Embed Size (px)
Citation preview
by: Aleia S.Guzman DDM-6A
ENDO-PERIO RELATIONSHIP
Periodontal therapy deals with many aspects of the supporting
structures, including the prevention and repair of lesions of the gingival
sulcus. Endodontics deals primarily with disease of the pulp and periapical
tissues. The success of both periodontal and endodontic therapy depends on
the elimination of both disease processes, whether they exist separately or as a
combined lesion. The relationship between periodontal and endodontic
disease has been a subject of speculation for many years. This paper aims at
presenting a comprehensive review of several aspects of perio-endo lesions.
The tooth, the pulp tissue within it and its supporting structures should
be viewed as one biologic unit. The interrelationship of these structures influences
each other during health, function and disease. The interrelationship between
periodontal and endodontic diseases has aroused much speculation, confusion and
controversy. The relationship between the periodontium and the pulp was first
discovered by Simring and Goldberg in 1964. The periodontium and pulp have
embryonic, anatomic and functional interrelationship. Ectomesenchymal cells
proliferate to form the dental papilla and follicle, which are the precursors of the
periodontium and the pulp respectively. This embryonic development gives rise to
anatomical connections, which remain throughout life.
INTRODUCTION
IT IS USED TO DENOTE AN INFLAMMATORY PROCESS IN
THE PERIO DONTAL TISSUES RESULTING FROM NOXIOUS
AGENTS PRESENTS IN THE ROOT CANAL SYSTEM OF THE
TOOTH, USUALLY A ROOT CANAL INFECTION .
WHAT IS ENDODONTIC LESION?
IT IS USED TO DENOTE AN INFLAMMATORY PROCESS IN
THE PERIODONTAL TISSUE RESULTING FROM ACCUMULATION
OF DENTAL PLAQUE ON THE EXTERNAL TOOTH SURFACE .
WHAT IS PERIODONTAL LESION?
Pulpal and periodontal problems are responsible for more
than 50% of tooth mortality. Periodontal disease is a slowly
progressing disease that may have an atrophic effect on the dental
pulp. Periodontal treatments such as deep root planning, usage of
localized medicaments and periodontal injury or wounding may
accelerate pulpal inflammation and provoke the interrelated
disease process.
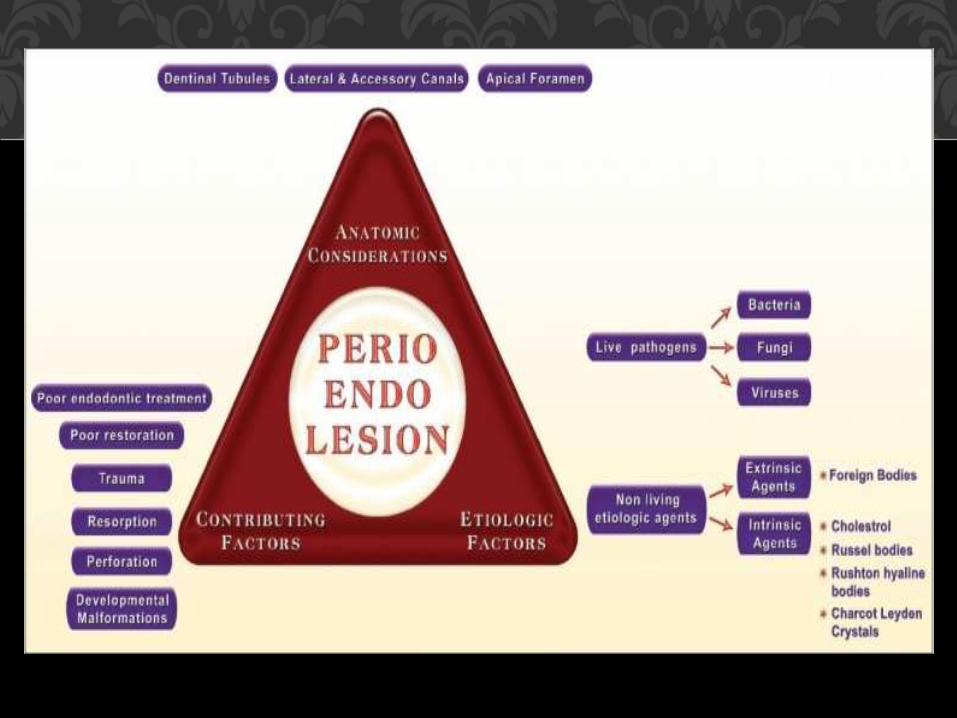
• Apical foramen
• Accessory cannals
• Congenital absence of cementum exposing dentinal tubules
• Permeability of cementum
• Developmental grooves
• Developmental anomalies such as projections and enamel pearl
PATHWAYS OF COMMUNICATION
• Empty spaces on root created by destroyed shrpey’s fibers
• Root fractures following trauma
• Idiopathic resorption- internal and external
• Loss of cementum due to external irritants
PATHWAYS OF PATHOLOGICAL ORIGIN
These comprise dentinal tubules which contain the odontoblastic
process that extends from the odontoblast at the pulpal dentin border to the
dentino-enamel junction or the cement-dentinal junction. Passage of
microorganisms between the pulp and periodontal tissues is possible through
these tubules, when the dentinal tubules are exposed in areas of denuded
cementum.
TUBULAR PATHWAYS
• Exposure of dentinal tubules following root planing
• Accidental lateral perforation during endodontic procedure
• Root fractures caused by endodontic procedures
PATHWAYS OF IATROGENIC ORIGIN
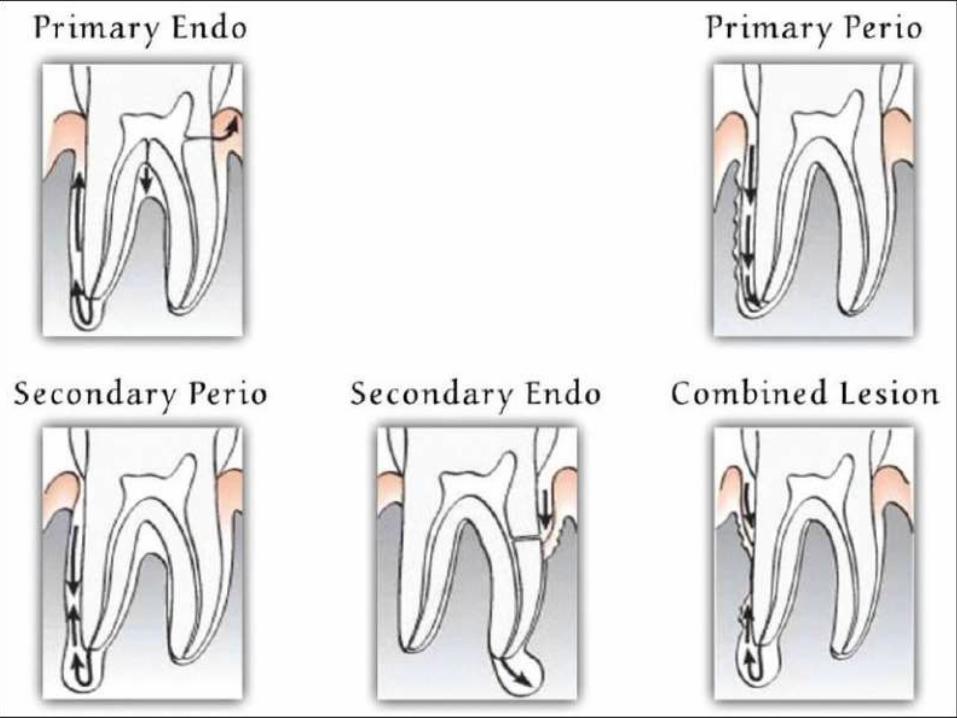
1. Primary endodontic lesion
2. Primary periodontal lesion
3. Primary endodontic lesion with secondary periodontal
involvement
4. Primary periodontal lesion with secondary endodontic
involvement
5. True combined lesion
CLASSIFICATION OF PERIO-ENDO LESIONS
An acute exacerbation of a chronic apical lesion on a tooth with a
necrotic pulp may drain coronally through the periodontal ligament into the
gingival sulcus. This condition may clinically mimic the presence of a
periodontal abscess. In reality, however, it would be a sinus tract originating
from the pulp that opens into the periodontal ligament. Primary endodontic
lesions usually heal following root canal therapy. The sinus tract extending
into the gingival sulcus or furcation area disappears at an early stage, if the
necrotic pulp has been removed and the root canals are well sealed.
PRIMARY ENDODONTIC LESION
These lesions are caused primarily by periodontal pathogens. In this
process, chronic periodontitis progresses apically along the root surface. In
most cases, pulpal tests indicate a clinically normal pulpal reaction. There is
frequently an accumulation of plaque and calculus and the presence of deep
pockets may be detected.
PRIMARY PERIODONTAL LESION
1. Primary endodontic lesion with secondary periodontal involvement
2. Primary periodontal disease with secondary endodontic involvement
3. True combined lesion
COMBINED DISEASES
Primary endodontic lesion with secondary periodontal involvement
may also occur as a result of root perforation during root canal treatment, or
where pins and posts may have been misplaced during restoration of the
crown. Symptoms may be acute, with periodontal abscess formation
associated with pain, swelling, pus or exudates, pocket formation, and tooth
mobility. A more chronic response may occur without pain, and involves the
sudden appearance of a pocket with bleeding on probing or exudation of pus.
PRIMARY ENDODONTIC LESION WITH SECONDARY PERIODONTAL
INVOLVEMENT
The apical progression of a periodontal pocket may continue until
the apical tissues are involved. In this case, the pulp may become necrotic as a
result of infection entering through lateral canals or the apical foramen. In
single-rooted teeth, the prognosis is usually poor. In molar teeth, the
prognosis may be better. Since not all the roots may suffer the same loss of
supporting tissue, root resection can be considered as a treatment alternative.
PRIMARY PERIODONTAL DISEASE WITH SECONDARY
ENDODONTIC INVOLVEMENT
True combined endodontic periodontal disease occurs less frequently
than other endodontic-periodontal problems. It is formed when an
endodontic lesion progressing coronally joins an infected periodontal pocket
progressing apically.The degree of attachment loss in this type of lesion is
invariably large and the prognosis guarded. This is particularly true in single-
rooted teeth. In molar teeth, root resection can be an alternative treatment.
The radiographic appearance of combined endodontic periodontal disease
may be similar to that of a vertically fractured tooth. If a sinus tract is present,
it may be necessary to raise a flap to determine the etiology of the lesion.
TRUE COMBINED LESION
Bacteria associated with pulpitis:
1. Fusobacterium
2. Prevotella
3. Streptococcus
4. lactobacillus
ETIOLOGY OF PULPAL DISEASE
Reversible pulpitis
• Symptomatic
• asymptomatic
Irreversible pulpitis acute – abnormally response to cold
abnormal response to heat
chronic – asymptomatic with pulp exposure
hyperplastic pulpitis
internal resorption
CLASSIFICATION OF PULPAL DISEASES
GINGIVAL DISEASES :
• Plaque induced gingival disease
• Non plaque induced gingival disease
CHRONIC PERIODONTITIS :
• Localized
• Generalized
AGGRESSIVE PERIODONTITIS:
• Localized
• Generalized
PERIODONTITIS AS A MANIFESTATION
CLASSIFICATION OF PERIODONTAL DISEASE
NECROTIZING PERIODONTAL DISEASE :
• Necrotizing ulcerative gingivitis
• Necrotizing ulcerative periodontitis
PERIODONTITIS ASSOCIATED WITH ENDODONTIC LESION :
• Endo-perio lesion
• Perio-endo lesion
• Combined lesion
ABSCESS OF PERIODNTIUM
• Gingival abscess
• Periodontal abscess
• Pericoronal abscess
• Bone resorption
• Radiolucency at the apex of the root
• Highly vascularized granulation tissue infiltrate to varrying
degrees by inflammatory cells
• Nutrophils are present near the apical foramen
• Plasma cells , macrophages, lymphocytes in fibroblast are
increased in the periphery of the lesion
EFFECTS OF PULPAL DISEASE ON PERIODONTIUM
• Visual examination
• Palpation
• Percussion
• Mobility
• Radiographs
• Pulp vitality testing
• Pocket probing
• Fistula tracking
• Cracked tooth testing
VARIOUS DIAGNOSTIC PROCEDURES THAT CAN BE
USED TO IDENTIFY PERIO ENDO LESIONS
Soft tissues:
• Inflmmation
• Ulcerations
• Sinus tracts
Teeth:
• Caries
• Deffective restorations
• Abrasions
• Crack
• Fractures
• Discolorations
VISUAL EXAMINATION
• Periradicular abnormalities
• Cannot differentiate between endodontic and periodontic
lesion
• Compare with control teeth
PALPATION
• Compare with control teeth
• Periraducular inflammation
PERCUSSION
• Loss of periodontal support
• Fractured roots
• Recent traumas
• Periradicular abscess
MOBILITY
• Periradicular resorption of endodontic origin- not
effective
• Bone loss due to periodontal disease- effective
RADIOGRAPHS

• Abnormal response- degenerative changes
• No response- pulp necrosis
• Modern transient response- normal vital pulp
• Quick painful response- reversible pulpitis
• Lingering painful response- irreversible pulpitis
PULP VITALITY TESTING
• Probing depth
• Clinical attachment level
• Sinus tracking
POCKET PROBING
• Semi-rigid radiopaque material (gutta percha)
FISTULA TRACKING
• Transillumination
• Wedging
• staining
CRACKED TOOTH TESTING
PRIMARY ENDODONTIC LESION –
conventional endodontic therapy
PRIMARY ENDODONTIC LESION WITH SECONDORY PERIODONTAL INVOLVEMENT –
endo-perio therapy
PRIMARY PERIODONTAL LESION -
Periodontal therapy
Guided tissue regeneration
Root amputation and hemisection
Pulp space therapy
TREATEMENT
PRIMARY PERIODONTAL LESION WITH SECONDARY ENDO LESION:
Space therapy
Periodontal therapy
Root amputation
GTR
TRUE COMBINED LESION
Endo therapy
Perio therapy
hemisection
bicuspidization
Root amputation
TREATMENT

THANK YOU !!!
• https://docs.google.com/presentation/d/1-
yp7WAURWOyETkyKhts8xAFMFpC0-
_4ra7Q8FqzCDYA/edit?pli=1#slide=id.p42
• http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2813095/
SOURCES: