Embed Size (px)
Citation preview

Thorax (1964), 19, 492.
Empyema and ruptured lung abscess in adults'ROWAN NICKS
From the Thoracic Surgical Unit, Page Chest Pavilion, Royal Prince Alfred Hospital, Melbourne
This brief annotation concerns 18 adult patientswith empyema complicating the rupture of a lungabscess into the pleural cavity who were referredto my service during the period 1957 to 1962.By different methods of treatment all these
patients have been returned to health, but in someearlier cases the illness was painful and prolongedand multiple operations were necessary to attaina final cure.These are compared with patients treated
recently in whom convalescence has been rapid,uncomplicated, and without loss of tissue.
CLINICAL MATERIAL
Particulars relevant to the treatment of 18 patientscomprising the series are summarized in Table I.
TABLE IEMPYEMA COMPLICATING INTRAPLEURAL RUPTURE OF
LUNG ABSCESS IN ADULTS, 1957 TO 1962
Total no. of cases 18Died. 0Final cure .. .. .. 18
Culture:Sterile. 7Infected .. .. .. 1 1
Organisms isolatedPneumococcus..Staphylococcus aureusHaemolytic streptococcusMixed Streptococcus viridans and
Staphylococcus albus ..
242
3
All patients were treated by antibiotics to whichsensitivity had been ascertained. It was notpossible to differentiate those in whom theabscess resulted from aspiration from those inwhom it complicated a pneumonic infection.
Eleven were infected at the time of presentationand seven were sterile. From the infected casesa mixed variety of pathogenic organisms werecultured.
RESULTS
The results of treatment are summarized inTable II.
I Delivered to the General Scientific Session, Royal AustralasianCollege of Surgeons, Melbourne, in May 1963
TABLE IIRESULTS OF TREATMENT
No. Cure No Cure
Medical treatmentAntibiotics .. 18
Primary surgical treatmentDrainage:
Infected.9 2 7Sterile. I
Primary decorticationNon-infected 5 5Infected .. 2 I I
Primary pleuro-resection .. 1
Total .. .. 18 10 8
A cure followed simple drainage in three of10 patients.Five sterile cases treated by primary decortica-
tion were cured, and, of two infected cases, onerecurred.
In the one with a localized empyema treatedby pleurolobectomy and thoracoplasty, a cureresulted.Primary surgery failed to achieve a cure in eight
patients, and secondary procedures wereperformed for these (Table III).
TABLE IIIRESPONSE TO SECONDARY SURGICAL PROCEDURES
No. Cure No Cure
Secondary treatmentTotal cases .. 8Decortication 5 2 3Pleuro-pneumonecton-y 2 1 IPleuro-lobectomy I
Tertiary treatmentSaucerization, closure of fis-
tula and muscle graft .. 3 3Pleuro-pneumonectomy .. 2 2
Quarternary treatmentThoracoplasty .. .. 2
Procedure 5Muscle graft and closure offistula.2 2
Of five patients subjected to decortication, twowere cured; in both, the fistula was closed andthe abscess cavity was marsupialized with the
492
copyright. on M
arch 22, 2020 by guest. Protected by
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.19.6.492 on 1 Novem
ber 1964. Dow
nloaded from

Empyema and ruptured lung abscess in adults
chest wall. Of three patients submitted topleuroresection, one of two was cured bypleuropneumonectomy and one failed withpleurolobectomy.
In tertiary treatment, saucerization of alocalized empyema, followed after an interval bysuture of the fistulae and the insertion of avascular muscle graft, was finally successful in allpatients.Pleuropneumonectomy was not successful in
two patients due to re-infection and to theoccurrence of a broncho-pleural fistula in one ofthese.
In the patients referred to above, total thoraco-plasty was palliative, and cure was only achievedby saucerization and closure of the fistulae bysuture and muscle grafting as described (Fig. 1).
COMMENT
The rupture of a lung abscess complicating astaphylococcal pneumonia or aspiration is not anuncommon event. Convalescence is often long andcomplicated.
It is fortunate that the infecting organisms aresensitive to antibiotics in most cases.
a b
L~~~~~~~~~~~~~
d e
It is significant that simple drainage was un-successful in seven of nine persistently infectedcases.
Decortication was successful in five uninfectedcases (including three with an open abscess cavityand fistulae at the time of operation) and in oneof two infected cases. In this latter group, dTbride-ment of the necrotic abscess, closure of thefistulae, and marsupialization of the closed abscessabove a soft drainage tube withdrawn through thechest wall was performed. Healing took placewithout complication. Treatment of one otherpatient treated in this way failed because of thedevelopment of osteomyelitis in a rib bared atoperation.Drainage and saucerization are wisely used as
temporary procedures in doubtful cases until theinfection has subsided and it is possible to studythe architecture of the remaining lung.
It appears that pleurolobectomy or pleuro-pneumonectomy should be reserved for localizedlesions with lobar or pulmonary suppuration.
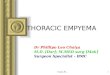
Secondary closure of fistulae in healthygranulating tissue supported by a muscle grafton the surface has been found to be a safe andsatisfactory operation (Fig. 1).
C
f 9FIG. 1. Diagrammatic representation of operation for sealing of bronchial fistula: (a)Incision, (b) saucerization of empyema cavity, cuffing of the fistulae; (c) suture of fistulaein two layers; (d) muscle flap as a secondary seal; (e) final closure with small drainagetube in position; (f) pressure pad; (g) arm in sling.
493
copyright. on M
arch 22, 2020 by guest. Protected by
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.19.6.492 on 1 Novem
ber 1964. Dow
nloaded from

Rowan Nicks
PRECIS OF ILLUSTRATIVE CASE HISTORIES
CASE 1 S. McH., aged 34 years. Diagnosis: Rupturedright lung abscess, d6bridement, decortication, andmarsupialization (Fig. 2).She was seven months pregnant when she devel-
oped right chest pain and rigors. The condition wasdiagnosed as pneumonia and she was treated for thiswith broad-spectrum antibiotics. She developedsudden dyspnoea one week later.On examination when admitted to the Page Chest
Pavilion on July 4, 1962, she was toxic and breath-less. The chest radiograph showed collapse of theright lung and a pleural effusion.
Fluid aspirated from the chest was inflammatoryand sterile on culture. Ruptured hydatid cyst wassuspected but the hydatid complement fixation andCasoni tests were negative. Thoracotomy performedshortly after admission revealed intrapleural ruptureof a gangrenous lung abscess in the anterior segmentof the right lung.The outer necrotic abscess wall was excised and all
gangrenous tissue was removed. Several large fistulaewere closed with catgut, and the lung was decorti-cated. The abscess cavity was partially closed about asoft catheter which was withdrawn through the chestwall, and the lung was sutured to the parietal pleuraat the point of exit. The chest was closed in the
..e... ...
.....* . ,=-e > t i ':S.:.: ..:..
:.''..::.
E)
FIG. 2. Case 1. (a) Right pleuro-pneumonia with cavitation ofthe right upper lobe; (b) right tension pneumothorax andempyema; (c) after decortication and debridement and marsupialization. The catheter is in position; (d) sinogramshowing obliteration of the cavity and small bronchial fistulae which sealed spontaneously on withdrawal.
AC9A
||l.
... s
..-aVW
copyright. on M
arch 22, 2020 by guest. Protected by
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.19.6.492 on 1 Novem
ber 1964. Dow
nloaded from

Einpyema and riiptured lung abscess in aduilts
(a) (b)
(') (d)FIG. 3. Case 2. (a) Left pneumothorax and empyema; (b) recurrent pyopneumothorax; (c) after decortication,debridement, and marsupialization. The catheter is in position; (d) final radiograph with restoration of lung.
usual way with two tubes connected to underwatersuction. The lung expanded and the wound healedby first intention. Premature labour pains were con-trolled successfully by diuadilan. The drainage fromthe intracavitary tube soon ceased. After verifying bya sinogram that there was no abscess cavity and thatthe trace merely led to small pulmonary fistulae, thetubes were removed. She remains well and withoutsymptoms.
2R
CASE 2 K. R., aged 40 years. Diagnosis: Rupturedlung abscess, debridement, decortication, and mar-supialization (Fig. 3).
This patient was admitted to the Page Chest Pavi-lion on September 29, 1962, with an infected lungabscess and empyema thoracis.He had had a pyrexial illness 10 days before admis-
sion for which he was treated by broad-spectrum anti-biotics. He developed sudden dyspnoea four days
495
copyright. on M
arch 22, 2020 by guest. Protected by
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.19.6.492 on 1 Novem
ber 1964. Dow
nloaded from

Rowan Nicks
later and was treated for spontaneous pneumothoraxby an apical intercostal catheter connected to under-water drainage.On admission the chest radiograph showed an
empyema in the left lower chest with an air fluidlevel indicating a bronchopleural fistula. Pus grewmixed organisms from which Staphylococcus albus,Streptococcus viridans, and non-haemolytic strepto-cocci were isolated.At operation, apart from a thick-walled fibrous
empyema, an abscess with bronchial fistulae was
found in the left lower lobe. Decortication was per-formed, and the necrotic top of the abscess in thelower lobe was removed, the fistulae were sutured,and the wall was closed about a soft drainage tubewhich was withdrawn through the chest wall andsutured to the parietal pleura to prevent an escapeof air into the pleural cavity.The chest was closed by two underwater drainage
tubes. The lung expanded, and finally the marsupial-ized tube was removed. Three weeks later the dis-charge stopped, the culture was sterile, and the
FIG. 4. Case 3. (a) Ruptured right lung abscess withpyopneumothorax; (b) bronchogram showing abscess inapical segment of the lower lobe; (c) deibridement andmarsupialization; (d)final bronchogram which is essentiallynormal.
496
copyright. on M
arch 22, 2020 by guest. Protected by
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.19.6.492 on 1 Novem
ber 1964. Dow
nloaded from

Empyema and ruptured lung abscess in adults
abscess obliterated except for a small broncho-cutaneous fistula. This closed when the tube wasremoved and has remained healed.
CASE 3 J. S., aged 55 years. Diagnosis: Rupturedlung abscess, debridement, decortication, andmarsupialization (Fig. 4).
This patient was admitted to Page Chest Pavilionin November, 1957, with empyema and intrapleuralrupture of an abscess of the right lower lobe of thelung, after a pneumonic attack six weeks previously.He was coughing up profuse pus. The pus aspiratedfrom the empyema and cultures showed sparsecolonies of pneumococci. He was treated with broad-spectrum antibiotics and chloramphenicol.A chest radiograph showed an empyema and con-
solidation of the right lower lobe. A bronchogramoutlined the walls of an oval cavity in the apicalsegment.At operation on December 13, 1957, there was a
foul organizing fibrinous empyema cavity with thickwalls and a resolving abscess of the apical segmentof the lower lobe with several bronchopleural fistulae.The lung was decorticated, and, after necrotic tissuehad been removed from the surface of the abscess,a soft drainage tube was stitched in place andbrought through the chest wall, the point of exitfrom the pleura being marsupialized to the chest wallby sutures to prevent collapse of the lung. The chestwas closed in the normal way with two underwaterdrainage tubes and suction.
Healing was uneventful and the temporary fistulaehealed rapidly.
CASE 4 G. R., aged 42 years. Diagnosis: Rupturedlung abscess, debridement, decortication, andmarsupialization; osteomyelitis of the ribs (Fig. 5).
This man was admitted to Page Chest Pavilionwith empyema necessitatis after the intrapleural rup-ture of a lung abscess. He had been unwell withrigors and malaise for some weeks and had developedhaemoptysis and a cough some days previously. Thechest radiograph showed a total empyema, and chestaspiration revealed pus which grew anaerobic strepto-cocci on culture.At thoracotomy on September 13, 1958, the pleural
cavity was seen to be filled with green offensive puscontaining large clots of fibrin. There was an abscess2 cm. in diameter in the apex of the lower lobe.Partial decortication was carried out, a tube wasinserted into the abscess crater, and the empyemawas drained.On January 16, 1959, he was re-admitted with
recurrent empyema and chronic osteomyelitis of therib which had been bared at operation. The over-lying ribs were excised, and the overlying thickparietal pleura (up to 1 cm.) was excised to saucerizethe cavity. A large vascular muscle graft was insertedto seal off the raw area. The wound healed rapidlyand has remained so. The patient is without disability.
Comment The osteomyelitis of the rib wasdirectly related to the stripping of the periosteumat the first operation and would not have occurredif the rib had been excised. The muscle graft wassuccessful in permanently sealing the empyemaand there is now no abnormality in the lungparenchyma.
CASE 5 M.B., aged 52 years. Diagnosis: Rupturedright lung abscess, recurrent after decortication(Fig. 6).
This man was admitted to Page Chest Pavilion onOctober 18, 1960, with a temperature of 102° F.He was in distress from dyspnoea and stated that hehad developed a sudden chest pain at work two weekspreviously. He had been treated by bed rest andchloramphenicol during this period.The chest radiograph showed a right pneumothorax
with multiple fluid levels. and aspirated pus grew ahaemolytic staphylococcus on culture.At thoracotomy on October 27, 1960, a thick-walled
empyema containing fibrinous lumps was found, anddecortication was performed with difficulty. Thelung expanded immediately and the wound healed.Six weeks later he again developed malaise, rigors,and cough with sputum.The chest radiograph revealed a localized cavity
with a fluid level. Pyogenic staphylococci were iso-lated on culture of the sputum.At operation segments of the overlying ribs were
removed, and the empyema containing bronchialfistulae was saucerized. This healed and epithelial-ized; but five weeks later, on July 12, 1961, persistentfistulae which were troublesome were finally suturedand supported by a muscle graft.
Comment Decortication failed in the presence ofinfection. The abscess was not marsupialized.
CASE 6 I. C., aged 60 years. Diagnosis: ruptured leftlung abscess, saucerization and subsequent closure offistulae and muscle graft.
This patient was admitted to Page Chest Paviliontwo weeks after discharge from the Royal PrinceAlfred Hospital where he had received treatmentfor duodenal ulceration. He had developed a coughand green purulent sputum. The chest radiographshowed a left lower empyema with an air fluid levelindicating broncho-pleural fistulae. Culture of pusaspirated from the chest revealed staphylococci andscanty coliform organisms sensitive to streptomycinand chloramphenicol.Thoracotomy on December 19, 1958, revealed a
thick-walled empyema containing lumps of fibrin anda large abscess cavity in the apex of the lower lobecontaining broncho-pleural fistulae.The empyema cavity was carefully cleaned and
drained by rib resection. The cavity became progres-sively smaller but the fistulae persisted. The cavitywas saucerized. The fistulae were enclosed, and the
497
copyright. on M
arch 22, 2020 by guest. Protected by
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.19.6.492 on 1 Novem
ber 1964. Dow
nloaded from

Rowan Nicks
j
FIG. 5. Case 4. (a) Tube draining right chest, after decortication and marsupialization of abscess in right lowerlobe accompanied by pyopneumothorax and empyema; (b) persistent sinus; (c) origin of sinus from the bed of theeighth rib, bared ofperiosteum at thoracotomy; (d) final bronchogram essentially normal.
bare granulation tissue was sealed off by a musclegraft on January 29, 1959. The wound healed rapidlyand has remained healed.
Comment It is probable that this patient wassuffering from an unsuspected lung abscess whenhe entered hospital but that this gave symptomsonly when it ruptured into the pleural cavity.Relief was immediate after drainage but cure was
attained only after saucerization and later closureof the fistulae supported by a muscle graft.
CASE 7 A. L., aged 46 years. Diagnosis: Rupturedlung abscess; pleuro-lobectomy (Fig. 7).
This patient was admitted to the Page ChestPavilion in March, 1960, with a left upper lobarabscess and localized empyema. He stated that thephysical illness which had come on one month
498
.Xa.9.
copyright. on M
arch 22, 2020 by guest. Protected by
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.19.6.492 on 1 Novem
ber 1964. Dow
nloaded from

Empyema and ruptured lung abscess in adults
(a)
z!w
_ws tS_at.
.::
.j_^w°' . ....w ...... e__ !A:X:S S ! w X_lE .+ { . :.::
:.o .: .....i::r&.o -:-:f.. : :*%_S ........ .. ...
='' 'Ss
w.. *;.dio.-,o2li:<.
: Ji,!
.
e(6)
_
(c) (d)FIG. 6. Case 5. (a) Pyopneumothorax; (b) after decortication, debridement, and closure of the abscess cavitywithout marsupialization. Small residual pneumothorax persists; (c) after six weeks, showing recurrent empyemaand bronchial fistula; (d) essentially normal chest radiograph after saucerization and delayed closure of fistulaeand muscle graft.
previously had been treated by his doctor with anti-biotics. During the previous two weeks he had beencoughing up large amounts of pus. He was ill anddrawn with a pulse rate of 100 and temperatureswinging to 101° F. The chest radiograph showed a
thick-walled abscess localized to the posterior axillarysegment of the right upper lobe. On culture theaspirated pus grew mixed organisms including Micro-coccus catarrhalis.
At operation on April 24, 1960, a localizedempyema cavity communicating with a large thick-walled abscess containing broncho-pleural fistulaewas encountered. Upper pleurolobectomy wascarried out with great difficulty and a thoracoplastywas performed.He made a good recovery, but his activity remains
restricted from chronic bronchitis and obstructiveairway disease.
4i99
4w.
.,l.Appm:k-7,AL.AMAM,116-.. ,::
W.,I -IOW46.
..V.-
copyright. on M
arch 22, 2020 by guest. Protected by
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.19.6.492 on 1 Novem
ber 1964. Dow
nloaded from

Rowan Nicks
:b
.I.
41.
Wt
d
FIG. 7. Case 7. (a) Pleuro-pulmonary abscess of left upper lobe; (b) abscess with fluid level in posterior segmentof upper lobe outlined by bronchogram; (c) after pleurolobectomy and thoracoplasty; (d) operation specimen ofthick-walled empyema connecting with abscess cavity.
CASE 8 S. A.. aged 66 years. Diagnosis: Pleuro-pneumonectomy for lung abscess and empyema com-plicated by tuberculosis.
This man was admitted to the Page Chest Pavilionon October 27, 1958, with an empyema and a
broncho-pleural fistula after intrapleural rupture of a
lung abscess. Pus was removed by pleural aspirationand grew non-haemolytic streptococci on culture. Hewas treated with terramycin and erythromycin. Rib
resection and drainage was performed four days later.Within four weeks of removal of the drainage tubethe empyema recurred with pyrexia and cough withpurulent sputum.
During decortication an unsuspected apical tuber-culous cavity was opened and pleuropneumonectomywas performed.He made a straightforward recovery and has
remained well since.
500
.,4 ;-..--'., -0t.
.1
copyright. on M
arch 22, 2020 by guest. Protected by
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.19.6.492 on 1 Novem
ber 1964. Dow
nloaded from

Empyema and ruptured lung abscess in adults
Comment A permanent cure was not obtainedby drainage. After opening the tuberculous cavityit was necessary to perform pleuropneumo-nectomy despite the risk.A cure might have been obtained more safely
by saucerization.
CASE 9 T. T., aged 47 years. Diagnosis: Rupturedgangrenous lung abscess, putrid empyema, sauceriza-tion, pleuropneumonectomy, thoracoplasty, stomaformation. and muscle graft (Fig. 8).
This man was admitted to the Page Chest Pavilionfrom sea; he was greatly shocked. He gave a history
f -.-Oo(
of a serious illness which had developed during avoyage from India.The chest radiograph showed an extensive opacity
of the right lower zone and infiltration of the upperzone of the right lung.Soon after admission a putrid empyema containing
much gangrenous lung was evacuated and theddbrided cavity was saucerized on to the skin afterremoval of the overlying ribs.A Staphylococcus pyogenes infection was treatud
with chloramphenicol and erythromycin.After a period of partial recovery large amounts of
purulent sputum continued to be expectorated. Theorganism was sensitive only to erythromycin; it was
(b)
.I
(c) (d)FIG. 8. Case 9. (a) Right pyopneumothorax with multiple abscesses; (b) after debridement and saucerization of aruptured gangrenous lung abscess in the lower lobe under antibiotic cover. Residual abscess in upper lobe resistant toantibiotics; (c) total empyema after pleuropneumonectomy and thoracoplasty; (d) successful cure by large 'whale tail'muscle graft.
1
501
copyright. on M
arch 22, 2020 by guest. Protected by
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.19.6.492 on 1 Novem
ber 1964. Dow
nloaded from

Rowan Nicks
resistant to penicillin, streptomycin, aureomycin,chloramphenicol, and terramycin.
It was clear that he would die unless the lung,which was shown to have residual abscesses in theupper and middle lobes as well as on the largelydestroyed lower lobe, was excised. This was donesuccessfully.
Total empyema resistant to all antibiotics super-vened, and thoracoplasty was performed.The residual cavity was widely opened by the
excision of remaining osteomyelitic rib segments,and the skin was sutured to the pleura.
Three weeks later the granulating cavity was closedsuccessfully by a giant muscle flap. The patientremained healed and free of cough and wasrepatriated to India three months later.
SUMMARY
In the acute stage of an.infective illness withpyopneumothorax and bronchopleural fistula, itis necessary to treat the pneumonic condition andto provide local physiological conditions forrecovery by two closed drainage tubes, an apicalto allow expansion of the lung, and a basal fordrainage.
It is not safe to perform resection in thepresence of acute infection.
In the subacute stage, when the lung infectionis controlled or is in a healing phase, it is safeto perform decortication provided any cavity withfistulae is debrided, the fistulae closed if suitablefor closure, and the residual cavity closed abouta tube brought through the chest wall, the lungbeing sutured to the pleura at this point. If thereis no residual abscess, healing will occur.
In chronic cases with localized empyema andwith residual bronchial fistulae, provided the lungarchitecture is normal and there is no residuallung suppuration, a satisfactory and safe surgicaltechnique recommended is to saucerize the cavityand, after an interval at a time when the surfaceis granulating, to suture the fistulae and supportthis suture line with a muscle graft.
In some cases where there has been gross lungdamage and a residual abscess cavity, it may benecessary to perform pleurolobectomy or pleuro-pneumonectomy, but caution is advised, for thepossibility of infection in the dead space is a realone.
REFERENCESPool, E. H., and Garlock, J. H. (1929). A treatment for bronchial
fistula-an experin ental and clinical study. Ann. Surg.. 90, 213.
502
copyright. on M
arch 22, 2020 by guest. Protected by
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.19.6.492 on 1 Novem
ber 1964. Dow
nloaded from