Embed Size (px)
Citation preview
VASCULAR IMAGES
Fibromuscular dysplasia with multiple visceral arteryinvolvement
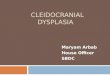
Natarajan Sekar, MD, MCh, and Rajendran Shankar, MS, MCh, Chennai, IndiaA 19-year-old female presented with episodic abdominal pain not related tofood intake. She had occasional vomiting but had no gastrointestinal bleed.Routine ultrasound examination picked up aneurysm of the superior mesen-teric artery (SMA). Computed tomography angiogram showed stenosis of theorigin of the SMA and multiple aneurysms involving the proximal SMA. Alarge collateral artery also showed aneurysm at its origin. The celiac artery andhepatic arteries were not visualized. Splenic artery was reconstituted throughgastroepiploic artery. Multiple collaterals from the phrenic and mammaryarteries were seen to supply the liver. Inferior mesenteric artery was dilated,and a large marginal artery was seen joining the superior mesenteric artery.Right renal artery showed mild irregularity at the proximal part (Cover).
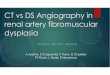
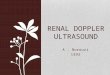
At surgery the stomach was pale, and no pulsations were felt in the splenicand epiploic vessels. Hepatic artery was thin and felt like a cord. The image in(A) shows the aneurysmal segment of SMA. The aneurysmal segment of theSMA was resected and an aorto-SMA interposition graft with polytetrafluo-roethylene was performed. The large collateral artery, which had an aneurysmat the origin, was also resected and reimplanted into the graft. A reversedsaphenous vein graft was anastomosed to the graft and to the splenic artery(B). The stomach regained color and good pulsations were felt in the epiploicarteries. Biopsy of the aneurysm sac confirmed fibromuscular dysplasia. Patienthad complete symptomatic relief. Postoperative angiogram done 2 monthslater showed patent grafts with good flow distally. The right renal artery lesionhad progressed to cause stenosis (C).
Fibromuscular dysplasia or arterial fibroplasia includes a heterogenousgroup of nonatherosclerotic occlusive and aneurysmal disease. Four types aredescribed, but medial fibroplasia is the most commonly seen. It is morecommon in young women, and the exact etiology is not known. Renal andcarotid arteries are commonly involved. Rarely, mesenteric and peripheralarteries are involved.1 Stenotic type is amenable for balloon dilatation but theaneurysmal one requires resection and replacement with a graft.2
REFERENCES
1. Schneider DB, Stanley JC, Messina LM. Renal artery fibroplasia and renovascular hypertension.In: Rutherford R, editor. Vascular surgery. 6th ed. Philadelphia PA: Elsevier Saunders; 2005. p.1789-1804.
2. Olin JW, Sealove BA. Diagnosis, management, and future developments of fibromusculardysplasia. J Vasc Surg 2011;53:826-36.
Submitted Oct 30, 2011; accepted Dec 27, 2011.
From the Apollo Hospitals.Author conflict of interest: none.E-mail: [email protected] editors and reviewers of this article have no relevant financial relationships to disclose per the JVS
policy that requires reviewers to decline review of any manuscript for which they may have a conflict ofinterest.
J Vasc Surg 2013;57:14010741-5214/$36.00Copyright © 2013 by the Society for Vascular Surgery.doi:10.1016/j.jvs.2011.12.079
1401