Embed Size (px)
Citation preview

�
CLINICAL REPORT
Focal Dermal Hypoplasia WithoutFocal Dermal Hypoplasia
Silvina N. Contreras-Capetillo,1* Maria Paola Lombardi,2 Doris Pinto-Escalante,1 andRaoul C. Hennekam2,31Departamento de Genetica, Centro de Investigaciones Regionales Dr. Hideyo Noguchi, Merida, Yucatan, Mexico2Department of Clinical Genetics, Academic Medical Center, University of Amsterdam, The Netherlands3Department of Pediatrics, Academic Medical Center, University of Amsterdam, The Netherlands
Manuscript Received: 14 May 2013; Manuscript Accepted: 6 October 2013
How to Cite this Article:Contreras-Capetillo SN, Lombardi MP,
Pinto-Escalante D, Hennekam RC. 2014.
Focal dermal hypoplasia without focal
dermal hypoplasia.
Am J Med Genet Part A 164A:778–781.
Focal dermal hypoplasia (FDH;Goltz–Gorlin syndrome) is anX-
linked dominant disorder affectingmainly tissues of ectodermal
and mesodermal origin. The phenotype is characterized by
hypoplastic linear skin lesions, eye malformations, hair and
teeth anomalies, and multiple limbs malformations. The disor-
der is caused by PORCNmutations. Here we describe a mother
and daughter with FDH in whom a c.938T>G in PORCN was
detected. Neither of the two had FDH, but otherwise the pheno-
typewas classical. Focal skin hypoplasia is a hallmark of FDHbut
the present family indicates that FDH should also be considered
in absence of this skin manifestation. � 2013 Wiley Periodicals, Inc.
Key words: Goltz–Gorlin syndrome; focal dermal hypoplasia;
PORCN; variability
�Correspondence to:
Silvina N. Contreras-Capetillo, M.D., Centro Regional de Investigaciones
“Dr. Hideyo Noguchi”, Universidad Autonoma de Yucatan. Calle 96 s/n
x Av. Jacinto Canek y calle 47 Paseo de Las Fuentes. C.P. 97225, Merida,
Yucatan, Mexico. E-mail: [email protected]
Article first published online in Wiley Online Library
(wileyonlinelibrary.com): 19 December 2013
DOI 10.1002/ajmg.a.36341
INTRODUCTION
Focal dermal hypoplasia (FDH; OMIM #305600) or Goltz–Gorlin
Syndrome is an infrequently reported X-linked dominant disorder
[Goltz et al., 1962]. About 250 patients have been reported, most are
females and few are (usually mosaic) males, 95% of the cases are
sporadic and 5% are familial [Goltz, 1990; Hennekam et al., 2010].
FDHaffectsmainly tissues of ectodermal andmesodermal origin. The
main skin sign is a linear FDH, often going along with linear hyper-
pigmentations or hypopigmentations and fat herniations. Multiple
papillomas around the orifices, and telangiectasias have also been
reported [Kore-Eda et al., 1995]. Skin manifestations can be highly
variable and be present at birth or develop with age, although dermal
hypoplasia is usually evident from birth. Other FDH characteristics
are craniofacial signs (microcephaly, sparse hair, microphthalmia,
colobomaof iris or retina, lacrimal duct anomalies, cleft lip andpalate,
and prominent ears), dental anomalies (small teeth, hypodontia,
and enamel defects) and skeletal anomalies (syndactyly, absent digits,
ectrodactyly and polydactyly, in any combination). A host of other
manifestations has been published [Hennekam et al., 2010].
In 2007, mutations in PORCN, located at Xp11.23 and encoding
the human homolog of Drosophila melanogaster porcupine, were
found to cause FDH[Grzeschik et al., 2007;Wang et al., 2007].Over
100 PORCN variants are known [Lombardi et al., 2011].
2013 Wiley Periodicals, Inc.
Here we report on a mother and daughter with a PORCN
mutation and a phenotype which was classical for FDH, but
who did not have the main dermal manifestation, that is, FDH.
CLINICAL REPORT
The proband was born at term after an uneventful pregnancy to
nonconsanguineous Mexican parents who had experienced two
earlier spontaneous miscarriages. At birth weight, length and OFC
were normal. Multiple anomalies of face and distal limbs and a
giant omphalocele were evident. She followed a normal cognitive
development. At 5 years all bodyparameterswere found tobe below
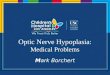
the 3rd centile. Physical examination (Fig. 1) showed sparse hair,
facial asymmetry, right microphthalmia and coloboma, irregular
vermilion of upper and lower lip, dental misalignment and thin,
prominent ears. She had syndactyly and brachydactyly of second
to third fingers bilaterally, absent third fingernail, clinodactyly
of the fifth fingers and ectrodactyly of her right foot. Her skin
showed slightly hyperpigmented lines following Blaschko’s lines
but no dermal hypoplasia or fat herniations. She had a bifid
sternum, underdeveloped labia majora and absent labia minora.
778

FIG. 1. Manifestation of FDH in the proband. A: Facial asymmetry. B: Hyperpigmented lines following Blaschko lines. C: Syndactyly and nails
defect. D: Right foot ectrodactyly.
CONTRERAS-CAPETILLO ET AL. 779
Chromosome analysis showed a normal female karyotype (46,XX).
Excretory urography showed vesicoureteral reflux, and a full
skeletal survey demonstrated osteopathia striata (Fig. 2).
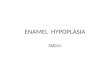
Her mother was found to have unilateral microphthalmia and
coloboma, irregular vermillion of the upper and lower lip, thin ears,
and abortive ectrodactyly of the right hand (Fig. 3). She had linear
hyperpigmented skin lesions on her legs, but no dermal hypoplasia
or fat herniation.
Molecular analysis showed a single nucleotide change, c.938T>G
(p.Leu313Arg) in PORCN in both proband and her mother.
This mutation has not been reported previously. In silico analysis
with four prediction programs (SIFT, Polyphen 2, Align GVGD and
MutationTaster) predicts this change to be pathogenic. In addition
Leu313isconservedacrossspeciesdowntoamphibians.Thismutation
isnot found inmore than10,000 control alleles of EuropeanAmerican
andAfricanAmericandescent (ESP6500SI-V2,ExomeVariant Server,
NHLBI GO Exome Sequencing Project (ESP), Seattle, WA (URL:
http://evs.gs.washington.edu/EVS/) May, 2013 accessed). X inactiva-
tion ratios were 50:50 in the mother and 65:35 in the daughter.
FIG. 2. Osteopathia striata in the proband (arrow).
DISCUSSION
FDH can be clinically diagnosed based on the multisystem
anomalies which are widely variable and of which the skin

FIG. 3. Mild FDH phenotype in the mother. A: Right eye microphthalmia. B: Linear hyperpigmented skin lesions. C: Abortive ectrodactyly. D:
Partial syndactyly.
780 AMERICAN JOURNAL OF MEDICAL GENETICS PART A
findings are paramount. Dermal hypoplasia with fat
herniations are the commonest cutaneous lesions, and a mildly
affected skin is unusual in FDH [Maas et al., 2009]. All
patients reported in literature had true dermal hypoplasia
except one, molecularly unproven patient in whom only
hypo-/hyperpigmentations of the skin were reported [Ayme
and Fraser, 1982].
In the present patients the facial and skeletalmanifestations were
strong clues for FDH despite the absence of the dermal hypoplasia.
The skin was involved however, showing in the hypo-/hyperpig-
mentations following Blaschko lines, and there were also hair and
nail abnormalities, which makes it unlikely that absence of the
mutation in tissues derived from the ectoderm explains the lack of
dermal hypoplasia.
FDH is an X-linked dominantly inherited disorder, which
usually occurs in sporadic patients but in 5% more than a single
individual in a family is affected. Intrafamilial variability has shown
that a diagnosis in an individual may go unrecognized until the
birth of amore severely affected child [Ruiz-Maldonado et al., 1974;
Temple et al., 1990; Maas et al., 2009]. Lyonization has been
suggested to explain the clinical variability of FDH [Grzeschik
et al., 2007]. In the present family random X inactivation was
observed in both mother and daughter. Maas et al. [2009], sug-
gested that other, as yet undetermined factors like environmental,
epigenetic ormodifying genes are of importance in determining the
FDHphenotype. It remains uncertain whether the unusual presen-
tation in this family can depend in part on the particular PORCN
mutation that was found. This PORCN mutation has not been
reported previously. In a recent overview of PORCN mutations
there was a single FDH patient without FDH [Lombardi et al.,
2011], and at present the LOVD database contains an additional
individual with a PORCNmutation in whom no FDH was found.
These PORCN mutations were c.787T>G and c.845þ1G>C,
respectively. This may indicate the presence of skin hypoplasia is
not depending on the nature or site of the PORCN mutation.
Including the present patients, four of the 121 individuals with
a PORCN mutation in whom sufficient clinical information is
available, do not have a FDH.
We conclude that the present family shows that the variability of
FDH is even larger than anticipated, and that it can also occur
without dermal hypoplasia. This denotes that the indication to
initiate molecular analysis of PORCN in children with only limited

CONTRERAS-CAPETILLO ET AL. 781
manifestations of FDH should be wide, also in the absence of the
name-giving skin manifestation.
ACKNOWLEDGMENTS
We are grateful to the family for their participation in this study.
REFERENCES
Ayme S, Fraser FC. 1982. Possible examples of the Goltz syndrome (focaldermal hypoplasia) without linear areas of skin hypoplasia. Birth defectsOrig Artic Ser 18:59–65.
Goltz RW. 1990. Focal dermal hypoplasia. Pediatr Dermatol 7:313–314.
Goltz RW, Peterson WC, Gorlin RJ, Ravits HG. 1962. Focal dermalhypoplasia. Arch Dermatol 86:708–717.
Grzeschik KH, Bornholdt D, Oeffner F, Konig A, del Carmen Boente M,Enders H, Fritz B, Hertl M, Grasshoff U, Hofling K, Oji V, Paradisi M,Schuchardt C, Szalai Z, Tadini G, Traupe H, Happle R. 2007. Deficiencyof PORCN, a regulator of Wnt signaling, is associated with focal dermalhypoplasia. Nat Genet 39:833–835.
HennekamRC,Krantz ID,Allanson J. 2010.Gorlin’s syndromesof theheadand neck. New York: Oxford University Press. p. 1452
Kore-Eda S, Yoneda K, Ohtani T, Tachibana T, Furukawa F, Imamura S.1995. Focal dermal hypoplasia (Goltz syndrome) associated with multi-ple giant papillomas. Br J Dermatol 133:997–9999.
Lombardi MP, Bulk S, Celli J, Lampe A, Gabbett MT, Ousager LB, van derSmagt JJ, Soller M, Stattin EL, Mannens MAMM, Smigiel R, HennekamRC. 2011. Mutation update for the PORCN gene. Hum Mutat 32:723–728.
Maas SM, Lombardi MP, van Essen AJ, Wakeling EL, Castle B, TempleIK, Kumar VKA, Writzl K, Hennekam RC. 2009. Phenotype andgenotype in 17 patients with Goltz–Gorlin syndrome. J Med Genet 46:716–720.
Ruiz-Maldonado R, Carnevale A, Tamayo L, Milonas de Montiel E. 1974.Focal dermal hypoplasia. Clin Genet 6:36–45.
Temple IK, MacDowall P, Baraitser M, Atherton DJ. 1990. Focal dermalhypoplasia (Goltz syndrome). J Med Genet 27:180–187.
Wang X, Reid Sutton V, Omar Peraza-Llanes J, Yu Z, Rosetta R, Kou YC,EbleT, PatelA, ThallerC, FangP,VandenVeyver IB. 2007.Mutation inXlinked PORCN, a putative regulator ofWnt signaling, cause focal dermalhypoplasia. Nat Genet 39:836–838.