Embed Size (px)
Citation preview

Thorax, 1978, 33, 520-523
Giant fibromyxoma of the parietal pleuraD C NWAFO AND F C ADI
From the Cardiothoracic Surgical Unit and the Department of Medicine,University of Nigeria, Enugu Campus, Enugu, Nigeria
Nwafo, D C, and Adi, F C (1978). Thorax, 33, 520-523. Giant fibromyxoma of the parietalpleura. A 23-year-old Nigerian man with a giant (8&5 kg) benign intrathoracic fibromyxomapresented in respiratory distress with what looked clinically and radiologically like a massiveleft-sided pleural effusion. The correct preoperative diagnosis was suggested by an almost 'drytap' together with a solid resistance to the aspiring needle at chest aspiration. Complete removalwas successfully accomplished through an extended left thoracotomy. The pathology, clinicalfeatures, and treatment of localised pleural fibromas are briefly discussed.
Primary pleural neoplasms are exceedingly rare.The tumours are now widely regarded as meso-theliomas of which two varieties are recognised-a 'diffuse malignant' and a 'localised fibrous'mesothelioma (Clagett et al., 1952). Owing toearlier confusion as to their origin, the localisedfibrous variety has been previously described by amultiplicity of names, including intrathoracicfibroma, pleural fibroma, benign localised meso-thelioma, and solitary localised mesothelioma.We will use the term intrathoracic fibroma.A common, though not widely recognised,
feature of localised fibrous intrathoracic fibromasis their tendency to recur after resection(Klemperer and Rabin, 1931; Clagett et al., 1952;Ehrenhaft et al., 1960; Kerr and Nohl, 1961).Dolley and Brewer (1943) maintain that all slowlygrowing intrathoracic fibromas have alreadyundergone malignant change. According to Willis(1953), those tumours in which pronounced myxo-matous degeneration has occurred are best re-garded as frankly malignant. We report here atypical intrathoracic fibromyxoma that is not onlyremarkable for its size (8 5 kg) but also in retain-ing its 'benign' characteristics despite its longhistory and extensive myxomatous change. More-over, it illustrates nearly all the features usuallyassociated with an intrathoracic fibroma. So faras we are aware there has been no previous reportof a similar case from West Africa.
Case report
A 25-year-old Igbo mechanic gave a four-yearhistory of progressive shortness of breath associ-
ated, in the last five months, with a dry unpro-ductive cough and precordial pain. There wereoccasional febrile episodes and joint pains, but nohaemoptysis. He had been treated at anotherhospital for orthopnoea and swelling of the legswithout much improvement. In 1972 he had alsobeen treated for shortness of breath and transientswelling of the legs.On arrival at the University of Nigeria Teach-
ing Hospital, Enugu (UNTH), he was orthopnoeicand too short of breath to talk for more than afew minutes. His fingers were clubbed. The neckveins were engorged, almost to the mandible. Thetrachea was markedly deviated to the right andthe apex beat located in the sixth right intercostalspace at the anterior axillary line. The left hemi-thorax was stony dull to percussion with absentbreath sounds. There were scattered rhonchi overthe right hemithorax, but breath sounds wereotherwise normal. The spleen and liver were en-larged three finger-breadths below the costalmargin. The chest radiograph (Fig. 1) suggesteda massive left-sided pleural effusion, but aspira-tion yielded only 100 ml blood-stained fluid beforea solid resistance was encountered with theaspirating needle. The aspirate contained nomalignant cells. At bronchoscopy the trachea was
compressed anteroposteriorly and markedly de-viated to the right. The left main bronchial orificecould not be identified. Pleural biopsy showedinflammation only. At thoracotomy (1 August1977), an enormous solid, lobulated, and well-encapsulated tumour weighing 8-5 kg (Fig. 2)filled the left chest, compressing the left lung intoa small crescent at the apex and pushing the
520
on January 4, 2020 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.33.4.520 on 1 August 1978. D
ownloaded from

Giant fibromyxoma of the parietal pleura
Fig. 1 Radiograph showing giant leftpleural tumour causing gross mediastinaldisplacement to right.
Fig. 2 Solid, lobulated, and well-encapsulatedfibromyxoma completely removed at thoracotomy(weight 8 5 kg).
heart into the right hemithorax. The pleura was
considerably thickened with large veins coursingover it, and it contained a large quantity of alteredblood. Despite a wide thoracotomy only piecemeal
removal was possible. This permitted full and sus-tained re-expansion of the left lung. Recoverywas uneventful.
Histologically, the thickened pleura showedonly nonspecific inflammation. The tumour itselfwas a fibromyxoma reported on as follows: 'Thepattern is benign, there being no mitotic figures.In parts, there are decussating sheets of connec-tive tissue. Elsewhere a myxomatous appearanceis noted (Figs. 3 and 4). The alternative diagnosis.of a solid mesothelioma is to be borne in mind, asthe latter tumour is occasionally solid, simulating afibromatous growth'.
Discussion
This case illustrates nearly all the featuresgenerally attributed to a benign localised intra-thoracic fibroma. Macroscopically, the tumoursare well encapsulated and lobulated. Some areembedded in the lung or mediastinum; others maybe pedunculated, and attached to some part of thepleura-visceral, parietal, or mediastinal. As inthe present case the cut surface may show awhitish and whorled appearance.
Microscopically, the tumours are composed ofcollagen-forming fibroblasts. The same tumourmay show in different parts a varying degree ofcellularity and collagen formation. Metaplasticchange-myxomatous, chondromatous, or lipo-
521
on January 4, 2020 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.33.4.520 on 1 August 1978. D
ownloaded from

522 DCNwaifoandFCAdi
xCA,~ ~ 4 -"
.4 4'~~~~~~~~~~~~~~~~~~~~8
... ......$4...4*
Nt~~~~~~~~~ L 4\~~~~~~~~~~~.
eosiX10)
si.~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~. .....
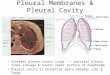
Fig. 4 High power view showing cells with some nuclear pleomorphism floating in myxomatousstroma (H & E X360).
on January 4, 2020 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.33.4.520 on 1 August 1978. D
ownloaded from

Giant fibromyxoma of the parietal pleura
matous-is common. Calcification, though notnoted here, may occur.
Clinically, intrathoracic fibromas may growsilently for a long time and are not infrequentlyrecognised on routine chest radiography. In thepresent patient distressing symptoms appearedfor the first time five months before admission,although the tumour had been present for at leastfour years-when the patient first observed short-ness of breath and peripheral oedema.Sometimes finger clubbing and the joint pains
of hypertrophic pulmonary osteoarthropathy arethe presenting symptoms (Clagett et al., 1952;Thomas and Drew, 1953). Respiratory symptoms,notably shortness of breath, may as in this patientarise from the bulky tumour interfering with pul-monary expansion or causing mediastinal dis-placement. The peripheral oedema noted in thispatient as well as the hepatosplenomegaly disap-peared after removal of the tumour, and theyprobably resulted from impaired venous returncaused by the bulky tumour.
Episodes of chills and fever may occur (Ehren-haft etal., 1960)-a notable feature in this patient.Rarely the patient may present with recurrentpleural effusion as in the cases reported byEhrenhaft et al. (1960) and by Aghina andBoscaino (1956). The latter patient had had arecurrent pleural effusion for six years.Haemorrhagic effusions may occur, as in our
patient. He had had no previous chest aspiration,and as the pleural fluid contained altered ratherthan fresh blood, it seems unlikely that thehaemorrhage was due to needling. A haemor-rhagic effusion signifies neither inoperability noran unfavourable prognosis (Clagett et al., 1952;Heaney et al., 1957). It is also unusual to recovermalignant cells from such effusions. While thereare no diagnostic radiographic appearances, anearly 'dry tap' in the presence of a massive'pleural effusion' especially if the aspiratingneedle encounters a solid resistance, suggests asolid intrapleural tumour. We had previously ob-served this in a patient who was moribund onadmission with 'a massive pleural effusion' whichwas found at necropsy to be a solid intrapleuralfibroma. The same finding led to a correct pre-operative diagnosis in the present patient.
Despite the piecemeal removal of the tumourin our patient, excision was probably complete
523
since the tumour was sharply circumscribed. Thisview is supported by the histological absence oftumour tissue in the adjacent pleura. A longerfollow-up is needed to obtain a reasonable idea ofthe prognosis. However, many rural Nigerianshave to travel long distances to hospital and seelittle point in attending for follow-up except fordistressing symptoms. Our patient has so farattended regularly-and remained clinically andradiologically symptom-free. As Stout and Himadi(1951) pointed out 'the pleomorphism, frequentmitosis, and other histological criteria associatedwith malignancy do not appear to affect the goodprognosis of most patients'.
References
Aghina, A., and Boscaino, N. (1956). Fibromixomadella pleura parietale. Riforma Medica, 70, 147-150.
Clagett, 0. T., McDonald, J. B., and Schmidt, H. W.(1952). Localised fibrous mesothelioma of thepleura. Journal of Thoracic Surgery, 24, 213-230.
Dolley, F. S., and Brewer, L. A. (1943). The diagnosisand treatment of primary intrathoracic tumours.Journal of the American Medical Association, 121,1130-1136.
Ehrenhaft, J. L., Sensenig, D. M., and Lawrence,M. S. (1960). Mesotheliomas of the pleura. Journalof Thoracic and Cardiovascular Surgery, 40, 393-409.
Heany, J. P., Overton, R. C., and De Bakey, M. E.(1957). Benign localised pleural mesothelioma.Journal of Thoracic Surgery, 34, 553-560.
Kerr, W. F., and Nohl, H. C. (1961). Recurrence of'benign' intrathoracic fibromas. Thorax, 16, 180-189.
Klemperer, P., and Rabin, C. B. (1931). Primaryneoplasms of the pleura. Archives of Pathology, 11,385-412.
Stout, A. P., and Himadi, G. M. (1951). Solitary(localised) mesothelioma of the pleura. Annals ofSurgery, 133, 50-64.
Thomas, C. P., and Drew, C. E. (1953). Fibroma ofvisceral pleural. Thorax, 8, 180-188.
Willis, R. A. (1953). Pathology of Tumours, 2ndedition. Butterworth, London.
Requests for reprints to: D. C. Nwafo, FRCS,Cardiothoracic Surgical Unit, University of Nigeria,Enugu, Nigeria.
on January 4, 2020 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.33.4.520 on 1 August 1978. D
ownloaded from