Embed Size (px)
Citation preview

Homework 1
Innervation of the stomach Sympathetic nerve?

A, Parasympathetic. Dashed lines indicate the cholinergic innervation of striated muscle in the esophagus and external anal sphincter. Solid lines indicate the afferent and preganglionic efferent innervation of the rest of the gastrointestinal tract.
B, Sympathetic. Solid lines denote the afferent and preganglionic efferent connections between the spinal cord and the prevertebral ganglia. Dashed lines indicate the afferent and postganglionic efferent innervation.
CG, celiac ganglion; IMG, inferior mesenteric ganglion; SMG, superior mesenteric ganglion. Gastrointestinal Physiology, Seventh Edition. LEONARD R. JOHNSON. 2007, Mosby, Inc.
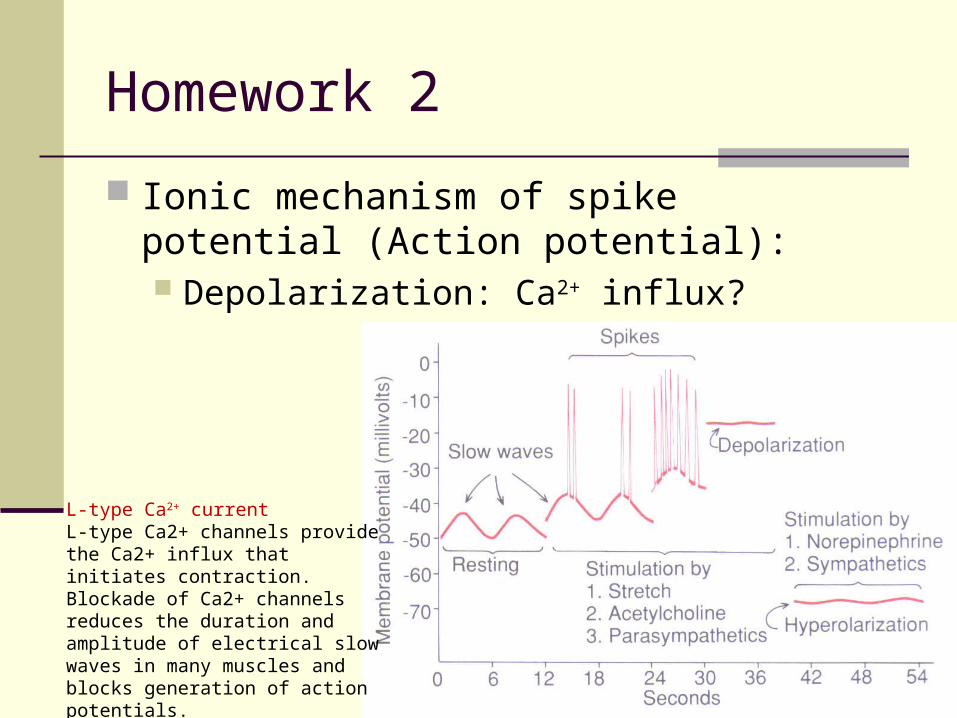
Homework 2
Ionic mechanism of spike potential (Action potential): Depolarization: Ca2+ influx?
L-type Ca2+ currentL-type Ca2+ channels provide the Ca2+ influx that initiates contraction. Blockade of Ca2+ channels reduces the duration and amplitude of electrical slow waves in many muscles and blocks generation of action potentials. Horowitz B, Ward SM, Sanders KM. Annu Rev Physiol. 1999;61:19-43.

Gastrointestinal Physiology (Part 2)
Xia Qiang, PhDDepartment of Physiology
Zhejiang University School of MedicineEmail: [email protected]


PANCREATIC SECRETION

Pancreatic juice
pH 7.8~8.4 ~1500 ml/day Isosmotic Components:
Pancreatic digestive enzymes: secreted by pancreatic acini
Sodium bicarbonate: secreted by small ductules and larger ducts

At low magnification
At higher magnification
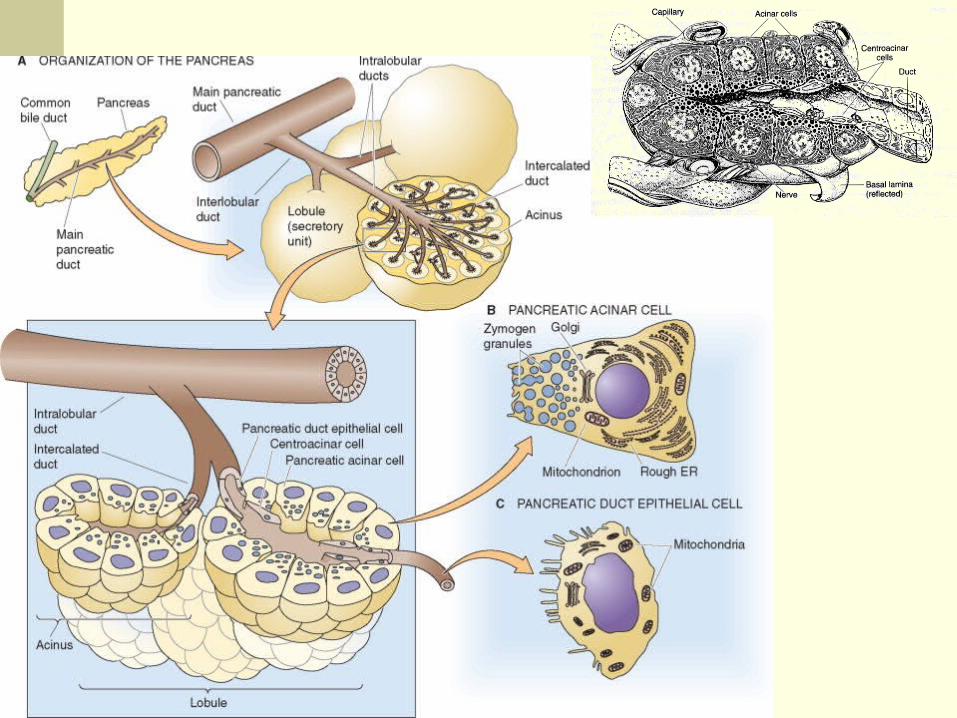

Secreted by the epithelial cells of the ductules
and ducts that lead from acini
Up to 145mmol/L in pancreatic juice (5 times
that in the plasma)
Neutralizing acid entering the duodenum from
the stomach
Secretion of bicarbonate ions

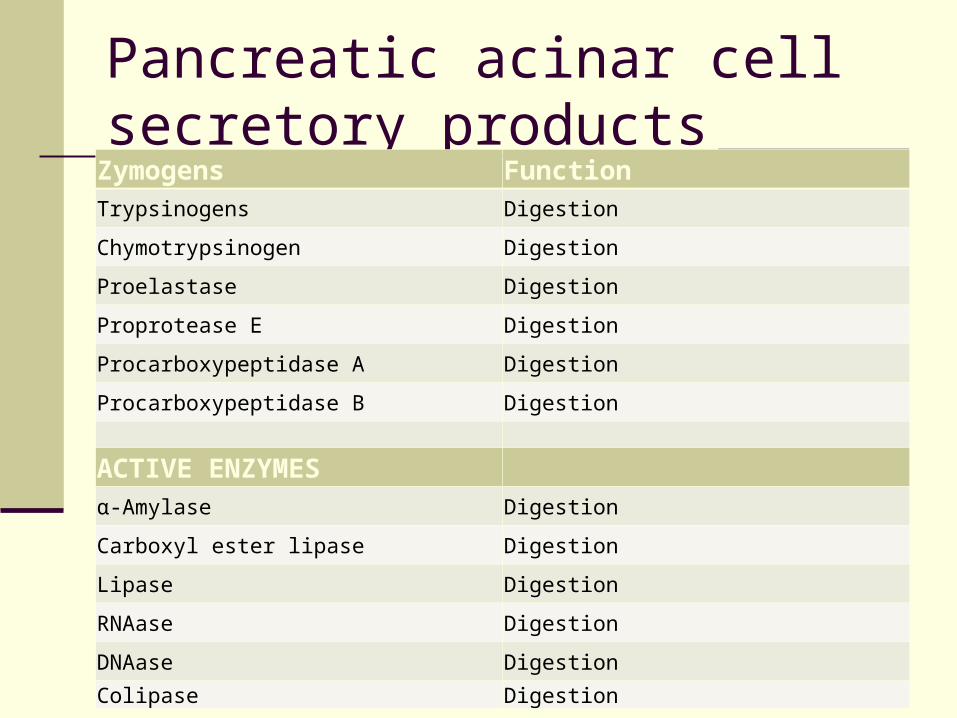
Pancreatic acinar cell secretory products
Zymogens FunctionTrypsinogens Digestion
Chymotrypsinogen Digestion
Proelastase Digestion
Proprotease E Digestion
Procarboxypeptidase A Digestion
Procarboxypeptidase B Digestion
ACTIVE ENZYMESα-Amylase Digestion
Carboxyl ester lipase Digestion
Lipase Digestion
RNAase Digestion
DNAase Digestion
Colipase Digestion

OTHERS
Trypsin inhibitor Blockade of trypsin activity
Lithostathine Possible prevention of stone formation; constituent of protein plugs
GP2 Endocytosis?; formation of protein plugs
Pancreatitis-associated protein Bacteriostasis?
Na , Cl , H2O Hydration of secretions
Ca ?

Carbohydrates -- Pancreatic amylase
Pancreatic lipase
Fat Cholesterol esterase
Phospholipase
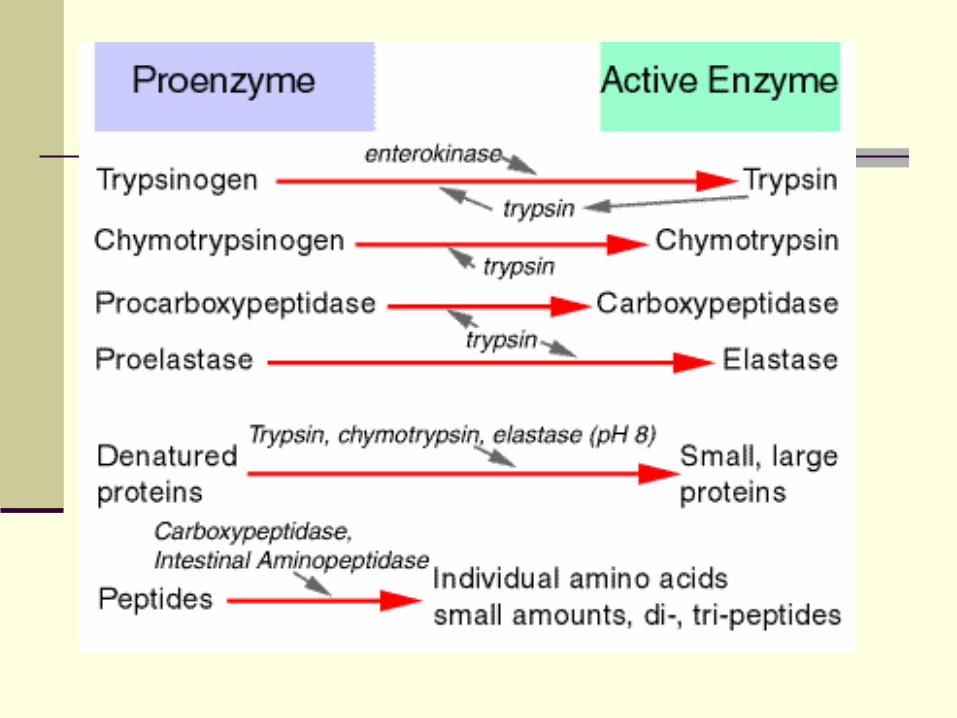
Trypsinogen
Proteins Chymotrypsinogen
Procarboxypolypeptidase
Proelastase
Secretion of pancreatic digestive enzymes
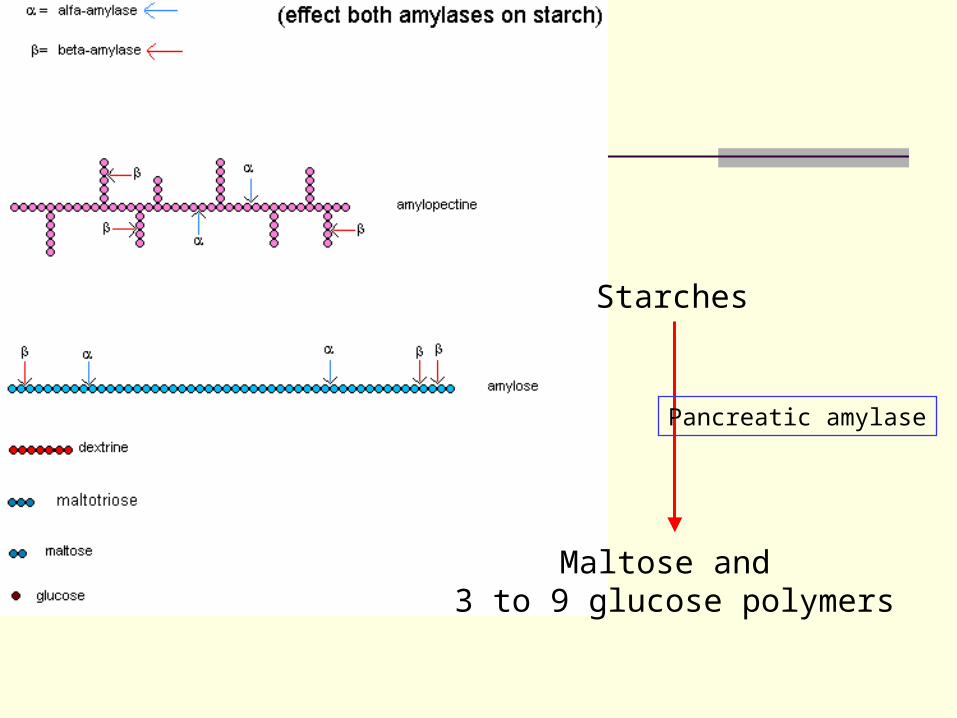
Starches
Maltose and 3 to 9 glucose polymers
Pancreatic amylase


Trypsin Inhibitor
Inhibits the activity of trypsin and thus
guards against the possible activation of
trypsin and the subsequent autodigestion of
the pancreas
Regulation of pancreatic secretion
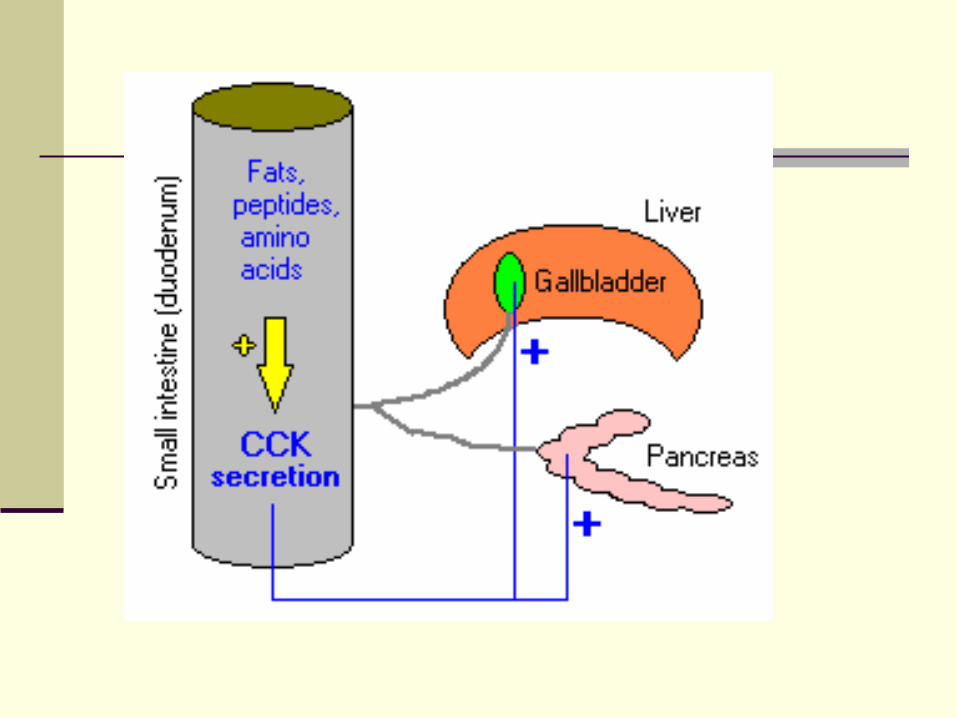
Basic stimuli that cause pancreatic secretion Ach Cholecystokinin:
Secreted by I cells Stimulates the acinar cells to secrete large
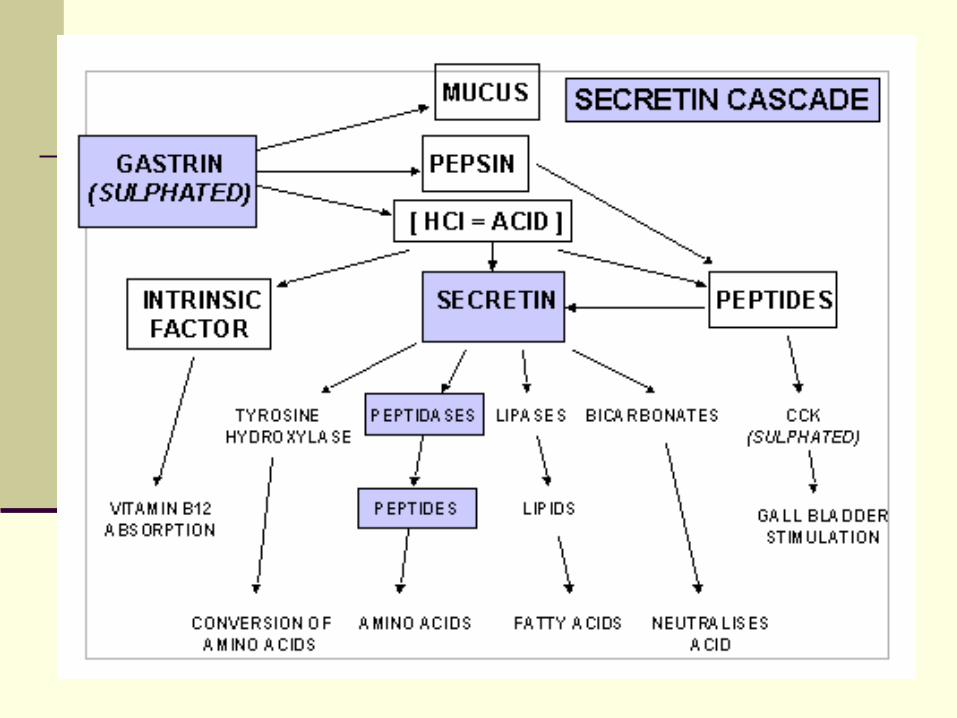
amounts of enzymes Secretin:
Released by S cells Acts primarily on the duct cells to stimulate the
secretion of a large volume of solution with a high HCO3
- concentration

Stimulation of protein secretion from the pancreatic acinar cell. A, The pancreatic acinar cell has at least two pathways for stimulating the insertion of zymogen granules and thus releasing digestive enzymes. ACh and CCK both activate Gα , which stimulates PLC, which ultimately leads to the activation of PKC and the release of Ca . Elevated [Ca ] also activates calmodulin (CaM), which can activate protein kinases (PK) and phosphatases (PP). Finally, VIP and secretin both activate Gα , which stimulates adenylyl cyclase (AC), leading to the production of cAMP and the activation of PKA. B, Applying a physiological dose of CCK (i.e., 10 pM) triggers a series of [Ca ] oscillations, as measured by a fluorescent dye. However, applying a supraphysiological concentration of CCK (1 nM) elicits a single large [Ca ] spike and halts the oscillations. Recall that high levels of CCK also are less effective in causing amylase secretion.

In addition to protein, acinar cells in the pancreas secrete an isotonic, plasma-like fluid.Stimulation of isotonic NaCl secretion by the pancreatic acinar cell. Both ACh and CCK stimulate NaCl secretion, probably through phosphorylation of basolateral and apical ion channels.The rise in [Cl ] produced by basolateral Cl uptake drives the secretion of Cl down its electrochemical gradient through channels in the apical membrane. As the transepithelial voltage becomes more lumen negative, Na moves through the cation-selective paracellular pathway (i.e., tight junctions) to join the Cl secreted into the lumen. Water also moves through this paracellular pathway, as well as through aquaporin water channels on the apical and basolateral membranes. Therefore, the net effect of these acinar cell transport processes is the production of an isotonic, NaCl-rich fluid that accounts for 25% of ∼total pancreatic fluid secretion.



Regulation of pancreatic secretion
Phases of pancreatic secretion: A meal
triggers cephalic, gastric, and intestinal
phases of pancreatic secretion
Cephalic Phase
Gastric Phase
Intestinal Phase

The three phases of pancreatic secretion
Phase Stimulant Regulatory Pathway Percentage of Maximum Enzyme Secretion
Cephalic
SightSmellTasteMastication
Vagal pathways 25%
Gastric DistentionGastrin? Vagal-cholinergic 10%-20%
IntestinalAmino acidsFatty acidsH+
CholecystokininSecretinEnteropancreatic reflexes
50%-80%

Three phases of pancreatic secretion. A, During the cephalic phase, the sight, taste, or smell of food stimulates pancreatic acinar cells, through the vagus nerve and muscarinic cholinergic receptors, to release digestive enzymes and, to a lesser extent, stimulates duct cells to secrete HCO and fluid. The release of gastrin from G cells is not important during this phase. During the gastric phase, the presence of food in the stomach stimulates pancreatic secretions'primarily from the acinar cells'through two routes. First, distention of the stomach activates a vagovagal reflex. Second, protein digestion products (peptones) stimulate G cells in the antrum of the stomach to release gastrin, which is a poor agonist of the CCK receptors on acinar cells. B, The arrival of gastric acid in the duodenum stimulates S cells to release secretin, which stimulates duct cells to secrete HCO and fluid. Protein and lipid breakdown products have two effects. First, they stimulate I cells to release CCK, which causes acinar cells to release digestive enzymes. Second, they stimulate afferent pathways that initiate a vagovagal reflex that primarily stimulates the acinar cells through M cholinergic receptors.
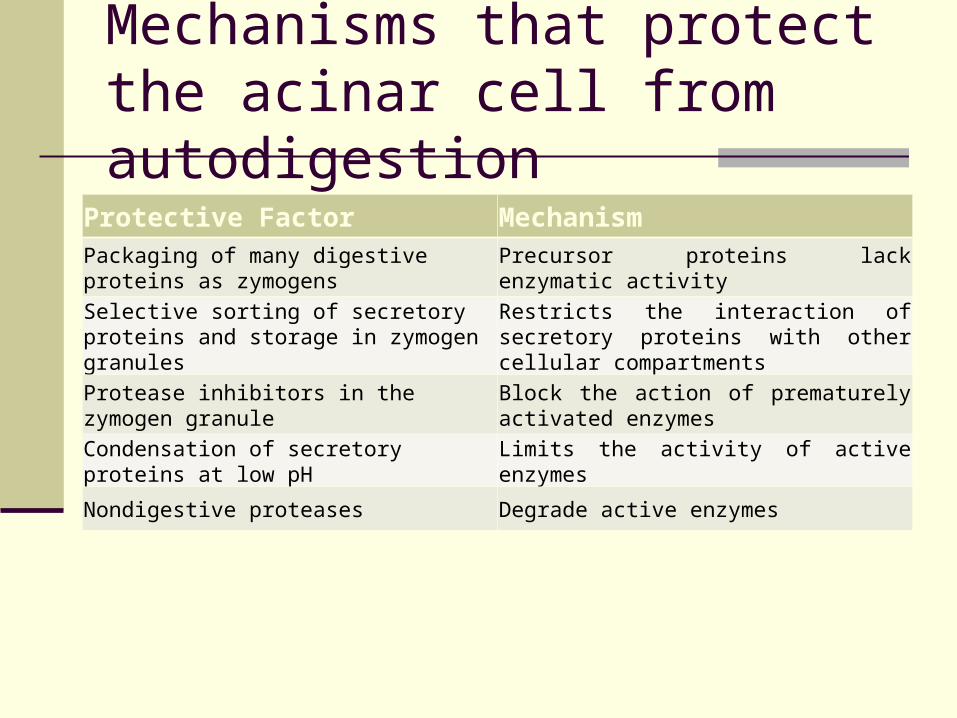
Mechanisms that protect the acinar cell from autodigestion
Protective Factor MechanismPackaging of many digestive proteins as zymogens Precursor proteins lack enzymatic activity
Selective sorting of secretory proteins and storage in zymogen granules
Restricts the interaction of secretory proteins with other cellular compartments
Protease inhibitors in the zymogen granule Block the action of prematurely activated enzymes
Condensation of secretory proteins at low pH Limits the activity of active enzymes
Nondigestive proteases Degrade active enzymes

Acute pancreatitis
Acute pancreatitis
Acute pancreatitis is sudden swelling and inflammation of the pancreas
The symptomatology and complications of acute pancreatitis are caused by autodigestion (resulting from the leakage of pancreatic enzymes) of the pancreas and surrounding tissue
It is commonly due to biliary tract disease, complications of heavy alcohol use, or idiopathic causes
Mortality rates range from below 10% to more than 50%, depending on severity

BILE SECRETION
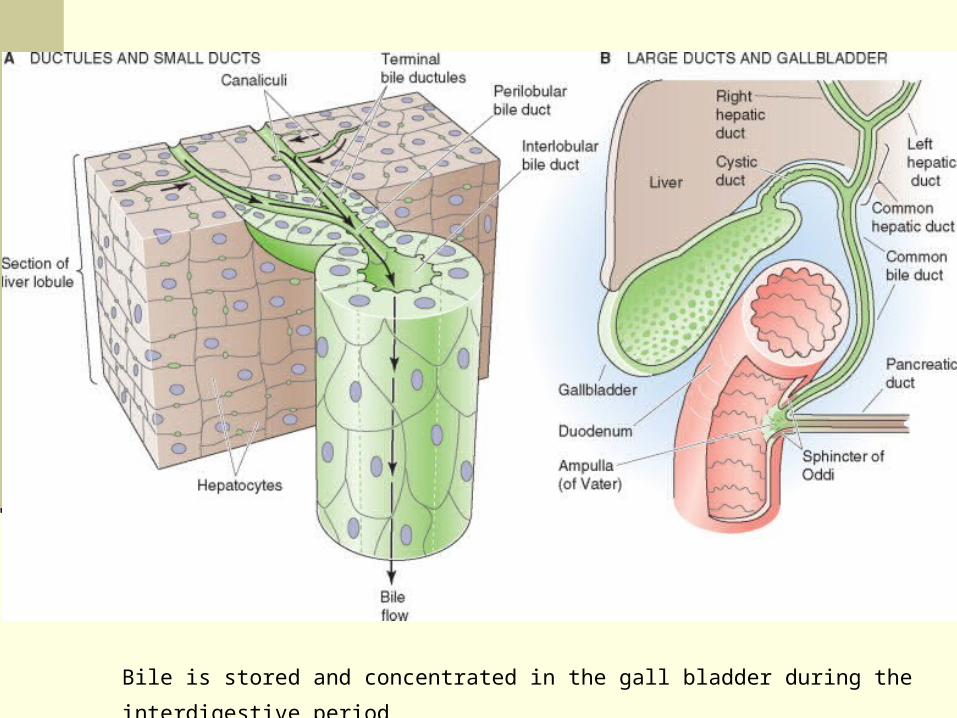
Bile is stored and concentrated in the gall bladder during the interdigestive period

Synthesis of bile acids

Composition of bile
HCO3-
Bile salts
Phospholipids
Cholesterol
Bile pigments (include: bilirubin)
…

Excretion of bilirubin

Jaundice
•Jaundice is the most visible manifestation of an underlying hepatic and/or biliary tract disease. •This is a yellow discoloration of the skin, sclerae, and mucous membranes that occurs secondary to elevated serum bilirubin in adults. •Jaundice is usually not clinically apparent until the serum bilirubin concentration is >2.5mg/dL.

Functions of bile
Emulsifying or detergent function of bile salts
Bile salts help in the absorption of:
Fatty acid
Monoglycerides
Cholesterol
Other lipids

Emulsifying large fat
particles to facilitate its
digestion


Bile salts interact with
cholesterol to form micelles
to facilitate the absorption
of insoluble fat products
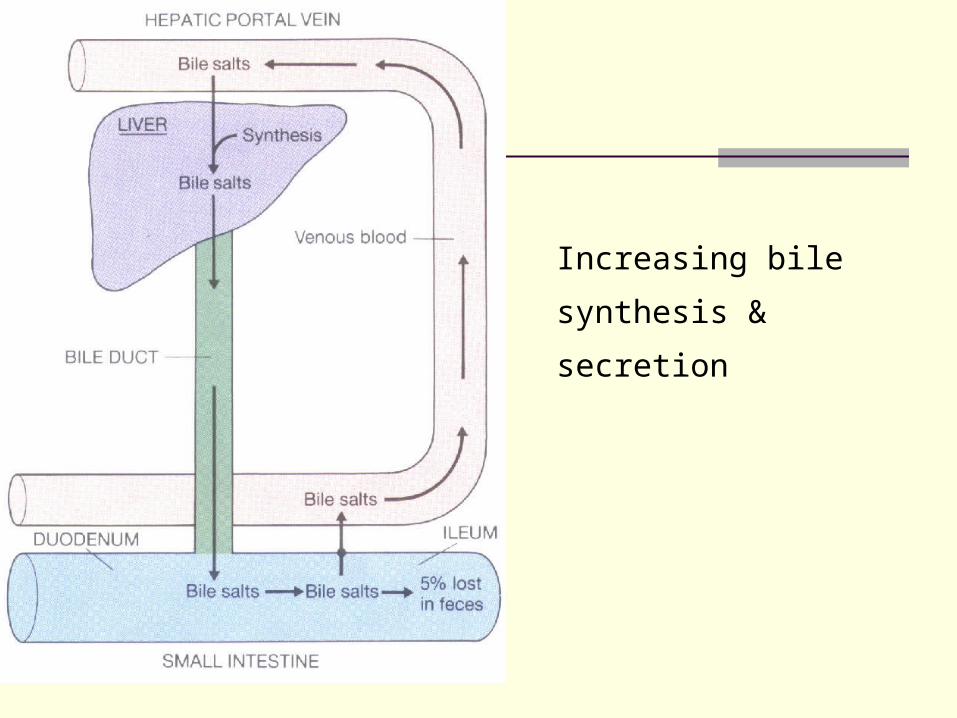
Increasing bile synthesis
& secretion

Enterohepatic circulation of bile acids


Regulation of bile secretion
Substances increasing bile production
Bile salts (Enterohepatic circulation of the bile)
Secretin: stimulating H2O and HCO3- secretion
from the duct cells
Substance inhibiting bile production
Somatostatin

Contraction of the gall bladder
Substances causing gall bladder contraction
ACh
CCK
Gastrin


Secretin and cholecystokinin are produced and secreted by cells in the lining of the alimentary tract. Which of the following statements about these 2 secretions is true?
A They are produced by enteroendocrine cells in the lining of the stomach
B They are digestive enzymes present within the lumen of the duodenum
C They are produced by Paneth cells
D They are hormones whose target cells are primarily in the pancreas and biliary tract
E They are produced by Brunner’s glands and released into the lumina of the crypts of Lieberkühn

Liver bile flow is increased by:
A Gastrin.
B Pancreatic secretion.
C Vagal stimulation.
D Sympathetic nerve stimulation

SMALL INTESTINE

Small intestinal juices
Secreted by: Brunners glands Crypts of Lieberkuhn
1~3 L/day pH 7.6 Isosmotic Components
H2O Electrolytes (Na+, K+, Ca2+, Cl-) Mucus IgA Enterokinase
Small intestinal juices
Function: Completing the digestion of
peptides, carbohydrates & fat
Secretion by intestinal glands is mainly due to
the local effects of chyme in the intestine and
is regulated by both neural and hormonal
factors

Movement of small intestine during digestion Tonic contraction: maintaining a basal state of intestinal smooth
muscle contraction
Segmentation: consisting of the alternate contraction and
relaxation of adjacent bands of circular smooth muscle
Peristalsis: a ring of muscle contraction appears on the oral
side of a bolus of ingesta and moves toward the anus,
propelling the contents of the lumen in that direction; as the ring
moves, the muscle on the other side of the distended area
relaxes, facilitating smooth passage of the bolus


Migrating motor complex (MMC)
Local areas of peristaltic contraction Present in the interdigestive period and
disappear when feeding begins Sweeping material (undigested food residues,
dead mucosal cells, bacteria) into the colon and keeping the small intestine clean
Regulated by autonomic nerves and by the release of motilin

Contractions at three loci in the small bowel. Note that at each locus, phases of no or intermittent contractions are followed by a phase of continuous contractions that ends abruptly. Also note that the phase of continuous contractions appears to migrate aborally along the bowel. Such a pattern is called the migrating motor complex (MMC). min, minute; mm Hg, millimeters of mercury

Regulation of intestinal motility
Autoregulation: Regulated by BER
Neural Reflexes:
mainly by ‘short’ reflexes in the intrinsic plexuses which are
responsible for peristalsis and segmentation
also by extrinsic nerves (sympathetic & vagal nerves) which
mediate ‘long’ reflexes
Hormonal control:
Gastrin, CCK, motilin, 5-HT (+)
Secretin, VIP, glucagon (-)

LARGE INTESTINE
Function of large intestine
The principle functions of the colon:
Absorption of water and electrolytes from the
chyme to form solid feces
Storage of fecal matter until it can be expelled
Digestion in large intestine: very limited
Bacteria: vitamin B, K

Motility of the colon
Haustration: mixing movement
Mass movement: propulsive movement
Segmentation

A normal colon, with the typical haustration

Two mass movements. A, Appearance of the colon before the entry of barium sulfate. B, As the barium enters from the ileum, it is acted on by haustral contractions. C, As more barium enters, a portion is swept into and through an area of the colon that has lost its haustral markings. D, The barium is acted on by the returning haustral contractions. E, A second mass movement propels the barium into and through areas of the transverse and descending colon. F, Haustrations again return. This type of contraction accomplishes most of the movement of feces through the colon

ABSORPTION

General mechanisms of digestion and absorption

Sites of nutrient absorption

Major gastrointestinal diseases and nutritional deficiencies
Disease Organ Site of Predominant Disease
Defects in Nutrient Digestion/Absorption
Celiac sprue Duodenum and jejunum Fat absorption, lactose hydrolysis
Chronic pancreatitis Exocrine pancreas Fat digestion
Surgical resection of ileum; Crohn disease of ileum Ileum Cobalamin and bile acid
absorption
Primary lactase deficiency Small intestine Lactose hydrolysis

Carbohydrates
The three monosaccharide products of carbohydrate digestion— glucose, galactose, and fructose—are absorbed by the small intestine in a two-step process involving their uptake across the apical membrane into the epithelial cell and their coordinated exit across the basolateral membrane.The Na/glucose transporter 1 (SGLT1) is the membrane protein responsible for glucose and galactose uptake at the apical membrane. The exit of all three monosaccharides across the basolateral membrane uses a facilitated sugar transporter (GLUT2).

Proteins
Action of luminal, brush border, and cytosolic peptidases. Pepsin from the stomach and the five pancreatic proteases hydrolyze proteins—both dietary and endogenous—to single amino acids, AA, or to oligopeptides, (AA) . These reactions occur in the lumen of the stomach or small intestine. Various peptidases at the brush borders of enterocytes then progressively hydrolyze oligopeptides to amino acids. The amino acids are directly taken up by any of several transporters. The enterocyte directly absorbs some of the small oligopeptides through the action of the H /oligopeptide cotransporter (PepT1). These small peptides are digested to amino acids by peptidases in the cytoplasm of the enterocyte. Several Na -independent amino acid transporters move amino acids out of the cell across the basolateral membrane

Absorption of whole proteins. Both enterocytes and specialized M cells can take up intact proteins. The more abundant enterocytes can endocytose far more total protein than can the M cells. However, the lysosomal proteases in the enterocytes degrade 90% of this endocytosed protein. The less ∼abundant M cells take up relatively little intact protein, but approximately half of this emerges intact at the basolateral membrane. There, immunocompetent cells process the target antigens and then transfer them to lymphocytes, thus initiating an immune response
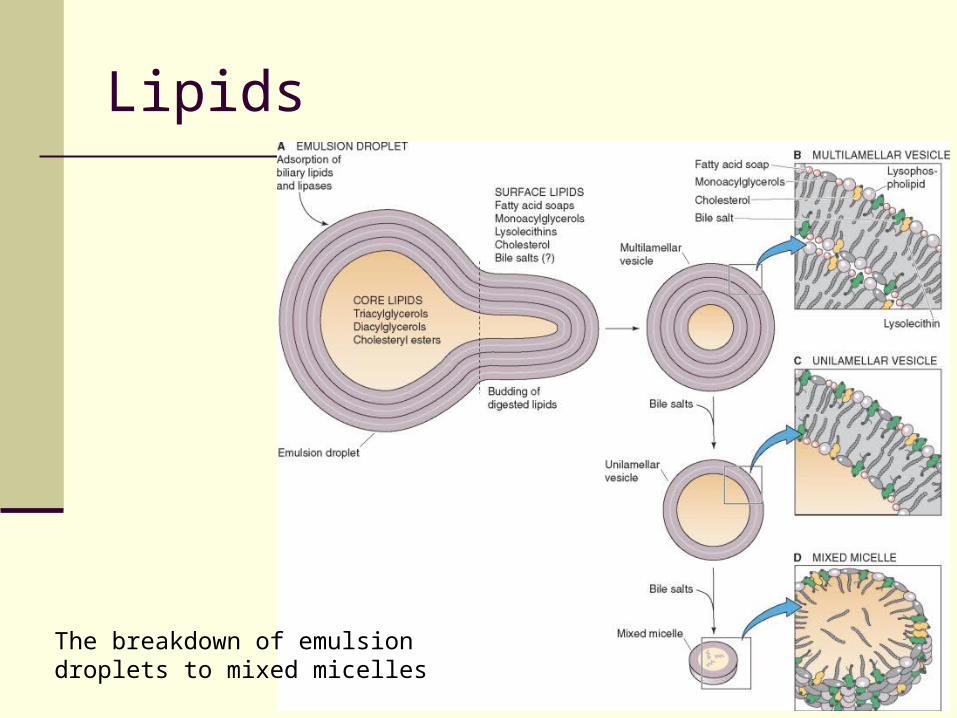
Lipids
The breakdown of emulsion droplets to mixed micelles
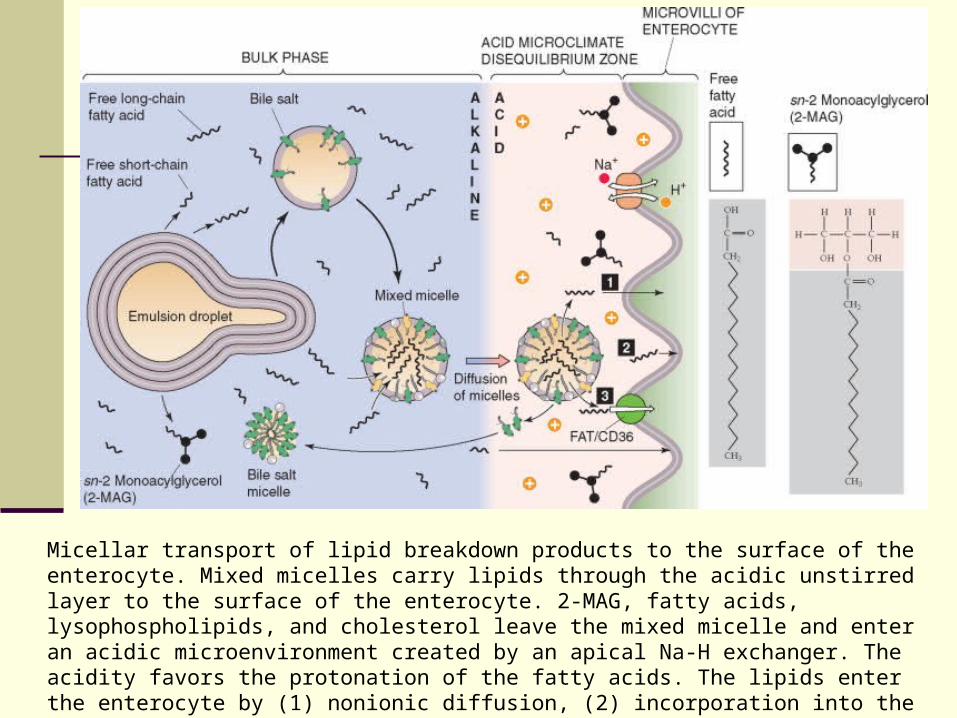
Micellar transport of lipid breakdown products to the surface of the enterocyte. Mixed micelles carry lipids through the acidic unstirred layer to the surface of the enterocyte. 2-MAG, fatty acids, lysophospholipids, and cholesterol leave the mixed micelle and enter an acidic microenvironment created by an apical Na-H exchanger. The acidity favors the protonation of the fatty acids. The lipids enter the enterocyte by (1) nonionic diffusion, (2) incorporation into the enterocyte membrane (collision), or (3) carrier-mediated transport.
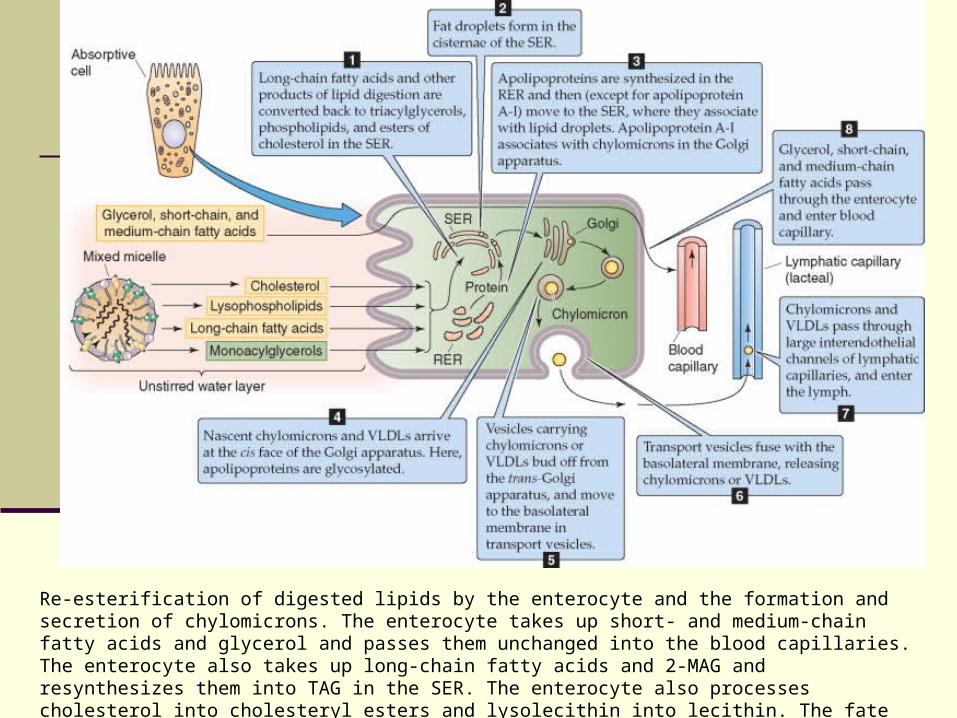
Re-esterification of digested lipids by the enterocyte and the formation and secretion of chylomicrons. The enterocyte takes up short- and medium-chain fatty acids and glycerol and passes them unchanged into the blood capillaries. The enterocyte also takes up long-chain fatty acids and 2-MAG and resynthesizes them into TAG in the SER. The enterocyte also processes cholesterol into cholesteryl esters and lysolecithin into lecithin. The fate of these substances, and the formation of chylomicrons, is illustrated by steps 1 to 8.

Calcium
Active Ca uptake in the duodenum. The small intestine absorbs Ca by two mechanisms. The passive, paracellular absorption of Ca occurs throughout the small intestine. This pathway predominates, but it is not under the control of vitamin D. The second mechanism—the active, transcellular absorption of Ca —occurs only in the duodenum. Ca enters the cell across the apical membrane through a channel. Inside the cell, the Ca is buffered by binding proteins, such as calbindin, and is also taken up into intracellular organelles, such as the endoplasmic reticulum

Iron
Absorption of nonheme and heme iron in the duodenum. The absorption of nonheme iron occurs almost exclusively as Fe , which crosses the duodenal apical membrane through DMT1, driven by a H gradient, which is maintained by Na-H exchange. Heme enters the enterocyte by an unknown mechanism. Inside the cell, heme oxygenase releases Fe , which is then reduced to Fe . Cytoplasmic Fe then binds to mobilferrin for transit across the cell to the basolateral membrane. Fe probably exits the enterocyte through basolateral ferroportin. The ferroxidase activity of hephaestin converts Fe to Fe for carriage in the blood plasma bound to transferrin.
Summary
General properties of GI Stomach Pancrea Small and large intestine Absorption

End.