Embed Size (px)
Citation preview

1
• Online Data Supplement
Hypertension, a leading cause of other cardiovascular diseases, is also a leading cause of disability and death
worldwide.1 Over 1 billion people are diagnosed with hyper-tension, such that 1 in 3 individuals has elevated blood pressure in numerous countries.2 About 90% of the burden of cardio-vascular disease is borne by the low-and middle-income coun-tries (LMIC) that have only ≈10% of the research capacity and healthcare resources to confront the scourge.3
Hypertension had been regarded as a disease of the afflu-ent people of the world.4,5 However, it has emerged in the LMIC where it affected ≈1 in 5 adults in 2013.5 This rate has been projected to increase such that 3 in 4 adults will be living with hypertension by 2025 in LMIC.6,7 Awareness and levels of hypertension control in LMIC are still low when compared with that in HIC.8 For instance, hypertension control in United States is 52% compared with 5% to 10% in Africa.9 The major reason for this disparity could be the lack of awareness of access and adherence to implementable hypertension guide-lines in LMIC.10
Furthermore, hypertension management is complicated by choice, availability, and affordability of appropriate medications.
The cultural aspects of life-long use of medications for hyper-tension, variable needs of individual patients, and inconsistent designs and outcomes from clinical trials have also compounded the management.11 The different genetic architectures of indi-viduals with hypertension12,13 may determine the choice and response to treatment. Some of these antihypertensive agents are costly and not evenly accessible and distributed in LMIC.
Therefore, guidelines that work in HIC settings may not be acceptable, effective, implementable, and applicable to LMIC because of the lack of supporting resources. In addition to broad international guidelines tailored to the needs of large regions with similar socioeconomic implementation contexts, it may be crucial for every country to further adapt implemen-tation aspects and dissemination channels of key recommen-dations by engaging and empowering all relevant stakeholders thereby enhancing adherence and impact.
This review is necessitated by the need to bring hyperten-sion control to the individual’s doorstep by developing and deploying such pragmatic hypertension guidelines in these countries to significantly reduce the burden of associated car-diovascular morbidities and mortalities.
From the Department of Medicine and University College Hospital (M.O., J.Y., T.M., L.O., T.F., E.S.M., B.S.) and Institute for Advanced Medical Research and Training, College of Medicine (R.A.), University of Ibadan, Nigeria; WFNR-Blossom Specialist Medical Center, Ibadan, Nigeria (M.O., E.U.); Federal Teaching Hospital, Ido-Ekiti, Nigeria (P.O.); Department of Medicine, CRONICAS Center of Excellence in Chronic Diseases, Universidad Peruana Cayetano Heredia, Lima, Peru (J.J.M.); Department of Neurology (W.F., R.S., B.O.) and Department of Public Health Sciences (M.G.), Medical University of South Carolina, Charleston; School of International Development and Global Studies, University of Ottawa, Ontario, Canada (S.Y.); Department of Family and Emergency Medicine, University of Montreal, Quebec, Canada (J.K.); Department of Public Health, Health Service Organization, Hamilton, Ontario, Canada (L.T.); Departments of Anesthesia/Pediatrics, McMaster University, Hamilton, Ontario, Canada (J.V.O.); Department of Health Research, Ministry of Health & Family Welfare, Government of India, New Delhi, India (P.M.); Sydney Medical School, University of Sydney, New South Wales, Australia (C.C., R.J.); Non Communicable Diseases Research Unit, South African Medical Research Council, Tygerberg, South Africa (A.K.); School of Clinical Sciences at Monash Health, Monash University, Clayton, Victoria, Australia (A.G.T.); Cardiovascular Global Health Division of Cardiology, Duke University Medical Center, Durham, NC (G.S.B.); Global Alliance for Chronic Diseases, UCL Institute for Global Health, London, United Kingdom (G.P.); Department of Public Health, Academic Medical Centre, University of Amsterdam, The Netherlands (C.A.); Department of Experimental and Clinical Medicine, University of Florence, Italy (P.A.M.); and Developmental Pathways for Health Research Unit, University of the Witwatersrand, Johannesburg, South Africa (S.N.).
*These authors contributed equally to this work.†Control Unique to Cardiovascular Diseases in Low and Middle Income Countries.The online-only Data Supplement is available with this article at http://hyper.ahajournals.org/lookup/suppl/doi:10.1161/HYPERTENSIONAHA.
116.08290/-/DC1.Correspondence to Mayowa Owolabi, Department of Medicine, University College Hospital and University of Ibadan, Ibadan, Nigeria. E-mail
Gaps in Hypertension Guidelines in Low- and Middle-Income Versus High-Income Countries
A Systematic Review
Mayowa Owolabi,* Paul Olowoyo,* J. Jaime Miranda, Rufus Akinyemi, Wuwei Feng, Joseph Yaria, Tomiwa Makanjuola, Sanni Yaya, Janusz Kaczorowski, Lehana Thabane,
Josefien Van Olmen, Prashant Mathur, Clara Chow, Andre Kengne, Raelle Saulson, Amanda G. Thrift, Rohina Joshi, Gerald S. Bloomfield, Mulugeta Gebregziabher, Gary Parker,
Charles Agyemang, Pietro Amedeo Modesti, Shane Norris, Luqman Ogunjimi, Temitope Farombi, Ezinne Sylvia Melikam, Ezinne Uvere, Babatunde Salako, Bruce Ovbiagele;
for the COUNCIL Initiative†
(Hypertension. 2016;68:00-00. DOI: 10.1161/HYPERTENSIONAHA.116.08290.)© 2016 American Heart Association, Inc.
Hypertension is available at http://hyper.ahajournals.org DOI: 10.1161/HYPERTENSIONAHA.116.08290
Brief Review
by guest on May 18, 2018
http://hyper.ahajournals.org/D
ownloaded from
by guest on M
ay 18, 2018http://hyper.ahajournals.org/
Dow
nloaded from
by guest on May 18, 2018
http://hyper.ahajournals.org/D
ownloaded from
by guest on M
ay 18, 2018http://hyper.ahajournals.org/
Dow
nloaded from
by guest on May 18, 2018
http://hyper.ahajournals.org/D
ownloaded from
by guest on M
ay 18, 2018http://hyper.ahajournals.org/
Dow
nloaded from
by guest on May 18, 2018
http://hyper.ahajournals.org/D
ownloaded from
by guest on M
ay 18, 2018http://hyper.ahajournals.org/
Dow
nloaded from
by guest on May 18, 2018
http://hyper.ahajournals.org/D
ownloaded from
by guest on M
ay 18, 2018http://hyper.ahajournals.org/
Dow
nloaded from
by guest on May 18, 2018
http://hyper.ahajournals.org/D
ownloaded from
by guest on M
ay 18, 2018http://hyper.ahajournals.org/
Dow
nloaded from
by guest on May 18, 2018
http://hyper.ahajournals.org/D
ownloaded from
by guest on M
ay 18, 2018http://hyper.ahajournals.org/
Dow
nloaded from
by guest on May 18, 2018
http://hyper.ahajournals.org/D
ownloaded from
by guest on M
ay 18, 2018http://hyper.ahajournals.org/
Dow
nloaded from
by guest on May 18, 2018
http://hyper.ahajournals.org/D
ownloaded from
by guest on M
ay 18, 2018http://hyper.ahajournals.org/
Dow
nloaded from
by guest on May 18, 2018
http://hyper.ahajournals.org/D
ownloaded from
by guest on M
ay 18, 2018http://hyper.ahajournals.org/
Dow
nloaded from
by guest on May 18, 2018
http://hyper.ahajournals.org/D
ownloaded from

2 Hypertension November 2016
We performed a systematic review to compare the quantity and quality of published clinical practice guidelines for hyper-tension in individual LMIC to HIC over the past decade in terms of their number, quality of evidence, socioeconomic and ethical–legal contextualization, ability to be implemented and dissemination to actively engage and empower all relevant stakeholders. Overall, we aimed to identify the gaps and to propose suitable solutions to enhance the quality and impact of hypertension guidelines in LMIC.
MethodologyUsing the Preferred Reporting Items for Systematic Review and Meta-Analyses guidelines,14 a systematic review was per-formed with hypertension, high blood pressure, and guide-line as the primary search items. Secondary search items included clinical practice, implementation, translation, and prevention, whereas the tertiary search items included World Health Organization, United States, American, International, European, African, Asian, Japanese, South and Latin American, Society, Association, League and Group.
Inclusion and Exclusion CriteriaThe review included guidelines published from January 1, 2005, to December 31, 2015, in PubMed, Google Scholar, African Journals Online, Excerpta Medica Database, and Directory of Open Access Journals databases. Guidelines in other languages that we were unable to translate into English were excluded.
Eligible guidelines were also searched country by coun-try and region by region. For instance, the following countries categorized as low-income countries were searched online for hypertension guidelines: Cambodia, Chad, South Sudan, Tanzania, Zimbabwe, Comoros, Haiti, Benin, Nepal, Mali, Sierra Leone, Burkina Faso, Afghanistan, Uganda, Rwanda, Mozambique, Togo, Guinea-Bissau, North Korea, Ethiopia, Eritrea, Guinea, Gambia, Madagascar, Niger, Democratic Republic of Congo, Liberia, Central African Republic, Burundi, Malawi, and Somalia. Some unpublished guidelines obtained by direct contact with clinicians in some countries were also included. Duplicates were excluded.
The guidelines were characterized according to income level, evidence class, recommendation level, and number of reviews performed during the study period.
Data Extraction, Critical Appraisal, and SynthesisGoogle translate was used to translate the Brazilian hyperten-sion guideline from Portuguese to English.
To determine the quality and the developmental processes of the guidelines, 2 independent reviewers extracted infor-mation on each guideline in terms of compliance with the Institute of Medicine’s (IOM) 15,16 standards for developing clinical practice guidelines that include transparency, conflicts of interest, multidisciplinary approach, systematic reviews, strength or recommendations, external review, and regular updates. Other quality indices include coverage of the cardio-vascular quadrangle17 (surveillance and research, prevention, acute care, and rehabilitation), contextualization and translat-ability, attention to socioeconomic, ethical, legal, and psycho-logical issues, and deployment through multiple dissemination
channels to all stakeholders. Stakeholders included physi-cians, nonphysician healthcare providers, primary caregivers, policy makers, payers, patients, the populace, and imple-mentation partners. Proportions of quality indices fulfilled in LMIC guidelines were compared with those in HIC.18
ResultsFifty hypertension guidelines are found Figures S1 and S2 in the online-only Data Supplement, including 20 from PubMed and 30 from Google Scholar databases. Six additional unpub-lished guidelines were obtained after consultation with col-leagues involved in hypertension control and management across the globe through the Global Alliance for Chronic Diseases.19–24 No guideline was found in African Journals Online, Excerpta Medica Database, and Directory of Open Access Journals databases. After the removal of duplicates, 39 guidelines from 28 countries were left. Of these, 16 were excluded because they were not written in English and could not be translated. Only 1 was found from the 31 countries in the low-income category, whereas 9 guidelines were found from middle-income countries. The remaining 13 were from HIC. Five guidelines from the United States were excluded leaving the American Society of Hypertension/International Society of Hypertension, which is the only one officially endorsed. Eighteen guidelines were included for qualitative and quantitative syntheses.
The guidelines were characterized according to organi-zations that developed them, year of publication, number of reviews, level of evidence, clinical spectrum addressed, and adherence to IOM recommendations (Tables 1 through 3). Appraisal was also based on country of origin (Table 4; Tables S1 through S3). Many guidelines from HIC were not named after individual countries unlike those from LMIC that were specific for the individual countries. Rather, guidelines from HIC were adopted by the countries in which the associations that developed them are based.
None of the guidelines retrieved utilized the Grading of Recommendations Assessment, Development and Evaluation system.42 Few guidelines covered the entire spectrum of the cardiovascular quadrangle (Table 4), ethical, social, legal, psychological, and economic considerations, or elaborated plans to deploy and disseminate recommendations to all rel-evant stakeholders (Table 4; Tables S1 and S2). None of them applied translatability weighting to their recommendations (Table S2).
More of the hypertension guidelines from HIC followed the IOM recommendations. However, the South African Hypertension Guideline26 and the 2010 Chinese guideline from LMIC were developed with strict adherence to the IOM recommendations (Table 3). The 2010 Chinese guidelines8 described the treatment of hypertension in chronic kidney disease, stroke, and coronary artery disease. The recommen-dations were based on high level of evidence (randomized controlled trials), meta-analysis, and local studies.8 Guidelines from Nigeria and Mexico have not been updated because they were published (Table 1).25 Compared with the guide-lines from HIC, the spectrum of the associated clinical issues addressed and the choice of antihypertensive agents were not clearly discussed (Table 2; Table S1).
by guest on May 18, 2018
http://hyper.ahajournals.org/D
ownloaded from

Owolabi et al Systematic Review of Hypertension Guidelines 3
Table 1. Summary of the Hypertension Guidelines
Guideline/Title Authors Organizations Country Year Strategy IncomeNo. of
Revisions*
1. Guidelines for the management of hypertension in Nigeria
Onwubere and Kadiri25
Nigerian Hypertension Society, Enugu
Nigeria 2005 PubMed, Google Scholar
Middle 0
2. South African hypertension guidelines Seedat and Rayner26
Hypertension Guideline Working Group
South Africa
2011 PubMed, Google Scholar
Middle 5
3. Brazilian guidelines on hypertension Socieda et al27 Brazilian Society of Cardiology, Hypertension
and Nephrology
Brazil 2010 Google Scholar Middle 2
4. 2010 Chinese guidelines for the management of hypertension
Liu8 Chinese Hypertension League, CDC
China 2011 PubMed, Google Scholar
Middle 3
5. Clinical guidelines for detection, prevention, diagnosis and treatment of systemic arterial hypertension in Mexico
Rosas et al28 National institute of Cardiology
Mexico 2008 Google Scholar Middle 0
6. The Japanese Society of Hypertension guidelines for the management of hypertension (JSH 2009)
Shimamoto et al29 Hypertension Committee for Guidelines for
the Management of Hypertension
Japan 2009 Google Scholar High 2
7. Hypertension guidelines Aronow30 American Heart Association America 2011 Google Scholar High 0
8. 2013 ESH/ESC guidelines for the management of arterial hypertension
Mancia et al.31 ESH and the ESC Europe 2013 Google Scholar High 2
9. JNC 8 James et al32 Not endorsed. Previous version endorsed by NHLBI.
America 2014 PubMed, Google Scholar
High 7
10. Management of hypertension in adults: the 2013 French Society of Hypertension guidelines
Blacher et al33 French Society of Hypertension, general
practitioners
France 2013 PubMed, Google Scholar
High 0
11. 2010 Guidelines of the Taiwan Society of Cardiology for the management of hypertension
Chiang et al34
Hypertension committee of the Taiwan Society of
Cardiology
Taiwan 2010 PubMed, Google Scholar
High Not stated
12. ASH/ISH Wood35 ASH/ISH/Asia Pacific Society of Hypertension
America 2013 PubMed, Google Scholar
High Not stated
13. ACCF/AHA Aronow et al36 ACCF/AHA America 2011 PubMed,Google Scholar
High Not stated
14. CHEP Dasgupta et al37 CHS, Blood Pressure Canada, The Canadian Stroke Network, The
Canadian Society of Internal Medicine
Canada 2014 PubMed, Google Scholar
High Not stated
15. AHA/ACC/CDC Go et al38 AHA/ACC/CDC America 2013 PubMed, Google Scholar
High Not stated
16. AHA Calhoun et al.39 AHA America 2008 PubMed, Google Scholar
High Not stated
17. NICE Ritchie et al40 BHS, NICE, ESH, patients representatives
UK 2011 PubMed, Google Scholar
High 4
18. Practical guidelines for hypertension management
Rau and Nayak19 Association of Physician of India
India 2012 Unpublished Middle Not stated
19. Clinical practice guidelines Wijesisiwardene and Mohideen20
Sri Lanka Unpublished Middle Not stated
20. Guide to management of hypertension 2008.23
Not stated National Heart Foundation of Australia
Australia 2010 Unpublished High 2
21. Ethiopia standard treatment guidelines Yewondwossen Tadesse et al21
Food, Medicine and Healthcare Administration and Control Authority of
Ethiopia
Ethiopia 2014 Unpublished Low 2
(Continued )
by guest on May 18, 2018
http://hyper.ahajournals.org/D
ownloaded from

4 Hypertension November 2016
Significantly more guidelines from HICs were developed with involvement of high-quality systematic reviews of rel-evant evidence (63.5% versus 10.0%; P=0.033). Overall, the proportions of guidelines that applied IOM recommendations, underwent frequent reviews, and developed active dissemina-tion channels to engage all relevant stakeholders were higher among the HIC (Table S3).
DiscussionIt is clear from this review that there is dearth of hyperten-sion guidelines in the LMIC, particularly in low-income coun-tries where only one existed.21 The available guidelines in the middle-income countries are just limited to several countries; 4 of which were not published in peer-reviewed journals and not accessible in any of the online databases.19,20,22 This is not in accordance with the recommendation of the World Health Assembly and the World Health Organization Regional Committee for Africa that countries in the region should be encouraged to establish country-specific recommendations for the prevention and management of hypertension.5,25
There is an urgent need for this as the genomics,43 socio-economic context, and healthcare policies of these countries vary from region to region, especially on healthcare financ-ing and implementation of lifestyle modifications44,45 such as smoking cessation and reduction in alcohol consumption. However, healthy lifestyle is an essential component of any effective hypertension treatment guideline, and it is recom-mended for the entire populace.46 The process of generat-ing LMIC-specific fine-tuning of recommendations can be facilitated and fast-tracked by first generating guidelines with unique recommendations that are broadly implementable in the socioeconomic setting of LMIC.
Currently, guidelines from LMIC are not unique to LMIC setting as they were adopted from the existing HIC guidelines without due considerations about their implementability.26 They were not based on contextually relevant locally derived evidence. Indeed, as alluded to in the 2012 South African Hypertension guidelines,26 the HIC guidelines have some recommendations that LMIC may not be able to implement because of the socioeconomic context within the countries.11
Moreover, many of the LMIC guidelines did not specify the level of evidence and did not address hypertension man-agement in special situations such as chronic kidney disease, coronary heart disease, heart failure, diabetes mellitus, and
stroke. The choice of medications and the target BP levels for hypertension in special situations were also not addressed.
Conversely, more HIC guidelines underwent frequent reviews, applied IOM recommendations, and developed active dissemination channels. However, guidelines from HIC also have rooms for improvement. For instance, the American Society of Hypertension/International Society of Hypertension guideline35 did not follow all the IOM recom-mendations. Even, the authors recommend that the readers should not consider the guideline as an evidence-based set of recommendations. Although, this guideline addressed the management of hypertension in people with comorbidities, the evidence for its recommendations is mostly based on the expert opinion. However, the American College of Cardiology Foundation/American Heart Association hypertension guide-line36 complied with some of the IOM recommendations for the development of formal guidelines. Its focus is mainly on the management of hypertension in the elderly and so it is not comprehensive. Other guidelines that address management in the elderly include the European Society of Hypertension/European Society of Cardiology,31 National Institute for Clinical Excellence,40 and Canadian Hypertension Education Program37 hypertension guidelines.
The American Heart Association, South African Hypertension guidelines, and National Institute for Clinical Excellence guidelines are the only hypertension guidelines that recommend specific drugs for the management of resis-tant hypertension.40 Despite the fact that the Joint National Committee 8 strictly followed the IOM recommendations, its recommendations are not officially endorsed and are not com-prehensive.32 This is because its development was based only on randomized controlled trials, unlike the European Society of Hypertension/European Society of Cardiology guide-line that included data from meta-analysis and observational studies.31The European Society of Hypertension/European Society of Cardiology guideline that is comprehensive enough addressing detection, evaluation, and treatment of hypertension can be useful, where there is limitation to direct application by virtue of different health systems, standard of care, and avail-ability of antihypertensive agents, especially in the LMIC.31
For implementation of these guidelines, both in LMIC and HIC, nonpharmacological and multidisciplinary approaches to the total care of the patients were advocated.31 However, the multidisciplinary approach was limited to the physicians
22. Sudan hypertension guidelines Sulima and Aboud22
Sudan Society of Hypertension, FMoH-NCDs
Directorate
Sudan 2012 Unpublished Middle Not stated
23. 2009 Kenya guideline for hypertension management
Crouch24 Ministry of Medical Services, Ministry of Public
Health and Sanitation
Kenya 2009 Unpublished Middle Not stated
ACC indicates American College of Cardiology; ACCF/AHA, American College of Cardiology Foundation/American Heart Association; ASH/ISH, American Society of Hypertension/International Society of Hypertension; BHS, British Society of Hypertension; CDC, Centers for Disease Control and Prevention; CHEP, Canadian Hypertension Education Program; CHS, Canadian Hypertension Society; ESH/ESC, European Society of Hypertension/European Society of Cardiology; FMoH-NCD, JNC 8, Eighth Joint National Committee; and NICE, National Institute for Clinical Excellence.
*How often each guideline has been reviewed since its first publication.
Table 1. Continued
Guideline/Title Authors Organizations Country Year Strategy IncomeNo. of
Revisions*
by guest on May 18, 2018
http://hyper.ahajournals.org/D
ownloaded from

Owolabi et al Systematic Review of Hypertension Guidelines 5
Table 2. Evidence Level and Spectrum of the Hypertension Guidelines
Guideline/Title Level of Evidence
Clinical Parameters Addressed
Hypertension in Special Situations Other Considerations
1. Guidelines for the management of hypertension in Nigeria
Not stated Not stated Not discussed Nil
2. South African hypertension guidelines
Adoption of ESH/ESC guidelines Weight, height, BMI, waist
circumference
DM, CKD Black, Asians, children, adolescents, HIV/AIDS
3. Brazilian guidelines on hypertension
Not stated DM, CKD, stroke …
4. 2010 Chinese guidelines for the management of hypertension
RCTs, meta-analyses, Chinese studies
Blood pressure, weight, height
CKD, stroke, coronary artery disease
…
5. Clinical guidelines for detection, prevention, diagnosis and treatment of systemic arterial hypertension in Mexico
Expert review Blood pressure, weight
Obesity, DM, dyslipidemia, smoking
Pregnancy, adolescents
6. The Japanese Society of Hypertension guidelines for the management of hypertension (JSH 2009)
Systematic review Blood pressure, weight
Stroke, MI, CKD Not stated
7. Hypertension guidelines Expert medical opinion Blood pressure Coronary artery disease, CKD,
Diabetes mellitus, Heart failure.
A therapeutic target of <140/90 mm Hg in patients <80 y and a systolic blood pressure of 140–145 mm Hg if tolerated in patients aged
≥80 y is reasonable
8. 2013 ESH/ESC guidelines for the management of arterial hypertension
Class 1; Level of Evidence A Systolic hypertension,
weight
Diabetic patients, elderly
Diuretics, β-blockers, CCB, ACEI, and ARB are viable options for initial hypertension therapy.
For DM, goal BP <140/85 mm Hg.
9. JNC 8 Most were based on expert opinion. Some systematic
review, RCTs, Class 1; Level of Evidence A.
Systolic and diastolic blood
pressure
CKD, DM, Nonblack, black
β-Blockers are no longer considered as an initial therapy option
10. Management of hypertension in adults: the 2013 French Society of Hypertension guidelines
Systematic review, literature analysis, meta-analysis, Consensus conferences, previous hypertension
recommendations
Blood pressure CKD, DM …
11. 2010 Guidelines of the Taiwan Society of Cardiology for the management of hypertension
RCTs, meta-analysis, epidemiological data: Taiwanese
cohort studies
Blood pressure Stroke, coronary artery disease, CKD
Not stated
12. ASH/ISH No classification or grading provided
Blood pressure DM, CKD, coronary artery disease. BP
<140/90.
Intended to be a primer with general information
13. ACCF/AHA Expert opinion, not RCTs Blood pressure … No recommendation with regards to antihypertensive agent selection
14. CHEP No classification or grading provided, RCT and systematic
review of RCT
BMI, waist circumference
Stroke, DM, CKD …
15. AHA/ACC/CDC No formal recommendation Blood pressure Stroke, CKD Specific recommendation regarding the diagnosis, evaluation or treatment of
hypertension are not provided
16. AHA No formal recommendation Blood pressure Stroke, CKD A scientific statement for the diagnosis, evaluation and management of patients with
resistant hypertension. Not a formal guideline. Consider incorporating mineralocorticoid
receptor antagonist (amiloride or spironolactone). Consider administering at
least 1 antihypertensive at bedtime.
(Continued )
by guest on May 18, 2018
http://hyper.ahajournals.org/D
ownloaded from

6 Hypertension November 2016
in their respective fields with little attention to the nurses, the pharmacists, and the dieticians in the guidelines from the LMIC (Table S1). Nearly all the guidelines from the HIC put this into consideration except the 2010 Guidelines of the Taiwan Society of Cardiology for the management of hypertension (Table S1). Indeed, almost all the guidelines regard management of comor-bidities as a component of hypertension treatment.
Other considerations in the development of these guide-lines such as translation, legal, and social issues were poorly addressed. In addition, there was no consideration of the psy-chological and economic situations of the targeted population. Socioeconomic situations of the targeted populace were only considered by the National Institute for Clinical Excellence and IV Brazilian hypertension guidelines, whereas only the Canadian Hypertension Education Program guidelines put the dissemination channels and hypertension surveillance into consideration (Table S2). Each guideline is expected to be updated every 3 years47 to include new evidence or treatment. Among the guidelines available for review as at the time of this publication, only the guidelines from Japan, Europe, and the United States are up-to-date.
Strengths and WeaknessesOur search strategy included all countries, and we critically appraised all available guidelines using rigorous and com-prehensive criteria. However, only the hypertension guide-lines written in or translated to the English language were included in this review. Other guidelines written in other
languages29,41,48–55 might have been missed.56 Furthermore, because we used the IOM recommendation to assess the quality of the guidelines, we did not use other similar param-eters such as the Global Rating Scale.57 The World Health Organization/International Society of Hypertension guideline (2003)47 was excluded because it was not covered in the stipu-lated time frame for our review.
We did not include the World Heart Federation Global car-diovascular disease Roadmap58 in this review because it is not a guideline per se. It enumerates the challenges to hypertension control and suggests some ways to overcome them in the deliv-ery of hypertension care to the populace. However, it did not demonstrate the developmental process of the recommendations that are to be delivered and the contextualization and other perti-nent implementation issues for hypertension guidelines. If these are faulty, hypertension control will still be a Herculean task.
Conclusions and Future PlansHypertension guidelines are necessary for proper and ade-quate prevention, early detection, evaluation, treatment and control of hypertension.44,59 However, they must meet basic criteria including validity, reliability/reproducibility, clini-cal applicability, clinical flexibility, socioeconomic, and ethical–legal contextualization, clarity, multidisciplinary process, scheduled review, and rigorous dissemination plan.60 Unfortunately, none of the available guidelines meet all of these criteria. This could explain why hypertension is still difficult to control in many regions of the world, as possible
17. NICE No classification or grading provided, systematic literature
search
Blood pressure CKD, MI, stroke Thiazides are no longer recommended as first line drugs. BP target for people >80 y is 150/90 mm Hg while it is 140/90 for others.
18. Practical guidelines for hypertension management
Not stated Blood pressure, weight
CKD, heart disease, DM, elderly,
pregnancy, resistant hypertension
Not stated
19. Clinical practice guidelines Adoption of JNC 6, JNC 7, WHO/ISH, ESH/ESC
Blood pressure, weight
CKD, DM, Not stated
20. Guide to management of hypertension 2008
Literature review Blood pressure, weight, JVP
CKD, DM, stroke Not stated
21. Ethiopia standard treatment guidelines
Adoption of JNC 7 Blood pressure, BMI
CKD, DM, heart disease
Not stated
22. Sudan hypertension guidelines
Adoption of JNC7, WHO/ISH, BHS, ESH/ESC, International
society of hypertension in black guidelines for management of
hypertension
Blood pressure, weight, height
CKD, DM, heart disease, stroke,
elderly
Not stated
23. 2009 Kenya guideline for hypertension management
Adoption of JNC7 Blood pressure Not stated Aim is to reduce diastolic BP to 90 mm Hg
ACC indicates American College of Cardiology; ACCF, American College of Cardiology Foundation; ACEI, angiotensin-converting enzyme inhibitors; AHA, American Heart Association; ARB, angiotensin receptor blockers; ASH/ISH, American Society of Hypertension/International Society of Hypertension; BHS, British Society of Hypertension; BMI, body mass index; BP, blood pressure; CCB, calcium channel blockers; CDC, Centers for Disease Control and Prevention; CHEP, Canadian Hypertension Education Program; CKD, chronic kidney disease; DM, diabetes mellitus; ESH/ESC, European Society of Hypertension/European Society of Cardiology; JNC, Joint National Committee; JVP, jugular venous pressure; MI, myocardial infarction; NICE, National Institute for Clinical Excellence; RCT, randomized controlled trials; and WHO, World Health Organization.
Table 2. Continued
Guideline/Title Level of Evidence
Clinical Parameters Addressed
Hypertension in Special Situations Other Considerations
by guest on May 18, 2018
http://hyper.ahajournals.org/D
ownloaded from

Owolabi et al Systematic Review of Hypertension Guidelines 7
valuable channels for the dissemination and implementation of guidelines are not harnessed.
It is obvious from this review that efforts are needed to develop hypertension guideline(s) for the LMIC (Table 5). The expected guideline(s) should be broad based, flex-ible, adaptable, socioculturally acceptable, and economically attainable for better health-related outcomes in patients with hypertension. As exemplified by National Institute for Clinical
Excellence guideline, patients’ participation should be incor-porated to enhance adherence to these recommendations.
Because de novo guideline development is time consum-ing, labor intensive, and costly, any guideline that fulfills most of the criteria used for this review may be considered as a template for the development of guidelines for LMIC, while incorporating local evidence only as available. This will be a more realistic approach to avoid duplication of efforts
Table 3. Compliance With Institute of Medicine’s15,16 Standards for Developing Clinical Practice Guideline
Guideline/Title TransparencyConflicts
of InterestMultidisciplinary
ApproachSystematic
ReviewsStrengths of
RecommendationClarity of
RecommendationExternal Review Updates
1. Guidelines for the management of hypertension in Nigeria
No No No No No No No No
2. South African hypertension guidelines Yes Yes Yes Yes Yes Yes Yes Yes
3. Brazilian guidelines on hypertension No No No No No No No No
4. 2010 Chinese guidelines for the management of hypertension
Yes Yes Yes Yes Yes Yes Yes Yes
5. Clinical guidelines for detection, prevention, diagnosis and treatment of systemic arterial hypertension in Mexico
Yes Yes Yes Yes Yes Yes Yes Yes
6. The Japanese Society of hypertension guidelines for the management of hypertension (JSH 2009)
Yes Yes Yes Yes Yes Yes Yes Yes
7. Hypertension guidelines41 No No No No No No No No
8. 2013 ESH/ESC guidelines for the management of arterial hypertension
Yes Yes Yes Yes Yes Yes Yes Yes
9. JNC 8 Yes Yes Yes Yes Yes Yes Yes Yes
10. Management of hypertension in adults: the 2013 French Society of Hypertension guidelines
Yes Yes Yes Yes Yes Yes Yes Yes
11. 2010 Guidelines of the Taiwan Society of Cardiology for the management of hypertension
No No No No No No No No
12. ASH/ISH No No No No No No No No
13. ACCF/AHA Yes Yes Yes Yes Yes Yes Yes Yes
14. CHEP No No No Yes Yes Yes No Yes
15. AHA/ACC/CDC No No No No No No No No
16. AHA No No No No No No No No
17. NICE Yes Yes Yes Yes Yes Yes Yes Yes
18. Practical guidelines for hypertension management
No No No No No No No No
19. Clinical practice guideline No No No No No No No No
20. Guide to management of hypertension 2008
Yes Yes Yes Yes Yes Yes Yes Yes
21. Ethiopia standard treatment guidelines
No No Yes No No No No No
22. Sudan hypertension guidelines Yes Yes Yes Yes Yes Yes Yes No
23. 2009 Kenya guideline for hypertension management
No No No No No No No No
AHA/ACC/CDC indicates American Heart Association/American College of Cardiology/Centers for Disease Control and Prevention; ACCF/AHA, American College of Cardiology Foundation/American Heart Association; ASH/ISH, American Society of Hypertension/International Society of Hypertension; CHEP, Canadian Hypertension Education Program; ESH/ESC, European Society of Hypertension/European Society of Cardiology; JNC, Joint National Committee; and NICE, National Institute for Clinical Excellence.
by guest on May 18, 2018
http://hyper.ahajournals.org/D
ownloaded from

8 Hypertension November 2016
while waiting for direct high-level evidence to accrue from the LMIC. Such guidelines should be socioculturally accept-able and cost-effective for successful implementation in the resource-poor regions of the world.
Developing and disseminating evidence-based pragmatic guidelines with concise implementable recommendations rel-evant to LMIC needs and socioeconomic context is urgently needed. With the active involvement of all stakeholders, the
recommended care and commodities could be made accept-able, accessible, available, appropriate, affordable, and effec-tive to reduce the global burden of hypertension.
Sources of FundingM. Owolabi and B. Ovbiagele are supported by U54 HG007479 and U01 NS079179 from the National Institutes of Health and the GACD (Global Alliance for Chronic Diseases). A.G. Thrift is supported by a fellowship from the National Health & Medical Research Council (1042600).
DisclosuresNone.
References 1. Cao X. A call for global research on non-communicable diseases. Lancet.
2015;385:e5–e6. doi: 10.1016/S0140-6736(14)62383-7. 2. Kearney PM, Whelton M, Reynolds K, Muntner P, Whelton PK, He J.
Global burden of hypertension: analysis of worldwide data. Lancet. 2005;365:217–223. doi: 10.1016/S0140-6736(05)17741-1.
3. Naghavi M, Wang H, Lozano R, et al. Global, regional, and national age-sex specific all-cause and cause-specific mortality for 240 causes of death, 1990–2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet. 2015;385:117–171. doi: 10.1016/S0140-6736(14)61682-2.
4. Hameed K, Kadir M, Gibson T, Sultana S, Fatima Z, Syed A. The fre-quency of known diabetes, hypertension and ischaemic heart disease in affluent and poor urban populations of Karachi, Pakistan. Diabet Med. 1995;12:500–503.
5. van de Vijver S, Akinyi H, Oti S, et al. Status report on hypertension in Africa-consultative review for the 6th Session of the African Union Conference of Ministers of Health on NCD’s. Pan African Medical Journal. 2014;16.
Table 4. Components of the Cardiovascular Quadrangle Addressed
Countries Income LevelPrimordial Prevention Prehypertension
Age-Specific Treatment Nutrition Exercise
Acute Care/Emergencies
Conventional Care Rehabilitation
America High No No Yes Yes Yes No Yes No
Australia High No Yes Yes Yes Yes Yes Yes No
Brazil Middle No Yes Yes Yes Yes Yes Yes No
Canada High Yes No Yes Yes Yes No Yes No
China Middle No No Yes Yes Yes No Yes No
Ethiopia Low No Yes No Yes Yes Yes Yes No
Europe High No Yes Yes Yes Yes Yes Yes No
France High No Yes Yes Yes Yes No Yes No
India Middle No No Yes yes yes yes yes No
Japan High No No No Yes Yes No Yes No
Kenya middle No No No Yes Yes Yes Yes No
Mexico Middle No No No Yes Yes No Yes No
Nigeria Middle Yes No No Yes Yes No Yes No
South Africa Middle Yes No Yes Yes Yes Yes Yes Yes
Sri Lanka Middle No Yes Yes Yes Yes Yes Yes No
Sudan Middle No Yes Yes Yes Yes Yes Yes Yes
Taiwan High No No Yes Yes Yes No Yes No
United Kingdom
High Yes No Yes Yes Yes No Yes No
Only Europe, Nigeria, and Sudan addressed epidemiological surveillance and research agenda (one of the pillars of the quadrangle).
Table 5. Suggested Suitable Solutions to Enhance the Quality and Impact of Hypertension Guidelines in LMIC
Collaboration among professional organizations to develop hypertension guidelines.
Involvement of patients, key opinion leaders, and policy makers in the development of hypertension guidelines.
The social, psychological, and economic situations of the region or country should be put into consideration while developing the guidelines.
Robust engagement of all stakeholders (stakeholders include physicians, nonphysician healthcare providers, primary caregivers, policy makers, payers, patients, populace, and implementation partners) during development, implementation, and evaluation.
Development of concise key active recommendations specially packaged and disseminated to all stakeholders (stakeholders include physicians, nonphysician healthcare providers, primary caregivers, policy makers, payers, patients, populace, and implementation partners).
Performance of high-quality studies in a context-specific manner in LMIC.
LMIC indicates low- and middle-income countries.
by guest on May 18, 2018
http://hyper.ahajournals.org/D
ownloaded from

Owolabi et al Systematic Review of Hypertension Guidelines 9
6. Seedat YK. Hypertension in developing nations in sub-Saharan Africa. J Hum Hypertens. 2000;14:739–747.
7. Opie LH, Seedat YK. Hypertension in sub-Saharan African populations. Circulation. 2005;112:3562–3568. doi: 10.1161/CIRCULATIONAHA.105.539569.
8. Liu LS; Writing Group of 2010 Chinese Guidelines for the Management of Hypertension. 2010 Chinese guidelines for the management of hyper-tension. Zhonghua Xin Xue Guan Bing Za Zhi. 2011;39:579–615.
9. Nwankwo T, Yoon S, Burt V, Gu Q. Hypertension among adults in the US: National Health and Nutrition Examination Survey, 2011–2012. NCHS data brief, no. 133. National Center for Health Statistics, Centers for Disease Control and Prevention, Hyattsville, MD, US Dept of Health and Human Services Ref Type: Report. 2013.
10. Odili V, Oghagbon E, Ugwa N, Ochei U, Aghomo O. Adherence to inter-national guidelines in the management of hypertension in a tertiary hospi-tal in Nigeria. Trop J Pharm Res. 2008;7:945–952.
11. Williams B. Recent hypertension trials: implications and controversies. J Am Coll Cardiol. 2005;45:813–827. doi: 10.1016/j.jacc.2004.10.069.
12. Saunders E. Hypertension in African-Americans. Circulation. 1991;83:1465–1467.
13. Baker EH, Ireson NJ, Carney C, Markandu ND, MacGregor GA. Transepithelial sodium absorption is increased in people of African origin. Hypertension. 2001;38:76–80.
14. Moher D, Liberati A, Tetzlaff J, Altman DG; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Ann Intern Med. 2009;151:264–9, W64.
15. Graham R, Mancher M, Wolman DM, Greenfield S, Steinberg E. Committee on Standards for Developing Trustworthy Clinical Practice Guidelines; Board on Health Care Services Clinical Practice Guidelines We can Trust. Washington, DC, National Academies Press; 2011.
16. Kung J, Miller RR, Mackowiak PA. Failure of clinical practice guidelines to meet institute of medicine standards: Two more decades of little, if any, progress. Arch Intern Med. 2012;172:1628–1633. doi: 10.1001/2013.jamainternmed.56.
17. Owolabi MO, Akarolo-Anthony S, Akinyemi R, et al; Members of the H3Africa Consortium. The burden of stroke in Africa: a glance at the present and a glimpse into the future. Cardiovasc J Afr. 2015;26(2 suppl 1):S27–S38. doi: 10.5830/CVJA-2015-038.
18. Z Score Calculator for 2 Population Proportions. http://www.socscista-tistics.com/tests/ztest/Default2.aspx Z Score Calculator for 2 Poulation Proportions. Accessed June 24, 2016.
19. Rau NR, Nayak SK. Practical guidelines for hypertension management. http://www.apiindia.org/medicine_update_2013/chap17.pdf. Accessed May 15, 2016.
20. Wijesisiwardene B, Mohideen R. Clinical practice guidelines. http://www.slcog.lk/img/guidelines/Other%20national%20Gidelines/Physicians/Book%201/Management%20of%20Hypertension.pdf. Accessed May 15, 2016.
21. Tadesse Y. Ethiopia standard treatment guidelines. http://siapsprogram.org/publication/ethiopia-standard-treatment-guidelines/”. Accessed June 2, 2016.
22. Sulima AA, Aboud MH. Sudan hypertension guidelines. http://ssh-sd.org/fileload/sudan%20hypertension%20guidelines.pdf. Accessed June 2, 2016.
23. Guide to Management of Hypertension 2008. www.heartfoundation.org.au/Professional_Information/Clinical_Practice/Hypertension. Accessed June 6, 2016.
24. Crouch M. 2009 Kenya guideline for hypertension management. http://apps.who.int/medicinedocs/documents/s21000en/s21000en.pdf. Accessed July 5, 2016.
25. Onwubere B, Kadiri S. Guidelines for the management of hypertension in Nigeria. In: Nigerian Hypertension Society Enugu. Ezu Books Limited. 2005:1–4.
26. Seedat YK, Rayner BL; Southern African Hypertension Society. South African hypertension guideline 2011. S Afr Med J. 2012;102(1 pt 2):57–83.
27. Sociedade BdH, Cardiologia SBd, Nefrologia SBd. VI Brazilian guide-lines on hypertension. Arq Bras Cardiol. 2010;95:1.
28. Rosas M, Pastelin G, Vargas-Alarcon G et al. . Arch Inst Cardiol Mex. 2007;78:S2-5–57.
29. Shimamoto K, Ando K, Fujita T, et al; Japanese Society of Hypertension Committee for Guidelines for the Management of Hypertension. The Japanese Society of Hypertension Guidelines for the Management of Hypertension (JSH 2014). Hypertens Res. 2014;37:253–390. doi: 10.1038/hr.2014.20.
30. Aronow WS. Hypertension guidelines. Hypertension. 2011;58:347–348. doi: 10.1161/HYPERTENSIONAHA.111.177147.
31. Mancia G, Fagard R, Narkiewicz K, et al. 2013 ESH/ESC guide-lines for the management of arterial hypertension: the Task Force for the Management of Arterial Hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC). Blood Pressure. 2013;22:193–278.
32. James PA, Oparil S, Carter BL, et al. 2014 evidence-based guideline for the management of high blood pressure in adults: report from the panel members appointed to the Eighth Joint National Committee (JNC 8). JAMA. 2014;311:507–520. doi: 10.1001/jama.2013.284427.
33. Blacher J, Halimi JM, Hanon O, Mourad JJ, Pathak A, Schnebert B, Girerd X; French Society of Hypertension. Management of hypertension in adults: the 2013 French Society of Hypertension guidelines. Fundam Clin Pharmacol. 2014;28:1–9. doi: 10.1111/fcp.12044.
34. Chiang CE, Wang TD, Li YH, Lin TH, Chien KL, Yeh HI, Shyu KG, Tsai WC, Chao TH, Hwang JJ, Chiang FT, Chen JH; Hypertension Committee of the Taiwan Society of Cardiology. 2010 guidelines of the Taiwan Society of Cardiology for the management of hyper-tension. J Formos Med Assoc. 2010;109:740–773. doi: 10.1016/S0929-6646(10)60120-9.
35. Wood S. ASH/ISH issue separate hypertension guidelines from JNC 8, hinting at discord. Medscape. 2013;19.
36. Aronow WS, Fleg JL, Pepine CJ, et al. ACCF/AHA 2011 expert consen-sus document on hypertension in the elderly: a report of the American College of Cardiology Foundation Task Force on Clinical Expert Consensus documents developed in collaboration with the American Academy of Neurology, American Geriatrics Society, American Society for Preventive Cardiology, American Society of Hypertension, American Society of Nephrology, Association of Black Cardiologists, and European Society of Hypertension. J Am Coll Cardiol. 2011;57:2037–2114. doi: 10.1016/j.jacc.2011.01.008.
37. Dasgupta K, Quinn RR, Zarnke KB, et al; Canadian Hypertension Education Program. The 2014 Canadian Hypertension Education Program recommendations for blood pressure measurement, diagnosis, assess-ment of risk, prevention, and treatment of hypertension. Can J Cardiol. 2014;30:485–501. doi: 10.1016/j.cjca.2014.02.002.
38. Go AS, Bauman MA, Coleman King SM, Fonarow GC, Lawrence W, Williams KA, Sanchez E; American Heart Association; American College of Cardiology; Centers for Disease Control and Prevention. An effective approach to high blood pressure control: a science advisory from the American Heart Association, the American College of Cardiology, and the Centers for Disease Control and Prevention. Hypertension. 2014;63:878–885. doi: 10.1161/HYP.0000000000000003.
39. Calhoun DA, Jones D, Textor S, Goff DC, Murphy TP, Toto RD, White A, Cushman WC, White W, Sica D, Ferdinand K, Giles TD, Falkner B, Carey RM. Resistant hypertension: diagnosis, evaluation, and treat-ment. A scientific statement from the American Heart Association Professional Education Committee of the Council for High Blood Pressure Research. Hypertension. 2008;51:1403–1419. doi: 10.1161/HYPERTENSIONAHA.108.189141.
40. Ritchie LD, Campbell NC, Murchie P. New NICE guidelines for hyper-tension. BMJ. 2011;343:d5644.
41. Argentina: Guias de la Sociedad Argentina de Hipertension para el Diagnostico, Estudio, Tratamiento y Seguimiento de la Hipertension Arterial. http://www.saha.org.ar/1/pdf/GUIA_SAHA_VERSION_COMPLETA.pdf. Accessed August 19, 2016.
42. Guyatt GH, Oxman AD, Kunz R, Vist GE, Falck-Ytter Y, Schünemann HJ; GRADE Working Group. What is “quality of evidence” and why is it important to clinicians? BMJ. 2008;336:995–998. doi: 10.1136/bmj.39490.551019.BE.
43. Ayanian JZ, Landon BE, Newhouse JP, Zaslavsky AM. Racial and ethnic disparities among enrollees in Medicare Advantage plans. N Engl J Med. 2014;371:2288–2297. doi: 10.1056/NEJMsa1407273.
44. Whelton PK, Beevers DG, Sonkodi S. Strategies for improvement of awareness, treatment and control of hypertension: results of a panel discussion. J Hum Hypertens. 2004;18:563–565. doi: 10.1038/sj.jhh.1001738.
45. Muntner P, Gu D, Wu X, Duan X, Wenqi G, Whelton PK, He J. Factors associated with hypertension awareness, treatment, and control in a repre-sentative sample of the Chinese population. Hypertension. 2004;43:578–585. doi: 10.1161/01.HYP.0000116302.08484.14.
46. World Health Organization, Group ISoHW. 2003 World Health Organization (WHO)/International Society of Hypertension (ISH) state-ment on management of hypertension. J Hyp. 2003;21:1983–1992.
by guest on May 18, 2018
http://hyper.ahajournals.org/D
ownloaded from

10 Hypertension November 2016
47. Whitworth JA, Chalmers J. World Health Organisation-International Society of Hypertension (WHO/ISH) hypertension guidelines. Clin Exp Hypertens. 2004;26:747–752.
48. Brasília: Ministério da Saúde. Estratégias para o cuidado da pessoa com doença crônica: hipertensão arterial sistêmica. (Cadernos de Atenção Básica, n. 37; 2013.) http://dab.saude.gov.br/portaldab/biblioteca.php?conteudo=publicacoes/cab37. Accessed August 19, 2016.
49. Chile: Ministerio de Salud. Guía Clínica 2010 Hipertensión Arterial Primaria o esencial en personas de 15 años y más. Santiago: Minsal, 2010. http://www.minsal.gob.cl/portal/url/item/7220fdc4341c44a9e04001011f0113b9.pdf. Accessed August 19, 2016.
50. Colombia: Sistema General de Seguridad Social en Salud. Guía de prác-tica clínica: Hipertensión Arterial Primaria (HTA). 2013 - Guía No. 18. https://www.minsalud.gov.co/sites/rid/Lists/BibliotecaDigital/RIDE/INEC/IETS/GPC_Ptes_HTA.pdf. Accessed August 19, 2016.
51. Costa Rica: Caja Costarricense de Seguro Social. Guias para la Detección, Diagnóstico y Tratamiento de la Hipertensión Arterial. III Edición. San José, Costa Rica, 2009 http://www.binasss.sa.cr/libros/hipertension09.pdf. Accessed August 19, 2016.
52. México: Instituto Mexicano del Seguro Social; 08/07/2014. Diagnóstico y Tratamiento de la Hipertensión Arterial en el Primer Nivel de Atención. http://www.cenetec.salud.gob.mx/descargas/gpc/CatalogoMaestro/076-GCP__HipertArterial1NA/HIPERTENSION_EVR_CENETEC.pdf. Accessed August 19, 2016.
53. Peru: Ministerio de Salud. Guía Técnica: Guía de Práctica Clínica para la Diagnóstico, Tratamiento y Control de la Enfermedad Hipertensiva; January 19, 2015. http://www.minsa.gob.pe/dgsp/documentos/Guias/RM031-2015-MINSA.pdf. Accessed August 19, 2016.
54. Panamá: Organización Panamericana de la Salud. Guía para la atención integral de las personas con Hipertensión arterial. Impresora Pacifico, 2009.
http://www.paho.org/pan/index.php?option=com_docman&task=doc_view&gid=298 &Itemid=224. Accessed August 19, 2016.
55. Argentina: La Revista Argentina de Cardiología. Consenso de Hipertensión Arterial. Vol 81 Suplemento 2, Agosto 2013. http://www.sac.org.ar/wp-content/uploads/2014/04/Consenso-de-Hipertension-Arterial.pdf. Accessed August 19, 2016.
56. Morrison A, Moulton K, Clark M, Polisena J, Fiander M, Mierzwinski-Urban M, Mensinkai S, Clifford T, Hutton B. English-Language Restriction When Conducting Systematic Review-Based Meta-Analyses: Systematic Review Of Published Studies. Ottawa: Canadian Agency for Drugs and Technologies in Health; 2009.
57. Brouwers MC, Kho ME, Browman GP, Burgers JS, Cluzeau F, Feder G, Fervers B, Graham ID, Grimshaw J, Hanna SE, Littlejohns P, Makarski J, Zitzelsberger L; AGREE Next Steps Consortium. The Global Rating Scale complements the AGREE II in advancing the quality of prac-tice guidelines. J Clin Epidemiol. 2012;65:526–534. doi: 10.1016/j.jclinepi.2011.10.008.
58. Adler AJ, Prabhakaran D, Bovet P, Kazi DS, Mancia G, Mungal-Singh V, Poulter N. Reducing Cardiovascular Mortality Through Prevention and Management of Raised Blood Pressure: A World Heart Federation Roadmap. Glob Heart. 2015;10:111–122. doi: 10.1016/j.gheart.2015.04.006.
59. McAlister FA, Feldman RD, Wyard K, Brant R, Campbell NR; CHEP Outcomes Research Task Force. The impact of the Canadian Hypertension Education Programme in its first decade. Eur Heart J. 2009;30:1434–1439. doi: 10.1093/eurheartj/ehp192.
60. Field MJ, Lohr KN. Attributes of Good Practice Guidelines. Washington, DC, National Academies Press; 1990.
61. Owolabi M, Miranda JJ, Yaria J, Ovbiagele B. Controlling cardiovascular diseases in low-and middle-income countries by placing proof in pragma-tism. BMJ Global Health. doi: 10.1136/bmjgh-2016-000105. In press.
by guest on May 18, 2018
http://hyper.ahajournals.org/D
ownloaded from

Melikam, Ezinne Uvere, Babatunde Salako, Bruce Ovbiagele and for the COUNCIL InitiativePietro Amedeo Modesti, Shane Norris, Luqman Ogunjimi, Temitope Farombi, Ezinne Sylvia
Agyemang,Rohina Joshi, Gerald S. Bloomfield, Mulugeta Gebregziabher, Gary Parker, Charles Olmen, Prashant Mathur, Clara Chow, Andre Kengne, Raelle Saulson, Amanda G. Thrift,
Yaria, Tomiwa Makanjuola, Sanni Yaya, Janusz Kaczorowski, Lehana Thabane, Josefien Van Mayowa Owolabi, Paul Olowoyo, J. Jaime Miranda, Rufus Akinyemi, Wuwei Feng, Joseph
Countries: A Systematic ReviewGaps in Hypertension Guidelines in Low- and Middle-Income Versus High-Income
Print ISSN: 0194-911X. Online ISSN: 1524-4563 Copyright © 2016 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Hypertension published online October 3, 2016;Hypertension.
http://hyper.ahajournals.org/content/early/2016/10/03/HYPERTENSIONAHA.116.08290.citationWorld Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://hyper.ahajournals.org/content/suppl/2017/07/10/HYPERTENSIONAHA.116.08290.DC2 http://hyper.ahajournals.org/content/suppl/2016/10/03/HYPERTENSIONAHA.116.08290.DC1
Data Supplement (unedited) at:
http://hyper.ahajournals.org//subscriptions/
is online at: Hypertension Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer this process is available in the
click Request Permissions in the middle column of the Web page under Services. Further information aboutOffice. Once the online version of the published article for which permission is being requested is located,
can be obtained via RightsLink, a service of the Copyright Clearance Center, not the EditorialHypertensionin Requests for permissions to reproduce figures, tables, or portions of articles originally publishedPermissions:
by guest on May 18, 2018
http://hyper.ahajournals.org/D
ownloaded from

Gaps in Hypertension Guidelines in Low- and Middle Income Versus High Income Countries: a Systematic Review
SUPPLEMENTARY TABLES AND FIGURES
Running title: Systematic Review of Hypertension Guidelines
Mayowa Owolabi1,2*, Paul Olowoyo3, J. Jaime Miranda4,5, Rufus Akinyemi6, Wuwei Feng7, Joseph Yaria1, Tomiwa Makanjuola1, Sanni Yaya8, Janusz Kaczorowski9, Lehana Thabane10, Josefien Van Olmen11, Prashant Mathur12, Clara Chow13, Andre Kengne14, Raelle Saulson7, Amanda G Thrift15, Rohina Joshi16, Gerald S. Bloomfield17, Mulugeta Gebregziabher18, Gary Parker19, Charles Agyemang20, Pietro Amedeo Modesti21, Shane Norris22, Luqman Ogunjimi1, Temitope Farombi1, Ezinne Sylvia Melikam1, Ezinne Uvere2, Babatunde Salako1, Bruce Ovbiagele7 for the COUNCIL** Initiative


Table S 1: Stakeholder Populations (6Ps) Targeted by the Guidelines
*This implies packaging of key recommendations into very brief messages for targeted audiences, disseminated through user-friendly interactive channels including social media.
Countries Income level
Physicians
Non-physician health care providers
Primary Caregivers
Policy Makers
Payers
Patients Populace Implementation Partners
Dissemination channels
America High Yes Yes No No No No Yes No Yes Australia High Yes No No No No No No Yes Yes Brazil Middle Yes No No No No Yes Yes Yes No Canada High Yes Yes Yes No No Yes Yes Yes Yes China Middle Yes No No No No No Yes No No Ethiopia Low Yes Yes Yes No No No Yes No No Europe High Yes Yes No No No No No Yes Yes France High Yes Yes Yes No No No Yes No No India Middle Yes No No No No No No No No Japan High Yes No No No No No Yes No No Kenya Middle Yes Yes Yes No No No No No No Mexico Middle Yes No No No No No Yes No No Nigeria Middle Yes Yes Yes No No No Yes Yes Yes South Africa
Middle Yes Yes Yes Yes No Yes Yes Yes Yes
Sri-Lanka Middle Yes Yes Yes No No No No No No Sudan Middle Yes Yes Yes Yes Yes Yes Yes Yes Yes Taiwan High Yes No No No No No No No No United Kingdom
High Yes Yes Yes No No Yes Yes No No

Table S 2 : Translatability* and Ethical, Legal, and Socio-economic (ELSE) Considerations applied by the Guidelines
Countries Income level
Translat-ability* rating 61
Ethical
Legal
Social
Psychological
Economic
Co-morbidity
Quality Indicator
Surveillance
Next Renewal Date
America High No No No No No No Yes No No 2016 Australia High No No No No No No Yes No No No Brazil Middle No No No Yes Yes Yes Yes No No No Canada High No No No No No No Yes No No No China Middle No No No No No No Yes No No No Ethiopia Low No No No No No No No No No No Europe High No No No No No No Yes No Yes 2016 France High No No No No No No Yes No No No India Middle No No No No No No Yes No No No Japan High No No No No No No Yes No No 2017 Kenya Middle No No No No No No No No No No Mexico Middle No No No No No No Yes No No No Nigeria Middle No No No Yes No Yes Yes No Yes No South Africa Middle No No No No No Yes Yes No No No Sri-Lanka Middle No No No No No No Yes No No No Sudan Middle Yes Yes No Yes Yes Yes Yes No Yes No Taiwan High No No No No No No Yes No No No United Kingdom
High No No No No No Yes Yes No No No
*Translatability Scale in descending order of suitability

Ta. Interventions that are relatively low-tech, easy to implement, limited neither by personnel nor cost (e.g. increased physical activity, dietary salt reduction, healthy dietary choices, attaining and maintaining ideal body weight and proportions) Tb. Interventions limited mainly by cost/availability only (e.g. medications that can be easily administered once correctly prescribed e.g. oral antiplatelet) Tc. Interventions limited mainly by absence of expert personnel only (eg speech therapy: when the potential beneficiaries are able to afford but not access the service) Td. Interventions limited by both personnel and cost (e.g. thrombolytic therapy)
Table S 3: Quality of the guidelines in LMICs vs HICs
Income level z p-value Criteria for quality LMIC (%)
n=10 HIC (%) n=8
Socioeconomic contextualization
4(40.0%) 1(12.5%) 1.294 0.197
Application of systematic review
1(10.0%) 5(63.5%) -2.133 0.033
Frequency of issue
3(30.0%) 6(75.0%) -1.348 0.177
Application of IOM standards
3(30.0%) 5(62.5%) -1.378 0.167
Use of dissemination channels 3(30.0%) 4(50.0%) -0.864 0.389Involvement of stakeholders 8(80.0%) 6(75.0%) 0.253 0.802

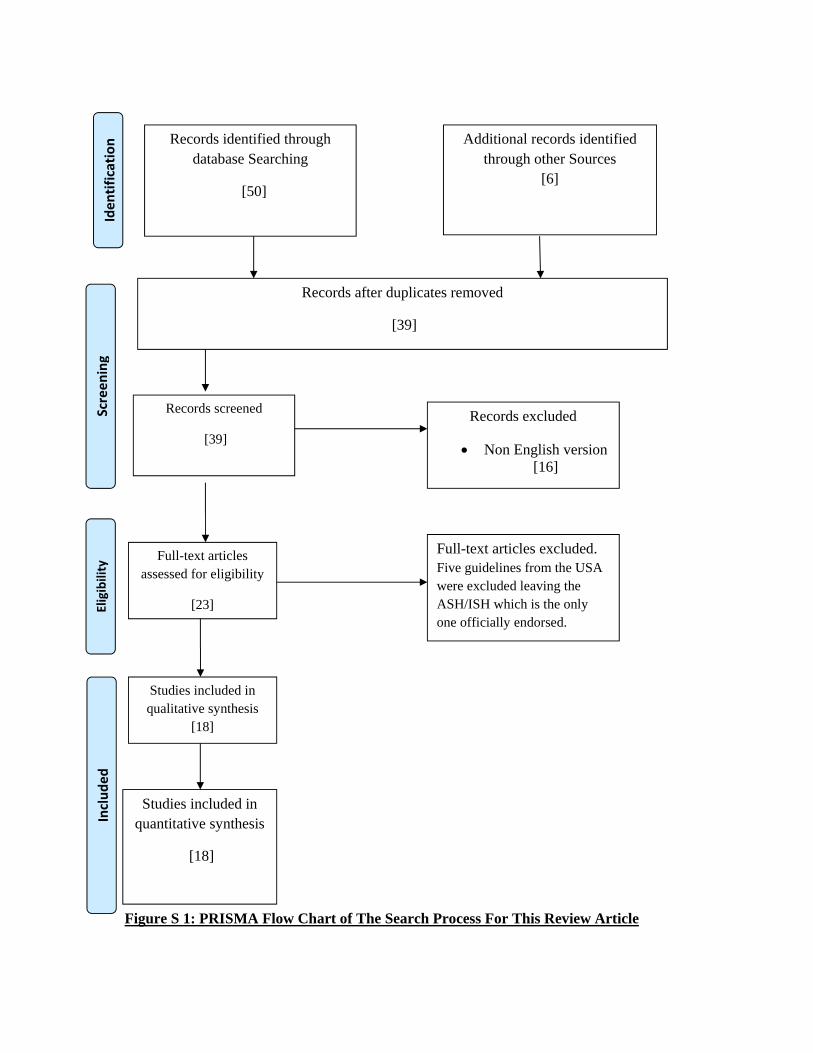
Figure S 1: PRISMA Flow Chart of The Search Process For This Review Article
Records after duplicates removed
[39]
Records excluded
Non English version [16]
Records screened
[39]
Studies included in qualitative synthesis
[18]
Full-text articles assessed for eligibility
[23]
Full-text articles excluded. Five guidelines from the USA were excluded leaving the ASH/ISH which is the only one officially endorsed.
Records identified through database Searching
[50]
Additional records identified through other Sources
[6]
Studies included in quantitative synthesis
[18]
Identification
Screening
Eligibility
Included

Figure availabl
S 2: Regiole and acces
ons/countriessible.
es of the woorld where HHypertensioon Managemment Guidel
lines are

39
Revisión breveHiatos en los lineamientos para hipertensión en países de bajos y medianos ingresos frente a países de altos ingresos
Revisión sistemática
Mayowa Owolabi,* Paul Olowoyo,* Jaime Miranda, Rufus Akinyemi, Wuwei Feng, Joseph Yaria, Tomiwa Makanjuola, Sanni Yaya, Janusz Kaczorowski, Lehan Thabane, Josefien Van Olmen, Prashant Mathur, Clara Chow, Andre Kengne, Raelle Saulson, Amanda G.
Thrift, Rohina Joshi, Gerald S. Bloomfield, Mulugeta Gebregziabher, Gary Parker, Charles Agyemang, Pietro Amadeo Modesti, Shane Norris, Luqman Ogunjimi, Temitope Farombi,
Ezinne Sylvia Melikam, Ezinne Uvere, Babatunde Salako, Bruce Ovbiagele; por la Iniciativa COUNCIL†
La hipertensión, una causa importante de otras enfermeda-des cardiovasculares, también es una de las principales
causas de discapacidad y muerte en todo el mundo.1 Se diag-nostica hipertensión a más de 1000 millones de personas, de manera que 1 de cada 3 individuos tiene presión arterial alta en numerosos países.3 Alrededor del 90% de la carga de en-fermedad cardiovascular corresponde a los países de bajos y medianos ingresos (PBMI), que tienen solo ≈10% de la capa-cidad de investigación y los recursos de atención médica para enfrentar el flagelo.3
La hipertensión se había considerado una enfermedad de las personas opulentas del mundo.4,5 Sin embargo, ha aparecido en los PBMI, donde afectó a ≈1 de cada 5 adultos en 2013.5 Se ha proyectado que esta tasa aumentará de modo tal que, en 2025, 3 de cada 4 adultos vivirá con hipertensión en los PBMI.6,7 La concientización y los niveles de control de la hipertensión aún son bajos en los PBMI en comparación con los PAI.8 Por ejem-plo, el control de la hipertensión en los Estados Unidos es del
52% respecto del 5-10% en África.9 La principal razón de esta disparidad podría ser la falta de conocimiento sobre acceso a los lineamientos de hipertensión pasibles de implementación en los PBMI y cumplimiento de ellos .10
Más aún, el tratamiento de la hipertensión se complica por la elección, disponibilidad y accesibilidad de medicaciones apropiadas. Los aspectos culturales del uso de por vida de me-dicaciones contra la hipertensión, las necesidades variables de cada paciente, y los diseños y resultados no uniformes de los estudios clínicos también han complicado el tratamiento.11 Las diferentes arquitecturas genéticas de los individuos con hiper-tensión12,33 pueden determinar la elección del tratamiento y la respuesta a este. Algunos de estos agentes antihipertensivos son costosos, y su accesibilidad y distribución no es igualitaria en los PBMI.
Por lo tanto, los lineamientos que dan resultado en con-textos de PAI pueden no ser aceptables, eficaces, pasibles de implementación ni aplicables en los PBMI, debido a la ausen-
Departamento de Medicina y University College Hospital (M.O., J.Y., L.O., T.F., E.S.SM., B.S.) e Institute for Advanced Medical Research and Training, College of Medicine (R.A.), University of Ibadan, Nigeria; WFNR-Blossom Specialist Medical Center, Ibadam, Nigeria (M.O., E.U.); Federal Teaching Hospital, Ido-Ekiti, Nigeria (P.O.), Departamento de Medicina, CRONICAS Centro de Excelencia en Enfermedades Crónicas, Universidad Peruana Cayetano Heredia, Lima, Perú (J.J.M.); Departamento de Neurología (W.F., R.S., B.O.) y Departamento de Ciencias de Salud Pública (M.G.), Medical University of South Carolina, Charleston; School of International Development and Global Studies, University of Ottawa, Ontario, Canadá (S.Y.); Departamento de Medicina familiar y de urgencia, University of Montreal, Quebec, Canadá (J.K.); Departamento de Salud Pública, Health Service Organization, Hamilton, Ontario, Canadá (L.T.); Departamentos de Anestesia/Pediatría, McMaster University, Hamilton, Ontario, Canadá (J.V.O.); Departamento de investigación en salud, Ministerio de Salud y Bienestar familiar, Gobierno de India, Nueva Delhi, India (P.M.); Sydney Medical School, University of Sydney, New South Wales, Australia (C.C., R.J.); Unidad de investigación de enfermedades no transmisibles, South African Medical Research Council, Tygerberg, Sudáfrica (A.K.); School of Clinical Sciences at Monash Health, Monash University, Clayton, Victoria, Australia (A.G.T.), Salud cardiovascular global, División de Cardiología, Duke University Medical Center, Durham, NC (G.S.B.); Global Alliance for Chronic Diseases, UCL Institute for Global Health, Londres, Reino Unido (G.P.); Departamento de Salud Pública, Academic Medical Center, Universidad de Amsterdam, Holanda (C.A.); Departamento de Medicina clínica y experimental, Universidad de Florencia, Italia (P.A.M.); y Unidad de vías de desarrollo para la investigación en salud, University of the Witwatersrand, Johanesburgo, Sudáfrica (S.N.).
*Estos autores contribuyeron por igual a este trabajo.†Control único para enfermedades cardiovasculares en países de bajos y medianos ingresos.Se puede consultar el Suplemento de datos en línea de este artículo en http;//hyper.journals.org/lookup/suppl/doi:10.1161/HYPER-
TENSIONAHA.116.08290/-/DCI.Correspondencia: Mayowa Owolabi, Department of Medicine, University College Hospital and University of Ibadan, Ibadan, Nigeria. Di-
rección de correo electrónico: [email protected](Hypertension. 2016:68:1328-1337. DOI: 10.116/HYPERTENSIONAHA.116.08290).© 2016 American Heart Association, Inc.
Se puede consultar Hypertension en http://hyper.ahajournals.org DOI: 10.1161/HYPERTENSIONAHA.116.07703

40 Hypertension Diciembre 2016
cia de recursos de respaldo. Además de los lineamientos inter-nacionales generales adaptados a las necesidades de grandes regiones con contextos socioeconómicos de implementación similares, puede ser crucial para cada país adaptar aún más los aspectos de implementación y los canales de difusión de reco-mendaciones clave comprometiendo y empoderando a todas las partes interesadas, con el consiguiente aumento del cum-plimiento y la repercusión.
Esta revisión se impone por la necesidad de llevar el control de la hipertensión al umbral del individuo mediante el desa-rrollo y el despliegue de estos lineamientos para hipertensión pragmáticos en estos países a fin de reducir de manera signi-ficativa la carga de morbimortalidad cardiovascular asociada.
Llevamos a cabo una revisión sistemática para comparar la cantidad y la calidad de los lineamientos de práctica clíni-ca publicados para hipertensión en PBMI y PAI individuales durante la década pasada en términos de número, calidad de la evidencia, contextualización socioeconómica y ética-legal, posibilidad de ser implementados y difundidos para compro-meter y empoderar en forma activa a todas las partes interesa-das pertinentes. En términos generales, nuestro objetivo fue detectar hiatos y proponer soluciones adecuadas para aumentar la calidad y la repercusión de los lineamientos para hiperten-sión en los PBMI.
MetodologíaUtilizando los lineamientos sobre Ítems de informe preferidos para revisión sistemática y metaanálisis,14 se realizó una revi-sión sistemática cuyos ítems de búsqueda fueron hipertensión, presión arterial alta y lineamientos. Los ítems de búsqueda se-cundarios fueron práctica clínica, implementación, traducción y prevención, mientras que los ítems de búsqueda terciarios fueron Organización Mundial de la Salud, Estados Unidos, Americano, Internacional, Europeo, Africano, Asiático, Japo-nés, Sud- y Latinoamericano, Sociedad, Asociación, Liga y Grupo.
Criterios de inclusión y exclusiónLa revisión incluyó lineamientos publicados desde el 1.° de enero de 2005 al 31 de diciembre de 2015 en PubMed, Google Scholar, African Journals Online, Excerpta Medica Database y bases de datos del Directory of Open Access Journals. Se excluyeron los lineamientos en otros idiomas que no pudieron ser traducidos al inglés.
Asimismo, se buscaron lineamientos elegibles país por país y región por región. Por ejemplo, se buscaron lineamientos de hipertensión en línea de los siguientes países clasificados como de bajos ingresos: Camboya, Chad, Sudán del Sur, Tanzania, Zimbabwe, Comoros, Haití, Benim, Nepal, Mali, Sierra Leo-na, Burkina Faso, Afganistán, Uganda, Ruanda, Mozambique, Togo, Guinea-Bissau, Corea del Norte, Etiopía, Eritrea, Gui-nea, Gambia, Madagascar, Níger, República democrática del Congo, Liberia, República Centroafricana, Burundi, Malawi y Somalia. También se incluyeron algunos lineamientos no pu-blicados obtenidos por contacto directo con médicos de algu-nos países. Se excluyeron los repetidos.
Los lineamientos se caracterizaron según nivel de ingresos,
clase de evidencia, nivel de recomendación y número de revi-siones realizadas durante el período del estudio.
Extracción de datosSe utilizó el traductor de Google para traducir los lineamientos de hipertensión brasileños del portugués al inglés.
Para determinar la calidad y los procesos de elaboración de los lineamientos, 2 revisores independientes extrajeron in-formación de cada lineamiento en términos de cumplimiento con los estándares del Institute of Medicine (IOM)15,16 para ela-boración de lineamientos de práctica clínica, que comprenden transparencia, conflictos de interés, enfoque multidisciplina-rio, revisiones sistemáticas, firmeza de las recomendaciones, revisión externa y actualizaciones regulares. Otros índices de calidad son la cobertura del cuadrángulo cardiovascular17 (vigilancia e investigación, prevención, atención aguda y re-habilitación); contextualización y posibilidad de traducción; atención a aspectos socioeconómicos, éticos, legales y psico-lógicos, y despliegue a través de múltiples canales de difusión entre todas las partes interesadas. Las partes interesadas eran médicos, prestadores de salud no médicos, cuidadores prima-rios, encargados de formular políticas, pagadores, pacientes, población y socios de implementación. Se compararon las proporciones de los índices de calidad cumplidos en los linea-mientos de los PMBI con las de los PAI.18
ResultadosEn las Figuras S1 y S2 del Suplemento de datos solo en lí-nea se presentan 50 lineamientos para hipertensión, incluidos 20 de PubMed y 30 de bases de datos de Google Scholar. Se obtuvieron otros seis lineamientos no publicados después de la consulta con colegas involucrados en el control y el tra-tamiento de la hipertensión en todo el mundo a través de la Global Alliance for Chronic Diseases (Alianza global para en-fermedades crónicas).19-24 No se halló ningún lineamiento en African Journals Online, Excerpta Medica Database ni en las bases de datos del Directory of Open Access Journals. Tras la eliminación de los repetidos, quedaron 39 lineamientos de 28 países. De estos, se excluyeron 16 porque no estaban escritos en inglés y no pudieron ser traducidos. Se halló solo 1 de los 31 países de la categoría bajos ingresos, mientras que se ha-llaron 9 lineamientos de los países de medianos ingresos. Los 13 restantes fueron de PAI. Se excluyeron cinco lineamientos de los Estados Unidos y se dejó el de la American Society of Hypertension/International Society of Hypertension, que es el único con respaldo oficial. Se incluyeron 18 lineamientos para síntesis cualitativas y cuantitativas.
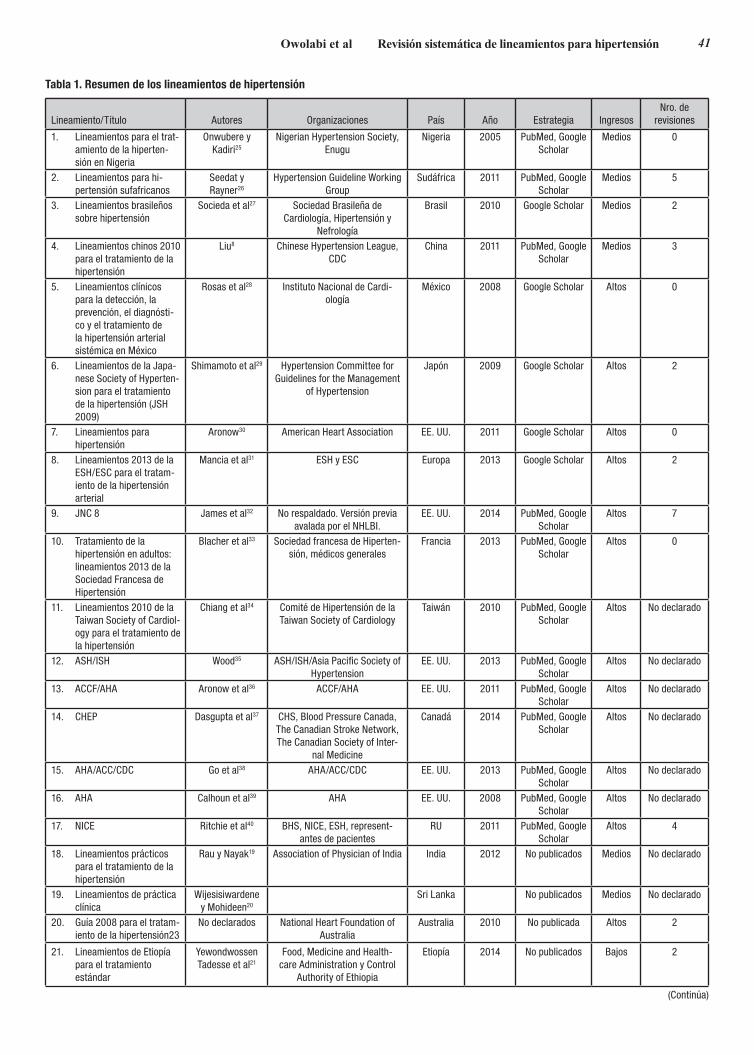
Los lineamientos se caracterizaron según las organizacio-nes que los elaboraron, el año de publicación, el número de re-visiones, el nivel de evidencia, el espectro clínico considerado y el cumplimiento de las recomendaciones del IOM (Tablas 1 a 3). La evaluación también se basó en el país de origen (Tabla 4; Tablas S1 a S3). Muchos lineamientos de los PAI no fueron denominados por países individuales, a diferencia de los de los PBMI que eran específicos de países individuales. Más bien, los lineamientos de los PAI fueron adoptados por los países en los que tienen sede las asociaciones que los elaboraron.
41Owolabi et al Revisión sistemática de lineamientos para hipertensión
Lineamiento/Título Autores Organizaciones País Año Estrategia IngresosNro. de
revisiones
1. Lineamientos para el trat-amiento de la hiperten-sión en Nigeria
Onwubere y Kadiri25
Nigerian Hypertension Society, Enugu
Nigeria 2005 PubMed, Google Scholar
Medios 0
2. Lineamientos para hi-pertensión sufafricanos
Seedat y Rayner26
Hypertension Guideline Working Group
Sudáfrica 2011 PubMed, Google Scholar
Medios 5
3. Lineamientos brasileños sobre hipertensión
Socieda et al27 Sociedad Brasileña de Cardiología, Hipertensión y
Nefrología
Brasil 2010 Google Scholar Medios 2
4. Lineamientos chinos 2010 para el tratamiento de la hipertensión
Liu8 Chinese Hypertension League, CDC
China 2011 PubMed, Google Scholar
Medios 3
5. Lineamientos clínicos para la detección, la prevención, el diagnósti-co y el tratamiento de la hipertensión arterial sistémica en México
Rosas et al28 Instituto Nacional de Cardi-ología
México 2008 Google Scholar Altos 0
6. Lineamientos de la Japa-nese Society of Hyperten-sion para el tratamiento de la hipertensión (JSH 2009)
Shimamoto et al29 Hypertension Committee for Guidelines for the Management
of Hypertension
Japón 2009 Google Scholar Altos 2
7. Lineamientos para hipertensión
Aronow30 American Heart Association EE. UU. 2011 Google Scholar Altos 0
8. Lineamientos 2013 de la ESH/ESC para el tratam-iento de la hipertensión arterial
Mancia et al31 ESH y ESC Europa 2013 Google Scholar Altos 2
9. JNC 8 James et al32 No respaldado. Versión previa avalada por el NHLBI.
EE. UU. 2014 PubMed, Google Scholar
Altos 7
10. Tratamiento de la hipertensión en adultos: lineamientos 2013 de la Sociedad Francesa de Hipertensión
Blacher et al33 Sociedad francesa de Hiperten-sión, médicos generales
Francia 2013 PubMed, Google Scholar
Altos 0
11. Lineamientos 2010 de la Taiwan Society of Cardiol-ogy para el tratamiento de la hipertensión
Chiang et al34 Comité de Hipertensión de la Taiwan Society of Cardiology
Taiwán 2010 PubMed, Google Scholar
Altos No declarado
12. ASH/ISH Wood35 ASH/ISH/Asia Pacific Society of Hypertension
EE. UU. 2013 PubMed, Google Scholar
Altos No declarado
13. ACCF/AHA Aronow et al36 ACCF/AHA EE. UU. 2011 PubMed, Google Scholar
Altos No declarado
14. CHEP Dasgupta et al37 CHS, Blood Pressure Canada, The Canadian Stroke Network, The Canadian Society of Inter-
nal Medicine
Canadá 2014 PubMed, Google Scholar
Altos No declarado
15. AHA/ACC/CDC Go et al38 AHA/ACC/CDC EE. UU. 2013 PubMed, Google Scholar
Altos No declarado
16. AHA Calhoun et al39 AHA EE. UU. 2008 PubMed, Google Scholar
Altos No declarado
17. NICE Ritchie et al40 BHS, NICE, ESH, represent-antes de pacientes
RU 2011 PubMed, Google Scholar
Altos 4
18. Lineamientos prácticos para el tratamiento de la hipertensión
Rau y Nayak19 Association of Physician of India India 2012 No publicados Medios No declarado
19. Lineamientos de práctica clínica
Wijesisiwardene y Mohideen20
Sri Lanka No publicados Medios No declarado
20. Guía 2008 para el tratam-iento de la hipertensión23
No declarados National Heart Foundation of Australia
Australia 2010 No publicada Altos 2
21. Lineamientos de Etiopía para el tratamiento estándar
Yewondwossen Tadesse et al21
Food, Medicine and Health-care Administration y Control
Authority of Ethiopia
Etiopía 2014 No publicados Bajos 2
Tabla 1. Resumen de los lineamientos de hipertensión
(Continúa)

42 Hypertension Diciembre 2016
Ninguno de los lineamientos recuperados utilizó el siste-ma Grading of Recommendations Assessment, Development and Evaluation (Clasificación de la valoración, desarrollo y evaluación de las recomendaciones).42 Pocos lineamientos cu-brieron todo el espectro del cuadrángulo cardiovascular (Ta-bla 4); consideraciones éticas, sociales, legales, psicológicas y económicas; o elaboraron planes para desplegar y difundir las recomendaciones entre todas las partes interesadas pertinentes (Tabla 4; Tablas S1 y S2). Ninguno de ellos aplicó a sus reco-mendaciones la ponderación de la traducibilidad (Tabla S2).
Más lineamientos de hipertensión de los PAI siguieron las recomendaciones del IOM. Sin embargo, los Lineamientos de hipertensión sudafricanos26 y los lineamientos chinos de 2010 de PBMI se elaboraron con estricto cumplimiento de las re-comendaciones del IOM (Tabla 3). Los lineamientos chinos de 20108 describieron el tratamiento de la hipertensión en la enfermedad renal crónica, el accidente cerebrovascular y la arteriopatía coronaria. Las recomendaciones se basaron en evidencia de alto nivel (estudios aleatorizados controlados), metaanálisis y estudios locales.8 Los lineamientos de Nigeria y México no se han actualizado porque fueron publicados (Tabla 1).25 En comparación con los lineamientos de los PAI, el espec-tro de problemas clínicos asociados considerados y la elección de agentes antihipertensivos no se analizaron con claridad (Ta-bla 2; Tabla S1).
La cantidad de lineamientos de los PAI que se elaboraron con participación de revisiones sistemáticas de la eviden-cia pertinente fue significativamente mayor (63,5% frente a 10,0%; P = 0,033). En términos generales, las proporciones de lineamientos que aplicaron las recomendaciones del IOM, fue-ron sometidos a revisiones frecuentes y desarrollaron canales de difusión activos para involucrar a todas las partes interesa-das relevantes fueron más altas en los PAI (Tabla S3).
DiscusiónA partir de esta revisión, es evidente que hay escasos linea-mientos para hipertensión en los PBMI, particularmente en países de bajos ingresos donde solo existía uno.21 Los linea-mientos disponibles en los países de medianos ingresos solo se limitan a varios países, 4 de los cuales no fueron publicados en revistas con revisión externa por expertos ni se puede acceder a ellos en ninguna de las bases de datos en línea.19,20,22 Esto no se ajusta a la recomendación de la Asamblea Mundial de la
Salud ni del Comité Regional para África de la Organización Mundial de la Salud de que los países deben ser alentados a establecer recomendaciones específicas del país para la pre-vención y el tratamiento de la hipertensión.5,25
Existe una necesidad urgente de que esto sea así, dado que la genómica,42 el contexto socioeconómico y las políticas sani-tarias de estos países varían entre las distintas regiones, en es-pecial respecto del financiamiento de la atención sanitaria y la implementación de modificaciones del estilo de vida44,45, como abandono del tabaquismo y reducción del consumo de alcohol. Sin embargo, un estilo de vida saludable es un componente esencial de cualquier lineamiento para el tratamiento de la hi-pertensión eficaz, y se lo recomienda para toda la población.46 El proceso de generar recomendaciones ajustadas, específicas de los PBMI puede ser facilitado y agilizado generando prime-ro lineamientos con recomendaciones únicas que pueden ser implementadas ampliamente en el contexto socioeconómico de los PBMI.
En la actualidad, los lineamientos de los PBMI no son priva-tivos del contexto de estos países, dado que fueron adoptados a partir de lineamientos existentes en los PAI sin las debidas consideraciones respecto de la posibilidad de implementación. No se basaron en evidencia obtenida localmente relevante para el contexto. De hecho, como se menciona en los Lineamien-tos para Hipertensión Sudafricanos de 2012,26 los lineamientos de los PAI tienen algunas recomendaciones que quizá no sea posible implementar en los PBMI debido al contexto socioeco-nómico de estos países.11
Además, muchos de los lineamientos de los PBMI no espe-cificaron el nivel de evidencia ni consideraron el tratamiento de la hipertensión en situaciones especiales, como enfermedad renal crónica, enfermedad coronaria, insuficiencia cardíaca, diabetes mellitus y accidente cerebrovascular. Tampoco se consideró la elección de medicaciones ni los niveles diana de PA en caso de hipertensión en situaciones especiales.
Por el contrario, más lineamientos de los PAI fueron some-tidos a revisiones frecuentes, aplicaron las recomendaciones del IOM y desarrollaron canales de difusión activos. De todos modos, también hay cabida para mejorar los lineamientos de los PAI. Por ejemplo, los lineamientos de la American Socie-ty of Hypertension/International Society of Hypertension35 no siguieron todas las recomendaciones del IOM. Incluso, los autores recomiendan que los lectores no consideren los linea-
Lineamiento/Título Autores Organizaciones País Año Estrategia IngresosNro. de
revisiones
22. Lineamientos de Sudán para la hipertensión
Sulima y Aboud22 Sudan Society of Hypertension, FMoH-NCDs Directorate
Sudán 2012 No publicada Medios No declarado
23. Lineamientos 2009 de Kenia para el tratamiento de la hipertensión
Crouch24 Ministerio de Servicios Médicos, Ministerio de Salud Pública y
Saneamiento
Kenia 2009 No publicada Medios No declarado
Tabla 1. Continuación
ACC indica American College of Cardiology; ACCF/AHA, American College of Cardiology Foundation/American Heart Association; ASH/ISA, American Society of Hypertension/International Society of Hypertension; BHS, British Society of Hypertension; CDC, Centers for Disease Control and Prevention; CHEP, Canadian Hyper-tension Education Program; CHS, Canadian Hypertension Society; ESH/ESC, European Society of Hypertension/European Society of Cardiology; FMoH-NCD, JNC 8, Eighth Joint National Committee; y NICE, National Institute for Clinical Excellence.
*Frecuencia de revisión de cada lineamiento desde su publicación inicial.

43Owolabi et al Revisión sistemática de lineamientos para hipertensión
Lineamiento/Título Nivel de evidencia
Parámetros clínicos consid-
eradosHipertensión en situa-
ciones especiales Otras consideraciones
1. Lineamientos para el tratamiento de la hipertensión en Nigeria
No declarado No declarados No analizado Ninguna
2. Lineamientos para hipertensión sudafricanos
Adopción de los lineamientos de la ESH/ESC
Peso, talla, IMC, circunferencia
de cintura
DM, ERC …
3. Lineamientos brasileños sobre hipertensión
No declarado DM, ERC, accidente cerebrovascular
…
4. Lineamientos chinos 2010 para el tratamiento de la hipertensión
EAC, metaanálisis, estudios chinos
Presión arterial, peso, talla
ERC, accidente cerebrovascular, arte-
riopatía coronaria
…
5. Lineamientos clínicos para la detección, la prevención, el diagnóstico y el tratamiento de la hipertensión arterial sistémica en México
Revisión por expertos Presión arterial, peso
Obesidad, DM, dislipi-demia, tabaquismo
Embarazo, adolescentes
6. Lineamientos de la Japanese Society of Hypertension para el tratamiento de la hipertensión (JSH 2009)
Revisión sistemática Presión arterial, peso
Accidente cerebrovas-cular, IM, ERC
No declaradas
7. Lineamientos para la hipertensión Opinión médica de expertos Presión arterial Arteriopatía coronaria, ERC, diabetes mellitus, insuficiencia cardíaca
Es razonable una diana terapéutica de <140/90 mm Hg en pacientes <80 años y presión arterial sistólica de 140-145 mm Hg si es tolrada en pacientes ≥80
años8. Lineamientos 2013 de la ESH/
ESC para el tratamiento de la hipertensión arterial
Clase 1; Nivel de evidencia A Hipertensión sistólica, peso
Pacientes diabéticos, ancianos
Los diuréticos, los β-bloqueantes, los BCC, los IECA y los BRA son opciones viables para el tratamiento inicial de la
hipertensión. En la DM, el objetivo de PA es <140/85 mm Hg.
9. JNC 8 La mayoría basados en opin-iones de expertos. Algunas revisiones sistemásticas,
EAC, clase 1; Nivel de evidencia A
Presión arterial sistólica y di-
astólica
ERC, DM, sujetos de raza no negra, de raza
negra
Los β-bloqueantes ya no se consideran una opción terapéutica inicial
10. Tratamiento de la hipertensión en adultos: lineamientos 2013 de la Sociedad Francesa de Hiperten-sión
Revisión sistemática, análisis de la bibliografía, metaanáli-sis. Conferencias de consen-so, recomendaciones previas
sobre hipertensión
Presión arterial ERC, DM …
11. Lineamientos 2010 de la Taiwan Society of Cardiology para el tratamiento de la hipertensión
EAC, metaanálisis, datos epidemiológicos: estudios de
cohortes taiwaneses
Presión arterial Accidente cerebro-vascular, arteriopatía
coronaria, ERC
No declaradas
12. ASH/ISH No se efectúa ninguna clasifi-cación ni graduación
Presión arterial DM, ERC, arteriopatía coronaria, PA <140/90
Destinado a ser un cebador con infor-mación general
13. ACCF/AHA Opinión de expertos, no EAC Presión arterial … Ninguna recomendación respecto de la selección de agentes antihipertensivos
14. CHEP No se efectúa ninguna clasi-ficación ni graduación, EAC y revisión sistemática de EAC
IMC, circunfer-encia de cintura
Accidente cerebrovas-cular, DM, ERC
…
15. AHA/ACC/CDC Ninguna recomendación formal
Presión arterial Accidente cerebrovas-cular, ERC
No se realiza ninguna recomendación específica respecto del diagnóstico, la evaluación o el tratamiento de la
hipertensión16. AHA Ninguna recomendación
formalPresión arterial Accidente cerebrovas-
cular, ERCDeclaración científica para el diagnósti-
co, la evaluación y el tratamiento de pacientes con hipertensión resistente.
No es un lineamiento formal. Considera incorporar antagonista del receptor de mineralocorticoides (amilorida o
espironolactona). Considera administs-rar por lo menos 1 antihipertensivo al
acostarse.
Tabla 2. Nivel de evidencia y espectro de los lineamientos para hipertensión
(Continúa)

44 Hypertension Diciembre 2016
mientos como un conjunto de recomendaciones basadas en la evidencia. Si bien estos lineamientos encararon el tratamiento de la hipertensión en personas con enfermedades concomi-tantes, la evidencia para sus recomendaciones se basa, en su mayor parte, en la opinión de expertos. En cambio, los linea-mientos de hipertensión del American College of Cardiology Foundation/American Heart Association36 cumplieron con algunas de las recomendaciones del IOM para la elaboración de lineamientos formales. Su foco principal es el tratamiento de la hipertensión en los ancianos, de manera que no son tan completos. Otros lineamientos que analizan el tratamiento en los ancianos son los lineamientos para hipertensión de la Eu-ropean Society of Hypertension/European Society of Cardio-logy,31 National Institute for Clinical Excellence40 y Canadian Hypertension Education Program.37
Los lineamientos de la American Heart Association, los Li-neamientos para Hipertensión sudafricanos y los lineamientos del National Institute for Clinical Excellence son los únicos que recomiendan fármacos específicos para el tratamiento de la hipertensión resistente.40 Pese al hecho de que el Joint Na-tional Committee 8 siguió estrictamente las recomendaciones del IOM, sus recomendaciones no tienen respaldo oficial y no son completas.32 Esto se debe a que su elaboración se basó solo en estudios aleatorizados controlados, a diferencia de los li-neamientos de la Euroepan Society of Hypertension/European Society of Cardiology que incluyeron datos de metaanálisis y estudios observacionales.31 Los lineamientos de la Euroe-pan Society of Hypertension/European Society of Cardiology que son lo bastante completos para considerar la detección,
la evaluación y el tratamiento de la hipertensión pueden ser útiles donde hay limitaciones para la aplicación directa en vir-tud de diferentes sistemas de salud, tratamiento de referencia y disponibilidad de agentes antihipertensivos, sobre todo en los PBMI.31
Para la implementación de estos lineamientos, tanto en PBMI como en PAI, se propugnaron enfoques no farmacoló-gicos y multidisciplinarios para la atención total de los pacien-tes.31 Sin embargo, el enfoque multidisciplinario se limitó a los médicos de sus respectivos campos, con escasa atención a enfermeros, farmacéuticos y dietistas en los lineamientos de los PBMI (Tabla S1). Casi todos los lineamientos de los PAI consideran esto, excepto los Lineamientos 2010 de la Taiwan Society of Cardiology para el tratamiento de la hipertensión (Tabla S1). De hecho, casi todos los lineamientos consideran el manejo de las enfermedades concomitantes como un com-ponente del tratamiento de la hipertensión.
Otras consideraciones en la elaboración de estos linea-mientos, como traducciones, aspectos legales y sociales, fue-ron escasamente tenidas en cuenta. Además, no se analizaron las situaciones psicológicas ni económicas de las poblaciones destinatarias. Solo los lineamientos del National Institute for Clinical Excellence y los lineamientos para hipertensión bra-sileños IV consideraron las situaciones socioeconómicas de la población destinataria, mientras que solo los lineamientos del Canadian Hypertension Education Program tuvieron en cuenta los canales de difusión y la vigilancia de la hipertensión (Ta-bla S2). Se prevé que cada lineamiento sea actualizado cada 3 años47 para incluir nueva evidencia o tratamiento. Entre los
Lineamiento/Título Nivel de evidencia
Parámetros clínicos consid-
eradosHipertensión en situa-
ciones especiales Otras consideraciones
17. NICE No se efectúa ninguna recomendación ni gradu-
ación, búsqueda bibliográfica sistemática
Presión arterial ERC, IM, accidente cerebrovascular
Ya no se recomiendan tiazidas como fármacos de primera línea. La diana de PA en personas >80 años es de 150/90,
mientras que es de 140/90 para las demás.
18. Lineamientos prácticos para el tratamiento de la hipertensión
No declarado Presión arterial, peso
ERC, cardiopatía, DM, ancianos, embarazo,
hipertensión resistente
No declaradas
19. Lineamientos de práctica clínica Adopción de JNC 6, JNC 7, OMS/ISH, ESH/ESC
Presión arterial, peso
ERC, DM No declaradas
20. Guía 2008 para el tratamiento de la hipertensión23
Revisión bibligráfica Presión arterial, peso, PVY
ERC, DM, accidente cerevrovascular
No declaradas
21. Lineamientos de Etiopía para el tratamiento estándar
Adopción de JNC 7 Presión arterial, IMC
No declarado No declaradas
22. Lineamientos de Sudán para la hipertensión
Adopción de JNC 7. OMS/ISH, BHS, ESH/ESC, International society of hypertension in
black guidelines for manage-ment of hypertension
Presión arterial, peso, talla
ERC, DM, cardiopatía, accidente cerebrovas-
cular, ancianos
No declaradas
23. Lineamientos 2009 de Kenia para el tratamiento de la hipertensión
Adopción de JNC 7 Presión arterial No declarado El objetivo es reducir la PA diastólica a 90 mm Hg
Tabla 2. Continuación
ACC indica American College of Cardiology; ACCF/AHA, American College of Cardiology Foundation; IECA, inhibidor de la enzima convertidora de angiotensina; AHA, American Heart Association; BRA, bloqueantes del receptor de angiotensina; ASH/ISA, American Society of Hypertension/International Society of Hypertension; BHS, British Society of Hypertension; IMC, índice de masa corporal; PA, presión arterial; BCC, bloqueantes de los canales de calcio; CDC, Centers for Disease Control and Prevention; CHEP, Canadian Hypertension Education Program; ERC, enfermedad renal crónica; DM, diabetes mellitus; ESH/ESC, European Society of Hyper-tension/European Society of Cardiology; JNC, Joint National Committee; PVY, presión venosa yugular; IM, infarto de miocardio; NICE, National Institute for Clinical Excellence; EAC, estudios aleatorizados controlados; y OMS, Organización Mundial de la Salud.

45Owolabi et al Revisión sistemática de lineamientos para hipertensión
lineamientos disponibles para revisión en el momento de esta publicación, solo los de Japón, Europa y Estados Unidos están actualizados.
Puntos fuertes y débilesNuestra estrategia de búsqueda incluyó todos los países, y eva-luamos de manera crítica todos los lineamientos disponibles mediante criterios rigurosos y exhaustivos. Sin embargo, esta revisión solo incluyó los lineamientos de hipertensión escri-tos en inglés o traducidos al inglés. Se podrían haber omitido
otros lineamientos escritos en otros idiomas29,41,48-55.56 Más aún, como utilizamos las recomendaciones del IOM para valorar la calidad de los lineamientos, no usamos otros parámetros si-milares, como la Global Rating Scale (Escala de clasificación global).57 Se excluyeron los lineamientos de la Organización Mundial de la Salud/International Society of Hypertension (2003)47 porque no fueron cubiertos en el marco de tiempo es-tipulado para nuestra revisión.
En esta revisión, no incluimos la World Heart Federation Global cardiovascular disease Roadmap (Hoja de ruta global
Lineamiento/TítuloTranspar-
enciaConflictos de interés
Enfoque multidisci-
plinario
Revisiones sistemáti-
cas
Puntos fuertes de las
recomen-dación
Claridad de la
recomen-dación
Revisión externa
Actualiza-ciones
1. Lineamientos para el tratamiento de la hipertensión en Nigeria
No No No No No No No No
2. Lineamientos de hipertensión sufafri-canos
Sí Sí Sí Sí Sí Sí Sí Sí
3. Lineamientos brasileños sobre hipertensión
No No No No No No No No
4. Lineamientos chinos 2010 para el tratamiento de la hipertensión
Sí Sí Sí Sí Sí Sí Sí Sí
5. Lineamientos clínicos para la detección, la prevención, el diagnóstico y el tratamiento de la hipertensión arterial sistémica en México
Sí Sí Sí Sí Sí Sí Sí Sí
6. Lineamientos de la Japanese Society of Hypertension para el tratamiento de la hipertensión (JSH 2009)
Sí Sí Sí Sí Sí Sí Sí Sí
7. Lineamientos para la hipertensión41 No No No No No No No No8. Lineamientos 2013 de la ESH/ESC para
el tratamiento de la hipertensión arterialSí Sí Sí Sí Sí Sí Sí Sí
9. JNC 8 Sí Sí Sí Sí Sí Sí Sí Sí10. Tratamiento de la hipertensión en adul-
tos: lineamientos 2013 de la Sociedad Francesa de Hipertensión
Sí Sí Sí Sí Sí Sí Sí Sí
11. Lineamientos 2010 de la Taiwan Socie-ty of Cardiology para el tratamiento de la hipertensión
No No No No No No No No
12. ASH/ISH No No No No No No No No13. ACCF/AHA Sí Sí Sí Sí Sí Sí Sí Sí14. CHEP No No No Sí Sí Sí No Sí15. AHA/ACC/CDC No No No No No No No No16. AHA No No No No No No No No17. NICE Sí Sí Sí Sí Sí Sí Sí Sí18. Lineamientos prácticos para el tratami-
ento de la hipertensiónNo No No No No No No No
19. Lineamientos de práctica clínica No No No No No No No No20. Guía 2008 para el tratamiento de la
hipertensión23Sí Sí Sí Sí Sí Sí Sí Sí
21. Lineamientos de Etiopía para el tratam-iento estándar
No No Sí No No No No No
22. Lineamientos de Sudán para la hipertensión
Sí Sí Sí Sí Sí Sí Sí No
23. Lineamientos 2009 de Kenia para el tratamiento de la hipertensión
No No No No No No No No
Tabla 3. Cumplimiento de los estándares del Institute of Medicine para la elaboración de lineamientos para la práctica clínica
AHA/ACC/CDC indica American Heart Association/American College of Cardiology/Centers for Disease Control and Prevention; ACCF/AHA, American College of Cardiology Foundation/American Heart Association; ASH/ISA, American Society of Hypertension/International Society of Hypertension; CHEP, Canadian Hyperten-sion Education Program; ESH/ESC, European Society of Hypertension/European Society of Cardiology; JNC, Joint National Committee; y NICE, National Institute for Clinical Excellence.

46 Hypertension Diciembre 2016
de enfermedad cardiovascular de la World Heart Federation)58 porque no son lineamientos per se. Enumera las dificultades para el control de la hipertensión y sugiere algunas maneras de superarlas al asistir a la población hipertensa. Sin embargo, no demuestra el proceso de elaboración de las recomendaciones que se deben efectuar ni la contextualización ni otros aspectos de implementación pertinentes de los lineamientos para hiper-tensión. Si estos son defectuosos, el control de la hipertensión será aún una tarea hercúlea.
Conclusiones y planes futurosLos lineamientos sobre hipertensión son necesarios para la prevención, la detección temprana, la evaluación, el tratamien-to y el control de la hipertensión correctos y adecuados.44,59 Sin embargo, deben cumplir con criterios básicos que incluyen va-lidez, fiabilidad/reproducibilidad, aplicabilidad clínica, flexibi-lidad clínica, contextualización socioeconómica y ético-legal, claridad, proceso multidisciplinario y plan de difusión riguro-so.60 Lamentablemente, ninguno de los lineamientos existentes cumple con todos estos criterios. Esto podría explicar por qué la hipertensión todavía es difícil de controlar en muchas regio-nes del mundo, dado que no se aprovechan posibles canales valiosos para la difusión y la implementación.
Esta revisión pone en evidencia que se requieren esfuer-zos para elaborar lineamientos para hipertensión destinados a los PBMI (Tabla 5). Los lineamientos previstos deben ser am-plios, flexibles, adaptables, aceptables desde el punto de vis-ta sociocultural y económicamente alcanzables para obtener mejores resultados relacionados con la salud en pacientes con hipertensión. Como ejemplifican los lineamientos del National Institute for Clinical Excellence, se debe incorporar la partici-pación de los pacientes para mejorar el cumplimiento de estas recomendaciones.
Como la elaboración de novo de lineamientos insume tiem-po, es trabajosa y costosa, cualquier lineamiento que cumpla con la mayoría de los criterios usados para esta revisión se puede considerar un modelo para el desarrollo de lineamientos para los PBMI, que incorporen a la vez evidencia local solo si se dispone de ella. Esto resultará un enfoque más realista para evitar la duplicación de esfuerzos mientras se aguarda
Tabla 4. Componentes del cuadrángulo cardiovascular considerados
Tabla 5. Soluciones adecuadas sugeridas para mejorar la calidad y la repercusión de los lineamientos para hipertensión en los PBMI
Solo Europa, Nigeria y Sudán consideraron la vigilancia epidemiológica y la agenda de investigación (uno de los pilares del cuadrángulo).
PaísesNivel de ingresos
Prevención primordial
Prehiperten-sión
Tratamiento específico de
edad Nutrición Ejercicio
Atención aguda/Emer-
genciasAtención
convencionalRehabilitac-
ión
Estados Unidos Alto No No Sí Sí Sí No Sí No
Australia Alto No Sí Sí Sí Sí Sí Sí No
Brasil Medio No Sí Sí Sí Sí Sí Sí No
Canadá Alto Sí No Sí Sí Sí No Sí No
China Medio No No Sí Sí Sí No Sí No
Etiopía Bajo No Sí No Sí Sí Sí Sí No
Europa Alto No Sí Sí Sí Sí Sí Sí No
Francia Alto No Sí Sí Sí Sí No Sí No
India Medio No No Sí Sí Sí Sí Sí No
Japón Alto No No No Sí Sí No Sí No
Kenia Medio No No No Sí Sí Sí Sí No
México Medio No No No Sí Sí No Sí No
Nigeria Medio Sí No No Sí Sí No Sí No
Sudáfrica Medio Sí No Sí Sí Sí Sí Sí Sí
Sri Lanka Medio No Sí Sí Sí Sí Sí Sí No
Sudán Medio No Sí Sí Sí Sí Sí Sí Sí
Taiwán Alto No No Sí Sí Sí No Sí No
Reino Unido Alto Sí No Sí Sí Sí No Sí No
Colaboración entre organizaciones de profesionales a fin de elaborar linea-mientos para hipertensión.
Participación de los pacientes, los líderes de opinión clave y los encargados de formular políticas en la elaboración de los lineamientos para hiperten-sión.
Al elaborar los lineamientos, se deben considerar las situaciones sociales, psicológicas y económicas de la región o el país.
Compromiso enérgico de todas las partes interesadas (médicos, presta-dores de salud no médicos, cuidadores primarios, encargados de formular políticas, pagadores, pacientes, población y socios de implementación) durante la elaboración, la implementación y la evaluación.
Elaboración de recomendaciones activas clave, concisas, especialmente empaquetadas y difundidas entre todas las partes interesadas (médicos, prestadores de salud no médicos, cuidadores primarios, encargados de formular políticas, pagadores, pacientes, población y socios de implement-ación).
Realización de estudios de alta calidad de una manera específica de contxto en los PBMI.
PBMI indica países de bajos y medianos ingresos.

47Owolabi et al Revisión sistemática de lineamientos para hipertensión
que se acumule evidencia de alto nivel de los PBMI. Estos lineamientos serán socioculturalmente aceptables y rentables para la implementación exitosa en las regiones del mundo con escasos recursos.
Se requiere con urgencia elaborar y difundir lineamientos pragmáticos basados en la evidencia con recomendaciones concisas pasibles de implementación relevantes para las ne-cesidades y el contexto socioeconómico de los PBMI. Con la participación activa de las partes interesadas, la atención y los productos recomendados se podrían tornar aceptables, accesi-bles, disponibles, apropiados, asequibles y eficaces para redu-cir la carga global de hipertensión.
Fuentes de financiamientoM. Owolabi y B. Ovbiagele son subvencionados por U54 HG007479 y U01 NS079179 de los National Institutes of Health y la GACD (Global Alliance for Chronic Diseases). A.G. Thrift es subvencionado por una beca del National Health & Medical Research Council (1042600).
Declaración de conflictos de interésNinguno.
Referencias1. Cao X. A call for global research on non-communicable diseases. Lancet.
2015;385:e5–e6. doi: 10.1016/S0140-6736(14)62383-7.2. Kearney PM, Whelton M, Reynolds K, Muntner P, Whelton PK, He J.
Global burden of hypertension: analysis of worldwide data. Lancet. 2005;365:217–223. doi: 10.1016/S0140-6736(05)17741-1.
3. Naghavi M, Wang H, Lozano R, et al. Global, regional, and national age-sex specific all-cause and cause-specific mortality for 240 causes of death, 1990–2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet. 2015;385:117–171. doi: 10.1016/ S0140-6736(14)61682-2.
4. Hameed K, Kadir M, Gibson T, Sultana S, Fatima Z, Syed A. The fre- quency of known diabetes, hypertension and ischaemic heart disease in affluent and poor urban populations of Karachi, Pakistan. Diabet Med. 1995;12:500–503.
5. van de Vijver S, Akinyi H, Oti S, et al. Status report on hypertension in Afri-ca-consultative review for the 6th Session of the African Union Conference of Ministers of Health on NCD’s. Pan African Medical Journal. 2014;16.
6. Seedat YK. Hypertension in developing nations in sub-Saharan Africa. J Hum Hypertens. 2000;14:739–747.
7. Opie LH, Seedat YK. Hypertension in sub-Saharan African popu-lations. Circulation. 2005;112:3562–3568. doi: 10.1161/ CIRCULATIONAHA.105.539569.
8. Liu LS; Writing Group of 2010 Chinese Guidelines for the Management of Hypertension. 2010 Chinese guidelines for the management of hyper- ten-sion. Zhonghua Xin Xue Guan Bing Za Zhi. 2011;39:579–615.
9. Nwankwo T, Yoon S, Burt V, Gu Q. Hypertension among adults in the US: National Health and Nutrition Examination Survey, 2011–2012. NCHS data brief, no. 133. National Center for Health Statistics, Centers for Disease Control and Prevention, Hyattsville, MD, US Dept of Health and Human Services Ref Type: Report. 2013.
10. Odili V, Oghagbon E, Ugwa N, Ochei U, Aghomo O. Adherence to inter- national guidelines in the management of hypertension in a tertiary hospital in Nigeria. Trop J Pharm Res. 2008;7:945–952.
11. Williams B. Recent hypertension trials: implications and controversies. J Am Coll Cardiol. 2005;45:813–827. doi: 10.1016/j.jacc.2004.10.069.
12. Saunders E. Hypertension in African-Americans. Circulation. 1991;83:1465–1467.
13. Baker EH, Ireson NJ, Carney C, Markandu ND, MacGregor GA. Transepithelial sodium absorption is increased in people of African origin. Hypertension. 2001;38:76–80.
14. Moher D, Liberati A, Tetzlaff J, Altman DG; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA sta-tement. Ann Intern Med. 2009;151:264–9, W64.
15. Graham R, Mancher M, Wolman DM, Greenfield S, Steinberg E. Committee on Standards for Developing Trustworthy Clinical Practice Gui-delines; Board on Health Care Services Clinical Practice Guidelines We can
Trust. Washington, DC, National Academies Press; 2011.16. Kung J, Miller RR, Mackowiak PA. Failure of clinical practice guidelines
to meet institute of medicine standards: Two more decades of little, if any, progress. Arch Intern Med. 2012;172:1628–1633. doi: 10.1001/2013. ja-mainternmed.56.
17. Owolabi MO, Akarolo-Anthony S, Akinyemi R, et al; Members of the H3A-frica Consortium. The burden of stroke in Africa: a glance at the present and a glimpse into the future. Cardiovasc J Afr. 2015;26(2 suppl 1):S27–S38. doi: 10.5830/CVJA-2015-038.
18. Z Score Calculator for 2 Population Proportions. http://www.socscista- tis-tics.com/tests/ztest/Default2.aspx Z Score Calculator for 2 Poulation Pro-portions. Accessed June 24, 2016.
19. Rau NR, Nayak SK. Practical guidelines for hypertension management. http://www.apiindia.org/medicine_update_2013/chap17.pdf. Accessed May 15, 2016.
20. Wijesisiwardene B, Mohideen R. Clinical practice guidelines. http://www. slcog.lk/img/guidelines/Other%20national%20Gidelines/Physicians/ Book%201/Management%20of%20Hypertension.pdf. Accessed May 15, 2016.
21. Tadesse Y. Ethiopia standard treatment guidelines. http://siapsprogram. org/publication/ethiopia-standard-treatment-guidelines/”. Accessed June 2, 2016.
22. Sulima AA, Aboud MH. Sudan hypertension guidelines. http://ssh-sd. org/fileload/sudan%20hypertension%20guidelines.pdf. Accessed June 2, 2016.
23. Guide to Management of Hypertension 2008. www.heartfoundation.org. au/Professional_Information/Clinical_Practice/Hypertension. Accessed June 6, 2016.
24. Crouch M. 2009 Kenya guideline for hypertension management. http://apps.who.int/medicinedocs/documents/s21000en/s21000en.pdf. Accessed July 5, 2016.
25. Onwubere B, Kadiri S. Guidelines for the management of hypertension in Nigeria. In: Nigerian Hypertension Society Enugu. Ezu Books Limited. 2005:1–4.
26. Seedat YK, Rayner BL; Southern African Hypertension Society. South Afri-can hypertension guideline 2011. S Afr Med J. 2012;102(1 pt 2):57–83.
27. Sociedade BdH, Cardiologia SBd, Nefrologia SBd. VI Brazilian guide- li-nes on hypertension. Arq Bras Cardiol. 2010;95:1.
28. Rosas M, Pastelin G, Vargas-Alarcon G et al. . Arch Inst Cardiol Mex. 2007;78:S2-5–57.
29. Shimamoto K, Ando K, Fujita T, et al; Japanese Society of Hypertension Committee for Guidelines for the Management of Hypertension. The Japa-nese Society of Hypertension Guidelines for the Management of Hyper-tension (JSH 2014). Hypertens Res. 2014;37:253–390. doi: 10.1038/hr.2014.20.
30. Aronow WS. Hypertension guidelines. Hypertension. 2011;58:347–348. doi: 10.1161/HYPERTENSIONAHA.111.177147.
31. Mancia G, Fagard R, Narkiewicz K, et al. 2013 ESH/ESC guide- lines for the management of arterial hypertension: the Task Force for the Mana-gement of Arterial Hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC). Blood Pressure. 2013;22:193–278.
32. James PA, Oparil S, Carter BL, et al. 2014 evidence-based guideline for the management of high blood pressure in adults: report from the panel mem-bers appointed to the Eighth Joint National Committee (JNC 8). JAMA. 2014;311:507–520. doi: 10.1001/jama.2013.284427.
33. Blacher J, Halimi JM, Hanon O, Mourad JJ, Pathak A, Schnebert B, Girerd X; French Society of Hypertension. Management of hypertension in adults: the 2013 French Society of Hypertension guidelines. Fundam Clin Pharma-col. 2014;28:1–9. doi: 10.1111/fcp.12044.
34. Chiang CE, Wang TD, Li YH, Lin TH, Chien KL, Yeh HI, Shyu KG, Tsai WC, Chao TH, Hwang JJ, Chiang FT, Chen JH; Hypertension Committee of the Taiwan Society of Cardiology. 2010 guidelines of the Taiwan Society of Cardiology for the management of hyper- tension. J Formos Med Assoc. 2010;109:740–773. doi: 10.1016/ S0929-6646(10)60120-9.
35. Wood S. ASH/ISH issue separate hypertension guidelines from JNC 8, hin-ting at discord. Medscape. 2013;19.
36. Aronow WS, Fleg JL, Pepine CJ, et al. ACCF/AHA 2011 expert consen- sus document on hypertension in the elderly: a report of the American College of Cardiology Foundation Task Force on Clinical Expert Consensus docu-ments developed in collaboration with the American Academy of Neuro-logy, American Geriatrics Society, American Society for Preventive Cardio-logy, American Society of Hypertension, American Society of Nephrology, Association of Black Cardiologists, and European Society of Hypertension. J Am Coll Cardiol. 2011;57:2037–2114. doi: 10.1016/j.jacc.2011.01.008.
37. Dasgupta K, Quinn RR, Zarnke KB, et al; Canadian Hypertension Edu-cation Program. The 2014 Canadian Hypertension Education Program recommendations for blood pressure measurement, diagnosis, assess-

48 Hypertension Diciembre 2016
ment of risk, prevention, and treatment of hypertension. Can J Cardiol. 2014;30:485–501. doi: 10.1016/j.cjca.2014.02.002.
38. Go AS, Bauman MA, Coleman King SM, Fonarow GC, Lawrence W, Wi-lliams KA, Sanchez E; American Heart Association; American College of Cardiology; Centers for Disease Control and Prevention. An effective approach to high blood pressure control: a science advisory from the Ameri-can Heart Association, the American College of Cardiology, and the Centers for Disease Control and Prevention. Hypertension. 2014;63:878–885. doi: 10.1161/HYP.0000000000000003.
39. Calhoun DA, Jones D, Textor S, Goff DC, Murphy TP, Toto RD, White A, Cushman WC, White W, Sica D, Ferdinand K, Giles TD, Falkner B, Carey RM. Resistant hypertension: diagnosis, evaluation, and treat- ment. A scien-tific statement from the American Heart Association Professional Education Committee of the Council for High Blood Pressure Research. Hypertension. 2008;51:1403–1419. doi: 10.1161/ HYPERTENSIONAHA.108.189141.
40. Ritchie LD, Campbell NC, Murchie P. New NICE guidelines for hyper- ten-sion. BMJ. 2011;343:d5644.
41. Argentina: Guias de la Sociedad Argentina de Hipertension para el Diag-nostico, Estudio, Tratamiento y Seguimiento de la Hipertension Arterial. http://www.saha.org.ar/1/pdf/GUIA_SAHA_VERSION_COMPLETA.pdf. Accessed August 19, 2016.
42. Guyatt GH, Oxman AD, Kunz R, Vist GE, Falck-Ytter Y, Schünemann HJ; GRADE Working Group. What is “quality of evidence” and why is it important to clinicians? BMJ. 2008;336:995–998. doi: 10.1136/ bmj.39490.551019.BE.
43. Ayanian JZ, Landon BE, Newhouse JP, Zaslavsky AM. Racial and ethnic disparities among enrollees in Medicare Advantage plans. N Engl J Med. 2014;371:2288–2297. doi: 10.1056/NEJMsa1407273.
44. Whelton PK, Beevers DG, Sonkodi S. Strategies for improvement of awareness, treatment and control of hypertension: results of a panel dis-cussion. J Hum Hypertens. 2004;18:563–565. doi: 10.1038/ sj.jhh.1001738.
45. Muntner P, Gu D, Wu X, Duan X, Wenqi G, Whelton PK, He J. Factors associated with hypertension awareness, treatment, and control in a repre- sentative sample of the Chinese population. Hypertension. 2004;43:578–585. doi: 10.1161/01.HYP.0000116302.08484.14.
46. World Health Organization, Group ISoHW. 2003 World Health Organi-zation (WHO)/International Society of Hypertension (ISH) state- ment on management of hypertension. J Hyp. 2003;21:1983–1992.
47. Whitworth JA, Chalmers J. World Health Organisation-International Socie-ty of Hypertension (WHO/ISH) hypertension guidelines. Clin Exp Hyper-tens. 2004;26:747–752.
48. Brasília: Ministério da Saúde. Estratégias para o cuidado da pessoa com doença crônica: hipertensão arterial sistêmica. (Cadernos de Atenção Bási-ca, n. 37; 2013.) http://dab.saude.gov.br/portaldab/biblioteca. php?conteu-do=publicacoes/cab37. Accessed August 19, 2016.
49. Chile: Ministerio de Salud. Guía Clínica 2010 Hipertensión Arterial Prima-ria o esencial en personas de 15 años y más. Santiago: Minsal, 2010. http://www.minsal.gob.cl/portal/url/item/7220fdc4341c44a9e04001011f0113b9.pdf. Accessed August 19, 2016.
50. Colombia: Sistema General de Seguridad Social en Salud. Guía de prác- tica clínica: Hipertensión Arterial Primaria (HTA). 2013 - Guía No. 18. ht-tps://www.minsalud.gov.co/sites/rid/Lists/BibliotecaDigital/RIDE/ INEC/IETS/GPC_Ptes_HTA.pdf. Accessed August 19, 2016.
51. Costa Rica: Caja Costarricense de Seguro Social. Guias para la Detección, Diagnóstico y Tratamiento de la Hipertensión Arterial. III Edición. San José, Costa Rica, 2009 http://www.binasss.sa.cr/libros/hipertension09. pdf. Accessed August 19, 2016.
52. México: Instituto Mexicano del Seguro Social; 08/07/2014. Diagnóstico y Tratamiento de la Hipertensión Arterial en el Primer Nivel de Atención. http://www.cenetec.salud.gob.mx/descargas/gpc/CatalogoMaestro/076- GCP__HipertArterial1NA/HIPERTENSION_EVR_CENETEC.pdf. Ac-cessed August 19, 2016.
53. Peru: Ministerio de Salud. Guía Técnica: Guía de Práctica Clínica para la Diagnóstico, Tratamiento y Control de la Enfermedad Hipertensiva; January 19, 2015. http://www.minsa.gob.pe/dgsp/documentos/Guias/ RM031-2015-MINSA.pdf. Accessed August 19, 2016.
54. Panamá: Organización Panamericana de la Salud. Guía para la atención in-tegral de las personas con Hipertensión arterial. Impresora Pacifico, 2009. http://www.paho.org/pan/index.php?option=com_docman&task=doc_view&gid=298 &Itemid=224. Accessed August 19, 2016.
55. Argentina: La Revista Argentina de Cardiología. Consenso de Hiper-tensión Arterial. Vol 81 Suplemento 2, Agosto 2013. http://www.sac. org.ar/wp-content/uploads/2014/04/Consenso-de-Hipertension-Arterial. pdf. Accessed August 19, 2016.
56. Morrison A, Moulton K, Clark M, Polisena J, Fiander M, Mierzwinski- Ur-ban M, Mensinkai S, Clifford T, Hutton B. English-Language Restriction When Conducting Systematic Review-Based Meta-Analyses: Systematic Review Of Published Studies. Ottawa: Canadian Agency for Drugs and Te-chnologies in Health; 2009.
57. Brouwers MC, Kho ME, Browman GP, Burgers JS, Cluzeau F, Feder G, Fervers B, Graham ID, Grimshaw J, Hanna SE, Littlejohns P, Makarski J, Zitzelsberger L; AGREE Next Steps Consortium. The Global Rating Scale complements the AGREE II in advancing the quality of prac- tice guidelines. J Clin Epidemiol. 2012;65:526–534. doi: 10.1016/j. jclinepi.2011.10.008.
58. Adler AJ, Prabhakaran D, Bovet P, Kazi DS, Mancia G, Mungal-Singh V, Poulter N. Reducing Cardiovascular Mortality Through Prevention and Ma-nagement of Raised Blood Pressure: A World Heart Federation Roadmap. Glob Heart. 2015;10:111–122. doi: 10.1016/j.gheart.2015.04.006.
59. McAlister FA, Feldman RD, Wyard K, Brant R, Campbell NR; CHEP Out-comes Research Task Force. The impact of the Canadian Hypertension Edu-cation Programme in its first decade. Eur Heart J. 2009;30:1434–1439. doi: 10.1093/eurheartj/ehp192.
60. Field MJ, Lohr KN. Attributes of Good Practice Guidelines. Washington, DC, National Academies Press; 1990.
61. Owolabi M, Miranda JJ, Yaria J, Ovbiagele B. Controlling cardiovascular diseases in low-and middle-income countries by placing proof in pragma- tism. BMJ Global Health. doi: 10.1136/bmjgh-2016-000105. In press.





























