some limitations of EMG studies?
What can I expect from an EMG report?
What are the indications for
-
7/30/2019 EMG Review Final Vandersluis
76/98
What are the indications for
electrodiagnostic
consultation/testing?
Suspected neuromuscular disease
nerve root pathology
peripheral nerve/plexus pathology
neuromuscular junction pathology
muscle pathology
-
7/30/2019 EMG Review Final Vandersluis
77/98
What is the value of NCSs/EMG?
Confirm the clinical impression of a neuromuscular
disorder
Rule out certain diagnoses
Enhance patient care
-
7/30/2019 EMG Review Final Vandersluis
78/98
Value of NCSs/EMG
When neuromuscular disease is present,electrodiagnostic testing
can:
Clarify the type of pathology (i.e. neuropathy
vs myopathy)
Determine severity & extent of pathology
Confirm site of pathology
Estimate chronicity of pathology
Complaints Suggestive of
-
7/30/2019 EMG Review Final Vandersluis
79/98
Complaints Suggestive of
Neuromuscular Pathology
Numbness or Tingling
Decreased Sensation
Pain or Cramping
Weakness
Gait difficulty
Fatigue
-
7/30/2019 EMG Review Final Vandersluis
80/98
Disorders Diagnosed/Evaluated by
NCSs/EMG Generalized Neuropathies
Axonal
DemyelinatingAcquired
Acute: GBS
Chronic: CIDP
Hereditary
Mixed Diabetic sensorimotor neuropathy
-
7/30/2019 EMG Review Final Vandersluis
81/98
Polyneuropathies
Polyneuropathies associated with many medicalconditions
Multiple investigations often needed
NCSs/EMGs: best initial test to clarify underlying
pathophysiology (i.e., axonal vs demyelination)
Results may help focus rest of work-up
-
7/30/2019 EMG Review Final Vandersluis
82/98
Disorders Diagnosed/Evaluated by
NCSs/EMG
Mononeuropathy multiplex
Vasculitic/ischemic neuropathies
Demyelinating neuropathies
Infectious neuropathies
Neoplastic infiltration
Granulomatous infiltration Compression neuropathy
-
7/30/2019 EMG Review Final Vandersluis
83/98
Disorders Diagnosed/Evaluated by
NCSs/EMG Focal Neuropathies
Carpal Tunnel Syndrome (median neuropathy at the wrist)
Ulnar Neuropathy Peroneal Nerve Palsy
Others: brachial plexus lesions, tarsal
tunnel syndrome, etc.
-
7/30/2019 EMG Review Final Vandersluis
84/98
Disorders Diagnosed/Evaluated by
NCSs/EMG Radiculopathy
Cervical
Lumbar
Motor Neuron Disease
Amyotrophic lateral sclerosis (ALS)
Spinal muscular atrophy (SMA)
Di d Di d/E l t d b
-
7/30/2019 EMG Review Final Vandersluis
85/98
Disorders Diagnosed/Evaluated by
NCSs/EMG Muscle Disease
Inflammatory
Polymyositis, Dermatomyositis Metabolic
Hereditary or Congenital
-
7/30/2019 EMG Review Final Vandersluis
86/98
Disorders Diagnosed/Evaluated by
NCSs/EMG
Neuromuscular Junction Disease
Myasthenia Gravis
Lambert Eaton Myasthenic Syndrome
Botulism
Medications
Di d Di d/E l t d b
-
7/30/2019 EMG Review Final Vandersluis
87/98
Disorders Diagnosed/Evaluated by
NCSs/EMG Generalized weakness in the critical care setting
Acute/unexplained onset of respiratory failure
Neuromuscular cause for failure to wean from
mechanical ventilation
Neuromuscular diseases unique to critical care
setting Critical illness neuropathy/myopathy
Disorders Evaluated/Diagnosed by
-
7/30/2019 EMG Review Final Vandersluis
88/98
Disorders Evaluated/Diagnosed by
NCSs/EMG
Specialized electrodiagnostic expertise can be useful in
evaluation of:
Ocular muscle weakness
Speech difficulties due to weakness of laryngeal muscles
Disorders of movement and tone from central nervous system
disorders
-
7/30/2019 EMG Review Final Vandersluis
89/98
Neuromuscular Junction Testing
Repetitive Nerve Stimulation
Stimulate nerve with train of supramaximal stimuli before and
after
exercise
Record from muscle
Attention to technical factors important
More sensitive recording from proximal muscles
Repetitive Nerve Stimulation:
-
7/30/2019 EMG Review Final Vandersluis
90/98
3Hz stimulation
Repetitive Nerve Stimulation:Normal
-
7/30/2019 EMG Review Final Vandersluis
91/98
-
7/30/2019 EMG Review Final Vandersluis
92/98
F-wave study (continued..)
-
7/30/2019 EMG Review Final Vandersluis
93/98
This is not a reflex, because action potentials travels from
the
site of the stimulating electrode in a limb to the spinal cord
and
back to the limb in the same nerve that was stimulated. The F-
waves latency can be used to derive the conduction
velocity of nerves between the limb and spinal cord, whereas
the motor and sensory nerve conduction study in the same
segment of the limb. Conduction velocity is derived by measuring
the limb length in
millimeters from the stimulation site to the corresponding
spinal
segment (ex: C7 spinous process to wrist crease for median
nerve).
This is multiplied by 2 as it goes to the cord and returns to
the
muscle.
Limitation: This evaluates a long neural pathway, which can
dilute focal lesions and hinder specificity of injury location.
It
Radiculopathy
-
7/30/2019 EMG Review Final Vandersluis
94/98
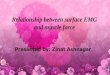
Radiculopathy(Spontaneous Activity)
EMG - Right LumbPara Mid Fibrillation potentials
Positive sharp waves
Fasciculations
Complex repetitive
discharges
Myokymia (rare)
Myotonia (rare)
Positive Sharp Wave
Complex Repetitive Discharge
Fibrillation Potential
Needle Electromyography:
-
7/30/2019 EMG Review Final Vandersluis
95/98
Needle Electromyography:Parameters Evaluated
Motor Unit Configuration Muscle is volitionally activated at
different force levels
Single motor units are assessed
Single motor unit: A motor axon and all its muscle fibers
Motor Unit Configuration: Amplitude, Duration, Morphology
Motor Unit Recruitment Pattern of motor unit activation with
increasing volitional activation
Interference Patterns Motor unit pattern with full voluntary
activation
Needle Electromyography:
-
7/30/2019 EMG Review Final Vandersluis
96/98
Needle Electromyography:Parameters Evaluated
Insertional activity
Spontaneous activity
Motor unit configuration
Motor unit recruitment
Interference pattern
Needle Electromyography:
-
7/30/2019 EMG Review Final Vandersluis
97/98
Needle Electromyography:Spontaneous Activity
EMG - Right LumbPara Mid Fibrillation potentials
Positive sharp waves
Fasciculations
Complex repetitive
discharges
Myokymia
Myotonia
Positive Sharp Wave
Complex Repetitive Discharge
Fibrillation Potential
-
7/30/2019 EMG Review Final Vandersluis
98/98