Embed Size (px)
Citation preview

109
Hearing Disorders andAudiogram Interpretation
As someone new to conducting hearingtests, you might find the process of uncov-ering various types of hearing disorderssomewhat mysterious. You might even thinkthat interpreting your first audiograms islike trying to uncover one of the greatunsolved mysteries of the world. Althoughsome of the hearing disorders we reviewmight seem a little mysterious to you rightnow we seriously doubt that you’ll get lostin the Bermuda Triangle or get carried offby Bigfoot.
We’ve already solved a couple of theworld’s mysteries—after the previouschapter you have a good workingknowledge of the normal auditory sys-tem and how to measure its function,let’s turn our attention to various dis-orders than can affect it. The primarypurpose of this chapter is to provideyou with a basic understanding ofhearing disorders, characteristics of thehearing loss, and, most importantly, theaudiometric configuration that is most
closely associated to the disorder. Thegoal is not for you to memorize everypossible disorder, along with the audio-metric pattern, but when you are fin-ished reading this chapter you shouldhave a better understanding of how theresults of the hearing test relate to thediagnosis of some common hearingdisorders.The first thing you need to know
about hearing disorders is that it is crit-ical to have a good understanding ofwhen to refer a patient to a physicianfor a medical evaluation. In fact, beforeyou even begin to discuss hearing aidswith a patient it is imperative that youhave ruled out a treatable medical prob-lem involving the auditory system.This means that you have to recognizewhat a hearing disorder looks like onan audiogram. Before reviewing thevarious types of hearing disorders, let’sdiscuss the difference between a symp-tom and an etiology.
There are many great unsolved mysteries of theworld. Maybe we can solve some of them in thischapter!

Symptoms Versus Etiology
Understanding the difference betweena symptom and an etiology is important.When someone walks through your doorfor a hearing test, they may be experi-encing several symptoms related to anynumber of possible hearing disorders.
� A symptom is a description by thepatient of what they are feeling, oran observation you make (e.g., dizzi-ness, pain, etc.).
� An etiology is the under lying causefor the disorder. It is only throughan accurate hearing test, whichmay lead to a diagnosis by a physi-cian, that you may know the causeor etiology.
In some cases the etiology is neverknown. It is common to conduct med-ical tests to “rule out” pathologies thatrequire further medical attention. A per-son with an unexplained unilateralloss, for example, may have an MRI torule out a space occupying lesion. Oncethe MRI shows there is no obviouspathology, the patient is cleared for the fitting of a hearing aid, although thetrue cause for the hearing loss stillremains unknown.With accurate audiometry you often
will be able to quantify the extent of theear problem. In most cases, regardless ofthe etiology, once a treatable medicalproblem involving the ear has beenruled out, you will fit the patient withhearing aids.Typically, the hearing disorders you
will encounter will involve the innerear. Not only are they much more com-mon, but disorders of the cochlea usu-
ally require the use of hearing aids aspart of the treatment process, and forthe most part, hearing aids are the onlytreatment.
Case History
Before completing any diagnosticaudiometry, it is important to carefullycomplete a case history. The case his-tory should always be completed face-to-face with the patient, rather thanhaving the patient complete a case his-tory checklist or questionnaire in thewaiting room. During the taking of thecase history, your job is to find out if thepatient has recently experienced any ofthe common symptoms listed below.Given that these symptoms occasionallyare an indication of a more threateningmedical problem, they are important toknow and understand.
Common Symptoms
The symptoms listed below are onesyou will frequently encounter, and areused by physicians and audiologists ona regular basis.
Tinnitus
This is the perceived sensation of earnoise, often described as a ringing orbuzzing in the ear. It is not a disorder,just the sensation to hear sounds gen-erated by the auditory system. Tinni-tus, however, is often associated withhearing loss and hearing disorders. Forexample, most people with noise-
110 UNDERSTANDING HEARING AIDS: GETTING STARTED

induced hearing loss have tinnitus. Inthis case, there is no medical treatment.On the other hand, someone with anacoustic nerve neuroma also may havetinnitus and, in this case, a medicalworkup is critical. Tinnitus can be anoccasional occurrence, or it can be con-stant. Tinnitus is actually more com-mon than hearing loss, as it believedthat over 50 million Americans experi-ence tinnitus to some degree. In caseyou’re wondering, tinnitus can be pro-nounced either as ti-NIGHT-us or TIN-i-tus; the latter is preferred by mostprofessionals.
Vertigo and Dizziness
True vertigo is a severe spinning sen -sation usually of short duration. It canbe spontaneous, or associated with headmovement. The patient can have the sen-sation the patient of spinning themselvesor that the room is spinning aroundthem. There are almost as many causesof dizziness as there are ways in whichpatients describe it. Recall from Chap-ter 3, that the balance and auditory sys-tem are located in the inner ear. There-fore, it is fairly common to encounterpatients with hearing loss (especially ifit is of relatively of sudden onset) whoare also experiencing vertigo.
Otalgia
Simply put, this is ear pain, sometimescalled an “earache.” Otalgia is notalways associated with hearing disor-ders, as it can be caused by conditionssuch as impacted teeth, sinus disease,and inflamed tonsils. If directly relatedto the ear, it may be due to middle orouter ear pathology. It’s common for
there to be a generalization of pain.That is, the external ear could bepainful resulting from an ear canalproblem.
Aural Fullness
The perceived sensation of a pluggedear that often accompanies vertigo andsudden hearing loss. Aural fullness canalso be a symptom of a problem involv-ing the middle ear, often related to pooreustachian tube function.
Hyperacusis
An abnormal sensitivity to sound.Hyperacusis is an internal oveamplifi-cation of environmental sounds by theauditory system. Environmental soundsof ordinary intensity that do not bothermost people, really bother those suffer-ing from hyperacusis—e.g., a sound of 65 dB SPL might be perceived like a100 dB SPL input. This is different frompeople who simply are “bothered” byloud noise.
TAKE FIVE:Medical Terminology
This chapter introduces you tomany of the common terms usedto describe hearing disorders andtheir symptoms. If you receivereferrals from physicians and othermedical professionals you are likelyto encounter terms you don’t know.One way to find out about themquickly is to use an on-linemedical dictionary. One exampleis http://www.medterms.com.
HEARING DISORDERS AND AUDIOGRAM INTERPRETATION 111

112 UNDERSTANDING HEARING AIDS: GETTING STARTED
TIPS and TRICKS: Cochlear Hearing Loss, Loudness, and Recruitment
As mentioned a number of timesalready, the majority of your patientswill be individuals with cochlear hearingloss. This population is uniqueregarding their loudness growthpattern; because of their hearing lossthey need a loudness boost for softsounds, but because of the way thecochlea works (see Chapter 3) theydo not need a loudness boost forloud sounds. Their loudness percep-tions for loud sounds are very similarto someone with normal hearing. Inother words, their floor has beenraised, but the ceiling has remainedin the same. As a result, there is arapid growth of loudness betweenthe point of audibility and the point ofdiscomfort. This abnormal growth ofloudness often has been referred toas recruitment. Recruitment isperhaps the most common, and mostcommonly talked about, yet mostmisunderstood, symptom of cochlear
hearing loss. It is a normal nonpatho-logical phenomenon associated witha damaged cochlea.
Sample Case: Your Mondaymorning patient has a 60 dB hearingloss, but when you did LDL testing,you found that he found thingsuncomfortably loud at 100 dB, thesame point as many people withnormal hearing, a dynamic range ofonly 40 dB. Does he have recruit-ment? Yes. Does he have “a lot ofrecruitment”? Well, if there were sucha thing, maybe yes. Is this somethingto be concerned about? No. It is theexpected finding. What is somethingto be concerned about is the patientwith a 60 dB hearing loss whodoesn’t have recruitment. That wouldmean that the hearing loss is prob-ably caused by a middle ear, eighthnerve, or brainstem pathology, andthe patient should be referred formedical evaluation.
TIPS and TRICKS: More on Tinnitus
Tinnitus is a condition that still is notcompletely understood. In fact,experts are still not in completeagreement the underlying causes oftinnitus and hyperacusis. To compli-cate matters, there is a wide range oftreatment options for each that gowell beyond the scope of this book.To learn more about the etiology oftinnitus, along with some of the treat-ment options supported by research
evidence, here are a couple of usefulWeb sites.
http://www.tinnitus.org—A BritishWeb site devoted to a specific type oftinnitus therapy called TinnitusRetraining Therapy (TRT)
http://www.ata.org—Sponsored bythe American Tinnitus Association, itcontains plenty of information forprofessionals and consumers.

Common Hearing Disorders
A close encounter is an event in which aperson witnesses an unidentified flyingobject or makes contact with an alien.According to ufologist (yes, that’s a realword) J. Allen Hynek, there are four types of close encounters. Close encounters of thefirst and second kind are sightings ofunidentified flying objects, whereas closeencounters of the third and fourth typeinvolve contact and even abduction by analien. In a clinic the only type of encounteryou are likely to find is one is which youcould uncover a hearing disorder.
The following is a summary of some ofthe most common hearing disordersyou will “encounter” in your dailypractice—and some probably will be amystery. The list is categorized by partsof the ear, and is not an exhaustive list.It is simply a summary of some of themost common conditions, their causes,and audiometric patterns. To makethings fairly straightforward, we haveorganized the disorders as they relateto parts of the ear. Thanks to the WorldWide Web, you can find many moreexamples of hearing disorders that we did not cover here. Among the Web sites devoted to hearing disordersare http:// www.merck .com.mmpe andhttp:// emedicine.med scape.com/ otolaryngology
Hearing Disorders of theOuter Ear
Most disorders of the outer ear are easyto observe, respond to treatment, andusually do not cause significant hear-ing loss. We review five of the mostcommon in this section.
Collapsing Ear Canal
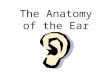
Recall that we discussed the advantagesof using insert earphones in Chapter 4;let’s talk about an important reason forusing them in a little more detail. Somepeople, especially the elderly, have earcanals that are collapsing. This meansthat the tissues lining the ear canal havebecome very soft. This is a normal con-dition and does not cause hearing lossin the vast majority of cases, becausesound only needs a small opening topass through. But for patients with thisproblem, this could change when you doa hearing test. When you place supra-aural headphones on someone with col-lapsing ear canals, it’s possible that thepressurewill totallycollapse theearcanal,and you are actually causing a hearingloss. It is as though the patient is wearingan earplug. This condition results in anaudiogram that has the appearance of aconductive hearing loss (usually greatestloss in the higher frequencies, as they arethe easiest to attenuate). This easily canbe prevented, however, by using insertearphones. Figure 5–1 gives an exampleof an audiogram of a patient with col-lapsing ear canals. The audiogram onthe right is after the use of insert phones.Note how the loss returns to near nor-mal levels (e.g., “correct” values) whenthe appropriate earphones are used.Failure to recognize collapsing canals,
and the resulting erroneous assump-tion that there is a conductive hearingloss present, is a good way to lose cred-ibility the physicians that you refer to,as their physical examination clearlywill be normal. Of course, if your scopeof practice includes the use of immit-tance audiometry, these results willquickly alert you that the measured air-bone gap is erroneous.
HEARING DISORDERS AND AUDIOGRAM INTERPRETATION 113

Impacted Cerumen
Cerumen (or ear wax) is a normalbyproduct of a healthy ear. It lubricatesthe ear canal and protects the canal andtympanic membrane. As cerumen isproduced by the subcutaneous glandsof the ear canal, it migrates out of the ear canal by way of the tiny hairslining the outer layer of the external ear canal.Some people produce more cerumen
than others, especially the elderly. Addi-tionally, other people may disturb thenatural cerumen excretion process byinserting Q-tips and other foreign ob -jects into their ear canal, attempting to remove the cerumen. These objectsoften irritate the canal, which thenresults in increased cerumen production,which then results in more probing bythe individual, not a good thing. Addi-
tionally, using foreign objects to attemptto remove cerumen can result in animpaction, a total blockage of an area ofthe ear canal. For individuals who produce exces-
sive cerumen, impaction sometimesalso occurs because of hearing aid use.That is, the hearing aid (in the case of acustom instrument) or the earmold atthe time of each insertion continues topush the cerumen to a given point(usually about 10 to 15 mm from the earcanal opening) and, eventually, a total(or near total)blockage will occur.Impacted cerumen results in a tempo-
rary conductive hearing loss of varyingdegree (in severe cases, an air-bone gapas large as 30 to 40 dB will be present).Once the cerumen is removed by a qual-ified professional, hearing returns to pre-impact levels. A good otoscopic exam-ination will reveal if impacted cerumen
114 UNDERSTANDING HEARING AIDS: GETTING STARTED
Figure 5–1. The effects of a collapsing ear canal. The audiogram on the left showsa mild conductive loss when traditional earphones are used. The audiogram on theright shows how air conduction thresholds return to normal levels for the same earwhen an insert earphone is used. High frequency conductive losses are rare, soalways consider collapsed canals when this pattern is present; the routine use ofinsert earphones of course will mostly eliminate the problem from the onset.

exists. If you observe this, you may wantto have the cerumen removed beforeconducting the hearing test, as there islittle reason to conduct a test when youknow a priori that the results do notrepresent the patient’s “true” hearing.
External Otitis
Otitis externa is an inflammation of the outer ear and ear canal. Along withotitis media, which we address short-ly, external otitis is one of two condi-tions commonly referred to as an “ear-ache.” One common name for thiscondition is “swimmer’s ear” becauseit frequently develops in people whohave been swimming and have hadwater trapped in their ears. External otitis is an extremely painful
condition requiring treatment from aphysician. Hearing tests often cannotbe conducted on patients with external
TIPS and TRICKS: Cerumen Management
Some audiologists and a fewhearing instrument specialistshave specialized training in theremoval of cerumen from the earcanal. Known as cerumenmanagement, your ability toconduct this service should onlyhappen after you have checkedwith your state licensing board tosee if you can offer it, and hadadditional training on it.
To find locations wherecerumen management coursesare offered check with theInternational Hearing Society oryour state licensing board.
otitis because the ear is too painful toallow for the placement of earphones.Acute external otitis often occurs
suddenly, rapidly worsens, and becomesextremely painful. Because the tissueslining the external ear canal are ex -tremely thin they are easily torn orabraded by minimal force. Inflamma-tion of the ear canal can begin whensomeone tries to self-clean their earcanal with a cotton swab or other smallimplement. Another cause of externalotitis is prolonged exposure to water orextreme humidity. Regardless of thecause, external otitis occurs when activebacteria or fungus begin to infect theskin of the ear canal.
Some hearing care professionalshave been specially trained to removecerumen from the ear canal. Due to thethinness of the tissues of ear canals it iseasy to abrade them, thus causing in-flammation and possibly external otitisin some patients.Pain that worsens on touching of the
outer ear is the predominant complaintassociated with external otitis. Patientsmay also experience discharge from theear canal and itchiness. Swelling of
TIPS and TRICKS: ExternalOtitis and Hearing Loss
In general, we would not expectexternal otitis to cause a hearingloss. If the swelling was such thatthere was complete closure of theear canal, then a mild conductiveloss would be expected (probablygreatest in the higher frequencies).In general, however, expect normalhearing with this pathology.
HEARING DISORDERS AND AUDIOGRAM INTERPRETATION 115

the ear canal is another symptom andwhen the swelling is severe enough aconductive hearing loss may occur. Inadvanced cases of external otitis, painmay radiate to the jaw and neck.Because the ear is a self-cleaning sys-
tem, milder cases of this condition canbe addressed by simply refraining fromswimming or not using implements to try and clear wax from the ear canal.Topical solutions or suspensions in theform of ear drops typically are used totreat mild and moderate cases of otitisexterna. In more advanced cases aphysician may have to use a binocularmicroscope to clean the ear canal andinsert what is called an ear wick todeliver medication to the infected area.Because external otitis is so commonand can be caused by the actions ofeven the most experienced hearing careprofessional during cerumen removalprocedures, it’s important to know thecommon symptoms and to immediatelyrefer your patient to a physician for anevaluation if you suspect it.
Tumors of the External Ear Canal
Both malignant and benign tumors havebeen found in the external ear canal.Bony tumors, called osteomas, are some-times seen in the ears of people whohave done a lot of swimming in coldwater. You may not observe a tumorper se, but rather just a narrowing ofthe canal. Unless the bony growth ortumor closes off the entire external earcanal, they do not cause hearing loss. Ade tailed otoscopic exam should revealthis, and, unless this is a long-standingcondition reported by the patient, aphysician referral is appropriate.
Perforated Tympanic Membrane
There are several ways the tympanicmembrane (TM) can become perforated.A perforated eardrum is a rupture orperforation (hole) of the eardrum thatcan occur as a result of infection, trauma(e.g., by trying to clean the ear withsharp instruments, or even a Q-Tip),explosion, barotrauma, or surgery(accidental creation of a rupture).Because traumatic perforations often
alter otherwise normal tissue, theyoften heal spontaneously. One commoncause of TM perforations is related tothe buildup of excessive pressure in themiddle ear as a result of a middle eardisorder (e.g., eustachian tube dysfunc-tion, infection, effusion, etc.). In thesecases, the excess pressure causes the TMto rupture. Because of the underlyingmiddle ear disorder, TM perforationscaused from this excessive pressureneed to be managed medically. Surgical repair of a perforated TM is
called myringoplasty or tympano plasty.In some cases, the “surgical patching”procedures are not successful, and thepatient more or less will have a “per-manent” perforation. Those with moresevere and long-standing ruptures mayneed to wear an earplug to avoid water(or other liquids) making contact withthe eardrum, and entering the middleear cavity.Perforation of the eardrum usually
leads to conductive hearing loss. Theamount of hearing loss caused by a per-forated TM varies by both the size ofthe perforation and the location of theopening. Some perforations can be sosmall that they cannot be detected dur-ing routine otoscopy. With large perfo-rations, it’s common to see a conduc-tive hearing loss of 30 to 40 dB. Once
116 UNDERSTANDING HEARING AIDS: GETTING STARTED

the perforation heals, hearing is usuallyrecovered fully (maybe with a slight 5-to 10-dB drop due to scarring), butchronic infection over a long periodmay lead to permanent hearing loss, asthe structure of the TM is altered.
Disorders of the Middle Ear
The Bermuda Triangle is a region in thewestern part of the North Atlantic Oceanwhere a number of aircraft and surfacevessels allegedly disappeared mysteriously.Popular culture has attributed these disap-pearances to the paranormal or activity byextraterrestrial beings. Documented evidenceindicates that a significant percentage of theincidents were inaccurately reported orembellished by later authors, and numerousofficial agencies have stated that the numberand nature of disappearances in the regionis similar to that in any other area of ocean.You can think of middle ear disorders likereports of lost vessels in the BermudaTriangle. On the surface the disorder mightbe unexplainable, but on further testingusing tympanometry and acoustic reflexes,the disorder is no longer mysterious.
Recall that the purpose of the middleear is to transmit the airborne soundfrom the eardrum to the cochlea. This isaccomplished quite effectively throughthe aerial ratio of the TM compared tothe oval window, the through the leveraction of the ossicular chain. As youwould expect, anything that disruptsthis flow will cause a middle ear (con-ductive) hearing loss. We’ll describesome of the most common.
Otosclerosis
Otosclerosis is caused by two mainsites of involvement of the sclerotic (or
scarlike) lesions. The best understoodmechanism is fixation of the stapesfootplate to the oval window of thecochlea. This greatly impairs move-ment of the stapes and therefore trans-mission of sound into the inner ear(“ossicular coupling”). Additionally, the cochlea’s round
window can also become sclerotic, andin a similar way impair movement ofsound pressure waves through the innerear (“acoustic coupling”). There is somedocumentation of sclerotic lesions thatalso are within the cochlea, sometimesreferred to as “cochlear otosclerosis.”Treatment of otosclerosis often in -
volves a surgical procedure called astapedectomy. A stapedectomy consistsof removing a portion of the scleroticstapes footplate and replacing it with animplant that is secured to the incus. Thisprocedure restores continuity of ossicu-lar movement and allows transmissionof sound waves from the eardrum to theinner ear. A modern variant of this sur-gery called a stapedotomy, is performedby drilling a small hole in the stapes foot-plate with a microdrill or a laser, andthe insertion of a pistonlike prosthesis.Otosclerosis can be hereditary, and
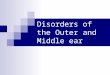
at least in the early stages, results in aconductive hearing loss of mild tomoderate-severe degree, usually withthe greatest loss in the lower frequen-cies. In the later stages, a mixed hear-ing loss may be present. Figure 5–2gives an example of oto sclerosis youmight see in your office or on an audio-gram. While this patient certainly is aheraring aid candidate, and probablywould be a successful user of hearingaids, most opt for surgical treatment.Typically, following surgery there is asignificant improvement in air conduc-tion thresholds.
HEARING DISORDERS AND AUDIOGRAM INTERPRETATION 117

Negative Middle Ear Pressureand Middle Ear Effusion
As mentioned in Chapter 3, theeustachian tube equalizes the pressurebetween the air filled middle ear andoutside air pressure. This tube is nor-mally closed, but when healthy, opensfrequently when we talk, chew, yawn,and so forth. When the eustachian tubebecomes blocked or swollen from an
TIPS and TRICKS:Carhart’s Notch
An audiometric characteristic ofotosclerosis is something called“Carhart’s notch.” This is anapparent bone conduction loss at2000 Hz, named after the personwho first described it, audiologistRaymond Carhart, Ph.D. Thisfinding is not a true sensorineuralloss, and usually disappearsfollowing surgery.
allergy or common cold, the air pres-sure outside the middle ear is greaterthan the air pressure within the middleear space. Children are more prone tonegative middle ear pressure and effu-sion, because the eustachian tube hasnot had the opportunity to grow to theproper angle (~45 degrees) and is muchmore horizontal.Eustachian tube dysfunction causes
the air trapped inside the middle ear tobecome absorbed by the tissues liningthe middle ear space, resulting in adrop in pressure within the middle earspace. The greater pressure from theoutside air causes the tympanic mem-brane to become retracted or pushedinto the middle ear space. This condi-tion can be observed with otoscopy,although sometimes it is quite subtle.A specific audiologic test battery
called immittance audiometry is usedto mea sure the function of the entiremiddle ear system. Tympanometry,which is part of this battery, easily willreveal a retracted TM, or a middle earsystem that is not moving effectively.
118 UNDERSTANDING HEARING AIDS: GETTING STARTED
Figure 5–2. A bilateral conductive hearing loss consistent with bilateral otosclero-sis. Notice the 2000 Hz or “Carhart” notch in the bone conduction scores in both ears.

If negative middle ear pressure con-tinues to develop, and is present for an extended time, the fluids normallysecreted by the mucous membranes arecollected in the middle ear cavity, result-ing in a condition called serous effusionor middle ear effusion. When fluid par-tially fills the middle ear space a mildto moderate conductive hearing loss canoccur. Often, when a young child hasfluid in their middle ears, it is referredto by the lay person (e.g., parents) as an“ear infection.” Middle ear effusion,however, is not necessarily infectious.The audiogram for this patient is
directly related to the amount of retrac-tion and/or the amount of fluid in themiddle ear. If the patient only has aretracted TM, there probably will be lit-tle effect on hearing thresholds. If fluidbegins to collect, expect thresholds,especially in the low frequencies, todrop accordingly.
Otitis Media
If middle ear effusion is allowed to con-tinue unabated, otitis media candevelop. Otitis media is any infectionof the mucous-membrane lining of themiddle ear space. Although otitis
media is thought of as a disease ofchildhood, it can occur at any age, andcan be quite painful. When these tis-sues become infected they becomeswollen, interfering with its pressureequalization function. During this pro -cess, the tympanic membrane becomesvery vascular, re sulting in the TM’s redappearance. There are two types of otitis media,
called chronic and acute. As you mightimagine, acute otitis media has a veryrapid onset time, whereas chronic con-ditions of otitis media are long-stand-ing. In some cases the fluid in the mid-dle ear becomes thick and sticky and,hence, the nonmedical term “glue ear”sometimes has been used to describethe condition. Like many pathologics ofthe middle ear, the audiogram will varywith the severity of the problem. It’s rea-sonable to expect a conductive hearingloss of 20 to 30 dB or worse. The config-uration might be similar to that shown inFigure 5–2. In severe cases, air-bornegaps of 30 dB or greater are common.Antibiotics are used in the treatment
of otitis media. If otitis media persists,however, pressure equalization (PE)tubes are inserted into the TM by an oto-laryngologist. This procedure is calledmyringotomy with PE tubes. These
HEARING DISORDERS AND AUDIOGRAM INTERPRETATION 119
TAKE FIVE: Valsalva and Toynbee
Patients with eustachian tubedysfunction may be asked by theirphysician to autoinflate theireustachian tube by attempting toforce air into the middle ear spacewhile holding their nostrils shut (Theyactually are instructed to try to blowair out of their nose, while holdingtheir nose shut). This is called the
Valsalva maneuver, which wediscussed in Chapter 3. Divers usethe Valsalva procedure to equalizepressure as they descend or surface.In a related procedure, called theToynbee maneuver, the patientattempts to open the eustachian tubeby holding his or her nose and swal-lowing (e.g., taking sips of water).

tubes are also referred to as grommetsor tympanostomy tubes. If the tubes areopen during audiometric testing (theysometimes become plugged), you wouldexpect to see relatively normal hearingIf you conduct immittance testing, vol-ume measures will quickly indicate ifthe tube is open or closed.
Cholesteatoma
In general, cholesteatomas are the resultof a long-standing middle ear condi-tion. Cholesteatomas form a sac withconcentric rings consisting of a proteincalled keratin; there is some evidence toclassify them as low-grade tumors. Inpatients with TM perforations, the tis-sue may enter the middle ear throughthe perforation, producing a choles -teatoma. Cholesteatomas may also becaused by chronic episodes of otitis
TIPS and TRICKS: EarImpressions and PE Tubes
It’s common for children with PEtubes to obtain ear impressions sothat they can obtain custom-fittingearplugs for swimming, show-ering, and so forth. Although we ofcourse suggest that you alwaysbe very careful when taking earimpressions, this becomes evenmore critical when the patient hasPE tubes. If im pression materialgoes around the ear canal block,it easily can attach to the tube,and the tube then could be pulledout of the TM when the earimpression is removed. This is notgood! It’s not common that adultpatient have PE tubes, but you willencounter this occasionally.
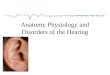
media. Cholesteatomas are dangerousbecause they eventually can erode thebones of the middle ear. They poten-tially also could damage the facial nerve,and will even invade the nose andbrain cavity in rare instances. In mostcases cholesteatoma are removed withsurgery. As with other middle ear path-ologies, the patient will have a conduc-tive hearing loss, although the patientwith a cholesteatoma will typicallyhave a more severe loss than most othermiddle ear conditions, due to the extentof the disease. It’s common to observeair-bone gaps of 30 to 40 dB. A samplecase study is shown in Figure 5–3.
Tympanosclerosis
Tympanosclerosis is characterized bywhite plaques on the surface of the tym-panic membrane and deposits on theossicles. It is often the result of chronicotitis media, which when untreatedleaves this white residue. Tympano scle -rosis can have a stiffening effect on theTM, which may result in a conductivehearing loss in the low frequencies. Asmentioned earlier, PE tubes are a com-mon treatment for otitis media. It’s com-mon for these patients (~30 to 40%) tohave resulting tympanosclerosis after thetubes have fallen out, or been removed.
Ossicular Disarticulation
This is also referred to as “dislocation”or “discontinuity.” As the name indi-cates, this condition results in one of thetwo joints between the three ossiclesbeing pulled apart or disarticulated(the incudostapedial juncture is themost common). It can produce a wide
120 UNDERSTANDING HEARING AIDS: GETTING STARTED

variety of conductive hearing lossesdepending on the location and extentof the disarticulation. The most com-mon causes of ossicular disarticulationare degenerative diseases and traumato the head. In severe head trauma aTM perforation also might be observed.Interestingly, the largest hearing loss(conductive) is present when the TM isintact, not perforated. In these cases, itis possible for an ossicular disarticula-tion to cause up to a 50 to 60 dB con-ductive hearing loss. This sometimeshas been referred to as “maximum”conductive loss, as the cochlea is stim-ulated via bone conduction for higherlevels (see Figure 5–3).
Patulous Eustachian Tube
In some cases the eustachian tube, whichis ordinarily closed, is chronically open(patent). These persons often complainthat their own voices sound hollow orthat they hear their own breathing insidetheir head. Many of these patients have
an overly patent or patulous eusta chiantube. One of the more common reasonsfor having a patulous eustachian tube isa loss of a significant amount of weight.Although a patulous eustachian tube isnot a pathologic condition, it can bequite annoying. Immitance audi ometrywhich we briefly mentioned in Chapter4 can be used to identify patulouseustachian tubes. There is little or noaccompanying hearing loss.
Disorders of the Cochlea
The scientific community regards the LochNess Monster as a modern-day myth, andexplains sightings as a mix of hoaxes andwishful thinking. Despite this, it remainsone of the most famous examples of crypto-zoology, which is the study of animals longthought extinct. When searching for disor-ders of the cochlea, in most cases you don’thave to search long or hard to encounter arelatively common cochlear problem causinga significant hearing loss.
HEARING DISORDERS AND AUDIOGRAM INTERPRETATION 121
Figure 5–3. A bilateral conductive hearing loss associated with a cholesteatoma inthe right ear, and otitis media in the left.

A significant number of people aroundthe world have sensorineural hearingloss as a consequence of damage to thecochlea. For adults, sensorineural hear-ing loss resulting from cochlear pathol-ogy is by far the most common type ofhearing impairment. In this section wespend some time reviewing the mostcommon types of sensorineural hearingloss resulting from cochlear pathology.Because there is very limited medical orsurgical treatment of cochlear hearingloss, these are the people that you willlikely see for hearing aid fittings.
Presbycusis
Don Juan Ponce de Leon completed Spain’sclaim on America in 1509, and soon after wasmade governor of Puerto Rico. Six years later,following Indian rumors, he traveled north tothe island of Bimini in search of the Fountainof Youth. Bimini turned out to be the penisulaof Florida. If you’ve ever been to an early-birddinner in southern Florida, you know thatpeople know that thousands of people are stillarriving in search of that elusive fountain.
If your patient is beyond the age of 60years old, it’s possible that the hearingsensitivity has progressively worsenedover the years, and this will now bereflected in the audiogram, especiallyin the higher frequencies. This gradualdeterioration of hearing is often a resultof prebycusis (sometimes written “pres-byacusis”). Simply stated, presbycusisis hearing loss caused by the cumula-tive effects of the aging process. Thisprogression is somewhat more rapidfor men than for women, although thispartially could be due to the fact thatmen experience more noise exposurethan women, which is difficult to sepa-rate from the aging effects on the innerear structures.
Presbycusis affects all parts of theear, including neural transmissions tothe brain, but the primary site of lesionis the cochlea. The outer hair cellswithin the cochlea are particularly sen-sitive to the wear and tear associatedwith the aging process. As a generalrule, the higher the frequency, thegreater effect of presbycusis (even peo-ple in their 20s and 30s experience lossof sensitivity in the >16,000-Hz range).The classic presbycusis audiogram
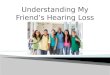
will show a gradually sloping down-ward pattern; nearly always, as the fre-quency be comes higher the hearing lossbecomes worse (Figure 5–4). Becausethis is a generalized aging process, wewould also expect the loss to be quitesymmetric. In fact, if the loss is down-ward sloping, but not symmetric, otheretiologies should be considered.
TIPS and TRICKS:Aging or Noise?
An intriguing question that oftencomes up regarding presbycusis,is whether this is indeed the resultof “aging,” per se, or the result ofaging in a noise- and stress-filledsociety. Is presbycusis just adifferent type of noise-inducedhearing loss? An often cited studyrelated to this topic dates back to1962, conducted with the Mabaantribe in Sudan. Because of theirisolation, there was very little noisein their lives. And guess what—there was little or no hearing lossfor even the older members of thetribe (~75 years old). Interpretationof this is a little tricky, as there werealso other differences (e.g., generalhealth, diet, etc.), but it certainly issomething to think about.
122 UNDERSTANDING HEARING AIDS: GETTING STARTED

TAKE FIVE: TakingAdvantage of Presbycusis
Given the known effects ofpresby cusis on high-frequencyhearing, a cell phone ring hasbeen developed with a centerfrequency around 16,000 Hz. Thenotion is that school children canuse it to call each other duringclass, and their teachers won’thear it! Another technology appli-cation related to presbycusis hasbeen to use a very loud high-pitched signal in stores whereteenagers loiter. The sound is veryannoying and drives them out, butthe older adult customers can’thear it! Sometimes presbycusiscan be a good thing.
Noise-Induced HearingLoss (NIHL)
Exposure to loud sounds can result intemporary or permanent hearing loss.This condition is called noise-inducedhearing loss (NIHL).Around30millionadults in theUnited
States are exposed to hazardous soundlevels in the workplace. Among these30 million people, it’s estimated that onein four will acquire a permanent hear-ing loss as a result of their occupation.The degree of hearing loss caused by
NIHL depends on the intensity of thesound, duration of the exposure, fre-quency spectrum of the sound, individ-ual susceptibility, along with othervariables. Usually, this type of hearingloss is due to continued exposure to
HEARING DISORDERS AND AUDIOGRAM INTERPRETATION 123
Figure 5–4. The progressive nature of presbycusis for an individual’s left ear. Theaudiogram on the left is from a 66-year-old male (showing a slight noise notch withsome recovery at 8000 Hz; given the relatively good threshold at 8000 Hz we wouldpredict that presbycusic effects are minimal at this time). The audiogram on the rightis for the same male patient at the age of 82. Note that that the pattern now no longerlooks like a noise-induced hearing loss, as the high-frequency presbycusic effectshave bended into the previous 800- to 4000-Hz hearing loss. We only show the leftear thresholds, but typically a symmetrical pattern is observed.

work or recreational noise exposurethat has occurred over several years. Itis possible, however, for NIHL to occurfor only a very short duration of expo-sure, or even a single blast (referred toas “acoustic trauma”). Because of theshape of the cochlea and the resonanteffects of the outer ear, most cases ofNIHL show a high-frequency hearingloss, with maximum loss in the 3000 to6000-Hz range, and usually with somerecovery at the highest frequencies.This pattern on the audiogram is calleda “noise notch” (see Figure 5–5). NIHLcan affect people of all ages.As NIHL is a fairly common condi-
tion it is worth spending a little bit oftime discussing the reason for the pre-cipitous slope and noise notch. Thereare a couple of reasons why the areaaround 4000 KHz is most susceptible todamage. Although the noise causing
NIHL may be broadband, with roughlyequal amplitude at all frequencies, theouter ear and ear canal resonances haveamplified the noise in the 2000 to 4000-kHZ region by the time the soundreaches the cochlea. This region, there-fore, shows the greatest amount ofdamage from noise exposure. Anotherreason for NIHL causing more loss inthe high frequencies compared to thelows is related to cochlear mechanicsand cochlear blood flow; the position-ing of the 3000 to 4000-Hz hair cellreceptors along the basal turn of thecochlea. It is possible, but quite uncom-mon, for a noise notch to occur at lowerfrequencies (e.g., 500 to 1500 Hz; thisis most commonly observed when theperson was continuously exposed to aunique noise of a narrow bandwidth.No matter the underlying reason,
NIHL is a common etiology of cochlear
124 UNDERSTANDING HEARING AIDS: GETTING STARTED
Figure 5–5. The effects of NIHL over time for one individual’s left ear. Thresholdswere measured 12 years apart for a male patient working in a condition of intensenoise (daily carpentry with skill saw). The audiogram on the right shows the progres-sive nature of the hearing loss consistent with the patient’s history of noise exposure.Notice how the dip at 400 Hz deepens, and other frequencies become more involved.The left ear had the same pattern but was not as severe; perhaps there was someattenuation of the noise from head shadow for this ear.

pathology. Given its prevalence, patientsthat are exposed to both workplace andrecreational noise need to be using prop-erly fitted hearing protection. Counselingregarding the need for hearing protec-tion is part of all audiologic exams.NIHL in its most common form is
of gradual onset. The two audiogramsbelow are from the same factory workertaken 8 years apart. Notice that the losshas become worse over the 10 yearperiod. People with significant NIHLroutinely are fitted with hearing aids,however, because many with NIHLhave normal hearing for low-frequencysounds they sometimes are challengingto fit. Many people with the hearingloss shown in the audiogram shown inFigure 5–5 say they can hear, but theyjust can’t understand completely. This isdue to the normal low-frequency hear-ing, which provides them “loudness,”but the missing high frequenciesreduces the audibility of critical speechcues for understanding.
TAKE FIVE: Personal Stereo Systems
In the past few years there hasbeen a lot of discussion regardingyoung people obtaining noise-induced hearing loss fromlisten ing to iPods and otherpersonal stereo systems. It prob-ably isn’t as bad as suggested bysome of the articles, but there is areal problem in that many of thesedevices can be turned up quiteloud and many people use themfor several hours without givingtheir ears a “rest.” The rest periodeach hour is critical (and lessloud, of course, is good too).
Permissible Levels
Our review of noise-induced hearingloss would not be complete without adiscussion of permissible levels of noiseexposure. There is a direct relationshipbetween the intensity of noise, the dura-tion of the exposure, and the degree ofpotential NIHL. When counseling pa -tients about noise exposure, it’s good tohave a general idea of what is “safe,”and when hearing protection is needed.The Occupational Health and SafetyAgency (OSHA) is an arm of the fed-eral government responsible for ensur-ing that workers are safely protectedfrom dangerous amounts of noise.Table 5–1 indicates when the intensityand duration of exposure becomes dan-gerous for individuals. If a worker isexposed to levels of sound greater than90 dB for 8 hours per day, they arerequired to wear hearing protection.Notice that as the intensity increasesthe exposure time needed to causedamage is reduced.
HEARING DISORDERS AND AUDIOGRAM INTERPRETATION 125
Table 5–1. Maximum PermissibleNoise Levels
90 dB
92 dB
95 dB
97 dB
100 dB
102 dB
105 dB
110 dB
115 dB
Source: Downloaded from http://www.quietsolution.com/Noise_Levels.pdf
8.0 hours
6.0 hours
4.0 hours
3.0 hours
2.0 hours
1.5 hours
1.0 hours
30 minutes
15 minutes

It may be obvious to some, butworkplaces are not the only conditionscausing NIHL. There are plenty of recre-ational activities, like hunting, dragracing, and going to the disco that cancause NIHL. Even though OSHA’s Per-missible Noise Exposure chart wasn’tcreated with them in mind, if you havea sound level meter, you can determineif your nightclub activities are causingsome permanent hearing loss.
Ototoxicity
There are several drugs used for thera-peutic treatment of diseases that havethe potential side effect of causing dam-age to the inner ear. Because the cochleais such a delicate organ it is susceptibleto damage from medications and chem-ical agents. Such drugs and agents areconsidered to be ototoxic or poisonousto the ears.
Ototoxic drugs have one thing incommon: they cause a senso rineuralhearing loss. The amount of ototoxichearing loss depends on the exactdosage and duration of use. When youencounter a patient who has used orbeen exposed to an ototoxic medicationor agent you should consult a physi-cian or pharmacist. A ototoxic hearingloss can present itself in different ways,but, typically, the high frequencies arethe first affected, and the hearing loss isusually downward sloping. Some facil-ities conduct high-frequency audiom -etry (10,000 to 18,000 Hz) to monitorearly changes in hearing.There are hundreds of otoxic med-
ications and agents. The most commonones along with their therapeutic usesare listed in Table 5–2. Also listed iswhether the drug causes a permanentor reversible hearing loss. The majorityof drugs cause a permanent hearing loss,but some cause reversible hearing loss.
126 UNDERSTANDING HEARING AIDS: GETTING STARTED
Table 5–2. A Summary of Common Drug Types and Their Effects on Hearing
Type of Drug Type of Hearing Loss Reversible? (Y/N)
1. Aminoglycoside Antibiotics Sensorineural No• streptomycin• gentamycin• kanamycin• vancomycin
2. Cancer Chemotherapeutics Sensorineural No• cisplatin• carboplatin
3. Loop Diuretics (Furosemide) Sensorineural Yes• lasix• bumax
4. Salicylates Sensorineural Yes• aspirin
5. Quinine Sensorineural Yes

This list is by no means exhaustive;rather, it is designed to represent a sam-ple of the most common ototoxic agentsyou will encounter. Because new med-ications are always being introducedonto the market it is best to consult withyour local physician or pharmacist forthe most current information.Ototoxic hearing loss is relatively
common in patients receiving platinum-based chemotherapy drugs. Accordingto several studies between 23 and 61%developed sensorineural hearing loss asa result of receiving these chemother-apy drugs. In many cases these hearinglosses develop 100 to 135 days followingthe onset of the chemotherapy regiment.Some of the more common platinum-based agents include cisplatin, carbo-platin, eloxtin, and vincristine.Figure 5–6 shows two audiograms
from a patient who has been receivinglarge doses of cisplatin for lung cancer.The first audiogram is 1 month after thefirst treatment and the second audio-
gram is 60 days later. Note the differencein the thresholds due to the treatmentduration. As a dispensing professionalyou probably will not be directly in -volved in collecting these types of serialaudiograms; however, it’s important tonote how and when various treatmentsmay affect someone’s hearing and asso-ciated hearing aid use.
TAKE FIVE: Important Reference
In addition to causing hearingloss, prescriptive medications cancause tinnitus, hyperacusis, dizzi-ness, and otalgia. Dr. RobertDeSogra, an audiologist in NewJersey, has created a Web sitedevoted to audiologic reactions tomedications. By going to http://www .ear serv .com and looking upa medication you quickly can findthe side effects.
HEARING DISORDERS AND AUDIOGRAM INTERPRETATION 127
Figure 5–6. Audiograms for a patient taking larges doses of cisplatin. The upper(better) is 30 days after the first treatment and the lower (worse) audiogram on theright is 60 days after the first treatment. Note the decline in hearing over that periodof time, which can be attributed to the drug regimen. The bilateral downward-slopingpattern is common.

Viral and Bacterial Diseases
There are several viral and bacterialinfections that can result in sensori -neural hearing loss. Infections, such ascytomegalovirus, can be transmitted tothe child from the mother in utero. Thisis a condition known as prenatal. Thefollowing diseases are considered pre-natal conditions that can result in a con-genital hearing loss:
� Syphilis� Rubella� Toxoplasmosis� Cytomegalovirus (CMV)� Herpes simplex virus
There also are several viral and bacterialinfections that occur after a child has beenborn that can produce sensori neural hear-ing loss. In most cases these postnatalinfections enter the inner ear throughthe blood supply, which is carrying theinfection. The following are some of themost common diseases acquired afterbirth (postnatal) causing hearing loss:
� Mumps� Measles� Bacterial meningitis� Herpes zoster oticus
Ménière’s Disease
The Lost City of Atlantis was introduced to the West 2,400 years ago by Plato, whoclaimed it to be the island home of anadvanced society. Legend says it was sunkby an earthquake, with later interpretationsas an underwater kingdom protected bymermaids. Its whereabouts are still amystery. Recent underwater evidencesuggests it was once part of a larger ????
Ménière’s disease is named after theFrench physician Prosper Ménière, whofirst reported that vertigo was causedby inner ear disorders in an article pub-lished in 1861. Ménière’s disease, in its“classic form” is used to describe a hear-ing disorder with one or more of thefollowing characteristics:
1. A hearing loss (usually in one ear)of sudden or rapid onset.
2. A fullness or pressure sensation inthe ear.
3. Brief and sudden episodes ofsevere dizziness (vertigo)
4. A roaring (tinnitus) in the affectedear.
One or all of the symptoms require animmediate referral to a physician. Thereare many subcategories of Ménière’s dis-ease beyond the scope of this chapter.Some types of cochlear hearing lossesof sudden onset, such as Ménière’s, al -though they are sensorineural manycases actually return to normal levels.The exact cause of Ménière’s disease
is not known, but it is believed to berelated to endolymphatic hydrops or excessfluid in the inner ear. It is thought thatendolymphatic fluid bursts from itsnormal channels in the ear and flowsinto other areas causing damage. Thisis called “hydrops.” This may be relatedto swelling of the endolymphatic sac orother tissues in the vestibular system ofthe inner ear, which is responsible forthe body’s sense of balance.There is no standard “signature”
audiogram for Ménière’s, but in generalthere tends to be more low-frequencyhearing loss than observed for mostother sensorineural pathologies. Thatis, the audiogram often appears “flat”or upward sloping rather than the more
128 UNDERSTANDING HEARING AIDS: GETTING STARTED

common downward sloping pattern.Figure 5–7 shows an audiogram of aclient diagnosed with Ménière’s dis-ease. Note the asymmetric (unilateral)nature of the hearing loss. After thishearing loss has stabilized, and thephysician has given authorization, thisperson might be fit with a hearing aidin the affected ear.
Retrocochlear Disorders
In general terms, retrocochlear disor-ders or pathology refers to damage tothe nerve fibers along the ascendingauditory pathways, running from theinternal auditory canal to the auditorycortex. In other words, we might bequite certain that the problem does notlie within the middle ear or the cochlea,and therefore, the locus must be some-where more medial. Commonly, inaudiologic practice, retrocochlear isused to refer to the eighth nerve and the
low brainstem, and auditory dysfunc-tion at higher auditory levels is referredto as “central.”In most cases, eighth nerve retroco -
chlear pathologies involve tumors. Retro-cochlear tumors, referred to as acous ticschmannomas, acoustic neu romas, neu -rinomas, or neurilemomas, typically (butnot always) produce unilateral high-frequency hearing loss in their moreadvanced stages. And, unlike presby-cusis and many other types of cochlearpathology, it is unlikely that therewould be uniform symmetric tumors,so there usually is asymmetry betweenears in the audiogram (Figure 5–8).The signs and symptoms of eighth
nerve retrocochlear pathology are sub-tle and difficult to identify with con-ventional audiometry. In many cases,in the early stages, there is no signifi-cant hearing loss (although there maybe a reduction of speech understandingfor speech in noise, or other difficultspeech tests). Many patients will com-plain of tinnitus on the affected side,
HEARING DISORDERS AND AUDIOGRAM INTERPRETATION 129
Figure 5–7. Asymmetric left sensorineural hearing loss consistent with Ménière’sdisease.

vertigo or dizziness, fullness, or speechnot sounding clear. In cases whereretrocochlear pathology is suspected, acomplete audiologic diagnostic batteryand otologic referral is needed. Yourjob is to refer the patient to a physicianor audiologist if a “red flag” for a retro-cochlear pathology exists.
Central Auditory Disorders
As mentioned earlier, technically aretrocochlear pathology would includeeverything medial of the cochlea, butusually we refer to pathology above the low brainstem as “central.” Whenthinking about auditory disorders, it’simportant to remember the “subtletyprinciple.” That is, as the pathologybecomes more central, going from themiddle ear to the auditory cortex, theimpact of the disorder on traditional
audiologic tests will be more subtle.For example, a cochlear pathology willnearly always cause a reduction inhearing thresholds and speech under-standing. A disorder of the brainstem(e.g., multiple sclerosis, tumors, etc.)may cause no hearing loss and no lossof speech understanding (unless a dif-ficult speech-in-noise test is conducted).The bottom line: If the patient’s historysuggests a problem with the auditoryor balance system, even if all the audio-metric results are very normal, medicalreferral is still warranted.
Nonorganic Hearing Loss
Every few years you read reports of Bigfootcarrying someone off. In 2008 there waseven a photo taken of a dead Bigfoot. Wewere skeptical of this finding when we heardthe creature was found in the woods next toa busy highway in Georgia! A few weekslater the entire report was found to be a
130 UNDERSTANDING HEARING AIDS: GETTING STARTED
Figure 5–8. A mild, right asymmetric sensorineural hearing loss consistent withpossible retrocochlear pathology.

hoax—the dead Bigfoot body was actuallymade out of wax! Bigfoot might be a hoax,but we are quite sure you will have a closeencounter with someone who presents amysterious hearing loss that turns out, withcareful testing, to be a hoax.
There are cases where a hearing lossmay be measured on the audiogram,but there is no organic basis to explainthe impairment. Some of the termsused to describe this include nonor-ganic hearing loss, pseudohypocusis,and functional hearing loss. If indeedthe patient knowingly is exaggeratingtheir hearing loss, the term malingeringis used.Aside from the cases of malingering,
where with adults, exaggeration of the
hearing loss usually is related to finan-cial com pensation, the reasons for non-organic hearing loss are not clearlyunderstood. A number of signs canalert you to the possibility, however.These signs may include inconsistenttest results, poor test-retest reliability,inappropriate be havior during the test(e.g., exaggerated attempt at listeningor lipreading), or poor agreementbetween test results and real-worldcommunication (e.g., the patient answersyour questions in the waiting room,but then demonstrates a flat 70 dB HLhearing loss). Is some cases, there maybe an underlying hearing loss, and thepatient is simply adding to it.One reason SRTs should be conducted
during routine testing is to cross check
HEARING DISORDERS AND AUDIOGRAM INTERPRETATION 131
TAKE FIVE: Pure-Tone Hearing Screenings
More than likely you will be workingprimarily with adults, you need toknow a little about hearing screen-ings. When it comes to actuallyconducting a hearing screening,there is no acceptable standard forthe identification of hearing loss in theadult population. The term “screening”implies that we are conducting sometype of a “pass/fail” procedure to seeif the patient needs further testing.
Some experts think that a pure-tone hearing screening should beconducted at 1, 2, and 4 kHz using a40 dB signal. Others suggest that a25 dB signal be used. Regardless ofthe cutoff criteria, the screening wouldbe considered a “fail” if the patientdoes not respond to the signal at thelowest intensity level tested. Keep in
mind that during a screening weconduct testing at a designated inten-sity level, rather than identifyingthreshold. When a patient fails ascreening, they usually are referredfor further testing, which includes acomplete auditory evaluation.
There are several tools that canbe used to screen older adults. TheWelch-Allyn Audioscope is a hand-held device with a built-in audiometer.There are many hand-held audiome-ters on the market today. There iseven an application, called uHEAR,that can be downloaded onto an iPod.If you do a Google search on UnitronuHear you can download it to yourfavorite MP3 player. Other hearingaid manufacturers have similarscreening tests.

the reliability of pure-tone thresholds.If the SRT and pure-tone average differby more than 10 dB, the reliability ofthe test should be questioned. If thereis a discrepancy, the SRT will nearlyalways be better than the pure-toneaverage. We recommend conductingthe SRT before the pure-tone thresholds,as this will provide you with a generalidea of where the thresholds should befalling for the speech frequencies. Ifthere is poor agreement, there is noneed to test all the other frequencies, asyou would simply assume that theentire exam is invalid. Many other spe-cial tests have been developed to detectnonorganic hearing loss, including theStenger test which is very effectivewhen the loss is only in one ear.
Hereditary Hearing Loss
As a professional who primarily fitsand dispenses hearing aids, we doubtyou will spend too much time thinkingabout hereditary hearing loss. How-ever, it’s good to know a few importantthings about it. Hearing disorders canbe classified into two types of groups:exogenous (outside the genes) andendogenous (within the genes).
� Exogenous hearing disorders arethose caused by toxicity, noise, acci-dent, or in jury that damages theinner ear. We have already summa-rized many exogenous factors ofhearing loss in this chapter.
� Endogenous hearing disordersoriginate in the genes of the indi-vidual. An endogenous hearingdisorder is transmitted from the
parents to the child as an inheritedtrait. Hearing losses resulting fromhereditary factors comprise a significant number of all hearingdisorders.
It is estimated that there are over 400different genetic syndromes in whichhearing loss is either a regular or occa-sional feature. Unless you are regularlytesting children, you are not likely to becommonly involved in the identifica-tion of hearing disorders related togenetic transmission. During a routinecase history with adults, you may en -counter various genetically transmittedsyndromes that have hearing loss asone of their characteristics. It’s alsoprobable that you will uncover a hear-ing loss that is genetic that the patientwas unaware of because many progressat a very slow rate. As a professional(nonaudiologist) who dispenses hearingaids you don’t need to have an in-depthunderstanding of genetic factors as theyrelate to hearing disorders; however, itis useful to know a few key conceptsthat you may even remember from highschool or college biology class.
Mendelian Laws
Hereditary hearing loss is based on theMendelian laws of inheritance. Accord-ing to Mendelian law, genetic traits maybe dominant, recessive, or sex-linked.Genes are located on the chromosomesand with the exception of those genesthat are located on the sex chromosomesof males, chromosomes come in pairs.One member of each gene pair is inher-ited from each parent. Humans have22 pairs of autosomes, or non-sex deter-
132 UNDERSTANDING HEARING AIDS: GETTING STARTED

mining chromosomes, and one pair ofchromosomes that determine sex. Thesex chromosomes for females consist of two X-chromosomes, and for males,one X and one Y. During reproductioneach egg and each sperm carries halfthe number of chromosomes from eachparent. When the egg is fertilized, thefull complement of chromosomes isrestored, so that half of a child’s genesare from the mother and the other halffrom the father.
Modes of Transmission
There are three modes of transmissionfor hereditary hearing loss: autosomaldominant inheritance, autosomal reces-sive inheritance,andX-linkedinheritance.The term autosomal implies that theabnormal gene is not carried on the sexchromosomes. In autosomal dominantinheritance one parent exhibits the inher-ited trait and this trait has a 50% chanceof being transmitted to the child. Exam-ples of autosomal dominant conditionsyou may encounter include Waarden-burg syndrome, branchio-otorenal syn-drome, and neurofibromatosis 2 (NF2).In cases of autosomal recessive inher-
itance, both parents of a child with hear-ing loss of the autosomal recessive typeare clinically normal. Appearance of thetrait in the child requires that an individ-ual possess two similar abnormal genes,one from each parent. Because the lawsof probability permit this type of hear-ing loss to be transmitted without man-ifestation through several generations,the detection of the origin of autosomalrecessive inheritance is very difficult.Usher syndrome and Pendred syndromeare two of the more common types of
HEARING DISORDERS AND AUDIOGRAM INTERPRETATION 133
autosomal recessive hearing disordersyou may encounter in clinical practice.Another type of genetically trans-
mitted hearing disorders is X-linked orsex-linked inheritance. X-linked inher-itance is determined by genes locatedon the X chromosome. About 2 to 3% ofall genetic hearing loss is a result of X-linked inheritance. Alport syndrome isone type of X-linked hearing disorder.More than 70% of hereditary hearing
loss is nonsyndromic, which means thehearing loss is not associated with anyother signs or symptoms. The causes ofnonsyndromic deafness are complex.Researchers have identified more than30 genes that, when mutated, may causenonsyndromic deafness; however, someof these genes have not been fully char-acterized. Different mutations in thesame gene can cause different types ofhearing loss, and some genes are asso-ciated with both syndromic and non-syndromic deafness. In many affectedfamilies, the gene responsible for hear-ing loss has not been found.Regardless of the hereditary pattern
of hearing loss, we are not even scratch-ing the surface of this topic. To learnmore go to http://www.ncbi.nlm .nih.gov and enter the key words geneticsand hearing loss.
Classification of HearingDisorders by Time of Onset
Hearing loss is also classified by the timein which the hearing loss is acquired.One important reason for knowingwhen a hearing disorder is acquired isrelated to language development. Whenan infant has a hearing loss at birth

he or she will not develop languagenormally. On the other hand, a childacquiring hearing loss at say, age 12would already have normal languagedevelopment. Hearing loss caused byviral and bacterial infections are mostcommonly associated with the termslisted below.
Congenital Hearing Loss:A hearing loss acquired at birth.Common causes include bacterialor viral infection, or ingestion ofototoxic medications.
Prenatal: A hearing loss that hasdeveloped before birth in which themother has passed the hearing dis-order onto the child. In other words,the hearing loss was acquired whilethe baby developed in utero. Themost common prenatal hearingdisorder are viral or bacterial infec-tions. Many hereditary hearingdisorders are acquired prenatally.
Perinatal: The hearing lossdevelops during or shortly after
birth. Many of the same conditionscausing a prenatal loss can occurperinatally.
Acquired or Postnatal: A hearingloss that develops later in life.Prelingual hearing loss is a hearingloss acquired during the criticallanguage development years ofbetween birth and about 12 years of age. Postlingual hearing loss isacquired after the most criticallanguage years.
In Closing
During your first few months on the job, you are likely to have a closeencounter with several of the hearingdisorders mentioned in this chapter.When you do encounter one that seemsa little mysterious, it’s wise to refer thatperson to an audiologist or a physicianspecializing in disorders of the ear.Unlike hearing aid technology, which is
134 UNDERSTANDING HEARING AIDS: GETTING STARTED
TAKE FIVE: Hearing Loss Prevalence
Hearing loss is the most commonbirth defect and the most prevalentsensorineural disorder in developedcountries. One of every 500 newbornshas a permanent, sensorineuralhearing loss. By the time a childreaches adolescence, 3.5 out of1,000 have this condition. In thegeneral population, the prev alence of hearing loss increases with age.This change reflects the impactbetween genetics and environment,as well as interactions between theenvironmental triggers and a
person’s genetic predisposition.According to the National Institutes of Health (NIH) Web site, more than50% of pre-lingual deafness isgenetic, most often autosomal recessive and nonsyndromic.Approximately 50% of autosomalrecessive nonsyndromic hearing losscan be attributed to the disorderDFNB1, caused by mutations in theGJB2 gene and the GJB6 gene. Thecarrier rate in the general populationfor a recessive deafness-causingmutation is about 1 in 33.

rapidly evolving, the subject of hearingdisorders changes at a much slowerpace. For this reason we recommendthat you invest some of your hard-earned dollars into one or two hearingdisorders textbooks. The text doesn’thave to be all that current to be useful.One we like is, Hearing Disorders by
Jerry Northern. The third edition, whichwas published in 1995, is availableonline for a reasonable price. Another isentitled, Audiology: The Fundamentals byFred Bess and Larry Humes. It has acomprehensive introductory chapteron hearing disorders that expands onthis chapter.
HEARING DISORDERS AND AUDIOGRAM INTERPRETATION 135