Embed Size (px)
Citation preview

Idiotype-specific T lymphocytes in monoclonal gammopathies:evidence for the presence of CD4þ and CD8þ subsets
QING YI,1:2 INGRID ERIKSSON,1;3 WEN HE,1;2 GORAN HOLM,1;2 HAKAN MELL STEDT1;3
AND ANDERS OST ERBORG1;3
1Immunological Research Laboratory and 2Department of Medicine, and 3Department of Oncology (Radiumhemmet),Karolinska Hospital, Stockholm, Sweden
Received 28 June 1996; accepted for publication 8 October 1996
Summary. Tumour-specific CD4þ T helper (Th) and CD8þ Tcytotoxic (Tc) cells may participate in the control anderadication of tumour cells. In the present study, idiotype-specific stimulation of CD4þ and CD8þ blood T cells frompatients with monoclonal gammopathy of undeterminedsignificance and patients with untreated multiple myelomastage I was examined. Activation was measured in the CD4þ
and CD8þ subsets enriched by magnetic microbeads as theincorporation of 3H-thymidine and the secretion of inter-feron (IFN)-g, interleukin (IL)-2 and IL-4 by single cells usingthe enzyme-linked immunospot assay. Idiotype-specific Tcells were found in four of seven patients. Stimulation wasmainly confined to the CD4þ subset in three of the fourresponding patients. This type of response was majorhistocompatibility complex (MHC) class II restricted as itcould be inhibited by monoclonal antibodies against MHCclass II (HLA-DR), but not against class I (HLA-ABC)
molecules. Idiotype-specific CD8þ T cells were also demon-strated in these patients although at a lower frequency. Onepatient showed a strong and dominating activation of CD8þ
T cells which could be blocked by antibodies against HLA-ABC but not against HLA-DR. Idiotype-specific CD4þ orCD8þ T cells were mainly of the type-1 subsets as judged bytheir secretion of IFN-g and IL-2. Thus, this study providesevidence for the presence of idiotype-specific and MHC-restricted CD4þ and CD8þ T cells of the type-1 subsets inpatients with monoclonal gammopathies. Such T cells withthe potential to control the growth of tumour B cells may bea suitable target for immunotherapeutic interventions inpatients.
Keywords: M-component, idiotype, CD4þ T cells, CD8þ Tcells, monoclonal gammopathies.
Monoclonal gammopathies (MG), such as multiple myeloma(MM) and monoclonal gammopathy of undeterminedsignificance (MGUS), are lymphoproliferative B-celldisorders. They are characterized by proliferation of clonal Blymphocytes which are present at various stages of matura-tion and by infiltration of plasma cells in the bone marrow(Mellstedt et al, 1984). The median survival of untreatedpatients with MM is less than a year (Osgood, 1960).Treatment with alkylating agents induces a clinical responsein about 50% of the patients with a median survival time ofabout 3 years (Alexanian et al, 1969). Although promisingresults have been reported with autologous (Harousseau et al,1995) or allogeneic (Gahrton et al, 1991) bone marrowtransplantation, MM is still an almost invariably fatal disease.Thus, new therapeutic approaches aimed to control oreradicate the malignant tumour clone are warranted.
In B-cell tumours, such as lymphoma and myeloma, the idstructures within the variable regions of the monoclonalimmunoglobulin (Ig) on the malignant B-cell surface andproduced as a serum M-component, represent a clonalmarker, and may act as a tumour-specific antigen (Lynchet al, 1972; Stevenson et al, 1990; Bogen & Weiss, 1993). Bcells producing anti-id antibodies and T cells reactive withthe idiotype of the autologous M-component have beendescribed in murine plasmacytoma (Lynch et al, 1979; Floodet al, 1980; Lynch 1987; Kristoffersen & Hannestad, 1988)and in human MM and MGUS (Dianzani et al, 1988;Andersson et al, 1989; Bergenbrant et al, 1991, 1994;Osterborg et al, 1991, 1995; Yi et al, 1993). The anti-idiotype immune response has been shown to be ofimportance for the control of the growth of murineplasmacytoma (Lynch et al, 1972; Lauritzen & Bogen,1993). As the excess of circulating id Ig in human MGmay function as an immunological barrier, anti-id antibodiesare less likely to be efficient effectors in vivo. T cells generallyrecognize processed id peptides in association with major
British Journal of Haematology, 1997, 96, 338–345
338 q 1997 Blackwell Science Ltd
Correspondence: Dr Qing Yi, Immunological Research Laboratory,Department of Medicine, Karolinska Hospital, S-171 76 Stockholm,Sweden.

339Idiotype-reactive CD4þ and CD8þ T cells in Monoclonal Gammopathies
q 1997 Blackwell Science Ltd, British Journal of Haematology 96: 338–345
histocompatibility complex (MHC) molecules (Bogen et al,1986; Yi et al, 1996), and may not be blocked by thecirculating id Ig. Furthermore, T cells are considered to bethe most important effector for rejection of tumour cells in avariety of tumour animal models (reviewed in Greenberg,1991) and in human malignancies (reviewed in Kedar &Klein, 1992). Our previous studies have demonstrated thepresence of idiotype-specific T cells in MM and MGUS (Yi et al,1993; Osterborg et al, 1995). Recently we have also shownthat idiotype-induced T-cell stimulation was MHC class II-restricted in most of the patients (Yi et al, 1995, 1996),thereby providing evidence for the presence of idiotype-specific CD4þ T cells. Whether MHC class I-restricted,idiotype-specific CD8þ T cells also exist in human MG isnot yet known. The aim of the present study was to furthercharacterize idiotype-specific T-cell reactivity in CD4þ andCD8þ T-cell subsets from patients with MM and MGUS.
MATERIALS AND METHODS
Subjects. As repeated blood samples were required fortesting, only patients with MGUS (n ¼ 2) and those withuntreated and stable MM clinical stage I (n ¼ 5) wereincluded in the study. The diagnostic criteria for MM andMGUS have been described elsewhere (Mellstedt et al, 1977;Pettersson et al, 1981). The clinical staging system for MMaccording to Durie & Salmon (1975) was used. None of thepatients had been treated with immunosuppressive drugs.Four blood donors were used as healthy controls, and bloodsamples taken as buffy coats were analysed.
Preparation of monoclonal IgG and F(ab9)2 fragments. Theprocedure has been described in detail elsewhere (Bergenbrantet al, 1994). The purity of the IgG fraction was confirmed bysodium dodecyl sulphate polyacrylamid gel electrophoresis(SDS-Page) under reducing and non-reducing conditions(Pharmacia Phast system). F(ab9)2 fragments were preparedby pepsin digestion as described (Bergenbrant et al, 1991).
Monoclonal antibodies (mAb). For the identification of bloodT cells and their subsets, B cells and monocytes, fluoresceinisothiocyanate (FITC)- or phycoerythrin (PE)-conjugatedmouse mAb against CD3, CD4, CD8, CD19 and CD14(Becton Dickinson Immunocytometry Systems, MountainView, Calif.) were used. To study MHC restriction, mouseIgG2b mAb against human MHC class-II molecules HLA-DR(Immunotech, Marseille, France), or class-I molecules HLA-ABC (Chemicon International Inc., Temecula, Calif., U.S.A.),and a mouse isotypic control IgG2b (Immunotech) wereused at a final concentration of 1 mg/ml in cell cultureexperiments (see below).
Preparation of peripheral blood mononuclear cells (PBMC).PBMC were isolated by centrifugation of heparinized wholeblood (500 g for 20 min) on a Ficoll-Paque density gradient(Pharmacia) (Holm et al, 1975). Interphase cells (PBMC)were collected, washed and resuspended in culture medium(RPMI 1640, Gibco Ltd, Paisley, Scotland) supplementedwith L-glutamine (4 mM), penicillin (100 IU/ml), strepto-mycin (100 mg/ml) and 10% heat-inactivated (568C, 30 min)pooled serum from individuals with blood group ABRhþ.
Flow-cytometry analyses. Cells were stained by FITC- and
PE-conjugated mAb and analysed by a FACScan flowcytometer (Becton Dickinson) as described previously (Yiet al, 1992).
Proliferation assay. The assay was performed as describedpreviously (Yi et al, 1996). PBMC or purified T-cell subsets(1 × 105/well) were added to each well and incubated withF(ab9)2 fragments of the autologous or isotypic monoclonalIgG at concentrations ranging from 10 pg/ml to 100 mg/ml,for 3–6 d in humidified air with 5% CO2 at 378C. Cellsincubated with medium only or with purified proteinderivative (PPD; 2.5 mg/ml) were used as controls. 18 hbefore harvest 1 mCi/well of 3H-thymidine (Amersham LifeScience, Amersham, U.K.) was added. Radioactivity was
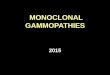
Fig 1. DNA synthesis (cpm) (mean 6 SEM) in unfractionated PBMC,CD4þ or CD8þ T cells enriched before (A) or after 3H-thymidine pulse(B). Cells were cultured with medium alone (open columns) or withPPD (filled columns). (C) Numbers of stimulated IFN-g- (filledcolumns), IL-2- (open columns) and IL-4- (solid columns) secretingcells in PBMC, enriched CD4þ and CD8þ T cells induced by PPD.

measured and the results were expressed as mean cpm oftriplicate cultures. The coefficient of variation betweentriplicate tests was 13.5%.
Detection of cell secreting IFN-g, IL-2 or IL-4. The enzyme-linked immunospot (ELISPOT) assay for identification ofinterferon (IFN)-g-, interleukin (IL)-2- or IL-4-secreting cellswas used as described earlier (Yi et al, 1993, 1995). PBMC(1 × 105/well) were incubated with F(ab9)2 fragments of theautologous or isotypic monoclonal IgG at concentrationsranging from 0.1 pg/ml to 10 mg/ml, for 48 h in humidifiedair with 5% CO2 at 378C. Cells incubated with medium aloneor with PPD (2.5 mg/ml) were used as controls. Spotscorresponding to IFN-g-, IL-2- or IL-4-secreting cellswere enumerated in a blind fashion under a dissectionmicroscope. All samples were incubated in duplicate wells.The coefficient of variation between duplicate values was8.5%.
Results were expressed as the numbers of IFN-g-, IL-2- orIL-4-secreting cells/105 PBMC or T cells. Both the total andstimulated numbers (defined as the total number of spotsminus the number of spots in cultures with medium only)were determined.
Preparation and cultivation of T-cell subsets. PBMC (2 × 106
cells/ml) were first cultured in 50 ml tissue culture flasks(Nunc A/S) in complete medium with F(ab9)2 fragments ofautologous or isotypic monoclonal IgG at an optimalconcentration obtained from preliminary experiments.Cultures with medium alone or with PPD (2.5 mg/ml) wereused as negative and positive controls, respectively.
After 5 d of culture in humidified air with 5% CO2 at 378C,the cells were collected and washed. CD4þ and CD8þ T cellswere enriched by magnetic microbeads (MiniMACS ,Miltenyi Biotec GmbH, Bergisch Gladbach, Germany),according to the manufacturer’s recommendation. EnrichedCD4þ and CD8þ cells and negatively selected CD4¹ andCD8¹ cells as well as unfractionated PBMC were thenincubated for a further 18 h with 3H-thymidine (Amersham).In parallel, the ELISPOT assay was used to detect cytokine-secreting cells. Positive responses were reproduced in threeexperiments.
Positively enriched T cells carry surface-bound beadswhich might alter their functional properties. To address thisquestion, PBMC were cultured in the presence of idiotypeprotein, PPD or medium alone for 6 d. 1 mCi/well of 3H-thymidine (Amersham) was added 18 h before separation ofCD4þ and CD8þ subsets. The results were compared withthose obtained from the experiments described above, i.e.separation of CD4þ and CD8þ cells followed by addition of3H-thymidine.
CD4þ and CD8þ T cells were also enriched immediately bymagnetic microbeads from freshly prepared PBMC. Antigen-presenting cells (APC) were obtained by incubating auto-logous PBMC in a Petri dish for 30 min at 378C. Adherentcells containing 80–90% CD14þ monocytes were thencollected. CD4þ and CD8þ T cells, respectively, were thencultured with 5% adherent cells with or without the additionof F(ab9)2 fragments of autologous or isotypic monoclonalIgG. After 5 d of culture in 5% CO2 at 378C, 3H-thymidinewas added for 18 h and the proliferative response wasmeasured as described above. Cytokine-secreting cells wereenumerated after 48 h of cultivation as described. Positiveresponses were reproduced in three experiments.
RESULTS
Purity of enriched T-cell subsetsIn the positively enriched T-cell fractions, more than 95% ofthe cells were CD3þCD4þ or CD3þCD8þ T cells. Thecontamination of CD4þ cells in enriched CD8þ T cells andvice versa was < 2%. CD19þ B cells and CD14þ monocyteswere < 1%. In the CD4¹ or CD8¹ cell suspensions, <1% cellswere CD3þCD4þ and CD3þCD8þ T cells, respectively.
PPD-induced T-cell stimulationTo set a positive control for this study, we first examinedpositively enriched CD4þ and CD8þ cells as well as PBMC fortheir response to PPD. Cells from four healthy individualsand one MM patient were tested. Mainly, a CD4þ T-cellresponse was seen (Fig 1) in all these individuals. Theresponse was the same irrespective of whether the cells were
q 1997 Blackwell Science Ltd, British Journal of Haematology 96: 338–345
340 Qing Yi et al
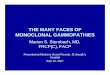
Fig 2. DNA synthesis (cpm) in PBMC inducedby F(ab9)2 fragments of the autologousmonoclonal IgG. The cells were cultured for 3 d(closed squares), 4 d (open squares), 5 d (closedcircles) or 6 d (open circles).

341Idiotype-reactive CD4þ and CD8þ T cells in Monoclonal Gammopathies
q 1997 Blackwell Science Ltd, British Journal of Haematology 96: 338–345
separated immediately from fresh PBMC and then incubatedwith autologous adherent cells in the presence of PPD for 5 d(Fig 1A) or if the cells were enriched from PBMC after beingcultured with the antigen for 5 d (Fig 1B). PPD preferentially
induced CD4þ T cells to secrete IFN-g- and IL-2, but not IL-4(Fig 1C). Similar results were obtained when negativelyenriched cell fractions were used (data not shown). The PPD-induced DNA synthesis in T cells was abrogated by addingmouse mAb against HLA-DR, but not against HLA-ABC orthe mouse isotypic control IgG (data not shown).
To analyse whether the surface-bound beads on positivelyenriched CD4þ and CD8þ cells may influence functionalcapacity, PBMC were cultured with PPD for 6 d. Separationusing magnetic beads was then performed either before orafter 18 h of incubation with 3H-thymidine. Lower prolif-erative response was noted within the CD4þ and CD8+ T cellsenriched after 3H-thymidine pulse (Fig 1B) than cellsenriched before the pulse, i.e. cells with surface-boundbeads (Fig 1A). However, the response pattern was the samecomparing cells with or without surface-bound beads.Similar results were obtained by examining idiotype-stimulated cells (data not shown). In the following experi-ments, we therefore chose the method of cell separationfollowed by addition of 3H-thymidine.
F(ab9)2 fragment-induced T-cell stimulationPBMC from seven patients with MG were incubated withF(ab9)2 fragments of the autologous monoclonal IgG. In fourpatients (one patient with MGUS and three patients withMM) an idiotype-specific proliferative response was noted. Asexemplified in Fig 2, a 6 d culture induced an optimalproliferative response in three of the four patients. In theother patient the proliferative response was not differentbetween day 3 and day 6 of culture. An increase in thenumber of IFN-g-secreting cells was also noted in these fourpatients (data not shown). These four responding patientswere selected for further studies.
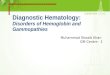
To determine whether the idiotype reactivity was confinedto CD4þ and/or CD8þ cells, PBMC were cultured withF(ab9)2 fragments of the autologous or isotypic IgG. After 5 dof culture, CD4þ and CD8þ T cells were positively enrichedby magnetic beads and assayed for proliferation and thenumber of cytokine-secreting cells. In three of the patientsan idiotype- but not isotype-specific proliferation as well asIFN-g secretion was noted within the CD4þ T-cell popula-tion, as exemplified by the experiments depicted in Figs 3A
Fig 3. DNA synthesis (cpm) (mean 6 SEM) (A), and total number ofIFN-g-secreting cells (mean 6 SEM) (B) in PBMC, enriched CD4þ andCD8þ T cells after incubation with medium alone (solid columns),F(ab9)2 fragments of the autologous IgG (10 mg/ml) (open columns)or isotypic IgG (10 mg/ml) (filled columns). The results are from onepatient tested three times.
Fig 4. Inhibition by anti-MHC antibodies ofidiotype-induced DNA synthesis in T cells(cpm) (mean 6 SEM). PBMC (filled columns)and enriched CD4þ T cells (open columns)were incubated with the autologous F(ab9)2
fragments (10 mg/ml) and with the addition ofanti-HLA-DR, anti-HLA-ABC antibodies orcontrol IgG (1 mg/ml). Cpm in cell cultureswith medium alone was 380 6 100. The testwas repeated three times.

and 3B. CD8þ cells also responded by secreting IFN-g, butthe number of IFN-g-secreting cells was usually lower thanthat within the CD4þ cell fraction (Fig 3B). Comparableresults were obtained using negatively selected (CD8¹ andCD4¹) cells (data not shown). The id response was alsoanalysed in initially enriched CD4þ and CD8þ subsets. Afterisolation, CD4þ and CD8þ cells were incubated with theautologous or isotypic protein in the presence of 5%autologous adherent cells. The number of idiotype-specificIFN-g-secreting cells in the CD4þ and CD8þ subsets,respectively, was similar either when enriched CD4þ andCD8þ cells were used, or when PBMC were stimulated withthe id IgG and then CD4þ and CD8þ cells were isolated (datanot shown). Finally, mAb against MHC class I (HLA-ABC)and class II (HLA-DR) molecules were used to block idiotype-induced T-cell stimulation. Antibodies against HLA-DR, butnot against HLA-ABC or the mouse control IgG, inhibited theidiotype-induced proliferative response in PBMC as well as inenriched CD4þ T cells, as shown in Fig 4. Similar resultswere obtained with PBMC and CD4þ cells, respectively, byenumerating idiotype-induced IFN-g-secreting cells. AnMHC class II-restricted response was demonstrated in thosethree patients where an idiotype-specific CD4þ T-cellresponse predominated.
The idiotype-induced cytokine-secretion pattern differedbetween CD4þ and CD8þ T cells. In two patients studied,high numbers of idiotype-induced IFN-g- and IL-2-secretingcells and a low number of IL-4-secreting cells were found inthe CD4þ T-cell population. In the CD8þ T-cell fraction fewerIFN-g and IL-2-secreting cells and no IL-4-secreting cellswere detected (Fig 5).
One (MM patient) of the four responding patients had apredominant MHC class-I restricted CD8+ T-cell response.Idiotype-induced proliferation (Fig 6A) and IFN-g secretion(Fig 6B) were seen within the CD8+ T-cell fraction whencultured for 3 d. However, when the cells were culturedfor 6 d, both CD8þ and CD4þ T cells proliferated (Fig 6C) and
secreted IFN-g (data not shown), although the CD8þ T-cellresponse still predominated. The specific CD8þ T-cellresponse was abolished by HLA-ABC antibodies, but not byHLA-DR antibodies in the 3 d culture (mean % inhibition6 SEM: 80 6 10 and 12 6 8, respectively). In the 6 d cultureanti-HLA-ABC and, to a lesser extent, anti-HLA-DR antibodiesinhibited the proliferative response. The mouse control IgGhad no effect (data not shown), which is in agreement withthe results in Fig 6.
DISCUSSION
This study aimed to explore subsets of idiotype-specific T cellsin patients with MGUS and patients with untreated MMstage I. In four out of seven patients an idiotype-specific T-cell
q 1997 Blackwell Science Ltd, British Journal of Haematology 96: 338–345
342 Qing Yi et al
Fig 5. Number of cytokine-secreting cells (mean 6 SEM) in CD4þ
(filled columns) and CD8þ (open columns) T-cell populationsenriched from PBMC after stimulation with F(ab9)2 fragments ofthe autologous IgG. The patient was tested three times.
Fig 6. Idiotype-induced DNA synthesis and IFN-g-secreting cells(mean 6 SEM) in PBMC, enriched CD4þ or CD8þ T cells cultured for3 d (A, B) or 6 d (C). The cells were cultured with medium alone(open columns) or F(ab9)2 fragments of the autologous IgG (1 mg/ml)(filled columns).

343Idiotype-reactive CD4þ and CD8þ T cells in Monoclonal Gammopathies
q 1997 Blackwell Science Ltd, British Journal of Haematology 96: 338–345
response was noted. In three of these patients a predominantCD4þ T-cell response was present, which could be blocked byanti-MHC class II (HLA-DR) antibodies, but also few idiotype-specific CD8þ T cells were found. In one patient a CD8þ T-cellresponse dominated, which in analogy could be blocked byanti-MHC class I antibodies. Therefore this study providesevidence for the presence not only of idiotype-specific CD4þ
but also idiotype-specific CD8þ T cells in patients with MG.The in vitro assay system was also tested using a
conventional antigen, PPD. A CD4þ T-cell response wasseen in all individuals. The response was MHC class IIrestricted and the PPD-specific CD4þ T cells secreted IFN-gand IL-2, but not IL-4, which is in line with a previous studyshowing that most PPD-specific T-cell clones were of the Th1type (Romagnani, 1991). Moreover, the separation proce-dure (MiniMACS beads) did not seem to influence theidiotype-specific response pattern (Fig 1).
The CD8þ T-cell subset contains cytotoxic T (Tc) cells thatmight be the most important effector cells in tumourrejection (Greenberg, 1991). CD8þ Tc cells recognizemainly endogenously synthesized antigen peptides presentedon MHC class I molecules (Germain, 1994). In mice bearingthe MOPC-315 plasmacytoma, tumour-specific CD8þ Tccells with a potent lytic activity capable of eradicating a largetumour burden have been described (Takesue et al, 1990;Mokyr et al, 1993). In the present report, functionally activeidiotype-specific MHC class I-restricted CD8þ T cells weredetected. Whether these cells are capable of binding andrejecting idiotype-expressing tumour B cells remains to beestablished. Recently, clonal expansion of CD8þ T cells basedon the nucleotide sequence of T-cell receptor (TCR) has alsobeen shown in MG, although the functional specificity wasnot determined (Moss et al, 1996; and unpublishedobservations).
The generation of a specific CD8þ cytolytic responseusually requires the presence of CD4þ Th cells (Keene &Forman, 1982; Greenberg, 1991). The molecular basis forthe Th function is local secretion of cytokines such as IL-2which act upon Tc whose TCRs have been engaged by theappropriate antigen–MHC complex (Zinkernagel et al, 1978;Keene & Forman, 1982; Fearon et al, 1990). It is unlikelythat the idiotype-reactive CD8þ T cells were unspecificallyactivated by cytokines secreted by specific CD4þ T cells. First,one patient showed a predominance of a CD8þ T-cellresponse after idiotype stimulation. Second, the sameresponse pattern was seen when CD4þ and CD8þ T cellswere first enriched and then stimulated with the idiotype aswhen PBMC was initially stimulated with the idiotype andthen separated into CD4þ and CD8þ T cells. The observationmay suggest that in vivo primed idiotype-specific CD8þ T cellsmight be activated independently of CD4þ T cells. Thefinding that only CD8þ idiotype-specific T cells were noted atday 3, but at day 6 both idiotype-specific CD8þ and CD4þ
cells were found, is not clear. The idiotype-specific CD4þ T-cell population in this patient may have been too small to bedetected after 3 d of culture and 6 d were needed.
CD8þ Tc cells can be subdivided to two types of cells basedon their cytokine-secretion profile: Tc1 and Tc2. Tc1 cellssecrete IL-2 and IFN-g, and Tc2 secrete IL-4, IL-5 and IL-10
(Cox & Liew, 1992; Mosmann & Sad, 1996). Both CD8þ Tc1and Tc2 cells may be cytotoxic. However, Tc1 cells seemed tobe the most efficient killer cells using both the Ca2þ/perforin-dependent mechanism, and to a lesser extent via Fas antigen(Mosmann & Sad, 1996). According to the cytokine-secretion profile (IFN-g but not IL-4), the idiotype-specificCD8þ T cells might belong to the Tc1 subset.
The importance of CD4þ T helper (Th) cells in tumourrejection has also been emphasized (Hamaoka & Fujiwara,1987; Bogen & Weiss, 1993). The generation of CD8þ
cytolytic cells requires the presence of CD4þ Th cells (Keene& Forman, 1982; Greenberg, 1991), but CD4þ T cellsthemselves also reject a wide variety of tumours (Greenberg,1991). Three of four patients with MM and MGUS displayedan idiotype-specific MHC class II-restricted CD4þ T-cellresponse in accordance with previous reports (Yi et al,1995, 1996). Based on the cytokine-secretion pattern, thecells seemed to belong to the Th1 fraction, the cells of whichsupport the induction of a CD8þ T-cell response and arethemselves cytotoxic (Romagnani, 1991, 1994). In a murineplasmacytoma model, idiotype-specific Th1 cells were shownto be cytotoxic and could protect against challenge withidiotype-expressing plasmacytoma-tumour cells (Lauritzenet al, 1993).
In conclusion, the present study provides evidence tosupport the presence of idiotype-specific T cells within boththe CD4þ and CD8þ subsets in MG. The cytokine-secretionprofile suggests that these T cells may be type-1 cells (CD4þ
Th1 and CD8þ Tc1) which might have a high cytotoxicactivity. Immunotherapy with the aim of enhancing theactivity of idiotype-specific type-1 T cells may be a rewardingapproach in patients with MM and high-risk MGUS.
ACKNOWLEDGMENTS
This work was supported by grants from the Swedish CancerSociety, the Cancer Society in Stockholm, The King Gustaf VJubilee Fund, the Swedish Society of Medicine, the Inga-Brittand Arne Lundbergs Foundation, and the KarolinskaInstitute Fund.
REFERENCES
Alexanian, R., Haut, A., Khan, A.U., Lane, M., McKelvey, E.M.,Migliore, P.J., Stuckey, W.J. & Wilson, H.E. (1969) Treatment formultiple myeloma: combination chemotherapy with differentmelphalan dose regimens. Journal of the American MedicalAssociation, 208, 1680–1685.
Andersson, M., Holm, G., Lefvert, A.K. & Mellstedt, H. (1989) Anti-idiotypic B cell lines from a patient with monoclonal gammopathyof undetermined significance. Scandinavian Journal of Immunology,130, 489–492.
Bergenbrant, S., Osterborg, A., Holm, G., Mellstedt, H. & Lefvert, A.K.(1991) Anti-idiotypic antibodies in patients with monoclonalgammopathies: relation to tumour load. British Journal ofHaematology, 78, 66–70.
Bergenbrant, S., Yi, Q., Osby, E., Osterborg, A., Ostman, R.,Bjorkholm, M., Holm, G. & Lefvert, A.K. (1994) Anti-idiotypic Blymphocytes in patients with monoclonal gammopathies. Scandi-navian Journal of Immunology, 40, 216–220.

Bogen, B., Malissen, B. & Haas, W. (1986) Idiotype-specific T cellclones that recognize syngeneic immunoglobulin fragments in thecontext of class II molecules. European Journal of Immunology, 16,1373–1378.
Bogen, B. & Weiss, S. (1993) Processing and presentation ofidiotypes to MHC-restricted T cells. International Review ofImmunology, 10, 337–355.
Cox, F.E.G. & Liew, F.Y. (1992) T-cell subsets and cytokines inparasitic infections. Immunology Today, 13, 445–448.
Dianzani, U., Pileri, A., Boccadoro, M., Palumbo, A., Pioppo, P.,Bianchi, A., Camponi, A., Fossati, G., Battaglio, S. & Massaia, M.(1988) Activated idiotype-reactive cells in suppressor/cytotoxicsubpopulations of monoclonal gammopathies: correlation withdiagnosis and disease status. Blood, 72, 1064–1068.
Durie, B.G.M. & Salmon, S.E. (1975) A clinical staging system formultiple myeloma. Cancer, 36, 842–854.
Fearon, E.R., Pardoll, D.M., Itaya, T., Golumbek, P., Levitsky, H.I.,Simons, J.W., Karasuyama, H., Vogelstein, B. & Frost, P. (1990)Interleukin-2 production by tumor cells bypasses T helperfunction in the generation of an antitumor response. Cell, 60,397–403.
Flood, P.M., Philipps, C., Taupier, M.A. & Schreiber, H. (1980)Regulation of myeloma growth in vitro by idiotype-specificlymphocytes. Journal of Immunology, 124, 424–430.
Gahrton, G., Tura, S., Ljungman, P., Belanger, C., Brandt, L.,Cavo, M., Facon, T., Granena, A., Gore, M., Gratwohl, A.,Lowenberg, B., Nikoskelainen, J., Reiffers, J.J., Samson, D.,Verdonck, L., Volin, L., for the European Group for BoneMarrow Transplantation (1991) Allogeneic bone marrow trans-plantation in multiple myeloma. New England Journal of Medicine325, 1267–1273.
Germain, R.N. (1994) MHC-dependent antigen processing andpeptide presentation: providing ligands for T lymphocyteactivation. Cell, 76, 287–299.
Greenberg, P.D. (1991) Adoptive T cell therapy of tumors: mecha-nisms operative in the recognition and elimination of tumor cells.Advances in Immunology, 49, 281–355.
Hamaoka, T. & Fujiwara, H. (1987) Phenotypically and functionallydistinct T-cell subsets in anti-tumor responses. Immunology Today,8, 267–269.
Harousseau, J.-L., Attal, M., Divine, M., Marit, G., Leblond, V.,Stoppa, A.-M., Bourhis, J.-H., Caillot, D., Boasson, M., Abgrall, J.-F.,Facon, T., Linassier, C., Cahn, J.-Y., Lamy, T., Troussard, X.,Gratecos, N., Pignon, B., Auzanneau, G. & Bataille, R. (1995)Autologous stem cell transplantation after first remission induc-tion treatment in multiple myeloma: a report of the Frenchregistry on autologous transplantation in multiple myeloma.Blood, 85, 3077–3085.
Holm, G., Pettersson, D., Mellstedt, H., Hedfors, E. & Bloth, B. (1975)Lymphocytic subpopulation in peripheral blood of healthypersons: characterization by surface markers and lack of selectionduring purification. Clinical and Experimental Immunology, 20,443–457.
Kedar, E. & Klein, E. (1992) Cancer immunotherapy: are the resultsdiscouraging? Can they be improved? Advances in Cancer Research,59, 245–322.
Keene, J.-A. & Forman, J. (1982) Helper activity is required for the invivo generation of cytotoxic T lymphocytes. Journal of ExperimentalMedicine, 155, 768–782.
Kristoffersen, G. & Hannestad, K. (1988) Immune response to anadjuvant-free native syngeneic myeloma protein (M315). Euro-pean Journal of Immunology, 18, 1785–1790.
Lauritzen, G.F. & Bogen, B. (1993) The role of idiotype-specific, CD4þ
T cells in tumor resistance against major histocompatibility
complex class II molecule negative plasmacytoma cells. CellularImmunology, 148, 177–188.
Lauritzen, G.F., Weiss, S. & Bogen, B. (1993) Anti-tumor activity ofidiotype-specific, MHC-restricted Th1 and Th2 clones in vitro andin vivo. Scandinavian Journal of Immunology, 37, 77–85.
Lynch, R.G. (1987) Immunoglobulin-specific suppressor T cells.Advances in Immunology, 40, 135–151.
Lynch, R.G., Graff, J.R., Sirisinha, S., Simms, E.S. & Eisen, H.N.(1972) Myeloma proteins as tumor-specific transplantationantigens. Proceedings of the National Academy of Sciences of theUnited States of America, 69, 1540–1544.
Lynch, R.G., Rohrer, J.W., Odermatt, B., Gebel, H.M., Autry, J.R. &Hoover, R. (1979) Immunoregulation of murine myeloma cellgrowth and differentiation: a monoclonal model of B celldifferentiation. Immunological Reviews, 48, 45–80.
Mellstedt, H., Bjorkholm, M. & Holm, G. (1977) Intermittentmelphalan and prednisone therapy in plasma cell myeloma. ActaMedica Scandinavica, 202, 5–9.
Mellstedt, H., Holm, G. & Bjorkholm, M. (1984) Multiple myeloma,Waldenstrom’s macroglobulinemia, and benign monoclonalgammopathy: characteristics of the B cell clone, immunoregula-tory cell populations and clinical implications. Advances in CancerResearch, 41, 257–289.
Mokyr, M.B., Rubin, M., Newell, K.A., Prokhorova, A. & Bluestone,J.A. (1993) Involvement of TCR-Vb8.3þ cells in the cure of micebearing a large MOPC-315 tumor by low dose melphalan. Journalof Immunology, 151, 4838–4846.
Mosmann, T.R. & Sad, S. (1996) The expanding universe of T-cellsubsets: Th1, Th2 and more. Immunology Today, 17, 138–146.
Moss, P.A.H., Gillespie, G., Frodsham, P., Bell, J. & Reyburn, H.(1996) Clonal populations of CD4þ and CD8þ T cells in patientswith myeloma and paraproteinemia. Blood, 87, 3297–3306.
Osgood, E.E. (1960) The survival time of patients with plasmacyticmyeloma. Cancer Chemotherapy Reports, 9, 1–10.
Osterborg, A., Masucci, M., Bergenbrant, S., Holm, G., Lefvert, A.K.& Mellstedt, H. (1991) Generation of T cell clones binding F(ab9)2
fragments of the idiotypic immunoglobulin in patients withmonoclonal gammopathy. Cancer Immunology and Immunotherapy,34, 157–162.
Osterborg, A., Yi, Q., Bergenbrant, S., Holm, G., Lefvert, A.K. &Mellstedt, H. (1995) Idiotype-specific T cells in multiple myelomastage I: an evaluation by four different functional tests. BritishJournal of Haematology, 89, 110–116.
Pettersson, D., Mellstedt, H., Holm, G. & Bjorkholm, M. (1981)Monoclonal blood lymphocytes in benign monoclonal gammo-pathy and myeloma in relation to clinical stage. ScandinavianJournal of Haematology, 27, 287–293.
Romagnani, S. (1991) Human TH1 and TH2 subsets: doubt nomore. Immunology Today, 12, 256–257.
Romagnani, S. (1994) Lymphokine production by human T cells indisease states. Annual Review of Immunology, 12, 227–257.
Stevenson, F.K., George, A.J.T. & Glennie, M.J. (1990) Anti-idiotypictherapy of leukemias and lymphomas. Chemical Immunology, 48,126–166.
Takesue, B.Y., Pyle, J.M. & Mokyr, M.B. (1990) Importance of tumor-specific cytotoxic CD8þ T-cells in eradication of a large sub-cutaneous MOPC-315 tumor following low-dose melphalantherapy. Cancer Research, 50, 7641–7649.
Yi, Q., Ahlberg, R., Pirskanen, R. & Lefvert, A.K. (1992) Levels ofCD5þ B lymphocytes do not differ between patients withmyasthenia gravis and healthy individuals. Neurology, 42,1081–1084.
Yi, Q., Bergenbrant, S., Osterborg, A., Osby, E., Ostman, R.,Bjorkholm, M., Holm, G. & Lefvert, A.K. (1993) T-cell stimulation
q 1997 Blackwell Science Ltd, British Journal of Haematology 96: 338–345
344 Qing Yi et al

345Idiotype-reactive CD4þ and CD8þ T cells in Monoclonal Gammopathies
q 1997 Blackwell Science Ltd, British Journal of Haematology 96: 338–345
induced by idiotypes on monoclonal immunoglobulins inpatients with monoclonal gammopathies. Scandinavian Journal ofImmunology, 38, 529–534.
Yi, Q., Holm, G. & Lefvert, A.K. (1996) Idiotype-induced T cellstimulation requires antigen presentation in association withHLA-DR molecules. Clinical and Experimental Immunology, 104,359–365.
Yi, Q., Osterborg, A., Bergenbrant, S., Mellstedt, H., Holm, G. &Lefvert, A.K. (1995) Idiotype-reactive T-cell subsets and tumorload in monoclonal gammopathies. Blood, 86, 3043–3049.
Zinkernagel, R.M., Callahan, G.N., Althage, A., Cooper, S.,Streilein, J.W. & Klein, J. (1978) The lymphoreticular system intriggering virus plus self-specific cytotoxic T cells: evidence for Thelp. Journal of Experimental Medicine, 147, 897–911.