-
7/30/2019 Gib in Infancy and Childhood
1/28
Intestinal bleeding in the
child
SURGICAL ASPECTS
Dr EW Muller
Block 8
2013
-
7/30/2019 Gib in Infancy and Childhood
2/28
Definition - UpperGIB (UGIB)
Bleeding proximal tothe ligament of
Treitz Source:
Oesophagus
Stomach
DuodenumLigament ofTreitz
-
7/30/2019 Gib in Infancy and Childhood
3/28
Bleeding is located distal to ligament of
Treitz Source: - Small bowel
- Colon
- Rectum
Definition - Lower GIB (LGIB)
-
7/30/2019 Gib in Infancy and Childhood
4/28
Relevant history in a bleeding child
Vomiting, diarrhoea, fever: Infectious cause
Recurrent forceful vomiting: Mallory - Weiss
Drugs: NSAIDS, tetracyclines, caustics or foreign
bodies: Damage of gastric mucosa
Jaundice, bruising, change in stool color: Liverdisease
Drugs and foods which might imitate bloodystools: Certain
antibiotics, iron supplements,bismuth containing products
-
7/30/2019 Gib in Infancy and Childhood
5/28
Physical examination
Look for signs of shock: Heart rate, BP, capillaryrefill
Rule out epistaxis, nasal polyps, oropharyngeal
erosions or the lung as the source of bleeding Abdominal scars:
What was reason for surgery?
Bowel sounds: Often hyperactive in upper GI
bleeding Abdominal tenderness: Intussusception,
Ischemia, Ulcer, Gastro-oesophageal reflux
-
7/30/2019 Gib in Infancy and Childhood
6/28
Physical examination
Hepatomegaly, splenomegaly, jaundice:Liver disease and portal
hypertension
Inspection of the anal area: Fissures,fistulas, skin breakdown,
trauma
Digital rectal examination: Polyps, masses
-
7/30/2019 Gib in Infancy and Childhood
7/28
Haematemesis Red blood + clots: ongoing bleeding Dark
coffee-ground (denatured blood) vomitus:
Slow bleeding or bleeding has stopped No haematemesis if source
of bleeding is in distal
duodenum
Melaena (= tarry black stools) passed
per rectum Melaena = Altered blood (oxidized haemoglobin)
after prolonged passage(>14 hours) throughbowel
CLINIC - UGIB
-
7/30/2019 Gib in Infancy and Childhood
8/28
CLINIC - LGIB
Haematochezia: Passage of bright redrectal blood on top or in
stool: Source: Usually distal bowel, but:
Severe haemorrhage from oesophagus,stomach or duodenum can also
causehaematochezia
Rectorrhagia: Passage of rectal blood,without stool: Source:
rectum, anus
-
7/30/2019 Gib in Infancy and Childhood
9/28
RESUSCITATION
Assess the Location, high or low - Place NGT:Aspiration of
blood: UGIB. Aspiration of bile withoutblood rules out UGIB.
Assess severity: Shock, haematemesis, ongoing
drainage of blood from NGT or rectum. Oxygen mask 2 good
peripheral lines; Ringers lactate bolus
20ml/kg If bleeding continues: Blood 10 15 ml/kg; give
somatostatin analogue Urgent referral for therapeutic
gastroscopy (UGIB) or
colonoscopy (LGIB), but Patient should be stabilisedfor
transport
-
7/30/2019 Gib in Infancy and Childhood
10/28
COMMON CAUSES OF GIB INCHILDHOOD
Age Group UGIB LGIB
Neonates Haemorrhagic disease ofthe Newborn (Vit K)
Swallowed maternal blood
Stress Gastritis (ICU set up)
Necrotizing Enterocolitis(immature infants)
Anal fissure
Malrotation with volvulus
Infants 1month to1 year
Oesophagitis (Reflux)
Stress Gastritis
Anal fissure
Intussusception
Milk protein allergy
Infants 1 2years
Peptic Ulcer disease (HP -or non HP - related)
Gastritis
PolypsMeckel Diverticulum
Children olderthan 2 years
Oesophageal varices
Peptic Ulcer disease
Polyps
Inflammatory bowel disease
Infectious diarrhoea
-
7/30/2019 Gib in Infancy and Childhood
11/28
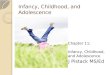
Necrotizing Enterocolitis (NEC)
Occurs in premature brittle newborns Aetiology: Bowel wall
bacterial infection due to
immature mucosal barrier Immunoglobulins in breast milk protect
against
NEC - Formula fed newborns are at risk Clinic: Sudden feeding
intolerance in premature
baby: Abdominal distension, vomiting, sepsis,acidosis, shock
Diagnosis: Pneumatosis intestinalis on AXR Treatment: NPO,
Antibiotics, parenteral feeds. If
necrotic bowel or perforation: Operation
-
7/30/2019 Gib in Infancy and Childhood
12/28
-
7/30/2019 Gib in Infancy and Childhood
13/28
Anal fissure
History of painful passage of bright red
blood which is not mixed with stool Baby usually in good
condition
Sometimes associated with constipation
Rectal examination: Small very painfulanal tear visible, +/-
hard stool
Treatment: Stool softeners, wait and see
-
7/30/2019 Gib in Infancy and Childhood
14/28
Polyps in Children
2 types: Hamartomas (common) and adenomas (rare)
Present with painless red bleeding or can protrudethrough
anus
Usually in distal colon
Hamartomas: Sporadic, single: with no malignantpotential; also
called hyperplastic polyps
Adenomas associated with familial polyposis syndrome,
high cancer risk: Colectomy in early adolescencerequired
-
7/30/2019 Gib in Infancy and Childhood
15/28
Familial adenomatous polyposis coli
-
7/30/2019 Gib in Infancy and Childhood
16/28
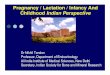
Meckels Diverticulum
Embryology: Remnant of omphalo-mesenteric duct
-
7/30/2019 Gib in Infancy and Childhood
17/28
MeckelsDiverticulum
Located in terminal
ileum, 60 70 cm
proximal to ileocolic
juntion
-
7/30/2019 Gib in Infancy and Childhood
18/28
Meckels Diverticulum
Complications associated withectopic gastric tissue:
Ulceration, perforation, bowel
obstruction Bleeding (most common
complication): usually painless, can be
massive, transfusion often necessary
Treatment: Must be surgically excised
-
7/30/2019 Gib in Infancy and Childhood
19/28
Meckels Diverticulum: Diagnosis
Technetium Scan
-
7/30/2019 Gib in Infancy and Childhood
20/28
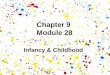
Intussusception
Condition where the proximal bowel moves into
the distal bowel like an inverted sock
Proximal bowel = Intussusceptum
Distal bowel = Intussuscipiens
Intussusception can be ileo-ileal, ileo-colonic (by
far the most common presentation) or colo-
colonic The intussusceptum might even protrude
through the anus mimicking a rectal prolapse
-
7/30/2019 Gib in Infancy and Childhood
21/28
-
7/30/2019 Gib in Infancy and Childhood
22/28
Intussusception: Pathophysiology
Caused by lead point which is pulled into thelumen by
peristalsis
Age group 5 9 months: lead point caused by
enlarged bowel lymphoid tissue (Peyersplaques) following viral
infection: this is by farthe most common reason for
intussusception
Older age group: Lead point might be Meckels
diverticulum, polyps, lymphoma, worms or otherforeign bodies
-
7/30/2019 Gib in Infancy and Childhood
23/28
-
7/30/2019 Gib in Infancy and Childhood
24/28
Intussusception: symptoms
Well fed baby who might have a history of
recent upper respiratory tract infection or
gastro-enteritis
Bloody, slimy stool (red currant jelly stool)
Signs of bowel obstruction (vomiting,
abdominal distension)
-
7/30/2019 Gib in Infancy and Childhood
25/28
Intussusception: Signs
The child might be dehydrated
Abdominal tenderness
A sausage-shaped mass can often bepalpated in the region of the
colon
-
7/30/2019 Gib in Infancy and Childhood
26/28
Intussusception: Special
investigations
Biochemistry: Electrolyte disturbances and
high urea in case of dehydration due to
vomiting
AXR: Multiple air fluid levels indicating
bowel obstruction. Mass effect in the
region of the colon. No air in colon. Free
air if perforation
Sonar: Imaging of choice: Mass visible
-
7/30/2019 Gib in Infancy and Childhood
27/28
-
7/30/2019 Gib in Infancy and Childhood
28/28
Intussusception: Management
Nil per os, nasogastric tube, iv fluids (rehydrationand
maintenance)
Pneumatic reduction should be attempted if Child fully
resuscitated
Abdomen without peritonitis No free air on AXR
Laparatomy If pneumatic reduction is contraindicated
If pneumatic reduction has failed Intraoperatively: Trial of
manual reduction. If this
maneuver fails: Resection of intussusception andprimary
anastomosis.