Embed Size (px)
Citation preview

GYNECOLOGIC ONCOLOGY 2, 460-475 (1974)
Gestational Trophoblastic Neoplasms
ROBERT D. HILGERS, M.D.
Diuision of Gynecologic Oncology, University of Minnesota Hospitals, Minneapolis, Minnesota 55455
AND
JOHN L. LEWIS, JR., M.D.
Chief, Division of Gynecologic Oncology, Memorial Hospital for Cancer and Allied Diseases, New York, New York 10021
Received May 28, 1974
A review of the classification, biological behavior, clinical diagnosis, and treat- ment of gestational trophoblastic neoplasms is presented. The events which followed the utilization of chemotherapy as a successful means of therapy are included. Especially important has been the recent recognition that high risk pa- tients, i.e., patients with HCG titers greater than 100,000 III/24 hr, duration of symptoms greater than four months, and metastasis to the brain and/or liver, with metastatic trophoblastic disease can be managed successfully if treated initially with combination chemotherapy and adjuvant measures including radiation and in- fusional therapy.
Detectable levels of human chorionic gonadotropin are necessary for diagnosis and management of patients with this disease. The lack of sensitivity of commer- cially available pregnancy tests and the recent ability to determine HCG by means of an antigenically different beta-subunit are discussed.
Chemotherapy, given with the intent to be curative of the neoplasm it is directed against, has found its most successful application in patients with gestational trophoblastic disease. While a brief period of 18 years has passed since the initial observation was made that a folic acid antagonist (metho- trexate) was found to be effective in eradicating neoplasms derived from the trophoblast of the placental villus, gestational trophoblastic neoplasms con- tinue to be the most sensitive of all neoplastic growths to appropriately selected anti-neoplastic agents. Before 1955 the prospect of survival for a pa- tient with metastatic choriocarcinoma was virtually nil. By utilizing che- motherapy it is now possible to achieve 90% survival in patients with meta- static gestational trophoblastic disease and to preserve reproductive function in patients with nonmetastatic gestational trophoblastic disease.
HISTORICAL DEVELOPMENT
Two observations led to selecting methotrexate for a therapeutic trial in patients with metastatic trophoblastic disease. The first occurred when spe- cific inhibition of estrogen induced growth was observed in the internal genitalia of experimental animals fed a folic acid deficient diet or treated with a folic acid antagonist [23,27]. Th e second occurred when a previously
460
Copyright @ 1974 by Academic Press, Inc. All rights of reproduction in any form reserved.

GESTATIONAL TROPHOBLASTIC NEOPLASM!3 461
high gonadotropin titer dropped following a course of methotrexate in a hypophysectomized woman with metastatic melanoma [35]. The initial trial of methotrexate consisted of two patients with metastatic choriocarcinoma and one patient with chorioadenoma destruens [38]. Two of these patients are alive today and have received no chemotherapy for 15 years.
While the initial response was unexpectedly good, results of a second study- involving a larger number of patients followed for 5 years-demon- strated that 50% of these patients eventually developed resistance to metho- trexate (25). Simultaneously, Li [35] observed that actinomycin D was useful in combination with methotrexate and an alkylating agent in the treat- ment of testicular and methotrexate resistant gestational choriocarcinomas. When actinomycin D [46] was used in women with metastatic gestational trophoblastic disease the following observations were made: gestational trophoblastic neoplasms did respond as predicted; actinomycin D was equally as effective as methotrexate; drug resistance to one drug did not imply resistance to the other; actinomycin D could be used more safely in patients with impaired liver function; a complete remission rate of 74% (37 of 50 patients) was achieved when the two drugs were utilized in a sequen- tial manner; and certain prognostic criteria became apparent.
When the results of the above studies were reviewed it was determined that the most reliable criteria for predicting a successful response included the height of the initial HCG titer, the duration of disease prior to chemo- therapy and the site of metastases. A cure rate of 95% was observed in women whose initial titer was less than 100,000 IU/24 hr, whose disease was treated within 4 months of the apparent onset and in whom metastases were limited to the lungs or pelvis. In contrast, patients with long-standing disease as- sociated with high gonadotropin titers and liver or brain metastases re- sponded much less favorably (36% complete remission rate) to single agent chemotherapy [46]. Two groups were thus defined for patients with meta- static disease: a “low risk” and a “high risk” group. Subsequently, a new pro- tocol was formulated to treat “high risk” patients by means other than with single agent chemotherapy [30]. As expected, better response rates were achieved. Complete remission can now be demonstrated in 100% of patients who fit the criteria of the “low risk” category: short duration, low titer, and metastases limited to the lungs or pelvis [16,19,31]. In the “high risk” cat- egory a 70-85% remission rate occurs when the patient is treated initially with combination chemotherapy and adjuvant measures including radiation and infusional therapy [19,31]. Lastly, a fourth factor, i.e., proper administra- tion of the chemotherapeutic agents, has been included as an important cri- teria for a successful response [19].
CLASSIFICATION
A histological classification exists for gestational trophoblastic neoplasms which is based on histology and location [22]. The degree of retention of the villus structures as well as the extent of invasion or the presence of metas- tasis are the prime determinants in making up this classification. For in-

462 HILGERS AND LEWIS
stance, a hydatidiform mole is defined by the presence of grossly swollen villi, absent fetal vessels, and varying degrees of trophoblastic cell growth whereas a choriocarcinoma is designated by sheets of malignant tropho- blastic cells in the absence of placental villi. A chorioadenoma destruens is an invasive mole.
The prime difficulty with this classification is that it cannot be utilized as a reliable indicator for prognosis, managing patients undergoing therapy, or determining a complete remission when it occurs. Likewise, attempts to grade the activity of the tumor by the relative degree of trophoblastic prolif- eration have proved unreliable. Experienced pathologists disagree and their diagnoses, while valid on the basis of the material studied, do not always agree with the clinical situation. In a given patient benign molar tissue can be present in the uterus at the same time choriocarcinoma is present in the lungs or a patient with an adequately evacuated benign hydatidiform mole can months later develop a metastasis which on biopsy proves to be chorio- carcinoma. Finally, because the treatment of metastatic disease is the same regardless of the histology, the risk-benefit relationship makes it unneces- sary to biopsy all metastatic sites for histology purposes only.
From his own clinical and laboratory experience, Hertz [35] emphasized a clinical classification based on grouping together those diseases which could be treated alike and recognized in a given group of patients that treatment could be modified accordingly. A clinical spectrum was recognized arising from a continuum of biologically interrelated conditions, i.e., hydatidiform mole, chorioadenoma destruens, and choriocarcinoma. The essential bio- logical features which they shared were their ability to produce human chorionic gonadotropin (HCG) and their ability to respond to chemotherapy. He termed these tumors “gestational trophoblastic neoplasms” to distin- guish them from the nongestational trophoblast-containing tumors which arise in the testes and ovaries. Clinically, gestational trophoblastic neo- plasms may be classified as metastatic or nonmetastatic depending upon whether extrauterine extension has occurred. This classification is therefore reliable, simple, and therapeutically applicable in patients with gestational trophoblastic neoplasms.
BIOLOGICAL BEHAVIOR
Each of the histopathologically designated entities, i.e., hydatidiform mole, invasive mole and choriocarcinoma, arise initially from an abnormal villus. Their growth pattern suggests that they share a common pathogenetic pathway. Nearly one-half of the cases of choriocarcinoma are preceded by a hydatidiform mole and in the very early stages of the disease formed villi have been found in one area while choriocarcinoma existed concomitantly elsewhere [3]. The disease begins in the two cell layers, i.e., the cyto- trophoblast and the syncytiotrophoblast, that overlie the chorionic villus. Here neoplastic transformation takes place and only differentiation and loca- tion of recognizable villus structures in the neoplastic chorionic tissue sepa- rates each of the histological types.

GESTATIONAL TROPHOBLASTIC NEOPLASMS 463
Characteristically these tumors are highly proliferative and extremely vas- cular, making them especially prone to cause clinically significant hemor- rhages. They exhibit a vast endothelial bed whose only supporting stroma is the tumor itself. Invasion of the neighboring blood vessels leads to early dis- semination. Discrete metastases or vascular obstruction by trophoblastic emboli may occur. In choriocarcinoma, particularly, this may lead to frequent complications such as external or internal hemorrhage, compression or infiltration of vital organs, and perforation [39]. The tumor most com- monly metastasizes to the lungs and less frequently to the vagina, brain or liver, Metastases have been observed in such unusual sites as the breast, bone, lymph nodes, as well as to a branch of a coronary artery [41]. Their growth pattern often leads to unusual initial manifestations of disease when the first symptoms are due to metastases in organs other than the reproduc- tive tract (Table I).
The biological behavior of these tumors varies widely (See Table II). Approximately 50% of the patients with metastatic trophoblastic disease and 75% of the patients with nonmetastatic trophoblastic disease develop them as a sequelae to molar pregnancy [25,46]. In the other 25-50% of cases the diagnosis is made following other types of pregnancy, i.e., term pregnancy, abortion or tubal pregnancy. Each histologic typel*‘is capable of metas- tasizing. Villus structures have been identified in setera extrauterine sites. Approximately 95% of such metastases, however, are choriocarcinoma. A sig- nificant number of patients with metastatic disease will have no demon- strable residual disease in the uterus as evidenced by both clinical and au- topsy studies [4,24]. Latent choriocarcinoma has been observed several years after the last known pregnancy [ll]. Spontaneous regressions are known to occur [l2].
The mortality rate for hydatidiform mole is relatively low, however, its at- tendant morbidity (hemorrhage, sepsis, toxemia) is significant. Once the uterus is evacuated, approximately 85-90% of these patients will eventually undergo complete remission and the remaining lo-15% will have persistent
TABLE I NONGYNECOLOGICAL MANIFESTATIONS OF METASTATIC TROPHOBLASTIC DISEASE
Pulmonary Coin lesion Progressive dyspnea or hemoptysis X-ray appearance of pneumonia Unexplained pulmonary hypertension
Central nervous system Signs of an expanding lesion Hemorrhage (intracerebral, subarachnoid or subdural)
Gastrointestinal Hemorrhage (lesions of small or large bowel)
Genitourinary Hemorrhage (renal or bladder) Ureteral obstruction
464 HILGERS AND LEWIS
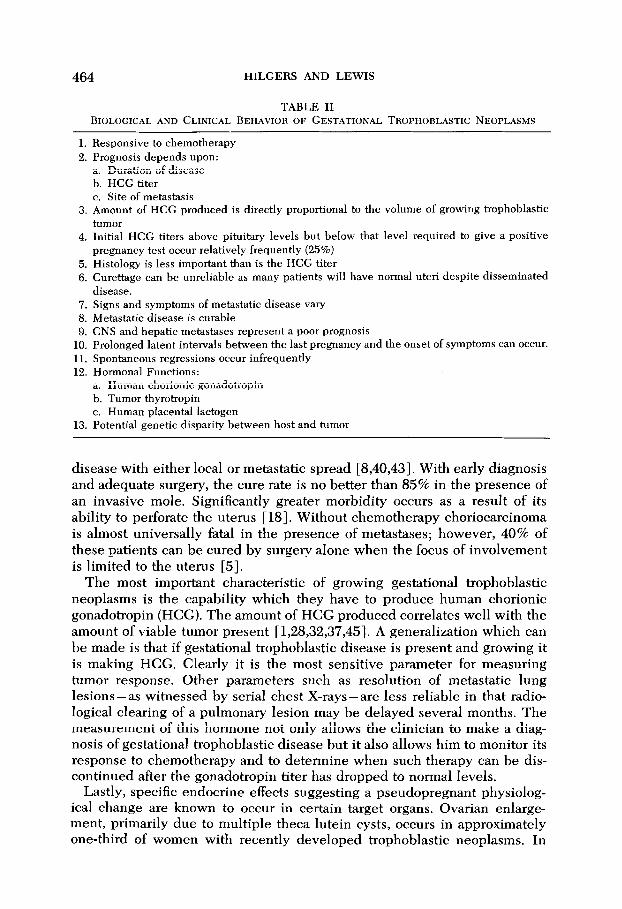
TABLE II BIOLOGICAL AND CLINICAL BEHAVIOR OF GESTATIONAL TROPHOBLASTIC NEOPLASMS
1. Responsive to chemotherapy 2. Prognosis depends upon:
a. Duration of disease b. HCG titer c. Site of metastasis
3. Amount of HCG produced is directly proportional to the volume of growing trophoblastic tumor
4. Initial HCG titers above pituitary levels but below that level required to give a positive pregnancy test occur relatively frequently (25%)
5. Histology is less important than is the HCG titer 6. Curettage can be unreliable as many patients will have normal uteri despite disseminated
disease. 7. Signs and symptoms of metastatic disease vary 8. Metastatic disease is curable 9. CNS and hepatic metastases represent a poor prognosis
10. Prolonged latent intervals between the last pregnancy and the onset of symptoms can occur. 11. Spontaneous regressions occur infrequently 12. Hormonal Functions:
a. Human chorionic gonadotropin b. Tumor thyrotropin c. Human placental lactogen
13. Potential genetic disparity between host and tumor
disease with either local or metastatic spread [8,40,43]. With early diagnosis and adequate surgery, the cure rate is no better than 85% in the presence of an invasive mole. Significantly greater morbidity occurs as a rest& of its ability to perforate the uterus [ 181. Without chemotherapy choriocarcinoma is almost universally fatal in the presence of metastases; however, 40% of these patients can be cured by surgery alone when the focus of involvement is limited to the uterus [5].
The most important characteristic of growing gestational trophoblastic neoplasms is the capability which they have to produce human chorionic gonadotropin (HCG). The amount of HCG produced correlates well with the amount of viable tumor present [1,28,32,37,45]. A generalization which can be made is that if gestational trophoblastic disease is present and growing it is making HCG. Clearly it is the most sensitive parameter for measuring tumor response. Other parameters such as resolution of metastatic lung lesions- as witnessed by serial chest X-rays-are less reliable in that radio- logical clearing of a pulmonary lesion may be delayed several months. The measurement of this hormone not only allows the clinician to make a diag- nosis of gestational trophoblastic disease but it also allows him to monitor its response to chemotherapy and to determine when such therapy can be dis- continued after the gonadotropin titer has dropped to normal levels.
Lastly, specific endocrine effects suggesting a pseudopregnant physiolog- ical change are known to occur in certain target organs. Ovarian enlarge- ment, primarily due to multiple theta lutein cysts, occurs in approximately one-third of women with recently developed trophoblastic neoplasms. In
GESTATIONAL TROPHOBLASTIC NEOPLASMS 465
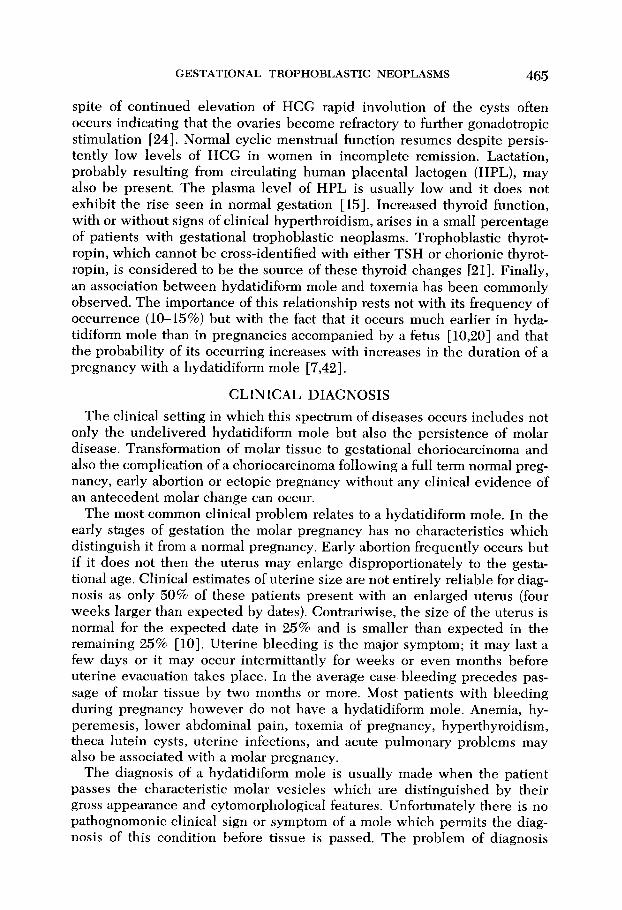
spite of continued elevation of HCG rapid involution of the cysts often occurs indicating that the ovaries become refractory to further gonadotropic stimulation [24]. Normal cyclic menstrual function resumes despite persis- tently low levels of HCG in women in incomplete remission. Lactation, probably resulting from circulating human placental lactogen (HPL), may also be present. The plasma level of HPL is usually low and it does not exhibit the rise seen in normal gestation [ 151. Increased thyroid function, with or without signs of clinical hyperthroidism, arises in a small percentage of patients with gestational trophoblastic neoplasms. Trophoblastic thyrot- ropin, which cannot be cross-identified with either TSH or chorionic thyrot- ropin, is considered to be the source of these thyroid changes 1213. Finally, an association between hydatidiform mole and toxemia has been commonly observed. The importance of this relationship rests not with its frequency of occurrence (lo-15%) but with the fact that it occurs much earlier in hyda- tidiform mole than in pregnancies accompanied by a fetus [10,20] and that the probability of its occurring increases with increases in the duration of a pregnancy with a hydatidiform mole [7,42].
CLINICAL DIAGNOSIS
The clinical setting in which this spectrum of diseases occurs includes not only the undelivered hydatidiform mole but also the persistence of molar disease. Transformation of molar tissue to gestational choriocarcinoma and also the complication of a choriocarcinoma following a full term normal preg- nancy, early abortion or ectopic pregnancy without any clinical evidence of an antecedent molar change can occur.
The most common clinical problem relates to a hydatidiform mole. In the early stages of gestation the molar pregnancy has no characteristics which distinguish it from a normal pregnancy. Early abortion frequently occurs but if it does not then the uterus may enlarge disproportionately to the gesta- tional age. Clinical estimates of uterine size are not entirely reliable for diag- nosis as only 50% of these patients present with an enlarged uterus (four weeks larger than expected by dates). Contrariwise, the size of the uterus is normal for the expected date in 25% and is smaller than expected in the remaining 25% [lo]. Uterine bleeding is the major symptom; it may last a few days or it may occur intermittantly for weeks or even months before uterine evacuation takes place. In the average case bleeding precedes pas- sage of molar tissue by two months or more. Most patients with bleeding during pregnancy however do not have a hydatidiform mole. Anemia, hy- peremesis, lower abdominal pain, toxemia of pregnancy, hyperthyroidism, theta lutein cysts, uterine infections, and acute pulmonary problems may also be associated with a molar pregnancy.
The diagnosis of a hydatidiform mole is usually made when the patient passes the characteristic molar vesicles which are distinguished by their gross appearance and cytomorphological features. Unfortunately there is no pathognomonic clinical sign or symptom of a mole which permits the diag- nosis of this condition before tissue is passed. The problem of diagnosis

466 HILGERS AND LEWIS
before evacuation is therefore complex and requires additional means of de- tection. Further difficulty results from the fact that a fetus is coincidentally present in less than 5% of these patients [2].
The most reliable methods for detecting the presence of a mole prior to evacuation are: amniography, ultrasonography, and pelvic arteriography. The most useful method is amniography (the transabdominal injection of a water soluble dye into the amniotic cavity) [13,15]. This method is com- monly available and the characteristic honeycomb pattern seen in a hyda- tidiform mole is specific. Ultrasonography is the safest and the most reliable for early diagnosis, but is not as available in as many institutions. Pelvic ar- teriography is not recommended for routine use in the diagnosis of a molar pregnancy as it involves relatively large doses of radiation which may be in- jurious to a possibly normal pregnancy. Other diagnostic aids, i.e., absence of fetal heart tones, fetal parts on an abdominal roentgenogram, fetal ballot- ment, and fetal activity as well as maximum levels of human chorionic gonadotropin are suggestive but are not reliable as absolute indicators for diagnosis.
Following evacuation of a molar pregnancy concern is directed towards minimizing the danger of metastases or persistent molar disease in the uterus. A metastatic work-up will direct attention to the presence or absence of metastases. The presence of persistent nonmetastatic disease confined to the uterus is determined by the HCG titer and the lack of metastases. Ordi- narily in 80% of patients the HCG level will drop to within normal limits by eight weeks following evacuation. Failure of the HCG titer to drop to normal within eight weeks, failure of the uterus to completely involute and con- tinued vaginal bleeding are signs that trophoblastic disease persists. Care- fully determined measurements of HCG must be performed in a sequential manner until complete remission has been determined.
Approximately 50% of choriocarcinomas are preceded by hydatidiform moles; no more than 2-5% of all trophoblastic disease is represented by choriocarcinoma. Persistent elevations of the HCG titer are diagnostically important. Histological examination of biopsied tissue can be helpful for diagnosis but it is not essential for treatment. Choriocarcinoma may occur without any immediately preceding symptoms and the dilatation and curet- tage and pelvic examination may be negative. In addition, nonmetastatic choriocarcinoma following a full term delivery will present with vaginal bleeding but metastatic disease often will not.
While most patients develop symptoms from trophoblastic neoplasms shortly after delivery, longer asymptomatic intervals may occur. In the in- terim normal menstruation may resume and pregnancy tests may remain negative. If the tumor appears in the uterus the first symptom may be vaginal bleeding and the clinical picture is often confused with that of a threatened or incomplete abortion. This may not occur however as is illustrated by the patient who presented six years after a hysterectomy for a mole with a large liver metastasis masquerading as cholecystitis [51] and by the patient who died from surgically demonstrated choriocarcinoma of the brain four years after a hysterectomy for a mole. [9]. Diagnostic errors occur more commonly

GESTATIONAL TROPHOBLASTIC NEOPLASMS 467
after such a prolonged latent period. Unfortunately, the diagnosis in these instances is often not made until after the patient has undergone a craniot- omy, thoracotomy, resection of a segment of small bowel or a nephrectomy. To guarantee a correct diagnosis at a lesser expense to the patient, a high index of suspicion is a prerequisite in every female patient in the reproduc- tive age. Especially pertinent to this problem are the nongynecological manifestations of trophoblastic disease which are listed in Table I.
An accurate measurement of the amount of human chorionic gonadotropin excreted in the urine or present in the serum is the key to the diagnosis and the management of patients with gestational trophoblastic neoplasms. The normal level of HCG in a nonpregnant woman is, by definition, zero. How- ever since most available pregnancy tests fail to differentiate HCG from pituitary LH a patient is considered to have normal gonadotropin levels when the levels are low enough to be consistent with pituitary gonadotropin production. HCG is ordinarily measured in terms of International Units (IU) or Mouse Uterine Units (MUU) per 24 hr. Ten MUU are equivalent to one IU. During most of the menstrual cycle this level is less than the equivalent of 10 IU HCG; even at the time of the midcycle peak of LH the level still remains less than the equivalent of 100 IU HCG.
HCG can be quantitatively determined by bioassay, immunoassay, or radioimmunoassay techniques. They are useful only to the extent that their lower limits of sensitivity for HCG allow them to be. The range of sensitivity of the commercially available pregnancy tests varies between 0.85 and 5 IU/ml. of urine and therefore they can detect levels above 850 to 5000 IU of HCG in an average 24 hr urine specimen of one liter depending upon the test used. When the HCG titer is high, an ordinary pregnancy test can be ex- pected to detect and quantitate the level present. These tests are not useful for detecting HCG below these levels of sensitivity even though persistent tumor may be producing amounts of HCG far in excess of pituitary gonado- tropin. To detect these lower levels of HCG, it is necessary to utilize a sensi- tive radioimmunoassay or techniques for concentrating the urine and then use a sensitive bioassay, such as the Klinefelter mouse uterine weight assay. Therefore one cannot rely on a negative pregnancy test for diagnostic exclu- sion. Approximately 25-30% of patients with gestational trophoblastic dis- ease will have an initial HCG titer in excess of the pituitary levels but below the 850-1000 IU/24 hr needed to give a positive pregnancy test [47].
These assays fail to distinguish between chorionic, tumor or pituitary gonadotropins and therefore when pituitary levels are reached HCG is no longer considered to be present. A radioimmunoassay has recently been developed which will differentiate HCG from pituitary LH by utilizing the antigenic difference which exists for one major polypeptide subunit, the beta subunit [49]. Unfortunately this test is available in only a few institutions at this time.
TREATMENT
Chemotherapy has revolutionized the treatment of patients with gesta- tional trophoblastic disease. Results of studies performed at NIH

468 HILGERS AND LEWIS
(1955-1965) established the effectiveness of methotrexate and actinomycin D and the predictability of their toxic effects in these patients. Chemo- therapy can be utilized as a single agent or as a combination of agents. The decision regarding what agent(s) is to be used depends upon the clinical sit- uation, i.e., the presence of metastatic vs nonmetastatic disease, the duration of the disease, the height of the HCG titer, the site of metastasis, and the results of tests of hepatic, renal and marrow function. The basic treatment plan is outlined in Table III. Methotrexate, 0.3-0.4 mg/kg/day, is most com- monly used, however, drug resistance and hepatic toxicity precludes its use in many instances. Actinomycin D, 8-13 pg/kg/day, may be slightly more ef- fective and can be used where methotrexate cannot. Drug toxicity is to be expected and consists of stomatitis, leucopenia, granulocytopenia, impair- ment of hepatic function, skin rash, gastrointestinal upset and alopecia [ 171. Criteria for avoiding dangerous toxicity have been established and appear in Table IV. The patient’s bone marrow, renal and hepatic function need to be closely monitored in order to modify drug administration so as to avoid po- tentially dangerous toxicity. Ross et al. [47] have established the criteria shown in Table IV as contraindications to initiating, continuing or resuming drug therapy. These should be checked for each day and the drug should not be given until the laboratory results are known for that day. Once a specific drug (or drugs) has been chosen, the patient is given a 5-day course with subsequent repeat courses being given only after all toxicity from the pre- vious course is reversed. When a single drug is used subsequent courses are given until there is evidence that the titer is rising, the titer has remained at a plateau after two courses, the titer has not returned to normal after four courses, new metastasis have appeared, or overwhelming toxicity has re- sulted from the drug used. At that time another drug is used. Therapy is stopped when the HCG level is normal for 3 consecutive weeks.
TABLE III BASIC TREATMENT
Drugs Single agent chemotherapy: Methotrexate or actinomycin D Combination chemotherapy: Methotrexate, actinomycin D plus an alkylating agent or
actinomycin D plus 6 mercaptopurine Toxicity studies
Marrow: Hbg. and Hcrit. WBC and differential Platelet count Renal: BUN and creatinine Hepatic: SGOT
Gonadotropin assays During treatment: Weekly until 3 consecutive assays are normal Following complete remission: 1. Every 2 weeks X 3
2. Monthly x 3
Chest x-rays
3. Every 2 months X 6 4. Every 6 months thereafter
Once a month for first year

GESTATIONAL TROPHOBLASTIC NEOPLASMS 469
TABLE IV INDICATIONS FOR ALTEFUNC OR STOPPING CHEMOTHERAPY
1. White blood cell count less than 3000/mm” 2. Polymorphonuclear leukocyte count less than 1500/mm3 3. Platelet count less than 100,000/mm~ 4. Abnormal Liver Function tests (e.g., serum bilirubin or transaminases) 5. Abnormal Renal Function tests (e.g., elevated serum urea, creatinine)
Weekly 24 hr urines are collected and assayed for HCG. The HCG levels are followed to determine differences in response. Once a complete remis- sion (three normal gonadotropin titers at weekly intervals) has been obtained the patient is followed very closely according to a set schedule (see Table III). A patient is not considered cured until she has survived 5 years fol- lowing complete remission and cessation of therapy. Previous studies from the NIH [25,46] showed that 90% of patients who enter complete remission will need no further therapy while 8% will relapse within eight weeks and 2% will relapse thereafter. Thus a patient with gonadotropin excretion in the pituitary range for three months after therapy had a 98% chance of re- maining free of disease without further chemotherapy. The use of oral con- traceptives during the year following diagnosis has facilitated the detection of slight elevations of tumor gonadotropin by depressing normal endogenous pituitary function. As a result 99% of the patients followed in this manner have remained free of disease once complete remission has been achieved 1191.
Surgery plays a definite role in the supportive treatment of patients with metastatic gestational trophoblastic disease [29,34] and is useful in some pa- tients with nonmetastatic trophoblastic disease, depending on age, parity and desire for preservation of reproductive function. It may also be useful in patients with persistent tumor localized to the uterus which remains resis- tant to chemotherapy. In metastatic disease the indications for surgery are primarily to control bleeding, drain abscesses, and occasionally to remove residual disease. While these efforts do not eradicate the disease they do control the complications of the disease temporarily, thereby allowing the patient to live long enough to respond to chemotherapy. On an experimental basis adjunctive chemotherapy, at less than full toxic dose, has been used to cover the patient during the time of surgery.
The clinical categories associated with gestational trophoblastic neoplasms are listed in Table V. The treatment of each of these conditions will be dis- cussed briefly.
Nonmetastatic Trophoblastic Disease
The primary therapeutic approach for a hydatidiform mole is surgical. In the past a dilatation and curettage was recommended when the uterus was less than I2 weeks gestational size and a hysterotomy when the uterus was

470 HILGERS AND LEWIS
TABLE V CLINICAL CATEGORIES ASSOCIATED WITH GESTATIONAL TROPHOBLASTIC NEOPLASMS
I. Nonmetastatic trophoblastic disease A. Hydatidiform mole
1. Undelivered 2. Delivered (<8 weeks)
B. Persistent mole (>8 weeks) C. Invasive mole or choriocarcinoma confined to the uterus
II. Metastatic trophoblastic disease A. Low risk category
1. Short duration (~4 mo) 2. Low HCG titer (< 100,000 IU/24 hr) 3. Lung or vaginal metastasis
B. High risk category 1. Long duration (>4 mo) 2. High HCG titer (> 100,000 IU/24 hr) 3. CNS or liver metastasis
larger. At the present time evacuation by means of intravenous pitocin and suction curettage seems to be the preferred method. Care must be taken to rule out the presence of a co-existent fetus if its size would make suction curettage unfeasible. If suction curettage equipment is not available then intravenous pitocin until the mole is delivered and subsequent curettage is recommended [6]. Hysterectomy is reserved for the woman who has com- pleted her childbearing or, who is 40 years or older. Prophylactic chemo- therapy utilized at the time of evacuation has caused a modest reduction in the rate of malignant progression after molar pregnancy. For the present, how- ever, it is felt that essentially 100% of patients who have the malignant sequelae of hydatidiform mole diagnosed in the period immediately fol- lowing a molar pregnancy can be cured by presently available techniques and that prophylactic treatment is not recommended for all patients who have had hydatidiform moles [20].
Once a mole has been evacuated the patient should be followed with weekly HCG titers for a period of 8 weeks. At that time approximately 20% will continue to exhibit an elevated HCG; this group of patients is con- sidered to have a persistent mole. Of this group approximately 50% will develop a clinically or histologically malignant condition, i.e., an invasive mole or choriocarcinoma [8]. They are treated on the basis of the elevated HCG titer and not on the basis of a specific histologic diagnosis.
The final group of patients which are included under the heading of non- metastatic gestational trophoblastic disease are those who present with a diagnosis of choriocarcinoma made by curettage following a full term deliv- ery or an abortion. The important diagnostic criteria are: a histological diag- nosis of a trophoblastic tumor, an elevated HCG titer, and no evidence of metastases [26,48].
The two most important factors which need to be considered in managing patients with nonmetastatic gestational trophoblastic disease are the pa-

GESTATIONAL TROPHOBLASTIC NEOPLASMS 471
tient’s desire to preserve her reproductive function, and the potential danger of her disease becoming metastatic and life threatening.
Women with a positive titer 8 weeks following evacuation of a mole, who desire children, should have a curettage during the midportion of a course of single agent chemotherapy. Surgery is therapeutic in this instance and will be helpful in determining if the tissue present is choriocarcinoma. The pa- tient is then treated with a course or several courses of the selected che- motherapeutic agent until the HCG titer drops to normal, i.e., low enough to be consistent with pituitary levels.
The best evidence that the quality of survival for these patients is ex- cellent comes from observing the large number of successful pregnancies following chemotherapy. The number of subsequent pregnancies now totals more than 200 [31]. There has not been any increase in prematurity, still- births, or congenital anomalies nor has there been any reactivation of a previous trophoblastic neoplasm in these pregnancies. An increased in- cidence of retained placenta and placenta accreta [50] and spontaneous abortions [44] in subsequent pregnancies has been reported, however this may reflect damage to the reproductive tract rather than to any drug effect.
If the patient is older and her family is completed then a hysterectomy is considered appropriate for primary treatment. If the HCG titer persists two or more weeks following the hysterectomy then metastatic disease should be suspected.
The woman who presents with a choriocarcinoma limited to the uterus presents a somewhat more difficult problem. This is particularly true when choriocarcinoma persists following repeated attempts with chemotherapy. If the patient desires more children it is reasonable to use chemotherapy alone; however, it may not be safe to wait until after the patient’s disease has been shown to be noncurable by chemotherapy before going on to a hys- terectomy as the appearance of a metastasis occurring during chemotherapy has been reported [33]. If no further children are desired then the wise pol- icy is to perform a hysterectomy on the third day of the first course of chemotherapy. When childbearing remains important, chemotherapy is rec- ommended until the disease clears or until it is evident that the patient is not responding to that particular drug. In this instance a hysterectomy should be performed during the first course of the next drug selected.
Complete remission occurs in 100% of patients with nonmetastatic gesta- tional trophoblastic neoplasms who are treated by single agent chemo- therapy 1311. In less than 10% of these patients it is necessary to resort to sec- ondary therapy, i.e., a hysterectomy, whereas in the other 90% reproductive function is preserved. The cure rate of 100% by chemotherapy alone and chemotherapy plus surgery amply exceeds the reported cure rate of approx- imately 40% for such patients by hysterectomy alone [5].
Metastatic gestational trophoblastic disease. Patients with obvious evi- dence of trophoblastic disease beyond the limits of the uterus belong in this category. These patients can be separated into two groups based on certain prognostic factors which predict their degree of risk (Table V).

472 HILGERS AND LEWIS
When the disease has been present for four months or less, the HCG titer is less than 100,000 IU/24 hr and only pulmonary or vaginal metastases are present the patient can be expected to respond satisfactorily to single agent chemotherapy. However, when the duration is longer, the HCG titer higher, and either brain or liver metastases are present, the response to conventional single agent chemotherapy is unsatisfactory and the patient is at greater risk of not responding to this therapy, Proper administration of the drugs and adequate laboratory support have recently been added as a fourth factor upon which a successful response depends [19].
Low risk patients are best treated by single agent chemotherapy, i.e., methotrexate or actinomycin D, according to the schedule previously out- lined (Table III). Reports of 100% complete remission are now being re- ported from several institutions for this group [16,19,31]. The overall results from any institution will, of course, depend upon the percentage of patients which ultimately fall into this low risk group.
Of the several major prognostic criteria, the site of metastasis is the most important in terms of response. Patients with either brain or liver metastases have traditionally responded poorly to conventional methods of therapy. Less important factors also may contribute to a poor prognosis and these are: unexplainable resistance to the usual drugs, prior inadequate therapy, pro- hibitive toxicity, and a histological diagnosis of choriocarcinoma [14].
The poor response rate in the “high risk” group of patients treated with single agent chemotherapy has improved since combination chemotherapy and adjunctive radiation therapy, where indicated, have been carried out as the initial form of treatment. A five day course of actinomycin D, chloram- bucil, and methotrexate is repeated cyclically until the HCG titer returns to normal. If metastases are demonstrated in tbe brain or the liver, whole organ irradiation of approximately 2000 rads is delivered to these areas. Radiation therapy alone has rarely been reported as curative, however it does seem to lessen the risk of acute hemorrhage during administration of the chemo- therapeutic agent. When these measures prove unsuccessful, then arterial drug infusions or high dose methotrexate with citrovorum rescue can be considered. The response rate, following this therapeutic approach, has improved from a previous figure of approximately 35-40% [46] to a cur- rent figure of 70-85% [19,31].
These results have come about, at least in part, as a consequence of the es- tablishment of regional centers. They have not only provided gonadotropin assay laboratories and expertise in treatment but they have also helped by making local physicians become more aware of the varied ways in which metastatic disease may present itself. Because of this awareness the diag- nosis is being made earlier at a time when the patient is still in a good prog- nostic category. In the past the primary errors have been a failure to consider the diagnosis, to perform the necessary tests when indicated and a failure to administer the drugs in a proper manner. All data supports the concept that early diagnosis is associated with limited disease and that limited disease is associated with a high cure rate and only modest toxicity.

GESTATIONAL TROPHOBLASTIC NEOPLASMS 473
REFERENCES
1. BAGSHAWE, B. D. Choriocarcinoma. The clinical biology of the trophoblast and its tumors, The Williams and Wilkins Company, Baltimore, MD (1969).
2. BEISCHER, N. Hydatidiform mole with coexistent fetus, Aust. N. 2. J. O&et. Gynecol. 6, 127-141 (1966).
3. BREWER, J. I., AND GERBIE, A. B. Early development of choriocarcinoma, Amer. J. Obstet. Gynecol. 94,692-705 (1966).
4. BREWER, J. I., RINEHART, J. J.. AND DUNBAR, R. Choriocarcinoma, Amer. J. Obstet. Gyn- ecol. 81,574-583 (1961).
5. BREWER, J. I., SMITH, R. T., AND PRATT, G. B. Choriocarcinoma. Absolute five year survival rates of 122 patients treated by hysterectomy, Amer. J. Obstet. Gynecol. 85, 841-843 (1963).
6. CHAN, D. P. C. A plea against abdominal hysterectomy in the treatment of hydatidiform mole, Med. J. Malaya 20,36-38 (1965).
7. CHESLEY, L. C., COSGROVE, S. A., AND PREECE, J. Hydatidiform mole with special refer- ence to recurrence and associated eclampsia, Amer. I. Obstet. Gynecol. 52, 311-320 (1946).
8. DELFS, E. Quantitative chorionic gonadotropin: Prognostic value in hydatidiform mole and chorioepithelioma, Obstet. Gynecol. 9, l-9 (1957).
9. DOCKERTY, M. B., AND CRAIG, W. McK. Chorioepithelioma. An unusual case in which cerebral metastasis occurred four years after hysterectomy, Amer. J. Obstet. Gynecol. 44, 497-501 (1942).
10. DOUGLAS, G. W. The diagnosis and management of hydatidiform mole, Szrrg. C&n. N. Amer. 37,379-392 (1957).
11. DYKE, P. C., AND FINK, L. M. Latent choriocarcinoma, Cancer 20, 150-154 (1967). 12. EVERSON, T. C., AND COLE, W. H. Spontaneous regression of cancer, W. B. Saunders Com-
pany, Philadelphia, PA, p. 221 (1966). 13. GERBER, A. H. Amniographic diagnosis of trophoblastic disease, I. Amer. Med. Ass. 212, 630
(1970). 14. GOLDSTEIN, D. P. The management of gestational tiophoblastic disease, in Meigs and
Stwgis progress in gynecology (S. H. Sturgis and M. L. Taymor, Eds.), Grune and Stratton, New York, Volume 5, Chapter 7, pp. 397-415 (1970).
15. GOLDSTEIN, D. P. Five years experience with the prevention of trophoblastic tumors by the prophylactic use of chemotherapy in patients with molar pregnancy, Clin. Obstet. Gyn- ecol. 13,945-961 (1971).
16. GOLDSTEIN, D. P. The chemotherapy of gestational tiophoblastic disease. Principles of clinical management, f. Amer. Med. Ass. 220,209-213 (1972).
17. GOLDSTEIN, D. P., AND REID, D. E. Recent developments in the management of molar pregnancy, Clin. Obstet. Gynecol. 10,313-322 (1967).
18. GREEN, R. R. Chorioadenoma destruens, Ann. N. Y. Acad. Sci. 80, 143-151 (1959). 19. HAMMOND, C. B., BORCHERT, L. G., TYREY, L., CREASMAN, W. T., AND PARKER, R. T.
Treatment of metastatic trophoblastic disease: Good and poor prognosis. Amer. j. Obstet. Gynecol. 115,451-457 (1973).
20. HAMMOND, C. B., AND LEWIS, J. L., JR. Gestational trophoblastic neoplasms, in Gynecology and obstetrics (Davis, Ed.), Harper and Row, Publishers, Inc., Hagerstown, Volume I, Chapter 37N, pp. l-30 (1972).
21. HERSHMAN, J. M. Hyperthyroidism induced by trophoblastic thyrotropin, Mayo Clin. Proc. 47,913-918 (1972).
22. HERTIC, A. T., AND MANSELL, H. Tumors of the female sex organs: I. Hydatidiform mole and choriocarcinoma, in Atlas of tumor pathology, Washington, D. C., Armed Forces In- stitute of Pathology (1956).
23. HERTZ, R. Interference with estrogen-induced tissue growth in the chick genital tract by a folic acid antagonist, Science 107,300 (1948).
24. HERTZ, R. Biological aspects of gestational neoplasms derived from trophoblast, Ann. N. Y. Acad. Sci. 172,279-287 (1971).

474 HILGERS AND LEWIS
25. HERTZ, R., LEWIS, J. L., JR., AND LIPSETT, M. B. Five years experience with the chemo- therapy of metastatic choriocarcinoma and related trophoblastic tumors in women, Amer. J. Obstet. Gynecol. 82,631-640 (1971).
26. HERTZ, R., Ross, G. R., AND LIPSETT, M. B. Primary chemotherapy of nonmetastatic trophoblastic disease in women, Amer. J. Obstet. Gynecol. 86,808-814 (1963).
27. HERTZ, R., AND TULLNER, W. W. Quantitative interference with estrogen induced tissue growth by folic acid antagonists, Endocrinology 44,278-282 (1949).
28. KOHLER, P. O., AND BRIDSON, W. E. Isolation of hormone-producing clonal lines of human choriocarcinoma, Comments 22,683-687 (1971).
29. LEWIS, J. L., JR. Chemotherapy and surgery in the treatment of gestational trophoblastic neoplasms, Surg. Clin. N. Amer. 49,371-380 (1969).
30. LEWIS, J. L., JR. Choriocarcinoma task force. Transactions of the annual meeting of the soci- ety of the alumni of the Sloane Hospital for Women, Bull. Sloane Hosp. Women 15,75-77 (1969).
31. LEWIS, J. L., JR. Chemotherapy of gestational choriocarcinoma, Cancer 30, 1517-1521 (1972).
32. LEWIS, J. L., JR., DAVIS, R. C., AND Ross, G. T. Hormonal, immunologic and chemothera- peutic studies of transplantable human choriocarcinoma, Amer. J. Obstet. Gynecol. 111, 547-554 (1971).
33. LEWIS, J. L., JR., GORE, H., HERTIG, A. T., AND GOSS, D. A. Treatment of trophoblastic disease with rationale for the use of adjunctive chemotherapy at the time of indicated operation, Amer. J. Obstet. Gynecol. 96,710-722 (1966).
34. LEWIS, J. L., JR., KETCHAM, A. S., AND HERTZ, R. Surgical intervention during chemo- therapy of gestational trophoblastic neoplasms. Cancer 19, 1517-1522 (1966).
35. LI, M. C. A discussion of the paper, “Chemotherapy of choriocarcinoma and related tro- phoblastic tumors in women”, Ann. N. Y. Acad. Sci. 80,280-284 (1959).
36. LI, M. C. Management of choriocarcinoma and related tumors of uterus and testis, Med. Clin. N. Amer. 45,661-676 (1961).
37. LI, M. C. Trophoblastic disease: Natural history, diagnosis and treatment,Ann. Int. Med. 74, 102-lll(1971).
38. LI, M. C., HERTZ, R., AND SPENCER, D. B. Effect of methotrexate therapy upon choriocar- cinema and chorioadenoma, Proc. Sot. Exp. Biol. Med. 93,361-366 (1956).
39. MAGRATH, I. T., GOLDING, P. R., AND BAGSHAWE, K. D. Medical presentations of choriocar- cinema, Brit. Med. J. 2,633-637 (1971).
40. NOVAK, E., AND SEAH, C. S. Choriocarcinoma of the uterus, Amer. J. Obstet. Gynecol. 67, 933-961 (1954).
41. OBER, W. B., EDGCOMB, J. H., AND PRICE, E. B. The pathology of choriocarcinoma, Ann. N. Y. Acad. Sci. 172,299-321 (1971).
42. PAGE, E. W. Hydatidiform mole, Amer. J. Obstet. Gynecol. 37,291-293 (1939). 43. PARK, W. W. Choriocarcinoma. A general review, with an analysis of 516 cases, Arch.
Pathol. 49,73-104, 205-241 (1951). 44. PASTORFIDE, G. B., AND GOLDSTEIN, D. P. Pregnancy after hydatidiform mole, Obstet.
Gynecol. 42,67-70 (1973). 45. PATTILLO, R. A., GEY, G. D., DELFS, E., AND MATTINGLY, R. F. Human hormone produc-
tion in uiuo, Science 159, 1467-1469 (1968). 46. ROSS, G. T., GOLDSTEIN, D. P., HERTZ, R., LIPSETT, M. B., AND ODELL, W. D. Sequential
use of methotrexate and actinomycin D in the treatment of metastatic choriocarcinoma and related trophoblastic diseases in women, Amer. J. Obstet. Gynecol. 93, 223-229 (1965).
47. ROSS, G. T., HAMMOND, C. B., HERTZ, R., LIPSETT, M. B., AND ODELL, W. Chemotherapy of metastatic and non-metastatic gestational trophoblastic neoplasms, Tex. Rep. Biol. Med. 24,326-338 (1966).
48. ROSS, G. T., HAMMOND, C. B., AND ODELL, W. D. Chemotherapy for nonmetastatic gesta- tional trophoblastic neoplasm, Clin. Obstet. Gynecol. l&323-329 (1967).

GESTATIONAL TROPHOBLASTIC NEOPLASMS 475
49. VAITIJKAITUS, J. L., BFNJNSTEIN, G. D., AND Ross, G. T. A radioimmunoassay which specifically measures human chorionic gonadotropin in the presence of human lu- teinizing hormone, Amer. J. O&et. Gynecol. 113, 751-758 (1972).
50. VAN THIEL, D. H., GRODIN, J. M., Ross, G. T., AND LIPSETT, M. B. Partial placenta accreta in pregnancies following chemotherapy for gestational trophoblastic neoplasms, Amer. J. Obstet. Gynecol. 112, 54-58 (1972).
51. WILDE, W. L., ARMSTRONG, S., AND BYRNE, J. J. Metastatic choriocarcinoma masquerading as acute cholecystitis six years after hysterectomy, Amer. J. Surg. 113, 414-417 (1967).