Embed Size (px)
Citation preview

EPILEPSY
Martyn Bracewell
Consultant Neurologist
The Walton Centre, Liverpool
Betsi Cadwaladr University Health Board
Noble’s Hospital, IOM
Senior Lecturer
Bangor University
Epilepsy – An Overview
• Definitions, Aetiology and Prevalence
• Seizure classification
• Differential diagnosis
• Investigation
• Treatment
• Prognosis
Definitions
• SEIZURE
• An episode of neuronal hypersynchrony which causes neurological symptoms
• EPILEPSY
• Recurrent unprovoked seizures
The burden of epilepsy
• lifetime prevalence of seizures 1-5%
• prevalence of epilepsy up to 1%
• 1% acute admissions
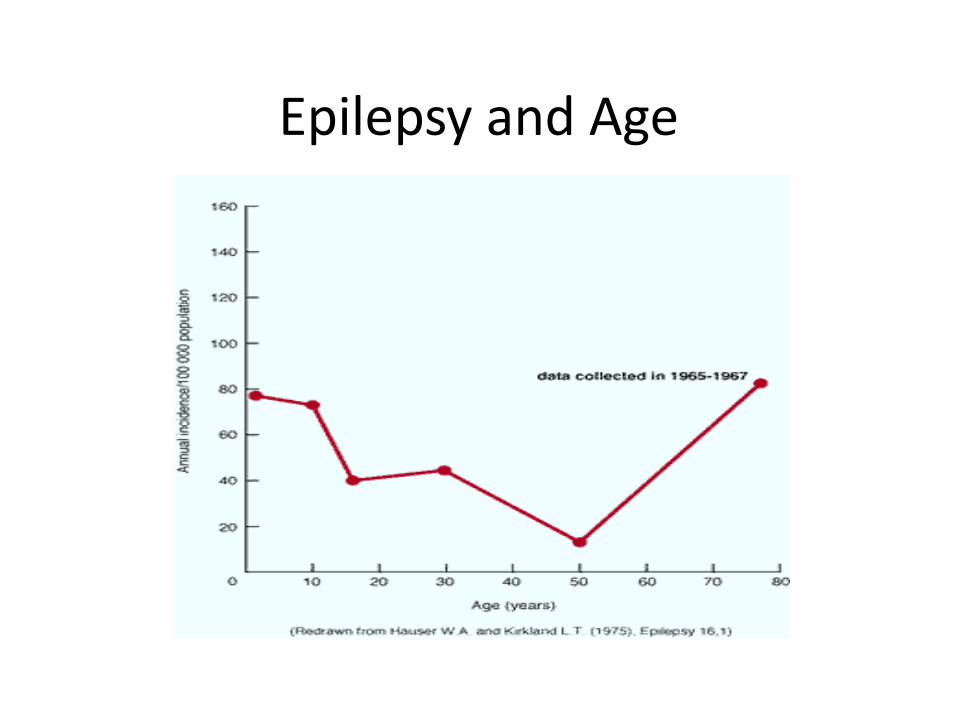
Epilepsy and Age

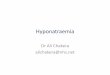
Cause of epilepsy
• Depends on age and geographical location
• Idiopathic (genetic) in >80% if under 9 years old
• Idiopathic extremely uncommon if presents over 25
• Vascular disease 49% if over 60
• Tumour 6% overall
• <30 years 1%
• 50-59 years19%
• >60years 11%
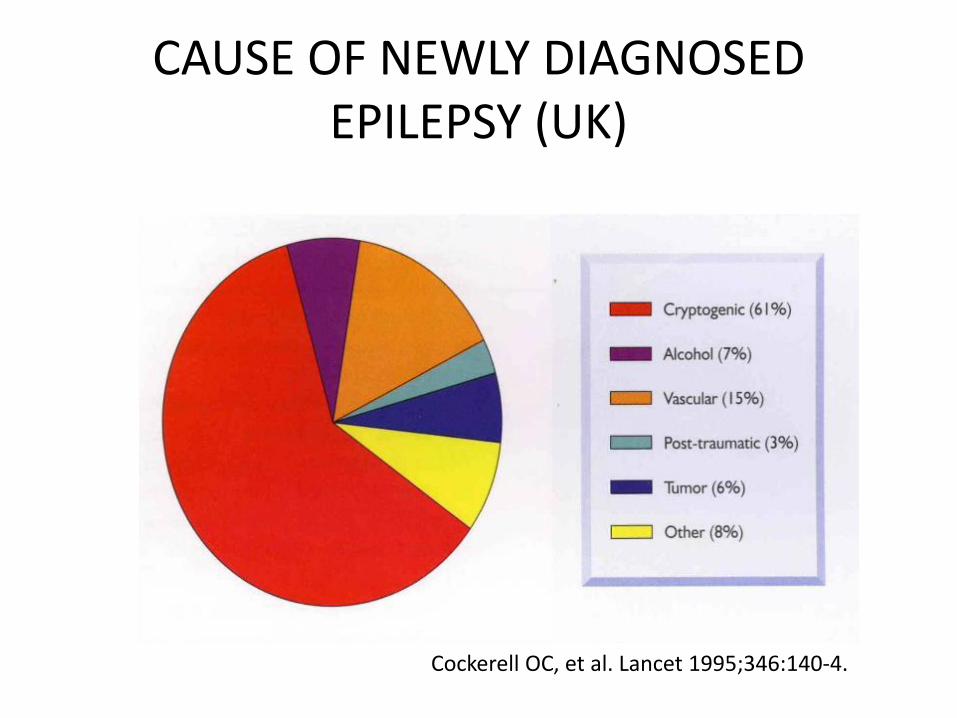
CAUSE OF NEWLY DIAGNOSED EPILEPSY (UK)
Cockerell OC, et al. Lancet 1995;346:140-4.
DIAGNOSIS
• Clinical History
• Eye witness account crucial
• Often need to defer diagnosis due to uncertainty
• INVESTIGATIONS RARELY HELP

Misdiagnosis of epilepsy
Misdiagnosis is common
26% in referrals to tertiary centre with ‘refractory’ epilepsy
Conditions most commonly mistaken are syncope and NEAD (non-epileptic attacks)
If unsure, it is better to express uncertainty than to start treatment
Smith, D et al (1999). Q J Med; 92: 15-23
QUESTIONS TO ASK
• Are there seizures?
• Acute symptomatic or epileptic?
• Type of seizures?
• Which epilepsy syndrome?
• What is the cause?
Common reasons for misdiagnosis
• Incomplete history
• Misinterpretation of syncopal or myoclonic jerks
• Lack of eye witness account
• Not taking notice of clues
• Over-reliance on tests (EEG)
Smith, D et al (1999). Q J Med; 92: 15-23

Differential diagnosis
• Seizures• Syncope• Non Epileptic Attack Disorder (NEAD)• Cardiac syncope
• Transient Ischaemic Attacks• Migraine• Paroxysmal movement disorders• Parasomnias• Cataplexy• etc
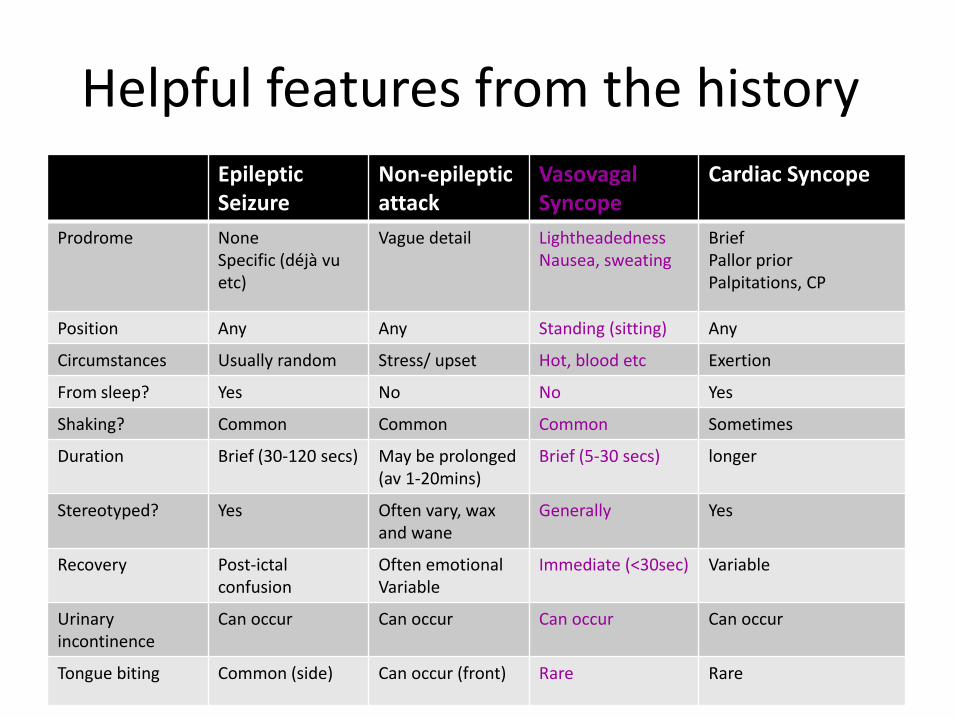
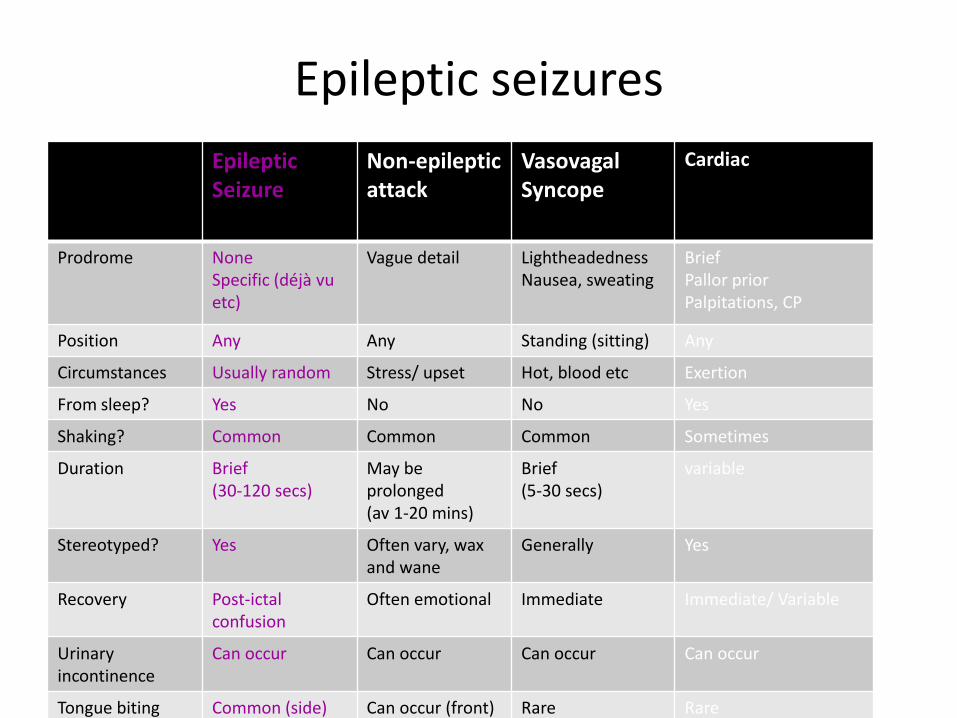
Helpful features from the history
Epileptic Seizure
Non-epilepticattack
Vasovagal Syncope
Cardiac Syncope
Prodrome NoneSpecific (déjà vu etc)
Vague detail LightheadednessNausea, sweating
BriefPallor priorPalpitations, CP
Position Any Any Standing (sitting) Any
Circumstances Usually random Stress/ upset Hot, blood etc Exertion
From sleep? Yes No No Yes
Shaking? Common Common Common Sometimes
Duration Brief (30-120 secs) May be prolonged(av 1-20mins)
Brief (5-30 secs) longer
Stereotyped? Yes Often vary, wax and wane
Generally Yes
Recovery Post-ictalconfusion
Often emotionalVariable
Immediate (<30sec) Variable
Urinary incontinence
Can occur Can occur Can occur Can occur
Tongue biting Common (side) Can occur (front) Rare Rare
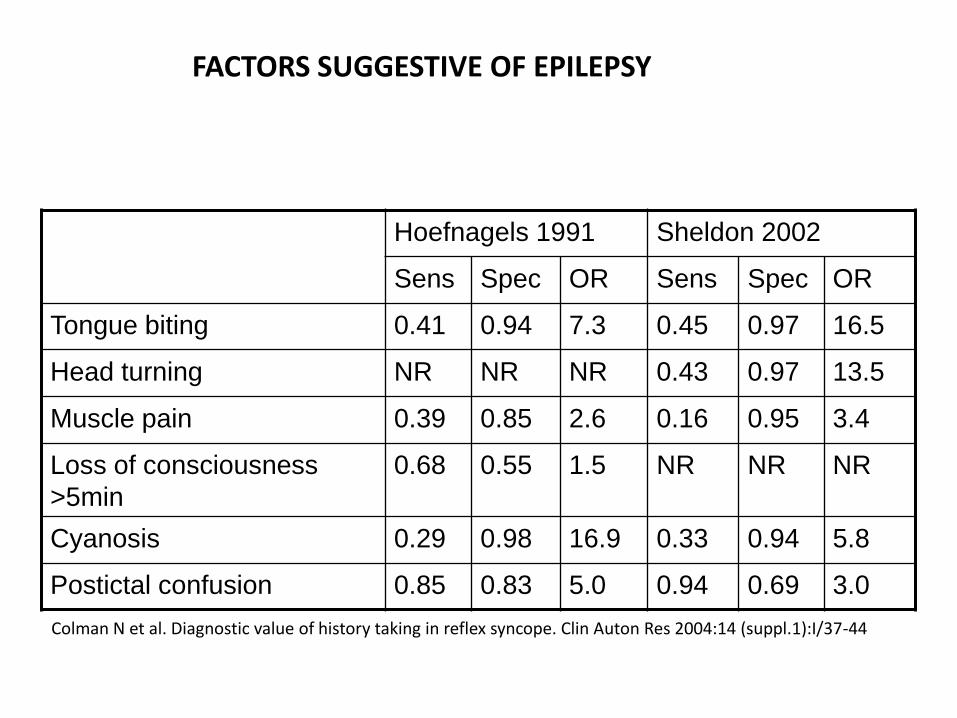
Hoefnagels 1991 Sheldon 2002
Sens Spec OR Sens Spec OR
Tongue biting 0.41 0.94 7.3 0.45 0.97 16.5
Head turning NR NR NR 0.43 0.97 13.5
Muscle pain 0.39 0.85 2.6 0.16 0.95 3.4
Loss of consciousness
>5min
0.68 0.55 1.5 NR NR NR
Cyanosis 0.29 0.98 16.9 0.33 0.94 5.8
Postictal confusion 0.85 0.83 5.0 0.94 0.69 3.0
Colman N et al. Diagnostic value of history taking in reflex syncope. Clin Auton Res 2004:14 (suppl.1):I/37-44
FACTORS SUGGESTIVE OF EPILEPSY
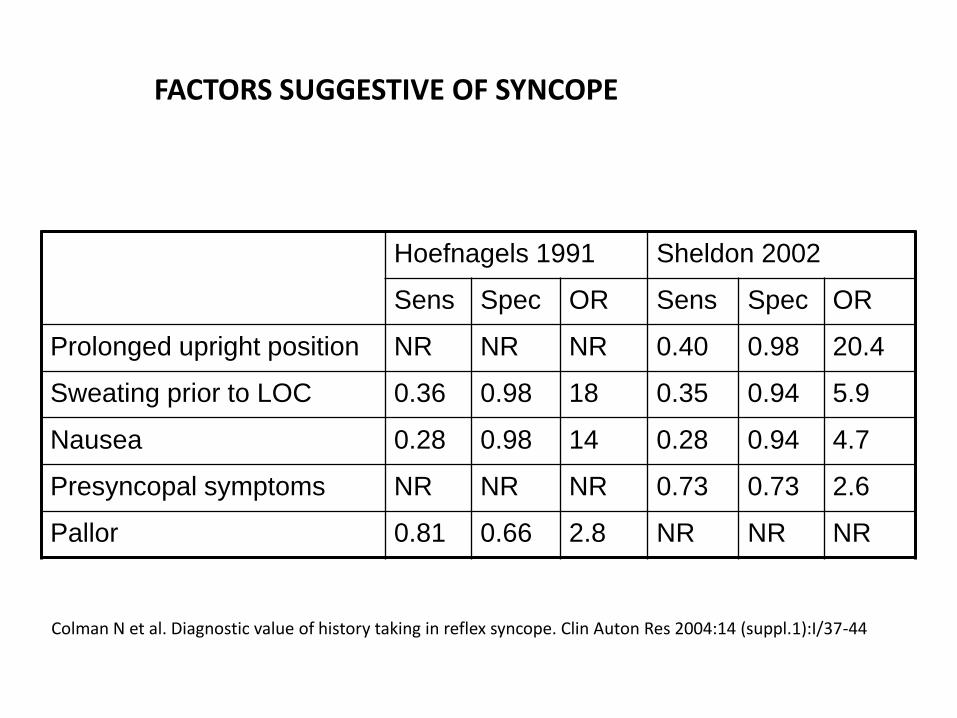
Hoefnagels 1991 Sheldon 2002
Sens Spec OR Sens Spec OR
Prolonged upright position NR NR NR 0.40 0.98 20.4
Sweating prior to LOC 0.36 0.98 18 0.35 0.94 5.9
Nausea 0.28 0.98 14 0.28 0.94 4.7
Presyncopal symptoms NR NR NR 0.73 0.73 2.6
Pallor 0.81 0.66 2.8 NR NR NR
Colman N et al. Diagnostic value of history taking in reflex syncope. Clin Auton Res 2004:14 (suppl.1):I/37-44
FACTORS SUGGESTIVE OF SYNCOPE
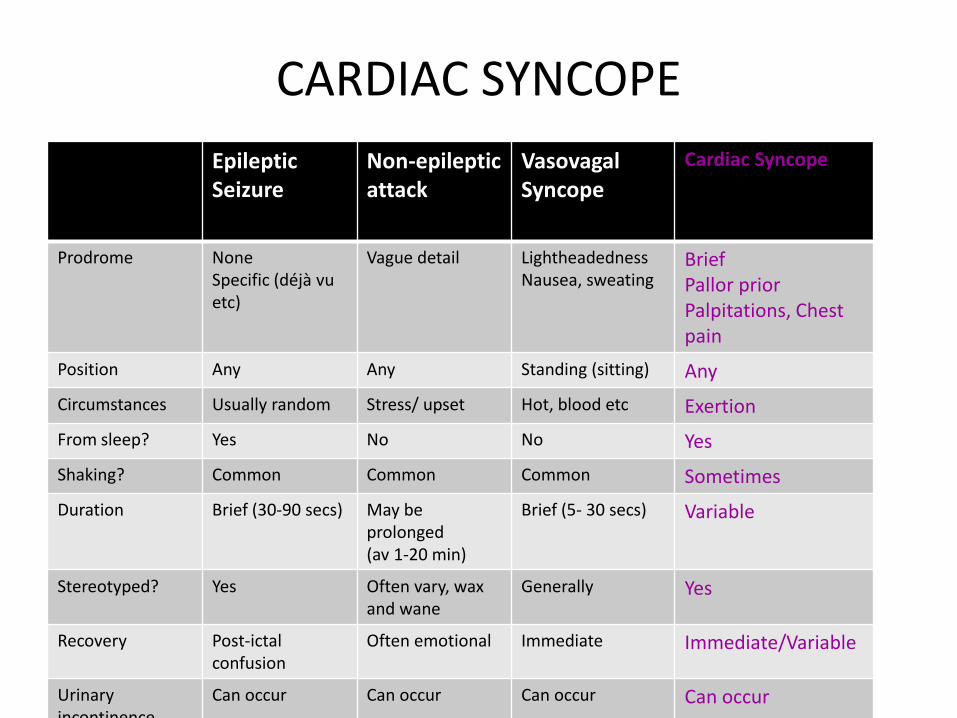
CARDIAC SYNCOPE
Epileptic Seizure
Non-epilepticattack
Vasovagal Syncope
Cardiac Syncope
Prodrome NoneSpecific (déjà vu etc)
Vague detail LightheadednessNausea, sweating
BriefPallor priorPalpitations, Chestpain
Position Any Any Standing (sitting) Any
Circumstances Usually random Stress/ upset Hot, blood etc Exertion
From sleep? Yes No No Yes
Shaking? Common Common Common Sometimes
Duration Brief (30-90 secs) May be prolonged(av 1-20 min)
Brief (5- 30 secs) Variable
Stereotyped? Yes Often vary, wax and wane
Generally Yes
Recovery Post-ictalconfusion
Often emotional Immediate Immediate/Variable
Urinary incontinence
Can occur Can occur Can occur Can occur
WHEN TO REFER TO CARDIOLOGY
• Exercise induced attacks
• ‘Syncope’ whilst supine
• Frequent syncope with no warning
• Mixture of syncope and seizures, or presyncopal warning
• Structural heart disease
• Abnormal ECG
• Family history of sudden death <40years
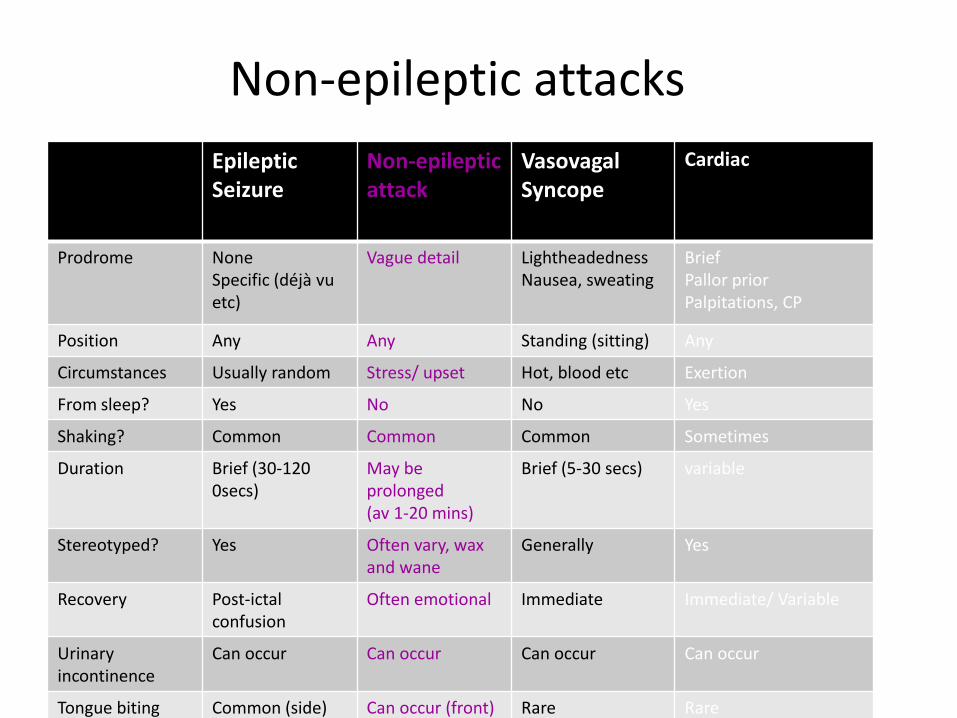
Non-epileptic attacks
Epileptic Seizure
Non-epilepticattack
Vasovagal Syncope
Cardiac Syncope
Prodrome NoneSpecific (déjà vu etc)
Vague detail LightheadednessNausea, sweating
BriefPallor priorPalpitations, CP
Position Any Any Standing (sitting) Any
Circumstances Usually random Stress/ upset Hot, blood etc Exertion
From sleep? Yes No No Yes
Shaking? Common Common Common Sometimes
Duration Brief (30-1200secs)
May be prolonged(av 1-20 mins)
Brief (5-30 secs) variable
Stereotyped? Yes Often vary, wax and wane
Generally Yes
Recovery Post-ictalconfusion
Often emotional Immediate Immediate/ Variable
Urinary incontinence
Can occur Can occur Can occur Can occur
Tongue biting Common (side) Can occur (front) Rare Rare
NEAD
• Attacks superficially resemble seizures
• They are not caused by abnormal brain activity
• Most are dissociative
• I prefer NEAD
• Avoid ‘psychogenic’ or ‘pseudo-seizures’
Incidence and Prevalence
• 2 to 33 per 100 000 (Benbadis SR Seizure 2000)
• 15 000 people in the UK (conservative estimate)
• 4 out of 10 pts referred for EEG telemetry for intractable seizures
Dissociative Non-Epileptic Seizures (NES)
• Dissociation usually manifests as– Depersonalisation
• Disconnection from your body or thoughts
• Feeling strange, weird, disconnected from myself, like I was there but not there
– Derealisation• Disconnection from your surroundings
• I felt spaced out, my surroundings seemed unreal/ far away, things appeared flat, diminished, artificial
• Feeling disconnected from your body can also result in functional weakness, imbalance or sensory problems

Clues to the diagnosis
• Situational
• Duration over a minute and sometimes hours
• Features wax and wane during attack
• Dramatic motor phenomena or prolonged atonia
• Head moves side to side
• Eyes closed
• Ictal crying or speaking
• Surprisingly rapid or slow recovery
• History of somatisation, trauma or psychiatric illness

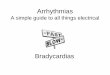
Triggers
M Reuber 2017
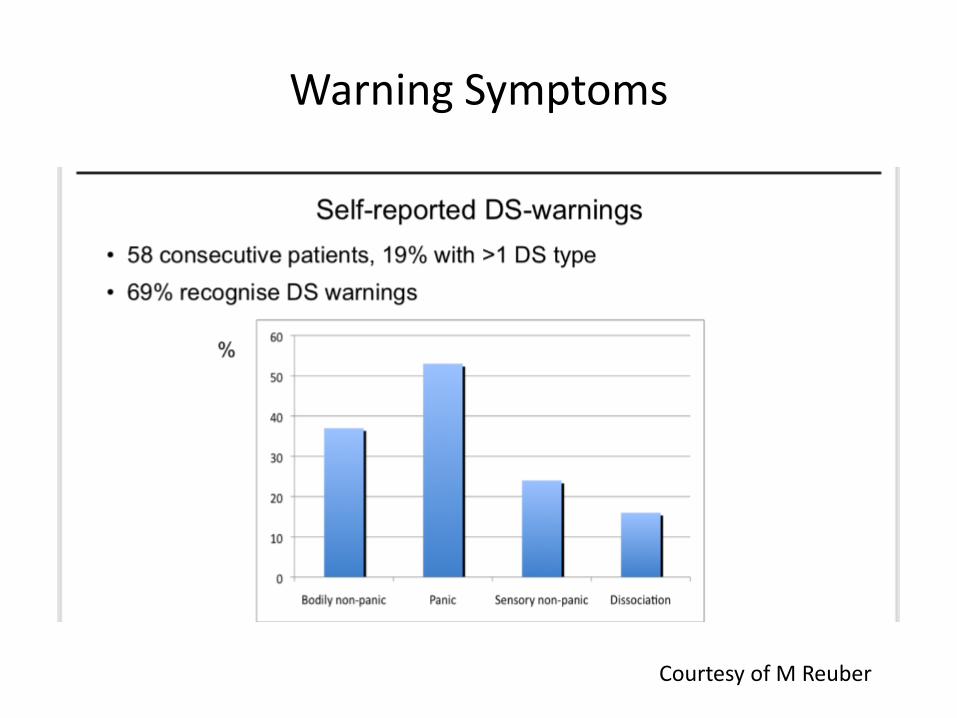
Warning Symptoms
Courtesy of M Reuber
Explaining the Diagnosis
• This is a positive diagnosis– Explain what IS wrong rather than what you have
excluded
• Explain about common aetiological factors
• Reinforce the fact that people experiencing dissociative seizures are not mad/ imagining it/ putting it on
• Give written information and website details– www.nonepilepticseizures.info
• Be empathic
Treatment
• Psychological Therapy
• CBT
• AEDs don’t help and may cause harm
• Treat anxiety and depression
• SSRIs can help even without depression/ anxiety
Epileptic seizures
Epileptic Seizure
Non-epilepticattack
Vasovagal Syncope
Cardiac Syncope
Prodrome NoneSpecific (déjà vu etc)
Vague detail LightheadednessNausea, sweating
BriefPallor priorPalpitations, CP
Position Any Any Standing (sitting) Any
Circumstances Usually random Stress/ upset Hot, blood etc Exertion
From sleep? Yes No No Yes
Shaking? Common Common Common Sometimes
Duration Brief (30-120 secs)
May be prolonged(av 1-20 mins)
Brief(5-30 secs)
variable
Stereotyped? Yes Often vary, wax and wane
Generally Yes
Recovery Post-ictalconfusion
Often emotional Immediate Immediate/ Variable
Urinary incontinence
Can occur Can occur Can occur Can occur
Tongue biting Common (side) Can occur (front) Rare Rare

Classification of epilepsy syndromes
• SYMPTOMATIC• Known underlying cause
• CRYPTOGENIC• Presumed underlying cause that cannot be
identified
• IDIOPATHIC• No known aetiology• Presumed to be genetic
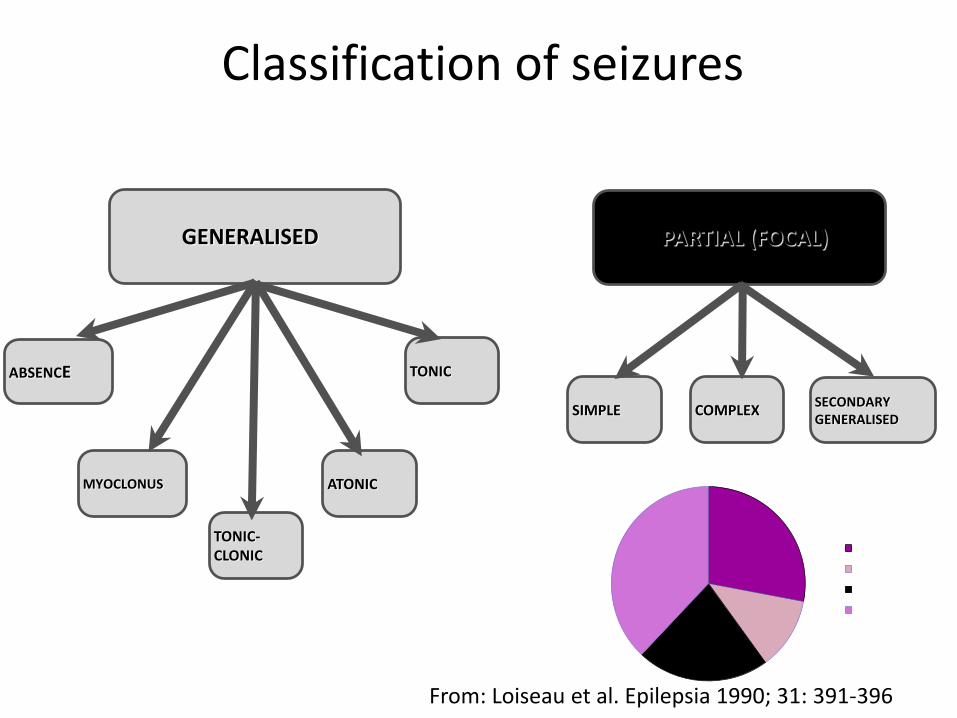
Classification of seizures
GENERALISED PARTIAL (FOCAL)
TONIC
ATONIC
SIMPLE COMPLEXSECONDARY GENERALISED
TONIC-CLONIC
MYOCLONUS
ABSENCE
Focal
Generalised
Unclassifiable
Provoked / Acute
From: Loiseau et al. Epilepsia 1990; 31: 391-396
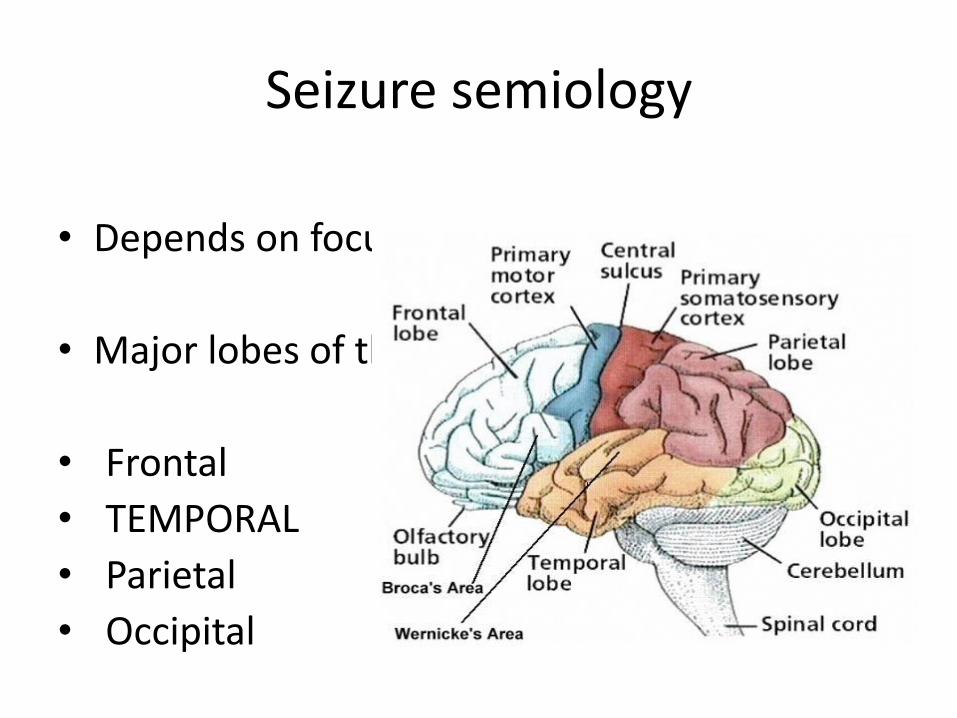
Seizure semiology
• Depends on focus
• Major lobes of the brain
• Frontal
• TEMPORAL
• Parietal
• Occipital

TEMPORAL LOBE EPILEPSY (TLE)
• Temporal lobe important for memory, language, emotion
• Deja vu, jamais vu, smell or taste, fear, dysphasia, visual hallucinations less common
• Up to 70% arise from sleep

Frontal lobe epilepsy (FLE)• Largest lobe of the brain, controls emotion, behaviour, movements• Seizures can be bizarre and involve vocalisation or ambulation• Often (90%) nocturnal• May be abrupt in onset and offset with little post-ictal confusion• EEG normal in 54% inter-ictal, 44% ictal1
• Commonly misdiagnosed – NEAD, parasomnias
• Focal motor (primary motor cortex)• Asymmetric tonic posturing (supplementary motor cortex)• Bizarre (thrashing, rapid movements, cycling) ‘hypermotor’
(anterior)
1Provini F, et al. Brain 1999;122:1017-31.
GENERALISED SEIZURES
• Arise from an epileptiform discharge from the whole of the cortical surface
• 3 main types
• Absence
• Myoclonus
• Tonic-clonic seizure

Investigations in new onset epilepsy
All new onset epilepsy >25 years is of focal onset
All presenting with a first seizure / new epilepsy >25 years need brain imaging
All patients with seizures with focal features require brain imaging
Do an ECG
Brain imaging
After a single seizure / new diagnosis of epilepsy the role of imaging is to identify a serious underlying structural cause
MRI if possible (if urgent CT is normal, can do MRI as an outpatient)
MRI will identify more subtle pathology
EEG
EEG of no use if new onset seizures >25 year old
EEG has no diagnostic role in “blackout ?cause”
So usually DO NOT order one

GENERALISED SEIZURE
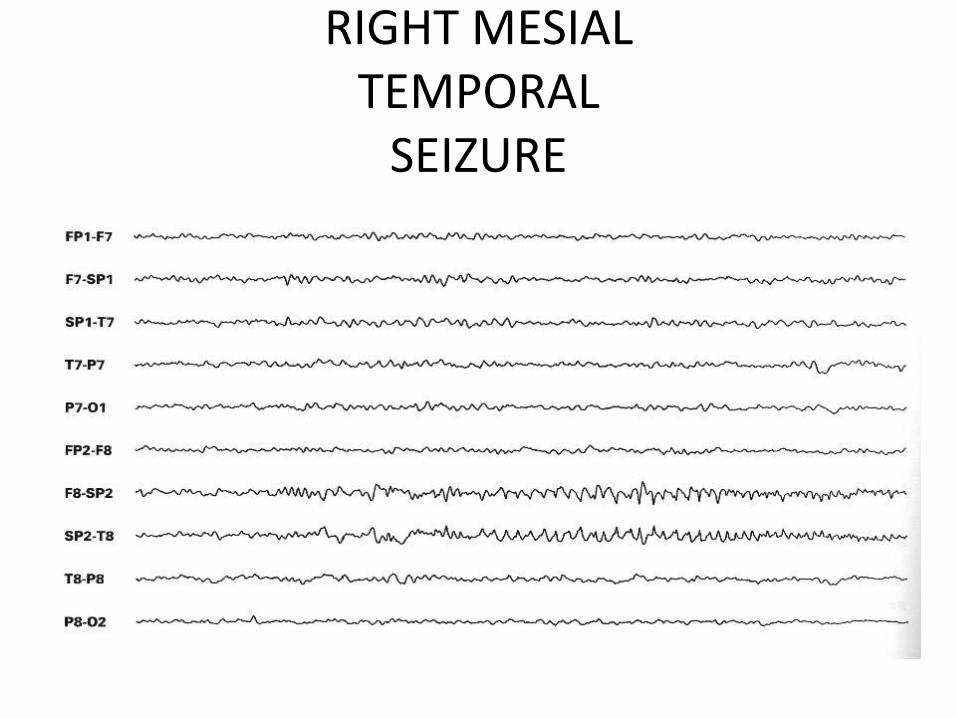
RIGHT MESIAL TEMPORAL
SEIZURE
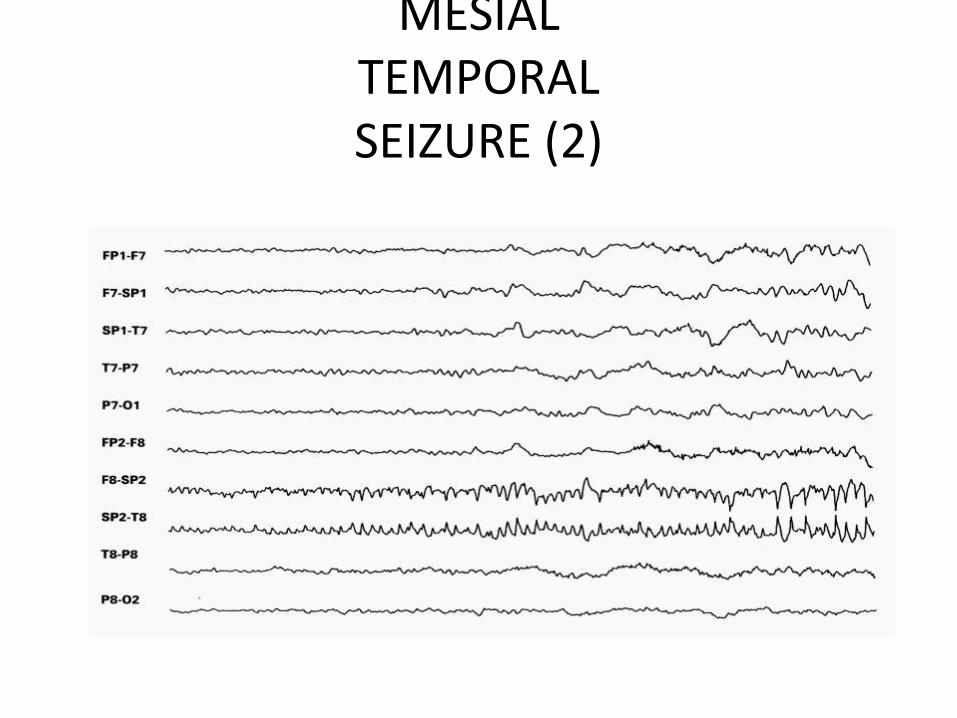
MESIAL TEMPORAL SEIZURE (2)
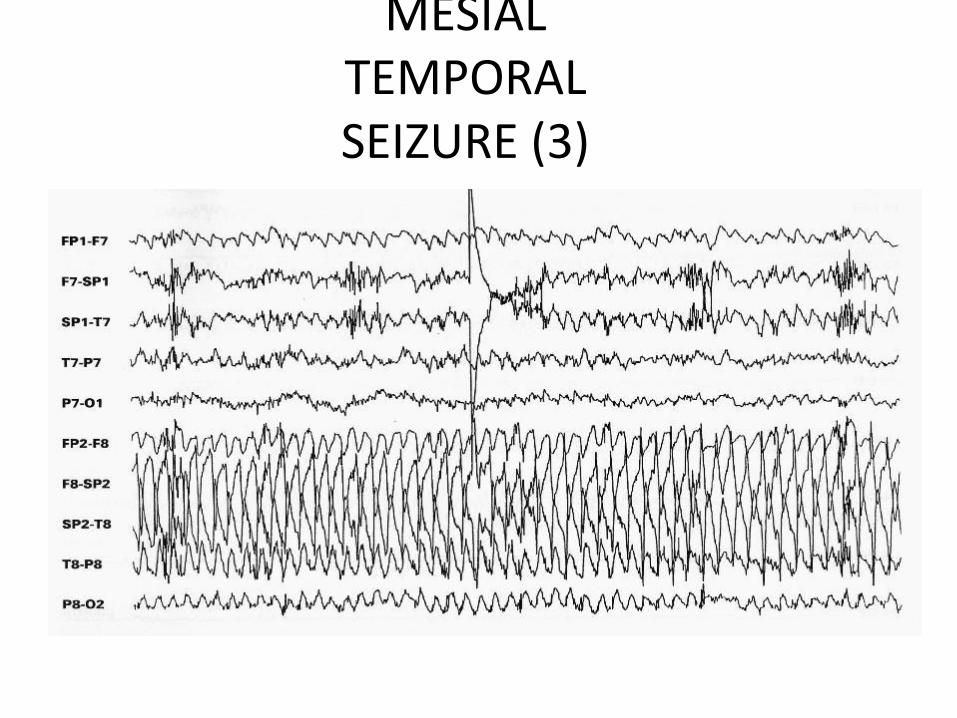
MESIAL TEMPORAL SEIZURE (3)
Anti-epileptic drug levels
• Only indicated
• in pregnancy
• suspected toxicity
• questionable adherence

Should I start an AED?
• If one seizure NO
• If several seizures in 24h NO
• Except possibly if high risk of recurrence
• If recurrent seizures YES
Choice of first-line AED
• Seizure control is not the only goal
• Side effect profile important
• Consider co-morbidities eg anxiety, depression,
obesity, migraine
• Numerous drugs
• Numerous comparison studies

AVAILABLE ANTIEPILEPTIC
DRUGS• AEDs pre 1988
• Barbiturates (1912)
• Phenytoin (1938)
• Benzodiazepines (1960)
• Valproate (1962)
• Carbamazepine (1965)
Vigabatrin
Lamotrigine
Gabapentin
Topiramate
Tiagabine
Oxcarbazepine
Levetiracetam
Pregabalin
Zonisamide
Rufinamide
Lacosamide
Eslicarbazapine
Retigabine
Perampanel
PRINCIPLES OF TREATMENT
Monotherapy
Cautious dosage escalation
Titrate to maximally tolerated dose or until seizures stop
Alternative monotherapy
Dual therapy

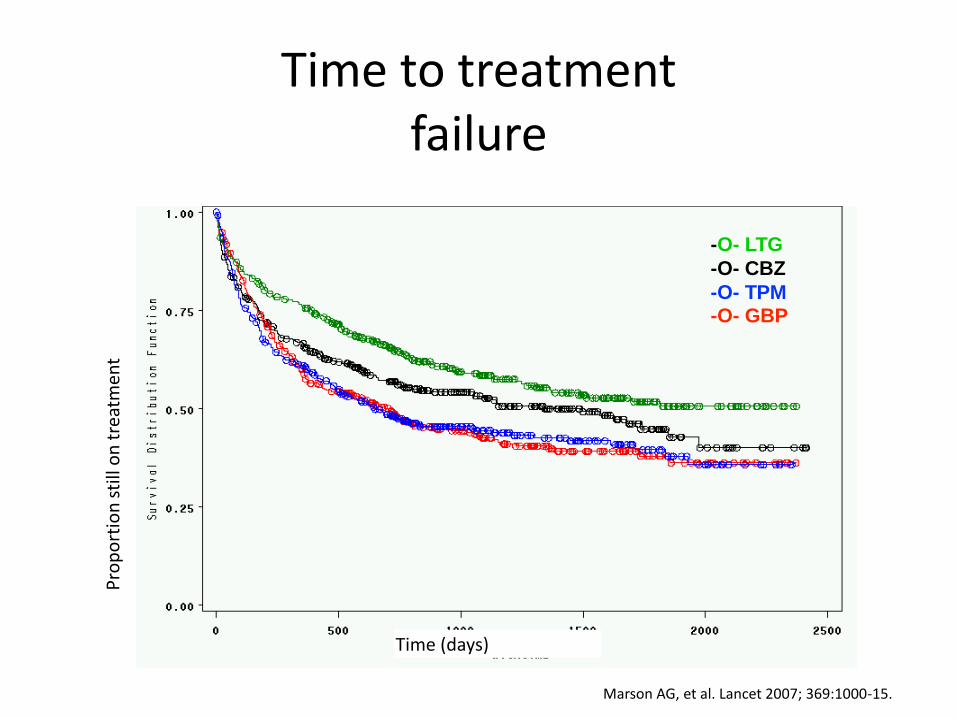
WHICH DRUG TO CHOOSE: SANAD
• SANAD (2007) Compared efficacy and tolerability of new vsstandard AED
• Multi-centre hospital-based, unblinded RCT
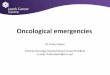
• Arm A Focal epilepsy (n=1721)• Carbamazepine (standard) vs Lamotrigine, Topiramate,
Gabapentin, Oxcarbazepine
• Arm B Generalised (n=716)• Sodium Valproate (standard) vs Lamotrigine and
Topiramate
Marson AG, et al. Lancet 2007; 369:1016-26..

Carbamazepine is standard first line AED
Carbamazepine
Gabapentin
Lamotrigine
Topiramate
Oxcarbazepine
N=1721
SANAD arm A
-O- LTG
-O- CBZ
-O- TPM-O- GBP
Time (days)
Pro
po
rtio
n s
till
on
tre
atm
ent
Marson AG, et al. Lancet 2007; 369:1000-15.
Time to treatment failure

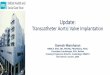
Valproate is standard first line AED
Valproate
Lamotrigine
Topiramate
N=716
SANAD arm B

-O- VPA
-O- LTG-O- TPM
Marson AG, et al. Lancet 2007; 369:1016-26..
Pro
po
rtio
n s
till
on
tre
atm
ent
SANAD ARM B TIME TO TREATMENT FAILURE
SANAD: conclusions and limitations
• WINNERS: LAMOTRIGINE (focal epilepsy)• VALPROATE (generalised epilepsy)
• Pragmatic trial • Reflects clinical practice• Limitations• Not blinded• Open to physician bias and error• Dosing and formulations not standardised• Newer drugs not included (Levetiracetam, Lacosamide etc)
• SANAD II underway• Arm A: Lamotrigine, Levetiracetam, Zonisamide• Arm B: Valproate, Levetiracetam• Watch this space……..

New onset focal epilepsy
• Consider other factors
• Lamotrigine
• Levetiracetam
• Carbamezepine
New onset generalised epilepsy
• Valproate (men)
• Lamotrigine (women, no myoclonus)
• Levetiracetam (women, myoclonus)

COUNSELLING WOMEN WITH EPILEPSY
Interaction (or not) of AED with OCP
Teratogenic risk of current treatment and potential other options
Role of folic acid
Risk of seizures in pregnancy
Genetic risk of transmission of epilepsy

TERATOGENICITY OF AEDS
Valproate most teratogenic (3-4x risk of MCM plus cognitive problems, autism etc)
Polytherapy worse than monotherapy (especially if with valproate)
Lamotrigine risk higher if dose > 400mg daily
Good data only for CBZ, VPA and LTG
Very little known about the other newer AEDs

TREATING ELDERLY PATIENTS WITH EPILEPSY
The elderly are more likely to have co-morbidity, to be on multiple medication and tolerate drugs poorly
AEDs with a lack of drug-drug interactions are Older AEDs are more likely to have interactions then newer AEDs
First-line AED Lamotrigine
Levetiracetam a good option in this group

When MONOTHERAPY FAILS
• Question diagnosis• Is the classification correct• Adequate dose tried?• Compliance• Co-morbidity• Lifestyle
• Then..• Try alternate monotherapy• Add on a second agent (different mechanism of action)
CHANCE OF SEIZURE REMISSION WITH AED
• Remission frequently occurs with a low dose of the first drug1
• 47% seizure freedom on first AED
• 13% second AED
• 4% third AED or combinations
• If failed >2 AEDs, chance of remission 4-5% per year
• 1 Kwan P and Brodie MJ. NEJM 2000;342:314-9.
• 2 Choi H, et al. Epilepsia 2008;49:1440-5.
Prognosis (1)
• Prolonged Remission 60-70%
• Negative predictors• Onset first year of life• ‘Symptomatic’ aetiology (previous brain insults or abnormal EEG1)• Neurological deficit/ learning disability• High frequency of pre-treatment seizures• Failure to respond to the first AED
• Largest study Pre-MESS in 397 patients followed for 2 years2. Early recurrence rate reduced by immediate treatment.
1 Berg and Shinnar. Neurology 1991;41:965-72.2 Beghi et al (FIRST). Ital J Neurol Sci 1993;14:295-301.
Prognosis (2)
• Status Epilepticus• Mortality for convulsive status 211-272%. Higher if late diagnosis.
• Sudden Unexpected Death in Epilepsy (SUDEP) 500 deaths per year in UK• Increased risk if• Uncontrolled GTCS• Poor compliance• Seizures not controlled by medication• young adult (particularly male)• Seizures when asleep or alone• excess alcohol consumption
• Patients with epilepsy have a 2-3x increase in premature death overall• 1 De Lorenzo et al J Clin Neurophysiology 1995
• 2 Treiman et al NEJM 1998
TAKE HOME messages
• Do not be afraid to express uncertainty• Do an ECG• (usually) do an MRI• (usually) do not do an EEG
• Lamotrigine or levetiracetam good choices for focal onset or uncertain classification
• Valproate only for idiopathic generalised epilepsy in men• Avoid in young women (Levetiracetam is a good alternative)
• Seek neurological advice
• Dr Christine Burness, Liverpool• Dr Richard Grunewald, Sheffield• Dr Rosalind Kandler, Sheffield• Dr Andrew Nicolson, Liverpool• Professor Markus Reuber, Sheffield
Acknowledgments

Case 1
19yr old with focal epilepsy treated with Carbamazepine
Experience – nocturnal tonic clonic seizures, daytime auditory hallucination
Seen in clinic and advised in relationship
What factors must you consider
What advise will you offer regarding contraception
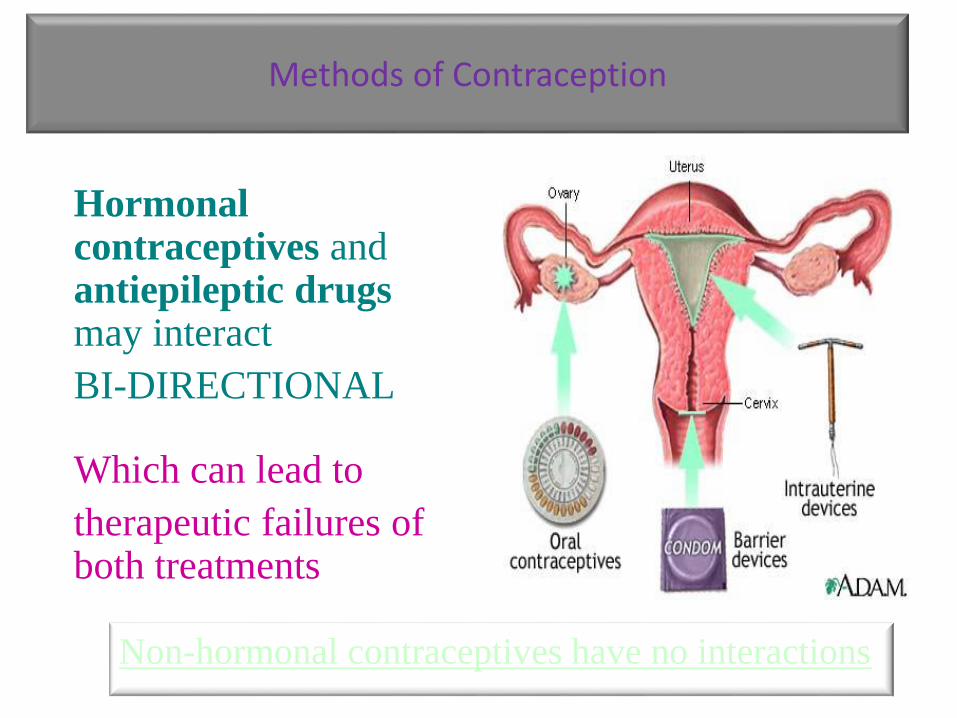
Hormonal contraceptives and antiepileptic drugs may interact
BI-DIRECTIONAL
Which can lead to
therapeutic failures of both treatments
Methods of Contraception
Non-hormonal contraceptives have no interactions
AEDs may reduce the effect of HCs
CLINICAL CONSEQUENCES
•Un-intended pregnancy
HCs may reduce the effect of AEDs
CLINICAL CONSEQUENCES
•Seizure deterioration
Interactions between antiepileptic drugs (AEDs) and hormonal contraceptions (HCs)

Non-inducers– Acetazolamide
– Clobazam
– Clonazepam
– Ethosuximide
– Gabapentin
– Lacosamide
– Lamotrigine*
– Levetiracetam
– Perampanel <12mg daily
– Retigabine
– Tiagabin
– Valproate
– Vigabatrin
– Zonisamide
Inducers– Carbamazepine
– Eslicarbazepine acetate
– Oxcarbazepine
– Perampanel ≥12mg daily
– Phenobarbital
– Phenytoin
– Primidone
– Rufinamide
– Topiramate ≥200mg daily
Interactions: AEDs and OCsCytochrome P450 (CYP 3A4)
SIGN 143 Diagnosis and management of epilepsy in adults May 2015
*Combined oral contraception affect metabolism of Lamotrigine

Clinical guidance – enzyme inducing AEDs contraceptionSIGN 143 Diagnosis and management of epilepsy in adults May 2015
Mirena coil can be used without restriction Depot progesterone injection without restriction (can
reduce bone mineral density) Enzyme inducing AEDs increase progesterone metabolism –
avoid POP & Progesterone implant To minimise risk women using COCP should avoid enzyme
inducing AEDs If no alternative to COCP – minimum 50mcg oestrogen
<50mcg warn and advise barrier methods Warn risk of pill failure action to take if breakthrough
bleeding – increase maximum 70mcg and tricycle pill Withdrawal of enzyme inducing AED – effect persists up to
four weeks – advise barrier methods
Clinical guidance – enzyme inducing AEDs & emergency contraception
SIGN 143 Diagnosis and management of epilepsy in adults May 2015
Require single dose 3mg levonorgestrel pill (double dose) asap and within 72hours of unprotected intercourse
Avoid ellaOne (ulipristol acetate) due to reduced efficacy
Advise option of non-hormonal intrauterine device within 5 days of intercourse
Clinical guidance
SIGN 143 Diagnosis and management of epilepsy in adults May 2015
Women receiving Lamotrigine can use progesterone only pill without restriction
Require warning of symptoms of Lamotrigine toxicity
If lamotrigine started in woman taking COCP adjust dose in response to seizure response, potential for higher dose requirement
If starting COCP when taking Lamotrigine - counsel about reduced circulating Lamotrigine and potential need to increase dose
Withdrawing - COCP warn of risk of lamotrigine toxicity
Women taking non-enzyme inducing AEDs and/or Lamotrigine, can use emergency contraception as for general population