Embed Size (px)
Citation preview
Journal of Clinical Virology 30S1 (2004) S16–S18
Experience with the IVDD performance evaluationsof the ADVIA Centaur infectious disease assays
Josef van Heldena,∗, Gérard A. Denoyelb
a Gemeinschaftspraxis fuer Laboratoriumsmedizin, Mikrobiologie und Humangenetik, Labor Dr. Stein und Kollegen,Wallstr. 10, D-41061 Moenchengladbach, Germany
b Laboratoire Marcel Merieux, 19 Avenue Tony Garnier, BP 7322, F-69357 Lyon, France
1. Introduction
The adoption of the new European Directive on In VitroDiagnostics (IVD Directive, 1998) by all western and themajority of the eastern European countries requires di-agnostic manufacturers to conduct extensive performanceevaluations to generate data for supporting and validatingtheir performance claims. In particular, high-risk IVDs forinfectious diseases must consider the specific requirementslisted in the European Union (EU) Common TechnicalSpecifications (CTS) (Commission Decision on CTS, 2002).The performance data along with other data obtained dur-ing the assay development are submitted to the appropriateregulatory agencies (Notified Bodies) in Europe in supportof obtaining the CE mark for European market distribution.
Bayer HealthCare, Diagnostics Division has devel-oped new immunoassays on the ADVIA Centaur® system(Hendriks et al., 2000) for the detection of hepatitis Bvirus (HBV), hepatitis C virus (HCV) and human immun-odeficiency virus type 1, including subtype O, and type 2(HIV 1/O/2) in human serum and plasma. These assays arefully automated and employ magnetic particle separationtechnology with chemiluminescence detection for optimalassay performance. The ADVIA Centaur assays for HBV,HCV and HIV 1/O/2 reagent kits, controls, and supplemen-tal materials used in this evaluation are all manufacturedunder GMP conditions with appropriate documentation andtraceability.
In this report, we present the results of the clinical eval-uations of the ADVIA Centaur assays for HBsAg, HBsAgconfirmatory test, anti-HCV and anti-HIV 1/O/2 assays as
Abbreviations: CTS, Common Technical Specifications; EU, Euro-pean Union; IVD, In Vitro Diagnostics; IVDD, In Vitro Diagnostics Di-rective; NB, Notified Body
∗ Corresponding author. Tel.:+49-2161-81940; fax:+49-2161-819450.E-mail address: [email protected] (J. van Helden).
performed at two sites in Europe. These evaluations demon-strate the clinical effectiveness of the ADVIA Centaur as-says in the laboratory diagnosis of HBV, HCV, HIV-1 andHIV-2 infections.
2. Results of performance evaluation studies of theADVIA Centaur assays for infectious disease testing
The performance evaluations were conducted at two Eu-ropean sites—Laboratoire Marcel Merieux in Lyon, France(site 1; principal investigator—Gérard A. Denoyel) and La-bor Dr. Stein und Kollegen in Moenchengladbach, Germany(site 2; principal investigator—Josef van Helden). Supple-mentary testing was performed at Bayer HealthCare, Diag-nostics Division in Tarrytown, NY, USA. The European sitesconducted testing in accordance with formal written proto-cols and defined testing algorithms.
The experimental design of the performance evaluationstudies followed the requirements defined in the CommonTechnical Specifications of the In Vitro Diagnostics Direc-tive 98/79/EC (IVDD) (IVD Directive, 1998). The respec-tive Abbott AxSYM assays served as the established devicesfor comparison.
2.1. ADVIA Centaur® HBsAg assay and ADVIA Centaur®
HBsAg confirmatory assay
The ADVIA Centaur® HBsAg assay and ADVIACentaur® HBsAg confirmatory assay are intended for thedetection of hepatitis B virus (HBV) surface antigen andconfirmation of its presence in repeatedly reactive samples.These assays, when used in conjunction with clinical in-formation and other HBV assays, help define the clinicalstatus of patients with acute or chronic HBV infection.
The ADVIA Centaur® HBsAg assay was evaluated us-ing samples obtained from patients with acute, chronic, and
1386-6532/$ – see front matter © 2004 Elsevier B.V. All rights reserved.doi:10.1016/j.jcv.2004.03.004
J. van Helden, G.A. Denoyel / Journal of Clinical Virology 30S1 (2004) S16–S18 S17
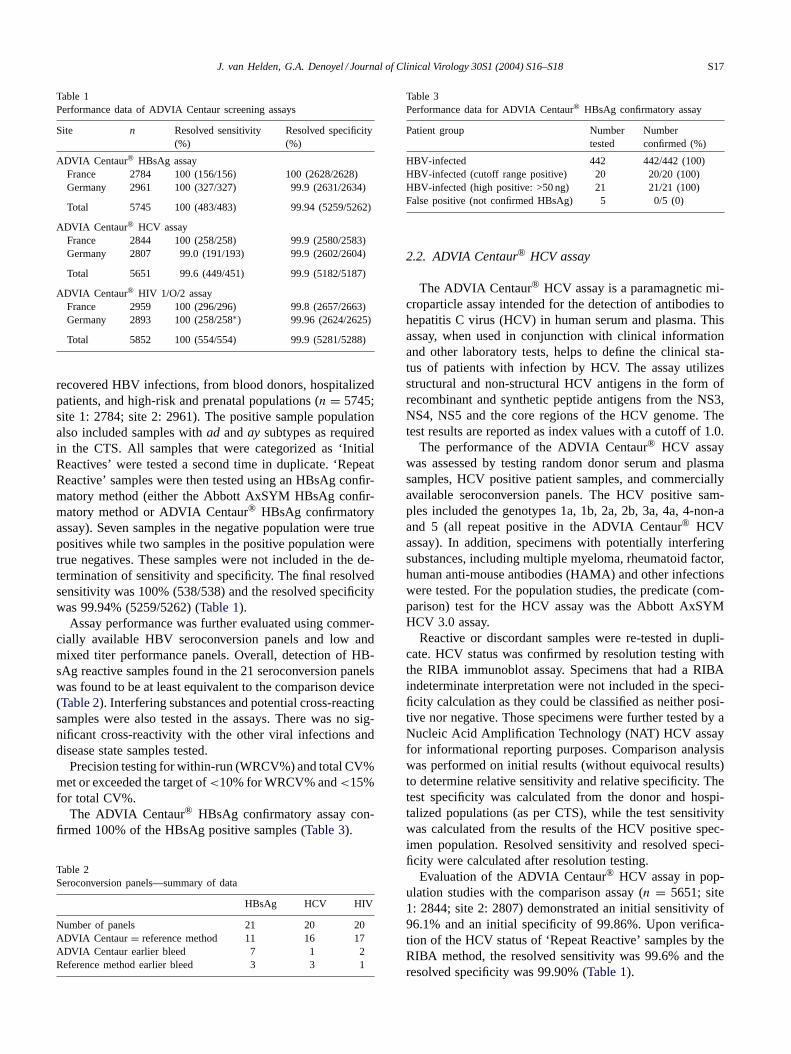
Table 1Performance data of ADVIA Centaur screening assays
Site n Resolved sensitivity(%)
Resolved specificity(%)
ADVIA Centaur® HBsAg assayFrance 2784 100 (156/156) 100 (2628/2628)Germany 2961 100 (327/327) 99.9 (2631/2634)
Total 5745 100 (483/483) 99.94 (5259/5262)
ADVIA Centaur® HCV assayFrance 2844 100 (258/258) 99.9 (2580/2583)Germany 2807 99.0 (191/193) 99.9 (2602/2604)
Total 5651 99.6 (449/451) 99.9 (5182/5187)
ADVIA Centaur® HIV 1/O/2 assayFrance 2959 100 (296/296) 99.8 (2657/2663)Germany 2893 100 (258/258∗) 99.96 (2624/2625)
Total 5852 100 (554/554) 99.9 (5281/5288)
recovered HBV infections, from blood donors, hospitalizedpatients, and high-risk and prenatal populations (n = 5745;site 1: 2784; site 2: 2961). The positive sample populationalso included samples withad anday subtypes as requiredin the CTS. All samples that were categorized as ‘InitialReactives’ were tested a second time in duplicate. ‘RepeatReactive’ samples were then tested using an HBsAg confir-matory method (either the Abbott AxSYM HBsAg confir-matory method or ADVIA Centaur® HBsAg confirmatoryassay). Seven samples in the negative population were truepositives while two samples in the positive population weretrue negatives. These samples were not included in the de-termination of sensitivity and specificity. The final resolvedsensitivity was 100% (538/538) and the resolved specificitywas 99.94% (5259/5262) (Table 1).
Assay performance was further evaluated using commer-cially available HBV seroconversion panels and low andmixed titer performance panels. Overall, detection of HB-sAg reactive samples found in the 21 seroconversion panelswas found to be at least equivalent to the comparison device(Table 2). Interfering substances and potential cross-reactingsamples were also tested in the assays. There was no sig-nificant cross-reactivity with the other viral infections anddisease state samples tested.
Precision testing for within-run (WRCV%) and total CV%met or exceeded the target of<10% for WRCV% and<15%for total CV%.
The ADVIA Centaur® HBsAg confirmatory assay con-firmed 100% of the HBsAg positive samples (Table 3).
Table 2Seroconversion panels—summary of data
HBsAg HCV HIV
Number of panels 21 20 20ADVIA Centaur= reference method 11 16 17ADVIA Centaur earlier bleed 7 1 2Reference method earlier bleed 3 3 1
Table 3Performance data for ADVIA Centaur® HBsAg confirmatory assay
Patient group Numbertested
Numberconfirmed (%)
HBV-infected 442 442/442 (100)HBV-infected (cutoff range positive) 20 20/20 (100)HBV-infected (high positive: >50 ng) 21 21/21 (100)False positive (not confirmed HBsAg) 5 0/5 (0)
2.2. ADVIA Centaur® HCV assay
The ADVIA Centaur® HCV assay is a paramagnetic mi-croparticle assay intended for the detection of antibodies tohepatitis C virus (HCV) in human serum and plasma. Thisassay, when used in conjunction with clinical informationand other laboratory tests, helps to define the clinical sta-tus of patients with infection by HCV. The assay utilizesstructural and non-structural HCV antigens in the form ofrecombinant and synthetic peptide antigens from the NS3,NS4, NS5 and the core regions of the HCV genome. Thetest results are reported as index values with a cutoff of 1.0.
The performance of the ADVIA Centaur® HCV assaywas assessed by testing random donor serum and plasmasamples, HCV positive patient samples, and commerciallyavailable seroconversion panels. The HCV positive sam-ples included the genotypes 1a, 1b, 2a, 2b, 3a, 4a, 4-non-aand 5 (all repeat positive in the ADVIA Centaur® HCVassay). In addition, specimens with potentially interferingsubstances, including multiple myeloma, rheumatoid factor,human anti-mouse antibodies (HAMA) and other infectionswere tested. For the population studies, the predicate (com-parison) test for the HCV assay was the Abbott AxSYMHCV 3.0 assay.
Reactive or discordant samples were re-tested in dupli-cate. HCV status was confirmed by resolution testing withthe RIBA immunoblot assay. Specimens that had a RIBAindeterminate interpretation were not included in the speci-ficity calculation as they could be classified as neither posi-tive nor negative. Those specimens were further tested by aNucleic Acid Amplification Technology (NAT) HCV assayfor informational reporting purposes. Comparison analysiswas performed on initial results (without equivocal results)to determine relative sensitivity and relative specificity. Thetest specificity was calculated from the donor and hospi-talized populations (as per CTS), while the test sensitivitywas calculated from the results of the HCV positive spec-imen population. Resolved sensitivity and resolved speci-ficity were calculated after resolution testing.
Evaluation of the ADVIA Centaur® HCV assay in pop-ulation studies with the comparison assay (n = 5651; site1: 2844; site 2: 2807) demonstrated an initial sensitivity of96.1% and an initial specificity of 99.86%. Upon verifica-tion of the HCV status of ‘Repeat Reactive’ samples by theRIBA method, the resolved sensitivity was 99.6% and theresolved specificity was 99.90% (Table 1).

S18 J. van Helden, G.A. Denoyel / Journal of Clinical Virology 30S1 (2004) S16–S18
Precision studies with the NCCLS testing protocol re-flected a total imprecision for samples in the index rangesof 1.0–3.0 and 5.0–10.0 of<10% and<10%, respectively(NCCLS, 1999).
Detection of HCV reactive samples in 20 seroconver-sion panels was relatively equivalent to the predicate device(AxSYM HCV 3.0) (Table 2). The cross-reactivity studydemonstrates no significant cross-reactivity with the otherviral infections and disease state samples tested.
In summary, the clinical and analytical performance ofthe ADVIA Centaur® HCV assay is equivalent to or betterthan the performance of the predicate device.
2.3. ADVIA Centaur® HIV 1/O/2 assay
The ADVIA Centaur® HIV 1/O/2 assay is based on atwo-step direct antibody-bridging format. The assay usesyeast recombinant derived antigens corresponding to theviral envelope and core proteins. Recombinant antigens in-clude an HIV-1 envelope protein, HIV-1 core protein p24,and an HIV-2 envelope-oriented protein, and an HIV-1group O peptide. Use of these recombinants and peptidesimproves detection of HIV-1 antibody to group M and groupO with specific antigens and/or HIV-2 antibody positivespecimens and minimizes non-specific reactions that occurdue to cross-reactions with human cell proteins present inwhole viral lysate preparations.
Results are reported as INDEX values read from a storedmaster curve. The test results are reported as INDEX valueswith a cutoff of 1.0.
Assay performance was evaluated by testing randomblood donor populations, HIV-1 (n = 447) and HIV-2positive (n = 100) patient populations and commerciallyavailable seroconversion panels. The HIV-1 positive sam-ples included HIV-1 non-B subtypes, HIV-1 subtypes A–G,as well as five HIV-1 subtype O (all repeat positive in theADVIA Centaur® HIV 1/O/2 assay). All samples weretested in parallel with the Abbott AxSYM HIV 1+ 2 gOassay (reference method). Samples that were reactive wererepeated in duplicate. Results of samples that were ‘Re-peat Reactive’ or remained discrepant were confirmed withWestern blot analysis. Samples that were indeterminate byWestern blot were further analyzed by Nucleic Acid Am-plification Technology assays. Comparison analysis wasperformed on initial results to determine relative sensitivityand relative specificity and again after repeat test results.Resolved sensitivity and resolved specificity calculationswere finalized after Western blot confirmatory testing.
Evaluation of the ADVIA Centaur® HIV 1/O/2 assay inthe population studies (n = 5852; site 1: 2959; site 2: 2893)
demonstrated an initial sensitivity of 98.23% and an initialspecificity of 99.94%. Upon verification of the HIV statusof ‘Repeat Reactive’ samples by Western blot method, theresolved sensitivity was 100% and the resolved specificitywas 99.87 (Table 1).
Detection of HIV reactive samples found in 20 sero-conversion panels was equivalent to the comparison device(AxSYM HIV 1 + 2 gO) (Table 2).
Specimens with potentially interfering substances, in-cluding HAMA, rheumatoid factor and other infectionswere tested and shown to not cause false positive results.Within-run and total assay imprecision (CV%) ranged from4.2% to 6.0% and from 6.9% to 9.4%, respectively.
These results prove that the clinical and analytical perfor-mance of the ADVIA Centaur® HIV 1/O/2 assay is equiva-lent to or better than other the commercially available HIVassays and performed equivalently with samples as speci-fied in the Common Technical Specifications of the IVDD.In conclusion, the ADVIA Centaur® HIV 1/O/2 assay is aspecific and precise automated immunoassay for the detec-tion of antibodies specific for HIV-1 group M and group Oand HIV-2.
3. Conclusions
The results of the European performance evaluation stud-ies fulfilled all requirements of the Common Technical Spec-ifications of the IVD Directive. Furthermore, the evaluationdata indicate that the fully automated ADVIA Centaur as-says for HBsAg, HBsAg confirmatory testing, anti-HCV,and anti−HIV 1/O/2 are specific and sensitive immunoas-says for the detection of HBV, HCV, HIV-1 and HIV-2. Theoverall performance of these methods is equivalent or bet-ter than currently available assays and is considered to bestate-of-the-art. Furthermore, these methods offer the flexi-bility of high throughput, reliability and the full automationbenefits of the ADVIA Centaur immunoassay system.
References
Commission Decision on common technical specifications for in vitro-diagnostic medical devices. Off J Eur Commun 2002;L131:17–30.
Directive 98/79/EC of the European Parliament and of the Council of27 October 1998 on in vitro diagnostic medical devices. Off J EurCommun 1998;L331:1–37.
Hendriks HA, Kortlandt W, Verweij WM. Standardized comparison ofprocessing capacity and efficiency of five new-generation immunoas-say analyzers. Clin Chem 2000;46:105–11.
NCCLS Document EP5-A. Evaluation of precision performance of clinicalchemistry devices. Approved guideline. 2nd ed. 1999.





























