Embed Size (px)
Citation preview

The clinical implication of monoclonal gammopathiesmonoclonal gammopathy of undetermined significance andmonoclonal gammopathy of renal significance
Krzysztof Batko1 Jolanta Malyszko2 Artur Jurczyszyn3 David H Vesole4 Morie A Gertz5 Xavier Leleu6Anna Suska3 Marcin Krzanowski1 Władysław Sułowicz1 Jacek S Malyszko7 and Katarzyna Krzanowska1
1Departament of Nephrology Jagiellonian University Medical College Krakow Poland 2Department of Nephrology Dialysis and InternalMedicine Warsaw Medical University Warszawa Poland 3Departament of Hematology Jagiellonian University Medical College KrakowPoland 4Myeloma DIvision John Theurer Cancer Center Hackensack University Medical Center Hackensack NJ USA 5Division ofHematology Mayo Clinic Rochester MN USA 6Service dHematologie CHU Hopital de la Miletrie Poitiers France and 71st Department ofNephrology Medical University Bialystok Poland
Correspondence and offprint requests to Jolanta Małyszko E-mail jolmalpocztaonetpl jmalyszkowumedupl
A B S T R A C T
Monoclonal gammopathy of renal significance (MGRS) hasintroduced a new perspective to several well-known diseaseentities impacting nephrology haematology and pathologyGiven the constantly changing disease spectrum of these enti-ties it is clinically imperative to establish diagnostic and treat-ment pathways supported by evidence-based medicineMGRS is a disease of the kidney secondary to plasma cellclonal proliferation or immune dysfunction requiring thera-peutic intervention to eradicate the offending clone To fullyunderstand the disease(s) it is prerequisite to determine thesignificance of the findings The diagnostic work up should beextensive due to the wide heterogeneity of clinical presenta-tion ultimately necessitating kidney biopsy Particular patientprofiles such as AL amyloidosis which may be diagnosedthrough biopsies of other tissuesorgans may be an exceptionTreatment decisions should be formulated by multi-disciplinary consensus nephrologists haematologists andpathologists The ultimate goal in managing MGRS is eradica-tion of the offending plasma cell clone which requires targetedchemotherapy and in eligible cases haematopoietic stem celltransplantation We present a review of diagnostic proce-dures treatment options and advances in the last few years inthe management of MGRS in an effort to acquaint specialistswith this new face of several older diseases
Keywords amyloidosis kidney function monoclonal gamm-opathy of renal significance monoclonal gammopathy ofundetermined significance multiple myeloma
D I A G N O S I S O F M O N O C L O N A LG A M M O P A T H Y O F U N D E T E R M I N E DS I G N I F I C A N C E
Monoclonal gammopathy of undetermined significance(MGUS) is a benign plasma cell dyscrasia first coined by Kyle[1] referring to his initial observations of an asymptomatic pa-tient with increased risk for plasma cell malignancy The cur-rent diagnostic criteria define MGUS as a plasma cell dyscrasiawith a serum protein electrophoresis (SPEP) lsquoM proteinrsquo in se-rum lt30 gL and bone marrow infiltration of clonal plasmacells lt10 with no disease-related end-organ damage [2] In ahistorical series in Olmsted County Minnesota the prevalenceof MGUS was estimated to be 32 for people aged 50 and53 in those aged70 [3] Prevalence in a US population sam-ple of ages 10ndash49 was 034 while estimates for persons aged50 are 24 with differences from the Minnesota populationattributed to geographical variability [4 5] Registry investiga-tions by Cabrera et al [6] projected the world standardized in-cidence to be 376 per 100 000 residents increasing with ageOlmsted County data estimates for annual incidence are 120and 60 per 100 000 for males and females aged 50 increasing to530 and 370 at age 90 respectively [7] MGUS is conventionallymanaged by monitoring SPEPurine protein electrophoresis(UPEP) scaled to risk assessment with treatment withheld untilthe development of SLiM-CRAB criteria (see below)
Transformation of MGUS has a cumulative annual risk pro-gression of 1 [8] However the frequency varies based on agerace and gender [3ndash6] Depending on the subtype of MGUS
VC The Author(s) 2018 Published by Oxford University Press on behalf of ERA-EDTA All rights reserved 1
RE
VIE
W
Nephrol Dial Transplant (2018) 1ndash13doi 101093ndtgfy259
Downloaded from httpsacademicoupcomndtadvance-article-abstractdoi101093ndtgfy2595086133by gueston 29 August 2018
the relative risk and nature of progression varies For IgMMGUS the relative risk for any progression is 108 most oftento Waldenstromrsquos macroglobulinaemia AL amyloidosis andnon-Hodgkinrsquos lymphoma Progression for non-IgM MGUScommonly arising from plasma cells after switch recombina-tion has a reported renal response (RR) of 57 leading to multi-ple myeloma (MM) plasmacytoma and AL amyloidosisrespectively [8] Progression to an MGUS-related disorder notaccounting for death to co-morbidities is estimated to be 10at 10 years and 18 at 20 years [8] MGUS risk can be stratifiedon three factors abnormal serum free light chain (sFLC) ratioM protein 15 gdL and immunoglobulin isotype Dependingon the number of these risk factors (0ndash3) the projected risk ofprogression ranges from 7 to 55 at 20 years [8]
Analysis of the Olmsted County cohort showed a prevalenceof 08 for light chain MGUS with 23 of patients developingrenal disease [9] Steiner et al [10] have shown that monoclonalgammopathy of renal significance (MGRS) patients are at in-creased risk of progression to MM than MGUS patients withmedian time to progression at 188 years Risk stratification isan estimate and these patients require life-long monitoringAmong 2935 MGUS patients MGRS was detected in 15with an estimated 10 risk of progression within 1 year after di-agnosis Due to the rarity and heterogenous presentation reli-able biomarkers are exceptionally difficult to find Perhaps abetter understanding of the disease pathogenesis will allow us todiscriminate high-risk patients Recently a prospective trial of331 asymptomatic monoclonal gammopathy patients(MGUSfrac14 152) analysed with clinical variables and gene ex-pression profiles demonstrated genomic features to predicthigh-risk disease suggesting the value of genomics in furtheringour understanding of myelomagenesis [11] Indeed aside frompredicting progression identifying risk for particular lesionsmay aid in discovering early stages of MGRS It is hypothesizedthat risk alleles for C3 glomerulopathy may require an instigat-ing trigger such as infection or monoclonal immunoglobulin(MIg) to develop the disease [12] Individuals with a high riskcould be screened more frequently and meticulously As of yetidentification of disease-related polymorphisms is largely lim-ited to an experimental setting
MM is defined as an M protein of gt30 gL or 10 clonalplasma cells Patients are screened for clinical manifestations ofMM under the acronym SLiM-CRAB bone marrow plasmacells60 involved to uninvolved sFLC ratio100 with abso-lute light chain100 mgL orgt1 focal lesions on magnetic res-onance imaging (MRI 5 mm) hypercalcaemia renaldysfunction anaemia and bone lesions [13] Approximately14 of individuals with MM have no SLiM-CRAB criteria andare designated smoldering myeloma an entity that is nottreated outside of the context of a clinical trial [14]
M G R S D I A G N O S I S
MGRS was introduced in 2012 Leung et al [2] noted that someindividuals who met the criteria for MGUS may have kidneydamage as a result of MIg production or of a fragment thereofThey termed the resulting pathological entity MGRS whichwas not considered to be a benign plasma cell clonal process
but one that was associated with end-organ damage and re-quired treatment [15] Thus the abridged definition of MGUSis the absence of renal lesions with their development warrant-ing re-definition as MGRS
I S M G U S E Q U I V A L E N T T O M G R S
MGRS encompasses an array of diseases linked to relatively be-nign proliferation of plasmaB cells with subsequent excessproduction of MIg or fragment thereof or paraprotein aggre-gating in renal tissues This may lead to loss of function and ul-timately renal failure It is usually secondary to plasma cellB-cell clonal expansion and may result in indirect complementdysregulation [12] In the absence of treatment the renal dam-age due to deposits in tubules and glomeruli is progressive andresults in irreversible damage where therapy to reverse renaldysfunction will no longer be effective [16] Approximately72 of MGRS patients have progressing renal insufficiency[10] Mortality may relate not only to an elevated risk of devel-oping chronic kidney disease (CKD) but also to malignancyinfection or other organ dysfunction [16 17] In 2005ndash2011 themedian MM survival rates were estimated at 54 monthswhereas when MM was associated with moderate to severe re-nal impairment (RI) they were 44 and 32 months respectively[18]
Kidney biopsy is required for the diagnosis of MGRS to in-clude immunohistochemistry immunofluorescence (IFE) andelectron microscopy (EM) [16 19] Lin et al [20] studiedpatients with monoclonal immunoglobulin deposition disease(MIDD) where 39 presented with MGUS Findings in kidneybiopsy preceded clinical diagnosis of dysproteinaemia in 68 ofall cases and 15 plasma cells was found only in 35 In 28cases of membranoproliferative glomerulonephritis (MPGN)with abnormal electrophoresis 16 patients were classified asMGUS on the basis of bone marrow biopsy and clinical imageRenal biopsy specifically IFE was described by the authors ascritical in initiating the evaluation for a gammopathy [21]Serum electrophoresis may be negative while biopsy indicates asetting of monoclonal gammopathy Depending on the diseaseentity evidence of MGRS may only consistently be foundthrough kidney biopsy In proliferative glomerulonephritis(PGN) with monoclonal IgG deposits (PGNMID) and non-IgGPGN detection of a circulating MIg is reported at best at 32combined with a low overall yield of bone marrow examination(25) [22] It is hypothesized that the small size of clonal popu-lations is beyond the detection limit of current methods andorthey are located in extramedullary lymphoid tissue
Finding nodular mesangial sclerosis in only 23 of MIDDcases highlights the need for methodical IFE analysis [23 24]In light chain deposition disease (LCDD) with minimal to noproteinuria nodular sclerosis was found in only 14 of cases[25] Although not a diagnostic criterion it is a common char-acteristic in light microscopy Furthermore defining the sub-type of MIDD requires IFE while diagnosis is set on IFEEMEM is estimated to be necessary in setting a correct diagnosis inapproximately 11ndash21 of renal lesions while in another 21ndash36 it may confirm or provide additional information [26]There are cases where the pathological protein may be hidden
2 K Batko et alDownloaded from httpsacademicoupcomndtadvance-article-abstractdoi101093ndtgfy2595086133by gueston 29 August 2018
and requires a specific approach In a review of 40 crystallineLCPT cases (21 patients classified to MGRS) paraffin IFE withprotease digestion antigen retrieval technique was required forcorrect diagnosis [27] Furthermore in biopsy findings of C3GN or membranoproliferative GN paraffin immunofixation(IF) with protease digestion may unmask MIg deposits and dis-cover MGRS [28]
Extrarenal lesions in MGRS are not uncommon Amyloiddeposits can be limited to the vasculature marking a differentclinical profile [29] In patients with C3 GN associated withmonoclonal gammopathy C3 deposits may coexist in renal andcutaneous vessels [30] Perhaps better understanding of patho-genesis will allow for targeting the mechanism of tissue injuryIn LCDD extrarenal manifestations may occur in the heart andliver [31 32] Cardiac manifestations are reported in 13 of MMpatients with LCDD and are associated with shorter survivaland worse treatment outcomes It is important to note that 85of those patients had MM while in studies where MM rateswere lower [23 24] the rate of cardiac involvement was only10 In rare cases LCDD patients may present without pro-teinuria with tubulointerstitial lesions where nephrologistsmight not screen for monoclonal gammopathy [25]Nephrologists and pathologists should closely cooperate withatypical and typical manifestations of rare diseases In 13 ofIgAndashPGNMID patients the initial diagnosis was IgA nephropa-thy despite the presence of MIg glomerular deposits resultingin a lack of haematological evaluation which is crucial inMGRS [33] Another difficulty in diagnosis may be related tomembranous nephropathy with singular monoclonal IgGwhich requires staining for phospholipase A2 receptor beforeinvestigating a low-grade malignancy [34]
I N V E S T I G A T I O N I N T O M G R S
Presenting symptoms should be closely evaluated and docu-mented MGUS is more commonly seen in older individuals asare metabolic disorders which can mimic MGRS clinicallyUnexplained RI or abnormalities such as proteinuria requireextensive testing AL amyloidosis is suspected with albuminuria(gt50 in urine electrophoresis) nephrotic syndrome and rela-tively preserved kidney function as opposed to MIDD [35]Cryoglobulinaemia (CG) Type I may present with hyperviscos-ity linked symptoms and Type II with skin lesions and vasculi-tis [36] The latter may be related to hepatitis C virus infectionin which case antiviral therapy should be promptly initiated [2]MIDD commonly causes asymptomatic multi-organ involve-ment [16]
SPEP is the most basic quantitative screening test for mono-clonal proteins owing to its general availability and low costSPEP is positive in 819 of MGUS 659 of AL and 556 ofLCDD [37] To increase sensitivity in MGRS it should alwaysbe combined with IF and respective urine studies UPEP andurine IF [16] IF is purely qualitative but it allows for identifica-tion of the MIg isotype Due to low disease burden of MGRS apossible migration of M proteins to different fractions and ahigh limit of detection in SPEP (500 mgL) compared with IF(150 mgdL) a negative SPEP does not exclude MGRS andshould be used together IF [38] Despite lower overall sensitivity
to SPEP the rationale for including the UPEP can be drawnfrom characteristic patterns which may be indicative of a pri-mary disease such as high urine albumin excretion in MIDD orAL amyloidosis or use in monitoring RI in MM [39 40] Theadditional use of antibodies targeting epitopes of sFLC detectscases missed by urine assay though it is also true for the reverseas such both assays cannot be replaced [37] Urine free lightchain assays should not be utilized as there are no establishednormal ranges [41] The established normal range for thekappalambda ratio is 026ndash165 whereas in patients with renaldysfunction a range of 034ndash31 is considered normal [42] Ithas been suggested that the lower threshold should be raised forproliferative glomerulonephritides with non-organized glomer-ular MIg deposition [22] sFLC should be assessed with theknowledge that kappa monomers are more easily filtered com-pared with lambda dimers Renal dysfunction defined as an ab-normal creatinine clearance (CrCl) results in elevated sFLCthough usually but not always with a maintained kappalambdaratio (21) [43] Thus all instances of a abnormal sFLC valuesshould not be immediately attributed to a monoclonal gamm-opathy [44] In a retrospective data review of 76 MGUS (295observations) patients sFLCs were observed with agt55 false-negative ratio compared with electrophoretic studies [45]Conversly Fulton et al [46] analysed 219 cases with all urineand serum studies to a conclusion of sFLC and SPEP detecting6 more cases than SPEPIF and UPEPIF Several authorshave indicated that studies criticizing IFE may use incorrectmethodology while urine studies are of equal sensitivity andmay be more useful in low burden light chain clones especiallylambda dominant [47 48] Katzmann et al [37] observed thatSPEP and sFLC is the most effective basic screening panel inidentifying several MGRS conditions In LCDD 42 of patientspresented with no abnormalities in SPEPIFE but FLCs wasraised in all and matched the isotype in biopsy [25] FLCs arenot universally accepted and must be performed in combina-tion with urine and serum studies A cut-off value of kappalambda ratio gt289 of 92 sensitivity and 97 specificity areestablished for plasma cell malignancy at an estimated glomeru-lar filtration rate (eGFR) lt60 mLmin173 m2 howeverMGRS specific light chain values require further study [49] In17 MGRS patients with nephritic range proteinuria serum andurine IF with sFLC was 100 sensitive Although three patientswith chronic glomerulonephritides were identified by sFLC andserum IF the results do not reliably reflect the spectrum ofMGRS In PGNMIDnon-IgG GN the detection rate is esti-mated at 32 for serum IF and sFLC [22 50] Another study on19 PGNMID patients reported an overall paraprotein andclonal detection rate of 37 and 32 respectively [51] In thethese conditions if testing for either serum IFE or sFLC is posi-tive bone marrow investigation with flow cytometry and im-munohistochemical study may uncover a pathological cloneDetermination of the best diagnostic algorithm is difficult and ifthere is a strong suspicion of MGRS all five tests should be or-dered At present there is no standard testing for the heteroge-nous presentation(s) of MGRS due to different diseasesubtypes
Clinical implication of monoclonal gammopathies 3Downloaded from httpsacademicoupcomndtadvance-article-abstractdoi101093ndtgfy2595086133by gueston 29 August 2018
Without chemotherapy there is a high recurrence rate ofMGRS conditions post-renal transplant and prioritizing func-tional improvement requires early diagnosis as opposed to thepassive monitoring in MGUS [2] (Table 3) Recent advancespoint to time of flight mass spectrometry (MS) without theneed for expensive proteomic analysis though the ability to dis-criminate and identify the pathological protein has to be dem-onstrated [52] Laser microdissection and MS proteomics arerecommended to confirm AL amyloidosis cases of abnormalMIDD with truncated MIg or instances where the specific MIgregion is of interest [19 42] Urinary exosomes which have dif-ferent characteristics in AL amyloidosis and MGUS combinedwith MS may become the diagnostic and monitoring tools aftermore evidence is available [53] In daily practice parameters ofkidney function creatinine and proteinuria can be comparedwith assessment of the course of progression and response totreatment [54] However first-line monitoring should includeparaprotein levels and indirect disease activity markers whichtrack evolution of the primary disease
Non-invasive screening tools for on-going diagnosis of plasmacell dyscrasia particularly in difficult to identify MGRS condi-tions are of interest Vij et al [55] reported on deep sequencingof peripheral blood demonstrating clonal plasma cells in 96 ofMM patients In the case of IgM MGRS which suggests the pres-ence of B-celllymphoplasmacytic clone it is necessary to attemptto specify the clonal population through bone marrow andorlymph node biopsy and radiographic imaging [2 16] F18 posi-tron emission computed tomography can identify potential ab-normal lymph nodes for biopsy in conjunction with peripheralblood flow cytometry [54] MRI to exclude marrow involvementmay also be considered With the heterogeneity of MGRS asidefrom determining the conclusive histopathology character exclu-sion of plasma cell malignancy is necessary
T R E A T M E N T F O R M G R S mdash A N O V E R V I E W
A multi-disciplinary collaboration between nephrologist pa-thologist and haematologist is a priority in the diagnosis andtreatment of these individuals Therapy should incorporate bi-opsy-driven diagnosis with particular clinical features and dis-ease course prediction Identification of the clone responsiblefor MGRS and appropriate haematological treatment shouldtranslate into better RR and prevention of progression MGRSpatients with doubled serum creatinine or reduced renal func-tion may be at higher risk of haematological progression (oddsratio 26 CI 03ndash24) [10] In MM the reversal of RI has beenshown to improve outcome [56] Treatment of CD20thorn clonesshould utilize rituximab (RTX) while MGRS conditions par-ticularly non-IgM MGRS should consider MM regimens asprovided below and summarized in Table 1 With the rarityand wide array of MGRS conditions establishing strong evi-dence for treatment is difficult and evidence is limited to anec-dotal cases or small patient series
C Y T O T O X I C D R U G S
Historically melphalan-prednisone (MP) was used for thetreatment of plasma cell dyscrasias but due to the low response T
able
1T
hera
peut
icre
gim
ens
for
prim
ary
MG
RS
con
diti
ons
Dru
gC
hara
cter
Dis
ease
char
acte
rSe
veri
tyof
kidn
eyin
suff
icie
ncy
Ref
eren
ce
Lena
lidom
ide
LoD
exM
PT
Clin
ical
tria
lM
Mw
ith
RI
149
pati
ents
CrC
llt30
mL
min
372
pts
CrC
l30
lt50
Dim
opou
los
etal
[57
]B
enda
mus
tine
PV
Ret
rosp
ecti
veM
Mw
ith
RI
18eG
FRlt
35m
Lm
in(1
1pt
seG
FR15
mL
min
)P
onis
chet
al[
58]
RT
XC
YC
Dex
Ret
rosp
ecti
veIn
dole
ntN
HL
Glo
mer
ulon
ephr
itis
rela
ted
toM
Ig14
pts
(71
5w
ith
eGFR
lt60
mL
min
)P
erry
etal
[59
]
PO
ML
oDex
Clin
ical
tria
lR
elap
sed
refr
acto
ryM
Mw
ith
RI
Thr
eeco
hort
smdash33
eGFR
30ndash4
5m
Lm
inpt
s34lt
30m
Lm
ineG
FRpt
s14
HD
pts
Dim
opou
los
etal
[60
]
RT
XC
linic
altr
ial
Mem
bran
ous
neph
ropa
thy
eGFR
40P
rote
inur
ia
5g
24h
Ferv
enza
etal
[61
]V
MP
vers
usM
PC
linic
altr
ial
MM
wit
hR
I34
ptslt
30m
Lm
inG
FR1
93pt
sG
FR31
ndash50
mL
min
Dim
opou
los
etal
[62
]V
MP
TndashV
Tve
rsus
VM
PC
linic
altr
ial
MM
wit
hR
I33
ptslt
30m
Lm
ineG
FR1
16pt
seG
FR31
ndash50
mL
min
Mor
abit
oet
al[
63]
Ixaz
omib
Lena
lidom
idendash
Dex
Clin
ical
tria
lR
efra
ctor
yre
laps
edM
M10
pts
CrC
llt30
mL
min
169
pts
CrC
l30ndash
60m
Lm
inM
orea
uet
al[
64]
Ben
tam
usti
nem
onot
hera
py
wit
hR
TX
Ret
rosp
ecti
veC
LLN
HL
104
pts
CrC
llt40
mL
min
Nor
dstr
omet
al[
65]
Vve
rsus
IMiD
vers
usC
CC
linic
altr
ial
MM
wit
hR
I55
pts
CrC
llt30
mL
min
(9di
alys
is)
41pt
sC
rCl
30lt
50m
Lm
inR
ouss
ouet
al[
66]
T-D
exC
linic
altr
iald
ata
MM
wit
hR
Ipr
ior
toA
SCT
(ind
ucti
onth
erap
y)16
pts
CrC
llt30
mL
min
15
pts
CrC
l30ndash
50m
Lm
in(t
otal
7on
HD
)T
osie
tal
[67]
L-D
exT
wo
clin
ical
tria
lsM
MR
Ive
rsus
non-
RI
16pt
sC
rCllt
30m
Lm
inC
rCl
30lt
60in
82pt
sD
imop
oulo
uset
al[
68]
PO
Mndashl
owD
exT
hree
clin
ical
tria
lsM
Mw
ith
RI
355
pts
wit
hC
rCl
30an
dlt
60m
Lm
in(1
66pt
sC
rCl
30lt
45)
Sieg
elet
al[
69]
Car
filzo
mib
Dex
vers
usB
orte
zom
ibD
exC
linic
altr
ial
Rel
apse
dre
frac
tory
MM
56pt
sC
rCllt
30m
Lm
in1
28pt
sw
ith
CrC
l30ndash
50m
Lm
inD
imop
oulo
set
al[
70]
Vb
orte
zom
ibM
mel
phal
anL
len
alid
omid
eT
tha
lidom
ide-
dexa
met
haso
ne
Vb
orte
zom
ibC
Cc
onve
ntio
nalc
hem
othe
rapy
CLL
chr
onic
lym
phoc
ytic
leuk
aem
iaN
HL
non-
Hod
gkin
lym
phom
apt
spa
tien
ts
4 K Batko et alDownloaded from httpsacademicoupcomndtadvance-article-abstractdoi101093ndtgfy2595086133by gueston 29 August 2018
rates has been replaced by more potent regimens In LCDDwith MGUS MP and plasmapheresis prolonged survival how-ever kidney function deteriorated which marks the inefficiencyof the old regimes
To achieve a higher and more durable haematological re-sponse (HR) and potentially to qualify for kidney transplant(Ktx) high-dose melphalan supported with autologous stemcell transplantation (ASCT) is considered highly efficacious inMM and AL SCT has been shown to improve survival in ALamyloidosis and MIDD [71 72] Achieving a very good partialresponse (VGPR)complete response (CR) is associated with abetter RR rate than a HR lt VGPR [31 32 73] Importantly anadvanced impairment of renal function may impact responseindependently of achieving HR [32 74] Preventing renal dam-age will likely only be achieved by earlier diagnosis
I M M U N O M O D U L A T O R Y A G E N T S
Thalidomide the first immunomodulatory drug (IMiD) agentapproved for the treatment of myeloma can be safely adminis-tered regardless of renal function Outside the USA thalido-mide remains a viable choice in CrCl lt50 mLmin1 73 m2since it is not renally cleared [67] Song et al [75] report that inpatients with a low glomerular filtration rate (GFR) defined aslt40 mLmin173 m2 cyclophosphamide (CYC) was betterthan MP when combined with thalidomide with regard to re-nal functional improvement adverse events overall survival(OS) and mortality due to infection (P lt 0001) Lenalidomideis renally cleared and doses need to be adjusted for renal insuffi-ciency (CrCl lt60 mLmin) Complete blood counts should beperformed on a regular basis in the setting of moderate to severerenal insufficiency so that the lenalidomide dose may be modi-fied in the setting of unacceptable cytopenias [68] In a study of41 AL amyloidosis patients treated with lenalidomide 66were observed with kidney dysfunction and 10 required dialy-sis [76] However for approximately 25 of patients the initialdoses were too high and for half dosage was not appropriatelyadjusted Another aspect was older age and worse renal statusin those who experienced more severe impairment Recently alarge MM trial reported that renal function-adapted lenalido-mide dose resulted in similar safety across all levels of RI(Table 1) [57]
Pomalidomide (POM) is effective in lenalidomide-refractorycases and suitable for any CrCl (Table 1) However the recom-mendation for patients on dialysis is 3 mg rather than the stan-dard 4 mg dose and should be administered following dialysis[77] The latest results of POM and low-dose dexamethasone(LoDex) showed acceptable safety of 4 mgday in patients witheGFRlt30 mLmin173 m2 and on dialysis though CR wasonly achieved in eGFR 30ndash45 mLmin173 m2 [60] IMiDshave been used with effectiveness in MM AL amyloidosisMIDD CG Type 1 and LCPT (Tables 1 and 2) [27 31 85]
P R O T E A S O M E I N H I B I T O R S mdash N O V E L D R U G S
In 2015 bortezomib a first-generation proteasome inhibitorwas established as a class 1 A treatment (BDex) standard by theEuropean Myeloma Network for MM with RI [86] Bortezomib
showed a favourable profile with metabolism independent ofkidney function and demonstrated to be beneficial in advancedrenal failure and dialysis [87 88] A systematic review in 2014concluded that bortezomib was preferable to other agents inMM with RI [89] The most prominent adverse event is periph-eral neuropathy which may be a troublesome side effect in of-ten mildly symptomatic MGRS conditions Bortezomibpromotes a high rate of haematological CR as well as RR inMM with RI [90] High-dose Dex is linked to a faster RR how-ever mildly symptomatic MGRS patients may not be willing tocomply with the side effects whereas treatment-wise achievinga faster RR may improve the disease course [88] Bortezomibhigh-dose Dex is recommended by the IMWG for patients withMM-related RI whereas a three-drug scheme is deemed to im-prove RR [91]
In 50 patients with C3 glomerulopathy associated withmonoclonal gammopathy chemotherapy effectively achievedHR the only predictor of RR in multivariate analysis into sig-nificantly higher RR and renal survival rates compared withstandard immunosuppression [92] Bortezomib-based regimesmade up 76 of the chemotherapy group also being signifi-cantly associated with RR in univariate analysis Bortezomib-based treatment in 49 patients with MIDD reported at least aVGPR in 704 with HR not significantly different fromHDMSCT [93] Maintained haematological remission was as-sociated with survival in all patients at 85 months follow-up incomparison with 52 at 48 months in a series published in2003 [74] Ziogas et al [94] reported on 18 MIDD patientstreated exclusively with bortezomib regimes with gt VGPR in333 and an equal number progressing to end-stage renal dis-ease (ESRD) In the 2003 study by Pozzi et al progression wassimilar at 368 suggesting that even late induction of noveltherapy will not overcome poor prognosis associated with ad-vanced renal insufficiency The higher efficacy reported byCohen et al may be explained by overall less advanced kidneyfailure and proteinuria Together the studies demonstrate thatprevention of poor kidney function is necessary to treat effec-tively regardless of treatment regime
Recently the spectrum of MGRS has been reviewed in thecontext of monoclonal IgA deposits RTX did not elicit a RRwhile bortezomib-based treatment was suggested as first-linestrategy [33] Of 22 LCPT patients six MGRS patients weretreated with bortezomib-based regimes with 333 reaching atleast VGPR while the remainder had stable disease [27]Untreated patients progressed to ESRD while multivariateanalysis showed initial eGFR to be the only predictor of renalfunction This brings further support to prioritizing early detec-tion and subsequent chemotherapy to prevent deterioration ofkidney function In AL amyloidosis CyBorDBDex is stem cellspairing and therefore can be used in patients who may yetqualify for SCT as well as renal failure [95] In 53 patients withLCDD of which 57 were in Stage 45 CKD achieving at leasta VGPR improved renal outcome with bortezomib-based regi-mens achieving CR in eight out of nine cases [31] MIDD haspreviously been reported with poor outcomes and progressionto ESRD [24] Kourelis et al [73] studied 88 patients withMIDD (42 MGRS) of which 69 presented with eGFR
Clinical implication of monoclonal gammopathies 5Downloaded from httpsacademicoupcomndtadvance-article-abstractdoi101093ndtgfy2595086133by gueston 29 August 2018
lt30 mLmin1732 reporting proteasome inhibitorSCT as themost feasible therapeutic choice Achievement of completevery good partial HR was necessary for a RR while RR was anindependent predictor of progression again highlighting theprinciples of MGRS treatment In patients with PGNMID whodo not respond to initial treatment with RTXCYC and ste-roids bortezomib-based treatment may elicit a response [51]Bortezomib-based therapy was effective even in refractory casesof CG Type 1 related to MM [85 96 97]
Carfilzomib is a second-generation proteasome inhibitorDimopoulos et al [98] reported that carfilzomib-based therapyimproved renal outcome in 55 of patients with eGFRlt60 mLmin173 m2 Renal function may initially temporarilydecrease though therapy improves renal function A cardiacrisk profile should be treated with exceptional care Patient pro-file assessment and further studies will determine the use inMGRS
M O N O C L O N A L A N T I B O D I E S
Patients with MGUS treated with RTX and prednisone had im-proved kidney function and decreased proteinuria In patientswith MPGN secondary to indolent clones RTX CYC andprednisone were more effective then RTX with steroidsmono-therapy [99] Therapeutic doses of monoclonal antibodies maybe administered even in renal failure and post-renal allograftsettings [100 101] In seven patients with glomerulonephritiswith monoclonal IgG deposits RTX has been observed withpromising results [five achieved CR two partial response (PR)][102] The added benefit of RTX over classic chemotherapyrelates to a more tolerable profile Treatment of 14 PGNMIDpatients in approaches of clone-directed and empirical therapywithout identifiable discrasia was effective with patients withno detectable clone responding with complete and PSs in allbut two cases Bortezomib-based therapy may be effective innon-responders While empirical treatment is not easily under-taken with clonal detection at 25ndash32 it seems justified con-sidering the rate of response [22 51] However the studypopulation is not robust and the benefitsafety of such an ap-proach is in need of confirmation by larger studiesInterestingly patients with eGFR 20 had similar rates of CRPR to eGFR45 and all patients were free of ESRD in follow-up underscoring the value of a haematological treatment ap-proach in MGRS [51] RTXndashCYCndashDex use in 14 patients withMIg-associated glomerulopathy secondary to indolent non-Hodgkin lymphomas was reported on with 64 achieving CR(Table 1) The antiproteinuric effect of RTX is another benefi-cial aspect A steroid-free regimen of bendamustine and RTXprospectively assessed in indolent B-cell lymphoma of renalsignificance resulted in 85 achieving a haematological CRand 75 a complete RR [103] Patients without RR did notachieve HR Bendamustine is primarily cleared by hydrolysiswith minimal kidney involvement and recently there is sub-stantial evidence suggesting its safety in advanced renal failurethough complete blood counts should be monitored for haema-tological abnormality [104 105] (Table 1) RTX should be con-sidered in patients with IgM-associated MGRS especially when
Tab
le2
AL
base
dre
gim
ens
for
trea
tmen
tof
MG
RS
Dru
gP
atie
nts
and
met
hods
Out
com
esC
oncl
usio
nsR
efer
ence
VC
Dve
rsus
VD
101
pts
AL
amyl
oido
sis
(11
rena
lSta
ge3)
Sim
ilar
HR
(Pfrac14
026
)R
R43
fo
rV
Dve
rsus
41
for
VC
D(Pgt
005
)si
mila
rsu
rviv
al(Pfrac14
045
)H
ighe
rdo
sing
ofD
exan
dC
YC
addi
tion
does
noti
m-
pact
ther
apy
outc
omes
sign
ifica
ntly
Kas
trit
iset
al[
78]
CV
Dve
rsus
CT
D13
9pt
sw
ith
AL
amyl
oido
sis
Hig
her
CR
inC
VD
(40
6ve
rsus
246
)
med
ian
PFS
280
vers
us14
0m
onth
sre
spec
tive
lyFa
stcl
onal
cont
rold
idno
tred
uce
earl
ym
orta
lity
Ven
ner
etal
[79
]
CyB
orD
230
pts
wit
h63
w
ith
rena
linv
olve
men
t60
H
R4
3V
GP
R2
5R
RE
ffica
ciou
sin
pati
ents
wit
hout
card
iac
invo
lvem
ent
sur-
viva
lis
depe
nden
ton
deep
resp
onse
Pal
ladi
niet
al[
80]
DA
RA
Ret
rosp
ecti
vere
view
of25
cons
ecut
ive
AL
pts
HR
in76
C
Rin
36
VG
PR
24
wel
ltol
erat
edev
enin
card
iac
pts
Effi
caci
ous
inhe
avily
pre-
trea
ted
Kau
fman
etal
[81
]
Pom
alid
omid
endashD
ex28
pts
wit
hA
Lam
yloi
dosi
s68
H
Rgt
VG
PR
in29
5
3w
ith
resp
onse
afte
r1
cycl
eA
noth
erch
oice
inre
frac
tory
AL
impr
oves
surv
ival
hae
-m
atol
ogic
alpr
ogre
ssio
npr
edic
tssu
rviv
alP
alla
dini
etal
[82
]
LMD
50A
Lam
yloi
dosi
spt
s62
w
ith
rena
lloa
d(4
inre
nalS
tage
III)
CR
18
VG
PR
32
OR
in48
h
aem
atol
ogic
and
card
iac
toxi
city
4
mor
talit
y1
case
ofac
ute
kidn
eyin
jury
len
alid
omid
edo
seha
sto
bem
onit
ored
and
adju
sted
oth
erw
ise
tole
rabl
ean
def
ficac
ious
Heg
enba
rtet
al[
83]
M-D
ex25
9A
Lam
yloi
dosi
spt
sH
R76
C
R31
in
high
dose
ver
sus
51an
d12
in
atte
nuat
edO
Ron
lyin
pati
ents
wit
hH
R(h
ighe
rin
CR
vers
usV
GP
R)
Pal
ladi
niet
al[
84]
VG
PH
Rv
ery
good
part
ialh
aem
atol
ogic
alre
spon
seE
GC
Ge
piga
lloca
tech
inga
llate
LM
Dl
enal
idom
ide
mel
phal
ande
xam
etha
sone
VC
Db
orte
zom
ibcy
clop
hosp
ham
ide
dexa
met
haso
neM
-Dex
mel
phal
ande
xam
etha
sone
6 K Batko et alDownloaded from httpsacademicoupcomndtadvance-article-abstractdoi101093ndtgfy2595086133by gueston 29 August 2018
Tab
le3
Mon
oclo
nal
gam
mop
athy
inth
ese
ttin
gof
kidn
eytr
ansp
lan
tati
on
Pat
ient
san
dm
etho
dsO
utco
mes
Con
clus
ions
Ref
eren
ce
27LC
PT
pati
ents
trea
ted
wit
hch
emo-
ther
apy
(11
SCT
)9
wit
hno
trea
tmen
tLo
wes
tm
orta
lity
best
HR
sin
SCT
tho
ugh
pati
ents
wer
eyo
unge
ran
dha
dbe
stin
itia
land
final
rena
lfu
ncti
on
Bes
tren
alou
tcom
eco
mpa
red
wit
hch
emot
hera
pyor
notr
eatm
ent
SCT
stab
ilize
dor
impr
oved
rena
lfun
ctio
nSt
okes
etal
[27
]
64M
IDD
pati
ents
16
pts
trea
ted
wit
hSC
T4
Ktx
3re
curr
ence
sin
4K
txpa
tien
tsr
ange
of7ndash
43m
onth
s38
pr
ogre
ssio
nto
ESR
Din
SCT
Hig
hcr
eati
nine
atbi
opsy
isas
soci
ated
wit
hpo
orou
t-co
me
chem
othe
rapy
afte
rre
curr
ence
isin
effic
ient
Nas
ret
al[
24]
49M
IDD
pati
ents
3K
txw
ith
1V
GP
Ran
d2
CR
18
SCT
No
recu
rren
ces
in3
Ktx
pati
ents
allo
graf
trej
ecti
onin
1pa
tien
taft
er3
year
sSC
Tw
assa
fean
dto
lera
ted
but
pati
ents
wer
eyo
unge
rbo
rtez
omib
-bas
edtr
eatm
enth
adsi
mila
rR
Rra
tes
Sust
aine
d
VG
PR
nece
ssar
yfo
rK
txS
CT
ispr
efer
red
CK
Dst
ages
Coh
enet
al[
93]
29M
PG
NK
txpa
tien
ts6
wit
hm
onoc
lona
lpro
tein
(4M
GU
S1
CLL
)23
of
MP
GN
pati
ents
have
mon
oclo
nalp
rote
ins
may
incr
ease
risk
ofre
curr
ence
SC
Tre
solv
edre
curr
ence
pl
asm
aphe
res
aspa
ssiv
em
aint
enan
ce
MP
GN
pati
ents
shou
ldbe
scre
ened
for
mon
oclo
nal
prot
eins
Lore
nzet
al[
110]
6LC
DD
wit
hSC
T1
pati
entd
idno
tsur
vive
SCT
all
othe
rsac
hiev
edH
R
2re
laps
esw
ith
1im
prov
edby
subs
eque
ntch
emot
hera
py
Insu
ffici
ent
resp
onse
toSC
Tm
aybe
anin
dica
tion
for
Ktx
inse
lect
pati
ents
afte
rac
hiev
ing
HR
Lore
nzet
al[
122]
7LC
DD
Ktx
pati
ents
Med
ian
recu
rren
ce2ndash
45m
onth
sfo
r5
pati
ents
sub
se-
quen
t4de
aths
onl
y1
pati
entf
ree
ofre
new
alA
HR
mus
tbe
achi
eved
befo
reat
tem
ptin
gK
txLe
ung
etal
[10
9]
2P
GN
MID
Ktx
pati
ents
(1de
novo
1re
curr
ent)
Impr
ovem
ent
ingr
aftf
unct
ion
and
seru
mcr
eati
nine
in2
year
follo
w-u
pR
TX
can
beef
fect
ive
inbo
thre
curr
enta
ndde
novo
PG
NM
IDpt
sM
erhi
etal
[12
3]
3P
GN
MID
(2C
LL)
Des
pite
RT
Xtr
eatm
entt
here
was
1pr
ogre
ssio
nto
ESR
Dan
don
em
alig
nanc
ypr
ogre
ssio
nR
TX
ther
apy
may
impr
ove
rena
lout
com
esin
shor
tter
mB
arbo
uret
al[
124]
53LC
DD
7K
tx1
6SC
T2
recu
rren
ces
inpa
tien
tsw
itho
utpr
ior
chem
othe
rapy
1
reje
ctio
nof
Ktx
3pa
tien
tsin
CR
ingt
68
year
follo
w-
up1
SCT
-rel
ated
deat
h13
15
achi
eved
CR
SCT
can
besu
cces
sful
even
inC
KD
Stag
e4
how
ever
re
nals
urvi
vali
sst
illw
orse
SC
Tap
pear
sm
ore
safe
than
inA
Lam
yloi
dosi
s
Saye
det
al[
31]
21K
txw
itC
3GN
667
re
curr
ence
ofw
hich
21
asso
ciat
edw
ith
mon
o-cl
onal
gam
mop
athy
rec
urre
nce
earl
ier
(36
mon
thm
e-di
anve
rsus
433
mon
th)
mor
epr
ogre
ssiv
eco
urse
(Pfrac14
NS)
SC
Tim
prov
edki
dney
func
tion
inon
epa
tien
tst
a-bl
egr
aft
in10
-yea
rfo
llow
-up
Mon
oclo
nalg
amm
opat
hypa
tien
tsar
eat
risk
ofan
ear-
lier
and
mor
eag
gres
sive
dise
ase
Zan
det
al[
125]
548
Ktx
pati
ents
Pre
vale
nce
81
52
year
med
ian
toM
GU
Sdi
scov
ery
high
erra
teof
MB
Lhi
stor
yof
infla
mm
ator
yki
dney
dis-
ease
aspr
edic
tive
fact
orn
oas
soci
atio
nw
ith
age
and
gend
ern
oim
pact
ongr
afts
urvi
val
over
alls
urvi
val
in-
cide
nce
ofm
alig
nanc
y
MG
US
pre-
and
post
-tra
nspl
antm
aybe
diff
eren
tcon
di-
tion
sin
term
sof
man
agem
ent
how
ever
str
ict
follo
w-u
pis
need
ede
spec
ially
inM
BL
pati
ents
Alfa
noet
al[
126]
159
3K
txre
cipi
ents
3pr
e-tr
ansp
lant
MG
(nfrac14
34)
No
case
sof
prog
ress
ion
noas
soci
atio
nw
ith
mal
igna
ncy
inci
denc
eor
mor
talit
yJi
men
ezZ
eped
aet
al[
117]
587
Ktx
reci
pien
ts2
9in
cide
nce
(9pt
spr
e-tr
ansp
lant
8po
st)
No
prog
ress
ion
duri
ng6-
year
follo
w-u
pM
GU
Sno
taco
ntra
indi
cati
onto
Ktx
Ban
cuet
al[
127]
351
8K
txre
cipi
ents
42pa
tien
ts(2
3pr
e-tr
ansp
lant
19
post
)m
edia
nsu
rviv
al26
1ve
rsus
280
year
sre
spec
tive
ly4
haem
atol
ogic
alm
a-lig
nanc
ies
deve
lope
din
pre
2P
TLD
gt15
year
spo
st-
tran
spla
nt
Dia
gnos
isof
PT
LDw
assy
mpt
om-b
ased
tru
ein
cide
nce
may
behi
gher
exc
lusi
onof
asso
ciat
edki
dney
dise
ase
and
mal
igna
ncy
isne
cess
ary
befo
reK
tx
Nai
naet
al[
118]
MB
Lm
onoc
lona
lB-c
elll
ymph
ocyt
osis
Clinical implication of monoclonal gammopathies 7Downloaded from httpsacademicoupcomndtadvance-article-abstractdoi101093ndtgfy2595086133by gueston 29 August 2018
CD20thorn cells can be identified while non-IgM-associated dis-eases more often require MM-like treatment
Recently an anti CD38 monoclonal antibody daratumumab(DARA) has been approved for the treatment of newly diag-nosed and relapsed MM patients [106] Like many Phase 3 reg-istration trials the study excluded patients with CrCl 20 mLmin Anecdotal evidence of safety and reduction of dialysis fre-quency in a patient with DARA monotherapy has recently beenreported [107] A case of PGNMID refractory to RTX and
bortezomib was successfully treated with DARA [108] Due toindependence of kidney clearance and positive results in RI itmay prove beneficial in MGRS There is an on-going Phase 2study of DARA in MGRS [NCT03095118]
M G R S T R A N S P L A N T A N D E S R D
Renal transplant in MGRS is controversial as frequent recur-rences are observed when the abnormal clone is not adequately
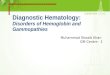
FIGURE 1 Diagnostic and therapeutic algorithm of monoclonal gammopathy of renal significance
8 K Batko et alDownloaded from httpsacademicoupcomndtadvance-article-abstractdoi101093ndtgfy2595086133by gueston 29 August 2018
suppressed [24 109 110] The current treatment paradigm inMGRS is to achieve a complete HR as a means of improvingpost-transplant outcome and preventing recurrence [71 72111] Cibeira et al [112] report that in 340 AL amyloidosispatients subject to SCT 43 attained CR improving long-termOS and organ response (OR) In recent years the treatment-re-lated mortality (TRM) has decreased from 138 between 1994and 2003 to 56 between 2004 and 2008 In part this probablyreflects the experience of established centres however with ac-cess to novel agents there are other options for treatmentCardiac involvement should be screened for in LCDD due to ahigh TRM (23) with SCT as opposed to non-cardiac patients[32] PS does not indicate treatment failure and significantlyincreases survival compared with patients lacking response[113]
A study in AL amyloidosis patients associated the need fordialysis within 30 days of SCT with highest early death risk andTRM Patients with both eGFRlt40 mLmin173 m2 and se-rum albumin lt25 mgdL had a 438 and 281 risk of requir-ing dialysis and chance of TRM respectively Identifying andscreening for such risk factors should improve the feasibility ofSCT in MGRS conditions [114] In a study of 36 patients withAL amyloidosisMIDD who were dialysis dependent for ESRDCR was reached in 53 at 1 year post SCT with an 8 TRM[72] Achievement of dialysis independence was possible inpatients receiving a Ktx after successful SCT Similarly a studyin MM with RI found no impact on survival for patients whowere dialysis dependent [115] Further research is required toevaluate risk factors and establish whether select ESRD patientsmay benefit from SCT
Literature reports are conflicting on the approach to Ktx inMGUS [116ndash118] Bansal et al [119] reflect that a select groupof plasma dyscrasia patients should be considered for Ktx espe-cially those subject to dialysis-associated complications In ALand MIDD patients achieving haematological CR have beenreported with successful Ktx [120 121] Monoclonal gammop-athy in the setting of Ktxs is presented in Table 3 In summaryprimary disease activity organ function and patient perfor-mance should dictate selection for Ktx We propose an algo-rithm for diagnostic and therapeutic treatment of MGRS(Figure 1)
C O N C L U S I O N
With under-recognition of the wide spectrum of MGRS accu-rate classification evidence-based therapy and expert estab-lished management is required Renal involvement in MGRSresults from the direct deposition of monoclonal protein and itslight- or heavy-chain fragments in the kidney IFE microscopyis essential to identify the offending monoclonal protein and itsrenal tissue distribution In selected cases MS is of valueMGRS therapy is directed to eliminate the clonal plasma cell orB-cell population Adverse events particular to the chosen drugshould complement the patient profile Early detection diagno-sis and chemotherapy may improve kidney function It shouldbe stressed that both the renal pathology and the underlyinghaematological disorders influence the management and
prognosis of MGRS Upon achieving HR ASCT and Ktx shouldbe considered as therapy endpoints in MGRS
C O N F L I C T O F I N T E R E S T S T A T E M E N T
None declared
R E F E R E N C E S
1 Kyle RA Monoclonal gammopathy of undetermined significance NaturalHistory in 241 Cases Am J Med [Internet] 1978 [cited 2017 Oct 24] 64814ndash826 Available from httpwwwncbinlmnihgovpubmed645746
2 Leung N Bridoux F Hutchison CA et al Monoclonal gammopathy of re-nal significance when MGUS is no longer undetermined or insignificantBlood [Internet] 2012 [cited 2017 Oct 24] 120 4292ndash4295 Available fromhttpwwwncbinlmnihgovpubmed23047823
3 Kyle RA Therneau TM Rajkumar SV et al Prevalence of monoclonalgammopathy of undetermined significance N Engl J Med [Internet] 2006[cited 2017 Oct 24] 354 1362ndash1369 Available from httpwwwncbinlmnihgovpubmed16571879
4 Landgren O Graubard BI Kumar S et al Prevalence of myeloma precur-sor state monoclonal gammopathy of undetermined significance in 12372individuals 10ndash49 years old a population-based study from the NationalHealth and Nutrition Examination Survey Blood Cancer J 2017 7 e618[cited 2018 Feb 9] 7 Available from httpwwwncbinlmnihgovpubmed29053158
5 Landgren O Graubard BI Katzmann JA et al Racial disparities in theprevalence of monoclonal gammopathies a population-based study of12 482 persons from the National Health and Nutritional ExaminationSurvey Leukemia [Internet] 2014 28 1537ndash1542 [cited 2018 Jun 22]Available from httpwwwncbinlmnihgovpubmed24441287
6 Cabrera Q Macro M Hebert B et al Epidemiology of monoclonal gamm-opathy of undetermined significance (MGUS) the experience from thespecialized registry of hematologic malignancies of Basse-Normandie(France) Cancer Epidemiol [Internet] 2014 38 354ndash356 [cited 2017 Oct24] Available from httpwwwncbinlmnihgovpubmed24880205
7 Therneau TM Kyle RA Melton LJ et al Incidence of monoclonal gamm-opathy of undetermined significance and estimation of duration beforefirst clinical recognition Mayo Clin Proc [Internet] 2012 [cited 2017 Dec23] 87 1071ndash1079 Available from httpwwwncbinlmnihgovpubmed22883742
8 Kyle RA Larson DR Therneau TM et al Long-term follow-up of mono-clonal gammopathy of undetermined significance N Engl J Med 2018[cited 2018 Apr 23] 378 241ndash249 Available from httpwwwncbinlmnihgovpubmed29342381
9 Dispenzieri A Katzmann JA Kyle RA et al Prevalence and risk of progres-sion of light-chain monoclonal gammopathy of undetermined significancea retrospective population-based cohort study Lancet [Internet] 2010[cited 2018 Feb 9] 375 1721ndash1728 Available from httpwwwncbinlmnihgovpubmed20472173
10 Steiner N Gobel G Suchecki P et al Monoclonal gammopathy of renalsignificance (MGRS) increases the risk for progression to multiple mye-loma an observational study of 2935 MGUS patients Oncotarget[Internet] 2018 [cited 2018 Apr 27] 9 2344ndash2356 Available from httpwwwncbinlmnihgovpubmed29416776
11 Dhodapkar MV Sexton R Waheed S et al Clinical genomic andimaging predictors of myeloma progression from asymptomaticmonoclonal gammopathies (SWOG S0120) Blood [Internet] 2014[cited 2018 Jun 22] 123 78ndash85 Available from httpwwwncbinlmnihgovpubmed24144643
12 Zand L Kattah A Fervenza FC et al C3 glomerulonephritis associatedwith monoclonal gammopathy a case series Am J Kidney Dis [Internet]2013 [cited 2017 Dec 29] 62 506ndash514 Available from httpwwwncbinlmnihgovpubmed23623956
13 Rajkumar SV Dimopoulos MA Palumbo A et al International MyelomaWorking Group updated criteria for the diagnosis of multiple myelomaLancet Oncol [Internet] 2014 [cited 2018 Jun 23] 15 e538ndashe548 Availablefrom httplinkinghubelseviercomretrievepiiS1470204514704425
Clinical implication of monoclonal gammopathies 9Downloaded from httpsacademicoupcomndtadvance-article-abstractdoi101093ndtgfy2595086133by gueston 29 August 2018
14 Ravindran A Bartley AC Holton SJ et al Prevalence incidence and sur-vival of smoldering multiple myeloma in the United States Nat PublishingGroup [Internet] 2016 6 2018ndash2023 [cited Jun] Available from httpswwwncbinlmnihgovpmcarticlesPMC5098258pdfbcj2016100apdf
15 Fermand J-P Bridoux F Kyle RA et al How I treat monoclonal gammop-athy of renal significance (MGRS) Blood [Internet] 2013 [cited 2017 Oct27] 122 3583ndash3590 Available from httpwwwncbinlmnihgovpubmed24108460
16 Bridoux F Leung N Hutchison CA et al Diagnosis of monoclonal gamm-opathy of renal significance Kidney Int [Internet] 2015 [cited 2017 Oct24] 87 698ndash711 Available from httpwwwncbinlmnihgovpubmed25607108
17 Kristinsson SY Bjorkholm M Andersson TM-L et al Patterns of survivaland causes of death following a diagnosis of monoclonal gammopathy ofundetermined significance a population-based study Haematologica[Internet] 2009 [cited 2018 Feb] 94 1714ndash1720 Available from httpwwwncbinlmnihgovpubmed19608666
18 Dimopoulos MA Delimpasi S Katodritou E et al Significant improve-ment in the survival of patients with multiple myeloma presenting with se-vere renal impairment after the introduction of novel agents Ann Oncol[Internet] 2014 [cited 2018 Apr 23] 25 195ndash200 Available from httpsacademicoupcomannoncarticle-lookupdoi101093annoncmdt483
19 Correia SO Santos S Malheiro J et al Monoclonal gammopathy of renalsignificance diagnostic workup WJN 2017 [cited 2017 Oct 27] 6 72ndash78Available from httpwwwncbinlmnihgovpubmed28316940
20 Lin J Markowitz GS Valeri AM et al Renal monoclonal immunoglobulindeposition disease the disease spectrum J Am Soc Nephrol [Internet] 2001[cited 2018 Jun 23] 12 1482ndash1492 Available from httpwwwncbinlmnihgovpubmed11423577
21 Sethi S Zand L Leung N et al Membranoproliferative glomerulonephritissecondary to monoclonal gammopathy Clin J Am Soc Nephrol [Internet]2010 [cited 2017 Dec 8] 5 770ndash782 Available from httpwwwncbinlmnihgovpubmed20185597
22 Bhutani G Nasr SH Said SM et al Hematologic characteristics of prolifer-ative glomerulonephritides with nonorganized monoclonal immunoglobu-lin deposits Mayo Clin Proc [Internet] 2015 [cited 2018 Jun 23] 90587ndash596 Available from httpwwwncbinlmnihgovpubmed25939936
23 Cohen C El-Karoui K Alyanakian M-A et al Light and heavy chain depo-sition disease associated with CH1 deletion Clin Kidney J [Internet] 2015[cited 2017 Oct 26] 8 237ndash239 Available from httpwwwncbinlmnihgovpubmed25815184
24 Nasr SH Valeri AM Cornell LD et al Renal monoclonal immunoglobulindeposition disease a report of 64 patients from a single institution Clin JAm Soc Nephrol [Internet] 2012 [cited 2018 Feb 9] 7 231ndash239 Availablefrom httpwwwncbinlmnihgovpubmed22156754
25 Sicard A Karras A Goujon J-M et al Light chain deposition disease with-out glomerular proteinuria a diagnostic challenge for the nephrologistNephrol Dial Transplant [Internet] 2014 [cited 2018 Jul 7] 29 1894ndash1902Available from httpwwwncbinlmnihgovpubmed24619059
26 Haas M A reevaluation of routine electron microscopy in the examinationof native renal biopsies J Am Soc Nephrol [Internet] 1997 8 70ndash76Available from httpwwwncbinlmnihgovpubmed9013450
27 Stokes MB Valeri AM Herlitz L et al Light chain proximal tubulopathyclinical and pathologic characteristics in the modern treatment era J AmSoc Nephrol [Internet] 2016 [cited 2018 Jun 23] 27 1555ndash1565 Availablefrom httpwwwncbinlmnihgovpubmed26374607
28 Larsen CP Messias NC Walker PD et al Membranoproliferative glomeru-lonephritis with masked monotypic immunoglobulin deposits Kidney Int[Internet] 2015 [cited 2018 Feb 10] 88 867ndash873 Available from httpwwwncbinlmnihgovpubmed26154922
29 Eirin A Irazabal MV Gertz MA et al Clinical features of patients with im-munoglobulin light chain amyloidosis (AL) with vascular-limited deposi-tion in the kidney Nephrol Dial Transplant [Internet] 2012 [cited 2018Feb 10] 27 1097ndash1101 Available from httpwwwncbinlmnihgovpubmed22067518
30 Alonso-Titos J Perea-Ortega L Sola E et al C3 glomerulonephritis associ-ated with monoclonal gammopathy of renal significance case report BMCNephrol 2018 Jul 6] 19 129 Available from httpwwwncbinlmnihgovpubmed29884135
31 Sayed RH Wechalekar AD Gilbertson JA et al Natural history and out-come of light chain deposition disease Blood [Internet] 2015 [cited 2017Dec 8] 126 2805ndash2810 Available from httpwwwncbinlmnihgovpubmed26392598
32 Mohan M Buros A Mathur P et al Clinical characteristics and prognosticfactors in multiple myeloma patients with light chain deposition diseaseAm J Hematol 2017 [cited 2018 Jul 7] 92 739ndash745 Available from httpwwwncbinlmnihgovpubmed28383130
33 Vignon M Cohen C Faguer S et al The clinicopathologic characteristicsof kidney diseases related to monotypic IgA deposits Kidney Int [Internet]2017 [cited 2018 Jul] 91 720ndash728 Available from httpwwwncbinlmnihgovpubmed28069266
34 Best Rocha A Larsen CP Membranous glomerulopathy with light chain-restricted deposits a clinicopathological analysis of 28 cases Kidney IntRep [Internet] 2017 [cited 2018 Jul 6] 2 1141ndash1148 Available from httpwwwncbinlmnihgovpubmed29270522
35 Nasr SH Valeri AM Sethi S et al Clinicopathologic correlations in multi-ple myeloma a case series of 190 patients with kidney biopsies Am JKidney Dis [Internet] 2012 [cited 2017 Oct 26] 59 786ndash794 Availablefrom httpwwwncbinlmnihgovpubmed22417785
36 Glavey SV Leung N Monoclonal gammopathy the good the bad and theugly Blood Rev [Internet] 2016 [cited 2017 Dec 24] 30 223ndash231 Availablefrom httpwwwsciencedirectcomsciencearticlepiiS0268960X15000946bb0130
37 Katzmann JA Kyle RA Benson J et al Screening panels for detection ofmonoclonal gammopathies Clin Chem [Internet] 2009 [cited 2017 Oct25] 55 1517ndash1522 Available from httpwwwncbinlmnihgovpubmed19520758
38 Yadav P Leung N Sanders PW et al The use of immunoglobulin lightchain assays in the diagnosis of paraprotein-related kidney disease KidneyInt [Internet] 2015 [cited 2018 Feb 9] 87 692ndash697 Available from httpwwwncbinlmnihgovpubmed25296094
39 Sugihara H Chihara D Seike K et al Percentage of urinary albumin excre-tion and serum-free light-chain reduction are important determinants ofrenal response in myeloma patients with moderate to severe renal impair-ment Blood Cancer J [Internet] 2014 [cited 2018 Jun 24] 4 e235 Availablefrom httpwwwncbinlmnihgovpubmed25083819
40 Leung N Gertz M Kyle RA et al Urinary albumin excretion patterns ofpatients with cast nephropathy and other monoclonal gammopathy-related kidney diseases Clin J Am Soc Nephrol [Internet] 2012 [cited 2018Jun 24] 7 1964ndash1968 Available from httpwwwncbinlmnihgovpubmed23024162
41 Ciocchini M Arbelbide J Musso CG Monoclonal gammopathy of renalsignificance (MGRS) the characteristics and significance of a new meta-entity Int Urol Nephrol [Internet] 2017 [cited 2017 Oct 26] 492171ndash2175 Available from httpwwwncbinlmnihgovpubmed28425076
42 Sethi S Rajkumar SV DrsquoAgati VD The complexity and heterogeneity ofmonoclonal immunoglobulinndashassociated renal diseases J Am Soc Nephrol2018 29 1810ndash1823
43 Hutchison CA Harding S Hewins P et al Quantitative assessment of se-rum and urinary polyclonal free light chains in patients with chronic kid-ney disease Clin J Am Soc Nephrol [Internet] 2008 [cited 2017 Dec 25] 31684ndash1690 Available from httpwwwncbinlmnihgovpubmed18945993
44 Jurczyszyn A Ochrem B Abnormal serum free light chain ratio does notalways indicate monoclonal gammopathy Polskie Archiwum MedycynyWewnetrznej [Internet] 2015 [cited 2017 Dec 29] 125 502ndash504 Availablefrom httpwwwncbinlmnihgovpubmed26266682
45 Singh G Serum free light chain assay and jk ratio performance inpatients with monoclonal gammopathy-high false negative rate for jk ra-tio J Clin Med Res 2017 [cited 2018 Jun 25] 9 46ndash57 Available fromhttpwwwncbinlmnihgovpubmed27924175
46 Fulton RB Fernando SL Serum free light chain assay reduces the need forserum and urine immunofixation electrophoresis in the evaluation ofmonoclonal gammopathy Ann Clin Biochem [Internet] 2009 [cited 2018Jun 25] 46 407ndash412 Available from httpwwwncbinlmnihgovpubmed19641008
10 K Batko et alDownloaded from httpsacademicoupcomndtadvance-article-abstractdoi101093ndtgfy2595086133by gueston 29 August 2018
47 Levinson SS Urine immunofixation electrophoresis remains importantand is complementary to serum free light chain Clin Chem Lab Med[Internet] 2011 [cited 2018 Jun 25] 49 1801ndash1804 Available from httpwwwncbinlmnihgovpubmed21663562 [CrossRef][Mismatch]
48 Lee WS Singh G Serum free light chains in neoplastic monoclonal gam-mopathies relative under-detection of lambda dominant KappaLambdaratio and underproduction of free lambda light chains as compared tokappa light chains in patients with neoplastic monoclonal gammopathiesJ Clin Med Res 2018 [cited 2018 Jun 25] 10 562ndash569 Available fromhttpwwwncbinlmnihgovpubmed29904440
49 Xu B Tang Y Zhou J et al Disease spectrum of abnormal serum free lightchain ratio and its diagnostic significance Oncotarget [Internet] 2017[cited 2017 Dec 29] 8 82268ndash82279 Available from httpwwwncbinlmnihgovpubmed29137262
50 Koo EH Shin J Jang HR et al Diagnostic performances of M-protein testsaccording to the clinical presentations of kidney disease Eur J Intern Med[Internet] 2016 [cited 2018 Feb 9] 33 88ndash92 Available from httpwwwncbinlmnihgovpubmed27421913
51 Gumber R Cohen JB Palmer MB et al A clone-directed approach mayimprove diagnosis and treatment of proliferative glomerulonephritis withmonoclonal immunoglobulin deposits Kidney Int [Internet] 2018 94199ndash205 Available from httpsdoiorg101016jkint201802020
52 Leung N Barnidge DR Hutchison CA Laboratory testing in monoclonalgammopathy of renal significance (MGRS) Clin Chem Lab Med [Internet]2016 [cited 2017 Oct 25] 54 929ndash937 Available from httpwwwncbinlmnihgovpubmed27107835 [CrossRef][Mismatch]
53 Ramirez-Alvarado M Ward CJ Huang BQ et al Differences in immuno-globulin light chain species found in urinary exosomes in light chain amy-loidosis (AL) PLoS ONE [Internet] 2012 [cited 2018 Jul 7] 7 e38061Available from httpwwwncbinlmnihgovpubmed22723846
54 Hogan JJ Weiss BM Bridging the divide an onco-nephrologic approachto the monoclonal gammopathies of renal significance Clin J Am SocNephrol [Internet] 2016 [cited 2017 Oct 26] 11 1681ndash1691 Availablefrom httpwwwncbinlmnihgovpubmed27416775
55 Vij R Mazumder A Klinger M et al Deep sequencing reveals myelomacells in peripheral blood in majority of multiple myeloma patients ClinLymphoma Myeloma Leuk [Internet] 2014 [cited 2017 Oct 25] 14131ndash139e1 Available from httpwwwncbinlmnihgovpubmed24629890
56 Gonsalves WI Leung N Rajkumar SV et al Improvement in renal func-tion and its impact on survival in patients with newly diagnosed multiplemyeloma Blood Cancer J 2015 [cited 2018 Feb 3] 5 e296 Available fromhttpwwwnaturecomdoifinder101038bcj201520
57 Dimopoulos MA Cheung MC Roussel M et al Impact of renal impair-ment on outcomes with lenalidomide and dexamethasone treatment in theFIRST trial a randomized open-label phase 3 trial in transplant-ineligiblepatients with multiple myeloma Haematologica [Internet] 2016 [cited2018 Jul 7] 101 363ndash370 Available from httpwwwncbinlmnihgovpubmed26659916
58 Ponisch W Andrea M Wagner I et al Successful treatment of patientswith newly diagnoseduntreated multiple myeloma and advanced renalfailure using bortezomib in combination with bendamustine and predni-sone J Cancer Res Clin Oncol 2012 [cited 2018 Jul 2] 138 1405ndash1412Available from httpwwwncbinlmnihgovpubmed22526157
59 Perry M Delarche A Ribes D et al Rituximab-cyclophosphamide-dexa-methasone is highly effective in patients with monoclonal Ig deposit-related glomerulopathy and indolent non-Hodgkin lymphomas Am JHematol 2014 [cited 2018 Jul 1] 89 969ndash973 Available from httpdoiwileycom101002ajh23798
60 Dimopoulos M Weisel K van de Donk Nwcj et al Pomalidomide pluslow-dose dexamethasone in patients with relapsedrefractory multiple my-eloma and renal impairment results from a Phase II trial J Clin Oncol2018 36 2035ndash2043
61 Fervenza FC Canetta PA Barbour SJ et al A multicenter randomized con-trolled trial of rituximab versus cyclosporine in the treatment of idiopathicmembranous nephropathy (MENTOR) Nephron [Internet] 2015 [cited2017 Dec 25] 130 159ndash168 Available from httpwwwncbinlmnihgovpubmed26087670
62 Dimopoulos MA Richardson PG Schlag R et al VMP (bortezomib mel-phalan and prednisone) is active and well tolerated in newly diagnosedpatients with multiple myeloma with moderately impaired renal functionand results in reversal of renal impairment cohort analysis of the Phase IIIVISTA study JCO 2009 [cited 2017 Dec 8] 27 6086ndash6093 Available fromhttpwwwncbinlmnihgovpubmed19858394
63 Morabito F Gentile M Mazzone C et al Safety and efficacy ofbortezomib-melphalan-prednisone-thalidomide followed by bortezomib-thalidomide maintenance (VMPT-VT) versus bortezomib-melphalan-prednisone (VMP) in untreated multiple myeloma patients with renal im-pairment Blood [Internet] 2011 [cited 2017 Dec 9] 118 5759ndash5766Available from httpwwwncbinlmnihgovpubmed21951682
64 Moreau P Masszi T Grzasko N et al Oral ixazomib lenalidomide anddexamethasone for multiple myeloma N Engl J Med 2016 [cited 2018 Apr27] 374 1621ndash1634 Available from httpwwwnejmorgdoi101056NEJMoa1516282
65 Nordstrom BL Knopf KB Teltsch DY et al The safety of bendamustine inpatients with chronic lymphocytic leukemia or non-Hodgkin lymphomaand concomitant renal impairment a retrospective electronic medical re-cord database analysis Leuk Lymphoma [Internet] 2014 [cited 2017 Dec13] 55 1266ndash1273 Available from httpwwwncbinlmnihgovpubmed23987821
66 Roussou M Kastritis E Christoulas D et al Reversibility of renal failure innewly diagnosed patients with multiple myeloma and the role of novelagents Leuk Res [Internet] 2010 [cited 2017 Dec 15] 34 1395ndash1397Available from httpwwwncbinlmnihgovpubmed20510452
67 Tosi P Zamagni E Tacchetti P et al Thalidomide-dexamethasone as in-duction therapy before autologous stem cell transplantation in patientswith newly diagnosed multiple myeloma and renal insufficiency BiolBlood Marrow Transplant [Internet] 2010 [cited 2018 Apr 27] 161115ndash1121 Available from httpwwwncbinlmnihgovpubmed20197100
68 Dimopoulos M Alegre A Stadtmauer EA et al The efficacy and safety oflenalidomide plus dexamethasone in relapsed andor refractory multiplemyeloma patients with impaired renal function Cancer [Internet] 2010116 3807 [cited 2017 Dec 15] Available from httpwwwncbinlmnihgovpubmed20564094
69 Siegel DS Weisel KC Dimopoulos MA et al Pomalidomide plus low-dosedexamethasone in patients with relapsedrefractory multiple myeloma andmoderate renal impairment a pooled analysis of three clinical trials LeukLymphoma [Internet] 2016 [cited 2017 Dec 15] 57 2833ndash2838 Availablefrom httpwwwncbinlmnihgovpubmed27267105
70 Dimopoulos MA Goldschmidt H Niesvizky R et al Carfilzomib or borte-zomib in relapsed or refractory multiple myeloma (ENDEAVOR) an in-terim overall survival analysis of an open-label randomised phase 3 trialLancet Oncol [Internet] 2017 [cited 2017 Dec 6] 18 1327ndash1337 Availablefrom httpwwwncbinlmnihgovpubmed28843768
71 Telio D Shepherd J Forrest D et al High-dose melphalan followed byauto-SCT has favorable safety and efficacy in selected patients with lightchain deposition disease and light and heavy chain deposition diseaseBone Marrow Transplant 2012 [cited 2017 Dec 8] 47 453ndash455 Availablefrom httpwwwnaturecomdoifinder101038bmt201187
72 Batalini F Econimo L Quillen K et al High-dose melphalan and stem celltransplantation in patients on dialysis due to immunoglobulin light-chainamyloidosis and monoclonal immunoglobulin deposition disease BiolBlood Marrow Transplant [Internet] 2018 [cited 2017 Dec 25] 24127ndash132 Available from httpwwwncbinlmnihgovpubmed28865972
73 Kourelis TV Nasr SH Dispenzieri A et al Outcomes of patients with renalmonoclonal immunoglobulin deposition disease Am J Hematol 2016[cited 2018 Jul 2] 91 1123ndash1128 Available from httpwwwncbinlmnihgovpubmed27501122
74 Pozzi C DrsquoAmico M Fogazzi GB et al Light chain deposition disease withrenal involvement clinical characteristics and prognostic factors Am JKidney Dis [Internet] 2003 [cited 2018 Jun 23] 42 1154ndash1163 Availablefrom httpwwwncbinlmnihgovpubmed14655186
75 Song M-K Chung J-S Shin H-J et al Cyclophosphamide-containing regi-men (TCD) is superior to melphalan-containing regimen (MPT) in elderlymultiple myeloma patients with renal impairment Ann Hematol
Clinical implication of monoclonal gammopathies 11Downloaded from httpsacademicoupcomndtadvance-article-abstractdoi101093ndtgfy2595086133by gueston 29 August 2018
[Internet] 2012 [cited 2017 Dec 9] 91 889ndash896 Available from httpwwwncbinlmnihgovpubmed22237937
76 Specter R Sanchorawala V Seldin DC et al Kidney dysfunction duringlenalidomide treatment for AL amyloidosis Nephrol Dial Transplant[Internet] 2011 [cited 2018 Jul 7] 26 881ndash886 Available from httpwwwncbinlmnihgovpubmed20693160
77 Li Y Wang X OrsquoMara E et al Population pharmacokinetics of pomalido-mide in patients with relapsed or refractory multiple myeloma with variousdegrees of impaired renal function CPAA 2017 [cited 2018 Feb 4] 9133ndash145 Available from httpwwwncbinlmnihgovpubmed29184451
78 Kastritis E Gavriatopoulou M Roussou M et al Addition of cyclophos-phamide and higher doses of dexamethasone do not improve outcomes ofpatients with AL amyloidosis treated with bortezomib Blood Cancer J2017 [cited 2017 Dec 15] 7 e570 Available from httpwwwncbinlmnihgovpubmed28622303
79 Venner CP Gillmore JD Sachchithanantham S et al A matched compari-son of cyclophosphamide bortezomib and dexamethasone (CVD) versusrisk-adapted cyclophosphamide thalidomide and dexamethasone (CTD)in AL amyloidosis Leukemia [Internet] 2014 [cited 2018 Jul 5] 282304ndash2310 Available from httpwwwncbinlmnihgovpubmed25027514
80 Palladini G Sachchithanantham S Milani P et al A European collabora-tive study of cyclophosphamide bortezomib and dexamethasone inupfront treatment of systemic AL amyloidosis Blood [Internet] 2015[cited 2017 Dec 9] 126 612ndash615 Available from httpwwwncbinlmnihgovpubmed25987656
81 Kopel T Kaufman JS Hamburg N et al Endothelium-dependent and -in-dependent vascular function in advanced chronic kidney disease CJASN2017 [cited 2018 Apr 18] 12 1588ndash1594 Available from httpcjasnasnjournalsorglookupdoi102215CJN12811216
82 Palladini G Milani P Foli A et al A Phase 2 trial of pomalidomide anddexamethasone rescue treatment in patients with AL amyloidosis Blood[Internet] 2017 [cited 2018 Apr 26] 129 2120ndash2123 Available fromhttpwwwncbinlmnihgovpubmed28130212
83 Hegenbart U Bochtler T Benner A et al Lenalidomidemelphalandexa-methasone in newly diagnosed patients with immunoglobulin light chainamyloidosis results of a prospective phase 2 study with long-term followup Haematologica [Internet] 2017 [cited 2017 Dec 26] 102 1424ndash1431Available from httpwwwncbinlmnihgovpubmed28522573
84 Palladini G Milani P Foli A et al Oral melphalan and dexamethasonegrants extended survival with minimal toxicity in AL amyloidosis long-term results of a risk-adapted approach Haematologica [Internet] 2014[cited 2017 Dec 15] 99 743ndash750 Available from httpwwwncbinlmnihgovpubmed24213149
85 Payet J Livartowski J Kavian N et al Type I cryoglobulinemia in multiplemyeloma a rare entity analysis of clinical and biological characteristics ofseven cases and review of the literature Leuk Lymphoma [Internet] 201354 767ndash777 Available from httpwwwtandfonlinecomdoifull103109104281942012671481
86 Terpos E Kleber M Engelhardt M et al European Myeloma Networkguidelines for the management of multiple myeloma-related complica-tions Haematologica [Internet] 2015 [cited 2017 Dec 4] 100 1254ndash1266Available from httpwwwncbinlmnihgovpubmed26432383
87 Chanan-Khan AA Kaufman JL Mehta J et al Activity and safety of borte-zomib in multiple myeloma patients with advanced renal failure a multi-center retrospective study Blood [Internet] 2007 [cited 2018 Jul 2] 1092604ndash2606 Available from httpwwwncbinlmnihgovpubmed17138816
88 Dimopoulos MA Roussou M Gkotzamanidou M et al The role of novelagents on the reversibility of renal impairment in newly diagnosed symp-tomatic patients with multiple myeloma Leukemia 2013 27 423ndash429
89 Kouroukis TC Baldassarre FG Haynes AE et al Bortezomib in multiplemyeloma systematic review and clinical considerations Curr Oncol(Toronto Ont) [Internet] 2014 [cited 2017 Dec 4] 21 e573ndashe603Available from httpwwwncbinlmnihgovpubmed25089109
90 Zhu W Chen W Bortezomib-based treatment for multiple myelomapatients with renal impairment a systematic review and meta-analysis ofobservational studies Medicine [Internet] 2016 95 e5202 Available fromhttpwwwncbinlmnihgovpmcarticlesPMC5120900
91 Dimopoulos MA Terpos E Chanan-Khan A et al Renal impairment inpatients with multiple myeloma a consensus statement on behalf of theInternational Myeloma Working Group JCO 2010 28 4976ndash4984
92 Chauvet S Fremeaux-Bacchi V Petitprez F et al Treatment of B-cell disor-der improves renal outcome of patients with monoclonal gammopathyndashassociated C3 glomerulopathy Blood [Internet] 2017 [cited 2017 Oct 26]129 1437ndash1447 Available from httpwwwncbinlmnihgovpubmed28069603
93 Cohen C Royer B Javaugue V et al Bortezomib produces high hematolog-ical response rates with prolonged renal survival in monoclonal immuno-globulin deposition disease Kidney Int [Internet] 2015 [cited 2017 Dec25] 88 1135ndash1143 Available from httpwwwncbinlmnihgovpubmed26176826
94 Ziogas DC Kastritis E Terpos E et al Hematologic and renal improve-ment of monoclonal immunoglobulin deposition disease after treatmentwith bortezomib-based regimens Leuk Lymphoma [Internet] 2017 [cited2017 Dec 25] 58 1832ndash1839 Available from httpwwwncbinlmnihgovpubmed27967286
95 Milani P Merlini G Palladini G Novel therapies in light chain amyloid-osis Kidney Int Rep [Internet] 2018 [cited 2018 Jul 4] 3 530ndash541 Availablefrom httpwwwncbinlmnihgovpubmed29854961
96 Spizzo G Mitterer M Gunsilius E Bortezomib for the treatment of refrac-tory Type-1 cryoglobulinaemia Br J Haematol [Internet] 2010 [cited 2018Jul 7] 150 235ndash237 Available from httpdoiwileycom101111j1365-2141201008184x
97 Talamo G Claxton D Tricot G et al Response to bortezomib in refractoryType I cryoglobulinemia Am J Hematol 2008 [cited 2018 Jul 7] 83883ndash884 Available from httpwwwncbinlmnihgovpubmed18756542
98 Dimopoulos MA Roussou M Gavriatopoulou M et al Cardiac and renalcomplications of carfilzomib in patients with multiple myeloma BloodAdv 2017 [cited 2017 Dec 6] 1 449ndash454 Available from httpwwwbloodadvancesorglookupdoi101182bloodadvances2016003269
99 Strati P Nasr SH Leung N et al Renal complications in chronic lympho-cytic leukemia and monoclonal B-cell lymphocytosis the Mayo Clinic ex-perience Haematologica [Internet] 2015 [cited 2018 Jul 3] 100 1180ndash1188Available from httpwwwncbinlmnihgovpubmed26088927
100 Salama AD Pusey CD Drug insight rituximab in renal disease and trans-plantation Nat Clin Pract Nephrol [Internet] 2006 [cited 2017 Dec 8] 2221ndash230 Available from httpwwwnaturecomdoifinder101038ncpneph0133
101 Jillella AP Dainer PM Kallab AM et al Treatment of a patient with end-stage renal disease with rituximab pharmacokinetic evaluation suggestsrituximab is not eliminated by hemodialysis Am J Hematol 2002 [cited2018 Jul] 71 219ndash222 Available from httpwwwncbinlmnihgovpubmed12410580
102 Guiard E Karras A Plaisier E et al Patterns of noncryoglobulinemic glo-merulonephritis with monoclonal Ig deposits correlation with IgG sub-class and response to rituximab Clin J Am Soc Nephrol 2011 6 1609ndash1616
103 Ribes D Hachem HEL Oberic L et al Bendamustine plus rituximab forindolent B-cell lymphoma of renal significance Am J Hematol 2018 93356ndash362
104 Darwish M Bond M Hellriegel E et al Pharmacokinetic and pharmacody-namic profile of bendamustine and its metabolites Cancer ChemotherPharmacol 2015 [cited 2017 Dec 15] 75 1143ndash1154 Available from httpwwwncbinlmnihgovpubmed25829094
105 Ponisch W Moll B Bourgeois M et al Bendamustine and prednisone incombination with bortezomib (BPV) in the treatment of patients with re-lapsed or refractory multiple myeloma and light chain-induced renal fail-ure J Cancer Res Clin Oncol [Internet] 2013 [cited 2018 Jul 2] 1391937ndash1946 Available from httpwwwncbinlmnihgovpubmed24046251
106 Mateos M-V Dimopoulos MA Cavo M et al Daratumumab plus bortezo-mib melphalan and prednisone for untreated myeloma N Engl J Med2018 378 518ndash528
107 Rocchi S Tacchetti P Pantani L et al Safety and efficacy of daratumumabin dialysis-dependent renal failure secondary to multiple myelomaHaematologica [Internet] 2018 [cited 2018 Jul 2] 103 e277ndashe278 Availablefrom httpwwwncbinlmnihgovpubmed29622654
12 K Batko et alDownloaded from httpsacademicoupcomndtadvance-article-abstractdoi101093ndtgfy2595086133by gueston 29 August 2018
108 Anand S Miller D Chipman G Morris D Srinivas S Daratumumab forsevere refractory proliferative glomerulonephritis with monoclonal im-mune deposits (PGNMID) ATC Abstr [Internet] 2017 [cited 2018 Jul 3]Available from httpsatcmeetingabstractscomabstractdaratumumab-for-severe-refractory-proliferative-glomerulonephritis-with-monoclonal-immune-deposits-pgnmid
109 Leung N Lager DJ Gertz MA et al Long-term outcome of renal transplan-tation in light-chain deposition disease Am J Kidney Dis [Internet] 2004[cited 2018 Feb 9] 43 147ndash153 Available from httpwwwncbinlmnihgovpubmed14712438
110 Lorenz EC Sethi S Leung N et al Recurrent membranoproliferative glo-merulonephritis after kidney transplantation Kidney Int [Internet] 2010[cited 2018 Feb 9] 77 721ndash728 Available from httpwwwncbinlmnihgovpubmed20130531
111 Leung N Nasr SH A patient with abnormal kidney function and a mono-clonal light chain in the urine Clin J Am Soc Nephrol 2016 11 1073ndash1082
112 Cibeira MT Sanchorawala V Seldin DC et al Outcome of AL amyloidosisafter high-dose melphalan and autologous stem cell transplantation long-term results in a series of 421 patients Blood [Internet] 2011 [cited 2018Feb 3] 118 4346ndash4352 Available from httpwwwncbinlmnihgovpubmed21828140
113 Gertz MA Lacy MQ Dispenzieri A et al Autologous stem cell transplantfor immunoglobulin light chain amyloidosis a status report LeukLymphoma [Internet] 2010 [cited 2018 Feb 3] 51 2181ndash2187 Availablefrom httpwwwncbinlmnihgovpubmed20958232
114 Leung N Kumar SK Glavey SV et al The impact of dialysis on the survivalof patients with immunoglobulin light chain (AL) amyloidosis undergoingautologous stem cell transplantation Nephrol Dial Transplant 2016 [cited2018 Jul 7] 31 1284ndash1289 Available from httpsacademicoupcomndtarticle-lookupdoi101093ndtgfv328
115 Badros A Barlogie B Siegel E et al Results of autologous stem cell trans-plant in multiple myeloma patients with renal failure Br J Haematol 2001[cited 2018 Jul 7] 114 822ndash829 Available from httpwwwncbinlmnihgovpubmed11564069
116 Soltero L Carbajal H Xu J et al Initial survival data of kidney transplantpatients with pre-transplant monoclonal gammopathy Clin Transplant[Internet] 2012 [cited 2018 Feb 3] 26 300ndash304 Available from httpwwwncbinlmnihgovpubmed22044717
117 Jimenez-Zepeda VH Heilman RL Engel RA et al Monoclonal gammopathyof undetermined significance does not affect outcomes in patients undergoingsolid organ transplants Transplantation [Internet] 2011 [cited 2018 Feb 3]92 570ndash574 Available from httpwwwncbinlmnihgovpubmed21712755
118 Naina HVK Harris S Dispenzieri A et al Long-term follow-up of patientswith monoclonal gammopathy of undetermined significance after kidney
transplantation Am J Nephrol 2012 [cited 2018 Feb] 35 365ndash371Available from httpwwwncbinlmnihgovpubmed22473253
119 Bansal T Garg A Snowden JA et al Defining the role of renal transplanta-tion in the modern management of multiple myeloma and other plasmacell dyscrasias Nephron Clin Pract [Internet] 2012 [cited 2018 Feb 3] 120c228 wwwkargercom
120 Hassoun H Flombaum C DrsquoAgati VD et al High-dose melphalan andauto-SCT in patients with monoclonal Ig deposition disease Bone MarrowTransplant 2008 [cited 2018 Feb 3] 42 405ndash412 Available from httpwwwncbinlmnihgovpubmed18574442
121 Herrmann SMS Gertz MA Stegall MD et al Long-term outcomes ofpatients with light chain amyloidosis (AL) after renal transplantation withor without stem cell transplantation Nephrol Dial Transplant [Internet]2011 [cited 2018 Feb 3] 26 2032ndash2036 Available from httpwwwncbinlmnihgovpubmed21543655
122 Lorenz EC Gertz MA Fervenza FC et al Long-term outcome of autolo-gous stem cell transplantation in light chain deposition disease NephrolDial Transplant [Internet] 2008 [cited 2018 Jul 5] 23 2052ndash2057 Availablefrom httpwwwncbinlmnihgovpubmed18178602
123 Merhi B Patel N Bayliss G et al Proliferative glomerulonephritis withmonoclonal IgG deposits in two kidney allografts successfully treated withrituximab Clin Kidney J [Internet] 2017 [cited 2018 Feb 10] 10 405ndash410Available from httpsacademicoupcomckjarticle-lookupdoi101093ckjsfx001
124 Barbour SJ Beaulieu MC Zalunardo NY et al Proliferative glomerulone-phritis with monoclonal IgG deposits secondary to chronic lymphocyticleukemia Report of two cases Nephrol Dial Transplant [Internet] 2011[cited 2018 Feb 10] 26 2712ndash2714 Available from httpsacademicoupcomndtarticle-lookupdoi101093ndtgfr251
125 Zand L Lorenz EC Cosio FG et al Clinical findings pathology and out-comes of C3GN after kidney transplantation J Am Soc Nephrol [Internet]2014 [cited 2018 Jul 5] 25 1110ndash1117 Available from httpwwwncbinlmnihgovpubmed24357668
126 Alfano G Fontana F Colaci E et al Monoclonal gammopathy of undeter-mined significance after kidney transplantation Transplantation [Internet]2017 [cited 2017 Oct 24] 101 e337ndashe342 Available from httpwwwncbinlmnihgovpubmed28731904
127 Bancu I Ca~nas L Juega FJ et al Outcomes of monoclonal gammopathyof undetermined significance in patients who underwent kidneytransplantation Transplant Proc [Internet] 2015 [cited 2018 Feb 10] 472344ndash2345 Available from httpwwwncbinlmnihgovpubmed26518922
Received 2632018 Editorial decision 1472018
Clinical implication of monoclonal gammopathies 13Downloaded from httpsacademicoupcomndtadvance-article-abstractdoi101093ndtgfy2595086133by gueston 29 August 2018

the relative risk and nature of progression varies For IgMMGUS the relative risk for any progression is 108 most oftento Waldenstromrsquos macroglobulinaemia AL amyloidosis andnon-Hodgkinrsquos lymphoma Progression for non-IgM MGUScommonly arising from plasma cells after switch recombina-tion has a reported renal response (RR) of 57 leading to multi-ple myeloma (MM) plasmacytoma and AL amyloidosisrespectively [8] Progression to an MGUS-related disorder notaccounting for death to co-morbidities is estimated to be 10at 10 years and 18 at 20 years [8] MGUS risk can be stratifiedon three factors abnormal serum free light chain (sFLC) ratioM protein 15 gdL and immunoglobulin isotype Dependingon the number of these risk factors (0ndash3) the projected risk ofprogression ranges from 7 to 55 at 20 years [8]
Analysis of the Olmsted County cohort showed a prevalenceof 08 for light chain MGUS with 23 of patients developingrenal disease [9] Steiner et al [10] have shown that monoclonalgammopathy of renal significance (MGRS) patients are at in-creased risk of progression to MM than MGUS patients withmedian time to progression at 188 years Risk stratification isan estimate and these patients require life-long monitoringAmong 2935 MGUS patients MGRS was detected in 15with an estimated 10 risk of progression within 1 year after di-agnosis Due to the rarity and heterogenous presentation reli-able biomarkers are exceptionally difficult to find Perhaps abetter understanding of the disease pathogenesis will allow us todiscriminate high-risk patients Recently a prospective trial of331 asymptomatic monoclonal gammopathy patients(MGUSfrac14 152) analysed with clinical variables and gene ex-pression profiles demonstrated genomic features to predicthigh-risk disease suggesting the value of genomics in furtheringour understanding of myelomagenesis [11] Indeed aside frompredicting progression identifying risk for particular lesionsmay aid in discovering early stages of MGRS It is hypothesizedthat risk alleles for C3 glomerulopathy may require an instigat-ing trigger such as infection or monoclonal immunoglobulin(MIg) to develop the disease [12] Individuals with a high riskcould be screened more frequently and meticulously As of yetidentification of disease-related polymorphisms is largely lim-ited to an experimental setting
MM is defined as an M protein of gt30 gL or 10 clonalplasma cells Patients are screened for clinical manifestations ofMM under the acronym SLiM-CRAB bone marrow plasmacells60 involved to uninvolved sFLC ratio100 with abso-lute light chain100 mgL orgt1 focal lesions on magnetic res-onance imaging (MRI 5 mm) hypercalcaemia renaldysfunction anaemia and bone lesions [13] Approximately14 of individuals with MM have no SLiM-CRAB criteria andare designated smoldering myeloma an entity that is nottreated outside of the context of a clinical trial [14]
M G R S D I A G N O S I S
MGRS was introduced in 2012 Leung et al [2] noted that someindividuals who met the criteria for MGUS may have kidneydamage as a result of MIg production or of a fragment thereofThey termed the resulting pathological entity MGRS whichwas not considered to be a benign plasma cell clonal process
but one that was associated with end-organ damage and re-quired treatment [15] Thus the abridged definition of MGUSis the absence of renal lesions with their development warrant-ing re-definition as MGRS
I S M G U S E Q U I V A L E N T T O M G R S
MGRS encompasses an array of diseases linked to relatively be-nign proliferation of plasmaB cells with subsequent excessproduction of MIg or fragment thereof or paraprotein aggre-gating in renal tissues This may lead to loss of function and ul-timately renal failure It is usually secondary to plasma cellB-cell clonal expansion and may result in indirect complementdysregulation [12] In the absence of treatment the renal dam-age due to deposits in tubules and glomeruli is progressive andresults in irreversible damage where therapy to reverse renaldysfunction will no longer be effective [16] Approximately72 of MGRS patients have progressing renal insufficiency[10] Mortality may relate not only to an elevated risk of devel-oping chronic kidney disease (CKD) but also to malignancyinfection or other organ dysfunction [16 17] In 2005ndash2011 themedian MM survival rates were estimated at 54 monthswhereas when MM was associated with moderate to severe re-nal impairment (RI) they were 44 and 32 months respectively[18]
Kidney biopsy is required for the diagnosis of MGRS to in-clude immunohistochemistry immunofluorescence (IFE) andelectron microscopy (EM) [16 19] Lin et al [20] studiedpatients with monoclonal immunoglobulin deposition disease(MIDD) where 39 presented with MGUS Findings in kidneybiopsy preceded clinical diagnosis of dysproteinaemia in 68 ofall cases and 15 plasma cells was found only in 35 In 28cases of membranoproliferative glomerulonephritis (MPGN)with abnormal electrophoresis 16 patients were classified asMGUS on the basis of bone marrow biopsy and clinical imageRenal biopsy specifically IFE was described by the authors ascritical in initiating the evaluation for a gammopathy [21]Serum electrophoresis may be negative while biopsy indicates asetting of monoclonal gammopathy Depending on the diseaseentity evidence of MGRS may only consistently be foundthrough kidney biopsy In proliferative glomerulonephritis(PGN) with monoclonal IgG deposits (PGNMID) and non-IgGPGN detection of a circulating MIg is reported at best at 32combined with a low overall yield of bone marrow examination(25) [22] It is hypothesized that the small size of clonal popu-lations is beyond the detection limit of current methods andorthey are located in extramedullary lymphoid tissue
Finding nodular mesangial sclerosis in only 23 of MIDDcases highlights the need for methodical IFE analysis [23 24]In light chain deposition disease (LCDD) with minimal to noproteinuria nodular sclerosis was found in only 14 of cases[25] Although not a diagnostic criterion it is a common char-acteristic in light microscopy Furthermore defining the sub-type of MIDD requires IFE while diagnosis is set on IFEEMEM is estimated to be necessary in setting a correct diagnosis inapproximately 11ndash21 of renal lesions while in another 21ndash36 it may confirm or provide additional information [26]There are cases where the pathological protein may be hidden
2 K Batko et alDownloaded from httpsacademicoupcomndtadvance-article-abstractdoi101093ndtgfy2595086133by gueston 29 August 2018
and requires a specific approach In a review of 40 crystallineLCPT cases (21 patients classified to MGRS) paraffin IFE withprotease digestion antigen retrieval technique was required forcorrect diagnosis [27] Furthermore in biopsy findings of C3GN or membranoproliferative GN paraffin immunofixation(IF) with protease digestion may unmask MIg deposits and dis-cover MGRS [28]
Extrarenal lesions in MGRS are not uncommon Amyloiddeposits can be limited to the vasculature marking a differentclinical profile [29] In patients with C3 GN associated withmonoclonal gammopathy C3 deposits may coexist in renal andcutaneous vessels [30] Perhaps better understanding of patho-genesis will allow for targeting the mechanism of tissue injuryIn LCDD extrarenal manifestations may occur in the heart andliver [31 32] Cardiac manifestations are reported in 13 of MMpatients with LCDD and are associated with shorter survivaland worse treatment outcomes It is important to note that 85of those patients had MM while in studies where MM rateswere lower [23 24] the rate of cardiac involvement was only10 In rare cases LCDD patients may present without pro-teinuria with tubulointerstitial lesions where nephrologistsmight not screen for monoclonal gammopathy [25]Nephrologists and pathologists should closely cooperate withatypical and typical manifestations of rare diseases In 13 ofIgAndashPGNMID patients the initial diagnosis was IgA nephropa-thy despite the presence of MIg glomerular deposits resultingin a lack of haematological evaluation which is crucial inMGRS [33] Another difficulty in diagnosis may be related tomembranous nephropathy with singular monoclonal IgGwhich requires staining for phospholipase A2 receptor beforeinvestigating a low-grade malignancy [34]
I N V E S T I G A T I O N I N T O M G R S
Presenting symptoms should be closely evaluated and docu-mented MGUS is more commonly seen in older individuals asare metabolic disorders which can mimic MGRS clinicallyUnexplained RI or abnormalities such as proteinuria requireextensive testing AL amyloidosis is suspected with albuminuria(gt50 in urine electrophoresis) nephrotic syndrome and rela-tively preserved kidney function as opposed to MIDD [35]Cryoglobulinaemia (CG) Type I may present with hyperviscos-ity linked symptoms and Type II with skin lesions and vasculi-tis [36] The latter may be related to hepatitis C virus infectionin which case antiviral therapy should be promptly initiated [2]MIDD commonly causes asymptomatic multi-organ involve-ment [16]
SPEP is the most basic quantitative screening test for mono-clonal proteins owing to its general availability and low costSPEP is positive in 819 of MGUS 659 of AL and 556 ofLCDD [37] To increase sensitivity in MGRS it should alwaysbe combined with IF and respective urine studies UPEP andurine IF [16] IF is purely qualitative but it allows for identifica-tion of the MIg isotype Due to low disease burden of MGRS apossible migration of M proteins to different fractions and ahigh limit of detection in SPEP (500 mgL) compared with IF(150 mgdL) a negative SPEP does not exclude MGRS andshould be used together IF [38] Despite lower overall sensitivity
to SPEP the rationale for including the UPEP can be drawnfrom characteristic patterns which may be indicative of a pri-mary disease such as high urine albumin excretion in MIDD orAL amyloidosis or use in monitoring RI in MM [39 40] Theadditional use of antibodies targeting epitopes of sFLC detectscases missed by urine assay though it is also true for the reverseas such both assays cannot be replaced [37] Urine free lightchain assays should not be utilized as there are no establishednormal ranges [41] The established normal range for thekappalambda ratio is 026ndash165 whereas in patients with renaldysfunction a range of 034ndash31 is considered normal [42] Ithas been suggested that the lower threshold should be raised forproliferative glomerulonephritides with non-organized glomer-ular MIg deposition [22] sFLC should be assessed with theknowledge that kappa monomers are more easily filtered com-pared with lambda dimers Renal dysfunction defined as an ab-normal creatinine clearance (CrCl) results in elevated sFLCthough usually but not always with a maintained kappalambdaratio (21) [43] Thus all instances of a abnormal sFLC valuesshould not be immediately attributed to a monoclonal gamm-opathy [44] In a retrospective data review of 76 MGUS (295observations) patients sFLCs were observed with agt55 false-negative ratio compared with electrophoretic studies [45]Conversly Fulton et al [46] analysed 219 cases with all urineand serum studies to a conclusion of sFLC and SPEP detecting6 more cases than SPEPIF and UPEPIF Several authorshave indicated that studies criticizing IFE may use incorrectmethodology while urine studies are of equal sensitivity andmay be more useful in low burden light chain clones especiallylambda dominant [47 48] Katzmann et al [37] observed thatSPEP and sFLC is the most effective basic screening panel inidentifying several MGRS conditions In LCDD 42 of patientspresented with no abnormalities in SPEPIFE but FLCs wasraised in all and matched the isotype in biopsy [25] FLCs arenot universally accepted and must be performed in combina-tion with urine and serum studies A cut-off value of kappalambda ratio gt289 of 92 sensitivity and 97 specificity areestablished for plasma cell malignancy at an estimated glomeru-lar filtration rate (eGFR) lt60 mLmin173 m2 howeverMGRS specific light chain values require further study [49] In17 MGRS patients with nephritic range proteinuria serum andurine IF with sFLC was 100 sensitive Although three patientswith chronic glomerulonephritides were identified by sFLC andserum IF the results do not reliably reflect the spectrum ofMGRS In PGNMIDnon-IgG GN the detection rate is esti-mated at 32 for serum IF and sFLC [22 50] Another study on19 PGNMID patients reported an overall paraprotein andclonal detection rate of 37 and 32 respectively [51] In thethese conditions if testing for either serum IFE or sFLC is posi-tive bone marrow investigation with flow cytometry and im-munohistochemical study may uncover a pathological cloneDetermination of the best diagnostic algorithm is difficult and ifthere is a strong suspicion of MGRS all five tests should be or-dered At present there is no standard testing for the heteroge-nous presentation(s) of MGRS due to different diseasesubtypes
Clinical implication of monoclonal gammopathies 3Downloaded from httpsacademicoupcomndtadvance-article-abstractdoi101093ndtgfy2595086133by gueston 29 August 2018
Without chemotherapy there is a high recurrence rate ofMGRS conditions post-renal transplant and prioritizing func-tional improvement requires early diagnosis as opposed to thepassive monitoring in MGUS [2] (Table 3) Recent advancespoint to time of flight mass spectrometry (MS) without theneed for expensive proteomic analysis though the ability to dis-criminate and identify the pathological protein has to be dem-onstrated [52] Laser microdissection and MS proteomics arerecommended to confirm AL amyloidosis cases of abnormalMIDD with truncated MIg or instances where the specific MIgregion is of interest [19 42] Urinary exosomes which have dif-ferent characteristics in AL amyloidosis and MGUS combinedwith MS may become the diagnostic and monitoring tools aftermore evidence is available [53] In daily practice parameters ofkidney function creatinine and proteinuria can be comparedwith assessment of the course of progression and response totreatment [54] However first-line monitoring should includeparaprotein levels and indirect disease activity markers whichtrack evolution of the primary disease
Non-invasive screening tools for on-going diagnosis of plasmacell dyscrasia particularly in difficult to identify MGRS condi-tions are of interest Vij et al [55] reported on deep sequencingof peripheral blood demonstrating clonal plasma cells in 96 ofMM patients In the case of IgM MGRS which suggests the pres-ence of B-celllymphoplasmacytic clone it is necessary to attemptto specify the clonal population through bone marrow andorlymph node biopsy and radiographic imaging [2 16] F18 posi-tron emission computed tomography can identify potential ab-normal lymph nodes for biopsy in conjunction with peripheralblood flow cytometry [54] MRI to exclude marrow involvementmay also be considered With the heterogeneity of MGRS asidefrom determining the conclusive histopathology character exclu-sion of plasma cell malignancy is necessary
T R E A T M E N T F O R M G R S mdash A N O V E R V I E W
A multi-disciplinary collaboration between nephrologist pa-thologist and haematologist is a priority in the diagnosis andtreatment of these individuals Therapy should incorporate bi-opsy-driven diagnosis with particular clinical features and dis-ease course prediction Identification of the clone responsiblefor MGRS and appropriate haematological treatment shouldtranslate into better RR and prevention of progression MGRSpatients with doubled serum creatinine or reduced renal func-tion may be at higher risk of haematological progression (oddsratio 26 CI 03ndash24) [10] In MM the reversal of RI has beenshown to improve outcome [56] Treatment of CD20thorn clonesshould utilize rituximab (RTX) while MGRS conditions par-ticularly non-IgM MGRS should consider MM regimens asprovided below and summarized in Table 1 With the rarityand wide array of MGRS conditions establishing strong evi-dence for treatment is difficult and evidence is limited to anec-dotal cases or small patient series
C Y T O T O X I C D R U G S
Historically melphalan-prednisone (MP) was used for thetreatment of plasma cell dyscrasias but due to the low response T
able
1T
hera
peut
icre
gim
ens
for
prim
ary
MG
RS
con
diti
ons
Dru
gC
hara
cter
Dis
ease
char
acte
rSe
veri
tyof
kidn
eyin
suff
icie
ncy
Ref
eren
ce
Lena
lidom
ide
LoD
exM
PT
Clin
ical
tria
lM
Mw
ith
RI
149
pati
ents
CrC
llt30
mL
min
372
pts
CrC
l30
lt50
Dim
opou
los
etal
[57
]B
enda
mus
tine
PV
Ret
rosp
ecti
veM
Mw
ith
RI
18eG
FRlt
35m
Lm
in(1
1pt
seG
FR15
mL
min
)P
onis
chet
al[
58]
RT
XC
YC
Dex
Ret
rosp
ecti
veIn
dole
ntN
HL
Glo
mer
ulon
ephr
itis
rela
ted
toM
Ig14
pts
(71
5w
ith
eGFR
lt60
mL
min
)P
erry
etal
[59
]
PO
ML
oDex
Clin
ical
tria
lR
elap
sed
refr
acto
ryM
Mw
ith
RI
Thr
eeco
hort
smdash33
eGFR
30ndash4
5m
Lm
inpt
s34lt
30m
Lm
ineG
FRpt
s14
HD
pts
Dim
opou
los
etal
[60
]
RT
XC
linic
altr
ial
Mem
bran
ous
neph
ropa
thy
eGFR
40P
rote
inur
ia
5g
24h
Ferv
enza
etal
[61
]V
MP
vers
usM
PC
linic
altr
ial
MM
wit
hR
I34
ptslt
30m
Lm
inG
FR1
93pt
sG
FR31
ndash50
mL
min
Dim
opou
los
etal
[62
]V
MP
TndashV
Tve
rsus
VM
PC
linic
altr
ial
MM
wit
hR
I33
ptslt
30m
Lm
ineG
FR1
16pt
seG
FR31
ndash50
mL
min
Mor
abit
oet
al[
63]
Ixaz
omib
Lena
lidom
idendash
Dex
Clin
ical
tria
lR
efra
ctor
yre
laps
edM
M10
pts
CrC
llt30
mL
min
169
pts
CrC
l30ndash
60m
Lm
inM
orea
uet
al[
64]
Ben
tam
usti
nem
onot
hera
py
wit
hR
TX
Ret
rosp
ecti
veC
LLN
HL
104
pts
CrC
llt40
mL
min
Nor
dstr
omet
al[
65]
Vve
rsus
IMiD
vers
usC
CC
linic
altr
ial
MM
wit
hR
I55
pts
CrC
llt30
mL
min
(9di
alys
is)
41pt
sC
rCl
30lt
50m
Lm
inR
ouss
ouet
al[
66]
T-D
exC
linic
altr
iald
ata
MM
wit
hR
Ipr
ior
toA
SCT
(ind
ucti
onth
erap
y)16
pts
CrC
llt30
mL
min
15
pts
CrC
l30ndash
50m
Lm
in(t
otal
7on
HD
)T
osie
tal
[67]
L-D
exT
wo
clin
ical
tria
lsM
MR
Ive
rsus
non-
RI
16pt
sC
rCllt
30m
Lm
inC
rCl
30lt
60in
82pt
sD
imop
oulo
uset
al[
68]
PO
Mndashl
owD
exT
hree
clin
ical
tria
lsM
Mw
ith
RI
355
pts
wit
hC
rCl
30an
dlt
60m
Lm
in(1
66pt
sC
rCl
30lt
45)
Sieg
elet
al[
69]
Car
filzo
mib
Dex
vers
usB
orte
zom
ibD
exC
linic
altr
ial
Rel
apse
dre
frac
tory
MM
56pt
sC
rCllt
30m
Lm
in1
28pt
sw
ith
CrC
l30ndash
50m
Lm
inD
imop
oulo
set
al[
70]
Vb
orte
zom
ibM
mel
phal
anL
len
alid
omid
eT
tha
lidom
ide-
dexa
met
haso
ne
Vb
orte
zom
ibC
Cc
onve
ntio
nalc
hem
othe
rapy
CLL
chr
onic
lym
phoc
ytic
leuk
aem
iaN
HL
non-
Hod
gkin
lym
phom
apt
spa
tien
ts
4 K Batko et alDownloaded from httpsacademicoupcomndtadvance-article-abstractdoi101093ndtgfy2595086133by gueston 29 August 2018
rates has been replaced by more potent regimens In LCDDwith MGUS MP and plasmapheresis prolonged survival how-ever kidney function deteriorated which marks the inefficiencyof the old regimes
To achieve a higher and more durable haematological re-sponse (HR) and potentially to qualify for kidney transplant(Ktx) high-dose melphalan supported with autologous stemcell transplantation (ASCT) is considered highly efficacious inMM and AL SCT has been shown to improve survival in ALamyloidosis and MIDD [71 72] Achieving a very good partialresponse (VGPR)complete response (CR) is associated with abetter RR rate than a HR lt VGPR [31 32 73] Importantly anadvanced impairment of renal function may impact responseindependently of achieving HR [32 74] Preventing renal dam-age will likely only be achieved by earlier diagnosis
I M M U N O M O D U L A T O R Y A G E N T S
Thalidomide the first immunomodulatory drug (IMiD) agentapproved for the treatment of myeloma can be safely adminis-tered regardless of renal function Outside the USA thalido-mide remains a viable choice in CrCl lt50 mLmin1 73 m2since it is not renally cleared [67] Song et al [75] report that inpatients with a low glomerular filtration rate (GFR) defined aslt40 mLmin173 m2 cyclophosphamide (CYC) was betterthan MP when combined with thalidomide with regard to re-nal functional improvement adverse events overall survival(OS) and mortality due to infection (P lt 0001) Lenalidomideis renally cleared and doses need to be adjusted for renal insuffi-ciency (CrCl lt60 mLmin) Complete blood counts should beperformed on a regular basis in the setting of moderate to severerenal insufficiency so that the lenalidomide dose may be modi-fied in the setting of unacceptable cytopenias [68] In a study of41 AL amyloidosis patients treated with lenalidomide 66were observed with kidney dysfunction and 10 required dialy-sis [76] However for approximately 25 of patients the initialdoses were too high and for half dosage was not appropriatelyadjusted Another aspect was older age and worse renal statusin those who experienced more severe impairment Recently alarge MM trial reported that renal function-adapted lenalido-mide dose resulted in similar safety across all levels of RI(Table 1) [57]
Pomalidomide (POM) is effective in lenalidomide-refractorycases and suitable for any CrCl (Table 1) However the recom-mendation for patients on dialysis is 3 mg rather than the stan-dard 4 mg dose and should be administered following dialysis[77] The latest results of POM and low-dose dexamethasone(LoDex) showed acceptable safety of 4 mgday in patients witheGFRlt30 mLmin173 m2 and on dialysis though CR wasonly achieved in eGFR 30ndash45 mLmin173 m2 [60] IMiDshave been used with effectiveness in MM AL amyloidosisMIDD CG Type 1 and LCPT (Tables 1 and 2) [27 31 85]
P R O T E A S O M E I N H I B I T O R S mdash N O V E L D R U G S
In 2015 bortezomib a first-generation proteasome inhibitorwas established as a class 1 A treatment (BDex) standard by theEuropean Myeloma Network for MM with RI [86] Bortezomib
showed a favourable profile with metabolism independent ofkidney function and demonstrated to be beneficial in advancedrenal failure and dialysis [87 88] A systematic review in 2014concluded that bortezomib was preferable to other agents inMM with RI [89] The most prominent adverse event is periph-eral neuropathy which may be a troublesome side effect in of-ten mildly symptomatic MGRS conditions Bortezomibpromotes a high rate of haematological CR as well as RR inMM with RI [90] High-dose Dex is linked to a faster RR how-ever mildly symptomatic MGRS patients may not be willing tocomply with the side effects whereas treatment-wise achievinga faster RR may improve the disease course [88] Bortezomibhigh-dose Dex is recommended by the IMWG for patients withMM-related RI whereas a three-drug scheme is deemed to im-prove RR [91]
In 50 patients with C3 glomerulopathy associated withmonoclonal gammopathy chemotherapy effectively achievedHR the only predictor of RR in multivariate analysis into sig-nificantly higher RR and renal survival rates compared withstandard immunosuppression [92] Bortezomib-based regimesmade up 76 of the chemotherapy group also being signifi-cantly associated with RR in univariate analysis Bortezomib-based treatment in 49 patients with MIDD reported at least aVGPR in 704 with HR not significantly different fromHDMSCT [93] Maintained haematological remission was as-sociated with survival in all patients at 85 months follow-up incomparison with 52 at 48 months in a series published in2003 [74] Ziogas et al [94] reported on 18 MIDD patientstreated exclusively with bortezomib regimes with gt VGPR in333 and an equal number progressing to end-stage renal dis-ease (ESRD) In the 2003 study by Pozzi et al progression wassimilar at 368 suggesting that even late induction of noveltherapy will not overcome poor prognosis associated with ad-vanced renal insufficiency The higher efficacy reported byCohen et al may be explained by overall less advanced kidneyfailure and proteinuria Together the studies demonstrate thatprevention of poor kidney function is necessary to treat effec-tively regardless of treatment regime
Recently the spectrum of MGRS has been reviewed in thecontext of monoclonal IgA deposits RTX did not elicit a RRwhile bortezomib-based treatment was suggested as first-linestrategy [33] Of 22 LCPT patients six MGRS patients weretreated with bortezomib-based regimes with 333 reaching atleast VGPR while the remainder had stable disease [27]Untreated patients progressed to ESRD while multivariateanalysis showed initial eGFR to be the only predictor of renalfunction This brings further support to prioritizing early detec-tion and subsequent chemotherapy to prevent deterioration ofkidney function In AL amyloidosis CyBorDBDex is stem cellspairing and therefore can be used in patients who may yetqualify for SCT as well as renal failure [95] In 53 patients withLCDD of which 57 were in Stage 45 CKD achieving at leasta VGPR improved renal outcome with bortezomib-based regi-mens achieving CR in eight out of nine cases [31] MIDD haspreviously been reported with poor outcomes and progressionto ESRD [24] Kourelis et al [73] studied 88 patients withMIDD (42 MGRS) of which 69 presented with eGFR
Clinical implication of monoclonal gammopathies 5Downloaded from httpsacademicoupcomndtadvance-article-abstractdoi101093ndtgfy2595086133by gueston 29 August 2018
lt30 mLmin1732 reporting proteasome inhibitorSCT as themost feasible therapeutic choice Achievement of completevery good partial HR was necessary for a RR while RR was anindependent predictor of progression again highlighting theprinciples of MGRS treatment In patients with PGNMID whodo not respond to initial treatment with RTXCYC and ste-roids bortezomib-based treatment may elicit a response [51]Bortezomib-based therapy was effective even in refractory casesof CG Type 1 related to MM [85 96 97]
Carfilzomib is a second-generation proteasome inhibitorDimopoulos et al [98] reported that carfilzomib-based therapyimproved renal outcome in 55 of patients with eGFRlt60 mLmin173 m2 Renal function may initially temporarilydecrease though therapy improves renal function A cardiacrisk profile should be treated with exceptional care Patient pro-file assessment and further studies will determine the use inMGRS
M O N O C L O N A L A N T I B O D I E S
Patients with MGUS treated with RTX and prednisone had im-proved kidney function and decreased proteinuria In patientswith MPGN secondary to indolent clones RTX CYC andprednisone were more effective then RTX with steroidsmono-therapy [99] Therapeutic doses of monoclonal antibodies maybe administered even in renal failure and post-renal allograftsettings [100 101] In seven patients with glomerulonephritiswith monoclonal IgG deposits RTX has been observed withpromising results [five achieved CR two partial response (PR)][102] The added benefit of RTX over classic chemotherapyrelates to a more tolerable profile Treatment of 14 PGNMIDpatients in approaches of clone-directed and empirical therapywithout identifiable discrasia was effective with patients withno detectable clone responding with complete and PSs in allbut two cases Bortezomib-based therapy may be effective innon-responders While empirical treatment is not easily under-taken with clonal detection at 25ndash32 it seems justified con-sidering the rate of response [22 51] However the studypopulation is not robust and the benefitsafety of such an ap-proach is in need of confirmation by larger studiesInterestingly patients with eGFR 20 had similar rates of CRPR to eGFR45 and all patients were free of ESRD in follow-up underscoring the value of a haematological treatment ap-proach in MGRS [51] RTXndashCYCndashDex use in 14 patients withMIg-associated glomerulopathy secondary to indolent non-Hodgkin lymphomas was reported on with 64 achieving CR(Table 1) The antiproteinuric effect of RTX is another benefi-cial aspect A steroid-free regimen of bendamustine and RTXprospectively assessed in indolent B-cell lymphoma of renalsignificance resulted in 85 achieving a haematological CRand 75 a complete RR [103] Patients without RR did notachieve HR Bendamustine is primarily cleared by hydrolysiswith minimal kidney involvement and recently there is sub-stantial evidence suggesting its safety in advanced renal failurethough complete blood counts should be monitored for haema-tological abnormality [104 105] (Table 1) RTX should be con-sidered in patients with IgM-associated MGRS especially when
Tab
le2
AL
base
dre
gim
ens
for
trea
tmen
tof
MG
RS
Dru
gP
atie
nts
and
met
hods
Out
com
esC
oncl
usio
nsR
efer
ence
VC
Dve
rsus
VD
101
pts
AL
amyl
oido
sis
(11
rena
lSta
ge3)
Sim
ilar
HR
(Pfrac14
026
)R
R43
fo
rV
Dve
rsus
41
for
VC
D(Pgt
005
)si
mila
rsu
rviv
al(Pfrac14
045
)H
ighe
rdo
sing
ofD
exan
dC
YC
addi
tion
does
noti
m-
pact
ther
apy
outc
omes
sign
ifica
ntly
Kas
trit
iset
al[
78]
CV
Dve
rsus
CT
D13
9pt
sw
ith
AL
amyl
oido
sis
Hig
her
CR
inC
VD
(40
6ve
rsus
246
)
med
ian
PFS
280
vers
us14
0m
onth
sre
spec
tive
lyFa
stcl
onal
cont
rold
idno
tred
uce
earl
ym
orta
lity
Ven
ner
etal
[79
]
CyB
orD
230
pts
wit
h63
w
ith
rena
linv
olve
men
t60
H
R4
3V
GP
R2
5R
RE
ffica
ciou
sin
pati
ents
wit
hout
card
iac
invo
lvem
ent
sur-
viva
lis
depe
nden
ton
deep
resp
onse
Pal
ladi
niet
al[
80]
DA
RA
Ret
rosp
ecti
vere
view
of25
cons
ecut
ive
AL
pts
HR
in76
C
Rin
36
VG
PR
24
wel
ltol
erat
edev
enin
card
iac
pts
Effi
caci
ous
inhe
avily
pre-
trea
ted
Kau
fman
etal
[81
]
Pom
alid
omid
endashD
ex28
pts
wit
hA
Lam
yloi
dosi
s68
H
Rgt
VG
PR
in29
5
3w
ith
resp
onse
afte
r1
cycl
eA
noth
erch
oice
inre
frac
tory
AL
impr
oves
surv
ival
hae
-m
atol
ogic
alpr
ogre
ssio
npr
edic
tssu
rviv
alP
alla
dini
etal
[82
]
LMD
50A
Lam
yloi
dosi
spt
s62
w
ith
rena
lloa
d(4
inre
nalS
tage
III)
CR
18
VG
PR
32
OR
in48
h
aem
atol
ogic
and
card
iac
toxi
city
4
mor
talit
y1
case
ofac
ute
kidn
eyin
jury
len
alid
omid
edo
seha
sto
bem
onit
ored
and
adju
sted
oth
erw
ise
tole
rabl
ean
def
ficac
ious
Heg
enba
rtet
al[
83]
M-D
ex25
9A
Lam
yloi
dosi
spt
sH
R76
C
R31
in
high
dose
ver
sus
51an
d12
in
atte
nuat
edO
Ron
lyin
pati
ents
wit
hH
R(h
ighe
rin
CR
vers
usV
GP
R)
Pal
ladi
niet
al[
84]
VG
PH
Rv
ery
good
part
ialh
aem
atol
ogic
alre
spon
seE
GC
Ge
piga
lloca
tech
inga
llate
LM
Dl
enal
idom
ide
mel
phal
ande
xam
etha
sone
VC
Db
orte
zom
ibcy
clop
hosp
ham
ide
dexa
met
haso
neM
-Dex
mel
phal
ande
xam
etha
sone
6 K Batko et alDownloaded from httpsacademicoupcomndtadvance-article-abstractdoi101093ndtgfy2595086133by gueston 29 August 2018
Tab
le3
Mon
oclo
nal
gam
mop
athy
inth
ese
ttin
gof
kidn
eytr
ansp
lan
tati
on
Pat
ient
san
dm
etho
dsO
utco
mes
Con
clus
ions
Ref
eren
ce
27LC
PT
pati
ents
trea
ted
wit
hch
emo-
ther
apy
(11
SCT
)9
wit
hno
trea
tmen
tLo
wes
tm
orta
lity
best
HR
sin
SCT
tho
ugh
pati
ents
wer
eyo
unge
ran
dha
dbe
stin
itia
land
final
rena
lfu
ncti
on
Bes
tren
alou
tcom
eco
mpa
red
wit
hch
emot
hera
pyor
notr
eatm
ent
SCT
stab
ilize
dor
impr
oved
rena
lfun
ctio
nSt
okes
etal
[27
]
64M
IDD
pati
ents
16
pts
trea
ted
wit
hSC
T4
Ktx
3re
curr
ence
sin
4K
txpa
tien
tsr
ange
of7ndash
43m
onth
s38
pr
ogre
ssio
nto
ESR
Din
SCT
Hig
hcr
eati
nine
atbi
opsy
isas
soci
ated
wit
hpo
orou
t-co
me
chem
othe
rapy
afte
rre
curr
ence
isin
effic
ient
Nas
ret
al[
24]
49M
IDD
pati
ents
3K
txw
ith
1V
GP
Ran
d2
CR
18
SCT
No
recu
rren
ces
in3
Ktx
pati
ents
allo
graf
trej
ecti
onin
1pa
tien
taft
er3
year
sSC
Tw
assa
fean
dto
lera
ted
but
pati
ents
wer
eyo
unge
rbo
rtez
omib
-bas
edtr
eatm
enth
adsi
mila
rR
Rra
tes
Sust
aine
d
VG
PR
nece
ssar
yfo
rK
txS
CT
ispr
efer
red
CK
Dst
ages
Coh
enet
al[
93]
29M
PG
NK
txpa
tien
ts6
wit
hm
onoc
lona
lpro
tein
(4M
GU
S1
CLL
)23
of
MP
GN
pati
ents
have
mon
oclo
nalp
rote
ins
may
incr
ease
risk
ofre
curr
ence
SC
Tre
solv
edre
curr
ence
pl
asm
aphe
res
aspa
ssiv
em
aint
enan
ce
MP
GN
pati
ents
shou
ldbe
scre
ened
for
mon
oclo
nal
prot
eins
Lore
nzet
al[
110]
6LC
DD
wit
hSC
T1
pati
entd
idno
tsur
vive
SCT
all
othe
rsac
hiev
edH
R
2re
laps
esw
ith
1im
prov
edby
subs
eque
ntch
emot
hera
py
Insu
ffici
ent
resp
onse
toSC
Tm
aybe
anin
dica
tion
for
Ktx
inse
lect
pati
ents
afte
rac
hiev
ing
HR
Lore
nzet
al[
122]
7LC
DD
Ktx
pati
ents
Med
ian
recu
rren
ce2ndash
45m
onth
sfo
r5
pati
ents
sub
se-
quen
t4de
aths
onl
y1
pati
entf
ree
ofre
new
alA
HR
mus
tbe
achi
eved
befo
reat
tem
ptin
gK
txLe
ung
etal
[10
9]
2P
GN
MID
Ktx
pati
ents
(1de
novo
1re
curr
ent)
Impr
ovem
ent
ingr
aftf
unct
ion
and
seru
mcr
eati
nine
in2
year
follo
w-u
pR
TX
can
beef
fect
ive
inbo
thre
curr
enta
ndde
novo
PG
NM
IDpt
sM
erhi
etal
[12
3]
3P
GN
MID
(2C
LL)
Des
pite
RT
Xtr
eatm
entt
here
was
1pr
ogre
ssio
nto
ESR
Dan
don
em
alig
nanc
ypr
ogre
ssio
nR
TX
ther
apy
may
impr
ove
rena
lout
com
esin
shor
tter
mB
arbo
uret
al[
124]
53LC
DD
7K
tx1
6SC
T2
recu
rren
ces
inpa
tien
tsw
itho
utpr
ior
chem
othe
rapy
1
reje
ctio
nof
Ktx
3pa
tien
tsin
CR
ingt
68
year
follo
w-
up1
SCT
-rel
ated
deat
h13
15
achi
eved
CR
SCT
can
besu
cces
sful
even
inC
KD
Stag
e4
how
ever
re
nals
urvi
vali
sst
illw
orse
SC
Tap
pear
sm
ore
safe
than
inA
Lam
yloi
dosi
s
Saye
det
al[
31]
21K
txw
itC
3GN
667
re
curr
ence
ofw
hich
21
asso
ciat
edw
ith
mon
o-cl
onal
gam
mop
athy
rec
urre
nce
earl
ier
(36
mon
thm
e-di
anve
rsus
433
mon
th)
mor
epr
ogre
ssiv
eco
urse
(Pfrac14
NS)
SC
Tim
prov
edki
dney
func
tion
inon
epa
tien
tst
a-bl
egr
aft
in10
-yea
rfo
llow
-up
Mon
oclo
nalg
amm
opat
hypa
tien
tsar
eat
risk
ofan
ear-
lier
and
mor
eag
gres
sive
dise
ase
Zan
det
al[
125]
548
Ktx
pati
ents
Pre
vale
nce
81
52
year
med
ian
toM
GU
Sdi
scov
ery
high
erra
teof
MB
Lhi
stor
yof
infla
mm
ator
yki
dney
dis-
ease
aspr
edic
tive
fact
orn
oas
soci
atio
nw
ith
age
and
gend
ern
oim
pact
ongr
afts
urvi
val
over
alls
urvi
val
in-
cide
nce
ofm
alig
nanc
y
MG
US
pre-
and
post
-tra
nspl
antm
aybe
diff
eren
tcon
di-
tion
sin
term
sof
man
agem
ent
how
ever
str
ict
follo
w-u
pis
need
ede
spec
ially
inM
BL
pati
ents
Alfa
noet
al[
126]
159
3K
txre
cipi
ents
3pr
e-tr
ansp
lant
MG
(nfrac14
34)
No
case
sof
prog
ress
ion
noas
soci
atio
nw
ith
mal
igna
ncy
inci
denc
eor
mor
talit
yJi
men
ezZ
eped
aet
al[
117]
587
Ktx
reci
pien
ts2
9in
cide
nce
(9pt
spr
e-tr
ansp
lant
8po
st)
No
prog
ress
ion
duri
ng6-
year
follo
w-u
pM
GU
Sno
taco
ntra
indi
cati
onto
Ktx
Ban
cuet
al[
127]
351
8K
txre
cipi
ents
42pa
tien
ts(2
3pr
e-tr
ansp
lant
19
post
)m
edia
nsu
rviv
al26
1ve
rsus
280
year
sre
spec
tive
ly4
haem
atol
ogic
alm
a-lig
nanc
ies
deve
lope
din
pre
2P
TLD
gt15
year
spo
st-
tran
spla
nt
Dia
gnos
isof
PT
LDw
assy
mpt
om-b
ased
tru
ein
cide
nce
may
behi
gher
exc
lusi
onof
asso
ciat
edki
dney
dise
ase
and
mal
igna
ncy
isne
cess
ary
befo
reK
tx
Nai
naet
al[
118]
MB
Lm
onoc
lona
lB-c
elll
ymph
ocyt
osis
Clinical implication of monoclonal gammopathies 7Downloaded from httpsacademicoupcomndtadvance-article-abstractdoi101093ndtgfy2595086133by gueston 29 August 2018
CD20thorn cells can be identified while non-IgM-associated dis-eases more often require MM-like treatment
Recently an anti CD38 monoclonal antibody daratumumab(DARA) has been approved for the treatment of newly diag-nosed and relapsed MM patients [106] Like many Phase 3 reg-istration trials the study excluded patients with CrCl 20 mLmin Anecdotal evidence of safety and reduction of dialysis fre-quency in a patient with DARA monotherapy has recently beenreported [107] A case of PGNMID refractory to RTX and
bortezomib was successfully treated with DARA [108] Due toindependence of kidney clearance and positive results in RI itmay prove beneficial in MGRS There is an on-going Phase 2study of DARA in MGRS [NCT03095118]
M G R S T R A N S P L A N T A N D E S R D
Renal transplant in MGRS is controversial as frequent recur-rences are observed when the abnormal clone is not adequately
FIGURE 1 Diagnostic and therapeutic algorithm of monoclonal gammopathy of renal significance
8 K Batko et alDownloaded from httpsacademicoupcomndtadvance-article-abstractdoi101093ndtgfy2595086133by gueston 29 August 2018
suppressed [24 109 110] The current treatment paradigm inMGRS is to achieve a complete HR as a means of improvingpost-transplant outcome and preventing recurrence [71 72111] Cibeira et al [112] report that in 340 AL amyloidosispatients subject to SCT 43 attained CR improving long-termOS and organ response (OR) In recent years the treatment-re-lated mortality (TRM) has decreased from 138 between 1994and 2003 to 56 between 2004 and 2008 In part this probablyreflects the experience of established centres however with ac-cess to novel agents there are other options for treatmentCardiac involvement should be screened for in LCDD due to ahigh TRM (23) with SCT as opposed to non-cardiac patients[32] PS does not indicate treatment failure and significantlyincreases survival compared with patients lacking response[113]
A study in AL amyloidosis patients associated the need fordialysis within 30 days of SCT with highest early death risk andTRM Patients with both eGFRlt40 mLmin173 m2 and se-rum albumin lt25 mgdL had a 438 and 281 risk of requir-ing dialysis and chance of TRM respectively Identifying andscreening for such risk factors should improve the feasibility ofSCT in MGRS conditions [114] In a study of 36 patients withAL amyloidosisMIDD who were dialysis dependent for ESRDCR was reached in 53 at 1 year post SCT with an 8 TRM[72] Achievement of dialysis independence was possible inpatients receiving a Ktx after successful SCT Similarly a studyin MM with RI found no impact on survival for patients whowere dialysis dependent [115] Further research is required toevaluate risk factors and establish whether select ESRD patientsmay benefit from SCT
Literature reports are conflicting on the approach to Ktx inMGUS [116ndash118] Bansal et al [119] reflect that a select groupof plasma dyscrasia patients should be considered for Ktx espe-cially those subject to dialysis-associated complications In ALand MIDD patients achieving haematological CR have beenreported with successful Ktx [120 121] Monoclonal gammop-athy in the setting of Ktxs is presented in Table 3 In summaryprimary disease activity organ function and patient perfor-mance should dictate selection for Ktx We propose an algo-rithm for diagnostic and therapeutic treatment of MGRS(Figure 1)
C O N C L U S I O N
With under-recognition of the wide spectrum of MGRS accu-rate classification evidence-based therapy and expert estab-lished management is required Renal involvement in MGRSresults from the direct deposition of monoclonal protein and itslight- or heavy-chain fragments in the kidney IFE microscopyis essential to identify the offending monoclonal protein and itsrenal tissue distribution In selected cases MS is of valueMGRS therapy is directed to eliminate the clonal plasma cell orB-cell population Adverse events particular to the chosen drugshould complement the patient profile Early detection diagno-sis and chemotherapy may improve kidney function It shouldbe stressed that both the renal pathology and the underlyinghaematological disorders influence the management and
prognosis of MGRS Upon achieving HR ASCT and Ktx shouldbe considered as therapy endpoints in MGRS
C O N F L I C T O F I N T E R E S T S T A T E M E N T
None declared
R E F E R E N C E S
1 Kyle RA Monoclonal gammopathy of undetermined significance NaturalHistory in 241 Cases Am J Med [Internet] 1978 [cited 2017 Oct 24] 64814ndash826 Available from httpwwwncbinlmnihgovpubmed645746
2 Leung N Bridoux F Hutchison CA et al Monoclonal gammopathy of re-nal significance when MGUS is no longer undetermined or insignificantBlood [Internet] 2012 [cited 2017 Oct 24] 120 4292ndash4295 Available fromhttpwwwncbinlmnihgovpubmed23047823
3 Kyle RA Therneau TM Rajkumar SV et al Prevalence of monoclonalgammopathy of undetermined significance N Engl J Med [Internet] 2006[cited 2017 Oct 24] 354 1362ndash1369 Available from httpwwwncbinlmnihgovpubmed16571879
4 Landgren O Graubard BI Kumar S et al Prevalence of myeloma precur-sor state monoclonal gammopathy of undetermined significance in 12372individuals 10ndash49 years old a population-based study from the NationalHealth and Nutrition Examination Survey Blood Cancer J 2017 7 e618[cited 2018 Feb 9] 7 Available from httpwwwncbinlmnihgovpubmed29053158
5 Landgren O Graubard BI Katzmann JA et al Racial disparities in theprevalence of monoclonal gammopathies a population-based study of12 482 persons from the National Health and Nutritional ExaminationSurvey Leukemia [Internet] 2014 28 1537ndash1542 [cited 2018 Jun 22]Available from httpwwwncbinlmnihgovpubmed24441287
6 Cabrera Q Macro M Hebert B et al Epidemiology of monoclonal gamm-opathy of undetermined significance (MGUS) the experience from thespecialized registry of hematologic malignancies of Basse-Normandie(France) Cancer Epidemiol [Internet] 2014 38 354ndash356 [cited 2017 Oct24] Available from httpwwwncbinlmnihgovpubmed24880205
7 Therneau TM Kyle RA Melton LJ et al Incidence of monoclonal gamm-opathy of undetermined significance and estimation of duration beforefirst clinical recognition Mayo Clin Proc [Internet] 2012 [cited 2017 Dec23] 87 1071ndash1079 Available from httpwwwncbinlmnihgovpubmed22883742
8 Kyle RA Larson DR Therneau TM et al Long-term follow-up of mono-clonal gammopathy of undetermined significance N Engl J Med 2018[cited 2018 Apr 23] 378 241ndash249 Available from httpwwwncbinlmnihgovpubmed29342381
9 Dispenzieri A Katzmann JA Kyle RA et al Prevalence and risk of progres-sion of light-chain monoclonal gammopathy of undetermined significancea retrospective population-based cohort study Lancet [Internet] 2010[cited 2018 Feb 9] 375 1721ndash1728 Available from httpwwwncbinlmnihgovpubmed20472173
10 Steiner N Gobel G Suchecki P et al Monoclonal gammopathy of renalsignificance (MGRS) increases the risk for progression to multiple mye-loma an observational study of 2935 MGUS patients Oncotarget[Internet] 2018 [cited 2018 Apr 27] 9 2344ndash2356 Available from httpwwwncbinlmnihgovpubmed29416776
11 Dhodapkar MV Sexton R Waheed S et al Clinical genomic andimaging predictors of myeloma progression from asymptomaticmonoclonal gammopathies (SWOG S0120) Blood [Internet] 2014[cited 2018 Jun 22] 123 78ndash85 Available from httpwwwncbinlmnihgovpubmed24144643
12 Zand L Kattah A Fervenza FC et al C3 glomerulonephritis associatedwith monoclonal gammopathy a case series Am J Kidney Dis [Internet]2013 [cited 2017 Dec 29] 62 506ndash514 Available from httpwwwncbinlmnihgovpubmed23623956
13 Rajkumar SV Dimopoulos MA Palumbo A et al International MyelomaWorking Group updated criteria for the diagnosis of multiple myelomaLancet Oncol [Internet] 2014 [cited 2018 Jun 23] 15 e538ndashe548 Availablefrom httplinkinghubelseviercomretrievepiiS1470204514704425
Clinical implication of monoclonal gammopathies 9Downloaded from httpsacademicoupcomndtadvance-article-abstractdoi101093ndtgfy2595086133by gueston 29 August 2018
14 Ravindran A Bartley AC Holton SJ et al Prevalence incidence and sur-vival of smoldering multiple myeloma in the United States Nat PublishingGroup [Internet] 2016 6 2018ndash2023 [cited Jun] Available from httpswwwncbinlmnihgovpmcarticlesPMC5098258pdfbcj2016100apdf
15 Fermand J-P Bridoux F Kyle RA et al How I treat monoclonal gammop-athy of renal significance (MGRS) Blood [Internet] 2013 [cited 2017 Oct27] 122 3583ndash3590 Available from httpwwwncbinlmnihgovpubmed24108460
16 Bridoux F Leung N Hutchison CA et al Diagnosis of monoclonal gamm-opathy of renal significance Kidney Int [Internet] 2015 [cited 2017 Oct24] 87 698ndash711 Available from httpwwwncbinlmnihgovpubmed25607108
17 Kristinsson SY Bjorkholm M Andersson TM-L et al Patterns of survivaland causes of death following a diagnosis of monoclonal gammopathy ofundetermined significance a population-based study Haematologica[Internet] 2009 [cited 2018 Feb] 94 1714ndash1720 Available from httpwwwncbinlmnihgovpubmed19608666
18 Dimopoulos MA Delimpasi S Katodritou E et al Significant improve-ment in the survival of patients with multiple myeloma presenting with se-vere renal impairment after the introduction of novel agents Ann Oncol[Internet] 2014 [cited 2018 Apr 23] 25 195ndash200 Available from httpsacademicoupcomannoncarticle-lookupdoi101093annoncmdt483
19 Correia SO Santos S Malheiro J et al Monoclonal gammopathy of renalsignificance diagnostic workup WJN 2017 [cited 2017 Oct 27] 6 72ndash78Available from httpwwwncbinlmnihgovpubmed28316940
20 Lin J Markowitz GS Valeri AM et al Renal monoclonal immunoglobulindeposition disease the disease spectrum J Am Soc Nephrol [Internet] 2001[cited 2018 Jun 23] 12 1482ndash1492 Available from httpwwwncbinlmnihgovpubmed11423577
21 Sethi S Zand L Leung N et al Membranoproliferative glomerulonephritissecondary to monoclonal gammopathy Clin J Am Soc Nephrol [Internet]2010 [cited 2017 Dec 8] 5 770ndash782 Available from httpwwwncbinlmnihgovpubmed20185597
22 Bhutani G Nasr SH Said SM et al Hematologic characteristics of prolifer-ative glomerulonephritides with nonorganized monoclonal immunoglobu-lin deposits Mayo Clin Proc [Internet] 2015 [cited 2018 Jun 23] 90587ndash596 Available from httpwwwncbinlmnihgovpubmed25939936
23 Cohen C El-Karoui K Alyanakian M-A et al Light and heavy chain depo-sition disease associated with CH1 deletion Clin Kidney J [Internet] 2015[cited 2017 Oct 26] 8 237ndash239 Available from httpwwwncbinlmnihgovpubmed25815184
24 Nasr SH Valeri AM Cornell LD et al Renal monoclonal immunoglobulindeposition disease a report of 64 patients from a single institution Clin JAm Soc Nephrol [Internet] 2012 [cited 2018 Feb 9] 7 231ndash239 Availablefrom httpwwwncbinlmnihgovpubmed22156754
25 Sicard A Karras A Goujon J-M et al Light chain deposition disease with-out glomerular proteinuria a diagnostic challenge for the nephrologistNephrol Dial Transplant [Internet] 2014 [cited 2018 Jul 7] 29 1894ndash1902Available from httpwwwncbinlmnihgovpubmed24619059
26 Haas M A reevaluation of routine electron microscopy in the examinationof native renal biopsies J Am Soc Nephrol [Internet] 1997 8 70ndash76Available from httpwwwncbinlmnihgovpubmed9013450
27 Stokes MB Valeri AM Herlitz L et al Light chain proximal tubulopathyclinical and pathologic characteristics in the modern treatment era J AmSoc Nephrol [Internet] 2016 [cited 2018 Jun 23] 27 1555ndash1565 Availablefrom httpwwwncbinlmnihgovpubmed26374607
28 Larsen CP Messias NC Walker PD et al Membranoproliferative glomeru-lonephritis with masked monotypic immunoglobulin deposits Kidney Int[Internet] 2015 [cited 2018 Feb 10] 88 867ndash873 Available from httpwwwncbinlmnihgovpubmed26154922
29 Eirin A Irazabal MV Gertz MA et al Clinical features of patients with im-munoglobulin light chain amyloidosis (AL) with vascular-limited deposi-tion in the kidney Nephrol Dial Transplant [Internet] 2012 [cited 2018Feb 10] 27 1097ndash1101 Available from httpwwwncbinlmnihgovpubmed22067518
30 Alonso-Titos J Perea-Ortega L Sola E et al C3 glomerulonephritis associ-ated with monoclonal gammopathy of renal significance case report BMCNephrol 2018 Jul 6] 19 129 Available from httpwwwncbinlmnihgovpubmed29884135
31 Sayed RH Wechalekar AD Gilbertson JA et al Natural history and out-come of light chain deposition disease Blood [Internet] 2015 [cited 2017Dec 8] 126 2805ndash2810 Available from httpwwwncbinlmnihgovpubmed26392598
32 Mohan M Buros A Mathur P et al Clinical characteristics and prognosticfactors in multiple myeloma patients with light chain deposition diseaseAm J Hematol 2017 [cited 2018 Jul 7] 92 739ndash745 Available from httpwwwncbinlmnihgovpubmed28383130
33 Vignon M Cohen C Faguer S et al The clinicopathologic characteristicsof kidney diseases related to monotypic IgA deposits Kidney Int [Internet]2017 [cited 2018 Jul] 91 720ndash728 Available from httpwwwncbinlmnihgovpubmed28069266
34 Best Rocha A Larsen CP Membranous glomerulopathy with light chain-restricted deposits a clinicopathological analysis of 28 cases Kidney IntRep [Internet] 2017 [cited 2018 Jul 6] 2 1141ndash1148 Available from httpwwwncbinlmnihgovpubmed29270522
35 Nasr SH Valeri AM Sethi S et al Clinicopathologic correlations in multi-ple myeloma a case series of 190 patients with kidney biopsies Am JKidney Dis [Internet] 2012 [cited 2017 Oct 26] 59 786ndash794 Availablefrom httpwwwncbinlmnihgovpubmed22417785
36 Glavey SV Leung N Monoclonal gammopathy the good the bad and theugly Blood Rev [Internet] 2016 [cited 2017 Dec 24] 30 223ndash231 Availablefrom httpwwwsciencedirectcomsciencearticlepiiS0268960X15000946bb0130
37 Katzmann JA Kyle RA Benson J et al Screening panels for detection ofmonoclonal gammopathies Clin Chem [Internet] 2009 [cited 2017 Oct25] 55 1517ndash1522 Available from httpwwwncbinlmnihgovpubmed19520758
38 Yadav P Leung N Sanders PW et al The use of immunoglobulin lightchain assays in the diagnosis of paraprotein-related kidney disease KidneyInt [Internet] 2015 [cited 2018 Feb 9] 87 692ndash697 Available from httpwwwncbinlmnihgovpubmed25296094
39 Sugihara H Chihara D Seike K et al Percentage of urinary albumin excre-tion and serum-free light-chain reduction are important determinants ofrenal response in myeloma patients with moderate to severe renal impair-ment Blood Cancer J [Internet] 2014 [cited 2018 Jun 24] 4 e235 Availablefrom httpwwwncbinlmnihgovpubmed25083819
40 Leung N Gertz M Kyle RA et al Urinary albumin excretion patterns ofpatients with cast nephropathy and other monoclonal gammopathy-related kidney diseases Clin J Am Soc Nephrol [Internet] 2012 [cited 2018Jun 24] 7 1964ndash1968 Available from httpwwwncbinlmnihgovpubmed23024162
41 Ciocchini M Arbelbide J Musso CG Monoclonal gammopathy of renalsignificance (MGRS) the characteristics and significance of a new meta-entity Int Urol Nephrol [Internet] 2017 [cited 2017 Oct 26] 492171ndash2175 Available from httpwwwncbinlmnihgovpubmed28425076
42 Sethi S Rajkumar SV DrsquoAgati VD The complexity and heterogeneity ofmonoclonal immunoglobulinndashassociated renal diseases J Am Soc Nephrol2018 29 1810ndash1823
43 Hutchison CA Harding S Hewins P et al Quantitative assessment of se-rum and urinary polyclonal free light chains in patients with chronic kid-ney disease Clin J Am Soc Nephrol [Internet] 2008 [cited 2017 Dec 25] 31684ndash1690 Available from httpwwwncbinlmnihgovpubmed18945993
44 Jurczyszyn A Ochrem B Abnormal serum free light chain ratio does notalways indicate monoclonal gammopathy Polskie Archiwum MedycynyWewnetrznej [Internet] 2015 [cited 2017 Dec 29] 125 502ndash504 Availablefrom httpwwwncbinlmnihgovpubmed26266682
45 Singh G Serum free light chain assay and jk ratio performance inpatients with monoclonal gammopathy-high false negative rate for jk ra-tio J Clin Med Res 2017 [cited 2018 Jun 25] 9 46ndash57 Available fromhttpwwwncbinlmnihgovpubmed27924175
46 Fulton RB Fernando SL Serum free light chain assay reduces the need forserum and urine immunofixation electrophoresis in the evaluation ofmonoclonal gammopathy Ann Clin Biochem [Internet] 2009 [cited 2018Jun 25] 46 407ndash412 Available from httpwwwncbinlmnihgovpubmed19641008
10 K Batko et alDownloaded from httpsacademicoupcomndtadvance-article-abstractdoi101093ndtgfy2595086133by gueston 29 August 2018
47 Levinson SS Urine immunofixation electrophoresis remains importantand is complementary to serum free light chain Clin Chem Lab Med[Internet] 2011 [cited 2018 Jun 25] 49 1801ndash1804 Available from httpwwwncbinlmnihgovpubmed21663562 [CrossRef][Mismatch]
48 Lee WS Singh G Serum free light chains in neoplastic monoclonal gam-mopathies relative under-detection of lambda dominant KappaLambdaratio and underproduction of free lambda light chains as compared tokappa light chains in patients with neoplastic monoclonal gammopathiesJ Clin Med Res 2018 [cited 2018 Jun 25] 10 562ndash569 Available fromhttpwwwncbinlmnihgovpubmed29904440
49 Xu B Tang Y Zhou J et al Disease spectrum of abnormal serum free lightchain ratio and its diagnostic significance Oncotarget [Internet] 2017[cited 2017 Dec 29] 8 82268ndash82279 Available from httpwwwncbinlmnihgovpubmed29137262
50 Koo EH Shin J Jang HR et al Diagnostic performances of M-protein testsaccording to the clinical presentations of kidney disease Eur J Intern Med[Internet] 2016 [cited 2018 Feb 9] 33 88ndash92 Available from httpwwwncbinlmnihgovpubmed27421913
51 Gumber R Cohen JB Palmer MB et al A clone-directed approach mayimprove diagnosis and treatment of proliferative glomerulonephritis withmonoclonal immunoglobulin deposits Kidney Int [Internet] 2018 94199ndash205 Available from httpsdoiorg101016jkint201802020
52 Leung N Barnidge DR Hutchison CA Laboratory testing in monoclonalgammopathy of renal significance (MGRS) Clin Chem Lab Med [Internet]2016 [cited 2017 Oct 25] 54 929ndash937 Available from httpwwwncbinlmnihgovpubmed27107835 [CrossRef][Mismatch]
53 Ramirez-Alvarado M Ward CJ Huang BQ et al Differences in immuno-globulin light chain species found in urinary exosomes in light chain amy-loidosis (AL) PLoS ONE [Internet] 2012 [cited 2018 Jul 7] 7 e38061Available from httpwwwncbinlmnihgovpubmed22723846
54 Hogan JJ Weiss BM Bridging the divide an onco-nephrologic approachto the monoclonal gammopathies of renal significance Clin J Am SocNephrol [Internet] 2016 [cited 2017 Oct 26] 11 1681ndash1691 Availablefrom httpwwwncbinlmnihgovpubmed27416775
55 Vij R Mazumder A Klinger M et al Deep sequencing reveals myelomacells in peripheral blood in majority of multiple myeloma patients ClinLymphoma Myeloma Leuk [Internet] 2014 [cited 2017 Oct 25] 14131ndash139e1 Available from httpwwwncbinlmnihgovpubmed24629890
56 Gonsalves WI Leung N Rajkumar SV et al Improvement in renal func-tion and its impact on survival in patients with newly diagnosed multiplemyeloma Blood Cancer J 2015 [cited 2018 Feb 3] 5 e296 Available fromhttpwwwnaturecomdoifinder101038bcj201520
57 Dimopoulos MA Cheung MC Roussel M et al Impact of renal impair-ment on outcomes with lenalidomide and dexamethasone treatment in theFIRST trial a randomized open-label phase 3 trial in transplant-ineligiblepatients with multiple myeloma Haematologica [Internet] 2016 [cited2018 Jul 7] 101 363ndash370 Available from httpwwwncbinlmnihgovpubmed26659916
58 Ponisch W Andrea M Wagner I et al Successful treatment of patientswith newly diagnoseduntreated multiple myeloma and advanced renalfailure using bortezomib in combination with bendamustine and predni-sone J Cancer Res Clin Oncol 2012 [cited 2018 Jul 2] 138 1405ndash1412Available from httpwwwncbinlmnihgovpubmed22526157
59 Perry M Delarche A Ribes D et al Rituximab-cyclophosphamide-dexa-methasone is highly effective in patients with monoclonal Ig deposit-related glomerulopathy and indolent non-Hodgkin lymphomas Am JHematol 2014 [cited 2018 Jul 1] 89 969ndash973 Available from httpdoiwileycom101002ajh23798
60 Dimopoulos M Weisel K van de Donk Nwcj et al Pomalidomide pluslow-dose dexamethasone in patients with relapsedrefractory multiple my-eloma and renal impairment results from a Phase II trial J Clin Oncol2018 36 2035ndash2043
61 Fervenza FC Canetta PA Barbour SJ et al A multicenter randomized con-trolled trial of rituximab versus cyclosporine in the treatment of idiopathicmembranous nephropathy (MENTOR) Nephron [Internet] 2015 [cited2017 Dec 25] 130 159ndash168 Available from httpwwwncbinlmnihgovpubmed26087670
62 Dimopoulos MA Richardson PG Schlag R et al VMP (bortezomib mel-phalan and prednisone) is active and well tolerated in newly diagnosedpatients with multiple myeloma with moderately impaired renal functionand results in reversal of renal impairment cohort analysis of the Phase IIIVISTA study JCO 2009 [cited 2017 Dec 8] 27 6086ndash6093 Available fromhttpwwwncbinlmnihgovpubmed19858394
63 Morabito F Gentile M Mazzone C et al Safety and efficacy ofbortezomib-melphalan-prednisone-thalidomide followed by bortezomib-thalidomide maintenance (VMPT-VT) versus bortezomib-melphalan-prednisone (VMP) in untreated multiple myeloma patients with renal im-pairment Blood [Internet] 2011 [cited 2017 Dec 9] 118 5759ndash5766Available from httpwwwncbinlmnihgovpubmed21951682
64 Moreau P Masszi T Grzasko N et al Oral ixazomib lenalidomide anddexamethasone for multiple myeloma N Engl J Med 2016 [cited 2018 Apr27] 374 1621ndash1634 Available from httpwwwnejmorgdoi101056NEJMoa1516282
65 Nordstrom BL Knopf KB Teltsch DY et al The safety of bendamustine inpatients with chronic lymphocytic leukemia or non-Hodgkin lymphomaand concomitant renal impairment a retrospective electronic medical re-cord database analysis Leuk Lymphoma [Internet] 2014 [cited 2017 Dec13] 55 1266ndash1273 Available from httpwwwncbinlmnihgovpubmed23987821
66 Roussou M Kastritis E Christoulas D et al Reversibility of renal failure innewly diagnosed patients with multiple myeloma and the role of novelagents Leuk Res [Internet] 2010 [cited 2017 Dec 15] 34 1395ndash1397Available from httpwwwncbinlmnihgovpubmed20510452
67 Tosi P Zamagni E Tacchetti P et al Thalidomide-dexamethasone as in-duction therapy before autologous stem cell transplantation in patientswith newly diagnosed multiple myeloma and renal insufficiency BiolBlood Marrow Transplant [Internet] 2010 [cited 2018 Apr 27] 161115ndash1121 Available from httpwwwncbinlmnihgovpubmed20197100
68 Dimopoulos M Alegre A Stadtmauer EA et al The efficacy and safety oflenalidomide plus dexamethasone in relapsed andor refractory multiplemyeloma patients with impaired renal function Cancer [Internet] 2010116 3807 [cited 2017 Dec 15] Available from httpwwwncbinlmnihgovpubmed20564094
69 Siegel DS Weisel KC Dimopoulos MA et al Pomalidomide plus low-dosedexamethasone in patients with relapsedrefractory multiple myeloma andmoderate renal impairment a pooled analysis of three clinical trials LeukLymphoma [Internet] 2016 [cited 2017 Dec 15] 57 2833ndash2838 Availablefrom httpwwwncbinlmnihgovpubmed27267105
70 Dimopoulos MA Goldschmidt H Niesvizky R et al Carfilzomib or borte-zomib in relapsed or refractory multiple myeloma (ENDEAVOR) an in-terim overall survival analysis of an open-label randomised phase 3 trialLancet Oncol [Internet] 2017 [cited 2017 Dec 6] 18 1327ndash1337 Availablefrom httpwwwncbinlmnihgovpubmed28843768
71 Telio D Shepherd J Forrest D et al High-dose melphalan followed byauto-SCT has favorable safety and efficacy in selected patients with lightchain deposition disease and light and heavy chain deposition diseaseBone Marrow Transplant 2012 [cited 2017 Dec 8] 47 453ndash455 Availablefrom httpwwwnaturecomdoifinder101038bmt201187
72 Batalini F Econimo L Quillen K et al High-dose melphalan and stem celltransplantation in patients on dialysis due to immunoglobulin light-chainamyloidosis and monoclonal immunoglobulin deposition disease BiolBlood Marrow Transplant [Internet] 2018 [cited 2017 Dec 25] 24127ndash132 Available from httpwwwncbinlmnihgovpubmed28865972
73 Kourelis TV Nasr SH Dispenzieri A et al Outcomes of patients with renalmonoclonal immunoglobulin deposition disease Am J Hematol 2016[cited 2018 Jul 2] 91 1123ndash1128 Available from httpwwwncbinlmnihgovpubmed27501122
74 Pozzi C DrsquoAmico M Fogazzi GB et al Light chain deposition disease withrenal involvement clinical characteristics and prognostic factors Am JKidney Dis [Internet] 2003 [cited 2018 Jun 23] 42 1154ndash1163 Availablefrom httpwwwncbinlmnihgovpubmed14655186
75 Song M-K Chung J-S Shin H-J et al Cyclophosphamide-containing regi-men (TCD) is superior to melphalan-containing regimen (MPT) in elderlymultiple myeloma patients with renal impairment Ann Hematol
Clinical implication of monoclonal gammopathies 11Downloaded from httpsacademicoupcomndtadvance-article-abstractdoi101093ndtgfy2595086133by gueston 29 August 2018
[Internet] 2012 [cited 2017 Dec 9] 91 889ndash896 Available from httpwwwncbinlmnihgovpubmed22237937
76 Specter R Sanchorawala V Seldin DC et al Kidney dysfunction duringlenalidomide treatment for AL amyloidosis Nephrol Dial Transplant[Internet] 2011 [cited 2018 Jul 7] 26 881ndash886 Available from httpwwwncbinlmnihgovpubmed20693160
77 Li Y Wang X OrsquoMara E et al Population pharmacokinetics of pomalido-mide in patients with relapsed or refractory multiple myeloma with variousdegrees of impaired renal function CPAA 2017 [cited 2018 Feb 4] 9133ndash145 Available from httpwwwncbinlmnihgovpubmed29184451
78 Kastritis E Gavriatopoulou M Roussou M et al Addition of cyclophos-phamide and higher doses of dexamethasone do not improve outcomes ofpatients with AL amyloidosis treated with bortezomib Blood Cancer J2017 [cited 2017 Dec 15] 7 e570 Available from httpwwwncbinlmnihgovpubmed28622303
79 Venner CP Gillmore JD Sachchithanantham S et al A matched compari-son of cyclophosphamide bortezomib and dexamethasone (CVD) versusrisk-adapted cyclophosphamide thalidomide and dexamethasone (CTD)in AL amyloidosis Leukemia [Internet] 2014 [cited 2018 Jul 5] 282304ndash2310 Available from httpwwwncbinlmnihgovpubmed25027514
80 Palladini G Sachchithanantham S Milani P et al A European collabora-tive study of cyclophosphamide bortezomib and dexamethasone inupfront treatment of systemic AL amyloidosis Blood [Internet] 2015[cited 2017 Dec 9] 126 612ndash615 Available from httpwwwncbinlmnihgovpubmed25987656
81 Kopel T Kaufman JS Hamburg N et al Endothelium-dependent and -in-dependent vascular function in advanced chronic kidney disease CJASN2017 [cited 2018 Apr 18] 12 1588ndash1594 Available from httpcjasnasnjournalsorglookupdoi102215CJN12811216
82 Palladini G Milani P Foli A et al A Phase 2 trial of pomalidomide anddexamethasone rescue treatment in patients with AL amyloidosis Blood[Internet] 2017 [cited 2018 Apr 26] 129 2120ndash2123 Available fromhttpwwwncbinlmnihgovpubmed28130212
83 Hegenbart U Bochtler T Benner A et al Lenalidomidemelphalandexa-methasone in newly diagnosed patients with immunoglobulin light chainamyloidosis results of a prospective phase 2 study with long-term followup Haematologica [Internet] 2017 [cited 2017 Dec 26] 102 1424ndash1431Available from httpwwwncbinlmnihgovpubmed28522573
84 Palladini G Milani P Foli A et al Oral melphalan and dexamethasonegrants extended survival with minimal toxicity in AL amyloidosis long-term results of a risk-adapted approach Haematologica [Internet] 2014[cited 2017 Dec 15] 99 743ndash750 Available from httpwwwncbinlmnihgovpubmed24213149
85 Payet J Livartowski J Kavian N et al Type I cryoglobulinemia in multiplemyeloma a rare entity analysis of clinical and biological characteristics ofseven cases and review of the literature Leuk Lymphoma [Internet] 201354 767ndash777 Available from httpwwwtandfonlinecomdoifull103109104281942012671481
86 Terpos E Kleber M Engelhardt M et al European Myeloma Networkguidelines for the management of multiple myeloma-related complica-tions Haematologica [Internet] 2015 [cited 2017 Dec 4] 100 1254ndash1266Available from httpwwwncbinlmnihgovpubmed26432383
87 Chanan-Khan AA Kaufman JL Mehta J et al Activity and safety of borte-zomib in multiple myeloma patients with advanced renal failure a multi-center retrospective study Blood [Internet] 2007 [cited 2018 Jul 2] 1092604ndash2606 Available from httpwwwncbinlmnihgovpubmed17138816
88 Dimopoulos MA Roussou M Gkotzamanidou M et al The role of novelagents on the reversibility of renal impairment in newly diagnosed symp-tomatic patients with multiple myeloma Leukemia 2013 27 423ndash429
89 Kouroukis TC Baldassarre FG Haynes AE et al Bortezomib in multiplemyeloma systematic review and clinical considerations Curr Oncol(Toronto Ont) [Internet] 2014 [cited 2017 Dec 4] 21 e573ndashe603Available from httpwwwncbinlmnihgovpubmed25089109
90 Zhu W Chen W Bortezomib-based treatment for multiple myelomapatients with renal impairment a systematic review and meta-analysis ofobservational studies Medicine [Internet] 2016 95 e5202 Available fromhttpwwwncbinlmnihgovpmcarticlesPMC5120900
91 Dimopoulos MA Terpos E Chanan-Khan A et al Renal impairment inpatients with multiple myeloma a consensus statement on behalf of theInternational Myeloma Working Group JCO 2010 28 4976ndash4984
92 Chauvet S Fremeaux-Bacchi V Petitprez F et al Treatment of B-cell disor-der improves renal outcome of patients with monoclonal gammopathyndashassociated C3 glomerulopathy Blood [Internet] 2017 [cited 2017 Oct 26]129 1437ndash1447 Available from httpwwwncbinlmnihgovpubmed28069603
93 Cohen C Royer B Javaugue V et al Bortezomib produces high hematolog-ical response rates with prolonged renal survival in monoclonal immuno-globulin deposition disease Kidney Int [Internet] 2015 [cited 2017 Dec25] 88 1135ndash1143 Available from httpwwwncbinlmnihgovpubmed26176826
94 Ziogas DC Kastritis E Terpos E et al Hematologic and renal improve-ment of monoclonal immunoglobulin deposition disease after treatmentwith bortezomib-based regimens Leuk Lymphoma [Internet] 2017 [cited2017 Dec 25] 58 1832ndash1839 Available from httpwwwncbinlmnihgovpubmed27967286
95 Milani P Merlini G Palladini G Novel therapies in light chain amyloid-osis Kidney Int Rep [Internet] 2018 [cited 2018 Jul 4] 3 530ndash541 Availablefrom httpwwwncbinlmnihgovpubmed29854961
96 Spizzo G Mitterer M Gunsilius E Bortezomib for the treatment of refrac-tory Type-1 cryoglobulinaemia Br J Haematol [Internet] 2010 [cited 2018Jul 7] 150 235ndash237 Available from httpdoiwileycom101111j1365-2141201008184x
97 Talamo G Claxton D Tricot G et al Response to bortezomib in refractoryType I cryoglobulinemia Am J Hematol 2008 [cited 2018 Jul 7] 83883ndash884 Available from httpwwwncbinlmnihgovpubmed18756542
98 Dimopoulos MA Roussou M Gavriatopoulou M et al Cardiac and renalcomplications of carfilzomib in patients with multiple myeloma BloodAdv 2017 [cited 2017 Dec 6] 1 449ndash454 Available from httpwwwbloodadvancesorglookupdoi101182bloodadvances2016003269
99 Strati P Nasr SH Leung N et al Renal complications in chronic lympho-cytic leukemia and monoclonal B-cell lymphocytosis the Mayo Clinic ex-perience Haematologica [Internet] 2015 [cited 2018 Jul 3] 100 1180ndash1188Available from httpwwwncbinlmnihgovpubmed26088927
100 Salama AD Pusey CD Drug insight rituximab in renal disease and trans-plantation Nat Clin Pract Nephrol [Internet] 2006 [cited 2017 Dec 8] 2221ndash230 Available from httpwwwnaturecomdoifinder101038ncpneph0133
101 Jillella AP Dainer PM Kallab AM et al Treatment of a patient with end-stage renal disease with rituximab pharmacokinetic evaluation suggestsrituximab is not eliminated by hemodialysis Am J Hematol 2002 [cited2018 Jul] 71 219ndash222 Available from httpwwwncbinlmnihgovpubmed12410580
102 Guiard E Karras A Plaisier E et al Patterns of noncryoglobulinemic glo-merulonephritis with monoclonal Ig deposits correlation with IgG sub-class and response to rituximab Clin J Am Soc Nephrol 2011 6 1609ndash1616
103 Ribes D Hachem HEL Oberic L et al Bendamustine plus rituximab forindolent B-cell lymphoma of renal significance Am J Hematol 2018 93356ndash362
104 Darwish M Bond M Hellriegel E et al Pharmacokinetic and pharmacody-namic profile of bendamustine and its metabolites Cancer ChemotherPharmacol 2015 [cited 2017 Dec 15] 75 1143ndash1154 Available from httpwwwncbinlmnihgovpubmed25829094
105 Ponisch W Moll B Bourgeois M et al Bendamustine and prednisone incombination with bortezomib (BPV) in the treatment of patients with re-lapsed or refractory multiple myeloma and light chain-induced renal fail-ure J Cancer Res Clin Oncol [Internet] 2013 [cited 2018 Jul 2] 1391937ndash1946 Available from httpwwwncbinlmnihgovpubmed24046251
106 Mateos M-V Dimopoulos MA Cavo M et al Daratumumab plus bortezo-mib melphalan and prednisone for untreated myeloma N Engl J Med2018 378 518ndash528
107 Rocchi S Tacchetti P Pantani L et al Safety and efficacy of daratumumabin dialysis-dependent renal failure secondary to multiple myelomaHaematologica [Internet] 2018 [cited 2018 Jul 2] 103 e277ndashe278 Availablefrom httpwwwncbinlmnihgovpubmed29622654
12 K Batko et alDownloaded from httpsacademicoupcomndtadvance-article-abstractdoi101093ndtgfy2595086133by gueston 29 August 2018
108 Anand S Miller D Chipman G Morris D Srinivas S Daratumumab forsevere refractory proliferative glomerulonephritis with monoclonal im-mune deposits (PGNMID) ATC Abstr [Internet] 2017 [cited 2018 Jul 3]Available from httpsatcmeetingabstractscomabstractdaratumumab-for-severe-refractory-proliferative-glomerulonephritis-with-monoclonal-immune-deposits-pgnmid
109 Leung N Lager DJ Gertz MA et al Long-term outcome of renal transplan-tation in light-chain deposition disease Am J Kidney Dis [Internet] 2004[cited 2018 Feb 9] 43 147ndash153 Available from httpwwwncbinlmnihgovpubmed14712438
110 Lorenz EC Sethi S Leung N et al Recurrent membranoproliferative glo-merulonephritis after kidney transplantation Kidney Int [Internet] 2010[cited 2018 Feb 9] 77 721ndash728 Available from httpwwwncbinlmnihgovpubmed20130531
111 Leung N Nasr SH A patient with abnormal kidney function and a mono-clonal light chain in the urine Clin J Am Soc Nephrol 2016 11 1073ndash1082
112 Cibeira MT Sanchorawala V Seldin DC et al Outcome of AL amyloidosisafter high-dose melphalan and autologous stem cell transplantation long-term results in a series of 421 patients Blood [Internet] 2011 [cited 2018Feb 3] 118 4346ndash4352 Available from httpwwwncbinlmnihgovpubmed21828140
113 Gertz MA Lacy MQ Dispenzieri A et al Autologous stem cell transplantfor immunoglobulin light chain amyloidosis a status report LeukLymphoma [Internet] 2010 [cited 2018 Feb 3] 51 2181ndash2187 Availablefrom httpwwwncbinlmnihgovpubmed20958232
114 Leung N Kumar SK Glavey SV et al The impact of dialysis on the survivalof patients with immunoglobulin light chain (AL) amyloidosis undergoingautologous stem cell transplantation Nephrol Dial Transplant 2016 [cited2018 Jul 7] 31 1284ndash1289 Available from httpsacademicoupcomndtarticle-lookupdoi101093ndtgfv328
115 Badros A Barlogie B Siegel E et al Results of autologous stem cell trans-plant in multiple myeloma patients with renal failure Br J Haematol 2001[cited 2018 Jul 7] 114 822ndash829 Available from httpwwwncbinlmnihgovpubmed11564069
116 Soltero L Carbajal H Xu J et al Initial survival data of kidney transplantpatients with pre-transplant monoclonal gammopathy Clin Transplant[Internet] 2012 [cited 2018 Feb 3] 26 300ndash304 Available from httpwwwncbinlmnihgovpubmed22044717
117 Jimenez-Zepeda VH Heilman RL Engel RA et al Monoclonal gammopathyof undetermined significance does not affect outcomes in patients undergoingsolid organ transplants Transplantation [Internet] 2011 [cited 2018 Feb 3]92 570ndash574 Available from httpwwwncbinlmnihgovpubmed21712755
118 Naina HVK Harris S Dispenzieri A et al Long-term follow-up of patientswith monoclonal gammopathy of undetermined significance after kidney
transplantation Am J Nephrol 2012 [cited 2018 Feb] 35 365ndash371Available from httpwwwncbinlmnihgovpubmed22473253
119 Bansal T Garg A Snowden JA et al Defining the role of renal transplanta-tion in the modern management of multiple myeloma and other plasmacell dyscrasias Nephron Clin Pract [Internet] 2012 [cited 2018 Feb 3] 120c228 wwwkargercom
120 Hassoun H Flombaum C DrsquoAgati VD et al High-dose melphalan andauto-SCT in patients with monoclonal Ig deposition disease Bone MarrowTransplant 2008 [cited 2018 Feb 3] 42 405ndash412 Available from httpwwwncbinlmnihgovpubmed18574442
121 Herrmann SMS Gertz MA Stegall MD et al Long-term outcomes ofpatients with light chain amyloidosis (AL) after renal transplantation withor without stem cell transplantation Nephrol Dial Transplant [Internet]2011 [cited 2018 Feb 3] 26 2032ndash2036 Available from httpwwwncbinlmnihgovpubmed21543655
122 Lorenz EC Gertz MA Fervenza FC et al Long-term outcome of autolo-gous stem cell transplantation in light chain deposition disease NephrolDial Transplant [Internet] 2008 [cited 2018 Jul 5] 23 2052ndash2057 Availablefrom httpwwwncbinlmnihgovpubmed18178602
123 Merhi B Patel N Bayliss G et al Proliferative glomerulonephritis withmonoclonal IgG deposits in two kidney allografts successfully treated withrituximab Clin Kidney J [Internet] 2017 [cited 2018 Feb 10] 10 405ndash410Available from httpsacademicoupcomckjarticle-lookupdoi101093ckjsfx001
124 Barbour SJ Beaulieu MC Zalunardo NY et al Proliferative glomerulone-phritis with monoclonal IgG deposits secondary to chronic lymphocyticleukemia Report of two cases Nephrol Dial Transplant [Internet] 2011[cited 2018 Feb 10] 26 2712ndash2714 Available from httpsacademicoupcomndtarticle-lookupdoi101093ndtgfr251
125 Zand L Lorenz EC Cosio FG et al Clinical findings pathology and out-comes of C3GN after kidney transplantation J Am Soc Nephrol [Internet]2014 [cited 2018 Jul 5] 25 1110ndash1117 Available from httpwwwncbinlmnihgovpubmed24357668
126 Alfano G Fontana F Colaci E et al Monoclonal gammopathy of undeter-mined significance after kidney transplantation Transplantation [Internet]2017 [cited 2017 Oct 24] 101 e337ndashe342 Available from httpwwwncbinlmnihgovpubmed28731904
127 Bancu I Ca~nas L Juega FJ et al Outcomes of monoclonal gammopathyof undetermined significance in patients who underwent kidneytransplantation Transplant Proc [Internet] 2015 [cited 2018 Feb 10] 472344ndash2345 Available from httpwwwncbinlmnihgovpubmed26518922
Received 2632018 Editorial decision 1472018
Clinical implication of monoclonal gammopathies 13Downloaded from httpsacademicoupcomndtadvance-article-abstractdoi101093ndtgfy2595086133by gueston 29 August 2018

and requires a specific approach In a review of 40 crystallineLCPT cases (21 patients classified to MGRS) paraffin IFE withprotease digestion antigen retrieval technique was required forcorrect diagnosis [27] Furthermore in biopsy findings of C3GN or membranoproliferative GN paraffin immunofixation(IF) with protease digestion may unmask MIg deposits and dis-cover MGRS [28]
Extrarenal lesions in MGRS are not uncommon Amyloiddeposits can be limited to the vasculature marking a differentclinical profile [29] In patients with C3 GN associated withmonoclonal gammopathy C3 deposits may coexist in renal andcutaneous vessels [30] Perhaps better understanding of patho-genesis will allow for targeting the mechanism of tissue injuryIn LCDD extrarenal manifestations may occur in the heart andliver [31 32] Cardiac manifestations are reported in 13 of MMpatients with LCDD and are associated with shorter survivaland worse treatment outcomes It is important to note that 85of those patients had MM while in studies where MM rateswere lower [23 24] the rate of cardiac involvement was only10 In rare cases LCDD patients may present without pro-teinuria with tubulointerstitial lesions where nephrologistsmight not screen for monoclonal gammopathy [25]Nephrologists and pathologists should closely cooperate withatypical and typical manifestations of rare diseases In 13 ofIgAndashPGNMID patients the initial diagnosis was IgA nephropa-thy despite the presence of MIg glomerular deposits resultingin a lack of haematological evaluation which is crucial inMGRS [33] Another difficulty in diagnosis may be related tomembranous nephropathy with singular monoclonal IgGwhich requires staining for phospholipase A2 receptor beforeinvestigating a low-grade malignancy [34]
I N V E S T I G A T I O N I N T O M G R S
Presenting symptoms should be closely evaluated and docu-mented MGUS is more commonly seen in older individuals asare metabolic disorders which can mimic MGRS clinicallyUnexplained RI or abnormalities such as proteinuria requireextensive testing AL amyloidosis is suspected with albuminuria(gt50 in urine electrophoresis) nephrotic syndrome and rela-tively preserved kidney function as opposed to MIDD [35]Cryoglobulinaemia (CG) Type I may present with hyperviscos-ity linked symptoms and Type II with skin lesions and vasculi-tis [36] The latter may be related to hepatitis C virus infectionin which case antiviral therapy should be promptly initiated [2]MIDD commonly causes asymptomatic multi-organ involve-ment [16]
SPEP is the most basic quantitative screening test for mono-clonal proteins owing to its general availability and low costSPEP is positive in 819 of MGUS 659 of AL and 556 ofLCDD [37] To increase sensitivity in MGRS it should alwaysbe combined with IF and respective urine studies UPEP andurine IF [16] IF is purely qualitative but it allows for identifica-tion of the MIg isotype Due to low disease burden of MGRS apossible migration of M proteins to different fractions and ahigh limit of detection in SPEP (500 mgL) compared with IF(150 mgdL) a negative SPEP does not exclude MGRS andshould be used together IF [38] Despite lower overall sensitivity
to SPEP the rationale for including the UPEP can be drawnfrom characteristic patterns which may be indicative of a pri-mary disease such as high urine albumin excretion in MIDD orAL amyloidosis or use in monitoring RI in MM [39 40] Theadditional use of antibodies targeting epitopes of sFLC detectscases missed by urine assay though it is also true for the reverseas such both assays cannot be replaced [37] Urine free lightchain assays should not be utilized as there are no establishednormal ranges [41] The established normal range for thekappalambda ratio is 026ndash165 whereas in patients with renaldysfunction a range of 034ndash31 is considered normal [42] Ithas been suggested that the lower threshold should be raised forproliferative glomerulonephritides with non-organized glomer-ular MIg deposition [22] sFLC should be assessed with theknowledge that kappa monomers are more easily filtered com-pared with lambda dimers Renal dysfunction defined as an ab-normal creatinine clearance (CrCl) results in elevated sFLCthough usually but not always with a maintained kappalambdaratio (21) [43] Thus all instances of a abnormal sFLC valuesshould not be immediately attributed to a monoclonal gamm-opathy [44] In a retrospective data review of 76 MGUS (295observations) patients sFLCs were observed with agt55 false-negative ratio compared with electrophoretic studies [45]Conversly Fulton et al [46] analysed 219 cases with all urineand serum studies to a conclusion of sFLC and SPEP detecting6 more cases than SPEPIF and UPEPIF Several authorshave indicated that studies criticizing IFE may use incorrectmethodology while urine studies are of equal sensitivity andmay be more useful in low burden light chain clones especiallylambda dominant [47 48] Katzmann et al [37] observed thatSPEP and sFLC is the most effective basic screening panel inidentifying several MGRS conditions In LCDD 42 of patientspresented with no abnormalities in SPEPIFE but FLCs wasraised in all and matched the isotype in biopsy [25] FLCs arenot universally accepted and must be performed in combina-tion with urine and serum studies A cut-off value of kappalambda ratio gt289 of 92 sensitivity and 97 specificity areestablished for plasma cell malignancy at an estimated glomeru-lar filtration rate (eGFR) lt60 mLmin173 m2 howeverMGRS specific light chain values require further study [49] In17 MGRS patients with nephritic range proteinuria serum andurine IF with sFLC was 100 sensitive Although three patientswith chronic glomerulonephritides were identified by sFLC andserum IF the results do not reliably reflect the spectrum ofMGRS In PGNMIDnon-IgG GN the detection rate is esti-mated at 32 for serum IF and sFLC [22 50] Another study on19 PGNMID patients reported an overall paraprotein andclonal detection rate of 37 and 32 respectively [51] In thethese conditions if testing for either serum IFE or sFLC is posi-tive bone marrow investigation with flow cytometry and im-munohistochemical study may uncover a pathological cloneDetermination of the best diagnostic algorithm is difficult and ifthere is a strong suspicion of MGRS all five tests should be or-dered At present there is no standard testing for the heteroge-nous presentation(s) of MGRS due to different diseasesubtypes
Clinical implication of monoclonal gammopathies 3Downloaded from httpsacademicoupcomndtadvance-article-abstractdoi101093ndtgfy2595086133by gueston 29 August 2018
Without chemotherapy there is a high recurrence rate ofMGRS conditions post-renal transplant and prioritizing func-tional improvement requires early diagnosis as opposed to thepassive monitoring in MGUS [2] (Table 3) Recent advancespoint to time of flight mass spectrometry (MS) without theneed for expensive proteomic analysis though the ability to dis-criminate and identify the pathological protein has to be dem-onstrated [52] Laser microdissection and MS proteomics arerecommended to confirm AL amyloidosis cases of abnormalMIDD with truncated MIg or instances where the specific MIgregion is of interest [19 42] Urinary exosomes which have dif-ferent characteristics in AL amyloidosis and MGUS combinedwith MS may become the diagnostic and monitoring tools aftermore evidence is available [53] In daily practice parameters ofkidney function creatinine and proteinuria can be comparedwith assessment of the course of progression and response totreatment [54] However first-line monitoring should includeparaprotein levels and indirect disease activity markers whichtrack evolution of the primary disease
Non-invasive screening tools for on-going diagnosis of plasmacell dyscrasia particularly in difficult to identify MGRS condi-tions are of interest Vij et al [55] reported on deep sequencingof peripheral blood demonstrating clonal plasma cells in 96 ofMM patients In the case of IgM MGRS which suggests the pres-ence of B-celllymphoplasmacytic clone it is necessary to attemptto specify the clonal population through bone marrow andorlymph node biopsy and radiographic imaging [2 16] F18 posi-tron emission computed tomography can identify potential ab-normal lymph nodes for biopsy in conjunction with peripheralblood flow cytometry [54] MRI to exclude marrow involvementmay also be considered With the heterogeneity of MGRS asidefrom determining the conclusive histopathology character exclu-sion of plasma cell malignancy is necessary
T R E A T M E N T F O R M G R S mdash A N O V E R V I E W
A multi-disciplinary collaboration between nephrologist pa-thologist and haematologist is a priority in the diagnosis andtreatment of these individuals Therapy should incorporate bi-opsy-driven diagnosis with particular clinical features and dis-ease course prediction Identification of the clone responsiblefor MGRS and appropriate haematological treatment shouldtranslate into better RR and prevention of progression MGRSpatients with doubled serum creatinine or reduced renal func-tion may be at higher risk of haematological progression (oddsratio 26 CI 03ndash24) [10] In MM the reversal of RI has beenshown to improve outcome [56] Treatment of CD20thorn clonesshould utilize rituximab (RTX) while MGRS conditions par-ticularly non-IgM MGRS should consider MM regimens asprovided below and summarized in Table 1 With the rarityand wide array of MGRS conditions establishing strong evi-dence for treatment is difficult and evidence is limited to anec-dotal cases or small patient series
C Y T O T O X I C D R U G S
Historically melphalan-prednisone (MP) was used for thetreatment of plasma cell dyscrasias but due to the low response T
able
1T
hera
peut
icre
gim
ens
for
prim
ary
MG
RS
con
diti
ons
Dru
gC
hara
cter
Dis
ease
char
acte
rSe
veri
tyof
kidn
eyin
suff
icie
ncy
Ref
eren
ce
Lena
lidom
ide
LoD
exM
PT
Clin
ical
tria
lM
Mw
ith
RI
149
pati
ents
CrC
llt30
mL
min
372
pts
CrC
l30
lt50
Dim
opou
los
etal
[57
]B
enda
mus
tine
PV
Ret
rosp
ecti
veM
Mw
ith
RI
18eG
FRlt
35m
Lm
in(1
1pt
seG
FR15
mL
min
)P
onis
chet
al[
58]
RT
XC
YC
Dex
Ret
rosp
ecti
veIn
dole
ntN
HL
Glo
mer
ulon
ephr
itis
rela
ted
toM
Ig14
pts
(71
5w
ith
eGFR
lt60
mL
min
)P
erry
etal
[59
]
PO
ML
oDex
Clin
ical
tria
lR
elap
sed
refr
acto
ryM
Mw
ith
RI
Thr
eeco
hort
smdash33
eGFR
30ndash4
5m
Lm
inpt
s34lt
30m
Lm
ineG
FRpt
s14
HD
pts
Dim
opou
los
etal
[60
]
RT
XC
linic
altr
ial
Mem
bran
ous
neph
ropa
thy
eGFR
40P
rote
inur
ia
5g
24h
Ferv
enza
etal
[61
]V
MP
vers
usM
PC
linic
altr
ial
MM
wit
hR
I34
ptslt
30m
Lm
inG
FR1
93pt
sG
FR31
ndash50
mL
min
Dim
opou
los
etal
[62
]V
MP
TndashV
Tve
rsus
VM
PC
linic
altr
ial
MM
wit
hR
I33
ptslt
30m
Lm
ineG
FR1
16pt
seG
FR31
ndash50
mL
min
Mor
abit
oet
al[
63]
Ixaz
omib
Lena
lidom
idendash
Dex
Clin
ical
tria
lR
efra
ctor
yre
laps
edM
M10
pts
CrC
llt30
mL
min
169
pts
CrC
l30ndash
60m
Lm
inM
orea
uet
al[
64]
Ben
tam
usti
nem
onot
hera
py
wit
hR
TX
Ret
rosp
ecti
veC
LLN
HL
104
pts
CrC
llt40
mL
min
Nor
dstr
omet
al[
65]
Vve
rsus
IMiD
vers
usC
CC
linic
altr
ial
MM
wit
hR
I55
pts
CrC
llt30
mL
min
(9di
alys
is)
41pt
sC
rCl
30lt
50m
Lm
inR
ouss
ouet
al[
66]
T-D
exC
linic
altr
iald
ata
MM
wit
hR
Ipr
ior
toA
SCT
(ind
ucti
onth
erap
y)16
pts
CrC
llt30
mL
min
15
pts
CrC
l30ndash
50m
Lm
in(t
otal
7on
HD
)T
osie
tal
[67]
L-D
exT
wo
clin
ical
tria
lsM
MR
Ive
rsus
non-
RI
16pt
sC
rCllt
30m
Lm
inC
rCl
30lt
60in
82pt
sD
imop
oulo
uset
al[
68]
PO
Mndashl
owD
exT
hree
clin
ical
tria
lsM
Mw
ith
RI
355
pts
wit
hC
rCl
30an
dlt
60m
Lm
in(1
66pt
sC
rCl
30lt
45)
Sieg
elet
al[
69]
Car
filzo
mib
Dex
vers
usB
orte
zom
ibD
exC
linic
altr
ial
Rel
apse
dre
frac
tory
MM
56pt
sC
rCllt
30m
Lm
in1
28pt
sw
ith
CrC
l30ndash
50m
Lm
inD
imop
oulo
set
al[
70]
Vb
orte
zom
ibM
mel
phal
anL
len
alid
omid
eT
tha
lidom
ide-
dexa
met
haso
ne
Vb
orte
zom
ibC
Cc
onve
ntio
nalc
hem
othe
rapy
CLL
chr
onic
lym
phoc
ytic
leuk
aem
iaN
HL
non-
Hod
gkin
lym
phom
apt
spa
tien
ts
4 K Batko et alDownloaded from httpsacademicoupcomndtadvance-article-abstractdoi101093ndtgfy2595086133by gueston 29 August 2018
rates has been replaced by more potent regimens In LCDDwith MGUS MP and plasmapheresis prolonged survival how-ever kidney function deteriorated which marks the inefficiencyof the old regimes
To achieve a higher and more durable haematological re-sponse (HR) and potentially to qualify for kidney transplant(Ktx) high-dose melphalan supported with autologous stemcell transplantation (ASCT) is considered highly efficacious inMM and AL SCT has been shown to improve survival in ALamyloidosis and MIDD [71 72] Achieving a very good partialresponse (VGPR)complete response (CR) is associated with abetter RR rate than a HR lt VGPR [31 32 73] Importantly anadvanced impairment of renal function may impact responseindependently of achieving HR [32 74] Preventing renal dam-age will likely only be achieved by earlier diagnosis
I M M U N O M O D U L A T O R Y A G E N T S
Thalidomide the first immunomodulatory drug (IMiD) agentapproved for the treatment of myeloma can be safely adminis-tered regardless of renal function Outside the USA thalido-mide remains a viable choice in CrCl lt50 mLmin1 73 m2since it is not renally cleared [67] Song et al [75] report that inpatients with a low glomerular filtration rate (GFR) defined aslt40 mLmin173 m2 cyclophosphamide (CYC) was betterthan MP when combined with thalidomide with regard to re-nal functional improvement adverse events overall survival(OS) and mortality due to infection (P lt 0001) Lenalidomideis renally cleared and doses need to be adjusted for renal insuffi-ciency (CrCl lt60 mLmin) Complete blood counts should beperformed on a regular basis in the setting of moderate to severerenal insufficiency so that the lenalidomide dose may be modi-fied in the setting of unacceptable cytopenias [68] In a study of41 AL amyloidosis patients treated with lenalidomide 66were observed with kidney dysfunction and 10 required dialy-sis [76] However for approximately 25 of patients the initialdoses were too high and for half dosage was not appropriatelyadjusted Another aspect was older age and worse renal statusin those who experienced more severe impairment Recently alarge MM trial reported that renal function-adapted lenalido-mide dose resulted in similar safety across all levels of RI(Table 1) [57]
Pomalidomide (POM) is effective in lenalidomide-refractorycases and suitable for any CrCl (Table 1) However the recom-mendation for patients on dialysis is 3 mg rather than the stan-dard 4 mg dose and should be administered following dialysis[77] The latest results of POM and low-dose dexamethasone(LoDex) showed acceptable safety of 4 mgday in patients witheGFRlt30 mLmin173 m2 and on dialysis though CR wasonly achieved in eGFR 30ndash45 mLmin173 m2 [60] IMiDshave been used with effectiveness in MM AL amyloidosisMIDD CG Type 1 and LCPT (Tables 1 and 2) [27 31 85]
P R O T E A S O M E I N H I B I T O R S mdash N O V E L D R U G S
In 2015 bortezomib a first-generation proteasome inhibitorwas established as a class 1 A treatment (BDex) standard by theEuropean Myeloma Network for MM with RI [86] Bortezomib
showed a favourable profile with metabolism independent ofkidney function and demonstrated to be beneficial in advancedrenal failure and dialysis [87 88] A systematic review in 2014concluded that bortezomib was preferable to other agents inMM with RI [89] The most prominent adverse event is periph-eral neuropathy which may be a troublesome side effect in of-ten mildly symptomatic MGRS conditions Bortezomibpromotes a high rate of haematological CR as well as RR inMM with RI [90] High-dose Dex is linked to a faster RR how-ever mildly symptomatic MGRS patients may not be willing tocomply with the side effects whereas treatment-wise achievinga faster RR may improve the disease course [88] Bortezomibhigh-dose Dex is recommended by the IMWG for patients withMM-related RI whereas a three-drug scheme is deemed to im-prove RR [91]
In 50 patients with C3 glomerulopathy associated withmonoclonal gammopathy chemotherapy effectively achievedHR the only predictor of RR in multivariate analysis into sig-nificantly higher RR and renal survival rates compared withstandard immunosuppression [92] Bortezomib-based regimesmade up 76 of the chemotherapy group also being signifi-cantly associated with RR in univariate analysis Bortezomib-based treatment in 49 patients with MIDD reported at least aVGPR in 704 with HR not significantly different fromHDMSCT [93] Maintained haematological remission was as-sociated with survival in all patients at 85 months follow-up incomparison with 52 at 48 months in a series published in2003 [74] Ziogas et al [94] reported on 18 MIDD patientstreated exclusively with bortezomib regimes with gt VGPR in333 and an equal number progressing to end-stage renal dis-ease (ESRD) In the 2003 study by Pozzi et al progression wassimilar at 368 suggesting that even late induction of noveltherapy will not overcome poor prognosis associated with ad-vanced renal insufficiency The higher efficacy reported byCohen et al may be explained by overall less advanced kidneyfailure and proteinuria Together the studies demonstrate thatprevention of poor kidney function is necessary to treat effec-tively regardless of treatment regime
Recently the spectrum of MGRS has been reviewed in thecontext of monoclonal IgA deposits RTX did not elicit a RRwhile bortezomib-based treatment was suggested as first-linestrategy [33] Of 22 LCPT patients six MGRS patients weretreated with bortezomib-based regimes with 333 reaching atleast VGPR while the remainder had stable disease [27]Untreated patients progressed to ESRD while multivariateanalysis showed initial eGFR to be the only predictor of renalfunction This brings further support to prioritizing early detec-tion and subsequent chemotherapy to prevent deterioration ofkidney function In AL amyloidosis CyBorDBDex is stem cellspairing and therefore can be used in patients who may yetqualify for SCT as well as renal failure [95] In 53 patients withLCDD of which 57 were in Stage 45 CKD achieving at leasta VGPR improved renal outcome with bortezomib-based regi-mens achieving CR in eight out of nine cases [31] MIDD haspreviously been reported with poor outcomes and progressionto ESRD [24] Kourelis et al [73] studied 88 patients withMIDD (42 MGRS) of which 69 presented with eGFR
Clinical implication of monoclonal gammopathies 5Downloaded from httpsacademicoupcomndtadvance-article-abstractdoi101093ndtgfy2595086133by gueston 29 August 2018
lt30 mLmin1732 reporting proteasome inhibitorSCT as themost feasible therapeutic choice Achievement of completevery good partial HR was necessary for a RR while RR was anindependent predictor of progression again highlighting theprinciples of MGRS treatment In patients with PGNMID whodo not respond to initial treatment with RTXCYC and ste-roids bortezomib-based treatment may elicit a response [51]Bortezomib-based therapy was effective even in refractory casesof CG Type 1 related to MM [85 96 97]
Carfilzomib is a second-generation proteasome inhibitorDimopoulos et al [98] reported that carfilzomib-based therapyimproved renal outcome in 55 of patients with eGFRlt60 mLmin173 m2 Renal function may initially temporarilydecrease though therapy improves renal function A cardiacrisk profile should be treated with exceptional care Patient pro-file assessment and further studies will determine the use inMGRS
M O N O C L O N A L A N T I B O D I E S
Patients with MGUS treated with RTX and prednisone had im-proved kidney function and decreased proteinuria In patientswith MPGN secondary to indolent clones RTX CYC andprednisone were more effective then RTX with steroidsmono-therapy [99] Therapeutic doses of monoclonal antibodies maybe administered even in renal failure and post-renal allograftsettings [100 101] In seven patients with glomerulonephritiswith monoclonal IgG deposits RTX has been observed withpromising results [five achieved CR two partial response (PR)][102] The added benefit of RTX over classic chemotherapyrelates to a more tolerable profile Treatment of 14 PGNMIDpatients in approaches of clone-directed and empirical therapywithout identifiable discrasia was effective with patients withno detectable clone responding with complete and PSs in allbut two cases Bortezomib-based therapy may be effective innon-responders While empirical treatment is not easily under-taken with clonal detection at 25ndash32 it seems justified con-sidering the rate of response [22 51] However the studypopulation is not robust and the benefitsafety of such an ap-proach is in need of confirmation by larger studiesInterestingly patients with eGFR 20 had similar rates of CRPR to eGFR45 and all patients were free of ESRD in follow-up underscoring the value of a haematological treatment ap-proach in MGRS [51] RTXndashCYCndashDex use in 14 patients withMIg-associated glomerulopathy secondary to indolent non-Hodgkin lymphomas was reported on with 64 achieving CR(Table 1) The antiproteinuric effect of RTX is another benefi-cial aspect A steroid-free regimen of bendamustine and RTXprospectively assessed in indolent B-cell lymphoma of renalsignificance resulted in 85 achieving a haematological CRand 75 a complete RR [103] Patients without RR did notachieve HR Bendamustine is primarily cleared by hydrolysiswith minimal kidney involvement and recently there is sub-stantial evidence suggesting its safety in advanced renal failurethough complete blood counts should be monitored for haema-tological abnormality [104 105] (Table 1) RTX should be con-sidered in patients with IgM-associated MGRS especially when
Tab
le2
AL
base
dre
gim
ens
for
trea
tmen
tof
MG
RS
Dru
gP
atie
nts
and
met
hods
Out
com
esC
oncl
usio
nsR
efer
ence
VC
Dve
rsus
VD
101
pts
AL
amyl
oido
sis
(11
rena
lSta
ge3)
Sim
ilar
HR
(Pfrac14
026
)R
R43
fo
rV
Dve
rsus
41
for
VC
D(Pgt
005
)si
mila
rsu
rviv
al(Pfrac14
045
)H
ighe
rdo
sing
ofD
exan
dC
YC
addi
tion
does
noti
m-
pact
ther
apy
outc
omes
sign
ifica
ntly
Kas
trit
iset
al[
78]
CV
Dve
rsus
CT
D13
9pt
sw
ith
AL
amyl
oido
sis
Hig
her
CR
inC
VD
(40
6ve
rsus
246
)
med
ian
PFS
280
vers
us14
0m
onth
sre
spec
tive
lyFa
stcl
onal
cont
rold
idno
tred
uce
earl
ym
orta
lity
Ven
ner
etal
[79
]
CyB
orD
230
pts
wit
h63
w
ith
rena
linv
olve
men
t60
H
R4
3V
GP
R2
5R
RE
ffica
ciou
sin
pati
ents
wit
hout
card
iac
invo
lvem
ent
sur-
viva
lis
depe
nden
ton
deep
resp
onse
Pal
ladi
niet
al[
80]
DA
RA
Ret
rosp
ecti
vere
view
of25
cons
ecut
ive
AL
pts
HR
in76
C
Rin
36
VG
PR
24
wel
ltol
erat
edev
enin
card
iac
pts
Effi
caci
ous
inhe
avily
pre-
trea
ted
Kau
fman
etal
[81
]
Pom
alid
omid
endashD
ex28
pts
wit
hA
Lam
yloi
dosi
s68
H
Rgt
VG
PR
in29
5
3w
ith
resp
onse
afte
r1
cycl
eA
noth
erch
oice
inre
frac
tory
AL
impr
oves
surv
ival
hae
-m
atol
ogic
alpr
ogre
ssio
npr
edic
tssu
rviv
alP
alla
dini
etal
[82
]
LMD
50A
Lam
yloi
dosi
spt
s62
w
ith
rena
lloa
d(4
inre
nalS
tage
III)
CR
18
VG
PR
32
OR
in48
h
aem
atol
ogic
and
card
iac
toxi
city
4
mor
talit
y1
case
ofac
ute
kidn
eyin
jury
len
alid
omid
edo
seha
sto
bem
onit
ored
and
adju
sted
oth
erw
ise
tole
rabl
ean
def
ficac
ious
Heg
enba
rtet
al[
83]
M-D
ex25
9A
Lam
yloi
dosi
spt
sH
R76
C
R31
in
high
dose
ver
sus
51an
d12
in
atte
nuat
edO
Ron
lyin
pati
ents
wit
hH
R(h
ighe
rin
CR
vers
usV
GP
R)
Pal
ladi
niet
al[
84]
VG
PH
Rv
ery
good
part
ialh
aem
atol
ogic
alre
spon
seE
GC
Ge
piga
lloca
tech
inga
llate
LM
Dl
enal
idom
ide
mel
phal
ande
xam
etha
sone
VC
Db
orte
zom
ibcy
clop
hosp
ham
ide
dexa
met
haso
neM
-Dex
mel
phal
ande
xam
etha
sone
6 K Batko et alDownloaded from httpsacademicoupcomndtadvance-article-abstractdoi101093ndtgfy2595086133by gueston 29 August 2018
Tab
le3
Mon
oclo
nal
gam
mop
athy
inth
ese
ttin
gof
kidn
eytr
ansp
lan
tati
on
Pat
ient
san
dm
etho
dsO
utco
mes
Con
clus
ions
Ref
eren
ce
27LC
PT
pati
ents
trea
ted
wit
hch
emo-
ther
apy
(11
SCT
)9
wit
hno
trea
tmen
tLo
wes
tm
orta
lity
best
HR
sin
SCT
tho
ugh
pati
ents
wer
eyo
unge
ran
dha
dbe
stin
itia
land
final
rena
lfu
ncti
on
Bes
tren
alou
tcom
eco
mpa
red
wit
hch
emot
hera
pyor
notr
eatm
ent
SCT
stab
ilize
dor
impr
oved
rena
lfun
ctio
nSt
okes
etal
[27
]
64M
IDD
pati
ents
16
pts
trea
ted
wit
hSC
T4
Ktx
3re
curr
ence
sin
4K
txpa
tien
tsr
ange
of7ndash
43m
onth
s38
pr
ogre
ssio
nto
ESR
Din
SCT
Hig
hcr
eati
nine
atbi
opsy
isas
soci
ated
wit
hpo
orou
t-co
me
chem
othe
rapy
afte
rre
curr
ence
isin
effic
ient
Nas
ret
al[
24]
49M
IDD
pati
ents
3K
txw
ith
1V
GP
Ran
d2
CR
18
SCT
No
recu
rren
ces
in3
Ktx
pati
ents
allo
graf
trej
ecti
onin
1pa
tien
taft
er3
year
sSC
Tw
assa
fean
dto
lera
ted
but
pati
ents
wer
eyo
unge
rbo
rtez
omib
-bas
edtr
eatm
enth
adsi
mila
rR
Rra
tes
Sust
aine
d
VG
PR
nece
ssar
yfo
rK
txS
CT
ispr
efer
red
CK
Dst
ages
Coh
enet
al[
93]
29M
PG
NK
txpa
tien
ts6
wit
hm
onoc
lona
lpro
tein
(4M
GU
S1
CLL
)23
of
MP
GN
pati
ents
have
mon
oclo
nalp
rote
ins
may
incr
ease
risk
ofre
curr
ence
SC
Tre
solv
edre
curr
ence
pl
asm
aphe
res
aspa
ssiv
em
aint
enan
ce
MP
GN
pati
ents
shou
ldbe
scre
ened
for
mon
oclo
nal
prot
eins
Lore
nzet
al[
110]
6LC
DD
wit
hSC
T1
pati
entd
idno
tsur
vive
SCT
all
othe
rsac
hiev
edH
R
2re
laps
esw
ith
1im
prov
edby
subs
eque
ntch
emot
hera
py
Insu
ffici
ent
resp
onse
toSC
Tm
aybe
anin
dica
tion
for
Ktx
inse
lect
pati
ents
afte
rac
hiev
ing
HR
Lore
nzet
al[
122]
7LC
DD
Ktx
pati
ents
Med
ian
recu
rren
ce2ndash
45m
onth
sfo
r5
pati
ents
sub
se-
quen
t4de
aths
onl
y1
pati
entf
ree
ofre
new
alA
HR
mus
tbe
achi
eved
befo
reat
tem
ptin
gK
txLe
ung
etal
[10
9]
2P
GN
MID
Ktx
pati
ents
(1de
novo
1re
curr
ent)
Impr
ovem
ent
ingr
aftf
unct
ion
and
seru
mcr
eati
nine
in2
year
follo
w-u
pR
TX
can
beef
fect
ive
inbo
thre
curr
enta
ndde
novo
PG
NM
IDpt
sM
erhi
etal
[12
3]
3P
GN
MID
(2C
LL)
Des
pite
RT
Xtr
eatm
entt
here
was
1pr
ogre
ssio
nto
ESR
Dan
don
em
alig
nanc
ypr
ogre
ssio
nR
TX
ther
apy
may
impr
ove
rena
lout
com
esin
shor
tter
mB
arbo
uret
al[
124]
53LC
DD
7K
tx1
6SC
T2
recu
rren
ces
inpa
tien
tsw
itho
utpr
ior
chem
othe
rapy
1
reje
ctio
nof
Ktx
3pa
tien
tsin
CR
ingt
68
year
follo
w-
up1
SCT
-rel
ated
deat
h13
15
achi
eved
CR
SCT
can
besu
cces
sful
even
inC
KD
Stag
e4
how
ever
re
nals
urvi
vali
sst
illw
orse
SC
Tap
pear
sm
ore
safe
than
inA
Lam
yloi
dosi
s
Saye
det
al[
31]
21K
txw
itC
3GN
667
re
curr
ence
ofw
hich
21
asso
ciat
edw
ith
mon
o-cl
onal
gam
mop
athy
rec
urre
nce
earl
ier
(36
mon
thm
e-di
anve
rsus
433
mon
th)
mor
epr
ogre
ssiv
eco
urse
(Pfrac14
NS)
SC
Tim
prov
edki
dney
func
tion
inon
epa
tien
tst
a-bl
egr
aft
in10
-yea
rfo
llow
-up
Mon
oclo
nalg
amm
opat
hypa
tien
tsar
eat
risk
ofan
ear-
lier
and
mor
eag
gres
sive
dise
ase
Zan
det
al[
125]
548
Ktx
pati
ents
Pre
vale
nce
81
52
year
med
ian
toM
GU
Sdi
scov
ery
high
erra
teof
MB
Lhi
stor
yof
infla
mm
ator
yki
dney
dis-
ease
aspr
edic
tive
fact
orn
oas
soci
atio
nw
ith
age
and
gend
ern
oim
pact
ongr
afts
urvi
val
over
alls
urvi
val
in-
cide
nce
ofm
alig
nanc
y
MG
US
pre-
and
post
-tra
nspl
antm
aybe
diff
eren
tcon
di-
tion
sin
term
sof
man
agem
ent
how
ever
str
ict
follo
w-u
pis
need
ede
spec
ially
inM
BL
pati
ents
Alfa
noet
al[
126]
159
3K
txre
cipi
ents
3pr
e-tr
ansp
lant
MG
(nfrac14
34)
No
case
sof
prog
ress
ion
noas
soci
atio
nw
ith
mal
igna
ncy
inci
denc
eor
mor
talit
yJi
men
ezZ
eped
aet
al[
117]
587
Ktx
reci
pien
ts2
9in
cide
nce
(9pt
spr
e-tr
ansp
lant
8po
st)
No
prog
ress
ion
duri
ng6-
year
follo
w-u
pM
GU
Sno
taco
ntra
indi
cati
onto
Ktx
Ban
cuet
al[
127]
351
8K
txre
cipi
ents
42pa
tien
ts(2
3pr
e-tr
ansp
lant
19
post
)m
edia
nsu
rviv
al26
1ve
rsus
280
year
sre
spec
tive
ly4
haem
atol
ogic
alm
a-lig
nanc
ies
deve
lope
din
pre
2P
TLD
gt15
year
spo
st-
tran
spla
nt
Dia
gnos
isof
PT
LDw
assy
mpt
om-b
ased
tru
ein
cide
nce
may
behi
gher
exc
lusi
onof
asso
ciat
edki
dney
dise
ase
and
mal
igna
ncy
isne
cess
ary
befo
reK
tx
Nai
naet
al[
118]
MB
Lm
onoc
lona
lB-c
elll
ymph
ocyt
osis
Clinical implication of monoclonal gammopathies 7Downloaded from httpsacademicoupcomndtadvance-article-abstractdoi101093ndtgfy2595086133by gueston 29 August 2018
CD20thorn cells can be identified while non-IgM-associated dis-eases more often require MM-like treatment
Recently an anti CD38 monoclonal antibody daratumumab(DARA) has been approved for the treatment of newly diag-nosed and relapsed MM patients [106] Like many Phase 3 reg-istration trials the study excluded patients with CrCl 20 mLmin Anecdotal evidence of safety and reduction of dialysis fre-quency in a patient with DARA monotherapy has recently beenreported [107] A case of PGNMID refractory to RTX and
bortezomib was successfully treated with DARA [108] Due toindependence of kidney clearance and positive results in RI itmay prove beneficial in MGRS There is an on-going Phase 2study of DARA in MGRS [NCT03095118]
M G R S T R A N S P L A N T A N D E S R D
Renal transplant in MGRS is controversial as frequent recur-rences are observed when the abnormal clone is not adequately
FIGURE 1 Diagnostic and therapeutic algorithm of monoclonal gammopathy of renal significance
8 K Batko et alDownloaded from httpsacademicoupcomndtadvance-article-abstractdoi101093ndtgfy2595086133by gueston 29 August 2018
suppressed [24 109 110] The current treatment paradigm inMGRS is to achieve a complete HR as a means of improvingpost-transplant outcome and preventing recurrence [71 72111] Cibeira et al [112] report that in 340 AL amyloidosispatients subject to SCT 43 attained CR improving long-termOS and organ response (OR) In recent years the treatment-re-lated mortality (TRM) has decreased from 138 between 1994and 2003 to 56 between 2004 and 2008 In part this probablyreflects the experience of established centres however with ac-cess to novel agents there are other options for treatmentCardiac involvement should be screened for in LCDD due to ahigh TRM (23) with SCT as opposed to non-cardiac patients[32] PS does not indicate treatment failure and significantlyincreases survival compared with patients lacking response[113]
A study in AL amyloidosis patients associated the need fordialysis within 30 days of SCT with highest early death risk andTRM Patients with both eGFRlt40 mLmin173 m2 and se-rum albumin lt25 mgdL had a 438 and 281 risk of requir-ing dialysis and chance of TRM respectively Identifying andscreening for such risk factors should improve the feasibility ofSCT in MGRS conditions [114] In a study of 36 patients withAL amyloidosisMIDD who were dialysis dependent for ESRDCR was reached in 53 at 1 year post SCT with an 8 TRM[72] Achievement of dialysis independence was possible inpatients receiving a Ktx after successful SCT Similarly a studyin MM with RI found no impact on survival for patients whowere dialysis dependent [115] Further research is required toevaluate risk factors and establish whether select ESRD patientsmay benefit from SCT
Literature reports are conflicting on the approach to Ktx inMGUS [116ndash118] Bansal et al [119] reflect that a select groupof plasma dyscrasia patients should be considered for Ktx espe-cially those subject to dialysis-associated complications In ALand MIDD patients achieving haematological CR have beenreported with successful Ktx [120 121] Monoclonal gammop-athy in the setting of Ktxs is presented in Table 3 In summaryprimary disease activity organ function and patient perfor-mance should dictate selection for Ktx We propose an algo-rithm for diagnostic and therapeutic treatment of MGRS(Figure 1)
C O N C L U S I O N
With under-recognition of the wide spectrum of MGRS accu-rate classification evidence-based therapy and expert estab-lished management is required Renal involvement in MGRSresults from the direct deposition of monoclonal protein and itslight- or heavy-chain fragments in the kidney IFE microscopyis essential to identify the offending monoclonal protein and itsrenal tissue distribution In selected cases MS is of valueMGRS therapy is directed to eliminate the clonal plasma cell orB-cell population Adverse events particular to the chosen drugshould complement the patient profile Early detection diagno-sis and chemotherapy may improve kidney function It shouldbe stressed that both the renal pathology and the underlyinghaematological disorders influence the management and
prognosis of MGRS Upon achieving HR ASCT and Ktx shouldbe considered as therapy endpoints in MGRS
C O N F L I C T O F I N T E R E S T S T A T E M E N T
None declared
R E F E R E N C E S
1 Kyle RA Monoclonal gammopathy of undetermined significance NaturalHistory in 241 Cases Am J Med [Internet] 1978 [cited 2017 Oct 24] 64814ndash826 Available from httpwwwncbinlmnihgovpubmed645746
2 Leung N Bridoux F Hutchison CA et al Monoclonal gammopathy of re-nal significance when MGUS is no longer undetermined or insignificantBlood [Internet] 2012 [cited 2017 Oct 24] 120 4292ndash4295 Available fromhttpwwwncbinlmnihgovpubmed23047823
3 Kyle RA Therneau TM Rajkumar SV et al Prevalence of monoclonalgammopathy of undetermined significance N Engl J Med [Internet] 2006[cited 2017 Oct 24] 354 1362ndash1369 Available from httpwwwncbinlmnihgovpubmed16571879
4 Landgren O Graubard BI Kumar S et al Prevalence of myeloma precur-sor state monoclonal gammopathy of undetermined significance in 12372individuals 10ndash49 years old a population-based study from the NationalHealth and Nutrition Examination Survey Blood Cancer J 2017 7 e618[cited 2018 Feb 9] 7 Available from httpwwwncbinlmnihgovpubmed29053158
5 Landgren O Graubard BI Katzmann JA et al Racial disparities in theprevalence of monoclonal gammopathies a population-based study of12 482 persons from the National Health and Nutritional ExaminationSurvey Leukemia [Internet] 2014 28 1537ndash1542 [cited 2018 Jun 22]Available from httpwwwncbinlmnihgovpubmed24441287
6 Cabrera Q Macro M Hebert B et al Epidemiology of monoclonal gamm-opathy of undetermined significance (MGUS) the experience from thespecialized registry of hematologic malignancies of Basse-Normandie(France) Cancer Epidemiol [Internet] 2014 38 354ndash356 [cited 2017 Oct24] Available from httpwwwncbinlmnihgovpubmed24880205
7 Therneau TM Kyle RA Melton LJ et al Incidence of monoclonal gamm-opathy of undetermined significance and estimation of duration beforefirst clinical recognition Mayo Clin Proc [Internet] 2012 [cited 2017 Dec23] 87 1071ndash1079 Available from httpwwwncbinlmnihgovpubmed22883742
8 Kyle RA Larson DR Therneau TM et al Long-term follow-up of mono-clonal gammopathy of undetermined significance N Engl J Med 2018[cited 2018 Apr 23] 378 241ndash249 Available from httpwwwncbinlmnihgovpubmed29342381
9 Dispenzieri A Katzmann JA Kyle RA et al Prevalence and risk of progres-sion of light-chain monoclonal gammopathy of undetermined significancea retrospective population-based cohort study Lancet [Internet] 2010[cited 2018 Feb 9] 375 1721ndash1728 Available from httpwwwncbinlmnihgovpubmed20472173
10 Steiner N Gobel G Suchecki P et al Monoclonal gammopathy of renalsignificance (MGRS) increases the risk for progression to multiple mye-loma an observational study of 2935 MGUS patients Oncotarget[Internet] 2018 [cited 2018 Apr 27] 9 2344ndash2356 Available from httpwwwncbinlmnihgovpubmed29416776
11 Dhodapkar MV Sexton R Waheed S et al Clinical genomic andimaging predictors of myeloma progression from asymptomaticmonoclonal gammopathies (SWOG S0120) Blood [Internet] 2014[cited 2018 Jun 22] 123 78ndash85 Available from httpwwwncbinlmnihgovpubmed24144643
12 Zand L Kattah A Fervenza FC et al C3 glomerulonephritis associatedwith monoclonal gammopathy a case series Am J Kidney Dis [Internet]2013 [cited 2017 Dec 29] 62 506ndash514 Available from httpwwwncbinlmnihgovpubmed23623956
13 Rajkumar SV Dimopoulos MA Palumbo A et al International MyelomaWorking Group updated criteria for the diagnosis of multiple myelomaLancet Oncol [Internet] 2014 [cited 2018 Jun 23] 15 e538ndashe548 Availablefrom httplinkinghubelseviercomretrievepiiS1470204514704425
Clinical implication of monoclonal gammopathies 9Downloaded from httpsacademicoupcomndtadvance-article-abstractdoi101093ndtgfy2595086133by gueston 29 August 2018
14 Ravindran A Bartley AC Holton SJ et al Prevalence incidence and sur-vival of smoldering multiple myeloma in the United States Nat PublishingGroup [Internet] 2016 6 2018ndash2023 [cited Jun] Available from httpswwwncbinlmnihgovpmcarticlesPMC5098258pdfbcj2016100apdf
15 Fermand J-P Bridoux F Kyle RA et al How I treat monoclonal gammop-athy of renal significance (MGRS) Blood [Internet] 2013 [cited 2017 Oct27] 122 3583ndash3590 Available from httpwwwncbinlmnihgovpubmed24108460
16 Bridoux F Leung N Hutchison CA et al Diagnosis of monoclonal gamm-opathy of renal significance Kidney Int [Internet] 2015 [cited 2017 Oct24] 87 698ndash711 Available from httpwwwncbinlmnihgovpubmed25607108
17 Kristinsson SY Bjorkholm M Andersson TM-L et al Patterns of survivaland causes of death following a diagnosis of monoclonal gammopathy ofundetermined significance a population-based study Haematologica[Internet] 2009 [cited 2018 Feb] 94 1714ndash1720 Available from httpwwwncbinlmnihgovpubmed19608666
18 Dimopoulos MA Delimpasi S Katodritou E et al Significant improve-ment in the survival of patients with multiple myeloma presenting with se-vere renal impairment after the introduction of novel agents Ann Oncol[Internet] 2014 [cited 2018 Apr 23] 25 195ndash200 Available from httpsacademicoupcomannoncarticle-lookupdoi101093annoncmdt483
19 Correia SO Santos S Malheiro J et al Monoclonal gammopathy of renalsignificance diagnostic workup WJN 2017 [cited 2017 Oct 27] 6 72ndash78Available from httpwwwncbinlmnihgovpubmed28316940
20 Lin J Markowitz GS Valeri AM et al Renal monoclonal immunoglobulindeposition disease the disease spectrum J Am Soc Nephrol [Internet] 2001[cited 2018 Jun 23] 12 1482ndash1492 Available from httpwwwncbinlmnihgovpubmed11423577
21 Sethi S Zand L Leung N et al Membranoproliferative glomerulonephritissecondary to monoclonal gammopathy Clin J Am Soc Nephrol [Internet]2010 [cited 2017 Dec 8] 5 770ndash782 Available from httpwwwncbinlmnihgovpubmed20185597
22 Bhutani G Nasr SH Said SM et al Hematologic characteristics of prolifer-ative glomerulonephritides with nonorganized monoclonal immunoglobu-lin deposits Mayo Clin Proc [Internet] 2015 [cited 2018 Jun 23] 90587ndash596 Available from httpwwwncbinlmnihgovpubmed25939936
23 Cohen C El-Karoui K Alyanakian M-A et al Light and heavy chain depo-sition disease associated with CH1 deletion Clin Kidney J [Internet] 2015[cited 2017 Oct 26] 8 237ndash239 Available from httpwwwncbinlmnihgovpubmed25815184
24 Nasr SH Valeri AM Cornell LD et al Renal monoclonal immunoglobulindeposition disease a report of 64 patients from a single institution Clin JAm Soc Nephrol [Internet] 2012 [cited 2018 Feb 9] 7 231ndash239 Availablefrom httpwwwncbinlmnihgovpubmed22156754
25 Sicard A Karras A Goujon J-M et al Light chain deposition disease with-out glomerular proteinuria a diagnostic challenge for the nephrologistNephrol Dial Transplant [Internet] 2014 [cited 2018 Jul 7] 29 1894ndash1902Available from httpwwwncbinlmnihgovpubmed24619059
26 Haas M A reevaluation of routine electron microscopy in the examinationof native renal biopsies J Am Soc Nephrol [Internet] 1997 8 70ndash76Available from httpwwwncbinlmnihgovpubmed9013450
27 Stokes MB Valeri AM Herlitz L et al Light chain proximal tubulopathyclinical and pathologic characteristics in the modern treatment era J AmSoc Nephrol [Internet] 2016 [cited 2018 Jun 23] 27 1555ndash1565 Availablefrom httpwwwncbinlmnihgovpubmed26374607
28 Larsen CP Messias NC Walker PD et al Membranoproliferative glomeru-lonephritis with masked monotypic immunoglobulin deposits Kidney Int[Internet] 2015 [cited 2018 Feb 10] 88 867ndash873 Available from httpwwwncbinlmnihgovpubmed26154922
29 Eirin A Irazabal MV Gertz MA et al Clinical features of patients with im-munoglobulin light chain amyloidosis (AL) with vascular-limited deposi-tion in the kidney Nephrol Dial Transplant [Internet] 2012 [cited 2018Feb 10] 27 1097ndash1101 Available from httpwwwncbinlmnihgovpubmed22067518
30 Alonso-Titos J Perea-Ortega L Sola E et al C3 glomerulonephritis associ-ated with monoclonal gammopathy of renal significance case report BMCNephrol 2018 Jul 6] 19 129 Available from httpwwwncbinlmnihgovpubmed29884135
31 Sayed RH Wechalekar AD Gilbertson JA et al Natural history and out-come of light chain deposition disease Blood [Internet] 2015 [cited 2017Dec 8] 126 2805ndash2810 Available from httpwwwncbinlmnihgovpubmed26392598
32 Mohan M Buros A Mathur P et al Clinical characteristics and prognosticfactors in multiple myeloma patients with light chain deposition diseaseAm J Hematol 2017 [cited 2018 Jul 7] 92 739ndash745 Available from httpwwwncbinlmnihgovpubmed28383130
33 Vignon M Cohen C Faguer S et al The clinicopathologic characteristicsof kidney diseases related to monotypic IgA deposits Kidney Int [Internet]2017 [cited 2018 Jul] 91 720ndash728 Available from httpwwwncbinlmnihgovpubmed28069266
34 Best Rocha A Larsen CP Membranous glomerulopathy with light chain-restricted deposits a clinicopathological analysis of 28 cases Kidney IntRep [Internet] 2017 [cited 2018 Jul 6] 2 1141ndash1148 Available from httpwwwncbinlmnihgovpubmed29270522
35 Nasr SH Valeri AM Sethi S et al Clinicopathologic correlations in multi-ple myeloma a case series of 190 patients with kidney biopsies Am JKidney Dis [Internet] 2012 [cited 2017 Oct 26] 59 786ndash794 Availablefrom httpwwwncbinlmnihgovpubmed22417785
36 Glavey SV Leung N Monoclonal gammopathy the good the bad and theugly Blood Rev [Internet] 2016 [cited 2017 Dec 24] 30 223ndash231 Availablefrom httpwwwsciencedirectcomsciencearticlepiiS0268960X15000946bb0130
37 Katzmann JA Kyle RA Benson J et al Screening panels for detection ofmonoclonal gammopathies Clin Chem [Internet] 2009 [cited 2017 Oct25] 55 1517ndash1522 Available from httpwwwncbinlmnihgovpubmed19520758
38 Yadav P Leung N Sanders PW et al The use of immunoglobulin lightchain assays in the diagnosis of paraprotein-related kidney disease KidneyInt [Internet] 2015 [cited 2018 Feb 9] 87 692ndash697 Available from httpwwwncbinlmnihgovpubmed25296094
39 Sugihara H Chihara D Seike K et al Percentage of urinary albumin excre-tion and serum-free light-chain reduction are important determinants ofrenal response in myeloma patients with moderate to severe renal impair-ment Blood Cancer J [Internet] 2014 [cited 2018 Jun 24] 4 e235 Availablefrom httpwwwncbinlmnihgovpubmed25083819
40 Leung N Gertz M Kyle RA et al Urinary albumin excretion patterns ofpatients with cast nephropathy and other monoclonal gammopathy-related kidney diseases Clin J Am Soc Nephrol [Internet] 2012 [cited 2018Jun 24] 7 1964ndash1968 Available from httpwwwncbinlmnihgovpubmed23024162
41 Ciocchini M Arbelbide J Musso CG Monoclonal gammopathy of renalsignificance (MGRS) the characteristics and significance of a new meta-entity Int Urol Nephrol [Internet] 2017 [cited 2017 Oct 26] 492171ndash2175 Available from httpwwwncbinlmnihgovpubmed28425076
42 Sethi S Rajkumar SV DrsquoAgati VD The complexity and heterogeneity ofmonoclonal immunoglobulinndashassociated renal diseases J Am Soc Nephrol2018 29 1810ndash1823
43 Hutchison CA Harding S Hewins P et al Quantitative assessment of se-rum and urinary polyclonal free light chains in patients with chronic kid-ney disease Clin J Am Soc Nephrol [Internet] 2008 [cited 2017 Dec 25] 31684ndash1690 Available from httpwwwncbinlmnihgovpubmed18945993
44 Jurczyszyn A Ochrem B Abnormal serum free light chain ratio does notalways indicate monoclonal gammopathy Polskie Archiwum MedycynyWewnetrznej [Internet] 2015 [cited 2017 Dec 29] 125 502ndash504 Availablefrom httpwwwncbinlmnihgovpubmed26266682
45 Singh G Serum free light chain assay and jk ratio performance inpatients with monoclonal gammopathy-high false negative rate for jk ra-tio J Clin Med Res 2017 [cited 2018 Jun 25] 9 46ndash57 Available fromhttpwwwncbinlmnihgovpubmed27924175
46 Fulton RB Fernando SL Serum free light chain assay reduces the need forserum and urine immunofixation electrophoresis in the evaluation ofmonoclonal gammopathy Ann Clin Biochem [Internet] 2009 [cited 2018Jun 25] 46 407ndash412 Available from httpwwwncbinlmnihgovpubmed19641008
10 K Batko et alDownloaded from httpsacademicoupcomndtadvance-article-abstractdoi101093ndtgfy2595086133by gueston 29 August 2018
47 Levinson SS Urine immunofixation electrophoresis remains importantand is complementary to serum free light chain Clin Chem Lab Med[Internet] 2011 [cited 2018 Jun 25] 49 1801ndash1804 Available from httpwwwncbinlmnihgovpubmed21663562 [CrossRef][Mismatch]
48 Lee WS Singh G Serum free light chains in neoplastic monoclonal gam-mopathies relative under-detection of lambda dominant KappaLambdaratio and underproduction of free lambda light chains as compared tokappa light chains in patients with neoplastic monoclonal gammopathiesJ Clin Med Res 2018 [cited 2018 Jun 25] 10 562ndash569 Available fromhttpwwwncbinlmnihgovpubmed29904440
49 Xu B Tang Y Zhou J et al Disease spectrum of abnormal serum free lightchain ratio and its diagnostic significance Oncotarget [Internet] 2017[cited 2017 Dec 29] 8 82268ndash82279 Available from httpwwwncbinlmnihgovpubmed29137262
50 Koo EH Shin J Jang HR et al Diagnostic performances of M-protein testsaccording to the clinical presentations of kidney disease Eur J Intern Med[Internet] 2016 [cited 2018 Feb 9] 33 88ndash92 Available from httpwwwncbinlmnihgovpubmed27421913
51 Gumber R Cohen JB Palmer MB et al A clone-directed approach mayimprove diagnosis and treatment of proliferative glomerulonephritis withmonoclonal immunoglobulin deposits Kidney Int [Internet] 2018 94199ndash205 Available from httpsdoiorg101016jkint201802020
52 Leung N Barnidge DR Hutchison CA Laboratory testing in monoclonalgammopathy of renal significance (MGRS) Clin Chem Lab Med [Internet]2016 [cited 2017 Oct 25] 54 929ndash937 Available from httpwwwncbinlmnihgovpubmed27107835 [CrossRef][Mismatch]
53 Ramirez-Alvarado M Ward CJ Huang BQ et al Differences in immuno-globulin light chain species found in urinary exosomes in light chain amy-loidosis (AL) PLoS ONE [Internet] 2012 [cited 2018 Jul 7] 7 e38061Available from httpwwwncbinlmnihgovpubmed22723846
54 Hogan JJ Weiss BM Bridging the divide an onco-nephrologic approachto the monoclonal gammopathies of renal significance Clin J Am SocNephrol [Internet] 2016 [cited 2017 Oct 26] 11 1681ndash1691 Availablefrom httpwwwncbinlmnihgovpubmed27416775
55 Vij R Mazumder A Klinger M et al Deep sequencing reveals myelomacells in peripheral blood in majority of multiple myeloma patients ClinLymphoma Myeloma Leuk [Internet] 2014 [cited 2017 Oct 25] 14131ndash139e1 Available from httpwwwncbinlmnihgovpubmed24629890
56 Gonsalves WI Leung N Rajkumar SV et al Improvement in renal func-tion and its impact on survival in patients with newly diagnosed multiplemyeloma Blood Cancer J 2015 [cited 2018 Feb 3] 5 e296 Available fromhttpwwwnaturecomdoifinder101038bcj201520
57 Dimopoulos MA Cheung MC Roussel M et al Impact of renal impair-ment on outcomes with lenalidomide and dexamethasone treatment in theFIRST trial a randomized open-label phase 3 trial in transplant-ineligiblepatients with multiple myeloma Haematologica [Internet] 2016 [cited2018 Jul 7] 101 363ndash370 Available from httpwwwncbinlmnihgovpubmed26659916
58 Ponisch W Andrea M Wagner I et al Successful treatment of patientswith newly diagnoseduntreated multiple myeloma and advanced renalfailure using bortezomib in combination with bendamustine and predni-sone J Cancer Res Clin Oncol 2012 [cited 2018 Jul 2] 138 1405ndash1412Available from httpwwwncbinlmnihgovpubmed22526157
59 Perry M Delarche A Ribes D et al Rituximab-cyclophosphamide-dexa-methasone is highly effective in patients with monoclonal Ig deposit-related glomerulopathy and indolent non-Hodgkin lymphomas Am JHematol 2014 [cited 2018 Jul 1] 89 969ndash973 Available from httpdoiwileycom101002ajh23798
60 Dimopoulos M Weisel K van de Donk Nwcj et al Pomalidomide pluslow-dose dexamethasone in patients with relapsedrefractory multiple my-eloma and renal impairment results from a Phase II trial J Clin Oncol2018 36 2035ndash2043
61 Fervenza FC Canetta PA Barbour SJ et al A multicenter randomized con-trolled trial of rituximab versus cyclosporine in the treatment of idiopathicmembranous nephropathy (MENTOR) Nephron [Internet] 2015 [cited2017 Dec 25] 130 159ndash168 Available from httpwwwncbinlmnihgovpubmed26087670
62 Dimopoulos MA Richardson PG Schlag R et al VMP (bortezomib mel-phalan and prednisone) is active and well tolerated in newly diagnosedpatients with multiple myeloma with moderately impaired renal functionand results in reversal of renal impairment cohort analysis of the Phase IIIVISTA study JCO 2009 [cited 2017 Dec 8] 27 6086ndash6093 Available fromhttpwwwncbinlmnihgovpubmed19858394
63 Morabito F Gentile M Mazzone C et al Safety and efficacy ofbortezomib-melphalan-prednisone-thalidomide followed by bortezomib-thalidomide maintenance (VMPT-VT) versus bortezomib-melphalan-prednisone (VMP) in untreated multiple myeloma patients with renal im-pairment Blood [Internet] 2011 [cited 2017 Dec 9] 118 5759ndash5766Available from httpwwwncbinlmnihgovpubmed21951682
64 Moreau P Masszi T Grzasko N et al Oral ixazomib lenalidomide anddexamethasone for multiple myeloma N Engl J Med 2016 [cited 2018 Apr27] 374 1621ndash1634 Available from httpwwwnejmorgdoi101056NEJMoa1516282
65 Nordstrom BL Knopf KB Teltsch DY et al The safety of bendamustine inpatients with chronic lymphocytic leukemia or non-Hodgkin lymphomaand concomitant renal impairment a retrospective electronic medical re-cord database analysis Leuk Lymphoma [Internet] 2014 [cited 2017 Dec13] 55 1266ndash1273 Available from httpwwwncbinlmnihgovpubmed23987821
66 Roussou M Kastritis E Christoulas D et al Reversibility of renal failure innewly diagnosed patients with multiple myeloma and the role of novelagents Leuk Res [Internet] 2010 [cited 2017 Dec 15] 34 1395ndash1397Available from httpwwwncbinlmnihgovpubmed20510452
67 Tosi P Zamagni E Tacchetti P et al Thalidomide-dexamethasone as in-duction therapy before autologous stem cell transplantation in patientswith newly diagnosed multiple myeloma and renal insufficiency BiolBlood Marrow Transplant [Internet] 2010 [cited 2018 Apr 27] 161115ndash1121 Available from httpwwwncbinlmnihgovpubmed20197100
68 Dimopoulos M Alegre A Stadtmauer EA et al The efficacy and safety oflenalidomide plus dexamethasone in relapsed andor refractory multiplemyeloma patients with impaired renal function Cancer [Internet] 2010116 3807 [cited 2017 Dec 15] Available from httpwwwncbinlmnihgovpubmed20564094
69 Siegel DS Weisel KC Dimopoulos MA et al Pomalidomide plus low-dosedexamethasone in patients with relapsedrefractory multiple myeloma andmoderate renal impairment a pooled analysis of three clinical trials LeukLymphoma [Internet] 2016 [cited 2017 Dec 15] 57 2833ndash2838 Availablefrom httpwwwncbinlmnihgovpubmed27267105
70 Dimopoulos MA Goldschmidt H Niesvizky R et al Carfilzomib or borte-zomib in relapsed or refractory multiple myeloma (ENDEAVOR) an in-terim overall survival analysis of an open-label randomised phase 3 trialLancet Oncol [Internet] 2017 [cited 2017 Dec 6] 18 1327ndash1337 Availablefrom httpwwwncbinlmnihgovpubmed28843768
71 Telio D Shepherd J Forrest D et al High-dose melphalan followed byauto-SCT has favorable safety and efficacy in selected patients with lightchain deposition disease and light and heavy chain deposition diseaseBone Marrow Transplant 2012 [cited 2017 Dec 8] 47 453ndash455 Availablefrom httpwwwnaturecomdoifinder101038bmt201187
72 Batalini F Econimo L Quillen K et al High-dose melphalan and stem celltransplantation in patients on dialysis due to immunoglobulin light-chainamyloidosis and monoclonal immunoglobulin deposition disease BiolBlood Marrow Transplant [Internet] 2018 [cited 2017 Dec 25] 24127ndash132 Available from httpwwwncbinlmnihgovpubmed28865972
73 Kourelis TV Nasr SH Dispenzieri A et al Outcomes of patients with renalmonoclonal immunoglobulin deposition disease Am J Hematol 2016[cited 2018 Jul 2] 91 1123ndash1128 Available from httpwwwncbinlmnihgovpubmed27501122
74 Pozzi C DrsquoAmico M Fogazzi GB et al Light chain deposition disease withrenal involvement clinical characteristics and prognostic factors Am JKidney Dis [Internet] 2003 [cited 2018 Jun 23] 42 1154ndash1163 Availablefrom httpwwwncbinlmnihgovpubmed14655186
75 Song M-K Chung J-S Shin H-J et al Cyclophosphamide-containing regi-men (TCD) is superior to melphalan-containing regimen (MPT) in elderlymultiple myeloma patients with renal impairment Ann Hematol
Clinical implication of monoclonal gammopathies 11Downloaded from httpsacademicoupcomndtadvance-article-abstractdoi101093ndtgfy2595086133by gueston 29 August 2018
[Internet] 2012 [cited 2017 Dec 9] 91 889ndash896 Available from httpwwwncbinlmnihgovpubmed22237937
76 Specter R Sanchorawala V Seldin DC et al Kidney dysfunction duringlenalidomide treatment for AL amyloidosis Nephrol Dial Transplant[Internet] 2011 [cited 2018 Jul 7] 26 881ndash886 Available from httpwwwncbinlmnihgovpubmed20693160
77 Li Y Wang X OrsquoMara E et al Population pharmacokinetics of pomalido-mide in patients with relapsed or refractory multiple myeloma with variousdegrees of impaired renal function CPAA 2017 [cited 2018 Feb 4] 9133ndash145 Available from httpwwwncbinlmnihgovpubmed29184451
78 Kastritis E Gavriatopoulou M Roussou M et al Addition of cyclophos-phamide and higher doses of dexamethasone do not improve outcomes ofpatients with AL amyloidosis treated with bortezomib Blood Cancer J2017 [cited 2017 Dec 15] 7 e570 Available from httpwwwncbinlmnihgovpubmed28622303
79 Venner CP Gillmore JD Sachchithanantham S et al A matched compari-son of cyclophosphamide bortezomib and dexamethasone (CVD) versusrisk-adapted cyclophosphamide thalidomide and dexamethasone (CTD)in AL amyloidosis Leukemia [Internet] 2014 [cited 2018 Jul 5] 282304ndash2310 Available from httpwwwncbinlmnihgovpubmed25027514
80 Palladini G Sachchithanantham S Milani P et al A European collabora-tive study of cyclophosphamide bortezomib and dexamethasone inupfront treatment of systemic AL amyloidosis Blood [Internet] 2015[cited 2017 Dec 9] 126 612ndash615 Available from httpwwwncbinlmnihgovpubmed25987656
81 Kopel T Kaufman JS Hamburg N et al Endothelium-dependent and -in-dependent vascular function in advanced chronic kidney disease CJASN2017 [cited 2018 Apr 18] 12 1588ndash1594 Available from httpcjasnasnjournalsorglookupdoi102215CJN12811216
82 Palladini G Milani P Foli A et al A Phase 2 trial of pomalidomide anddexamethasone rescue treatment in patients with AL amyloidosis Blood[Internet] 2017 [cited 2018 Apr 26] 129 2120ndash2123 Available fromhttpwwwncbinlmnihgovpubmed28130212
83 Hegenbart U Bochtler T Benner A et al Lenalidomidemelphalandexa-methasone in newly diagnosed patients with immunoglobulin light chainamyloidosis results of a prospective phase 2 study with long-term followup Haematologica [Internet] 2017 [cited 2017 Dec 26] 102 1424ndash1431Available from httpwwwncbinlmnihgovpubmed28522573
84 Palladini G Milani P Foli A et al Oral melphalan and dexamethasonegrants extended survival with minimal toxicity in AL amyloidosis long-term results of a risk-adapted approach Haematologica [Internet] 2014[cited 2017 Dec 15] 99 743ndash750 Available from httpwwwncbinlmnihgovpubmed24213149
85 Payet J Livartowski J Kavian N et al Type I cryoglobulinemia in multiplemyeloma a rare entity analysis of clinical and biological characteristics ofseven cases and review of the literature Leuk Lymphoma [Internet] 201354 767ndash777 Available from httpwwwtandfonlinecomdoifull103109104281942012671481
86 Terpos E Kleber M Engelhardt M et al European Myeloma Networkguidelines for the management of multiple myeloma-related complica-tions Haematologica [Internet] 2015 [cited 2017 Dec 4] 100 1254ndash1266Available from httpwwwncbinlmnihgovpubmed26432383
87 Chanan-Khan AA Kaufman JL Mehta J et al Activity and safety of borte-zomib in multiple myeloma patients with advanced renal failure a multi-center retrospective study Blood [Internet] 2007 [cited 2018 Jul 2] 1092604ndash2606 Available from httpwwwncbinlmnihgovpubmed17138816
88 Dimopoulos MA Roussou M Gkotzamanidou M et al The role of novelagents on the reversibility of renal impairment in newly diagnosed symp-tomatic patients with multiple myeloma Leukemia 2013 27 423ndash429
89 Kouroukis TC Baldassarre FG Haynes AE et al Bortezomib in multiplemyeloma systematic review and clinical considerations Curr Oncol(Toronto Ont) [Internet] 2014 [cited 2017 Dec 4] 21 e573ndashe603Available from httpwwwncbinlmnihgovpubmed25089109
90 Zhu W Chen W Bortezomib-based treatment for multiple myelomapatients with renal impairment a systematic review and meta-analysis ofobservational studies Medicine [Internet] 2016 95 e5202 Available fromhttpwwwncbinlmnihgovpmcarticlesPMC5120900
91 Dimopoulos MA Terpos E Chanan-Khan A et al Renal impairment inpatients with multiple myeloma a consensus statement on behalf of theInternational Myeloma Working Group JCO 2010 28 4976ndash4984
92 Chauvet S Fremeaux-Bacchi V Petitprez F et al Treatment of B-cell disor-der improves renal outcome of patients with monoclonal gammopathyndashassociated C3 glomerulopathy Blood [Internet] 2017 [cited 2017 Oct 26]129 1437ndash1447 Available from httpwwwncbinlmnihgovpubmed28069603
93 Cohen C Royer B Javaugue V et al Bortezomib produces high hematolog-ical response rates with prolonged renal survival in monoclonal immuno-globulin deposition disease Kidney Int [Internet] 2015 [cited 2017 Dec25] 88 1135ndash1143 Available from httpwwwncbinlmnihgovpubmed26176826
94 Ziogas DC Kastritis E Terpos E et al Hematologic and renal improve-ment of monoclonal immunoglobulin deposition disease after treatmentwith bortezomib-based regimens Leuk Lymphoma [Internet] 2017 [cited2017 Dec 25] 58 1832ndash1839 Available from httpwwwncbinlmnihgovpubmed27967286
95 Milani P Merlini G Palladini G Novel therapies in light chain amyloid-osis Kidney Int Rep [Internet] 2018 [cited 2018 Jul 4] 3 530ndash541 Availablefrom httpwwwncbinlmnihgovpubmed29854961
96 Spizzo G Mitterer M Gunsilius E Bortezomib for the treatment of refrac-tory Type-1 cryoglobulinaemia Br J Haematol [Internet] 2010 [cited 2018Jul 7] 150 235ndash237 Available from httpdoiwileycom101111j1365-2141201008184x
97 Talamo G Claxton D Tricot G et al Response to bortezomib in refractoryType I cryoglobulinemia Am J Hematol 2008 [cited 2018 Jul 7] 83883ndash884 Available from httpwwwncbinlmnihgovpubmed18756542
98 Dimopoulos MA Roussou M Gavriatopoulou M et al Cardiac and renalcomplications of carfilzomib in patients with multiple myeloma BloodAdv 2017 [cited 2017 Dec 6] 1 449ndash454 Available from httpwwwbloodadvancesorglookupdoi101182bloodadvances2016003269
99 Strati P Nasr SH Leung N et al Renal complications in chronic lympho-cytic leukemia and monoclonal B-cell lymphocytosis the Mayo Clinic ex-perience Haematologica [Internet] 2015 [cited 2018 Jul 3] 100 1180ndash1188Available from httpwwwncbinlmnihgovpubmed26088927
100 Salama AD Pusey CD Drug insight rituximab in renal disease and trans-plantation Nat Clin Pract Nephrol [Internet] 2006 [cited 2017 Dec 8] 2221ndash230 Available from httpwwwnaturecomdoifinder101038ncpneph0133
101 Jillella AP Dainer PM Kallab AM et al Treatment of a patient with end-stage renal disease with rituximab pharmacokinetic evaluation suggestsrituximab is not eliminated by hemodialysis Am J Hematol 2002 [cited2018 Jul] 71 219ndash222 Available from httpwwwncbinlmnihgovpubmed12410580
102 Guiard E Karras A Plaisier E et al Patterns of noncryoglobulinemic glo-merulonephritis with monoclonal Ig deposits correlation with IgG sub-class and response to rituximab Clin J Am Soc Nephrol 2011 6 1609ndash1616
103 Ribes D Hachem HEL Oberic L et al Bendamustine plus rituximab forindolent B-cell lymphoma of renal significance Am J Hematol 2018 93356ndash362
104 Darwish M Bond M Hellriegel E et al Pharmacokinetic and pharmacody-namic profile of bendamustine and its metabolites Cancer ChemotherPharmacol 2015 [cited 2017 Dec 15] 75 1143ndash1154 Available from httpwwwncbinlmnihgovpubmed25829094
105 Ponisch W Moll B Bourgeois M et al Bendamustine and prednisone incombination with bortezomib (BPV) in the treatment of patients with re-lapsed or refractory multiple myeloma and light chain-induced renal fail-ure J Cancer Res Clin Oncol [Internet] 2013 [cited 2018 Jul 2] 1391937ndash1946 Available from httpwwwncbinlmnihgovpubmed24046251
106 Mateos M-V Dimopoulos MA Cavo M et al Daratumumab plus bortezo-mib melphalan and prednisone for untreated myeloma N Engl J Med2018 378 518ndash528
107 Rocchi S Tacchetti P Pantani L et al Safety and efficacy of daratumumabin dialysis-dependent renal failure secondary to multiple myelomaHaematologica [Internet] 2018 [cited 2018 Jul 2] 103 e277ndashe278 Availablefrom httpwwwncbinlmnihgovpubmed29622654
12 K Batko et alDownloaded from httpsacademicoupcomndtadvance-article-abstractdoi101093ndtgfy2595086133by gueston 29 August 2018
108 Anand S Miller D Chipman G Morris D Srinivas S Daratumumab forsevere refractory proliferative glomerulonephritis with monoclonal im-mune deposits (PGNMID) ATC Abstr [Internet] 2017 [cited 2018 Jul 3]Available from httpsatcmeetingabstractscomabstractdaratumumab-for-severe-refractory-proliferative-glomerulonephritis-with-monoclonal-immune-deposits-pgnmid
109 Leung N Lager DJ Gertz MA et al Long-term outcome of renal transplan-tation in light-chain deposition disease Am J Kidney Dis [Internet] 2004[cited 2018 Feb 9] 43 147ndash153 Available from httpwwwncbinlmnihgovpubmed14712438
110 Lorenz EC Sethi S Leung N et al Recurrent membranoproliferative glo-merulonephritis after kidney transplantation Kidney Int [Internet] 2010[cited 2018 Feb 9] 77 721ndash728 Available from httpwwwncbinlmnihgovpubmed20130531
111 Leung N Nasr SH A patient with abnormal kidney function and a mono-clonal light chain in the urine Clin J Am Soc Nephrol 2016 11 1073ndash1082
112 Cibeira MT Sanchorawala V Seldin DC et al Outcome of AL amyloidosisafter high-dose melphalan and autologous stem cell transplantation long-term results in a series of 421 patients Blood [Internet] 2011 [cited 2018Feb 3] 118 4346ndash4352 Available from httpwwwncbinlmnihgovpubmed21828140
113 Gertz MA Lacy MQ Dispenzieri A et al Autologous stem cell transplantfor immunoglobulin light chain amyloidosis a status report LeukLymphoma [Internet] 2010 [cited 2018 Feb 3] 51 2181ndash2187 Availablefrom httpwwwncbinlmnihgovpubmed20958232
114 Leung N Kumar SK Glavey SV et al The impact of dialysis on the survivalof patients with immunoglobulin light chain (AL) amyloidosis undergoingautologous stem cell transplantation Nephrol Dial Transplant 2016 [cited2018 Jul 7] 31 1284ndash1289 Available from httpsacademicoupcomndtarticle-lookupdoi101093ndtgfv328
115 Badros A Barlogie B Siegel E et al Results of autologous stem cell trans-plant in multiple myeloma patients with renal failure Br J Haematol 2001[cited 2018 Jul 7] 114 822ndash829 Available from httpwwwncbinlmnihgovpubmed11564069
116 Soltero L Carbajal H Xu J et al Initial survival data of kidney transplantpatients with pre-transplant monoclonal gammopathy Clin Transplant[Internet] 2012 [cited 2018 Feb 3] 26 300ndash304 Available from httpwwwncbinlmnihgovpubmed22044717
117 Jimenez-Zepeda VH Heilman RL Engel RA et al Monoclonal gammopathyof undetermined significance does not affect outcomes in patients undergoingsolid organ transplants Transplantation [Internet] 2011 [cited 2018 Feb 3]92 570ndash574 Available from httpwwwncbinlmnihgovpubmed21712755
118 Naina HVK Harris S Dispenzieri A et al Long-term follow-up of patientswith monoclonal gammopathy of undetermined significance after kidney
transplantation Am J Nephrol 2012 [cited 2018 Feb] 35 365ndash371Available from httpwwwncbinlmnihgovpubmed22473253
119 Bansal T Garg A Snowden JA et al Defining the role of renal transplanta-tion in the modern management of multiple myeloma and other plasmacell dyscrasias Nephron Clin Pract [Internet] 2012 [cited 2018 Feb 3] 120c228 wwwkargercom
120 Hassoun H Flombaum C DrsquoAgati VD et al High-dose melphalan andauto-SCT in patients with monoclonal Ig deposition disease Bone MarrowTransplant 2008 [cited 2018 Feb 3] 42 405ndash412 Available from httpwwwncbinlmnihgovpubmed18574442
121 Herrmann SMS Gertz MA Stegall MD et al Long-term outcomes ofpatients with light chain amyloidosis (AL) after renal transplantation withor without stem cell transplantation Nephrol Dial Transplant [Internet]2011 [cited 2018 Feb 3] 26 2032ndash2036 Available from httpwwwncbinlmnihgovpubmed21543655
122 Lorenz EC Gertz MA Fervenza FC et al Long-term outcome of autolo-gous stem cell transplantation in light chain deposition disease NephrolDial Transplant [Internet] 2008 [cited 2018 Jul 5] 23 2052ndash2057 Availablefrom httpwwwncbinlmnihgovpubmed18178602
123 Merhi B Patel N Bayliss G et al Proliferative glomerulonephritis withmonoclonal IgG deposits in two kidney allografts successfully treated withrituximab Clin Kidney J [Internet] 2017 [cited 2018 Feb 10] 10 405ndash410Available from httpsacademicoupcomckjarticle-lookupdoi101093ckjsfx001
124 Barbour SJ Beaulieu MC Zalunardo NY et al Proliferative glomerulone-phritis with monoclonal IgG deposits secondary to chronic lymphocyticleukemia Report of two cases Nephrol Dial Transplant [Internet] 2011[cited 2018 Feb 10] 26 2712ndash2714 Available from httpsacademicoupcomndtarticle-lookupdoi101093ndtgfr251
125 Zand L Lorenz EC Cosio FG et al Clinical findings pathology and out-comes of C3GN after kidney transplantation J Am Soc Nephrol [Internet]2014 [cited 2018 Jul 5] 25 1110ndash1117 Available from httpwwwncbinlmnihgovpubmed24357668
126 Alfano G Fontana F Colaci E et al Monoclonal gammopathy of undeter-mined significance after kidney transplantation Transplantation [Internet]2017 [cited 2017 Oct 24] 101 e337ndashe342 Available from httpwwwncbinlmnihgovpubmed28731904
127 Bancu I Ca~nas L Juega FJ et al Outcomes of monoclonal gammopathyof undetermined significance in patients who underwent kidneytransplantation Transplant Proc [Internet] 2015 [cited 2018 Feb 10] 472344ndash2345 Available from httpwwwncbinlmnihgovpubmed26518922
Received 2632018 Editorial decision 1472018
Clinical implication of monoclonal gammopathies 13Downloaded from httpsacademicoupcomndtadvance-article-abstractdoi101093ndtgfy2595086133by gueston 29 August 2018

Without chemotherapy there is a high recurrence rate ofMGRS conditions post-renal transplant and prioritizing func-tional improvement requires early diagnosis as opposed to thepassive monitoring in MGUS [2] (Table 3) Recent advancespoint to time of flight mass spectrometry (MS) without theneed for expensive proteomic analysis though the ability to dis-criminate and identify the pathological protein has to be dem-onstrated [52] Laser microdissection and MS proteomics arerecommended to confirm AL amyloidosis cases of abnormalMIDD with truncated MIg or instances where the specific MIgregion is of interest [19 42] Urinary exosomes which have dif-ferent characteristics in AL amyloidosis and MGUS combinedwith MS may become the diagnostic and monitoring tools aftermore evidence is available [53] In daily practice parameters ofkidney function creatinine and proteinuria can be comparedwith assessment of the course of progression and response totreatment [54] However first-line monitoring should includeparaprotein levels and indirect disease activity markers whichtrack evolution of the primary disease
Non-invasive screening tools for on-going diagnosis of plasmacell dyscrasia particularly in difficult to identify MGRS condi-tions are of interest Vij et al [55] reported on deep sequencingof peripheral blood demonstrating clonal plasma cells in 96 ofMM patients In the case of IgM MGRS which suggests the pres-ence of B-celllymphoplasmacytic clone it is necessary to attemptto specify the clonal population through bone marrow andorlymph node biopsy and radiographic imaging [2 16] F18 posi-tron emission computed tomography can identify potential ab-normal lymph nodes for biopsy in conjunction with peripheralblood flow cytometry [54] MRI to exclude marrow involvementmay also be considered With the heterogeneity of MGRS asidefrom determining the conclusive histopathology character exclu-sion of plasma cell malignancy is necessary
T R E A T M E N T F O R M G R S mdash A N O V E R V I E W
A multi-disciplinary collaboration between nephrologist pa-thologist and haematologist is a priority in the diagnosis andtreatment of these individuals Therapy should incorporate bi-opsy-driven diagnosis with particular clinical features and dis-ease course prediction Identification of the clone responsiblefor MGRS and appropriate haematological treatment shouldtranslate into better RR and prevention of progression MGRSpatients with doubled serum creatinine or reduced renal func-tion may be at higher risk of haematological progression (oddsratio 26 CI 03ndash24) [10] In MM the reversal of RI has beenshown to improve outcome [56] Treatment of CD20thorn clonesshould utilize rituximab (RTX) while MGRS conditions par-ticularly non-IgM MGRS should consider MM regimens asprovided below and summarized in Table 1 With the rarityand wide array of MGRS conditions establishing strong evi-dence for treatment is difficult and evidence is limited to anec-dotal cases or small patient series
C Y T O T O X I C D R U G S
Historically melphalan-prednisone (MP) was used for thetreatment of plasma cell dyscrasias but due to the low response T
able
1T
hera
peut
icre
gim
ens
for
prim
ary
MG
RS
con
diti
ons
Dru
gC
hara
cter
Dis
ease
char
acte
rSe
veri
tyof
kidn
eyin
suff
icie
ncy
Ref
eren
ce
Lena
lidom
ide
LoD
exM
PT
Clin
ical
tria
lM
Mw
ith
RI
149
pati
ents
CrC
llt30
mL
min
372
pts
CrC
l30
lt50
Dim
opou
los
etal
[57
]B
enda
mus
tine
PV
Ret
rosp
ecti
veM
Mw
ith
RI
18eG
FRlt
35m
Lm
in(1
1pt
seG
FR15
mL
min
)P
onis
chet
al[
58]
RT
XC
YC
Dex
Ret
rosp
ecti
veIn
dole
ntN
HL
Glo
mer
ulon
ephr
itis
rela
ted
toM
Ig14
pts
(71
5w
ith
eGFR
lt60
mL
min
)P
erry
etal
[59
]
PO
ML
oDex
Clin
ical
tria
lR
elap
sed
refr
acto
ryM
Mw
ith
RI
Thr
eeco
hort
smdash33
eGFR
30ndash4
5m
Lm
inpt
s34lt
30m
Lm
ineG
FRpt
s14
HD
pts
Dim
opou
los
etal
[60
]
RT
XC
linic
altr
ial
Mem
bran
ous
neph
ropa
thy
eGFR
40P
rote
inur
ia
5g
24h
Ferv
enza
etal
[61
]V
MP
vers
usM
PC
linic
altr
ial
MM
wit
hR
I34
ptslt
30m
Lm
inG
FR1
93pt
sG
FR31
ndash50
mL
min
Dim
opou
los
etal
[62
]V
MP
TndashV
Tve
rsus
VM
PC
linic
altr
ial
MM
wit
hR
I33
ptslt
30m
Lm
ineG
FR1
16pt
seG
FR31
ndash50
mL
min
Mor
abit
oet
al[
63]
Ixaz
omib
Lena
lidom
idendash
Dex
Clin
ical
tria
lR
efra
ctor
yre
laps
edM
M10
pts
CrC
llt30
mL
min
169
pts
CrC
l30ndash
60m
Lm
inM
orea
uet
al[
64]
Ben
tam
usti
nem
onot
hera
py
wit
hR
TX
Ret
rosp
ecti
veC
LLN
HL
104
pts
CrC
llt40
mL
min
Nor
dstr
omet
al[
65]
Vve
rsus
IMiD
vers
usC
CC
linic
altr
ial
MM
wit
hR
I55
pts
CrC
llt30
mL
min
(9di
alys
is)
41pt
sC
rCl
30lt
50m
Lm
inR
ouss
ouet
al[
66]
T-D
exC
linic
altr
iald
ata
MM
wit
hR
Ipr
ior
toA
SCT
(ind
ucti
onth
erap
y)16
pts
CrC
llt30
mL
min
15
pts
CrC
l30ndash
50m
Lm
in(t
otal
7on
HD
)T
osie
tal
[67]
L-D
exT
wo
clin
ical
tria
lsM
MR
Ive
rsus
non-
RI
16pt
sC
rCllt
30m
Lm
inC
rCl
30lt
60in
82pt
sD
imop
oulo
uset
al[
68]
PO
Mndashl
owD
exT
hree
clin
ical
tria
lsM
Mw
ith
RI
355
pts
wit
hC
rCl
30an
dlt
60m
Lm
in(1
66pt
sC
rCl
30lt
45)
Sieg
elet
al[
69]
Car
filzo
mib
Dex
vers
usB
orte
zom
ibD
exC
linic
altr
ial
Rel
apse
dre
frac
tory
MM
56pt
sC
rCllt
30m
Lm
in1
28pt
sw
ith
CrC
l30ndash
50m
Lm
inD
imop
oulo
set
al[
70]
Vb
orte
zom
ibM
mel
phal
anL
len
alid
omid
eT
tha
lidom
ide-
dexa
met
haso
ne
Vb
orte
zom
ibC
Cc
onve
ntio
nalc
hem
othe
rapy
CLL
chr
onic
lym
phoc
ytic
leuk
aem
iaN
HL
non-
Hod
gkin
lym
phom
apt
spa
tien
ts
4 K Batko et alDownloaded from httpsacademicoupcomndtadvance-article-abstractdoi101093ndtgfy2595086133by gueston 29 August 2018
rates has been replaced by more potent regimens In LCDDwith MGUS MP and plasmapheresis prolonged survival how-ever kidney function deteriorated which marks the inefficiencyof the old regimes
To achieve a higher and more durable haematological re-sponse (HR) and potentially to qualify for kidney transplant(Ktx) high-dose melphalan supported with autologous stemcell transplantation (ASCT) is considered highly efficacious inMM and AL SCT has been shown to improve survival in ALamyloidosis and MIDD [71 72] Achieving a very good partialresponse (VGPR)complete response (CR) is associated with abetter RR rate than a HR lt VGPR [31 32 73] Importantly anadvanced impairment of renal function may impact responseindependently of achieving HR [32 74] Preventing renal dam-age will likely only be achieved by earlier diagnosis
I M M U N O M O D U L A T O R Y A G E N T S
Thalidomide the first immunomodulatory drug (IMiD) agentapproved for the treatment of myeloma can be safely adminis-tered regardless of renal function Outside the USA thalido-mide remains a viable choice in CrCl lt50 mLmin1 73 m2since it is not renally cleared [67] Song et al [75] report that inpatients with a low glomerular filtration rate (GFR) defined aslt40 mLmin173 m2 cyclophosphamide (CYC) was betterthan MP when combined with thalidomide with regard to re-nal functional improvement adverse events overall survival(OS) and mortality due to infection (P lt 0001) Lenalidomideis renally cleared and doses need to be adjusted for renal insuffi-ciency (CrCl lt60 mLmin) Complete blood counts should beperformed on a regular basis in the setting of moderate to severerenal insufficiency so that the lenalidomide dose may be modi-fied in the setting of unacceptable cytopenias [68] In a study of41 AL amyloidosis patients treated with lenalidomide 66were observed with kidney dysfunction and 10 required dialy-sis [76] However for approximately 25 of patients the initialdoses were too high and for half dosage was not appropriatelyadjusted Another aspect was older age and worse renal statusin those who experienced more severe impairment Recently alarge MM trial reported that renal function-adapted lenalido-mide dose resulted in similar safety across all levels of RI(Table 1) [57]
Pomalidomide (POM) is effective in lenalidomide-refractorycases and suitable for any CrCl (Table 1) However the recom-mendation for patients on dialysis is 3 mg rather than the stan-dard 4 mg dose and should be administered following dialysis[77] The latest results of POM and low-dose dexamethasone(LoDex) showed acceptable safety of 4 mgday in patients witheGFRlt30 mLmin173 m2 and on dialysis though CR wasonly achieved in eGFR 30ndash45 mLmin173 m2 [60] IMiDshave been used with effectiveness in MM AL amyloidosisMIDD CG Type 1 and LCPT (Tables 1 and 2) [27 31 85]
P R O T E A S O M E I N H I B I T O R S mdash N O V E L D R U G S
In 2015 bortezomib a first-generation proteasome inhibitorwas established as a class 1 A treatment (BDex) standard by theEuropean Myeloma Network for MM with RI [86] Bortezomib
showed a favourable profile with metabolism independent ofkidney function and demonstrated to be beneficial in advancedrenal failure and dialysis [87 88] A systematic review in 2014concluded that bortezomib was preferable to other agents inMM with RI [89] The most prominent adverse event is periph-eral neuropathy which may be a troublesome side effect in of-ten mildly symptomatic MGRS conditions Bortezomibpromotes a high rate of haematological CR as well as RR inMM with RI [90] High-dose Dex is linked to a faster RR how-ever mildly symptomatic MGRS patients may not be willing tocomply with the side effects whereas treatment-wise achievinga faster RR may improve the disease course [88] Bortezomibhigh-dose Dex is recommended by the IMWG for patients withMM-related RI whereas a three-drug scheme is deemed to im-prove RR [91]
In 50 patients with C3 glomerulopathy associated withmonoclonal gammopathy chemotherapy effectively achievedHR the only predictor of RR in multivariate analysis into sig-nificantly higher RR and renal survival rates compared withstandard immunosuppression [92] Bortezomib-based regimesmade up 76 of the chemotherapy group also being signifi-cantly associated with RR in univariate analysis Bortezomib-based treatment in 49 patients with MIDD reported at least aVGPR in 704 with HR not significantly different fromHDMSCT [93] Maintained haematological remission was as-sociated with survival in all patients at 85 months follow-up incomparison with 52 at 48 months in a series published in2003 [74] Ziogas et al [94] reported on 18 MIDD patientstreated exclusively with bortezomib regimes with gt VGPR in333 and an equal number progressing to end-stage renal dis-ease (ESRD) In the 2003 study by Pozzi et al progression wassimilar at 368 suggesting that even late induction of noveltherapy will not overcome poor prognosis associated with ad-vanced renal insufficiency The higher efficacy reported byCohen et al may be explained by overall less advanced kidneyfailure and proteinuria Together the studies demonstrate thatprevention of poor kidney function is necessary to treat effec-tively regardless of treatment regime
Recently the spectrum of MGRS has been reviewed in thecontext of monoclonal IgA deposits RTX did not elicit a RRwhile bortezomib-based treatment was suggested as first-linestrategy [33] Of 22 LCPT patients six MGRS patients weretreated with bortezomib-based regimes with 333 reaching atleast VGPR while the remainder had stable disease [27]Untreated patients progressed to ESRD while multivariateanalysis showed initial eGFR to be the only predictor of renalfunction This brings further support to prioritizing early detec-tion and subsequent chemotherapy to prevent deterioration ofkidney function In AL amyloidosis CyBorDBDex is stem cellspairing and therefore can be used in patients who may yetqualify for SCT as well as renal failure [95] In 53 patients withLCDD of which 57 were in Stage 45 CKD achieving at leasta VGPR improved renal outcome with bortezomib-based regi-mens achieving CR in eight out of nine cases [31] MIDD haspreviously been reported with poor outcomes and progressionto ESRD [24] Kourelis et al [73] studied 88 patients withMIDD (42 MGRS) of which 69 presented with eGFR
Clinical implication of monoclonal gammopathies 5Downloaded from httpsacademicoupcomndtadvance-article-abstractdoi101093ndtgfy2595086133by gueston 29 August 2018
lt30 mLmin1732 reporting proteasome inhibitorSCT as themost feasible therapeutic choice Achievement of completevery good partial HR was necessary for a RR while RR was anindependent predictor of progression again highlighting theprinciples of MGRS treatment In patients with PGNMID whodo not respond to initial treatment with RTXCYC and ste-roids bortezomib-based treatment may elicit a response [51]Bortezomib-based therapy was effective even in refractory casesof CG Type 1 related to MM [85 96 97]
Carfilzomib is a second-generation proteasome inhibitorDimopoulos et al [98] reported that carfilzomib-based therapyimproved renal outcome in 55 of patients with eGFRlt60 mLmin173 m2 Renal function may initially temporarilydecrease though therapy improves renal function A cardiacrisk profile should be treated with exceptional care Patient pro-file assessment and further studies will determine the use inMGRS
M O N O C L O N A L A N T I B O D I E S
Patients with MGUS treated with RTX and prednisone had im-proved kidney function and decreased proteinuria In patientswith MPGN secondary to indolent clones RTX CYC andprednisone were more effective then RTX with steroidsmono-therapy [99] Therapeutic doses of monoclonal antibodies maybe administered even in renal failure and post-renal allograftsettings [100 101] In seven patients with glomerulonephritiswith monoclonal IgG deposits RTX has been observed withpromising results [five achieved CR two partial response (PR)][102] The added benefit of RTX over classic chemotherapyrelates to a more tolerable profile Treatment of 14 PGNMIDpatients in approaches of clone-directed and empirical therapywithout identifiable discrasia was effective with patients withno detectable clone responding with complete and PSs in allbut two cases Bortezomib-based therapy may be effective innon-responders While empirical treatment is not easily under-taken with clonal detection at 25ndash32 it seems justified con-sidering the rate of response [22 51] However the studypopulation is not robust and the benefitsafety of such an ap-proach is in need of confirmation by larger studiesInterestingly patients with eGFR 20 had similar rates of CRPR to eGFR45 and all patients were free of ESRD in follow-up underscoring the value of a haematological treatment ap-proach in MGRS [51] RTXndashCYCndashDex use in 14 patients withMIg-associated glomerulopathy secondary to indolent non-Hodgkin lymphomas was reported on with 64 achieving CR(Table 1) The antiproteinuric effect of RTX is another benefi-cial aspect A steroid-free regimen of bendamustine and RTXprospectively assessed in indolent B-cell lymphoma of renalsignificance resulted in 85 achieving a haematological CRand 75 a complete RR [103] Patients without RR did notachieve HR Bendamustine is primarily cleared by hydrolysiswith minimal kidney involvement and recently there is sub-stantial evidence suggesting its safety in advanced renal failurethough complete blood counts should be monitored for haema-tological abnormality [104 105] (Table 1) RTX should be con-sidered in patients with IgM-associated MGRS especially when
Tab
le2
AL
base
dre
gim
ens
for
trea
tmen
tof
MG
RS
Dru
gP
atie
nts
and
met
hods
Out
com
esC
oncl
usio
nsR
efer
ence
VC
Dve
rsus
VD
101
pts
AL
amyl
oido
sis
(11
rena
lSta
ge3)
Sim
ilar
HR
(Pfrac14
026
)R
R43
fo
rV
Dve
rsus
41
for
VC
D(Pgt
005
)si
mila
rsu
rviv
al(Pfrac14
045
)H
ighe
rdo
sing
ofD
exan
dC
YC
addi
tion
does
noti
m-
pact
ther
apy
outc
omes
sign
ifica
ntly
Kas
trit
iset
al[
78]
CV
Dve
rsus
CT
D13
9pt
sw
ith
AL
amyl
oido
sis
Hig
her
CR
inC
VD
(40
6ve
rsus
246
)
med
ian
PFS
280
vers
us14
0m
onth
sre
spec
tive
lyFa
stcl
onal
cont
rold
idno
tred
uce
earl
ym
orta
lity
Ven
ner
etal
[79
]
CyB
orD
230
pts
wit
h63
w
ith
rena
linv
olve
men
t60
H
R4
3V
GP
R2
5R
RE
ffica
ciou
sin
pati
ents
wit
hout
card
iac
invo
lvem
ent
sur-
viva
lis
depe
nden
ton
deep
resp
onse
Pal
ladi
niet
al[
80]
DA
RA
Ret
rosp
ecti
vere
view
of25
cons
ecut
ive
AL
pts
HR
in76
C
Rin
36
VG
PR
24
wel
ltol
erat
edev
enin
card
iac
pts
Effi
caci
ous
inhe
avily
pre-
trea
ted
Kau
fman
etal
[81
]
Pom
alid
omid
endashD
ex28
pts
wit
hA
Lam
yloi
dosi
s68
H
Rgt
VG
PR
in29
5
3w
ith
resp
onse
afte
r1
cycl
eA
noth
erch
oice
inre
frac
tory
AL
impr
oves
surv
ival
hae
-m
atol
ogic
alpr
ogre
ssio
npr
edic
tssu
rviv
alP
alla
dini
etal
[82
]
LMD
50A
Lam
yloi
dosi
spt
s62
w
ith
rena
lloa
d(4
inre
nalS
tage
III)
CR
18
VG
PR
32
OR
in48
h
aem
atol
ogic
and
card
iac
toxi
city
4
mor
talit
y1
case
ofac
ute
kidn
eyin
jury
len
alid
omid
edo
seha
sto
bem
onit
ored
and
adju
sted
oth
erw
ise
tole
rabl
ean
def
ficac
ious
Heg
enba
rtet
al[
83]
M-D
ex25
9A
Lam
yloi
dosi
spt
sH
R76
C
R31
in
high
dose
ver
sus
51an
d12
in
atte
nuat
edO
Ron
lyin
pati
ents
wit
hH
R(h
ighe
rin
CR
vers
usV
GP
R)
Pal
ladi
niet
al[
84]
VG
PH
Rv
ery
good
part
ialh
aem
atol
ogic
alre
spon
seE
GC
Ge
piga
lloca
tech
inga
llate
LM
Dl
enal
idom
ide
mel
phal
ande
xam
etha
sone
VC
Db
orte
zom
ibcy
clop
hosp
ham
ide
dexa
met
haso
neM
-Dex
mel
phal
ande
xam
etha
sone
6 K Batko et alDownloaded from httpsacademicoupcomndtadvance-article-abstractdoi101093ndtgfy2595086133by gueston 29 August 2018
Tab
le3
Mon
oclo
nal
gam
mop
athy
inth
ese
ttin
gof
kidn
eytr
ansp
lan
tati
on
Pat
ient
san
dm
etho
dsO
utco
mes
Con
clus
ions
Ref
eren
ce
27LC
PT
pati
ents
trea
ted
wit
hch
emo-
ther
apy
(11
SCT
)9
wit
hno
trea
tmen
tLo
wes
tm
orta
lity
best
HR
sin
SCT
tho
ugh
pati
ents
wer
eyo
unge
ran
dha
dbe
stin
itia
land
final
rena
lfu
ncti
on
Bes
tren
alou
tcom
eco
mpa
red
wit
hch
emot
hera
pyor
notr
eatm
ent
SCT
stab
ilize
dor
impr
oved
rena
lfun
ctio
nSt
okes
etal
[27
]
64M
IDD
pati
ents
16
pts
trea
ted
wit
hSC
T4
Ktx
3re
curr
ence
sin
4K
txpa
tien
tsr
ange
of7ndash
43m
onth
s38
pr
ogre
ssio
nto
ESR
Din
SCT
Hig
hcr
eati
nine
atbi
opsy
isas
soci
ated
wit
hpo
orou
t-co
me
chem
othe
rapy
afte
rre
curr
ence
isin
effic
ient
Nas
ret
al[
24]
49M
IDD
pati
ents
3K
txw
ith
1V
GP
Ran
d2
CR
18
SCT
No
recu
rren
ces
in3
Ktx
pati
ents
allo
graf
trej
ecti
onin
1pa
tien
taft
er3
year
sSC
Tw
assa
fean
dto
lera
ted
but
pati
ents
wer
eyo
unge
rbo
rtez
omib
-bas
edtr
eatm
enth
adsi
mila
rR
Rra
tes
Sust
aine
d
VG
PR
nece
ssar
yfo
rK
txS
CT
ispr
efer
red
CK
Dst
ages
Coh
enet
al[
93]
29M
PG
NK
txpa
tien
ts6
wit
hm
onoc
lona
lpro
tein
(4M
GU
S1
CLL
)23
of
MP
GN
pati
ents
have
mon
oclo
nalp
rote
ins
may
incr
ease
risk
ofre
curr
ence
SC
Tre
solv
edre
curr
ence
pl
asm
aphe
res
aspa
ssiv
em
aint
enan
ce
MP
GN
pati
ents
shou
ldbe
scre
ened
for
mon
oclo
nal
prot
eins
Lore
nzet
al[
110]
6LC
DD
wit
hSC
T1
pati
entd
idno
tsur
vive
SCT
all
othe
rsac
hiev
edH
R
2re
laps
esw
ith
1im
prov
edby
subs
eque
ntch
emot
hera
py
Insu
ffici
ent
resp
onse
toSC
Tm
aybe
anin
dica
tion
for
Ktx
inse
lect
pati
ents
afte
rac
hiev
ing
HR
Lore
nzet
al[
122]
7LC
DD
Ktx
pati
ents
Med
ian
recu
rren
ce2ndash
45m
onth
sfo
r5
pati
ents
sub
se-
quen
t4de
aths
onl
y1
pati
entf
ree
ofre
new
alA
HR
mus
tbe
achi
eved
befo
reat
tem
ptin
gK
txLe
ung
etal
[10
9]
2P
GN
MID
Ktx
pati
ents
(1de
novo
1re
curr
ent)
Impr
ovem
ent
ingr
aftf
unct
ion
and
seru
mcr
eati
nine
in2
year
follo
w-u
pR
TX
can
beef
fect
ive
inbo
thre
curr
enta
ndde
novo
PG
NM
IDpt
sM
erhi
etal
[12
3]
3P
GN
MID
(2C
LL)
Des
pite
RT
Xtr
eatm
entt
here
was
1pr
ogre
ssio
nto
ESR
Dan
don
em
alig
nanc
ypr
ogre
ssio
nR
TX
ther
apy
may
impr
ove
rena
lout
com
esin
shor
tter
mB
arbo
uret
al[
124]
53LC
DD
7K
tx1
6SC
T2
recu
rren
ces
inpa
tien
tsw
itho
utpr
ior
chem
othe
rapy
1
reje
ctio
nof
Ktx
3pa
tien
tsin
CR
ingt
68
year
follo
w-
up1
SCT
-rel
ated
deat
h13
15
achi
eved
CR
SCT
can
besu
cces
sful
even
inC
KD
Stag
e4
how
ever
re
nals
urvi
vali
sst
illw
orse
SC
Tap
pear
sm
ore
safe
than
inA
Lam
yloi
dosi
s
Saye
det
al[
31]
21K
txw
itC
3GN
667
re
curr
ence
ofw
hich
21
asso
ciat
edw
ith
mon
o-cl
onal
gam
mop
athy
rec
urre
nce
earl
ier
(36
mon
thm
e-di
anve
rsus
433
mon
th)
mor
epr
ogre
ssiv
eco
urse
(Pfrac14
NS)
SC
Tim
prov
edki
dney
func
tion
inon
epa
tien
tst
a-bl
egr
aft
in10
-yea
rfo
llow
-up
Mon
oclo
nalg
amm
opat
hypa
tien
tsar
eat
risk
ofan
ear-
lier
and
mor
eag
gres
sive
dise
ase
Zan
det
al[
125]
548
Ktx
pati
ents
Pre
vale
nce
81
52
year
med
ian
toM
GU
Sdi
scov
ery
high
erra
teof
MB
Lhi
stor
yof
infla
mm
ator
yki
dney
dis-
ease
aspr
edic
tive
fact
orn
oas
soci
atio
nw
ith
age
and
gend
ern
oim
pact
ongr
afts
urvi
val
over
alls
urvi
val
in-
cide
nce
ofm
alig
nanc
y
MG
US
pre-
and
post
-tra
nspl
antm
aybe
diff
eren
tcon
di-
tion
sin
term
sof
man
agem
ent
how
ever
str
ict
follo
w-u
pis
need
ede
spec
ially
inM
BL
pati
ents
Alfa
noet
al[
126]
159
3K
txre
cipi
ents
3pr
e-tr
ansp
lant
MG
(nfrac14
34)
No
case
sof
prog
ress
ion
noas
soci
atio
nw
ith
mal
igna
ncy
inci
denc
eor
mor
talit
yJi
men
ezZ
eped
aet
al[
117]
587
Ktx
reci
pien
ts2
9in
cide
nce
(9pt
spr
e-tr
ansp
lant
8po
st)
No
prog
ress
ion
duri
ng6-
year
follo
w-u
pM
GU
Sno
taco
ntra
indi
cati
onto
Ktx
Ban
cuet
al[
127]
351
8K
txre
cipi
ents
42pa
tien
ts(2
3pr
e-tr
ansp
lant
19
post
)m
edia
nsu
rviv
al26
1ve
rsus
280
year
sre
spec
tive
ly4
haem
atol
ogic
alm
a-lig
nanc
ies
deve
lope
din
pre
2P
TLD
gt15
year
spo
st-
tran
spla
nt
Dia
gnos
isof
PT
LDw
assy
mpt
om-b
ased
tru
ein
cide
nce
may
behi
gher
exc
lusi
onof
asso
ciat
edki
dney
dise
ase
and
mal
igna
ncy
isne
cess
ary
befo
reK
tx
Nai
naet
al[
118]
MB
Lm
onoc
lona
lB-c
elll
ymph
ocyt
osis
Clinical implication of monoclonal gammopathies 7Downloaded from httpsacademicoupcomndtadvance-article-abstractdoi101093ndtgfy2595086133by gueston 29 August 2018
CD20thorn cells can be identified while non-IgM-associated dis-eases more often require MM-like treatment
Recently an anti CD38 monoclonal antibody daratumumab(DARA) has been approved for the treatment of newly diag-nosed and relapsed MM patients [106] Like many Phase 3 reg-istration trials the study excluded patients with CrCl 20 mLmin Anecdotal evidence of safety and reduction of dialysis fre-quency in a patient with DARA monotherapy has recently beenreported [107] A case of PGNMID refractory to RTX and
bortezomib was successfully treated with DARA [108] Due toindependence of kidney clearance and positive results in RI itmay prove beneficial in MGRS There is an on-going Phase 2study of DARA in MGRS [NCT03095118]
M G R S T R A N S P L A N T A N D E S R D
Renal transplant in MGRS is controversial as frequent recur-rences are observed when the abnormal clone is not adequately
FIGURE 1 Diagnostic and therapeutic algorithm of monoclonal gammopathy of renal significance
8 K Batko et alDownloaded from httpsacademicoupcomndtadvance-article-abstractdoi101093ndtgfy2595086133by gueston 29 August 2018
suppressed [24 109 110] The current treatment paradigm inMGRS is to achieve a complete HR as a means of improvingpost-transplant outcome and preventing recurrence [71 72111] Cibeira et al [112] report that in 340 AL amyloidosispatients subject to SCT 43 attained CR improving long-termOS and organ response (OR) In recent years the treatment-re-lated mortality (TRM) has decreased from 138 between 1994and 2003 to 56 between 2004 and 2008 In part this probablyreflects the experience of established centres however with ac-cess to novel agents there are other options for treatmentCardiac involvement should be screened for in LCDD due to ahigh TRM (23) with SCT as opposed to non-cardiac patients[32] PS does not indicate treatment failure and significantlyincreases survival compared with patients lacking response[113]
A study in AL amyloidosis patients associated the need fordialysis within 30 days of SCT with highest early death risk andTRM Patients with both eGFRlt40 mLmin173 m2 and se-rum albumin lt25 mgdL had a 438 and 281 risk of requir-ing dialysis and chance of TRM respectively Identifying andscreening for such risk factors should improve the feasibility ofSCT in MGRS conditions [114] In a study of 36 patients withAL amyloidosisMIDD who were dialysis dependent for ESRDCR was reached in 53 at 1 year post SCT with an 8 TRM[72] Achievement of dialysis independence was possible inpatients receiving a Ktx after successful SCT Similarly a studyin MM with RI found no impact on survival for patients whowere dialysis dependent [115] Further research is required toevaluate risk factors and establish whether select ESRD patientsmay benefit from SCT
Literature reports are conflicting on the approach to Ktx inMGUS [116ndash118] Bansal et al [119] reflect that a select groupof plasma dyscrasia patients should be considered for Ktx espe-cially those subject to dialysis-associated complications In ALand MIDD patients achieving haematological CR have beenreported with successful Ktx [120 121] Monoclonal gammop-athy in the setting of Ktxs is presented in Table 3 In summaryprimary disease activity organ function and patient perfor-mance should dictate selection for Ktx We propose an algo-rithm for diagnostic and therapeutic treatment of MGRS(Figure 1)
C O N C L U S I O N
With under-recognition of the wide spectrum of MGRS accu-rate classification evidence-based therapy and expert estab-lished management is required Renal involvement in MGRSresults from the direct deposition of monoclonal protein and itslight- or heavy-chain fragments in the kidney IFE microscopyis essential to identify the offending monoclonal protein and itsrenal tissue distribution In selected cases MS is of valueMGRS therapy is directed to eliminate the clonal plasma cell orB-cell population Adverse events particular to the chosen drugshould complement the patient profile Early detection diagno-sis and chemotherapy may improve kidney function It shouldbe stressed that both the renal pathology and the underlyinghaematological disorders influence the management and
prognosis of MGRS Upon achieving HR ASCT and Ktx shouldbe considered as therapy endpoints in MGRS
C O N F L I C T O F I N T E R E S T S T A T E M E N T
None declared
R E F E R E N C E S
1 Kyle RA Monoclonal gammopathy of undetermined significance NaturalHistory in 241 Cases Am J Med [Internet] 1978 [cited 2017 Oct 24] 64814ndash826 Available from httpwwwncbinlmnihgovpubmed645746
2 Leung N Bridoux F Hutchison CA et al Monoclonal gammopathy of re-nal significance when MGUS is no longer undetermined or insignificantBlood [Internet] 2012 [cited 2017 Oct 24] 120 4292ndash4295 Available fromhttpwwwncbinlmnihgovpubmed23047823
3 Kyle RA Therneau TM Rajkumar SV et al Prevalence of monoclonalgammopathy of undetermined significance N Engl J Med [Internet] 2006[cited 2017 Oct 24] 354 1362ndash1369 Available from httpwwwncbinlmnihgovpubmed16571879
4 Landgren O Graubard BI Kumar S et al Prevalence of myeloma precur-sor state monoclonal gammopathy of undetermined significance in 12372individuals 10ndash49 years old a population-based study from the NationalHealth and Nutrition Examination Survey Blood Cancer J 2017 7 e618[cited 2018 Feb 9] 7 Available from httpwwwncbinlmnihgovpubmed29053158
5 Landgren O Graubard BI Katzmann JA et al Racial disparities in theprevalence of monoclonal gammopathies a population-based study of12 482 persons from the National Health and Nutritional ExaminationSurvey Leukemia [Internet] 2014 28 1537ndash1542 [cited 2018 Jun 22]Available from httpwwwncbinlmnihgovpubmed24441287
6 Cabrera Q Macro M Hebert B et al Epidemiology of monoclonal gamm-opathy of undetermined significance (MGUS) the experience from thespecialized registry of hematologic malignancies of Basse-Normandie(France) Cancer Epidemiol [Internet] 2014 38 354ndash356 [cited 2017 Oct24] Available from httpwwwncbinlmnihgovpubmed24880205
7 Therneau TM Kyle RA Melton LJ et al Incidence of monoclonal gamm-opathy of undetermined significance and estimation of duration beforefirst clinical recognition Mayo Clin Proc [Internet] 2012 [cited 2017 Dec23] 87 1071ndash1079 Available from httpwwwncbinlmnihgovpubmed22883742
8 Kyle RA Larson DR Therneau TM et al Long-term follow-up of mono-clonal gammopathy of undetermined significance N Engl J Med 2018[cited 2018 Apr 23] 378 241ndash249 Available from httpwwwncbinlmnihgovpubmed29342381
9 Dispenzieri A Katzmann JA Kyle RA et al Prevalence and risk of progres-sion of light-chain monoclonal gammopathy of undetermined significancea retrospective population-based cohort study Lancet [Internet] 2010[cited 2018 Feb 9] 375 1721ndash1728 Available from httpwwwncbinlmnihgovpubmed20472173
10 Steiner N Gobel G Suchecki P et al Monoclonal gammopathy of renalsignificance (MGRS) increases the risk for progression to multiple mye-loma an observational study of 2935 MGUS patients Oncotarget[Internet] 2018 [cited 2018 Apr 27] 9 2344ndash2356 Available from httpwwwncbinlmnihgovpubmed29416776
11 Dhodapkar MV Sexton R Waheed S et al Clinical genomic andimaging predictors of myeloma progression from asymptomaticmonoclonal gammopathies (SWOG S0120) Blood [Internet] 2014[cited 2018 Jun 22] 123 78ndash85 Available from httpwwwncbinlmnihgovpubmed24144643
12 Zand L Kattah A Fervenza FC et al C3 glomerulonephritis associatedwith monoclonal gammopathy a case series Am J Kidney Dis [Internet]2013 [cited 2017 Dec 29] 62 506ndash514 Available from httpwwwncbinlmnihgovpubmed23623956
13 Rajkumar SV Dimopoulos MA Palumbo A et al International MyelomaWorking Group updated criteria for the diagnosis of multiple myelomaLancet Oncol [Internet] 2014 [cited 2018 Jun 23] 15 e538ndashe548 Availablefrom httplinkinghubelseviercomretrievepiiS1470204514704425
Clinical implication of monoclonal gammopathies 9Downloaded from httpsacademicoupcomndtadvance-article-abstractdoi101093ndtgfy2595086133by gueston 29 August 2018
14 Ravindran A Bartley AC Holton SJ et al Prevalence incidence and sur-vival of smoldering multiple myeloma in the United States Nat PublishingGroup [Internet] 2016 6 2018ndash2023 [cited Jun] Available from httpswwwncbinlmnihgovpmcarticlesPMC5098258pdfbcj2016100apdf
15 Fermand J-P Bridoux F Kyle RA et al How I treat monoclonal gammop-athy of renal significance (MGRS) Blood [Internet] 2013 [cited 2017 Oct27] 122 3583ndash3590 Available from httpwwwncbinlmnihgovpubmed24108460
16 Bridoux F Leung N Hutchison CA et al Diagnosis of monoclonal gamm-opathy of renal significance Kidney Int [Internet] 2015 [cited 2017 Oct24] 87 698ndash711 Available from httpwwwncbinlmnihgovpubmed25607108
17 Kristinsson SY Bjorkholm M Andersson TM-L et al Patterns of survivaland causes of death following a diagnosis of monoclonal gammopathy ofundetermined significance a population-based study Haematologica[Internet] 2009 [cited 2018 Feb] 94 1714ndash1720 Available from httpwwwncbinlmnihgovpubmed19608666
18 Dimopoulos MA Delimpasi S Katodritou E et al Significant improve-ment in the survival of patients with multiple myeloma presenting with se-vere renal impairment after the introduction of novel agents Ann Oncol[Internet] 2014 [cited 2018 Apr 23] 25 195ndash200 Available from httpsacademicoupcomannoncarticle-lookupdoi101093annoncmdt483
19 Correia SO Santos S Malheiro J et al Monoclonal gammopathy of renalsignificance diagnostic workup WJN 2017 [cited 2017 Oct 27] 6 72ndash78Available from httpwwwncbinlmnihgovpubmed28316940
20 Lin J Markowitz GS Valeri AM et al Renal monoclonal immunoglobulindeposition disease the disease spectrum J Am Soc Nephrol [Internet] 2001[cited 2018 Jun 23] 12 1482ndash1492 Available from httpwwwncbinlmnihgovpubmed11423577
21 Sethi S Zand L Leung N et al Membranoproliferative glomerulonephritissecondary to monoclonal gammopathy Clin J Am Soc Nephrol [Internet]2010 [cited 2017 Dec 8] 5 770ndash782 Available from httpwwwncbinlmnihgovpubmed20185597
22 Bhutani G Nasr SH Said SM et al Hematologic characteristics of prolifer-ative glomerulonephritides with nonorganized monoclonal immunoglobu-lin deposits Mayo Clin Proc [Internet] 2015 [cited 2018 Jun 23] 90587ndash596 Available from httpwwwncbinlmnihgovpubmed25939936
23 Cohen C El-Karoui K Alyanakian M-A et al Light and heavy chain depo-sition disease associated with CH1 deletion Clin Kidney J [Internet] 2015[cited 2017 Oct 26] 8 237ndash239 Available from httpwwwncbinlmnihgovpubmed25815184
24 Nasr SH Valeri AM Cornell LD et al Renal monoclonal immunoglobulindeposition disease a report of 64 patients from a single institution Clin JAm Soc Nephrol [Internet] 2012 [cited 2018 Feb 9] 7 231ndash239 Availablefrom httpwwwncbinlmnihgovpubmed22156754
25 Sicard A Karras A Goujon J-M et al Light chain deposition disease with-out glomerular proteinuria a diagnostic challenge for the nephrologistNephrol Dial Transplant [Internet] 2014 [cited 2018 Jul 7] 29 1894ndash1902Available from httpwwwncbinlmnihgovpubmed24619059
26 Haas M A reevaluation of routine electron microscopy in the examinationof native renal biopsies J Am Soc Nephrol [Internet] 1997 8 70ndash76Available from httpwwwncbinlmnihgovpubmed9013450
27 Stokes MB Valeri AM Herlitz L et al Light chain proximal tubulopathyclinical and pathologic characteristics in the modern treatment era J AmSoc Nephrol [Internet] 2016 [cited 2018 Jun 23] 27 1555ndash1565 Availablefrom httpwwwncbinlmnihgovpubmed26374607
28 Larsen CP Messias NC Walker PD et al Membranoproliferative glomeru-lonephritis with masked monotypic immunoglobulin deposits Kidney Int[Internet] 2015 [cited 2018 Feb 10] 88 867ndash873 Available from httpwwwncbinlmnihgovpubmed26154922
29 Eirin A Irazabal MV Gertz MA et al Clinical features of patients with im-munoglobulin light chain amyloidosis (AL) with vascular-limited deposi-tion in the kidney Nephrol Dial Transplant [Internet] 2012 [cited 2018Feb 10] 27 1097ndash1101 Available from httpwwwncbinlmnihgovpubmed22067518
30 Alonso-Titos J Perea-Ortega L Sola E et al C3 glomerulonephritis associ-ated with monoclonal gammopathy of renal significance case report BMCNephrol 2018 Jul 6] 19 129 Available from httpwwwncbinlmnihgovpubmed29884135
31 Sayed RH Wechalekar AD Gilbertson JA et al Natural history and out-come of light chain deposition disease Blood [Internet] 2015 [cited 2017Dec 8] 126 2805ndash2810 Available from httpwwwncbinlmnihgovpubmed26392598
32 Mohan M Buros A Mathur P et al Clinical characteristics and prognosticfactors in multiple myeloma patients with light chain deposition diseaseAm J Hematol 2017 [cited 2018 Jul 7] 92 739ndash745 Available from httpwwwncbinlmnihgovpubmed28383130
33 Vignon M Cohen C Faguer S et al The clinicopathologic characteristicsof kidney diseases related to monotypic IgA deposits Kidney Int [Internet]2017 [cited 2018 Jul] 91 720ndash728 Available from httpwwwncbinlmnihgovpubmed28069266
34 Best Rocha A Larsen CP Membranous glomerulopathy with light chain-restricted deposits a clinicopathological analysis of 28 cases Kidney IntRep [Internet] 2017 [cited 2018 Jul 6] 2 1141ndash1148 Available from httpwwwncbinlmnihgovpubmed29270522
35 Nasr SH Valeri AM Sethi S et al Clinicopathologic correlations in multi-ple myeloma a case series of 190 patients with kidney biopsies Am JKidney Dis [Internet] 2012 [cited 2017 Oct 26] 59 786ndash794 Availablefrom httpwwwncbinlmnihgovpubmed22417785
36 Glavey SV Leung N Monoclonal gammopathy the good the bad and theugly Blood Rev [Internet] 2016 [cited 2017 Dec 24] 30 223ndash231 Availablefrom httpwwwsciencedirectcomsciencearticlepiiS0268960X15000946bb0130
37 Katzmann JA Kyle RA Benson J et al Screening panels for detection ofmonoclonal gammopathies Clin Chem [Internet] 2009 [cited 2017 Oct25] 55 1517ndash1522 Available from httpwwwncbinlmnihgovpubmed19520758
38 Yadav P Leung N Sanders PW et al The use of immunoglobulin lightchain assays in the diagnosis of paraprotein-related kidney disease KidneyInt [Internet] 2015 [cited 2018 Feb 9] 87 692ndash697 Available from httpwwwncbinlmnihgovpubmed25296094
39 Sugihara H Chihara D Seike K et al Percentage of urinary albumin excre-tion and serum-free light-chain reduction are important determinants ofrenal response in myeloma patients with moderate to severe renal impair-ment Blood Cancer J [Internet] 2014 [cited 2018 Jun 24] 4 e235 Availablefrom httpwwwncbinlmnihgovpubmed25083819
40 Leung N Gertz M Kyle RA et al Urinary albumin excretion patterns ofpatients with cast nephropathy and other monoclonal gammopathy-related kidney diseases Clin J Am Soc Nephrol [Internet] 2012 [cited 2018Jun 24] 7 1964ndash1968 Available from httpwwwncbinlmnihgovpubmed23024162
41 Ciocchini M Arbelbide J Musso CG Monoclonal gammopathy of renalsignificance (MGRS) the characteristics and significance of a new meta-entity Int Urol Nephrol [Internet] 2017 [cited 2017 Oct 26] 492171ndash2175 Available from httpwwwncbinlmnihgovpubmed28425076
42 Sethi S Rajkumar SV DrsquoAgati VD The complexity and heterogeneity ofmonoclonal immunoglobulinndashassociated renal diseases J Am Soc Nephrol2018 29 1810ndash1823
43 Hutchison CA Harding S Hewins P et al Quantitative assessment of se-rum and urinary polyclonal free light chains in patients with chronic kid-ney disease Clin J Am Soc Nephrol [Internet] 2008 [cited 2017 Dec 25] 31684ndash1690 Available from httpwwwncbinlmnihgovpubmed18945993
44 Jurczyszyn A Ochrem B Abnormal serum free light chain ratio does notalways indicate monoclonal gammopathy Polskie Archiwum MedycynyWewnetrznej [Internet] 2015 [cited 2017 Dec 29] 125 502ndash504 Availablefrom httpwwwncbinlmnihgovpubmed26266682
45 Singh G Serum free light chain assay and jk ratio performance inpatients with monoclonal gammopathy-high false negative rate for jk ra-tio J Clin Med Res 2017 [cited 2018 Jun 25] 9 46ndash57 Available fromhttpwwwncbinlmnihgovpubmed27924175
46 Fulton RB Fernando SL Serum free light chain assay reduces the need forserum and urine immunofixation electrophoresis in the evaluation ofmonoclonal gammopathy Ann Clin Biochem [Internet] 2009 [cited 2018Jun 25] 46 407ndash412 Available from httpwwwncbinlmnihgovpubmed19641008
10 K Batko et alDownloaded from httpsacademicoupcomndtadvance-article-abstractdoi101093ndtgfy2595086133by gueston 29 August 2018
47 Levinson SS Urine immunofixation electrophoresis remains importantand is complementary to serum free light chain Clin Chem Lab Med[Internet] 2011 [cited 2018 Jun 25] 49 1801ndash1804 Available from httpwwwncbinlmnihgovpubmed21663562 [CrossRef][Mismatch]
48 Lee WS Singh G Serum free light chains in neoplastic monoclonal gam-mopathies relative under-detection of lambda dominant KappaLambdaratio and underproduction of free lambda light chains as compared tokappa light chains in patients with neoplastic monoclonal gammopathiesJ Clin Med Res 2018 [cited 2018 Jun 25] 10 562ndash569 Available fromhttpwwwncbinlmnihgovpubmed29904440
49 Xu B Tang Y Zhou J et al Disease spectrum of abnormal serum free lightchain ratio and its diagnostic significance Oncotarget [Internet] 2017[cited 2017 Dec 29] 8 82268ndash82279 Available from httpwwwncbinlmnihgovpubmed29137262
50 Koo EH Shin J Jang HR et al Diagnostic performances of M-protein testsaccording to the clinical presentations of kidney disease Eur J Intern Med[Internet] 2016 [cited 2018 Feb 9] 33 88ndash92 Available from httpwwwncbinlmnihgovpubmed27421913
51 Gumber R Cohen JB Palmer MB et al A clone-directed approach mayimprove diagnosis and treatment of proliferative glomerulonephritis withmonoclonal immunoglobulin deposits Kidney Int [Internet] 2018 94199ndash205 Available from httpsdoiorg101016jkint201802020
52 Leung N Barnidge DR Hutchison CA Laboratory testing in monoclonalgammopathy of renal significance (MGRS) Clin Chem Lab Med [Internet]2016 [cited 2017 Oct 25] 54 929ndash937 Available from httpwwwncbinlmnihgovpubmed27107835 [CrossRef][Mismatch]
53 Ramirez-Alvarado M Ward CJ Huang BQ et al Differences in immuno-globulin light chain species found in urinary exosomes in light chain amy-loidosis (AL) PLoS ONE [Internet] 2012 [cited 2018 Jul 7] 7 e38061Available from httpwwwncbinlmnihgovpubmed22723846
54 Hogan JJ Weiss BM Bridging the divide an onco-nephrologic approachto the monoclonal gammopathies of renal significance Clin J Am SocNephrol [Internet] 2016 [cited 2017 Oct 26] 11 1681ndash1691 Availablefrom httpwwwncbinlmnihgovpubmed27416775
55 Vij R Mazumder A Klinger M et al Deep sequencing reveals myelomacells in peripheral blood in majority of multiple myeloma patients ClinLymphoma Myeloma Leuk [Internet] 2014 [cited 2017 Oct 25] 14131ndash139e1 Available from httpwwwncbinlmnihgovpubmed24629890
56 Gonsalves WI Leung N Rajkumar SV et al Improvement in renal func-tion and its impact on survival in patients with newly diagnosed multiplemyeloma Blood Cancer J 2015 [cited 2018 Feb 3] 5 e296 Available fromhttpwwwnaturecomdoifinder101038bcj201520
57 Dimopoulos MA Cheung MC Roussel M et al Impact of renal impair-ment on outcomes with lenalidomide and dexamethasone treatment in theFIRST trial a randomized open-label phase 3 trial in transplant-ineligiblepatients with multiple myeloma Haematologica [Internet] 2016 [cited2018 Jul 7] 101 363ndash370 Available from httpwwwncbinlmnihgovpubmed26659916
58 Ponisch W Andrea M Wagner I et al Successful treatment of patientswith newly diagnoseduntreated multiple myeloma and advanced renalfailure using bortezomib in combination with bendamustine and predni-sone J Cancer Res Clin Oncol 2012 [cited 2018 Jul 2] 138 1405ndash1412Available from httpwwwncbinlmnihgovpubmed22526157
59 Perry M Delarche A Ribes D et al Rituximab-cyclophosphamide-dexa-methasone is highly effective in patients with monoclonal Ig deposit-related glomerulopathy and indolent non-Hodgkin lymphomas Am JHematol 2014 [cited 2018 Jul 1] 89 969ndash973 Available from httpdoiwileycom101002ajh23798
60 Dimopoulos M Weisel K van de Donk Nwcj et al Pomalidomide pluslow-dose dexamethasone in patients with relapsedrefractory multiple my-eloma and renal impairment results from a Phase II trial J Clin Oncol2018 36 2035ndash2043
61 Fervenza FC Canetta PA Barbour SJ et al A multicenter randomized con-trolled trial of rituximab versus cyclosporine in the treatment of idiopathicmembranous nephropathy (MENTOR) Nephron [Internet] 2015 [cited2017 Dec 25] 130 159ndash168 Available from httpwwwncbinlmnihgovpubmed26087670
62 Dimopoulos MA Richardson PG Schlag R et al VMP (bortezomib mel-phalan and prednisone) is active and well tolerated in newly diagnosedpatients with multiple myeloma with moderately impaired renal functionand results in reversal of renal impairment cohort analysis of the Phase IIIVISTA study JCO 2009 [cited 2017 Dec 8] 27 6086ndash6093 Available fromhttpwwwncbinlmnihgovpubmed19858394
63 Morabito F Gentile M Mazzone C et al Safety and efficacy ofbortezomib-melphalan-prednisone-thalidomide followed by bortezomib-thalidomide maintenance (VMPT-VT) versus bortezomib-melphalan-prednisone (VMP) in untreated multiple myeloma patients with renal im-pairment Blood [Internet] 2011 [cited 2017 Dec 9] 118 5759ndash5766Available from httpwwwncbinlmnihgovpubmed21951682
64 Moreau P Masszi T Grzasko N et al Oral ixazomib lenalidomide anddexamethasone for multiple myeloma N Engl J Med 2016 [cited 2018 Apr27] 374 1621ndash1634 Available from httpwwwnejmorgdoi101056NEJMoa1516282
65 Nordstrom BL Knopf KB Teltsch DY et al The safety of bendamustine inpatients with chronic lymphocytic leukemia or non-Hodgkin lymphomaand concomitant renal impairment a retrospective electronic medical re-cord database analysis Leuk Lymphoma [Internet] 2014 [cited 2017 Dec13] 55 1266ndash1273 Available from httpwwwncbinlmnihgovpubmed23987821
66 Roussou M Kastritis E Christoulas D et al Reversibility of renal failure innewly diagnosed patients with multiple myeloma and the role of novelagents Leuk Res [Internet] 2010 [cited 2017 Dec 15] 34 1395ndash1397Available from httpwwwncbinlmnihgovpubmed20510452
67 Tosi P Zamagni E Tacchetti P et al Thalidomide-dexamethasone as in-duction therapy before autologous stem cell transplantation in patientswith newly diagnosed multiple myeloma and renal insufficiency BiolBlood Marrow Transplant [Internet] 2010 [cited 2018 Apr 27] 161115ndash1121 Available from httpwwwncbinlmnihgovpubmed20197100
68 Dimopoulos M Alegre A Stadtmauer EA et al The efficacy and safety oflenalidomide plus dexamethasone in relapsed andor refractory multiplemyeloma patients with impaired renal function Cancer [Internet] 2010116 3807 [cited 2017 Dec 15] Available from httpwwwncbinlmnihgovpubmed20564094
69 Siegel DS Weisel KC Dimopoulos MA et al Pomalidomide plus low-dosedexamethasone in patients with relapsedrefractory multiple myeloma andmoderate renal impairment a pooled analysis of three clinical trials LeukLymphoma [Internet] 2016 [cited 2017 Dec 15] 57 2833ndash2838 Availablefrom httpwwwncbinlmnihgovpubmed27267105
70 Dimopoulos MA Goldschmidt H Niesvizky R et al Carfilzomib or borte-zomib in relapsed or refractory multiple myeloma (ENDEAVOR) an in-terim overall survival analysis of an open-label randomised phase 3 trialLancet Oncol [Internet] 2017 [cited 2017 Dec 6] 18 1327ndash1337 Availablefrom httpwwwncbinlmnihgovpubmed28843768
71 Telio D Shepherd J Forrest D et al High-dose melphalan followed byauto-SCT has favorable safety and efficacy in selected patients with lightchain deposition disease and light and heavy chain deposition diseaseBone Marrow Transplant 2012 [cited 2017 Dec 8] 47 453ndash455 Availablefrom httpwwwnaturecomdoifinder101038bmt201187
72 Batalini F Econimo L Quillen K et al High-dose melphalan and stem celltransplantation in patients on dialysis due to immunoglobulin light-chainamyloidosis and monoclonal immunoglobulin deposition disease BiolBlood Marrow Transplant [Internet] 2018 [cited 2017 Dec 25] 24127ndash132 Available from httpwwwncbinlmnihgovpubmed28865972
73 Kourelis TV Nasr SH Dispenzieri A et al Outcomes of patients with renalmonoclonal immunoglobulin deposition disease Am J Hematol 2016[cited 2018 Jul 2] 91 1123ndash1128 Available from httpwwwncbinlmnihgovpubmed27501122
74 Pozzi C DrsquoAmico M Fogazzi GB et al Light chain deposition disease withrenal involvement clinical characteristics and prognostic factors Am JKidney Dis [Internet] 2003 [cited 2018 Jun 23] 42 1154ndash1163 Availablefrom httpwwwncbinlmnihgovpubmed14655186
75 Song M-K Chung J-S Shin H-J et al Cyclophosphamide-containing regi-men (TCD) is superior to melphalan-containing regimen (MPT) in elderlymultiple myeloma patients with renal impairment Ann Hematol
Clinical implication of monoclonal gammopathies 11Downloaded from httpsacademicoupcomndtadvance-article-abstractdoi101093ndtgfy2595086133by gueston 29 August 2018
[Internet] 2012 [cited 2017 Dec 9] 91 889ndash896 Available from httpwwwncbinlmnihgovpubmed22237937
76 Specter R Sanchorawala V Seldin DC et al Kidney dysfunction duringlenalidomide treatment for AL amyloidosis Nephrol Dial Transplant[Internet] 2011 [cited 2018 Jul 7] 26 881ndash886 Available from httpwwwncbinlmnihgovpubmed20693160
77 Li Y Wang X OrsquoMara E et al Population pharmacokinetics of pomalido-mide in patients with relapsed or refractory multiple myeloma with variousdegrees of impaired renal function CPAA 2017 [cited 2018 Feb 4] 9133ndash145 Available from httpwwwncbinlmnihgovpubmed29184451
78 Kastritis E Gavriatopoulou M Roussou M et al Addition of cyclophos-phamide and higher doses of dexamethasone do not improve outcomes ofpatients with AL amyloidosis treated with bortezomib Blood Cancer J2017 [cited 2017 Dec 15] 7 e570 Available from httpwwwncbinlmnihgovpubmed28622303
79 Venner CP Gillmore JD Sachchithanantham S et al A matched compari-son of cyclophosphamide bortezomib and dexamethasone (CVD) versusrisk-adapted cyclophosphamide thalidomide and dexamethasone (CTD)in AL amyloidosis Leukemia [Internet] 2014 [cited 2018 Jul 5] 282304ndash2310 Available from httpwwwncbinlmnihgovpubmed25027514
80 Palladini G Sachchithanantham S Milani P et al A European collabora-tive study of cyclophosphamide bortezomib and dexamethasone inupfront treatment of systemic AL amyloidosis Blood [Internet] 2015[cited 2017 Dec 9] 126 612ndash615 Available from httpwwwncbinlmnihgovpubmed25987656
81 Kopel T Kaufman JS Hamburg N et al Endothelium-dependent and -in-dependent vascular function in advanced chronic kidney disease CJASN2017 [cited 2018 Apr 18] 12 1588ndash1594 Available from httpcjasnasnjournalsorglookupdoi102215CJN12811216
82 Palladini G Milani P Foli A et al A Phase 2 trial of pomalidomide anddexamethasone rescue treatment in patients with AL amyloidosis Blood[Internet] 2017 [cited 2018 Apr 26] 129 2120ndash2123 Available fromhttpwwwncbinlmnihgovpubmed28130212
83 Hegenbart U Bochtler T Benner A et al Lenalidomidemelphalandexa-methasone in newly diagnosed patients with immunoglobulin light chainamyloidosis results of a prospective phase 2 study with long-term followup Haematologica [Internet] 2017 [cited 2017 Dec 26] 102 1424ndash1431Available from httpwwwncbinlmnihgovpubmed28522573
84 Palladini G Milani P Foli A et al Oral melphalan and dexamethasonegrants extended survival with minimal toxicity in AL amyloidosis long-term results of a risk-adapted approach Haematologica [Internet] 2014[cited 2017 Dec 15] 99 743ndash750 Available from httpwwwncbinlmnihgovpubmed24213149
85 Payet J Livartowski J Kavian N et al Type I cryoglobulinemia in multiplemyeloma a rare entity analysis of clinical and biological characteristics ofseven cases and review of the literature Leuk Lymphoma [Internet] 201354 767ndash777 Available from httpwwwtandfonlinecomdoifull103109104281942012671481
86 Terpos E Kleber M Engelhardt M et al European Myeloma Networkguidelines for the management of multiple myeloma-related complica-tions Haematologica [Internet] 2015 [cited 2017 Dec 4] 100 1254ndash1266Available from httpwwwncbinlmnihgovpubmed26432383
87 Chanan-Khan AA Kaufman JL Mehta J et al Activity and safety of borte-zomib in multiple myeloma patients with advanced renal failure a multi-center retrospective study Blood [Internet] 2007 [cited 2018 Jul 2] 1092604ndash2606 Available from httpwwwncbinlmnihgovpubmed17138816
88 Dimopoulos MA Roussou M Gkotzamanidou M et al The role of novelagents on the reversibility of renal impairment in newly diagnosed symp-tomatic patients with multiple myeloma Leukemia 2013 27 423ndash429
89 Kouroukis TC Baldassarre FG Haynes AE et al Bortezomib in multiplemyeloma systematic review and clinical considerations Curr Oncol(Toronto Ont) [Internet] 2014 [cited 2017 Dec 4] 21 e573ndashe603Available from httpwwwncbinlmnihgovpubmed25089109
90 Zhu W Chen W Bortezomib-based treatment for multiple myelomapatients with renal impairment a systematic review and meta-analysis ofobservational studies Medicine [Internet] 2016 95 e5202 Available fromhttpwwwncbinlmnihgovpmcarticlesPMC5120900
91 Dimopoulos MA Terpos E Chanan-Khan A et al Renal impairment inpatients with multiple myeloma a consensus statement on behalf of theInternational Myeloma Working Group JCO 2010 28 4976ndash4984
92 Chauvet S Fremeaux-Bacchi V Petitprez F et al Treatment of B-cell disor-der improves renal outcome of patients with monoclonal gammopathyndashassociated C3 glomerulopathy Blood [Internet] 2017 [cited 2017 Oct 26]129 1437ndash1447 Available from httpwwwncbinlmnihgovpubmed28069603
93 Cohen C Royer B Javaugue V et al Bortezomib produces high hematolog-ical response rates with prolonged renal survival in monoclonal immuno-globulin deposition disease Kidney Int [Internet] 2015 [cited 2017 Dec25] 88 1135ndash1143 Available from httpwwwncbinlmnihgovpubmed26176826
94 Ziogas DC Kastritis E Terpos E et al Hematologic and renal improve-ment of monoclonal immunoglobulin deposition disease after treatmentwith bortezomib-based regimens Leuk Lymphoma [Internet] 2017 [cited2017 Dec 25] 58 1832ndash1839 Available from httpwwwncbinlmnihgovpubmed27967286
95 Milani P Merlini G Palladini G Novel therapies in light chain amyloid-osis Kidney Int Rep [Internet] 2018 [cited 2018 Jul 4] 3 530ndash541 Availablefrom httpwwwncbinlmnihgovpubmed29854961
96 Spizzo G Mitterer M Gunsilius E Bortezomib for the treatment of refrac-tory Type-1 cryoglobulinaemia Br J Haematol [Internet] 2010 [cited 2018Jul 7] 150 235ndash237 Available from httpdoiwileycom101111j1365-2141201008184x
97 Talamo G Claxton D Tricot G et al Response to bortezomib in refractoryType I cryoglobulinemia Am J Hematol 2008 [cited 2018 Jul 7] 83883ndash884 Available from httpwwwncbinlmnihgovpubmed18756542
98 Dimopoulos MA Roussou M Gavriatopoulou M et al Cardiac and renalcomplications of carfilzomib in patients with multiple myeloma BloodAdv 2017 [cited 2017 Dec 6] 1 449ndash454 Available from httpwwwbloodadvancesorglookupdoi101182bloodadvances2016003269
99 Strati P Nasr SH Leung N et al Renal complications in chronic lympho-cytic leukemia and monoclonal B-cell lymphocytosis the Mayo Clinic ex-perience Haematologica [Internet] 2015 [cited 2018 Jul 3] 100 1180ndash1188Available from httpwwwncbinlmnihgovpubmed26088927
100 Salama AD Pusey CD Drug insight rituximab in renal disease and trans-plantation Nat Clin Pract Nephrol [Internet] 2006 [cited 2017 Dec 8] 2221ndash230 Available from httpwwwnaturecomdoifinder101038ncpneph0133
101 Jillella AP Dainer PM Kallab AM et al Treatment of a patient with end-stage renal disease with rituximab pharmacokinetic evaluation suggestsrituximab is not eliminated by hemodialysis Am J Hematol 2002 [cited2018 Jul] 71 219ndash222 Available from httpwwwncbinlmnihgovpubmed12410580
102 Guiard E Karras A Plaisier E et al Patterns of noncryoglobulinemic glo-merulonephritis with monoclonal Ig deposits correlation with IgG sub-class and response to rituximab Clin J Am Soc Nephrol 2011 6 1609ndash1616
103 Ribes D Hachem HEL Oberic L et al Bendamustine plus rituximab forindolent B-cell lymphoma of renal significance Am J Hematol 2018 93356ndash362
104 Darwish M Bond M Hellriegel E et al Pharmacokinetic and pharmacody-namic profile of bendamustine and its metabolites Cancer ChemotherPharmacol 2015 [cited 2017 Dec 15] 75 1143ndash1154 Available from httpwwwncbinlmnihgovpubmed25829094
105 Ponisch W Moll B Bourgeois M et al Bendamustine and prednisone incombination with bortezomib (BPV) in the treatment of patients with re-lapsed or refractory multiple myeloma and light chain-induced renal fail-ure J Cancer Res Clin Oncol [Internet] 2013 [cited 2018 Jul 2] 1391937ndash1946 Available from httpwwwncbinlmnihgovpubmed24046251
106 Mateos M-V Dimopoulos MA Cavo M et al Daratumumab plus bortezo-mib melphalan and prednisone for untreated myeloma N Engl J Med2018 378 518ndash528
107 Rocchi S Tacchetti P Pantani L et al Safety and efficacy of daratumumabin dialysis-dependent renal failure secondary to multiple myelomaHaematologica [Internet] 2018 [cited 2018 Jul 2] 103 e277ndashe278 Availablefrom httpwwwncbinlmnihgovpubmed29622654
12 K Batko et alDownloaded from httpsacademicoupcomndtadvance-article-abstractdoi101093ndtgfy2595086133by gueston 29 August 2018
108 Anand S Miller D Chipman G Morris D Srinivas S Daratumumab forsevere refractory proliferative glomerulonephritis with monoclonal im-mune deposits (PGNMID) ATC Abstr [Internet] 2017 [cited 2018 Jul 3]Available from httpsatcmeetingabstractscomabstractdaratumumab-for-severe-refractory-proliferative-glomerulonephritis-with-monoclonal-immune-deposits-pgnmid
109 Leung N Lager DJ Gertz MA et al Long-term outcome of renal transplan-tation in light-chain deposition disease Am J Kidney Dis [Internet] 2004[cited 2018 Feb 9] 43 147ndash153 Available from httpwwwncbinlmnihgovpubmed14712438
110 Lorenz EC Sethi S Leung N et al Recurrent membranoproliferative glo-merulonephritis after kidney transplantation Kidney Int [Internet] 2010[cited 2018 Feb 9] 77 721ndash728 Available from httpwwwncbinlmnihgovpubmed20130531
111 Leung N Nasr SH A patient with abnormal kidney function and a mono-clonal light chain in the urine Clin J Am Soc Nephrol 2016 11 1073ndash1082
112 Cibeira MT Sanchorawala V Seldin DC et al Outcome of AL amyloidosisafter high-dose melphalan and autologous stem cell transplantation long-term results in a series of 421 patients Blood [Internet] 2011 [cited 2018Feb 3] 118 4346ndash4352 Available from httpwwwncbinlmnihgovpubmed21828140
113 Gertz MA Lacy MQ Dispenzieri A et al Autologous stem cell transplantfor immunoglobulin light chain amyloidosis a status report LeukLymphoma [Internet] 2010 [cited 2018 Feb 3] 51 2181ndash2187 Availablefrom httpwwwncbinlmnihgovpubmed20958232
114 Leung N Kumar SK Glavey SV et al The impact of dialysis on the survivalof patients with immunoglobulin light chain (AL) amyloidosis undergoingautologous stem cell transplantation Nephrol Dial Transplant 2016 [cited2018 Jul 7] 31 1284ndash1289 Available from httpsacademicoupcomndtarticle-lookupdoi101093ndtgfv328
115 Badros A Barlogie B Siegel E et al Results of autologous stem cell trans-plant in multiple myeloma patients with renal failure Br J Haematol 2001[cited 2018 Jul 7] 114 822ndash829 Available from httpwwwncbinlmnihgovpubmed11564069
116 Soltero L Carbajal H Xu J et al Initial survival data of kidney transplantpatients with pre-transplant monoclonal gammopathy Clin Transplant[Internet] 2012 [cited 2018 Feb 3] 26 300ndash304 Available from httpwwwncbinlmnihgovpubmed22044717
117 Jimenez-Zepeda VH Heilman RL Engel RA et al Monoclonal gammopathyof undetermined significance does not affect outcomes in patients undergoingsolid organ transplants Transplantation [Internet] 2011 [cited 2018 Feb 3]92 570ndash574 Available from httpwwwncbinlmnihgovpubmed21712755
118 Naina HVK Harris S Dispenzieri A et al Long-term follow-up of patientswith monoclonal gammopathy of undetermined significance after kidney
transplantation Am J Nephrol 2012 [cited 2018 Feb] 35 365ndash371Available from httpwwwncbinlmnihgovpubmed22473253
119 Bansal T Garg A Snowden JA et al Defining the role of renal transplanta-tion in the modern management of multiple myeloma and other plasmacell dyscrasias Nephron Clin Pract [Internet] 2012 [cited 2018 Feb 3] 120c228 wwwkargercom
120 Hassoun H Flombaum C DrsquoAgati VD et al High-dose melphalan andauto-SCT in patients with monoclonal Ig deposition disease Bone MarrowTransplant 2008 [cited 2018 Feb 3] 42 405ndash412 Available from httpwwwncbinlmnihgovpubmed18574442
121 Herrmann SMS Gertz MA Stegall MD et al Long-term outcomes ofpatients with light chain amyloidosis (AL) after renal transplantation withor without stem cell transplantation Nephrol Dial Transplant [Internet]2011 [cited 2018 Feb 3] 26 2032ndash2036 Available from httpwwwncbinlmnihgovpubmed21543655
122 Lorenz EC Gertz MA Fervenza FC et al Long-term outcome of autolo-gous stem cell transplantation in light chain deposition disease NephrolDial Transplant [Internet] 2008 [cited 2018 Jul 5] 23 2052ndash2057 Availablefrom httpwwwncbinlmnihgovpubmed18178602
123 Merhi B Patel N Bayliss G et al Proliferative glomerulonephritis withmonoclonal IgG deposits in two kidney allografts successfully treated withrituximab Clin Kidney J [Internet] 2017 [cited 2018 Feb 10] 10 405ndash410Available from httpsacademicoupcomckjarticle-lookupdoi101093ckjsfx001
124 Barbour SJ Beaulieu MC Zalunardo NY et al Proliferative glomerulone-phritis with monoclonal IgG deposits secondary to chronic lymphocyticleukemia Report of two cases Nephrol Dial Transplant [Internet] 2011[cited 2018 Feb 10] 26 2712ndash2714 Available from httpsacademicoupcomndtarticle-lookupdoi101093ndtgfr251
125 Zand L Lorenz EC Cosio FG et al Clinical findings pathology and out-comes of C3GN after kidney transplantation J Am Soc Nephrol [Internet]2014 [cited 2018 Jul 5] 25 1110ndash1117 Available from httpwwwncbinlmnihgovpubmed24357668
126 Alfano G Fontana F Colaci E et al Monoclonal gammopathy of undeter-mined significance after kidney transplantation Transplantation [Internet]2017 [cited 2017 Oct 24] 101 e337ndashe342 Available from httpwwwncbinlmnihgovpubmed28731904
127 Bancu I Ca~nas L Juega FJ et al Outcomes of monoclonal gammopathyof undetermined significance in patients who underwent kidneytransplantation Transplant Proc [Internet] 2015 [cited 2018 Feb 10] 472344ndash2345 Available from httpwwwncbinlmnihgovpubmed26518922
Received 2632018 Editorial decision 1472018
Clinical implication of monoclonal gammopathies 13Downloaded from httpsacademicoupcomndtadvance-article-abstractdoi101093ndtgfy2595086133by gueston 29 August 2018

rates has been replaced by more potent regimens In LCDDwith MGUS MP and plasmapheresis prolonged survival how-ever kidney function deteriorated which marks the inefficiencyof the old regimes
To achieve a higher and more durable haematological re-sponse (HR) and potentially to qualify for kidney transplant(Ktx) high-dose melphalan supported with autologous stemcell transplantation (ASCT) is considered highly efficacious inMM and AL SCT has been shown to improve survival in ALamyloidosis and MIDD [71 72] Achieving a very good partialresponse (VGPR)complete response (CR) is associated with abetter RR rate than a HR lt VGPR [31 32 73] Importantly anadvanced impairment of renal function may impact responseindependently of achieving HR [32 74] Preventing renal dam-age will likely only be achieved by earlier diagnosis
I M M U N O M O D U L A T O R Y A G E N T S
Thalidomide the first immunomodulatory drug (IMiD) agentapproved for the treatment of myeloma can be safely adminis-tered regardless of renal function Outside the USA thalido-mide remains a viable choice in CrCl lt50 mLmin1 73 m2since it is not renally cleared [67] Song et al [75] report that inpatients with a low glomerular filtration rate (GFR) defined aslt40 mLmin173 m2 cyclophosphamide (CYC) was betterthan MP when combined with thalidomide with regard to re-nal functional improvement adverse events overall survival(OS) and mortality due to infection (P lt 0001) Lenalidomideis renally cleared and doses need to be adjusted for renal insuffi-ciency (CrCl lt60 mLmin) Complete blood counts should beperformed on a regular basis in the setting of moderate to severerenal insufficiency so that the lenalidomide dose may be modi-fied in the setting of unacceptable cytopenias [68] In a study of41 AL amyloidosis patients treated with lenalidomide 66were observed with kidney dysfunction and 10 required dialy-sis [76] However for approximately 25 of patients the initialdoses were too high and for half dosage was not appropriatelyadjusted Another aspect was older age and worse renal statusin those who experienced more severe impairment Recently alarge MM trial reported that renal function-adapted lenalido-mide dose resulted in similar safety across all levels of RI(Table 1) [57]
Pomalidomide (POM) is effective in lenalidomide-refractorycases and suitable for any CrCl (Table 1) However the recom-mendation for patients on dialysis is 3 mg rather than the stan-dard 4 mg dose and should be administered following dialysis[77] The latest results of POM and low-dose dexamethasone(LoDex) showed acceptable safety of 4 mgday in patients witheGFRlt30 mLmin173 m2 and on dialysis though CR wasonly achieved in eGFR 30ndash45 mLmin173 m2 [60] IMiDshave been used with effectiveness in MM AL amyloidosisMIDD CG Type 1 and LCPT (Tables 1 and 2) [27 31 85]
P R O T E A S O M E I N H I B I T O R S mdash N O V E L D R U G S
In 2015 bortezomib a first-generation proteasome inhibitorwas established as a class 1 A treatment (BDex) standard by theEuropean Myeloma Network for MM with RI [86] Bortezomib
showed a favourable profile with metabolism independent ofkidney function and demonstrated to be beneficial in advancedrenal failure and dialysis [87 88] A systematic review in 2014concluded that bortezomib was preferable to other agents inMM with RI [89] The most prominent adverse event is periph-eral neuropathy which may be a troublesome side effect in of-ten mildly symptomatic MGRS conditions Bortezomibpromotes a high rate of haematological CR as well as RR inMM with RI [90] High-dose Dex is linked to a faster RR how-ever mildly symptomatic MGRS patients may not be willing tocomply with the side effects whereas treatment-wise achievinga faster RR may improve the disease course [88] Bortezomibhigh-dose Dex is recommended by the IMWG for patients withMM-related RI whereas a three-drug scheme is deemed to im-prove RR [91]
In 50 patients with C3 glomerulopathy associated withmonoclonal gammopathy chemotherapy effectively achievedHR the only predictor of RR in multivariate analysis into sig-nificantly higher RR and renal survival rates compared withstandard immunosuppression [92] Bortezomib-based regimesmade up 76 of the chemotherapy group also being signifi-cantly associated with RR in univariate analysis Bortezomib-based treatment in 49 patients with MIDD reported at least aVGPR in 704 with HR not significantly different fromHDMSCT [93] Maintained haematological remission was as-sociated with survival in all patients at 85 months follow-up incomparison with 52 at 48 months in a series published in2003 [74] Ziogas et al [94] reported on 18 MIDD patientstreated exclusively with bortezomib regimes with gt VGPR in333 and an equal number progressing to end-stage renal dis-ease (ESRD) In the 2003 study by Pozzi et al progression wassimilar at 368 suggesting that even late induction of noveltherapy will not overcome poor prognosis associated with ad-vanced renal insufficiency The higher efficacy reported byCohen et al may be explained by overall less advanced kidneyfailure and proteinuria Together the studies demonstrate thatprevention of poor kidney function is necessary to treat effec-tively regardless of treatment regime
Recently the spectrum of MGRS has been reviewed in thecontext of monoclonal IgA deposits RTX did not elicit a RRwhile bortezomib-based treatment was suggested as first-linestrategy [33] Of 22 LCPT patients six MGRS patients weretreated with bortezomib-based regimes with 333 reaching atleast VGPR while the remainder had stable disease [27]Untreated patients progressed to ESRD while multivariateanalysis showed initial eGFR to be the only predictor of renalfunction This brings further support to prioritizing early detec-tion and subsequent chemotherapy to prevent deterioration ofkidney function In AL amyloidosis CyBorDBDex is stem cellspairing and therefore can be used in patients who may yetqualify for SCT as well as renal failure [95] In 53 patients withLCDD of which 57 were in Stage 45 CKD achieving at leasta VGPR improved renal outcome with bortezomib-based regi-mens achieving CR in eight out of nine cases [31] MIDD haspreviously been reported with poor outcomes and progressionto ESRD [24] Kourelis et al [73] studied 88 patients withMIDD (42 MGRS) of which 69 presented with eGFR
Clinical implication of monoclonal gammopathies 5Downloaded from httpsacademicoupcomndtadvance-article-abstractdoi101093ndtgfy2595086133by gueston 29 August 2018
lt30 mLmin1732 reporting proteasome inhibitorSCT as themost feasible therapeutic choice Achievement of completevery good partial HR was necessary for a RR while RR was anindependent predictor of progression again highlighting theprinciples of MGRS treatment In patients with PGNMID whodo not respond to initial treatment with RTXCYC and ste-roids bortezomib-based treatment may elicit a response [51]Bortezomib-based therapy was effective even in refractory casesof CG Type 1 related to MM [85 96 97]
Carfilzomib is a second-generation proteasome inhibitorDimopoulos et al [98] reported that carfilzomib-based therapyimproved renal outcome in 55 of patients with eGFRlt60 mLmin173 m2 Renal function may initially temporarilydecrease though therapy improves renal function A cardiacrisk profile should be treated with exceptional care Patient pro-file assessment and further studies will determine the use inMGRS
M O N O C L O N A L A N T I B O D I E S
Patients with MGUS treated with RTX and prednisone had im-proved kidney function and decreased proteinuria In patientswith MPGN secondary to indolent clones RTX CYC andprednisone were more effective then RTX with steroidsmono-therapy [99] Therapeutic doses of monoclonal antibodies maybe administered even in renal failure and post-renal allograftsettings [100 101] In seven patients with glomerulonephritiswith monoclonal IgG deposits RTX has been observed withpromising results [five achieved CR two partial response (PR)][102] The added benefit of RTX over classic chemotherapyrelates to a more tolerable profile Treatment of 14 PGNMIDpatients in approaches of clone-directed and empirical therapywithout identifiable discrasia was effective with patients withno detectable clone responding with complete and PSs in allbut two cases Bortezomib-based therapy may be effective innon-responders While empirical treatment is not easily under-taken with clonal detection at 25ndash32 it seems justified con-sidering the rate of response [22 51] However the studypopulation is not robust and the benefitsafety of such an ap-proach is in need of confirmation by larger studiesInterestingly patients with eGFR 20 had similar rates of CRPR to eGFR45 and all patients were free of ESRD in follow-up underscoring the value of a haematological treatment ap-proach in MGRS [51] RTXndashCYCndashDex use in 14 patients withMIg-associated glomerulopathy secondary to indolent non-Hodgkin lymphomas was reported on with 64 achieving CR(Table 1) The antiproteinuric effect of RTX is another benefi-cial aspect A steroid-free regimen of bendamustine and RTXprospectively assessed in indolent B-cell lymphoma of renalsignificance resulted in 85 achieving a haematological CRand 75 a complete RR [103] Patients without RR did notachieve HR Bendamustine is primarily cleared by hydrolysiswith minimal kidney involvement and recently there is sub-stantial evidence suggesting its safety in advanced renal failurethough complete blood counts should be monitored for haema-tological abnormality [104 105] (Table 1) RTX should be con-sidered in patients with IgM-associated MGRS especially when
Tab
le2
AL
base
dre
gim
ens
for
trea
tmen
tof
MG
RS
Dru
gP
atie
nts
and
met
hods
Out
com
esC
oncl
usio
nsR
efer
ence
VC
Dve
rsus
VD
101
pts
AL
amyl
oido
sis
(11
rena
lSta
ge3)
Sim
ilar
HR
(Pfrac14
026
)R
R43
fo
rV
Dve
rsus
41
for
VC
D(Pgt
005
)si
mila
rsu
rviv
al(Pfrac14
045
)H
ighe
rdo
sing
ofD
exan
dC
YC
addi
tion
does
noti
m-
pact
ther
apy
outc
omes
sign
ifica
ntly
Kas
trit
iset
al[
78]
CV
Dve
rsus
CT
D13
9pt
sw
ith
AL
amyl
oido
sis
Hig
her
CR
inC
VD
(40
6ve
rsus
246
)
med
ian
PFS
280
vers
us14
0m
onth
sre
spec
tive
lyFa
stcl
onal
cont
rold
idno
tred
uce
earl
ym
orta
lity
Ven
ner
etal
[79
]
CyB
orD
230
pts
wit
h63
w
ith
rena
linv
olve
men
t60
H
R4
3V
GP
R2
5R
RE
ffica
ciou
sin
pati
ents
wit
hout
card
iac
invo
lvem
ent
sur-
viva
lis
depe
nden
ton
deep
resp
onse
Pal
ladi
niet
al[
80]
DA
RA
Ret
rosp
ecti
vere
view
of25
cons
ecut
ive
AL
pts
HR
in76
C
Rin
36
VG
PR
24
wel
ltol
erat
edev
enin
card
iac
pts
Effi
caci
ous
inhe
avily
pre-
trea
ted
Kau
fman
etal
[81
]
Pom
alid
omid
endashD
ex28
pts
wit
hA
Lam
yloi
dosi
s68
H
Rgt
VG
PR
in29
5
3w
ith
resp
onse
afte
r1
cycl
eA
noth
erch
oice
inre
frac
tory
AL
impr
oves
surv
ival
hae
-m
atol
ogic
alpr
ogre
ssio
npr
edic
tssu
rviv
alP
alla
dini
etal
[82
]
LMD
50A
Lam
yloi
dosi
spt
s62
w
ith
rena
lloa
d(4
inre
nalS
tage
III)
CR
18
VG
PR
32
OR
in48
h
aem
atol
ogic
and
card
iac
toxi
city
4
mor
talit
y1
case
ofac
ute
kidn
eyin
jury
len
alid
omid
edo
seha
sto
bem
onit
ored
and
adju
sted
oth
erw
ise
tole
rabl
ean
def
ficac
ious
Heg
enba
rtet
al[
83]
M-D
ex25
9A
Lam
yloi
dosi
spt
sH
R76
C
R31
in
high
dose
ver
sus
51an
d12
in
atte
nuat
edO
Ron
lyin
pati
ents
wit
hH
R(h
ighe
rin
CR
vers
usV
GP
R)
Pal
ladi
niet
al[
84]
VG
PH
Rv
ery
good
part
ialh
aem
atol
ogic
alre
spon
seE
GC
Ge
piga
lloca
tech
inga
llate
LM
Dl
enal
idom
ide
mel
phal
ande
xam
etha
sone
VC
Db
orte
zom
ibcy
clop
hosp
ham
ide
dexa
met
haso
neM
-Dex
mel
phal
ande
xam
etha
sone
6 K Batko et alDownloaded from httpsacademicoupcomndtadvance-article-abstractdoi101093ndtgfy2595086133by gueston 29 August 2018
Tab
le3
Mon
oclo
nal
gam
mop
athy
inth
ese
ttin
gof
kidn
eytr
ansp
lan
tati
on
Pat
ient
san
dm
etho
dsO
utco
mes
Con
clus
ions
Ref
eren
ce
27LC
PT
pati
ents
trea
ted
wit
hch
emo-
ther
apy
(11
SCT
)9
wit
hno
trea
tmen
tLo
wes
tm
orta
lity
best
HR
sin
SCT
tho
ugh
pati
ents
wer
eyo
unge
ran
dha
dbe
stin
itia
land
final
rena
lfu
ncti
on
Bes
tren
alou
tcom
eco
mpa
red
wit
hch
emot
hera
pyor
notr
eatm
ent
SCT
stab
ilize
dor
impr
oved
rena
lfun
ctio
nSt
okes
etal
[27
]
64M
IDD
pati
ents
16
pts
trea
ted
wit
hSC
T4
Ktx
3re
curr
ence
sin
4K
txpa
tien
tsr
ange
of7ndash
43m
onth
s38
pr
ogre
ssio
nto
ESR
Din
SCT
Hig
hcr
eati
nine
atbi
opsy
isas
soci
ated
wit
hpo
orou
t-co
me
chem
othe
rapy
afte
rre
curr
ence
isin
effic
ient
Nas
ret
al[
24]
49M
IDD
pati
ents
3K
txw
ith
1V
GP
Ran
d2
CR
18
SCT
No
recu
rren
ces
in3
Ktx
pati
ents
allo
graf
trej
ecti
onin
1pa
tien
taft
er3
year
sSC
Tw
assa
fean
dto
lera
ted
but
pati
ents
wer
eyo
unge
rbo
rtez
omib
-bas
edtr
eatm
enth
adsi
mila
rR
Rra
tes
Sust
aine
d
VG
PR
nece
ssar
yfo
rK
txS
CT
ispr
efer
red
CK
Dst
ages
Coh
enet
al[
93]
29M
PG
NK
txpa
tien
ts6
wit
hm
onoc
lona
lpro
tein
(4M
GU
S1
CLL
)23
of
MP
GN
pati
ents
have
mon
oclo
nalp
rote
ins
may
incr
ease
risk
ofre
curr
ence
SC
Tre
solv
edre
curr
ence
pl
asm
aphe
res
aspa
ssiv
em
aint
enan
ce
MP
GN
pati
ents
shou
ldbe
scre
ened
for
mon
oclo
nal
prot
eins
Lore
nzet
al[
110]
6LC
DD
wit
hSC
T1
pati
entd
idno
tsur
vive
SCT
all
othe
rsac
hiev
edH
R
2re
laps
esw
ith
1im
prov
edby
subs
eque
ntch
emot
hera
py
Insu
ffici
ent
resp
onse
toSC
Tm
aybe
anin
dica
tion
for
Ktx
inse
lect
pati
ents
afte
rac
hiev
ing
HR
Lore
nzet
al[
122]
7LC
DD
Ktx
pati
ents
Med
ian
recu
rren
ce2ndash
45m
onth
sfo
r5
pati
ents
sub
se-
quen
t4de
aths
onl
y1
pati
entf
ree
ofre
new
alA
HR
mus
tbe
achi
eved
befo
reat
tem
ptin
gK
txLe
ung
etal
[10
9]
2P
GN
MID
Ktx
pati
ents
(1de
novo
1re
curr
ent)
Impr
ovem
ent
ingr
aftf
unct
ion
and
seru
mcr
eati
nine
in2
year
follo
w-u
pR
TX
can
beef
fect
ive
inbo
thre
curr
enta
ndde
novo
PG
NM
IDpt
sM
erhi
etal
[12
3]
3P
GN
MID
(2C
LL)
Des
pite
RT
Xtr
eatm
entt
here
was
1pr
ogre
ssio
nto
ESR
Dan
don
em
alig
nanc
ypr
ogre
ssio
nR
TX
ther
apy
may
impr
ove
rena
lout
com
esin
shor
tter
mB
arbo
uret
al[
124]
53LC
DD
7K
tx1
6SC
T2
recu
rren
ces
inpa
tien
tsw
itho
utpr
ior
chem
othe
rapy
1
reje
ctio
nof
Ktx
3pa
tien
tsin
CR
ingt
68
year
follo
w-
up1
SCT
-rel
ated
deat
h13
15
achi
eved
CR
SCT
can
besu
cces
sful
even
inC
KD
Stag
e4
how
ever
re
nals
urvi
vali
sst
illw
orse
SC
Tap
pear
sm
ore
safe
than
inA
Lam
yloi
dosi
s
Saye
det
al[
31]
21K
txw
itC
3GN
667
re
curr
ence
ofw
hich
21
asso
ciat
edw
ith
mon
o-cl
onal
gam
mop
athy
rec
urre
nce
earl
ier
(36
mon
thm
e-di
anve
rsus
433
mon
th)
mor
epr
ogre
ssiv
eco
urse
(Pfrac14
NS)
SC
Tim
prov
edki
dney
func
tion
inon
epa
tien
tst
a-bl
egr
aft
in10
-yea
rfo
llow
-up
Mon
oclo
nalg
amm
opat
hypa
tien
tsar
eat
risk
ofan
ear-
lier
and
mor
eag
gres
sive
dise
ase
Zan
det
al[
125]
548
Ktx
pati
ents
Pre
vale
nce
81
52
year
med
ian
toM
GU
Sdi
scov
ery
high
erra
teof
MB
Lhi
stor
yof
infla
mm
ator
yki
dney
dis-
ease
aspr
edic
tive
fact
orn
oas
soci
atio
nw
ith
age
and
gend
ern
oim
pact
ongr
afts
urvi
val
over
alls
urvi
val
in-
cide
nce
ofm
alig
nanc
y
MG
US
pre-
and
post
-tra
nspl
antm
aybe
diff
eren
tcon
di-
tion
sin
term
sof
man
agem
ent
how
ever
str
ict
follo
w-u
pis
need
ede
spec
ially
inM
BL
pati
ents
Alfa
noet
al[
126]
159
3K
txre
cipi
ents
3pr
e-tr
ansp
lant
MG
(nfrac14
34)
No
case
sof
prog
ress
ion
noas
soci
atio
nw
ith
mal
igna
ncy
inci
denc
eor
mor
talit
yJi
men
ezZ
eped
aet
al[
117]
587
Ktx
reci
pien
ts2
9in
cide
nce
(9pt
spr
e-tr
ansp
lant
8po
st)
No
prog
ress
ion
duri
ng6-
year
follo
w-u
pM
GU
Sno
taco
ntra
indi
cati
onto
Ktx
Ban
cuet
al[
127]
351
8K
txre
cipi
ents
42pa
tien
ts(2
3pr
e-tr
ansp
lant
19
post
)m
edia
nsu
rviv
al26
1ve
rsus
280
year
sre
spec
tive
ly4
haem
atol
ogic
alm
a-lig
nanc
ies
deve
lope
din
pre
2P
TLD
gt15
year
spo
st-
tran
spla
nt
Dia
gnos
isof
PT
LDw
assy
mpt
om-b
ased
tru
ein
cide
nce
may
behi
gher
exc
lusi
onof
asso
ciat
edki
dney
dise
ase
and
mal
igna
ncy
isne
cess
ary
befo
reK
tx
Nai
naet
al[
118]
MB
Lm
onoc
lona
lB-c
elll
ymph
ocyt
osis
Clinical implication of monoclonal gammopathies 7Downloaded from httpsacademicoupcomndtadvance-article-abstractdoi101093ndtgfy2595086133by gueston 29 August 2018
CD20thorn cells can be identified while non-IgM-associated dis-eases more often require MM-like treatment
Recently an anti CD38 monoclonal antibody daratumumab(DARA) has been approved for the treatment of newly diag-nosed and relapsed MM patients [106] Like many Phase 3 reg-istration trials the study excluded patients with CrCl 20 mLmin Anecdotal evidence of safety and reduction of dialysis fre-quency in a patient with DARA monotherapy has recently beenreported [107] A case of PGNMID refractory to RTX and
bortezomib was successfully treated with DARA [108] Due toindependence of kidney clearance and positive results in RI itmay prove beneficial in MGRS There is an on-going Phase 2study of DARA in MGRS [NCT03095118]
M G R S T R A N S P L A N T A N D E S R D
Renal transplant in MGRS is controversial as frequent recur-rences are observed when the abnormal clone is not adequately
FIGURE 1 Diagnostic and therapeutic algorithm of monoclonal gammopathy of renal significance
8 K Batko et alDownloaded from httpsacademicoupcomndtadvance-article-abstractdoi101093ndtgfy2595086133by gueston 29 August 2018
suppressed [24 109 110] The current treatment paradigm inMGRS is to achieve a complete HR as a means of improvingpost-transplant outcome and preventing recurrence [71 72111] Cibeira et al [112] report that in 340 AL amyloidosispatients subject to SCT 43 attained CR improving long-termOS and organ response (OR) In recent years the treatment-re-lated mortality (TRM) has decreased from 138 between 1994and 2003 to 56 between 2004 and 2008 In part this probablyreflects the experience of established centres however with ac-cess to novel agents there are other options for treatmentCardiac involvement should be screened for in LCDD due to ahigh TRM (23) with SCT as opposed to non-cardiac patients[32] PS does not indicate treatment failure and significantlyincreases survival compared with patients lacking response[113]
A study in AL amyloidosis patients associated the need fordialysis within 30 days of SCT with highest early death risk andTRM Patients with both eGFRlt40 mLmin173 m2 and se-rum albumin lt25 mgdL had a 438 and 281 risk of requir-ing dialysis and chance of TRM respectively Identifying andscreening for such risk factors should improve the feasibility ofSCT in MGRS conditions [114] In a study of 36 patients withAL amyloidosisMIDD who were dialysis dependent for ESRDCR was reached in 53 at 1 year post SCT with an 8 TRM[72] Achievement of dialysis independence was possible inpatients receiving a Ktx after successful SCT Similarly a studyin MM with RI found no impact on survival for patients whowere dialysis dependent [115] Further research is required toevaluate risk factors and establish whether select ESRD patientsmay benefit from SCT
Literature reports are conflicting on the approach to Ktx inMGUS [116ndash118] Bansal et al [119] reflect that a select groupof plasma dyscrasia patients should be considered for Ktx espe-cially those subject to dialysis-associated complications In ALand MIDD patients achieving haematological CR have beenreported with successful Ktx [120 121] Monoclonal gammop-athy in the setting of Ktxs is presented in Table 3 In summaryprimary disease activity organ function and patient perfor-mance should dictate selection for Ktx We propose an algo-rithm for diagnostic and therapeutic treatment of MGRS(Figure 1)
C O N C L U S I O N
With under-recognition of the wide spectrum of MGRS accu-rate classification evidence-based therapy and expert estab-lished management is required Renal involvement in MGRSresults from the direct deposition of monoclonal protein and itslight- or heavy-chain fragments in the kidney IFE microscopyis essential to identify the offending monoclonal protein and itsrenal tissue distribution In selected cases MS is of valueMGRS therapy is directed to eliminate the clonal plasma cell orB-cell population Adverse events particular to the chosen drugshould complement the patient profile Early detection diagno-sis and chemotherapy may improve kidney function It shouldbe stressed that both the renal pathology and the underlyinghaematological disorders influence the management and
prognosis of MGRS Upon achieving HR ASCT and Ktx shouldbe considered as therapy endpoints in MGRS
C O N F L I C T O F I N T E R E S T S T A T E M E N T
None declared
R E F E R E N C E S
1 Kyle RA Monoclonal gammopathy of undetermined significance NaturalHistory in 241 Cases Am J Med [Internet] 1978 [cited 2017 Oct 24] 64814ndash826 Available from httpwwwncbinlmnihgovpubmed645746
2 Leung N Bridoux F Hutchison CA et al Monoclonal gammopathy of re-nal significance when MGUS is no longer undetermined or insignificantBlood [Internet] 2012 [cited 2017 Oct 24] 120 4292ndash4295 Available fromhttpwwwncbinlmnihgovpubmed23047823
3 Kyle RA Therneau TM Rajkumar SV et al Prevalence of monoclonalgammopathy of undetermined significance N Engl J Med [Internet] 2006[cited 2017 Oct 24] 354 1362ndash1369 Available from httpwwwncbinlmnihgovpubmed16571879
4 Landgren O Graubard BI Kumar S et al Prevalence of myeloma precur-sor state monoclonal gammopathy of undetermined significance in 12372individuals 10ndash49 years old a population-based study from the NationalHealth and Nutrition Examination Survey Blood Cancer J 2017 7 e618[cited 2018 Feb 9] 7 Available from httpwwwncbinlmnihgovpubmed29053158
5 Landgren O Graubard BI Katzmann JA et al Racial disparities in theprevalence of monoclonal gammopathies a population-based study of12 482 persons from the National Health and Nutritional ExaminationSurvey Leukemia [Internet] 2014 28 1537ndash1542 [cited 2018 Jun 22]Available from httpwwwncbinlmnihgovpubmed24441287
6 Cabrera Q Macro M Hebert B et al Epidemiology of monoclonal gamm-opathy of undetermined significance (MGUS) the experience from thespecialized registry of hematologic malignancies of Basse-Normandie(France) Cancer Epidemiol [Internet] 2014 38 354ndash356 [cited 2017 Oct24] Available from httpwwwncbinlmnihgovpubmed24880205
7 Therneau TM Kyle RA Melton LJ et al Incidence of monoclonal gamm-opathy of undetermined significance and estimation of duration beforefirst clinical recognition Mayo Clin Proc [Internet] 2012 [cited 2017 Dec23] 87 1071ndash1079 Available from httpwwwncbinlmnihgovpubmed22883742
8 Kyle RA Larson DR Therneau TM et al Long-term follow-up of mono-clonal gammopathy of undetermined significance N Engl J Med 2018[cited 2018 Apr 23] 378 241ndash249 Available from httpwwwncbinlmnihgovpubmed29342381
9 Dispenzieri A Katzmann JA Kyle RA et al Prevalence and risk of progres-sion of light-chain monoclonal gammopathy of undetermined significancea retrospective population-based cohort study Lancet [Internet] 2010[cited 2018 Feb 9] 375 1721ndash1728 Available from httpwwwncbinlmnihgovpubmed20472173
10 Steiner N Gobel G Suchecki P et al Monoclonal gammopathy of renalsignificance (MGRS) increases the risk for progression to multiple mye-loma an observational study of 2935 MGUS patients Oncotarget[Internet] 2018 [cited 2018 Apr 27] 9 2344ndash2356 Available from httpwwwncbinlmnihgovpubmed29416776
11 Dhodapkar MV Sexton R Waheed S et al Clinical genomic andimaging predictors of myeloma progression from asymptomaticmonoclonal gammopathies (SWOG S0120) Blood [Internet] 2014[cited 2018 Jun 22] 123 78ndash85 Available from httpwwwncbinlmnihgovpubmed24144643
12 Zand L Kattah A Fervenza FC et al C3 glomerulonephritis associatedwith monoclonal gammopathy a case series Am J Kidney Dis [Internet]2013 [cited 2017 Dec 29] 62 506ndash514 Available from httpwwwncbinlmnihgovpubmed23623956
13 Rajkumar SV Dimopoulos MA Palumbo A et al International MyelomaWorking Group updated criteria for the diagnosis of multiple myelomaLancet Oncol [Internet] 2014 [cited 2018 Jun 23] 15 e538ndashe548 Availablefrom httplinkinghubelseviercomretrievepiiS1470204514704425
Clinical implication of monoclonal gammopathies 9Downloaded from httpsacademicoupcomndtadvance-article-abstractdoi101093ndtgfy2595086133by gueston 29 August 2018
14 Ravindran A Bartley AC Holton SJ et al Prevalence incidence and sur-vival of smoldering multiple myeloma in the United States Nat PublishingGroup [Internet] 2016 6 2018ndash2023 [cited Jun] Available from httpswwwncbinlmnihgovpmcarticlesPMC5098258pdfbcj2016100apdf
15 Fermand J-P Bridoux F Kyle RA et al How I treat monoclonal gammop-athy of renal significance (MGRS) Blood [Internet] 2013 [cited 2017 Oct27] 122 3583ndash3590 Available from httpwwwncbinlmnihgovpubmed24108460
16 Bridoux F Leung N Hutchison CA et al Diagnosis of monoclonal gamm-opathy of renal significance Kidney Int [Internet] 2015 [cited 2017 Oct24] 87 698ndash711 Available from httpwwwncbinlmnihgovpubmed25607108
17 Kristinsson SY Bjorkholm M Andersson TM-L et al Patterns of survivaland causes of death following a diagnosis of monoclonal gammopathy ofundetermined significance a population-based study Haematologica[Internet] 2009 [cited 2018 Feb] 94 1714ndash1720 Available from httpwwwncbinlmnihgovpubmed19608666
18 Dimopoulos MA Delimpasi S Katodritou E et al Significant improve-ment in the survival of patients with multiple myeloma presenting with se-vere renal impairment after the introduction of novel agents Ann Oncol[Internet] 2014 [cited 2018 Apr 23] 25 195ndash200 Available from httpsacademicoupcomannoncarticle-lookupdoi101093annoncmdt483
19 Correia SO Santos S Malheiro J et al Monoclonal gammopathy of renalsignificance diagnostic workup WJN 2017 [cited 2017 Oct 27] 6 72ndash78Available from httpwwwncbinlmnihgovpubmed28316940
20 Lin J Markowitz GS Valeri AM et al Renal monoclonal immunoglobulindeposition disease the disease spectrum J Am Soc Nephrol [Internet] 2001[cited 2018 Jun 23] 12 1482ndash1492 Available from httpwwwncbinlmnihgovpubmed11423577
21 Sethi S Zand L Leung N et al Membranoproliferative glomerulonephritissecondary to monoclonal gammopathy Clin J Am Soc Nephrol [Internet]2010 [cited 2017 Dec 8] 5 770ndash782 Available from httpwwwncbinlmnihgovpubmed20185597
22 Bhutani G Nasr SH Said SM et al Hematologic characteristics of prolifer-ative glomerulonephritides with nonorganized monoclonal immunoglobu-lin deposits Mayo Clin Proc [Internet] 2015 [cited 2018 Jun 23] 90587ndash596 Available from httpwwwncbinlmnihgovpubmed25939936
23 Cohen C El-Karoui K Alyanakian M-A et al Light and heavy chain depo-sition disease associated with CH1 deletion Clin Kidney J [Internet] 2015[cited 2017 Oct 26] 8 237ndash239 Available from httpwwwncbinlmnihgovpubmed25815184
24 Nasr SH Valeri AM Cornell LD et al Renal monoclonal immunoglobulindeposition disease a report of 64 patients from a single institution Clin JAm Soc Nephrol [Internet] 2012 [cited 2018 Feb 9] 7 231ndash239 Availablefrom httpwwwncbinlmnihgovpubmed22156754
25 Sicard A Karras A Goujon J-M et al Light chain deposition disease with-out glomerular proteinuria a diagnostic challenge for the nephrologistNephrol Dial Transplant [Internet] 2014 [cited 2018 Jul 7] 29 1894ndash1902Available from httpwwwncbinlmnihgovpubmed24619059
26 Haas M A reevaluation of routine electron microscopy in the examinationof native renal biopsies J Am Soc Nephrol [Internet] 1997 8 70ndash76Available from httpwwwncbinlmnihgovpubmed9013450
27 Stokes MB Valeri AM Herlitz L et al Light chain proximal tubulopathyclinical and pathologic characteristics in the modern treatment era J AmSoc Nephrol [Internet] 2016 [cited 2018 Jun 23] 27 1555ndash1565 Availablefrom httpwwwncbinlmnihgovpubmed26374607
28 Larsen CP Messias NC Walker PD et al Membranoproliferative glomeru-lonephritis with masked monotypic immunoglobulin deposits Kidney Int[Internet] 2015 [cited 2018 Feb 10] 88 867ndash873 Available from httpwwwncbinlmnihgovpubmed26154922
29 Eirin A Irazabal MV Gertz MA et al Clinical features of patients with im-munoglobulin light chain amyloidosis (AL) with vascular-limited deposi-tion in the kidney Nephrol Dial Transplant [Internet] 2012 [cited 2018Feb 10] 27 1097ndash1101 Available from httpwwwncbinlmnihgovpubmed22067518
30 Alonso-Titos J Perea-Ortega L Sola E et al C3 glomerulonephritis associ-ated with monoclonal gammopathy of renal significance case report BMCNephrol 2018 Jul 6] 19 129 Available from httpwwwncbinlmnihgovpubmed29884135
31 Sayed RH Wechalekar AD Gilbertson JA et al Natural history and out-come of light chain deposition disease Blood [Internet] 2015 [cited 2017Dec 8] 126 2805ndash2810 Available from httpwwwncbinlmnihgovpubmed26392598
32 Mohan M Buros A Mathur P et al Clinical characteristics and prognosticfactors in multiple myeloma patients with light chain deposition diseaseAm J Hematol 2017 [cited 2018 Jul 7] 92 739ndash745 Available from httpwwwncbinlmnihgovpubmed28383130
33 Vignon M Cohen C Faguer S et al The clinicopathologic characteristicsof kidney diseases related to monotypic IgA deposits Kidney Int [Internet]2017 [cited 2018 Jul] 91 720ndash728 Available from httpwwwncbinlmnihgovpubmed28069266
34 Best Rocha A Larsen CP Membranous glomerulopathy with light chain-restricted deposits a clinicopathological analysis of 28 cases Kidney IntRep [Internet] 2017 [cited 2018 Jul 6] 2 1141ndash1148 Available from httpwwwncbinlmnihgovpubmed29270522
35 Nasr SH Valeri AM Sethi S et al Clinicopathologic correlations in multi-ple myeloma a case series of 190 patients with kidney biopsies Am JKidney Dis [Internet] 2012 [cited 2017 Oct 26] 59 786ndash794 Availablefrom httpwwwncbinlmnihgovpubmed22417785
36 Glavey SV Leung N Monoclonal gammopathy the good the bad and theugly Blood Rev [Internet] 2016 [cited 2017 Dec 24] 30 223ndash231 Availablefrom httpwwwsciencedirectcomsciencearticlepiiS0268960X15000946bb0130
37 Katzmann JA Kyle RA Benson J et al Screening panels for detection ofmonoclonal gammopathies Clin Chem [Internet] 2009 [cited 2017 Oct25] 55 1517ndash1522 Available from httpwwwncbinlmnihgovpubmed19520758
38 Yadav P Leung N Sanders PW et al The use of immunoglobulin lightchain assays in the diagnosis of paraprotein-related kidney disease KidneyInt [Internet] 2015 [cited 2018 Feb 9] 87 692ndash697 Available from httpwwwncbinlmnihgovpubmed25296094
39 Sugihara H Chihara D Seike K et al Percentage of urinary albumin excre-tion and serum-free light-chain reduction are important determinants ofrenal response in myeloma patients with moderate to severe renal impair-ment Blood Cancer J [Internet] 2014 [cited 2018 Jun 24] 4 e235 Availablefrom httpwwwncbinlmnihgovpubmed25083819
40 Leung N Gertz M Kyle RA et al Urinary albumin excretion patterns ofpatients with cast nephropathy and other monoclonal gammopathy-related kidney diseases Clin J Am Soc Nephrol [Internet] 2012 [cited 2018Jun 24] 7 1964ndash1968 Available from httpwwwncbinlmnihgovpubmed23024162
41 Ciocchini M Arbelbide J Musso CG Monoclonal gammopathy of renalsignificance (MGRS) the characteristics and significance of a new meta-entity Int Urol Nephrol [Internet] 2017 [cited 2017 Oct 26] 492171ndash2175 Available from httpwwwncbinlmnihgovpubmed28425076
42 Sethi S Rajkumar SV DrsquoAgati VD The complexity and heterogeneity ofmonoclonal immunoglobulinndashassociated renal diseases J Am Soc Nephrol2018 29 1810ndash1823
43 Hutchison CA Harding S Hewins P et al Quantitative assessment of se-rum and urinary polyclonal free light chains in patients with chronic kid-ney disease Clin J Am Soc Nephrol [Internet] 2008 [cited 2017 Dec 25] 31684ndash1690 Available from httpwwwncbinlmnihgovpubmed18945993
44 Jurczyszyn A Ochrem B Abnormal serum free light chain ratio does notalways indicate monoclonal gammopathy Polskie Archiwum MedycynyWewnetrznej [Internet] 2015 [cited 2017 Dec 29] 125 502ndash504 Availablefrom httpwwwncbinlmnihgovpubmed26266682
45 Singh G Serum free light chain assay and jk ratio performance inpatients with monoclonal gammopathy-high false negative rate for jk ra-tio J Clin Med Res 2017 [cited 2018 Jun 25] 9 46ndash57 Available fromhttpwwwncbinlmnihgovpubmed27924175
46 Fulton RB Fernando SL Serum free light chain assay reduces the need forserum and urine immunofixation electrophoresis in the evaluation ofmonoclonal gammopathy Ann Clin Biochem [Internet] 2009 [cited 2018Jun 25] 46 407ndash412 Available from httpwwwncbinlmnihgovpubmed19641008
10 K Batko et alDownloaded from httpsacademicoupcomndtadvance-article-abstractdoi101093ndtgfy2595086133by gueston 29 August 2018
47 Levinson SS Urine immunofixation electrophoresis remains importantand is complementary to serum free light chain Clin Chem Lab Med[Internet] 2011 [cited 2018 Jun 25] 49 1801ndash1804 Available from httpwwwncbinlmnihgovpubmed21663562 [CrossRef][Mismatch]
48 Lee WS Singh G Serum free light chains in neoplastic monoclonal gam-mopathies relative under-detection of lambda dominant KappaLambdaratio and underproduction of free lambda light chains as compared tokappa light chains in patients with neoplastic monoclonal gammopathiesJ Clin Med Res 2018 [cited 2018 Jun 25] 10 562ndash569 Available fromhttpwwwncbinlmnihgovpubmed29904440
49 Xu B Tang Y Zhou J et al Disease spectrum of abnormal serum free lightchain ratio and its diagnostic significance Oncotarget [Internet] 2017[cited 2017 Dec 29] 8 82268ndash82279 Available from httpwwwncbinlmnihgovpubmed29137262
50 Koo EH Shin J Jang HR et al Diagnostic performances of M-protein testsaccording to the clinical presentations of kidney disease Eur J Intern Med[Internet] 2016 [cited 2018 Feb 9] 33 88ndash92 Available from httpwwwncbinlmnihgovpubmed27421913
51 Gumber R Cohen JB Palmer MB et al A clone-directed approach mayimprove diagnosis and treatment of proliferative glomerulonephritis withmonoclonal immunoglobulin deposits Kidney Int [Internet] 2018 94199ndash205 Available from httpsdoiorg101016jkint201802020
52 Leung N Barnidge DR Hutchison CA Laboratory testing in monoclonalgammopathy of renal significance (MGRS) Clin Chem Lab Med [Internet]2016 [cited 2017 Oct 25] 54 929ndash937 Available from httpwwwncbinlmnihgovpubmed27107835 [CrossRef][Mismatch]
53 Ramirez-Alvarado M Ward CJ Huang BQ et al Differences in immuno-globulin light chain species found in urinary exosomes in light chain amy-loidosis (AL) PLoS ONE [Internet] 2012 [cited 2018 Jul 7] 7 e38061Available from httpwwwncbinlmnihgovpubmed22723846
54 Hogan JJ Weiss BM Bridging the divide an onco-nephrologic approachto the monoclonal gammopathies of renal significance Clin J Am SocNephrol [Internet] 2016 [cited 2017 Oct 26] 11 1681ndash1691 Availablefrom httpwwwncbinlmnihgovpubmed27416775
55 Vij R Mazumder A Klinger M et al Deep sequencing reveals myelomacells in peripheral blood in majority of multiple myeloma patients ClinLymphoma Myeloma Leuk [Internet] 2014 [cited 2017 Oct 25] 14131ndash139e1 Available from httpwwwncbinlmnihgovpubmed24629890
56 Gonsalves WI Leung N Rajkumar SV et al Improvement in renal func-tion and its impact on survival in patients with newly diagnosed multiplemyeloma Blood Cancer J 2015 [cited 2018 Feb 3] 5 e296 Available fromhttpwwwnaturecomdoifinder101038bcj201520
57 Dimopoulos MA Cheung MC Roussel M et al Impact of renal impair-ment on outcomes with lenalidomide and dexamethasone treatment in theFIRST trial a randomized open-label phase 3 trial in transplant-ineligiblepatients with multiple myeloma Haematologica [Internet] 2016 [cited2018 Jul 7] 101 363ndash370 Available from httpwwwncbinlmnihgovpubmed26659916
58 Ponisch W Andrea M Wagner I et al Successful treatment of patientswith newly diagnoseduntreated multiple myeloma and advanced renalfailure using bortezomib in combination with bendamustine and predni-sone J Cancer Res Clin Oncol 2012 [cited 2018 Jul 2] 138 1405ndash1412Available from httpwwwncbinlmnihgovpubmed22526157
59 Perry M Delarche A Ribes D et al Rituximab-cyclophosphamide-dexa-methasone is highly effective in patients with monoclonal Ig deposit-related glomerulopathy and indolent non-Hodgkin lymphomas Am JHematol 2014 [cited 2018 Jul 1] 89 969ndash973 Available from httpdoiwileycom101002ajh23798
60 Dimopoulos M Weisel K van de Donk Nwcj et al Pomalidomide pluslow-dose dexamethasone in patients with relapsedrefractory multiple my-eloma and renal impairment results from a Phase II trial J Clin Oncol2018 36 2035ndash2043
61 Fervenza FC Canetta PA Barbour SJ et al A multicenter randomized con-trolled trial of rituximab versus cyclosporine in the treatment of idiopathicmembranous nephropathy (MENTOR) Nephron [Internet] 2015 [cited2017 Dec 25] 130 159ndash168 Available from httpwwwncbinlmnihgovpubmed26087670
62 Dimopoulos MA Richardson PG Schlag R et al VMP (bortezomib mel-phalan and prednisone) is active and well tolerated in newly diagnosedpatients with multiple myeloma with moderately impaired renal functionand results in reversal of renal impairment cohort analysis of the Phase IIIVISTA study JCO 2009 [cited 2017 Dec 8] 27 6086ndash6093 Available fromhttpwwwncbinlmnihgovpubmed19858394
63 Morabito F Gentile M Mazzone C et al Safety and efficacy ofbortezomib-melphalan-prednisone-thalidomide followed by bortezomib-thalidomide maintenance (VMPT-VT) versus bortezomib-melphalan-prednisone (VMP) in untreated multiple myeloma patients with renal im-pairment Blood [Internet] 2011 [cited 2017 Dec 9] 118 5759ndash5766Available from httpwwwncbinlmnihgovpubmed21951682
64 Moreau P Masszi T Grzasko N et al Oral ixazomib lenalidomide anddexamethasone for multiple myeloma N Engl J Med 2016 [cited 2018 Apr27] 374 1621ndash1634 Available from httpwwwnejmorgdoi101056NEJMoa1516282
65 Nordstrom BL Knopf KB Teltsch DY et al The safety of bendamustine inpatients with chronic lymphocytic leukemia or non-Hodgkin lymphomaand concomitant renal impairment a retrospective electronic medical re-cord database analysis Leuk Lymphoma [Internet] 2014 [cited 2017 Dec13] 55 1266ndash1273 Available from httpwwwncbinlmnihgovpubmed23987821
66 Roussou M Kastritis E Christoulas D et al Reversibility of renal failure innewly diagnosed patients with multiple myeloma and the role of novelagents Leuk Res [Internet] 2010 [cited 2017 Dec 15] 34 1395ndash1397Available from httpwwwncbinlmnihgovpubmed20510452
67 Tosi P Zamagni E Tacchetti P et al Thalidomide-dexamethasone as in-duction therapy before autologous stem cell transplantation in patientswith newly diagnosed multiple myeloma and renal insufficiency BiolBlood Marrow Transplant [Internet] 2010 [cited 2018 Apr 27] 161115ndash1121 Available from httpwwwncbinlmnihgovpubmed20197100
68 Dimopoulos M Alegre A Stadtmauer EA et al The efficacy and safety oflenalidomide plus dexamethasone in relapsed andor refractory multiplemyeloma patients with impaired renal function Cancer [Internet] 2010116 3807 [cited 2017 Dec 15] Available from httpwwwncbinlmnihgovpubmed20564094
69 Siegel DS Weisel KC Dimopoulos MA et al Pomalidomide plus low-dosedexamethasone in patients with relapsedrefractory multiple myeloma andmoderate renal impairment a pooled analysis of three clinical trials LeukLymphoma [Internet] 2016 [cited 2017 Dec 15] 57 2833ndash2838 Availablefrom httpwwwncbinlmnihgovpubmed27267105
70 Dimopoulos MA Goldschmidt H Niesvizky R et al Carfilzomib or borte-zomib in relapsed or refractory multiple myeloma (ENDEAVOR) an in-terim overall survival analysis of an open-label randomised phase 3 trialLancet Oncol [Internet] 2017 [cited 2017 Dec 6] 18 1327ndash1337 Availablefrom httpwwwncbinlmnihgovpubmed28843768
71 Telio D Shepherd J Forrest D et al High-dose melphalan followed byauto-SCT has favorable safety and efficacy in selected patients with lightchain deposition disease and light and heavy chain deposition diseaseBone Marrow Transplant 2012 [cited 2017 Dec 8] 47 453ndash455 Availablefrom httpwwwnaturecomdoifinder101038bmt201187
72 Batalini F Econimo L Quillen K et al High-dose melphalan and stem celltransplantation in patients on dialysis due to immunoglobulin light-chainamyloidosis and monoclonal immunoglobulin deposition disease BiolBlood Marrow Transplant [Internet] 2018 [cited 2017 Dec 25] 24127ndash132 Available from httpwwwncbinlmnihgovpubmed28865972
73 Kourelis TV Nasr SH Dispenzieri A et al Outcomes of patients with renalmonoclonal immunoglobulin deposition disease Am J Hematol 2016[cited 2018 Jul 2] 91 1123ndash1128 Available from httpwwwncbinlmnihgovpubmed27501122
74 Pozzi C DrsquoAmico M Fogazzi GB et al Light chain deposition disease withrenal involvement clinical characteristics and prognostic factors Am JKidney Dis [Internet] 2003 [cited 2018 Jun 23] 42 1154ndash1163 Availablefrom httpwwwncbinlmnihgovpubmed14655186
75 Song M-K Chung J-S Shin H-J et al Cyclophosphamide-containing regi-men (TCD) is superior to melphalan-containing regimen (MPT) in elderlymultiple myeloma patients with renal impairment Ann Hematol
Clinical implication of monoclonal gammopathies 11Downloaded from httpsacademicoupcomndtadvance-article-abstractdoi101093ndtgfy2595086133by gueston 29 August 2018
[Internet] 2012 [cited 2017 Dec 9] 91 889ndash896 Available from httpwwwncbinlmnihgovpubmed22237937
76 Specter R Sanchorawala V Seldin DC et al Kidney dysfunction duringlenalidomide treatment for AL amyloidosis Nephrol Dial Transplant[Internet] 2011 [cited 2018 Jul 7] 26 881ndash886 Available from httpwwwncbinlmnihgovpubmed20693160
77 Li Y Wang X OrsquoMara E et al Population pharmacokinetics of pomalido-mide in patients with relapsed or refractory multiple myeloma with variousdegrees of impaired renal function CPAA 2017 [cited 2018 Feb 4] 9133ndash145 Available from httpwwwncbinlmnihgovpubmed29184451
78 Kastritis E Gavriatopoulou M Roussou M et al Addition of cyclophos-phamide and higher doses of dexamethasone do not improve outcomes ofpatients with AL amyloidosis treated with bortezomib Blood Cancer J2017 [cited 2017 Dec 15] 7 e570 Available from httpwwwncbinlmnihgovpubmed28622303
79 Venner CP Gillmore JD Sachchithanantham S et al A matched compari-son of cyclophosphamide bortezomib and dexamethasone (CVD) versusrisk-adapted cyclophosphamide thalidomide and dexamethasone (CTD)in AL amyloidosis Leukemia [Internet] 2014 [cited 2018 Jul 5] 282304ndash2310 Available from httpwwwncbinlmnihgovpubmed25027514
80 Palladini G Sachchithanantham S Milani P et al A European collabora-tive study of cyclophosphamide bortezomib and dexamethasone inupfront treatment of systemic AL amyloidosis Blood [Internet] 2015[cited 2017 Dec 9] 126 612ndash615 Available from httpwwwncbinlmnihgovpubmed25987656
81 Kopel T Kaufman JS Hamburg N et al Endothelium-dependent and -in-dependent vascular function in advanced chronic kidney disease CJASN2017 [cited 2018 Apr 18] 12 1588ndash1594 Available from httpcjasnasnjournalsorglookupdoi102215CJN12811216
82 Palladini G Milani P Foli A et al A Phase 2 trial of pomalidomide anddexamethasone rescue treatment in patients with AL amyloidosis Blood[Internet] 2017 [cited 2018 Apr 26] 129 2120ndash2123 Available fromhttpwwwncbinlmnihgovpubmed28130212
83 Hegenbart U Bochtler T Benner A et al Lenalidomidemelphalandexa-methasone in newly diagnosed patients with immunoglobulin light chainamyloidosis results of a prospective phase 2 study with long-term followup Haematologica [Internet] 2017 [cited 2017 Dec 26] 102 1424ndash1431Available from httpwwwncbinlmnihgovpubmed28522573
84 Palladini G Milani P Foli A et al Oral melphalan and dexamethasonegrants extended survival with minimal toxicity in AL amyloidosis long-term results of a risk-adapted approach Haematologica [Internet] 2014[cited 2017 Dec 15] 99 743ndash750 Available from httpwwwncbinlmnihgovpubmed24213149
85 Payet J Livartowski J Kavian N et al Type I cryoglobulinemia in multiplemyeloma a rare entity analysis of clinical and biological characteristics ofseven cases and review of the literature Leuk Lymphoma [Internet] 201354 767ndash777 Available from httpwwwtandfonlinecomdoifull103109104281942012671481
86 Terpos E Kleber M Engelhardt M et al European Myeloma Networkguidelines for the management of multiple myeloma-related complica-tions Haematologica [Internet] 2015 [cited 2017 Dec 4] 100 1254ndash1266Available from httpwwwncbinlmnihgovpubmed26432383
87 Chanan-Khan AA Kaufman JL Mehta J et al Activity and safety of borte-zomib in multiple myeloma patients with advanced renal failure a multi-center retrospective study Blood [Internet] 2007 [cited 2018 Jul 2] 1092604ndash2606 Available from httpwwwncbinlmnihgovpubmed17138816
88 Dimopoulos MA Roussou M Gkotzamanidou M et al The role of novelagents on the reversibility of renal impairment in newly diagnosed symp-tomatic patients with multiple myeloma Leukemia 2013 27 423ndash429
89 Kouroukis TC Baldassarre FG Haynes AE et al Bortezomib in multiplemyeloma systematic review and clinical considerations Curr Oncol(Toronto Ont) [Internet] 2014 [cited 2017 Dec 4] 21 e573ndashe603Available from httpwwwncbinlmnihgovpubmed25089109
90 Zhu W Chen W Bortezomib-based treatment for multiple myelomapatients with renal impairment a systematic review and meta-analysis ofobservational studies Medicine [Internet] 2016 95 e5202 Available fromhttpwwwncbinlmnihgovpmcarticlesPMC5120900
91 Dimopoulos MA Terpos E Chanan-Khan A et al Renal impairment inpatients with multiple myeloma a consensus statement on behalf of theInternational Myeloma Working Group JCO 2010 28 4976ndash4984
92 Chauvet S Fremeaux-Bacchi V Petitprez F et al Treatment of B-cell disor-der improves renal outcome of patients with monoclonal gammopathyndashassociated C3 glomerulopathy Blood [Internet] 2017 [cited 2017 Oct 26]129 1437ndash1447 Available from httpwwwncbinlmnihgovpubmed28069603
93 Cohen C Royer B Javaugue V et al Bortezomib produces high hematolog-ical response rates with prolonged renal survival in monoclonal immuno-globulin deposition disease Kidney Int [Internet] 2015 [cited 2017 Dec25] 88 1135ndash1143 Available from httpwwwncbinlmnihgovpubmed26176826
94 Ziogas DC Kastritis E Terpos E et al Hematologic and renal improve-ment of monoclonal immunoglobulin deposition disease after treatmentwith bortezomib-based regimens Leuk Lymphoma [Internet] 2017 [cited2017 Dec 25] 58 1832ndash1839 Available from httpwwwncbinlmnihgovpubmed27967286
95 Milani P Merlini G Palladini G Novel therapies in light chain amyloid-osis Kidney Int Rep [Internet] 2018 [cited 2018 Jul 4] 3 530ndash541 Availablefrom httpwwwncbinlmnihgovpubmed29854961
96 Spizzo G Mitterer M Gunsilius E Bortezomib for the treatment of refrac-tory Type-1 cryoglobulinaemia Br J Haematol [Internet] 2010 [cited 2018Jul 7] 150 235ndash237 Available from httpdoiwileycom101111j1365-2141201008184x
97 Talamo G Claxton D Tricot G et al Response to bortezomib in refractoryType I cryoglobulinemia Am J Hematol 2008 [cited 2018 Jul 7] 83883ndash884 Available from httpwwwncbinlmnihgovpubmed18756542
98 Dimopoulos MA Roussou M Gavriatopoulou M et al Cardiac and renalcomplications of carfilzomib in patients with multiple myeloma BloodAdv 2017 [cited 2017 Dec 6] 1 449ndash454 Available from httpwwwbloodadvancesorglookupdoi101182bloodadvances2016003269
99 Strati P Nasr SH Leung N et al Renal complications in chronic lympho-cytic leukemia and monoclonal B-cell lymphocytosis the Mayo Clinic ex-perience Haematologica [Internet] 2015 [cited 2018 Jul 3] 100 1180ndash1188Available from httpwwwncbinlmnihgovpubmed26088927
100 Salama AD Pusey CD Drug insight rituximab in renal disease and trans-plantation Nat Clin Pract Nephrol [Internet] 2006 [cited 2017 Dec 8] 2221ndash230 Available from httpwwwnaturecomdoifinder101038ncpneph0133
101 Jillella AP Dainer PM Kallab AM et al Treatment of a patient with end-stage renal disease with rituximab pharmacokinetic evaluation suggestsrituximab is not eliminated by hemodialysis Am J Hematol 2002 [cited2018 Jul] 71 219ndash222 Available from httpwwwncbinlmnihgovpubmed12410580
102 Guiard E Karras A Plaisier E et al Patterns of noncryoglobulinemic glo-merulonephritis with monoclonal Ig deposits correlation with IgG sub-class and response to rituximab Clin J Am Soc Nephrol 2011 6 1609ndash1616
103 Ribes D Hachem HEL Oberic L et al Bendamustine plus rituximab forindolent B-cell lymphoma of renal significance Am J Hematol 2018 93356ndash362
104 Darwish M Bond M Hellriegel E et al Pharmacokinetic and pharmacody-namic profile of bendamustine and its metabolites Cancer ChemotherPharmacol 2015 [cited 2017 Dec 15] 75 1143ndash1154 Available from httpwwwncbinlmnihgovpubmed25829094
105 Ponisch W Moll B Bourgeois M et al Bendamustine and prednisone incombination with bortezomib (BPV) in the treatment of patients with re-lapsed or refractory multiple myeloma and light chain-induced renal fail-ure J Cancer Res Clin Oncol [Internet] 2013 [cited 2018 Jul 2] 1391937ndash1946 Available from httpwwwncbinlmnihgovpubmed24046251
106 Mateos M-V Dimopoulos MA Cavo M et al Daratumumab plus bortezo-mib melphalan and prednisone for untreated myeloma N Engl J Med2018 378 518ndash528
107 Rocchi S Tacchetti P Pantani L et al Safety and efficacy of daratumumabin dialysis-dependent renal failure secondary to multiple myelomaHaematologica [Internet] 2018 [cited 2018 Jul 2] 103 e277ndashe278 Availablefrom httpwwwncbinlmnihgovpubmed29622654
12 K Batko et alDownloaded from httpsacademicoupcomndtadvance-article-abstractdoi101093ndtgfy2595086133by gueston 29 August 2018
108 Anand S Miller D Chipman G Morris D Srinivas S Daratumumab forsevere refractory proliferative glomerulonephritis with monoclonal im-mune deposits (PGNMID) ATC Abstr [Internet] 2017 [cited 2018 Jul 3]Available from httpsatcmeetingabstractscomabstractdaratumumab-for-severe-refractory-proliferative-glomerulonephritis-with-monoclonal-immune-deposits-pgnmid
109 Leung N Lager DJ Gertz MA et al Long-term outcome of renal transplan-tation in light-chain deposition disease Am J Kidney Dis [Internet] 2004[cited 2018 Feb 9] 43 147ndash153 Available from httpwwwncbinlmnihgovpubmed14712438
110 Lorenz EC Sethi S Leung N et al Recurrent membranoproliferative glo-merulonephritis after kidney transplantation Kidney Int [Internet] 2010[cited 2018 Feb 9] 77 721ndash728 Available from httpwwwncbinlmnihgovpubmed20130531
111 Leung N Nasr SH A patient with abnormal kidney function and a mono-clonal light chain in the urine Clin J Am Soc Nephrol 2016 11 1073ndash1082
112 Cibeira MT Sanchorawala V Seldin DC et al Outcome of AL amyloidosisafter high-dose melphalan and autologous stem cell transplantation long-term results in a series of 421 patients Blood [Internet] 2011 [cited 2018Feb 3] 118 4346ndash4352 Available from httpwwwncbinlmnihgovpubmed21828140
113 Gertz MA Lacy MQ Dispenzieri A et al Autologous stem cell transplantfor immunoglobulin light chain amyloidosis a status report LeukLymphoma [Internet] 2010 [cited 2018 Feb 3] 51 2181ndash2187 Availablefrom httpwwwncbinlmnihgovpubmed20958232
114 Leung N Kumar SK Glavey SV et al The impact of dialysis on the survivalof patients with immunoglobulin light chain (AL) amyloidosis undergoingautologous stem cell transplantation Nephrol Dial Transplant 2016 [cited2018 Jul 7] 31 1284ndash1289 Available from httpsacademicoupcomndtarticle-lookupdoi101093ndtgfv328
115 Badros A Barlogie B Siegel E et al Results of autologous stem cell trans-plant in multiple myeloma patients with renal failure Br J Haematol 2001[cited 2018 Jul 7] 114 822ndash829 Available from httpwwwncbinlmnihgovpubmed11564069
116 Soltero L Carbajal H Xu J et al Initial survival data of kidney transplantpatients with pre-transplant monoclonal gammopathy Clin Transplant[Internet] 2012 [cited 2018 Feb 3] 26 300ndash304 Available from httpwwwncbinlmnihgovpubmed22044717
117 Jimenez-Zepeda VH Heilman RL Engel RA et al Monoclonal gammopathyof undetermined significance does not affect outcomes in patients undergoingsolid organ transplants Transplantation [Internet] 2011 [cited 2018 Feb 3]92 570ndash574 Available from httpwwwncbinlmnihgovpubmed21712755
118 Naina HVK Harris S Dispenzieri A et al Long-term follow-up of patientswith monoclonal gammopathy of undetermined significance after kidney
transplantation Am J Nephrol 2012 [cited 2018 Feb] 35 365ndash371Available from httpwwwncbinlmnihgovpubmed22473253
119 Bansal T Garg A Snowden JA et al Defining the role of renal transplanta-tion in the modern management of multiple myeloma and other plasmacell dyscrasias Nephron Clin Pract [Internet] 2012 [cited 2018 Feb 3] 120c228 wwwkargercom
120 Hassoun H Flombaum C DrsquoAgati VD et al High-dose melphalan andauto-SCT in patients with monoclonal Ig deposition disease Bone MarrowTransplant 2008 [cited 2018 Feb 3] 42 405ndash412 Available from httpwwwncbinlmnihgovpubmed18574442
121 Herrmann SMS Gertz MA Stegall MD et al Long-term outcomes ofpatients with light chain amyloidosis (AL) after renal transplantation withor without stem cell transplantation Nephrol Dial Transplant [Internet]2011 [cited 2018 Feb 3] 26 2032ndash2036 Available from httpwwwncbinlmnihgovpubmed21543655
122 Lorenz EC Gertz MA Fervenza FC et al Long-term outcome of autolo-gous stem cell transplantation in light chain deposition disease NephrolDial Transplant [Internet] 2008 [cited 2018 Jul 5] 23 2052ndash2057 Availablefrom httpwwwncbinlmnihgovpubmed18178602
123 Merhi B Patel N Bayliss G et al Proliferative glomerulonephritis withmonoclonal IgG deposits in two kidney allografts successfully treated withrituximab Clin Kidney J [Internet] 2017 [cited 2018 Feb 10] 10 405ndash410Available from httpsacademicoupcomckjarticle-lookupdoi101093ckjsfx001
124 Barbour SJ Beaulieu MC Zalunardo NY et al Proliferative glomerulone-phritis with monoclonal IgG deposits secondary to chronic lymphocyticleukemia Report of two cases Nephrol Dial Transplant [Internet] 2011[cited 2018 Feb 10] 26 2712ndash2714 Available from httpsacademicoupcomndtarticle-lookupdoi101093ndtgfr251
125 Zand L Lorenz EC Cosio FG et al Clinical findings pathology and out-comes of C3GN after kidney transplantation J Am Soc Nephrol [Internet]2014 [cited 2018 Jul 5] 25 1110ndash1117 Available from httpwwwncbinlmnihgovpubmed24357668
126 Alfano G Fontana F Colaci E et al Monoclonal gammopathy of undeter-mined significance after kidney transplantation Transplantation [Internet]2017 [cited 2017 Oct 24] 101 e337ndashe342 Available from httpwwwncbinlmnihgovpubmed28731904
127 Bancu I Ca~nas L Juega FJ et al Outcomes of monoclonal gammopathyof undetermined significance in patients who underwent kidneytransplantation Transplant Proc [Internet] 2015 [cited 2018 Feb 10] 472344ndash2345 Available from httpwwwncbinlmnihgovpubmed26518922
Received 2632018 Editorial decision 1472018
Clinical implication of monoclonal gammopathies 13Downloaded from httpsacademicoupcomndtadvance-article-abstractdoi101093ndtgfy2595086133by gueston 29 August 2018

lt30 mLmin1732 reporting proteasome inhibitorSCT as themost feasible therapeutic choice Achievement of completevery good partial HR was necessary for a RR while RR was anindependent predictor of progression again highlighting theprinciples of MGRS treatment In patients with PGNMID whodo not respond to initial treatment with RTXCYC and ste-roids bortezomib-based treatment may elicit a response [51]Bortezomib-based therapy was effective even in refractory casesof CG Type 1 related to MM [85 96 97]
Carfilzomib is a second-generation proteasome inhibitorDimopoulos et al [98] reported that carfilzomib-based therapyimproved renal outcome in 55 of patients with eGFRlt60 mLmin173 m2 Renal function may initially temporarilydecrease though therapy improves renal function A cardiacrisk profile should be treated with exceptional care Patient pro-file assessment and further studies will determine the use inMGRS
M O N O C L O N A L A N T I B O D I E S
Patients with MGUS treated with RTX and prednisone had im-proved kidney function and decreased proteinuria In patientswith MPGN secondary to indolent clones RTX CYC andprednisone were more effective then RTX with steroidsmono-therapy [99] Therapeutic doses of monoclonal antibodies maybe administered even in renal failure and post-renal allograftsettings [100 101] In seven patients with glomerulonephritiswith monoclonal IgG deposits RTX has been observed withpromising results [five achieved CR two partial response (PR)][102] The added benefit of RTX over classic chemotherapyrelates to a more tolerable profile Treatment of 14 PGNMIDpatients in approaches of clone-directed and empirical therapywithout identifiable discrasia was effective with patients withno detectable clone responding with complete and PSs in allbut two cases Bortezomib-based therapy may be effective innon-responders While empirical treatment is not easily under-taken with clonal detection at 25ndash32 it seems justified con-sidering the rate of response [22 51] However the studypopulation is not robust and the benefitsafety of such an ap-proach is in need of confirmation by larger studiesInterestingly patients with eGFR 20 had similar rates of CRPR to eGFR45 and all patients were free of ESRD in follow-up underscoring the value of a haematological treatment ap-proach in MGRS [51] RTXndashCYCndashDex use in 14 patients withMIg-associated glomerulopathy secondary to indolent non-Hodgkin lymphomas was reported on with 64 achieving CR(Table 1) The antiproteinuric effect of RTX is another benefi-cial aspect A steroid-free regimen of bendamustine and RTXprospectively assessed in indolent B-cell lymphoma of renalsignificance resulted in 85 achieving a haematological CRand 75 a complete RR [103] Patients without RR did notachieve HR Bendamustine is primarily cleared by hydrolysiswith minimal kidney involvement and recently there is sub-stantial evidence suggesting its safety in advanced renal failurethough complete blood counts should be monitored for haema-tological abnormality [104 105] (Table 1) RTX should be con-sidered in patients with IgM-associated MGRS especially when
Tab
le2
AL
base
dre
gim
ens
for
trea
tmen
tof
MG
RS
Dru
gP
atie
nts
and
met
hods
Out
com
esC
oncl
usio
nsR
efer
ence
VC
Dve
rsus
VD
101
pts
AL
amyl
oido
sis
(11
rena
lSta
ge3)
Sim
ilar
HR
(Pfrac14
026
)R
R43
fo
rV
Dve
rsus
41
for
VC
D(Pgt
005
)si
mila
rsu
rviv
al(Pfrac14
045
)H
ighe
rdo
sing
ofD
exan
dC
YC
addi
tion
does
noti
m-
pact
ther
apy
outc
omes
sign
ifica
ntly
Kas
trit
iset
al[
78]
CV
Dve
rsus
CT
D13
9pt
sw
ith
AL
amyl
oido
sis
Hig
her
CR
inC
VD
(40
6ve
rsus
246
)
med
ian
PFS
280
vers
us14
0m
onth
sre
spec
tive
lyFa
stcl
onal
cont
rold
idno
tred
uce
earl
ym
orta
lity
Ven
ner
etal
[79
]
CyB
orD
230
pts
wit
h63
w
ith
rena
linv
olve
men
t60
H
R4
3V
GP
R2
5R
RE
ffica
ciou
sin
pati
ents
wit
hout
card
iac
invo
lvem
ent
sur-
viva
lis
depe
nden
ton
deep
resp
onse
Pal
ladi
niet
al[
80]
DA
RA
Ret
rosp
ecti
vere
view
of25
cons
ecut
ive
AL
pts
HR
in76
C
Rin
36
VG
PR
24
wel
ltol
erat
edev
enin
card
iac
pts
Effi
caci
ous
inhe
avily
pre-
trea
ted
Kau
fman
etal
[81
]
Pom
alid
omid
endashD
ex28
pts
wit
hA
Lam
yloi
dosi
s68
H
Rgt
VG
PR
in29
5
3w
ith
resp
onse
afte
r1
cycl
eA
noth
erch
oice
inre
frac
tory
AL
impr
oves
surv
ival
hae
-m
atol
ogic
alpr
ogre
ssio
npr
edic
tssu
rviv
alP
alla
dini
etal
[82
]
LMD
50A
Lam
yloi
dosi
spt
s62
w
ith
rena
lloa
d(4
inre
nalS
tage
III)
CR
18
VG
PR
32
OR
in48
h
aem
atol
ogic
and
card
iac
toxi
city
4
mor
talit
y1
case
ofac
ute
kidn
eyin
jury
len
alid
omid
edo
seha
sto
bem
onit
ored
and
adju
sted
oth
erw
ise
tole
rabl
ean
def
ficac
ious
Heg
enba
rtet
al[
83]
M-D
ex25
9A
Lam
yloi
dosi
spt
sH
R76
C
R31
in
high
dose
ver
sus
51an
d12
in
atte
nuat
edO
Ron
lyin
pati
ents
wit
hH
R(h
ighe
rin
CR
vers
usV
GP
R)
Pal
ladi
niet
al[
84]
VG
PH
Rv
ery
good
part
ialh
aem
atol
ogic
alre
spon
seE
GC
Ge
piga
lloca
tech
inga
llate
LM
Dl
enal
idom
ide
mel
phal
ande
xam
etha
sone
VC
Db
orte
zom
ibcy
clop
hosp
ham
ide
dexa
met
haso
neM
-Dex
mel
phal
ande
xam
etha
sone
6 K Batko et alDownloaded from httpsacademicoupcomndtadvance-article-abstractdoi101093ndtgfy2595086133by gueston 29 August 2018
Tab
le3
Mon
oclo
nal
gam
mop
athy
inth
ese
ttin
gof
kidn
eytr
ansp
lan
tati
on
Pat
ient
san
dm
etho
dsO
utco
mes
Con
clus
ions
Ref
eren
ce
27LC
PT
pati
ents
trea
ted
wit
hch
emo-
ther
apy
(11
SCT
)9
wit
hno
trea
tmen
tLo
wes
tm
orta
lity
best
HR
sin
SCT
tho
ugh
pati
ents
wer
eyo
unge
ran
dha
dbe
stin
itia
land
final
rena
lfu
ncti
on
Bes
tren
alou
tcom
eco
mpa
red
wit
hch
emot
hera
pyor
notr
eatm
ent
SCT
stab
ilize
dor
impr
oved
rena
lfun
ctio
nSt
okes
etal
[27
]
64M
IDD
pati
ents
16
pts
trea
ted
wit
hSC
T4
Ktx
3re
curr
ence
sin
4K
txpa
tien
tsr
ange
of7ndash
43m
onth
s38
pr
ogre
ssio
nto
ESR
Din
SCT
Hig
hcr
eati
nine
atbi
opsy
isas
soci
ated
wit
hpo
orou
t-co
me
chem
othe
rapy
afte
rre
curr
ence
isin
effic
ient
Nas
ret
al[
24]
49M
IDD
pati
ents
3K
txw
ith
1V
GP
Ran
d2
CR
18
SCT
No
recu
rren
ces
in3
Ktx
pati
ents
allo
graf
trej
ecti
onin
1pa
tien
taft
er3
year
sSC
Tw
assa
fean
dto
lera
ted
but
pati
ents
wer
eyo
unge
rbo
rtez
omib
-bas
edtr
eatm
enth
adsi
mila
rR
Rra
tes
Sust
aine
d
VG
PR
nece
ssar
yfo
rK
txS
CT
ispr
efer
red
CK
Dst
ages
Coh
enet
al[
93]
29M
PG
NK
txpa
tien
ts6
wit
hm
onoc
lona
lpro
tein
(4M
GU
S1
CLL
)23
of
MP
GN
pati
ents
have
mon
oclo
nalp
rote
ins
may
incr
ease
risk
ofre
curr
ence
SC
Tre
solv
edre
curr
ence
pl
asm
aphe
res
aspa
ssiv
em
aint
enan
ce
MP
GN
pati
ents
shou
ldbe
scre
ened
for
mon
oclo
nal
prot
eins
Lore
nzet
al[
110]
6LC
DD
wit
hSC
T1
pati
entd
idno
tsur
vive
SCT
all
othe
rsac
hiev
edH
R
2re
laps
esw
ith
1im
prov
edby
subs
eque
ntch
emot
hera
py
Insu
ffici
ent
resp
onse
toSC
Tm
aybe
anin
dica
tion
for
Ktx
inse
lect
pati
ents
afte
rac
hiev
ing
HR
Lore
nzet
al[
122]
7LC
DD
Ktx
pati
ents
Med
ian
recu
rren
ce2ndash
45m
onth
sfo
r5
pati
ents
sub
se-
quen
t4de
aths
onl
y1
pati
entf
ree
ofre
new
alA
HR
mus
tbe
achi
eved
befo
reat
tem
ptin
gK
txLe
ung
etal
[10
9]
2P
GN
MID
Ktx
pati
ents
(1de
novo
1re
curr
ent)
Impr
ovem
ent
ingr
aftf
unct
ion
and
seru
mcr
eati
nine
in2
year
follo
w-u
pR
TX
can
beef
fect
ive
inbo
thre
curr
enta
ndde
novo
PG
NM
IDpt
sM
erhi
etal
[12
3]
3P
GN
MID
(2C
LL)
Des
pite
RT
Xtr
eatm
entt
here
was
1pr
ogre
ssio
nto
ESR
Dan
don
em
alig
nanc
ypr
ogre
ssio
nR
TX
ther
apy
may
impr
ove
rena
lout
com
esin
shor
tter
mB
arbo
uret
al[
124]
53LC
DD
7K
tx1
6SC
T2
recu
rren
ces
inpa
tien
tsw
itho
utpr
ior
chem
othe
rapy
1
reje
ctio
nof
Ktx
3pa
tien
tsin
CR
ingt
68
year
follo
w-
up1
SCT
-rel
ated
deat
h13
15
achi
eved
CR
SCT
can
besu
cces
sful
even
inC
KD
Stag
e4
how
ever
re
nals
urvi
vali
sst
illw
orse
SC
Tap
pear
sm
ore
safe
than
inA
Lam
yloi
dosi
s
Saye
det
al[
31]
21K
txw
itC
3GN
667
re
curr
ence
ofw
hich
21
asso
ciat
edw
ith
mon
o-cl
onal
gam
mop
athy
rec
urre
nce
earl
ier
(36
mon
thm
e-di
anve
rsus
433
mon
th)
mor
epr
ogre
ssiv
eco
urse
(Pfrac14
NS)
SC
Tim
prov
edki
dney
func
tion
inon
epa
tien
tst
a-bl
egr
aft
in10
-yea
rfo
llow
-up
Mon
oclo
nalg
amm
opat
hypa
tien
tsar
eat
risk
ofan
ear-
lier
and
mor
eag
gres
sive
dise
ase
Zan
det
al[
125]
548
Ktx
pati
ents
Pre
vale
nce
81
52
year
med
ian
toM
GU
Sdi
scov
ery
high
erra
teof
MB
Lhi
stor
yof
infla
mm
ator
yki
dney
dis-
ease
aspr
edic
tive
fact
orn
oas
soci
atio
nw
ith
age
and
gend
ern
oim
pact
ongr
afts
urvi
val
over
alls
urvi
val
in-
cide
nce
ofm
alig
nanc
y
MG
US
pre-
and
post
-tra
nspl
antm
aybe
diff
eren
tcon
di-
tion
sin
term
sof
man
agem
ent
how
ever
str
ict
follo
w-u
pis
need
ede
spec
ially
inM
BL
pati
ents
Alfa
noet
al[
126]
159
3K
txre
cipi
ents
3pr
e-tr
ansp
lant
MG
(nfrac14
34)
No
case
sof
prog
ress
ion
noas
soci
atio
nw
ith
mal
igna
ncy
inci
denc
eor
mor
talit
yJi
men
ezZ
eped
aet
al[
117]
587
Ktx
reci
pien
ts2
9in
cide
nce
(9pt
spr
e-tr
ansp
lant
8po
st)
No
prog
ress
ion
duri
ng6-
year
follo
w-u
pM
GU
Sno
taco
ntra
indi
cati
onto
Ktx
Ban
cuet
al[
127]
351
8K
txre
cipi
ents
42pa
tien
ts(2
3pr
e-tr
ansp
lant
19
post
)m
edia
nsu
rviv
al26
1ve
rsus
280
year
sre
spec
tive
ly4
haem
atol
ogic
alm
a-lig
nanc
ies
deve
lope
din
pre
2P
TLD
gt15
year
spo
st-
tran
spla
nt
Dia
gnos
isof
PT
LDw
assy
mpt
om-b
ased
tru
ein
cide
nce
may
behi
gher
exc
lusi
onof
asso
ciat
edki
dney
dise
ase
and
mal
igna
ncy
isne
cess
ary
befo
reK
tx
Nai
naet
al[
118]
MB
Lm
onoc
lona
lB-c
elll
ymph
ocyt
osis
Clinical implication of monoclonal gammopathies 7Downloaded from httpsacademicoupcomndtadvance-article-abstractdoi101093ndtgfy2595086133by gueston 29 August 2018
CD20thorn cells can be identified while non-IgM-associated dis-eases more often require MM-like treatment
Recently an anti CD38 monoclonal antibody daratumumab(DARA) has been approved for the treatment of newly diag-nosed and relapsed MM patients [106] Like many Phase 3 reg-istration trials the study excluded patients with CrCl 20 mLmin Anecdotal evidence of safety and reduction of dialysis fre-quency in a patient with DARA monotherapy has recently beenreported [107] A case of PGNMID refractory to RTX and
bortezomib was successfully treated with DARA [108] Due toindependence of kidney clearance and positive results in RI itmay prove beneficial in MGRS There is an on-going Phase 2study of DARA in MGRS [NCT03095118]
M G R S T R A N S P L A N T A N D E S R D
Renal transplant in MGRS is controversial as frequent recur-rences are observed when the abnormal clone is not adequately
FIGURE 1 Diagnostic and therapeutic algorithm of monoclonal gammopathy of renal significance
8 K Batko et alDownloaded from httpsacademicoupcomndtadvance-article-abstractdoi101093ndtgfy2595086133by gueston 29 August 2018
suppressed [24 109 110] The current treatment paradigm inMGRS is to achieve a complete HR as a means of improvingpost-transplant outcome and preventing recurrence [71 72111] Cibeira et al [112] report that in 340 AL amyloidosispatients subject to SCT 43 attained CR improving long-termOS and organ response (OR) In recent years the treatment-re-lated mortality (TRM) has decreased from 138 between 1994and 2003 to 56 between 2004 and 2008 In part this probablyreflects the experience of established centres however with ac-cess to novel agents there are other options for treatmentCardiac involvement should be screened for in LCDD due to ahigh TRM (23) with SCT as opposed to non-cardiac patients[32] PS does not indicate treatment failure and significantlyincreases survival compared with patients lacking response[113]
A study in AL amyloidosis patients associated the need fordialysis within 30 days of SCT with highest early death risk andTRM Patients with both eGFRlt40 mLmin173 m2 and se-rum albumin lt25 mgdL had a 438 and 281 risk of requir-ing dialysis and chance of TRM respectively Identifying andscreening for such risk factors should improve the feasibility ofSCT in MGRS conditions [114] In a study of 36 patients withAL amyloidosisMIDD who were dialysis dependent for ESRDCR was reached in 53 at 1 year post SCT with an 8 TRM[72] Achievement of dialysis independence was possible inpatients receiving a Ktx after successful SCT Similarly a studyin MM with RI found no impact on survival for patients whowere dialysis dependent [115] Further research is required toevaluate risk factors and establish whether select ESRD patientsmay benefit from SCT
Literature reports are conflicting on the approach to Ktx inMGUS [116ndash118] Bansal et al [119] reflect that a select groupof plasma dyscrasia patients should be considered for Ktx espe-cially those subject to dialysis-associated complications In ALand MIDD patients achieving haematological CR have beenreported with successful Ktx [120 121] Monoclonal gammop-athy in the setting of Ktxs is presented in Table 3 In summaryprimary disease activity organ function and patient perfor-mance should dictate selection for Ktx We propose an algo-rithm for diagnostic and therapeutic treatment of MGRS(Figure 1)
C O N C L U S I O N
With under-recognition of the wide spectrum of MGRS accu-rate classification evidence-based therapy and expert estab-lished management is required Renal involvement in MGRSresults from the direct deposition of monoclonal protein and itslight- or heavy-chain fragments in the kidney IFE microscopyis essential to identify the offending monoclonal protein and itsrenal tissue distribution In selected cases MS is of valueMGRS therapy is directed to eliminate the clonal plasma cell orB-cell population Adverse events particular to the chosen drugshould complement the patient profile Early detection diagno-sis and chemotherapy may improve kidney function It shouldbe stressed that both the renal pathology and the underlyinghaematological disorders influence the management and
prognosis of MGRS Upon achieving HR ASCT and Ktx shouldbe considered as therapy endpoints in MGRS
C O N F L I C T O F I N T E R E S T S T A T E M E N T
None declared
R E F E R E N C E S
1 Kyle RA Monoclonal gammopathy of undetermined significance NaturalHistory in 241 Cases Am J Med [Internet] 1978 [cited 2017 Oct 24] 64814ndash826 Available from httpwwwncbinlmnihgovpubmed645746
2 Leung N Bridoux F Hutchison CA et al Monoclonal gammopathy of re-nal significance when MGUS is no longer undetermined or insignificantBlood [Internet] 2012 [cited 2017 Oct 24] 120 4292ndash4295 Available fromhttpwwwncbinlmnihgovpubmed23047823
3 Kyle RA Therneau TM Rajkumar SV et al Prevalence of monoclonalgammopathy of undetermined significance N Engl J Med [Internet] 2006[cited 2017 Oct 24] 354 1362ndash1369 Available from httpwwwncbinlmnihgovpubmed16571879
4 Landgren O Graubard BI Kumar S et al Prevalence of myeloma precur-sor state monoclonal gammopathy of undetermined significance in 12372individuals 10ndash49 years old a population-based study from the NationalHealth and Nutrition Examination Survey Blood Cancer J 2017 7 e618[cited 2018 Feb 9] 7 Available from httpwwwncbinlmnihgovpubmed29053158
5 Landgren O Graubard BI Katzmann JA et al Racial disparities in theprevalence of monoclonal gammopathies a population-based study of12 482 persons from the National Health and Nutritional ExaminationSurvey Leukemia [Internet] 2014 28 1537ndash1542 [cited 2018 Jun 22]Available from httpwwwncbinlmnihgovpubmed24441287
6 Cabrera Q Macro M Hebert B et al Epidemiology of monoclonal gamm-opathy of undetermined significance (MGUS) the experience from thespecialized registry of hematologic malignancies of Basse-Normandie(France) Cancer Epidemiol [Internet] 2014 38 354ndash356 [cited 2017 Oct24] Available from httpwwwncbinlmnihgovpubmed24880205
7 Therneau TM Kyle RA Melton LJ et al Incidence of monoclonal gamm-opathy of undetermined significance and estimation of duration beforefirst clinical recognition Mayo Clin Proc [Internet] 2012 [cited 2017 Dec23] 87 1071ndash1079 Available from httpwwwncbinlmnihgovpubmed22883742
8 Kyle RA Larson DR Therneau TM et al Long-term follow-up of mono-clonal gammopathy of undetermined significance N Engl J Med 2018[cited 2018 Apr 23] 378 241ndash249 Available from httpwwwncbinlmnihgovpubmed29342381
9 Dispenzieri A Katzmann JA Kyle RA et al Prevalence and risk of progres-sion of light-chain monoclonal gammopathy of undetermined significancea retrospective population-based cohort study Lancet [Internet] 2010[cited 2018 Feb 9] 375 1721ndash1728 Available from httpwwwncbinlmnihgovpubmed20472173
10 Steiner N Gobel G Suchecki P et al Monoclonal gammopathy of renalsignificance (MGRS) increases the risk for progression to multiple mye-loma an observational study of 2935 MGUS patients Oncotarget[Internet] 2018 [cited 2018 Apr 27] 9 2344ndash2356 Available from httpwwwncbinlmnihgovpubmed29416776
11 Dhodapkar MV Sexton R Waheed S et al Clinical genomic andimaging predictors of myeloma progression from asymptomaticmonoclonal gammopathies (SWOG S0120) Blood [Internet] 2014[cited 2018 Jun 22] 123 78ndash85 Available from httpwwwncbinlmnihgovpubmed24144643
12 Zand L Kattah A Fervenza FC et al C3 glomerulonephritis associatedwith monoclonal gammopathy a case series Am J Kidney Dis [Internet]2013 [cited 2017 Dec 29] 62 506ndash514 Available from httpwwwncbinlmnihgovpubmed23623956
13 Rajkumar SV Dimopoulos MA Palumbo A et al International MyelomaWorking Group updated criteria for the diagnosis of multiple myelomaLancet Oncol [Internet] 2014 [cited 2018 Jun 23] 15 e538ndashe548 Availablefrom httplinkinghubelseviercomretrievepiiS1470204514704425
Clinical implication of monoclonal gammopathies 9Downloaded from httpsacademicoupcomndtadvance-article-abstractdoi101093ndtgfy2595086133by gueston 29 August 2018
14 Ravindran A Bartley AC Holton SJ et al Prevalence incidence and sur-vival of smoldering multiple myeloma in the United States Nat PublishingGroup [Internet] 2016 6 2018ndash2023 [cited Jun] Available from httpswwwncbinlmnihgovpmcarticlesPMC5098258pdfbcj2016100apdf
15 Fermand J-P Bridoux F Kyle RA et al How I treat monoclonal gammop-athy of renal significance (MGRS) Blood [Internet] 2013 [cited 2017 Oct27] 122 3583ndash3590 Available from httpwwwncbinlmnihgovpubmed24108460
16 Bridoux F Leung N Hutchison CA et al Diagnosis of monoclonal gamm-opathy of renal significance Kidney Int [Internet] 2015 [cited 2017 Oct24] 87 698ndash711 Available from httpwwwncbinlmnihgovpubmed25607108
17 Kristinsson SY Bjorkholm M Andersson TM-L et al Patterns of survivaland causes of death following a diagnosis of monoclonal gammopathy ofundetermined significance a population-based study Haematologica[Internet] 2009 [cited 2018 Feb] 94 1714ndash1720 Available from httpwwwncbinlmnihgovpubmed19608666
18 Dimopoulos MA Delimpasi S Katodritou E et al Significant improve-ment in the survival of patients with multiple myeloma presenting with se-vere renal impairment after the introduction of novel agents Ann Oncol[Internet] 2014 [cited 2018 Apr 23] 25 195ndash200 Available from httpsacademicoupcomannoncarticle-lookupdoi101093annoncmdt483
19 Correia SO Santos S Malheiro J et al Monoclonal gammopathy of renalsignificance diagnostic workup WJN 2017 [cited 2017 Oct 27] 6 72ndash78Available from httpwwwncbinlmnihgovpubmed28316940
20 Lin J Markowitz GS Valeri AM et al Renal monoclonal immunoglobulindeposition disease the disease spectrum J Am Soc Nephrol [Internet] 2001[cited 2018 Jun 23] 12 1482ndash1492 Available from httpwwwncbinlmnihgovpubmed11423577
21 Sethi S Zand L Leung N et al Membranoproliferative glomerulonephritissecondary to monoclonal gammopathy Clin J Am Soc Nephrol [Internet]2010 [cited 2017 Dec 8] 5 770ndash782 Available from httpwwwncbinlmnihgovpubmed20185597
22 Bhutani G Nasr SH Said SM et al Hematologic characteristics of prolifer-ative glomerulonephritides with nonorganized monoclonal immunoglobu-lin deposits Mayo Clin Proc [Internet] 2015 [cited 2018 Jun 23] 90587ndash596 Available from httpwwwncbinlmnihgovpubmed25939936
23 Cohen C El-Karoui K Alyanakian M-A et al Light and heavy chain depo-sition disease associated with CH1 deletion Clin Kidney J [Internet] 2015[cited 2017 Oct 26] 8 237ndash239 Available from httpwwwncbinlmnihgovpubmed25815184
24 Nasr SH Valeri AM Cornell LD et al Renal monoclonal immunoglobulindeposition disease a report of 64 patients from a single institution Clin JAm Soc Nephrol [Internet] 2012 [cited 2018 Feb 9] 7 231ndash239 Availablefrom httpwwwncbinlmnihgovpubmed22156754
25 Sicard A Karras A Goujon J-M et al Light chain deposition disease with-out glomerular proteinuria a diagnostic challenge for the nephrologistNephrol Dial Transplant [Internet] 2014 [cited 2018 Jul 7] 29 1894ndash1902Available from httpwwwncbinlmnihgovpubmed24619059
26 Haas M A reevaluation of routine electron microscopy in the examinationof native renal biopsies J Am Soc Nephrol [Internet] 1997 8 70ndash76Available from httpwwwncbinlmnihgovpubmed9013450
27 Stokes MB Valeri AM Herlitz L et al Light chain proximal tubulopathyclinical and pathologic characteristics in the modern treatment era J AmSoc Nephrol [Internet] 2016 [cited 2018 Jun 23] 27 1555ndash1565 Availablefrom httpwwwncbinlmnihgovpubmed26374607
28 Larsen CP Messias NC Walker PD et al Membranoproliferative glomeru-lonephritis with masked monotypic immunoglobulin deposits Kidney Int[Internet] 2015 [cited 2018 Feb 10] 88 867ndash873 Available from httpwwwncbinlmnihgovpubmed26154922
29 Eirin A Irazabal MV Gertz MA et al Clinical features of patients with im-munoglobulin light chain amyloidosis (AL) with vascular-limited deposi-tion in the kidney Nephrol Dial Transplant [Internet] 2012 [cited 2018Feb 10] 27 1097ndash1101 Available from httpwwwncbinlmnihgovpubmed22067518
30 Alonso-Titos J Perea-Ortega L Sola E et al C3 glomerulonephritis associ-ated with monoclonal gammopathy of renal significance case report BMCNephrol 2018 Jul 6] 19 129 Available from httpwwwncbinlmnihgovpubmed29884135
31 Sayed RH Wechalekar AD Gilbertson JA et al Natural history and out-come of light chain deposition disease Blood [Internet] 2015 [cited 2017Dec 8] 126 2805ndash2810 Available from httpwwwncbinlmnihgovpubmed26392598
32 Mohan M Buros A Mathur P et al Clinical characteristics and prognosticfactors in multiple myeloma patients with light chain deposition diseaseAm J Hematol 2017 [cited 2018 Jul 7] 92 739ndash745 Available from httpwwwncbinlmnihgovpubmed28383130
33 Vignon M Cohen C Faguer S et al The clinicopathologic characteristicsof kidney diseases related to monotypic IgA deposits Kidney Int [Internet]2017 [cited 2018 Jul] 91 720ndash728 Available from httpwwwncbinlmnihgovpubmed28069266
34 Best Rocha A Larsen CP Membranous glomerulopathy with light chain-restricted deposits a clinicopathological analysis of 28 cases Kidney IntRep [Internet] 2017 [cited 2018 Jul 6] 2 1141ndash1148 Available from httpwwwncbinlmnihgovpubmed29270522
35 Nasr SH Valeri AM Sethi S et al Clinicopathologic correlations in multi-ple myeloma a case series of 190 patients with kidney biopsies Am JKidney Dis [Internet] 2012 [cited 2017 Oct 26] 59 786ndash794 Availablefrom httpwwwncbinlmnihgovpubmed22417785
36 Glavey SV Leung N Monoclonal gammopathy the good the bad and theugly Blood Rev [Internet] 2016 [cited 2017 Dec 24] 30 223ndash231 Availablefrom httpwwwsciencedirectcomsciencearticlepiiS0268960X15000946bb0130
37 Katzmann JA Kyle RA Benson J et al Screening panels for detection ofmonoclonal gammopathies Clin Chem [Internet] 2009 [cited 2017 Oct25] 55 1517ndash1522 Available from httpwwwncbinlmnihgovpubmed19520758
38 Yadav P Leung N Sanders PW et al The use of immunoglobulin lightchain assays in the diagnosis of paraprotein-related kidney disease KidneyInt [Internet] 2015 [cited 2018 Feb 9] 87 692ndash697 Available from httpwwwncbinlmnihgovpubmed25296094
39 Sugihara H Chihara D Seike K et al Percentage of urinary albumin excre-tion and serum-free light-chain reduction are important determinants ofrenal response in myeloma patients with moderate to severe renal impair-ment Blood Cancer J [Internet] 2014 [cited 2018 Jun 24] 4 e235 Availablefrom httpwwwncbinlmnihgovpubmed25083819
40 Leung N Gertz M Kyle RA et al Urinary albumin excretion patterns ofpatients with cast nephropathy and other monoclonal gammopathy-related kidney diseases Clin J Am Soc Nephrol [Internet] 2012 [cited 2018Jun 24] 7 1964ndash1968 Available from httpwwwncbinlmnihgovpubmed23024162
41 Ciocchini M Arbelbide J Musso CG Monoclonal gammopathy of renalsignificance (MGRS) the characteristics and significance of a new meta-entity Int Urol Nephrol [Internet] 2017 [cited 2017 Oct 26] 492171ndash2175 Available from httpwwwncbinlmnihgovpubmed28425076
42 Sethi S Rajkumar SV DrsquoAgati VD The complexity and heterogeneity ofmonoclonal immunoglobulinndashassociated renal diseases J Am Soc Nephrol2018 29 1810ndash1823
43 Hutchison CA Harding S Hewins P et al Quantitative assessment of se-rum and urinary polyclonal free light chains in patients with chronic kid-ney disease Clin J Am Soc Nephrol [Internet] 2008 [cited 2017 Dec 25] 31684ndash1690 Available from httpwwwncbinlmnihgovpubmed18945993
44 Jurczyszyn A Ochrem B Abnormal serum free light chain ratio does notalways indicate monoclonal gammopathy Polskie Archiwum MedycynyWewnetrznej [Internet] 2015 [cited 2017 Dec 29] 125 502ndash504 Availablefrom httpwwwncbinlmnihgovpubmed26266682
45 Singh G Serum free light chain assay and jk ratio performance inpatients with monoclonal gammopathy-high false negative rate for jk ra-tio J Clin Med Res 2017 [cited 2018 Jun 25] 9 46ndash57 Available fromhttpwwwncbinlmnihgovpubmed27924175
46 Fulton RB Fernando SL Serum free light chain assay reduces the need forserum and urine immunofixation electrophoresis in the evaluation ofmonoclonal gammopathy Ann Clin Biochem [Internet] 2009 [cited 2018Jun 25] 46 407ndash412 Available from httpwwwncbinlmnihgovpubmed19641008
10 K Batko et alDownloaded from httpsacademicoupcomndtadvance-article-abstractdoi101093ndtgfy2595086133by gueston 29 August 2018
47 Levinson SS Urine immunofixation electrophoresis remains importantand is complementary to serum free light chain Clin Chem Lab Med[Internet] 2011 [cited 2018 Jun 25] 49 1801ndash1804 Available from httpwwwncbinlmnihgovpubmed21663562 [CrossRef][Mismatch]
48 Lee WS Singh G Serum free light chains in neoplastic monoclonal gam-mopathies relative under-detection of lambda dominant KappaLambdaratio and underproduction of free lambda light chains as compared tokappa light chains in patients with neoplastic monoclonal gammopathiesJ Clin Med Res 2018 [cited 2018 Jun 25] 10 562ndash569 Available fromhttpwwwncbinlmnihgovpubmed29904440
49 Xu B Tang Y Zhou J et al Disease spectrum of abnormal serum free lightchain ratio and its diagnostic significance Oncotarget [Internet] 2017[cited 2017 Dec 29] 8 82268ndash82279 Available from httpwwwncbinlmnihgovpubmed29137262
50 Koo EH Shin J Jang HR et al Diagnostic performances of M-protein testsaccording to the clinical presentations of kidney disease Eur J Intern Med[Internet] 2016 [cited 2018 Feb 9] 33 88ndash92 Available from httpwwwncbinlmnihgovpubmed27421913
51 Gumber R Cohen JB Palmer MB et al A clone-directed approach mayimprove diagnosis and treatment of proliferative glomerulonephritis withmonoclonal immunoglobulin deposits Kidney Int [Internet] 2018 94199ndash205 Available from httpsdoiorg101016jkint201802020
52 Leung N Barnidge DR Hutchison CA Laboratory testing in monoclonalgammopathy of renal significance (MGRS) Clin Chem Lab Med [Internet]2016 [cited 2017 Oct 25] 54 929ndash937 Available from httpwwwncbinlmnihgovpubmed27107835 [CrossRef][Mismatch]
53 Ramirez-Alvarado M Ward CJ Huang BQ et al Differences in immuno-globulin light chain species found in urinary exosomes in light chain amy-loidosis (AL) PLoS ONE [Internet] 2012 [cited 2018 Jul 7] 7 e38061Available from httpwwwncbinlmnihgovpubmed22723846
54 Hogan JJ Weiss BM Bridging the divide an onco-nephrologic approachto the monoclonal gammopathies of renal significance Clin J Am SocNephrol [Internet] 2016 [cited 2017 Oct 26] 11 1681ndash1691 Availablefrom httpwwwncbinlmnihgovpubmed27416775
55 Vij R Mazumder A Klinger M et al Deep sequencing reveals myelomacells in peripheral blood in majority of multiple myeloma patients ClinLymphoma Myeloma Leuk [Internet] 2014 [cited 2017 Oct 25] 14131ndash139e1 Available from httpwwwncbinlmnihgovpubmed24629890
56 Gonsalves WI Leung N Rajkumar SV et al Improvement in renal func-tion and its impact on survival in patients with newly diagnosed multiplemyeloma Blood Cancer J 2015 [cited 2018 Feb 3] 5 e296 Available fromhttpwwwnaturecomdoifinder101038bcj201520
57 Dimopoulos MA Cheung MC Roussel M et al Impact of renal impair-ment on outcomes with lenalidomide and dexamethasone treatment in theFIRST trial a randomized open-label phase 3 trial in transplant-ineligiblepatients with multiple myeloma Haematologica [Internet] 2016 [cited2018 Jul 7] 101 363ndash370 Available from httpwwwncbinlmnihgovpubmed26659916
58 Ponisch W Andrea M Wagner I et al Successful treatment of patientswith newly diagnoseduntreated multiple myeloma and advanced renalfailure using bortezomib in combination with bendamustine and predni-sone J Cancer Res Clin Oncol 2012 [cited 2018 Jul 2] 138 1405ndash1412Available from httpwwwncbinlmnihgovpubmed22526157
59 Perry M Delarche A Ribes D et al Rituximab-cyclophosphamide-dexa-methasone is highly effective in patients with monoclonal Ig deposit-related glomerulopathy and indolent non-Hodgkin lymphomas Am JHematol 2014 [cited 2018 Jul 1] 89 969ndash973 Available from httpdoiwileycom101002ajh23798
60 Dimopoulos M Weisel K van de Donk Nwcj et al Pomalidomide pluslow-dose dexamethasone in patients with relapsedrefractory multiple my-eloma and renal impairment results from a Phase II trial J Clin Oncol2018 36 2035ndash2043
61 Fervenza FC Canetta PA Barbour SJ et al A multicenter randomized con-trolled trial of rituximab versus cyclosporine in the treatment of idiopathicmembranous nephropathy (MENTOR) Nephron [Internet] 2015 [cited2017 Dec 25] 130 159ndash168 Available from httpwwwncbinlmnihgovpubmed26087670
62 Dimopoulos MA Richardson PG Schlag R et al VMP (bortezomib mel-phalan and prednisone) is active and well tolerated in newly diagnosedpatients with multiple myeloma with moderately impaired renal functionand results in reversal of renal impairment cohort analysis of the Phase IIIVISTA study JCO 2009 [cited 2017 Dec 8] 27 6086ndash6093 Available fromhttpwwwncbinlmnihgovpubmed19858394
63 Morabito F Gentile M Mazzone C et al Safety and efficacy ofbortezomib-melphalan-prednisone-thalidomide followed by bortezomib-thalidomide maintenance (VMPT-VT) versus bortezomib-melphalan-prednisone (VMP) in untreated multiple myeloma patients with renal im-pairment Blood [Internet] 2011 [cited 2017 Dec 9] 118 5759ndash5766Available from httpwwwncbinlmnihgovpubmed21951682
64 Moreau P Masszi T Grzasko N et al Oral ixazomib lenalidomide anddexamethasone for multiple myeloma N Engl J Med 2016 [cited 2018 Apr27] 374 1621ndash1634 Available from httpwwwnejmorgdoi101056NEJMoa1516282
65 Nordstrom BL Knopf KB Teltsch DY et al The safety of bendamustine inpatients with chronic lymphocytic leukemia or non-Hodgkin lymphomaand concomitant renal impairment a retrospective electronic medical re-cord database analysis Leuk Lymphoma [Internet] 2014 [cited 2017 Dec13] 55 1266ndash1273 Available from httpwwwncbinlmnihgovpubmed23987821
66 Roussou M Kastritis E Christoulas D et al Reversibility of renal failure innewly diagnosed patients with multiple myeloma and the role of novelagents Leuk Res [Internet] 2010 [cited 2017 Dec 15] 34 1395ndash1397Available from httpwwwncbinlmnihgovpubmed20510452
67 Tosi P Zamagni E Tacchetti P et al Thalidomide-dexamethasone as in-duction therapy before autologous stem cell transplantation in patientswith newly diagnosed multiple myeloma and renal insufficiency BiolBlood Marrow Transplant [Internet] 2010 [cited 2018 Apr 27] 161115ndash1121 Available from httpwwwncbinlmnihgovpubmed20197100
68 Dimopoulos M Alegre A Stadtmauer EA et al The efficacy and safety oflenalidomide plus dexamethasone in relapsed andor refractory multiplemyeloma patients with impaired renal function Cancer [Internet] 2010116 3807 [cited 2017 Dec 15] Available from httpwwwncbinlmnihgovpubmed20564094
69 Siegel DS Weisel KC Dimopoulos MA et al Pomalidomide plus low-dosedexamethasone in patients with relapsedrefractory multiple myeloma andmoderate renal impairment a pooled analysis of three clinical trials LeukLymphoma [Internet] 2016 [cited 2017 Dec 15] 57 2833ndash2838 Availablefrom httpwwwncbinlmnihgovpubmed27267105
70 Dimopoulos MA Goldschmidt H Niesvizky R et al Carfilzomib or borte-zomib in relapsed or refractory multiple myeloma (ENDEAVOR) an in-terim overall survival analysis of an open-label randomised phase 3 trialLancet Oncol [Internet] 2017 [cited 2017 Dec 6] 18 1327ndash1337 Availablefrom httpwwwncbinlmnihgovpubmed28843768
71 Telio D Shepherd J Forrest D et al High-dose melphalan followed byauto-SCT has favorable safety and efficacy in selected patients with lightchain deposition disease and light and heavy chain deposition diseaseBone Marrow Transplant 2012 [cited 2017 Dec 8] 47 453ndash455 Availablefrom httpwwwnaturecomdoifinder101038bmt201187
72 Batalini F Econimo L Quillen K et al High-dose melphalan and stem celltransplantation in patients on dialysis due to immunoglobulin light-chainamyloidosis and monoclonal immunoglobulin deposition disease BiolBlood Marrow Transplant [Internet] 2018 [cited 2017 Dec 25] 24127ndash132 Available from httpwwwncbinlmnihgovpubmed28865972
73 Kourelis TV Nasr SH Dispenzieri A et al Outcomes of patients with renalmonoclonal immunoglobulin deposition disease Am J Hematol 2016[cited 2018 Jul 2] 91 1123ndash1128 Available from httpwwwncbinlmnihgovpubmed27501122
74 Pozzi C DrsquoAmico M Fogazzi GB et al Light chain deposition disease withrenal involvement clinical characteristics and prognostic factors Am JKidney Dis [Internet] 2003 [cited 2018 Jun 23] 42 1154ndash1163 Availablefrom httpwwwncbinlmnihgovpubmed14655186
75 Song M-K Chung J-S Shin H-J et al Cyclophosphamide-containing regi-men (TCD) is superior to melphalan-containing regimen (MPT) in elderlymultiple myeloma patients with renal impairment Ann Hematol
Clinical implication of monoclonal gammopathies 11Downloaded from httpsacademicoupcomndtadvance-article-abstractdoi101093ndtgfy2595086133by gueston 29 August 2018
[Internet] 2012 [cited 2017 Dec 9] 91 889ndash896 Available from httpwwwncbinlmnihgovpubmed22237937
76 Specter R Sanchorawala V Seldin DC et al Kidney dysfunction duringlenalidomide treatment for AL amyloidosis Nephrol Dial Transplant[Internet] 2011 [cited 2018 Jul 7] 26 881ndash886 Available from httpwwwncbinlmnihgovpubmed20693160
77 Li Y Wang X OrsquoMara E et al Population pharmacokinetics of pomalido-mide in patients with relapsed or refractory multiple myeloma with variousdegrees of impaired renal function CPAA 2017 [cited 2018 Feb 4] 9133ndash145 Available from httpwwwncbinlmnihgovpubmed29184451
78 Kastritis E Gavriatopoulou M Roussou M et al Addition of cyclophos-phamide and higher doses of dexamethasone do not improve outcomes ofpatients with AL amyloidosis treated with bortezomib Blood Cancer J2017 [cited 2017 Dec 15] 7 e570 Available from httpwwwncbinlmnihgovpubmed28622303
79 Venner CP Gillmore JD Sachchithanantham S et al A matched compari-son of cyclophosphamide bortezomib and dexamethasone (CVD) versusrisk-adapted cyclophosphamide thalidomide and dexamethasone (CTD)in AL amyloidosis Leukemia [Internet] 2014 [cited 2018 Jul 5] 282304ndash2310 Available from httpwwwncbinlmnihgovpubmed25027514
80 Palladini G Sachchithanantham S Milani P et al A European collabora-tive study of cyclophosphamide bortezomib and dexamethasone inupfront treatment of systemic AL amyloidosis Blood [Internet] 2015[cited 2017 Dec 9] 126 612ndash615 Available from httpwwwncbinlmnihgovpubmed25987656
81 Kopel T Kaufman JS Hamburg N et al Endothelium-dependent and -in-dependent vascular function in advanced chronic kidney disease CJASN2017 [cited 2018 Apr 18] 12 1588ndash1594 Available from httpcjasnasnjournalsorglookupdoi102215CJN12811216
82 Palladini G Milani P Foli A et al A Phase 2 trial of pomalidomide anddexamethasone rescue treatment in patients with AL amyloidosis Blood[Internet] 2017 [cited 2018 Apr 26] 129 2120ndash2123 Available fromhttpwwwncbinlmnihgovpubmed28130212
83 Hegenbart U Bochtler T Benner A et al Lenalidomidemelphalandexa-methasone in newly diagnosed patients with immunoglobulin light chainamyloidosis results of a prospective phase 2 study with long-term followup Haematologica [Internet] 2017 [cited 2017 Dec 26] 102 1424ndash1431Available from httpwwwncbinlmnihgovpubmed28522573
84 Palladini G Milani P Foli A et al Oral melphalan and dexamethasonegrants extended survival with minimal toxicity in AL amyloidosis long-term results of a risk-adapted approach Haematologica [Internet] 2014[cited 2017 Dec 15] 99 743ndash750 Available from httpwwwncbinlmnihgovpubmed24213149
85 Payet J Livartowski J Kavian N et al Type I cryoglobulinemia in multiplemyeloma a rare entity analysis of clinical and biological characteristics ofseven cases and review of the literature Leuk Lymphoma [Internet] 201354 767ndash777 Available from httpwwwtandfonlinecomdoifull103109104281942012671481
86 Terpos E Kleber M Engelhardt M et al European Myeloma Networkguidelines for the management of multiple myeloma-related complica-tions Haematologica [Internet] 2015 [cited 2017 Dec 4] 100 1254ndash1266Available from httpwwwncbinlmnihgovpubmed26432383
87 Chanan-Khan AA Kaufman JL Mehta J et al Activity and safety of borte-zomib in multiple myeloma patients with advanced renal failure a multi-center retrospective study Blood [Internet] 2007 [cited 2018 Jul 2] 1092604ndash2606 Available from httpwwwncbinlmnihgovpubmed17138816
88 Dimopoulos MA Roussou M Gkotzamanidou M et al The role of novelagents on the reversibility of renal impairment in newly diagnosed symp-tomatic patients with multiple myeloma Leukemia 2013 27 423ndash429
89 Kouroukis TC Baldassarre FG Haynes AE et al Bortezomib in multiplemyeloma systematic review and clinical considerations Curr Oncol(Toronto Ont) [Internet] 2014 [cited 2017 Dec 4] 21 e573ndashe603Available from httpwwwncbinlmnihgovpubmed25089109
90 Zhu W Chen W Bortezomib-based treatment for multiple myelomapatients with renal impairment a systematic review and meta-analysis ofobservational studies Medicine [Internet] 2016 95 e5202 Available fromhttpwwwncbinlmnihgovpmcarticlesPMC5120900
91 Dimopoulos MA Terpos E Chanan-Khan A et al Renal impairment inpatients with multiple myeloma a consensus statement on behalf of theInternational Myeloma Working Group JCO 2010 28 4976ndash4984
92 Chauvet S Fremeaux-Bacchi V Petitprez F et al Treatment of B-cell disor-der improves renal outcome of patients with monoclonal gammopathyndashassociated C3 glomerulopathy Blood [Internet] 2017 [cited 2017 Oct 26]129 1437ndash1447 Available from httpwwwncbinlmnihgovpubmed28069603
93 Cohen C Royer B Javaugue V et al Bortezomib produces high hematolog-ical response rates with prolonged renal survival in monoclonal immuno-globulin deposition disease Kidney Int [Internet] 2015 [cited 2017 Dec25] 88 1135ndash1143 Available from httpwwwncbinlmnihgovpubmed26176826
94 Ziogas DC Kastritis E Terpos E et al Hematologic and renal improve-ment of monoclonal immunoglobulin deposition disease after treatmentwith bortezomib-based regimens Leuk Lymphoma [Internet] 2017 [cited2017 Dec 25] 58 1832ndash1839 Available from httpwwwncbinlmnihgovpubmed27967286
95 Milani P Merlini G Palladini G Novel therapies in light chain amyloid-osis Kidney Int Rep [Internet] 2018 [cited 2018 Jul 4] 3 530ndash541 Availablefrom httpwwwncbinlmnihgovpubmed29854961
96 Spizzo G Mitterer M Gunsilius E Bortezomib for the treatment of refrac-tory Type-1 cryoglobulinaemia Br J Haematol [Internet] 2010 [cited 2018Jul 7] 150 235ndash237 Available from httpdoiwileycom101111j1365-2141201008184x
97 Talamo G Claxton D Tricot G et al Response to bortezomib in refractoryType I cryoglobulinemia Am J Hematol 2008 [cited 2018 Jul 7] 83883ndash884 Available from httpwwwncbinlmnihgovpubmed18756542
98 Dimopoulos MA Roussou M Gavriatopoulou M et al Cardiac and renalcomplications of carfilzomib in patients with multiple myeloma BloodAdv 2017 [cited 2017 Dec 6] 1 449ndash454 Available from httpwwwbloodadvancesorglookupdoi101182bloodadvances2016003269
99 Strati P Nasr SH Leung N et al Renal complications in chronic lympho-cytic leukemia and monoclonal B-cell lymphocytosis the Mayo Clinic ex-perience Haematologica [Internet] 2015 [cited 2018 Jul 3] 100 1180ndash1188Available from httpwwwncbinlmnihgovpubmed26088927
100 Salama AD Pusey CD Drug insight rituximab in renal disease and trans-plantation Nat Clin Pract Nephrol [Internet] 2006 [cited 2017 Dec 8] 2221ndash230 Available from httpwwwnaturecomdoifinder101038ncpneph0133
101 Jillella AP Dainer PM Kallab AM et al Treatment of a patient with end-stage renal disease with rituximab pharmacokinetic evaluation suggestsrituximab is not eliminated by hemodialysis Am J Hematol 2002 [cited2018 Jul] 71 219ndash222 Available from httpwwwncbinlmnihgovpubmed12410580
102 Guiard E Karras A Plaisier E et al Patterns of noncryoglobulinemic glo-merulonephritis with monoclonal Ig deposits correlation with IgG sub-class and response to rituximab Clin J Am Soc Nephrol 2011 6 1609ndash1616
103 Ribes D Hachem HEL Oberic L et al Bendamustine plus rituximab forindolent B-cell lymphoma of renal significance Am J Hematol 2018 93356ndash362
104 Darwish M Bond M Hellriegel E et al Pharmacokinetic and pharmacody-namic profile of bendamustine and its metabolites Cancer ChemotherPharmacol 2015 [cited 2017 Dec 15] 75 1143ndash1154 Available from httpwwwncbinlmnihgovpubmed25829094
105 Ponisch W Moll B Bourgeois M et al Bendamustine and prednisone incombination with bortezomib (BPV) in the treatment of patients with re-lapsed or refractory multiple myeloma and light chain-induced renal fail-ure J Cancer Res Clin Oncol [Internet] 2013 [cited 2018 Jul 2] 1391937ndash1946 Available from httpwwwncbinlmnihgovpubmed24046251
106 Mateos M-V Dimopoulos MA Cavo M et al Daratumumab plus bortezo-mib melphalan and prednisone for untreated myeloma N Engl J Med2018 378 518ndash528
107 Rocchi S Tacchetti P Pantani L et al Safety and efficacy of daratumumabin dialysis-dependent renal failure secondary to multiple myelomaHaematologica [Internet] 2018 [cited 2018 Jul 2] 103 e277ndashe278 Availablefrom httpwwwncbinlmnihgovpubmed29622654
12 K Batko et alDownloaded from httpsacademicoupcomndtadvance-article-abstractdoi101093ndtgfy2595086133by gueston 29 August 2018
108 Anand S Miller D Chipman G Morris D Srinivas S Daratumumab forsevere refractory proliferative glomerulonephritis with monoclonal im-mune deposits (PGNMID) ATC Abstr [Internet] 2017 [cited 2018 Jul 3]Available from httpsatcmeetingabstractscomabstractdaratumumab-for-severe-refractory-proliferative-glomerulonephritis-with-monoclonal-immune-deposits-pgnmid
109 Leung N Lager DJ Gertz MA et al Long-term outcome of renal transplan-tation in light-chain deposition disease Am J Kidney Dis [Internet] 2004[cited 2018 Feb 9] 43 147ndash153 Available from httpwwwncbinlmnihgovpubmed14712438
110 Lorenz EC Sethi S Leung N et al Recurrent membranoproliferative glo-merulonephritis after kidney transplantation Kidney Int [Internet] 2010[cited 2018 Feb 9] 77 721ndash728 Available from httpwwwncbinlmnihgovpubmed20130531
111 Leung N Nasr SH A patient with abnormal kidney function and a mono-clonal light chain in the urine Clin J Am Soc Nephrol 2016 11 1073ndash1082
112 Cibeira MT Sanchorawala V Seldin DC et al Outcome of AL amyloidosisafter high-dose melphalan and autologous stem cell transplantation long-term results in a series of 421 patients Blood [Internet] 2011 [cited 2018Feb 3] 118 4346ndash4352 Available from httpwwwncbinlmnihgovpubmed21828140
113 Gertz MA Lacy MQ Dispenzieri A et al Autologous stem cell transplantfor immunoglobulin light chain amyloidosis a status report LeukLymphoma [Internet] 2010 [cited 2018 Feb 3] 51 2181ndash2187 Availablefrom httpwwwncbinlmnihgovpubmed20958232
114 Leung N Kumar SK Glavey SV et al The impact of dialysis on the survivalof patients with immunoglobulin light chain (AL) amyloidosis undergoingautologous stem cell transplantation Nephrol Dial Transplant 2016 [cited2018 Jul 7] 31 1284ndash1289 Available from httpsacademicoupcomndtarticle-lookupdoi101093ndtgfv328
115 Badros A Barlogie B Siegel E et al Results of autologous stem cell trans-plant in multiple myeloma patients with renal failure Br J Haematol 2001[cited 2018 Jul 7] 114 822ndash829 Available from httpwwwncbinlmnihgovpubmed11564069
116 Soltero L Carbajal H Xu J et al Initial survival data of kidney transplantpatients with pre-transplant monoclonal gammopathy Clin Transplant[Internet] 2012 [cited 2018 Feb 3] 26 300ndash304 Available from httpwwwncbinlmnihgovpubmed22044717
117 Jimenez-Zepeda VH Heilman RL Engel RA et al Monoclonal gammopathyof undetermined significance does not affect outcomes in patients undergoingsolid organ transplants Transplantation [Internet] 2011 [cited 2018 Feb 3]92 570ndash574 Available from httpwwwncbinlmnihgovpubmed21712755
118 Naina HVK Harris S Dispenzieri A et al Long-term follow-up of patientswith monoclonal gammopathy of undetermined significance after kidney
transplantation Am J Nephrol 2012 [cited 2018 Feb] 35 365ndash371Available from httpwwwncbinlmnihgovpubmed22473253
119 Bansal T Garg A Snowden JA et al Defining the role of renal transplanta-tion in the modern management of multiple myeloma and other plasmacell dyscrasias Nephron Clin Pract [Internet] 2012 [cited 2018 Feb 3] 120c228 wwwkargercom
120 Hassoun H Flombaum C DrsquoAgati VD et al High-dose melphalan andauto-SCT in patients with monoclonal Ig deposition disease Bone MarrowTransplant 2008 [cited 2018 Feb 3] 42 405ndash412 Available from httpwwwncbinlmnihgovpubmed18574442
121 Herrmann SMS Gertz MA Stegall MD et al Long-term outcomes ofpatients with light chain amyloidosis (AL) after renal transplantation withor without stem cell transplantation Nephrol Dial Transplant [Internet]2011 [cited 2018 Feb 3] 26 2032ndash2036 Available from httpwwwncbinlmnihgovpubmed21543655
122 Lorenz EC Gertz MA Fervenza FC et al Long-term outcome of autolo-gous stem cell transplantation in light chain deposition disease NephrolDial Transplant [Internet] 2008 [cited 2018 Jul 5] 23 2052ndash2057 Availablefrom httpwwwncbinlmnihgovpubmed18178602
123 Merhi B Patel N Bayliss G et al Proliferative glomerulonephritis withmonoclonal IgG deposits in two kidney allografts successfully treated withrituximab Clin Kidney J [Internet] 2017 [cited 2018 Feb 10] 10 405ndash410Available from httpsacademicoupcomckjarticle-lookupdoi101093ckjsfx001
124 Barbour SJ Beaulieu MC Zalunardo NY et al Proliferative glomerulone-phritis with monoclonal IgG deposits secondary to chronic lymphocyticleukemia Report of two cases Nephrol Dial Transplant [Internet] 2011[cited 2018 Feb 10] 26 2712ndash2714 Available from httpsacademicoupcomndtarticle-lookupdoi101093ndtgfr251
125 Zand L Lorenz EC Cosio FG et al Clinical findings pathology and out-comes of C3GN after kidney transplantation J Am Soc Nephrol [Internet]2014 [cited 2018 Jul 5] 25 1110ndash1117 Available from httpwwwncbinlmnihgovpubmed24357668
126 Alfano G Fontana F Colaci E et al Monoclonal gammopathy of undeter-mined significance after kidney transplantation Transplantation [Internet]2017 [cited 2017 Oct 24] 101 e337ndashe342 Available from httpwwwncbinlmnihgovpubmed28731904
127 Bancu I Ca~nas L Juega FJ et al Outcomes of monoclonal gammopathyof undetermined significance in patients who underwent kidneytransplantation Transplant Proc [Internet] 2015 [cited 2018 Feb 10] 472344ndash2345 Available from httpwwwncbinlmnihgovpubmed26518922
Received 2632018 Editorial decision 1472018
Clinical implication of monoclonal gammopathies 13Downloaded from httpsacademicoupcomndtadvance-article-abstractdoi101093ndtgfy2595086133by gueston 29 August 2018

Tab
le3
Mon
oclo
nal
gam
mop
athy
inth
ese
ttin
gof
kidn
eytr
ansp
lan
tati
on
Pat
ient
san
dm
etho
dsO
utco
mes
Con
clus
ions
Ref
eren
ce
27LC
PT
pati
ents
trea
ted
wit
hch
emo-
ther
apy
(11
SCT
)9
wit
hno
trea
tmen
tLo
wes
tm
orta
lity
best
HR
sin
SCT
tho
ugh
pati
ents
wer
eyo
unge
ran
dha
dbe
stin
itia
land
final
rena
lfu
ncti
on
Bes
tren
alou
tcom
eco
mpa
red
wit
hch
emot
hera
pyor
notr
eatm
ent
SCT
stab
ilize
dor
impr
oved
rena
lfun
ctio
nSt
okes
etal
[27
]
64M
IDD
pati
ents
16
pts
trea
ted
wit
hSC
T4
Ktx
3re
curr
ence
sin
4K
txpa
tien
tsr
ange
of7ndash
43m
onth
s38
pr
ogre
ssio
nto
ESR
Din
SCT
Hig
hcr
eati
nine
atbi
opsy
isas
soci
ated
wit
hpo
orou
t-co
me
chem
othe
rapy
afte
rre
curr
ence
isin
effic
ient
Nas
ret
al[
24]
49M
IDD
pati
ents
3K
txw
ith
1V
GP
Ran
d2
CR
18
SCT
No
recu
rren
ces
in3
Ktx
pati
ents
allo
graf
trej
ecti
onin
1pa
tien
taft
er3
year
sSC
Tw
assa
fean
dto
lera
ted
but
pati
ents
wer
eyo
unge
rbo
rtez
omib
-bas
edtr
eatm
enth
adsi
mila
rR
Rra
tes
Sust
aine
d
VG
PR
nece
ssar
yfo
rK
txS
CT
ispr
efer
red
CK
Dst
ages
Coh
enet
al[
93]
29M
PG
NK
txpa
tien
ts6
wit
hm
onoc
lona
lpro
tein
(4M
GU
S1
CLL
)23
of
MP
GN
pati
ents
have
mon
oclo
nalp
rote
ins
may
incr
ease
risk
ofre
curr
ence
SC
Tre
solv
edre
curr
ence
pl
asm
aphe
res
aspa
ssiv
em
aint
enan
ce
MP
GN
pati
ents
shou
ldbe
scre
ened
for
mon
oclo
nal
prot
eins
Lore
nzet
al[
110]
6LC
DD
wit
hSC
T1
pati
entd
idno
tsur
vive
SCT
all
othe
rsac
hiev
edH
R
2re
laps
esw
ith
1im
prov
edby
subs
eque
ntch
emot
hera
py
Insu
ffici
ent
resp
onse
toSC
Tm
aybe
anin
dica
tion
for
Ktx
inse
lect
pati
ents
afte
rac
hiev
ing
HR
Lore
nzet
al[
122]
7LC
DD
Ktx
pati
ents
Med
ian
recu
rren
ce2ndash
45m
onth
sfo
r5
pati
ents
sub
se-
quen
t4de
aths
onl
y1
pati
entf
ree
ofre
new
alA
HR
mus
tbe
achi
eved
befo
reat
tem
ptin
gK
txLe
ung
etal
[10
9]
2P
GN
MID
Ktx
pati
ents
(1de
novo
1re
curr
ent)
Impr
ovem
ent
ingr
aftf
unct
ion
and
seru
mcr
eati
nine
in2
year
follo
w-u
pR
TX
can
beef
fect
ive
inbo
thre
curr
enta
ndde
novo
PG
NM
IDpt
sM
erhi
etal
[12
3]
3P
GN
MID
(2C
LL)
Des
pite
RT
Xtr
eatm
entt
here
was
1pr
ogre
ssio
nto
ESR
Dan
don
em
alig
nanc
ypr
ogre
ssio
nR
TX
ther
apy
may
impr
ove
rena
lout
com
esin
shor
tter
mB
arbo
uret
al[
124]
53LC
DD
7K
tx1
6SC
T2
recu
rren
ces
inpa
tien
tsw
itho
utpr
ior
chem
othe
rapy
1
reje
ctio
nof
Ktx
3pa
tien
tsin
CR
ingt
68
year
follo
w-
up1
SCT
-rel
ated
deat
h13
15
achi
eved
CR
SCT
can
besu
cces
sful
even
inC
KD
Stag
e4
how
ever
re
nals
urvi
vali
sst
illw
orse
SC
Tap
pear
sm
ore
safe
than
inA
Lam
yloi
dosi
s
Saye
det
al[
31]
21K
txw
itC
3GN
667
re
curr
ence
ofw
hich
21
asso
ciat
edw
ith
mon
o-cl
onal
gam
mop
athy
rec
urre
nce
earl
ier
(36
mon
thm
e-di
anve
rsus
433
mon
th)
mor
epr
ogre
ssiv
eco
urse
(Pfrac14
NS)
SC
Tim
prov
edki
dney
func
tion
inon
epa
tien
tst
a-bl
egr
aft
in10
-yea
rfo
llow
-up
Mon
oclo
nalg
amm
opat
hypa
tien
tsar
eat
risk
ofan
ear-
lier
and
mor
eag
gres
sive
dise
ase
Zan
det
al[
125]
548
Ktx
pati
ents
Pre
vale
nce
81
52
year
med
ian
toM
GU
Sdi
scov
ery
high
erra
teof
MB
Lhi
stor
yof
infla
mm
ator
yki
dney
dis-
ease
aspr
edic
tive
fact
orn
oas
soci
atio
nw
ith
age
and
gend
ern
oim
pact
ongr
afts
urvi
val
over
alls
urvi
val
in-
cide
nce
ofm
alig
nanc
y
MG
US
pre-
and
post
-tra
nspl
antm
aybe
diff
eren
tcon
di-
tion
sin
term
sof
man
agem
ent
how
ever
str
ict
follo
w-u
pis
need
ede
spec
ially
inM
BL
pati
ents
Alfa
noet
al[
126]
159
3K
txre
cipi
ents
3pr
e-tr
ansp
lant
MG
(nfrac14
34)
No
case
sof
prog
ress
ion
noas
soci
atio
nw
ith
mal
igna
ncy
inci
denc
eor
mor
talit
yJi
men
ezZ
eped
aet
al[
117]
587
Ktx
reci
pien
ts2
9in
cide
nce
(9pt
spr
e-tr
ansp
lant
8po
st)
No
prog
ress
ion
duri
ng6-
year
follo
w-u
pM
GU
Sno
taco
ntra
indi
cati
onto
Ktx
Ban
cuet
al[
127]
351
8K
txre
cipi
ents
42pa
tien
ts(2
3pr
e-tr
ansp
lant
19
post
)m
edia
nsu
rviv
al26
1ve
rsus
280
year
sre
spec
tive
ly4
haem
atol
ogic
alm
a-lig
nanc
ies
deve
lope
din
pre
2P
TLD
gt15
year
spo
st-
tran
spla
nt
Dia
gnos
isof
PT
LDw
assy
mpt
om-b
ased
tru
ein
cide
nce
may
behi
gher
exc
lusi
onof
asso
ciat
edki
dney
dise
ase
and
mal
igna
ncy
isne
cess
ary
befo
reK
tx
Nai
naet
al[
118]
MB
Lm
onoc
lona
lB-c
elll
ymph
ocyt
osis
Clinical implication of monoclonal gammopathies 7Downloaded from httpsacademicoupcomndtadvance-article-abstractdoi101093ndtgfy2595086133by gueston 29 August 2018
CD20thorn cells can be identified while non-IgM-associated dis-eases more often require MM-like treatment
Recently an anti CD38 monoclonal antibody daratumumab(DARA) has been approved for the treatment of newly diag-nosed and relapsed MM patients [106] Like many Phase 3 reg-istration trials the study excluded patients with CrCl 20 mLmin Anecdotal evidence of safety and reduction of dialysis fre-quency in a patient with DARA monotherapy has recently beenreported [107] A case of PGNMID refractory to RTX and
bortezomib was successfully treated with DARA [108] Due toindependence of kidney clearance and positive results in RI itmay prove beneficial in MGRS There is an on-going Phase 2study of DARA in MGRS [NCT03095118]
M G R S T R A N S P L A N T A N D E S R D
Renal transplant in MGRS is controversial as frequent recur-rences are observed when the abnormal clone is not adequately
FIGURE 1 Diagnostic and therapeutic algorithm of monoclonal gammopathy of renal significance
8 K Batko et alDownloaded from httpsacademicoupcomndtadvance-article-abstractdoi101093ndtgfy2595086133by gueston 29 August 2018
suppressed [24 109 110] The current treatment paradigm inMGRS is to achieve a complete HR as a means of improvingpost-transplant outcome and preventing recurrence [71 72111] Cibeira et al [112] report that in 340 AL amyloidosispatients subject to SCT 43 attained CR improving long-termOS and organ response (OR) In recent years the treatment-re-lated mortality (TRM) has decreased from 138 between 1994and 2003 to 56 between 2004 and 2008 In part this probablyreflects the experience of established centres however with ac-cess to novel agents there are other options for treatmentCardiac involvement should be screened for in LCDD due to ahigh TRM (23) with SCT as opposed to non-cardiac patients[32] PS does not indicate treatment failure and significantlyincreases survival compared with patients lacking response[113]
A study in AL amyloidosis patients associated the need fordialysis within 30 days of SCT with highest early death risk andTRM Patients with both eGFRlt40 mLmin173 m2 and se-rum albumin lt25 mgdL had a 438 and 281 risk of requir-ing dialysis and chance of TRM respectively Identifying andscreening for such risk factors should improve the feasibility ofSCT in MGRS conditions [114] In a study of 36 patients withAL amyloidosisMIDD who were dialysis dependent for ESRDCR was reached in 53 at 1 year post SCT with an 8 TRM[72] Achievement of dialysis independence was possible inpatients receiving a Ktx after successful SCT Similarly a studyin MM with RI found no impact on survival for patients whowere dialysis dependent [115] Further research is required toevaluate risk factors and establish whether select ESRD patientsmay benefit from SCT
Literature reports are conflicting on the approach to Ktx inMGUS [116ndash118] Bansal et al [119] reflect that a select groupof plasma dyscrasia patients should be considered for Ktx espe-cially those subject to dialysis-associated complications In ALand MIDD patients achieving haematological CR have beenreported with successful Ktx [120 121] Monoclonal gammop-athy in the setting of Ktxs is presented in Table 3 In summaryprimary disease activity organ function and patient perfor-mance should dictate selection for Ktx We propose an algo-rithm for diagnostic and therapeutic treatment of MGRS(Figure 1)
C O N C L U S I O N
With under-recognition of the wide spectrum of MGRS accu-rate classification evidence-based therapy and expert estab-lished management is required Renal involvement in MGRSresults from the direct deposition of monoclonal protein and itslight- or heavy-chain fragments in the kidney IFE microscopyis essential to identify the offending monoclonal protein and itsrenal tissue distribution In selected cases MS is of valueMGRS therapy is directed to eliminate the clonal plasma cell orB-cell population Adverse events particular to the chosen drugshould complement the patient profile Early detection diagno-sis and chemotherapy may improve kidney function It shouldbe stressed that both the renal pathology and the underlyinghaematological disorders influence the management and
prognosis of MGRS Upon achieving HR ASCT and Ktx shouldbe considered as therapy endpoints in MGRS
C O N F L I C T O F I N T E R E S T S T A T E M E N T
None declared
R E F E R E N C E S
1 Kyle RA Monoclonal gammopathy of undetermined significance NaturalHistory in 241 Cases Am J Med [Internet] 1978 [cited 2017 Oct 24] 64814ndash826 Available from httpwwwncbinlmnihgovpubmed645746
2 Leung N Bridoux F Hutchison CA et al Monoclonal gammopathy of re-nal significance when MGUS is no longer undetermined or insignificantBlood [Internet] 2012 [cited 2017 Oct 24] 120 4292ndash4295 Available fromhttpwwwncbinlmnihgovpubmed23047823
3 Kyle RA Therneau TM Rajkumar SV et al Prevalence of monoclonalgammopathy of undetermined significance N Engl J Med [Internet] 2006[cited 2017 Oct 24] 354 1362ndash1369 Available from httpwwwncbinlmnihgovpubmed16571879
4 Landgren O Graubard BI Kumar S et al Prevalence of myeloma precur-sor state monoclonal gammopathy of undetermined significance in 12372individuals 10ndash49 years old a population-based study from the NationalHealth and Nutrition Examination Survey Blood Cancer J 2017 7 e618[cited 2018 Feb 9] 7 Available from httpwwwncbinlmnihgovpubmed29053158
5 Landgren O Graubard BI Katzmann JA et al Racial disparities in theprevalence of monoclonal gammopathies a population-based study of12 482 persons from the National Health and Nutritional ExaminationSurvey Leukemia [Internet] 2014 28 1537ndash1542 [cited 2018 Jun 22]Available from httpwwwncbinlmnihgovpubmed24441287
6 Cabrera Q Macro M Hebert B et al Epidemiology of monoclonal gamm-opathy of undetermined significance (MGUS) the experience from thespecialized registry of hematologic malignancies of Basse-Normandie(France) Cancer Epidemiol [Internet] 2014 38 354ndash356 [cited 2017 Oct24] Available from httpwwwncbinlmnihgovpubmed24880205
7 Therneau TM Kyle RA Melton LJ et al Incidence of monoclonal gamm-opathy of undetermined significance and estimation of duration beforefirst clinical recognition Mayo Clin Proc [Internet] 2012 [cited 2017 Dec23] 87 1071ndash1079 Available from httpwwwncbinlmnihgovpubmed22883742
8 Kyle RA Larson DR Therneau TM et al Long-term follow-up of mono-clonal gammopathy of undetermined significance N Engl J Med 2018[cited 2018 Apr 23] 378 241ndash249 Available from httpwwwncbinlmnihgovpubmed29342381
9 Dispenzieri A Katzmann JA Kyle RA et al Prevalence and risk of progres-sion of light-chain monoclonal gammopathy of undetermined significancea retrospective population-based cohort study Lancet [Internet] 2010[cited 2018 Feb 9] 375 1721ndash1728 Available from httpwwwncbinlmnihgovpubmed20472173
10 Steiner N Gobel G Suchecki P et al Monoclonal gammopathy of renalsignificance (MGRS) increases the risk for progression to multiple mye-loma an observational study of 2935 MGUS patients Oncotarget[Internet] 2018 [cited 2018 Apr 27] 9 2344ndash2356 Available from httpwwwncbinlmnihgovpubmed29416776
11 Dhodapkar MV Sexton R Waheed S et al Clinical genomic andimaging predictors of myeloma progression from asymptomaticmonoclonal gammopathies (SWOG S0120) Blood [Internet] 2014[cited 2018 Jun 22] 123 78ndash85 Available from httpwwwncbinlmnihgovpubmed24144643
12 Zand L Kattah A Fervenza FC et al C3 glomerulonephritis associatedwith monoclonal gammopathy a case series Am J Kidney Dis [Internet]2013 [cited 2017 Dec 29] 62 506ndash514 Available from httpwwwncbinlmnihgovpubmed23623956
13 Rajkumar SV Dimopoulos MA Palumbo A et al International MyelomaWorking Group updated criteria for the diagnosis of multiple myelomaLancet Oncol [Internet] 2014 [cited 2018 Jun 23] 15 e538ndashe548 Availablefrom httplinkinghubelseviercomretrievepiiS1470204514704425
Clinical implication of monoclonal gammopathies 9Downloaded from httpsacademicoupcomndtadvance-article-abstractdoi101093ndtgfy2595086133by gueston 29 August 2018
14 Ravindran A Bartley AC Holton SJ et al Prevalence incidence and sur-vival of smoldering multiple myeloma in the United States Nat PublishingGroup [Internet] 2016 6 2018ndash2023 [cited Jun] Available from httpswwwncbinlmnihgovpmcarticlesPMC5098258pdfbcj2016100apdf
15 Fermand J-P Bridoux F Kyle RA et al How I treat monoclonal gammop-athy of renal significance (MGRS) Blood [Internet] 2013 [cited 2017 Oct27] 122 3583ndash3590 Available from httpwwwncbinlmnihgovpubmed24108460
16 Bridoux F Leung N Hutchison CA et al Diagnosis of monoclonal gamm-opathy of renal significance Kidney Int [Internet] 2015 [cited 2017 Oct24] 87 698ndash711 Available from httpwwwncbinlmnihgovpubmed25607108
17 Kristinsson SY Bjorkholm M Andersson TM-L et al Patterns of survivaland causes of death following a diagnosis of monoclonal gammopathy ofundetermined significance a population-based study Haematologica[Internet] 2009 [cited 2018 Feb] 94 1714ndash1720 Available from httpwwwncbinlmnihgovpubmed19608666
18 Dimopoulos MA Delimpasi S Katodritou E et al Significant improve-ment in the survival of patients with multiple myeloma presenting with se-vere renal impairment after the introduction of novel agents Ann Oncol[Internet] 2014 [cited 2018 Apr 23] 25 195ndash200 Available from httpsacademicoupcomannoncarticle-lookupdoi101093annoncmdt483
19 Correia SO Santos S Malheiro J et al Monoclonal gammopathy of renalsignificance diagnostic workup WJN 2017 [cited 2017 Oct 27] 6 72ndash78Available from httpwwwncbinlmnihgovpubmed28316940
20 Lin J Markowitz GS Valeri AM et al Renal monoclonal immunoglobulindeposition disease the disease spectrum J Am Soc Nephrol [Internet] 2001[cited 2018 Jun 23] 12 1482ndash1492 Available from httpwwwncbinlmnihgovpubmed11423577
21 Sethi S Zand L Leung N et al Membranoproliferative glomerulonephritissecondary to monoclonal gammopathy Clin J Am Soc Nephrol [Internet]2010 [cited 2017 Dec 8] 5 770ndash782 Available from httpwwwncbinlmnihgovpubmed20185597
22 Bhutani G Nasr SH Said SM et al Hematologic characteristics of prolifer-ative glomerulonephritides with nonorganized monoclonal immunoglobu-lin deposits Mayo Clin Proc [Internet] 2015 [cited 2018 Jun 23] 90587ndash596 Available from httpwwwncbinlmnihgovpubmed25939936
23 Cohen C El-Karoui K Alyanakian M-A et al Light and heavy chain depo-sition disease associated with CH1 deletion Clin Kidney J [Internet] 2015[cited 2017 Oct 26] 8 237ndash239 Available from httpwwwncbinlmnihgovpubmed25815184
24 Nasr SH Valeri AM Cornell LD et al Renal monoclonal immunoglobulindeposition disease a report of 64 patients from a single institution Clin JAm Soc Nephrol [Internet] 2012 [cited 2018 Feb 9] 7 231ndash239 Availablefrom httpwwwncbinlmnihgovpubmed22156754
25 Sicard A Karras A Goujon J-M et al Light chain deposition disease with-out glomerular proteinuria a diagnostic challenge for the nephrologistNephrol Dial Transplant [Internet] 2014 [cited 2018 Jul 7] 29 1894ndash1902Available from httpwwwncbinlmnihgovpubmed24619059
26 Haas M A reevaluation of routine electron microscopy in the examinationof native renal biopsies J Am Soc Nephrol [Internet] 1997 8 70ndash76Available from httpwwwncbinlmnihgovpubmed9013450
27 Stokes MB Valeri AM Herlitz L et al Light chain proximal tubulopathyclinical and pathologic characteristics in the modern treatment era J AmSoc Nephrol [Internet] 2016 [cited 2018 Jun 23] 27 1555ndash1565 Availablefrom httpwwwncbinlmnihgovpubmed26374607
28 Larsen CP Messias NC Walker PD et al Membranoproliferative glomeru-lonephritis with masked monotypic immunoglobulin deposits Kidney Int[Internet] 2015 [cited 2018 Feb 10] 88 867ndash873 Available from httpwwwncbinlmnihgovpubmed26154922
29 Eirin A Irazabal MV Gertz MA et al Clinical features of patients with im-munoglobulin light chain amyloidosis (AL) with vascular-limited deposi-tion in the kidney Nephrol Dial Transplant [Internet] 2012 [cited 2018Feb 10] 27 1097ndash1101 Available from httpwwwncbinlmnihgovpubmed22067518
30 Alonso-Titos J Perea-Ortega L Sola E et al C3 glomerulonephritis associ-ated with monoclonal gammopathy of renal significance case report BMCNephrol 2018 Jul 6] 19 129 Available from httpwwwncbinlmnihgovpubmed29884135
31 Sayed RH Wechalekar AD Gilbertson JA et al Natural history and out-come of light chain deposition disease Blood [Internet] 2015 [cited 2017Dec 8] 126 2805ndash2810 Available from httpwwwncbinlmnihgovpubmed26392598
32 Mohan M Buros A Mathur P et al Clinical characteristics and prognosticfactors in multiple myeloma patients with light chain deposition diseaseAm J Hematol 2017 [cited 2018 Jul 7] 92 739ndash745 Available from httpwwwncbinlmnihgovpubmed28383130
33 Vignon M Cohen C Faguer S et al The clinicopathologic characteristicsof kidney diseases related to monotypic IgA deposits Kidney Int [Internet]2017 [cited 2018 Jul] 91 720ndash728 Available from httpwwwncbinlmnihgovpubmed28069266
34 Best Rocha A Larsen CP Membranous glomerulopathy with light chain-restricted deposits a clinicopathological analysis of 28 cases Kidney IntRep [Internet] 2017 [cited 2018 Jul 6] 2 1141ndash1148 Available from httpwwwncbinlmnihgovpubmed29270522
35 Nasr SH Valeri AM Sethi S et al Clinicopathologic correlations in multi-ple myeloma a case series of 190 patients with kidney biopsies Am JKidney Dis [Internet] 2012 [cited 2017 Oct 26] 59 786ndash794 Availablefrom httpwwwncbinlmnihgovpubmed22417785
36 Glavey SV Leung N Monoclonal gammopathy the good the bad and theugly Blood Rev [Internet] 2016 [cited 2017 Dec 24] 30 223ndash231 Availablefrom httpwwwsciencedirectcomsciencearticlepiiS0268960X15000946bb0130
37 Katzmann JA Kyle RA Benson J et al Screening panels for detection ofmonoclonal gammopathies Clin Chem [Internet] 2009 [cited 2017 Oct25] 55 1517ndash1522 Available from httpwwwncbinlmnihgovpubmed19520758
38 Yadav P Leung N Sanders PW et al The use of immunoglobulin lightchain assays in the diagnosis of paraprotein-related kidney disease KidneyInt [Internet] 2015 [cited 2018 Feb 9] 87 692ndash697 Available from httpwwwncbinlmnihgovpubmed25296094
39 Sugihara H Chihara D Seike K et al Percentage of urinary albumin excre-tion and serum-free light-chain reduction are important determinants ofrenal response in myeloma patients with moderate to severe renal impair-ment Blood Cancer J [Internet] 2014 [cited 2018 Jun 24] 4 e235 Availablefrom httpwwwncbinlmnihgovpubmed25083819
40 Leung N Gertz M Kyle RA et al Urinary albumin excretion patterns ofpatients with cast nephropathy and other monoclonal gammopathy-related kidney diseases Clin J Am Soc Nephrol [Internet] 2012 [cited 2018Jun 24] 7 1964ndash1968 Available from httpwwwncbinlmnihgovpubmed23024162
41 Ciocchini M Arbelbide J Musso CG Monoclonal gammopathy of renalsignificance (MGRS) the characteristics and significance of a new meta-entity Int Urol Nephrol [Internet] 2017 [cited 2017 Oct 26] 492171ndash2175 Available from httpwwwncbinlmnihgovpubmed28425076
42 Sethi S Rajkumar SV DrsquoAgati VD The complexity and heterogeneity ofmonoclonal immunoglobulinndashassociated renal diseases J Am Soc Nephrol2018 29 1810ndash1823
43 Hutchison CA Harding S Hewins P et al Quantitative assessment of se-rum and urinary polyclonal free light chains in patients with chronic kid-ney disease Clin J Am Soc Nephrol [Internet] 2008 [cited 2017 Dec 25] 31684ndash1690 Available from httpwwwncbinlmnihgovpubmed18945993
44 Jurczyszyn A Ochrem B Abnormal serum free light chain ratio does notalways indicate monoclonal gammopathy Polskie Archiwum MedycynyWewnetrznej [Internet] 2015 [cited 2017 Dec 29] 125 502ndash504 Availablefrom httpwwwncbinlmnihgovpubmed26266682
45 Singh G Serum free light chain assay and jk ratio performance inpatients with monoclonal gammopathy-high false negative rate for jk ra-tio J Clin Med Res 2017 [cited 2018 Jun 25] 9 46ndash57 Available fromhttpwwwncbinlmnihgovpubmed27924175
46 Fulton RB Fernando SL Serum free light chain assay reduces the need forserum and urine immunofixation electrophoresis in the evaluation ofmonoclonal gammopathy Ann Clin Biochem [Internet] 2009 [cited 2018Jun 25] 46 407ndash412 Available from httpwwwncbinlmnihgovpubmed19641008
10 K Batko et alDownloaded from httpsacademicoupcomndtadvance-article-abstractdoi101093ndtgfy2595086133by gueston 29 August 2018
47 Levinson SS Urine immunofixation electrophoresis remains importantand is complementary to serum free light chain Clin Chem Lab Med[Internet] 2011 [cited 2018 Jun 25] 49 1801ndash1804 Available from httpwwwncbinlmnihgovpubmed21663562 [CrossRef][Mismatch]
48 Lee WS Singh G Serum free light chains in neoplastic monoclonal gam-mopathies relative under-detection of lambda dominant KappaLambdaratio and underproduction of free lambda light chains as compared tokappa light chains in patients with neoplastic monoclonal gammopathiesJ Clin Med Res 2018 [cited 2018 Jun 25] 10 562ndash569 Available fromhttpwwwncbinlmnihgovpubmed29904440
49 Xu B Tang Y Zhou J et al Disease spectrum of abnormal serum free lightchain ratio and its diagnostic significance Oncotarget [Internet] 2017[cited 2017 Dec 29] 8 82268ndash82279 Available from httpwwwncbinlmnihgovpubmed29137262
50 Koo EH Shin J Jang HR et al Diagnostic performances of M-protein testsaccording to the clinical presentations of kidney disease Eur J Intern Med[Internet] 2016 [cited 2018 Feb 9] 33 88ndash92 Available from httpwwwncbinlmnihgovpubmed27421913
51 Gumber R Cohen JB Palmer MB et al A clone-directed approach mayimprove diagnosis and treatment of proliferative glomerulonephritis withmonoclonal immunoglobulin deposits Kidney Int [Internet] 2018 94199ndash205 Available from httpsdoiorg101016jkint201802020
52 Leung N Barnidge DR Hutchison CA Laboratory testing in monoclonalgammopathy of renal significance (MGRS) Clin Chem Lab Med [Internet]2016 [cited 2017 Oct 25] 54 929ndash937 Available from httpwwwncbinlmnihgovpubmed27107835 [CrossRef][Mismatch]
53 Ramirez-Alvarado M Ward CJ Huang BQ et al Differences in immuno-globulin light chain species found in urinary exosomes in light chain amy-loidosis (AL) PLoS ONE [Internet] 2012 [cited 2018 Jul 7] 7 e38061Available from httpwwwncbinlmnihgovpubmed22723846
54 Hogan JJ Weiss BM Bridging the divide an onco-nephrologic approachto the monoclonal gammopathies of renal significance Clin J Am SocNephrol [Internet] 2016 [cited 2017 Oct 26] 11 1681ndash1691 Availablefrom httpwwwncbinlmnihgovpubmed27416775
55 Vij R Mazumder A Klinger M et al Deep sequencing reveals myelomacells in peripheral blood in majority of multiple myeloma patients ClinLymphoma Myeloma Leuk [Internet] 2014 [cited 2017 Oct 25] 14131ndash139e1 Available from httpwwwncbinlmnihgovpubmed24629890
56 Gonsalves WI Leung N Rajkumar SV et al Improvement in renal func-tion and its impact on survival in patients with newly diagnosed multiplemyeloma Blood Cancer J 2015 [cited 2018 Feb 3] 5 e296 Available fromhttpwwwnaturecomdoifinder101038bcj201520
57 Dimopoulos MA Cheung MC Roussel M et al Impact of renal impair-ment on outcomes with lenalidomide and dexamethasone treatment in theFIRST trial a randomized open-label phase 3 trial in transplant-ineligiblepatients with multiple myeloma Haematologica [Internet] 2016 [cited2018 Jul 7] 101 363ndash370 Available from httpwwwncbinlmnihgovpubmed26659916
58 Ponisch W Andrea M Wagner I et al Successful treatment of patientswith newly diagnoseduntreated multiple myeloma and advanced renalfailure using bortezomib in combination with bendamustine and predni-sone J Cancer Res Clin Oncol 2012 [cited 2018 Jul 2] 138 1405ndash1412Available from httpwwwncbinlmnihgovpubmed22526157
59 Perry M Delarche A Ribes D et al Rituximab-cyclophosphamide-dexa-methasone is highly effective in patients with monoclonal Ig deposit-related glomerulopathy and indolent non-Hodgkin lymphomas Am JHematol 2014 [cited 2018 Jul 1] 89 969ndash973 Available from httpdoiwileycom101002ajh23798
60 Dimopoulos M Weisel K van de Donk Nwcj et al Pomalidomide pluslow-dose dexamethasone in patients with relapsedrefractory multiple my-eloma and renal impairment results from a Phase II trial J Clin Oncol2018 36 2035ndash2043
61 Fervenza FC Canetta PA Barbour SJ et al A multicenter randomized con-trolled trial of rituximab versus cyclosporine in the treatment of idiopathicmembranous nephropathy (MENTOR) Nephron [Internet] 2015 [cited2017 Dec 25] 130 159ndash168 Available from httpwwwncbinlmnihgovpubmed26087670
62 Dimopoulos MA Richardson PG Schlag R et al VMP (bortezomib mel-phalan and prednisone) is active and well tolerated in newly diagnosedpatients with multiple myeloma with moderately impaired renal functionand results in reversal of renal impairment cohort analysis of the Phase IIIVISTA study JCO 2009 [cited 2017 Dec 8] 27 6086ndash6093 Available fromhttpwwwncbinlmnihgovpubmed19858394
63 Morabito F Gentile M Mazzone C et al Safety and efficacy ofbortezomib-melphalan-prednisone-thalidomide followed by bortezomib-thalidomide maintenance (VMPT-VT) versus bortezomib-melphalan-prednisone (VMP) in untreated multiple myeloma patients with renal im-pairment Blood [Internet] 2011 [cited 2017 Dec 9] 118 5759ndash5766Available from httpwwwncbinlmnihgovpubmed21951682
64 Moreau P Masszi T Grzasko N et al Oral ixazomib lenalidomide anddexamethasone for multiple myeloma N Engl J Med 2016 [cited 2018 Apr27] 374 1621ndash1634 Available from httpwwwnejmorgdoi101056NEJMoa1516282
65 Nordstrom BL Knopf KB Teltsch DY et al The safety of bendamustine inpatients with chronic lymphocytic leukemia or non-Hodgkin lymphomaand concomitant renal impairment a retrospective electronic medical re-cord database analysis Leuk Lymphoma [Internet] 2014 [cited 2017 Dec13] 55 1266ndash1273 Available from httpwwwncbinlmnihgovpubmed23987821
66 Roussou M Kastritis E Christoulas D et al Reversibility of renal failure innewly diagnosed patients with multiple myeloma and the role of novelagents Leuk Res [Internet] 2010 [cited 2017 Dec 15] 34 1395ndash1397Available from httpwwwncbinlmnihgovpubmed20510452
67 Tosi P Zamagni E Tacchetti P et al Thalidomide-dexamethasone as in-duction therapy before autologous stem cell transplantation in patientswith newly diagnosed multiple myeloma and renal insufficiency BiolBlood Marrow Transplant [Internet] 2010 [cited 2018 Apr 27] 161115ndash1121 Available from httpwwwncbinlmnihgovpubmed20197100
68 Dimopoulos M Alegre A Stadtmauer EA et al The efficacy and safety oflenalidomide plus dexamethasone in relapsed andor refractory multiplemyeloma patients with impaired renal function Cancer [Internet] 2010116 3807 [cited 2017 Dec 15] Available from httpwwwncbinlmnihgovpubmed20564094
69 Siegel DS Weisel KC Dimopoulos MA et al Pomalidomide plus low-dosedexamethasone in patients with relapsedrefractory multiple myeloma andmoderate renal impairment a pooled analysis of three clinical trials LeukLymphoma [Internet] 2016 [cited 2017 Dec 15] 57 2833ndash2838 Availablefrom httpwwwncbinlmnihgovpubmed27267105
70 Dimopoulos MA Goldschmidt H Niesvizky R et al Carfilzomib or borte-zomib in relapsed or refractory multiple myeloma (ENDEAVOR) an in-terim overall survival analysis of an open-label randomised phase 3 trialLancet Oncol [Internet] 2017 [cited 2017 Dec 6] 18 1327ndash1337 Availablefrom httpwwwncbinlmnihgovpubmed28843768
71 Telio D Shepherd J Forrest D et al High-dose melphalan followed byauto-SCT has favorable safety and efficacy in selected patients with lightchain deposition disease and light and heavy chain deposition diseaseBone Marrow Transplant 2012 [cited 2017 Dec 8] 47 453ndash455 Availablefrom httpwwwnaturecomdoifinder101038bmt201187
72 Batalini F Econimo L Quillen K et al High-dose melphalan and stem celltransplantation in patients on dialysis due to immunoglobulin light-chainamyloidosis and monoclonal immunoglobulin deposition disease BiolBlood Marrow Transplant [Internet] 2018 [cited 2017 Dec 25] 24127ndash132 Available from httpwwwncbinlmnihgovpubmed28865972
73 Kourelis TV Nasr SH Dispenzieri A et al Outcomes of patients with renalmonoclonal immunoglobulin deposition disease Am J Hematol 2016[cited 2018 Jul 2] 91 1123ndash1128 Available from httpwwwncbinlmnihgovpubmed27501122
74 Pozzi C DrsquoAmico M Fogazzi GB et al Light chain deposition disease withrenal involvement clinical characteristics and prognostic factors Am JKidney Dis [Internet] 2003 [cited 2018 Jun 23] 42 1154ndash1163 Availablefrom httpwwwncbinlmnihgovpubmed14655186
75 Song M-K Chung J-S Shin H-J et al Cyclophosphamide-containing regi-men (TCD) is superior to melphalan-containing regimen (MPT) in elderlymultiple myeloma patients with renal impairment Ann Hematol
Clinical implication of monoclonal gammopathies 11Downloaded from httpsacademicoupcomndtadvance-article-abstractdoi101093ndtgfy2595086133by gueston 29 August 2018
[Internet] 2012 [cited 2017 Dec 9] 91 889ndash896 Available from httpwwwncbinlmnihgovpubmed22237937
76 Specter R Sanchorawala V Seldin DC et al Kidney dysfunction duringlenalidomide treatment for AL amyloidosis Nephrol Dial Transplant[Internet] 2011 [cited 2018 Jul 7] 26 881ndash886 Available from httpwwwncbinlmnihgovpubmed20693160
77 Li Y Wang X OrsquoMara E et al Population pharmacokinetics of pomalido-mide in patients with relapsed or refractory multiple myeloma with variousdegrees of impaired renal function CPAA 2017 [cited 2018 Feb 4] 9133ndash145 Available from httpwwwncbinlmnihgovpubmed29184451
78 Kastritis E Gavriatopoulou M Roussou M et al Addition of cyclophos-phamide and higher doses of dexamethasone do not improve outcomes ofpatients with AL amyloidosis treated with bortezomib Blood Cancer J2017 [cited 2017 Dec 15] 7 e570 Available from httpwwwncbinlmnihgovpubmed28622303
79 Venner CP Gillmore JD Sachchithanantham S et al A matched compari-son of cyclophosphamide bortezomib and dexamethasone (CVD) versusrisk-adapted cyclophosphamide thalidomide and dexamethasone (CTD)in AL amyloidosis Leukemia [Internet] 2014 [cited 2018 Jul 5] 282304ndash2310 Available from httpwwwncbinlmnihgovpubmed25027514
80 Palladini G Sachchithanantham S Milani P et al A European collabora-tive study of cyclophosphamide bortezomib and dexamethasone inupfront treatment of systemic AL amyloidosis Blood [Internet] 2015[cited 2017 Dec 9] 126 612ndash615 Available from httpwwwncbinlmnihgovpubmed25987656
81 Kopel T Kaufman JS Hamburg N et al Endothelium-dependent and -in-dependent vascular function in advanced chronic kidney disease CJASN2017 [cited 2018 Apr 18] 12 1588ndash1594 Available from httpcjasnasnjournalsorglookupdoi102215CJN12811216
82 Palladini G Milani P Foli A et al A Phase 2 trial of pomalidomide anddexamethasone rescue treatment in patients with AL amyloidosis Blood[Internet] 2017 [cited 2018 Apr 26] 129 2120ndash2123 Available fromhttpwwwncbinlmnihgovpubmed28130212
83 Hegenbart U Bochtler T Benner A et al Lenalidomidemelphalandexa-methasone in newly diagnosed patients with immunoglobulin light chainamyloidosis results of a prospective phase 2 study with long-term followup Haematologica [Internet] 2017 [cited 2017 Dec 26] 102 1424ndash1431Available from httpwwwncbinlmnihgovpubmed28522573
84 Palladini G Milani P Foli A et al Oral melphalan and dexamethasonegrants extended survival with minimal toxicity in AL amyloidosis long-term results of a risk-adapted approach Haematologica [Internet] 2014[cited 2017 Dec 15] 99 743ndash750 Available from httpwwwncbinlmnihgovpubmed24213149
85 Payet J Livartowski J Kavian N et al Type I cryoglobulinemia in multiplemyeloma a rare entity analysis of clinical and biological characteristics ofseven cases and review of the literature Leuk Lymphoma [Internet] 201354 767ndash777 Available from httpwwwtandfonlinecomdoifull103109104281942012671481
86 Terpos E Kleber M Engelhardt M et al European Myeloma Networkguidelines for the management of multiple myeloma-related complica-tions Haematologica [Internet] 2015 [cited 2017 Dec 4] 100 1254ndash1266Available from httpwwwncbinlmnihgovpubmed26432383
87 Chanan-Khan AA Kaufman JL Mehta J et al Activity and safety of borte-zomib in multiple myeloma patients with advanced renal failure a multi-center retrospective study Blood [Internet] 2007 [cited 2018 Jul 2] 1092604ndash2606 Available from httpwwwncbinlmnihgovpubmed17138816
88 Dimopoulos MA Roussou M Gkotzamanidou M et al The role of novelagents on the reversibility of renal impairment in newly diagnosed symp-tomatic patients with multiple myeloma Leukemia 2013 27 423ndash429
89 Kouroukis TC Baldassarre FG Haynes AE et al Bortezomib in multiplemyeloma systematic review and clinical considerations Curr Oncol(Toronto Ont) [Internet] 2014 [cited 2017 Dec 4] 21 e573ndashe603Available from httpwwwncbinlmnihgovpubmed25089109
90 Zhu W Chen W Bortezomib-based treatment for multiple myelomapatients with renal impairment a systematic review and meta-analysis ofobservational studies Medicine [Internet] 2016 95 e5202 Available fromhttpwwwncbinlmnihgovpmcarticlesPMC5120900
91 Dimopoulos MA Terpos E Chanan-Khan A et al Renal impairment inpatients with multiple myeloma a consensus statement on behalf of theInternational Myeloma Working Group JCO 2010 28 4976ndash4984
92 Chauvet S Fremeaux-Bacchi V Petitprez F et al Treatment of B-cell disor-der improves renal outcome of patients with monoclonal gammopathyndashassociated C3 glomerulopathy Blood [Internet] 2017 [cited 2017 Oct 26]129 1437ndash1447 Available from httpwwwncbinlmnihgovpubmed28069603
93 Cohen C Royer B Javaugue V et al Bortezomib produces high hematolog-ical response rates with prolonged renal survival in monoclonal immuno-globulin deposition disease Kidney Int [Internet] 2015 [cited 2017 Dec25] 88 1135ndash1143 Available from httpwwwncbinlmnihgovpubmed26176826
94 Ziogas DC Kastritis E Terpos E et al Hematologic and renal improve-ment of monoclonal immunoglobulin deposition disease after treatmentwith bortezomib-based regimens Leuk Lymphoma [Internet] 2017 [cited2017 Dec 25] 58 1832ndash1839 Available from httpwwwncbinlmnihgovpubmed27967286
95 Milani P Merlini G Palladini G Novel therapies in light chain amyloid-osis Kidney Int Rep [Internet] 2018 [cited 2018 Jul 4] 3 530ndash541 Availablefrom httpwwwncbinlmnihgovpubmed29854961
96 Spizzo G Mitterer M Gunsilius E Bortezomib for the treatment of refrac-tory Type-1 cryoglobulinaemia Br J Haematol [Internet] 2010 [cited 2018Jul 7] 150 235ndash237 Available from httpdoiwileycom101111j1365-2141201008184x
97 Talamo G Claxton D Tricot G et al Response to bortezomib in refractoryType I cryoglobulinemia Am J Hematol 2008 [cited 2018 Jul 7] 83883ndash884 Available from httpwwwncbinlmnihgovpubmed18756542
98 Dimopoulos MA Roussou M Gavriatopoulou M et al Cardiac and renalcomplications of carfilzomib in patients with multiple myeloma BloodAdv 2017 [cited 2017 Dec 6] 1 449ndash454 Available from httpwwwbloodadvancesorglookupdoi101182bloodadvances2016003269
99 Strati P Nasr SH Leung N et al Renal complications in chronic lympho-cytic leukemia and monoclonal B-cell lymphocytosis the Mayo Clinic ex-perience Haematologica [Internet] 2015 [cited 2018 Jul 3] 100 1180ndash1188Available from httpwwwncbinlmnihgovpubmed26088927
100 Salama AD Pusey CD Drug insight rituximab in renal disease and trans-plantation Nat Clin Pract Nephrol [Internet] 2006 [cited 2017 Dec 8] 2221ndash230 Available from httpwwwnaturecomdoifinder101038ncpneph0133
101 Jillella AP Dainer PM Kallab AM et al Treatment of a patient with end-stage renal disease with rituximab pharmacokinetic evaluation suggestsrituximab is not eliminated by hemodialysis Am J Hematol 2002 [cited2018 Jul] 71 219ndash222 Available from httpwwwncbinlmnihgovpubmed12410580
102 Guiard E Karras A Plaisier E et al Patterns of noncryoglobulinemic glo-merulonephritis with monoclonal Ig deposits correlation with IgG sub-class and response to rituximab Clin J Am Soc Nephrol 2011 6 1609ndash1616
103 Ribes D Hachem HEL Oberic L et al Bendamustine plus rituximab forindolent B-cell lymphoma of renal significance Am J Hematol 2018 93356ndash362
104 Darwish M Bond M Hellriegel E et al Pharmacokinetic and pharmacody-namic profile of bendamustine and its metabolites Cancer ChemotherPharmacol 2015 [cited 2017 Dec 15] 75 1143ndash1154 Available from httpwwwncbinlmnihgovpubmed25829094
105 Ponisch W Moll B Bourgeois M et al Bendamustine and prednisone incombination with bortezomib (BPV) in the treatment of patients with re-lapsed or refractory multiple myeloma and light chain-induced renal fail-ure J Cancer Res Clin Oncol [Internet] 2013 [cited 2018 Jul 2] 1391937ndash1946 Available from httpwwwncbinlmnihgovpubmed24046251
106 Mateos M-V Dimopoulos MA Cavo M et al Daratumumab plus bortezo-mib melphalan and prednisone for untreated myeloma N Engl J Med2018 378 518ndash528
107 Rocchi S Tacchetti P Pantani L et al Safety and efficacy of daratumumabin dialysis-dependent renal failure secondary to multiple myelomaHaematologica [Internet] 2018 [cited 2018 Jul 2] 103 e277ndashe278 Availablefrom httpwwwncbinlmnihgovpubmed29622654
12 K Batko et alDownloaded from httpsacademicoupcomndtadvance-article-abstractdoi101093ndtgfy2595086133by gueston 29 August 2018
108 Anand S Miller D Chipman G Morris D Srinivas S Daratumumab forsevere refractory proliferative glomerulonephritis with monoclonal im-mune deposits (PGNMID) ATC Abstr [Internet] 2017 [cited 2018 Jul 3]Available from httpsatcmeetingabstractscomabstractdaratumumab-for-severe-refractory-proliferative-glomerulonephritis-with-monoclonal-immune-deposits-pgnmid
109 Leung N Lager DJ Gertz MA et al Long-term outcome of renal transplan-tation in light-chain deposition disease Am J Kidney Dis [Internet] 2004[cited 2018 Feb 9] 43 147ndash153 Available from httpwwwncbinlmnihgovpubmed14712438
110 Lorenz EC Sethi S Leung N et al Recurrent membranoproliferative glo-merulonephritis after kidney transplantation Kidney Int [Internet] 2010[cited 2018 Feb 9] 77 721ndash728 Available from httpwwwncbinlmnihgovpubmed20130531
111 Leung N Nasr SH A patient with abnormal kidney function and a mono-clonal light chain in the urine Clin J Am Soc Nephrol 2016 11 1073ndash1082
112 Cibeira MT Sanchorawala V Seldin DC et al Outcome of AL amyloidosisafter high-dose melphalan and autologous stem cell transplantation long-term results in a series of 421 patients Blood [Internet] 2011 [cited 2018Feb 3] 118 4346ndash4352 Available from httpwwwncbinlmnihgovpubmed21828140
113 Gertz MA Lacy MQ Dispenzieri A et al Autologous stem cell transplantfor immunoglobulin light chain amyloidosis a status report LeukLymphoma [Internet] 2010 [cited 2018 Feb 3] 51 2181ndash2187 Availablefrom httpwwwncbinlmnihgovpubmed20958232
114 Leung N Kumar SK Glavey SV et al The impact of dialysis on the survivalof patients with immunoglobulin light chain (AL) amyloidosis undergoingautologous stem cell transplantation Nephrol Dial Transplant 2016 [cited2018 Jul 7] 31 1284ndash1289 Available from httpsacademicoupcomndtarticle-lookupdoi101093ndtgfv328
115 Badros A Barlogie B Siegel E et al Results of autologous stem cell trans-plant in multiple myeloma patients with renal failure Br J Haematol 2001[cited 2018 Jul 7] 114 822ndash829 Available from httpwwwncbinlmnihgovpubmed11564069
116 Soltero L Carbajal H Xu J et al Initial survival data of kidney transplantpatients with pre-transplant monoclonal gammopathy Clin Transplant[Internet] 2012 [cited 2018 Feb 3] 26 300ndash304 Available from httpwwwncbinlmnihgovpubmed22044717
117 Jimenez-Zepeda VH Heilman RL Engel RA et al Monoclonal gammopathyof undetermined significance does not affect outcomes in patients undergoingsolid organ transplants Transplantation [Internet] 2011 [cited 2018 Feb 3]92 570ndash574 Available from httpwwwncbinlmnihgovpubmed21712755
118 Naina HVK Harris S Dispenzieri A et al Long-term follow-up of patientswith monoclonal gammopathy of undetermined significance after kidney
transplantation Am J Nephrol 2012 [cited 2018 Feb] 35 365ndash371Available from httpwwwncbinlmnihgovpubmed22473253
119 Bansal T Garg A Snowden JA et al Defining the role of renal transplanta-tion in the modern management of multiple myeloma and other plasmacell dyscrasias Nephron Clin Pract [Internet] 2012 [cited 2018 Feb 3] 120c228 wwwkargercom
120 Hassoun H Flombaum C DrsquoAgati VD et al High-dose melphalan andauto-SCT in patients with monoclonal Ig deposition disease Bone MarrowTransplant 2008 [cited 2018 Feb 3] 42 405ndash412 Available from httpwwwncbinlmnihgovpubmed18574442
121 Herrmann SMS Gertz MA Stegall MD et al Long-term outcomes ofpatients with light chain amyloidosis (AL) after renal transplantation withor without stem cell transplantation Nephrol Dial Transplant [Internet]2011 [cited 2018 Feb 3] 26 2032ndash2036 Available from httpwwwncbinlmnihgovpubmed21543655
122 Lorenz EC Gertz MA Fervenza FC et al Long-term outcome of autolo-gous stem cell transplantation in light chain deposition disease NephrolDial Transplant [Internet] 2008 [cited 2018 Jul 5] 23 2052ndash2057 Availablefrom httpwwwncbinlmnihgovpubmed18178602
123 Merhi B Patel N Bayliss G et al Proliferative glomerulonephritis withmonoclonal IgG deposits in two kidney allografts successfully treated withrituximab Clin Kidney J [Internet] 2017 [cited 2018 Feb 10] 10 405ndash410Available from httpsacademicoupcomckjarticle-lookupdoi101093ckjsfx001
124 Barbour SJ Beaulieu MC Zalunardo NY et al Proliferative glomerulone-phritis with monoclonal IgG deposits secondary to chronic lymphocyticleukemia Report of two cases Nephrol Dial Transplant [Internet] 2011[cited 2018 Feb 10] 26 2712ndash2714 Available from httpsacademicoupcomndtarticle-lookupdoi101093ndtgfr251
125 Zand L Lorenz EC Cosio FG et al Clinical findings pathology and out-comes of C3GN after kidney transplantation J Am Soc Nephrol [Internet]2014 [cited 2018 Jul 5] 25 1110ndash1117 Available from httpwwwncbinlmnihgovpubmed24357668
126 Alfano G Fontana F Colaci E et al Monoclonal gammopathy of undeter-mined significance after kidney transplantation Transplantation [Internet]2017 [cited 2017 Oct 24] 101 e337ndashe342 Available from httpwwwncbinlmnihgovpubmed28731904
127 Bancu I Ca~nas L Juega FJ et al Outcomes of monoclonal gammopathyof undetermined significance in patients who underwent kidneytransplantation Transplant Proc [Internet] 2015 [cited 2018 Feb 10] 472344ndash2345 Available from httpwwwncbinlmnihgovpubmed26518922
Received 2632018 Editorial decision 1472018
Clinical implication of monoclonal gammopathies 13Downloaded from httpsacademicoupcomndtadvance-article-abstractdoi101093ndtgfy2595086133by gueston 29 August 2018

CD20thorn cells can be identified while non-IgM-associated dis-eases more often require MM-like treatment
Recently an anti CD38 monoclonal antibody daratumumab(DARA) has been approved for the treatment of newly diag-nosed and relapsed MM patients [106] Like many Phase 3 reg-istration trials the study excluded patients with CrCl 20 mLmin Anecdotal evidence of safety and reduction of dialysis fre-quency in a patient with DARA monotherapy has recently beenreported [107] A case of PGNMID refractory to RTX and
bortezomib was successfully treated with DARA [108] Due toindependence of kidney clearance and positive results in RI itmay prove beneficial in MGRS There is an on-going Phase 2study of DARA in MGRS [NCT03095118]
M G R S T R A N S P L A N T A N D E S R D
Renal transplant in MGRS is controversial as frequent recur-rences are observed when the abnormal clone is not adequately
FIGURE 1 Diagnostic and therapeutic algorithm of monoclonal gammopathy of renal significance
8 K Batko et alDownloaded from httpsacademicoupcomndtadvance-article-abstractdoi101093ndtgfy2595086133by gueston 29 August 2018
suppressed [24 109 110] The current treatment paradigm inMGRS is to achieve a complete HR as a means of improvingpost-transplant outcome and preventing recurrence [71 72111] Cibeira et al [112] report that in 340 AL amyloidosispatients subject to SCT 43 attained CR improving long-termOS and organ response (OR) In recent years the treatment-re-lated mortality (TRM) has decreased from 138 between 1994and 2003 to 56 between 2004 and 2008 In part this probablyreflects the experience of established centres however with ac-cess to novel agents there are other options for treatmentCardiac involvement should be screened for in LCDD due to ahigh TRM (23) with SCT as opposed to non-cardiac patients[32] PS does not indicate treatment failure and significantlyincreases survival compared with patients lacking response[113]
A study in AL amyloidosis patients associated the need fordialysis within 30 days of SCT with highest early death risk andTRM Patients with both eGFRlt40 mLmin173 m2 and se-rum albumin lt25 mgdL had a 438 and 281 risk of requir-ing dialysis and chance of TRM respectively Identifying andscreening for such risk factors should improve the feasibility ofSCT in MGRS conditions [114] In a study of 36 patients withAL amyloidosisMIDD who were dialysis dependent for ESRDCR was reached in 53 at 1 year post SCT with an 8 TRM[72] Achievement of dialysis independence was possible inpatients receiving a Ktx after successful SCT Similarly a studyin MM with RI found no impact on survival for patients whowere dialysis dependent [115] Further research is required toevaluate risk factors and establish whether select ESRD patientsmay benefit from SCT
Literature reports are conflicting on the approach to Ktx inMGUS [116ndash118] Bansal et al [119] reflect that a select groupof plasma dyscrasia patients should be considered for Ktx espe-cially those subject to dialysis-associated complications In ALand MIDD patients achieving haematological CR have beenreported with successful Ktx [120 121] Monoclonal gammop-athy in the setting of Ktxs is presented in Table 3 In summaryprimary disease activity organ function and patient perfor-mance should dictate selection for Ktx We propose an algo-rithm for diagnostic and therapeutic treatment of MGRS(Figure 1)
C O N C L U S I O N
With under-recognition of the wide spectrum of MGRS accu-rate classification evidence-based therapy and expert estab-lished management is required Renal involvement in MGRSresults from the direct deposition of monoclonal protein and itslight- or heavy-chain fragments in the kidney IFE microscopyis essential to identify the offending monoclonal protein and itsrenal tissue distribution In selected cases MS is of valueMGRS therapy is directed to eliminate the clonal plasma cell orB-cell population Adverse events particular to the chosen drugshould complement the patient profile Early detection diagno-sis and chemotherapy may improve kidney function It shouldbe stressed that both the renal pathology and the underlyinghaematological disorders influence the management and
prognosis of MGRS Upon achieving HR ASCT and Ktx shouldbe considered as therapy endpoints in MGRS
C O N F L I C T O F I N T E R E S T S T A T E M E N T
None declared
R E F E R E N C E S
1 Kyle RA Monoclonal gammopathy of undetermined significance NaturalHistory in 241 Cases Am J Med [Internet] 1978 [cited 2017 Oct 24] 64814ndash826 Available from httpwwwncbinlmnihgovpubmed645746
2 Leung N Bridoux F Hutchison CA et al Monoclonal gammopathy of re-nal significance when MGUS is no longer undetermined or insignificantBlood [Internet] 2012 [cited 2017 Oct 24] 120 4292ndash4295 Available fromhttpwwwncbinlmnihgovpubmed23047823
3 Kyle RA Therneau TM Rajkumar SV et al Prevalence of monoclonalgammopathy of undetermined significance N Engl J Med [Internet] 2006[cited 2017 Oct 24] 354 1362ndash1369 Available from httpwwwncbinlmnihgovpubmed16571879
4 Landgren O Graubard BI Kumar S et al Prevalence of myeloma precur-sor state monoclonal gammopathy of undetermined significance in 12372individuals 10ndash49 years old a population-based study from the NationalHealth and Nutrition Examination Survey Blood Cancer J 2017 7 e618[cited 2018 Feb 9] 7 Available from httpwwwncbinlmnihgovpubmed29053158
5 Landgren O Graubard BI Katzmann JA et al Racial disparities in theprevalence of monoclonal gammopathies a population-based study of12 482 persons from the National Health and Nutritional ExaminationSurvey Leukemia [Internet] 2014 28 1537ndash1542 [cited 2018 Jun 22]Available from httpwwwncbinlmnihgovpubmed24441287
6 Cabrera Q Macro M Hebert B et al Epidemiology of monoclonal gamm-opathy of undetermined significance (MGUS) the experience from thespecialized registry of hematologic malignancies of Basse-Normandie(France) Cancer Epidemiol [Internet] 2014 38 354ndash356 [cited 2017 Oct24] Available from httpwwwncbinlmnihgovpubmed24880205
7 Therneau TM Kyle RA Melton LJ et al Incidence of monoclonal gamm-opathy of undetermined significance and estimation of duration beforefirst clinical recognition Mayo Clin Proc [Internet] 2012 [cited 2017 Dec23] 87 1071ndash1079 Available from httpwwwncbinlmnihgovpubmed22883742
8 Kyle RA Larson DR Therneau TM et al Long-term follow-up of mono-clonal gammopathy of undetermined significance N Engl J Med 2018[cited 2018 Apr 23] 378 241ndash249 Available from httpwwwncbinlmnihgovpubmed29342381
9 Dispenzieri A Katzmann JA Kyle RA et al Prevalence and risk of progres-sion of light-chain monoclonal gammopathy of undetermined significancea retrospective population-based cohort study Lancet [Internet] 2010[cited 2018 Feb 9] 375 1721ndash1728 Available from httpwwwncbinlmnihgovpubmed20472173
10 Steiner N Gobel G Suchecki P et al Monoclonal gammopathy of renalsignificance (MGRS) increases the risk for progression to multiple mye-loma an observational study of 2935 MGUS patients Oncotarget[Internet] 2018 [cited 2018 Apr 27] 9 2344ndash2356 Available from httpwwwncbinlmnihgovpubmed29416776
11 Dhodapkar MV Sexton R Waheed S et al Clinical genomic andimaging predictors of myeloma progression from asymptomaticmonoclonal gammopathies (SWOG S0120) Blood [Internet] 2014[cited 2018 Jun 22] 123 78ndash85 Available from httpwwwncbinlmnihgovpubmed24144643
12 Zand L Kattah A Fervenza FC et al C3 glomerulonephritis associatedwith monoclonal gammopathy a case series Am J Kidney Dis [Internet]2013 [cited 2017 Dec 29] 62 506ndash514 Available from httpwwwncbinlmnihgovpubmed23623956
13 Rajkumar SV Dimopoulos MA Palumbo A et al International MyelomaWorking Group updated criteria for the diagnosis of multiple myelomaLancet Oncol [Internet] 2014 [cited 2018 Jun 23] 15 e538ndashe548 Availablefrom httplinkinghubelseviercomretrievepiiS1470204514704425
Clinical implication of monoclonal gammopathies 9Downloaded from httpsacademicoupcomndtadvance-article-abstractdoi101093ndtgfy2595086133by gueston 29 August 2018
14 Ravindran A Bartley AC Holton SJ et al Prevalence incidence and sur-vival of smoldering multiple myeloma in the United States Nat PublishingGroup [Internet] 2016 6 2018ndash2023 [cited Jun] Available from httpswwwncbinlmnihgovpmcarticlesPMC5098258pdfbcj2016100apdf
15 Fermand J-P Bridoux F Kyle RA et al How I treat monoclonal gammop-athy of renal significance (MGRS) Blood [Internet] 2013 [cited 2017 Oct27] 122 3583ndash3590 Available from httpwwwncbinlmnihgovpubmed24108460
16 Bridoux F Leung N Hutchison CA et al Diagnosis of monoclonal gamm-opathy of renal significance Kidney Int [Internet] 2015 [cited 2017 Oct24] 87 698ndash711 Available from httpwwwncbinlmnihgovpubmed25607108
17 Kristinsson SY Bjorkholm M Andersson TM-L et al Patterns of survivaland causes of death following a diagnosis of monoclonal gammopathy ofundetermined significance a population-based study Haematologica[Internet] 2009 [cited 2018 Feb] 94 1714ndash1720 Available from httpwwwncbinlmnihgovpubmed19608666
18 Dimopoulos MA Delimpasi S Katodritou E et al Significant improve-ment in the survival of patients with multiple myeloma presenting with se-vere renal impairment after the introduction of novel agents Ann Oncol[Internet] 2014 [cited 2018 Apr 23] 25 195ndash200 Available from httpsacademicoupcomannoncarticle-lookupdoi101093annoncmdt483
19 Correia SO Santos S Malheiro J et al Monoclonal gammopathy of renalsignificance diagnostic workup WJN 2017 [cited 2017 Oct 27] 6 72ndash78Available from httpwwwncbinlmnihgovpubmed28316940
20 Lin J Markowitz GS Valeri AM et al Renal monoclonal immunoglobulindeposition disease the disease spectrum J Am Soc Nephrol [Internet] 2001[cited 2018 Jun 23] 12 1482ndash1492 Available from httpwwwncbinlmnihgovpubmed11423577
21 Sethi S Zand L Leung N et al Membranoproliferative glomerulonephritissecondary to monoclonal gammopathy Clin J Am Soc Nephrol [Internet]2010 [cited 2017 Dec 8] 5 770ndash782 Available from httpwwwncbinlmnihgovpubmed20185597
22 Bhutani G Nasr SH Said SM et al Hematologic characteristics of prolifer-ative glomerulonephritides with nonorganized monoclonal immunoglobu-lin deposits Mayo Clin Proc [Internet] 2015 [cited 2018 Jun 23] 90587ndash596 Available from httpwwwncbinlmnihgovpubmed25939936
23 Cohen C El-Karoui K Alyanakian M-A et al Light and heavy chain depo-sition disease associated with CH1 deletion Clin Kidney J [Internet] 2015[cited 2017 Oct 26] 8 237ndash239 Available from httpwwwncbinlmnihgovpubmed25815184
24 Nasr SH Valeri AM Cornell LD et al Renal monoclonal immunoglobulindeposition disease a report of 64 patients from a single institution Clin JAm Soc Nephrol [Internet] 2012 [cited 2018 Feb 9] 7 231ndash239 Availablefrom httpwwwncbinlmnihgovpubmed22156754
25 Sicard A Karras A Goujon J-M et al Light chain deposition disease with-out glomerular proteinuria a diagnostic challenge for the nephrologistNephrol Dial Transplant [Internet] 2014 [cited 2018 Jul 7] 29 1894ndash1902Available from httpwwwncbinlmnihgovpubmed24619059
26 Haas M A reevaluation of routine electron microscopy in the examinationof native renal biopsies J Am Soc Nephrol [Internet] 1997 8 70ndash76Available from httpwwwncbinlmnihgovpubmed9013450
27 Stokes MB Valeri AM Herlitz L et al Light chain proximal tubulopathyclinical and pathologic characteristics in the modern treatment era J AmSoc Nephrol [Internet] 2016 [cited 2018 Jun 23] 27 1555ndash1565 Availablefrom httpwwwncbinlmnihgovpubmed26374607
28 Larsen CP Messias NC Walker PD et al Membranoproliferative glomeru-lonephritis with masked monotypic immunoglobulin deposits Kidney Int[Internet] 2015 [cited 2018 Feb 10] 88 867ndash873 Available from httpwwwncbinlmnihgovpubmed26154922
29 Eirin A Irazabal MV Gertz MA et al Clinical features of patients with im-munoglobulin light chain amyloidosis (AL) with vascular-limited deposi-tion in the kidney Nephrol Dial Transplant [Internet] 2012 [cited 2018Feb 10] 27 1097ndash1101 Available from httpwwwncbinlmnihgovpubmed22067518
30 Alonso-Titos J Perea-Ortega L Sola E et al C3 glomerulonephritis associ-ated with monoclonal gammopathy of renal significance case report BMCNephrol 2018 Jul 6] 19 129 Available from httpwwwncbinlmnihgovpubmed29884135
31 Sayed RH Wechalekar AD Gilbertson JA et al Natural history and out-come of light chain deposition disease Blood [Internet] 2015 [cited 2017Dec 8] 126 2805ndash2810 Available from httpwwwncbinlmnihgovpubmed26392598
32 Mohan M Buros A Mathur P et al Clinical characteristics and prognosticfactors in multiple myeloma patients with light chain deposition diseaseAm J Hematol 2017 [cited 2018 Jul 7] 92 739ndash745 Available from httpwwwncbinlmnihgovpubmed28383130
33 Vignon M Cohen C Faguer S et al The clinicopathologic characteristicsof kidney diseases related to monotypic IgA deposits Kidney Int [Internet]2017 [cited 2018 Jul] 91 720ndash728 Available from httpwwwncbinlmnihgovpubmed28069266
34 Best Rocha A Larsen CP Membranous glomerulopathy with light chain-restricted deposits a clinicopathological analysis of 28 cases Kidney IntRep [Internet] 2017 [cited 2018 Jul 6] 2 1141ndash1148 Available from httpwwwncbinlmnihgovpubmed29270522
35 Nasr SH Valeri AM Sethi S et al Clinicopathologic correlations in multi-ple myeloma a case series of 190 patients with kidney biopsies Am JKidney Dis [Internet] 2012 [cited 2017 Oct 26] 59 786ndash794 Availablefrom httpwwwncbinlmnihgovpubmed22417785
36 Glavey SV Leung N Monoclonal gammopathy the good the bad and theugly Blood Rev [Internet] 2016 [cited 2017 Dec 24] 30 223ndash231 Availablefrom httpwwwsciencedirectcomsciencearticlepiiS0268960X15000946bb0130
37 Katzmann JA Kyle RA Benson J et al Screening panels for detection ofmonoclonal gammopathies Clin Chem [Internet] 2009 [cited 2017 Oct25] 55 1517ndash1522 Available from httpwwwncbinlmnihgovpubmed19520758
38 Yadav P Leung N Sanders PW et al The use of immunoglobulin lightchain assays in the diagnosis of paraprotein-related kidney disease KidneyInt [Internet] 2015 [cited 2018 Feb 9] 87 692ndash697 Available from httpwwwncbinlmnihgovpubmed25296094
39 Sugihara H Chihara D Seike K et al Percentage of urinary albumin excre-tion and serum-free light-chain reduction are important determinants ofrenal response in myeloma patients with moderate to severe renal impair-ment Blood Cancer J [Internet] 2014 [cited 2018 Jun 24] 4 e235 Availablefrom httpwwwncbinlmnihgovpubmed25083819
40 Leung N Gertz M Kyle RA et al Urinary albumin excretion patterns ofpatients with cast nephropathy and other monoclonal gammopathy-related kidney diseases Clin J Am Soc Nephrol [Internet] 2012 [cited 2018Jun 24] 7 1964ndash1968 Available from httpwwwncbinlmnihgovpubmed23024162
41 Ciocchini M Arbelbide J Musso CG Monoclonal gammopathy of renalsignificance (MGRS) the characteristics and significance of a new meta-entity Int Urol Nephrol [Internet] 2017 [cited 2017 Oct 26] 492171ndash2175 Available from httpwwwncbinlmnihgovpubmed28425076
42 Sethi S Rajkumar SV DrsquoAgati VD The complexity and heterogeneity ofmonoclonal immunoglobulinndashassociated renal diseases J Am Soc Nephrol2018 29 1810ndash1823
43 Hutchison CA Harding S Hewins P et al Quantitative assessment of se-rum and urinary polyclonal free light chains in patients with chronic kid-ney disease Clin J Am Soc Nephrol [Internet] 2008 [cited 2017 Dec 25] 31684ndash1690 Available from httpwwwncbinlmnihgovpubmed18945993
44 Jurczyszyn A Ochrem B Abnormal serum free light chain ratio does notalways indicate monoclonal gammopathy Polskie Archiwum MedycynyWewnetrznej [Internet] 2015 [cited 2017 Dec 29] 125 502ndash504 Availablefrom httpwwwncbinlmnihgovpubmed26266682
45 Singh G Serum free light chain assay and jk ratio performance inpatients with monoclonal gammopathy-high false negative rate for jk ra-tio J Clin Med Res 2017 [cited 2018 Jun 25] 9 46ndash57 Available fromhttpwwwncbinlmnihgovpubmed27924175
46 Fulton RB Fernando SL Serum free light chain assay reduces the need forserum and urine immunofixation electrophoresis in the evaluation ofmonoclonal gammopathy Ann Clin Biochem [Internet] 2009 [cited 2018Jun 25] 46 407ndash412 Available from httpwwwncbinlmnihgovpubmed19641008
10 K Batko et alDownloaded from httpsacademicoupcomndtadvance-article-abstractdoi101093ndtgfy2595086133by gueston 29 August 2018
47 Levinson SS Urine immunofixation electrophoresis remains importantand is complementary to serum free light chain Clin Chem Lab Med[Internet] 2011 [cited 2018 Jun 25] 49 1801ndash1804 Available from httpwwwncbinlmnihgovpubmed21663562 [CrossRef][Mismatch]
48 Lee WS Singh G Serum free light chains in neoplastic monoclonal gam-mopathies relative under-detection of lambda dominant KappaLambdaratio and underproduction of free lambda light chains as compared tokappa light chains in patients with neoplastic monoclonal gammopathiesJ Clin Med Res 2018 [cited 2018 Jun 25] 10 562ndash569 Available fromhttpwwwncbinlmnihgovpubmed29904440
49 Xu B Tang Y Zhou J et al Disease spectrum of abnormal serum free lightchain ratio and its diagnostic significance Oncotarget [Internet] 2017[cited 2017 Dec 29] 8 82268ndash82279 Available from httpwwwncbinlmnihgovpubmed29137262
50 Koo EH Shin J Jang HR et al Diagnostic performances of M-protein testsaccording to the clinical presentations of kidney disease Eur J Intern Med[Internet] 2016 [cited 2018 Feb 9] 33 88ndash92 Available from httpwwwncbinlmnihgovpubmed27421913
51 Gumber R Cohen JB Palmer MB et al A clone-directed approach mayimprove diagnosis and treatment of proliferative glomerulonephritis withmonoclonal immunoglobulin deposits Kidney Int [Internet] 2018 94199ndash205 Available from httpsdoiorg101016jkint201802020
52 Leung N Barnidge DR Hutchison CA Laboratory testing in monoclonalgammopathy of renal significance (MGRS) Clin Chem Lab Med [Internet]2016 [cited 2017 Oct 25] 54 929ndash937 Available from httpwwwncbinlmnihgovpubmed27107835 [CrossRef][Mismatch]
53 Ramirez-Alvarado M Ward CJ Huang BQ et al Differences in immuno-globulin light chain species found in urinary exosomes in light chain amy-loidosis (AL) PLoS ONE [Internet] 2012 [cited 2018 Jul 7] 7 e38061Available from httpwwwncbinlmnihgovpubmed22723846
54 Hogan JJ Weiss BM Bridging the divide an onco-nephrologic approachto the monoclonal gammopathies of renal significance Clin J Am SocNephrol [Internet] 2016 [cited 2017 Oct 26] 11 1681ndash1691 Availablefrom httpwwwncbinlmnihgovpubmed27416775
55 Vij R Mazumder A Klinger M et al Deep sequencing reveals myelomacells in peripheral blood in majority of multiple myeloma patients ClinLymphoma Myeloma Leuk [Internet] 2014 [cited 2017 Oct 25] 14131ndash139e1 Available from httpwwwncbinlmnihgovpubmed24629890
56 Gonsalves WI Leung N Rajkumar SV et al Improvement in renal func-tion and its impact on survival in patients with newly diagnosed multiplemyeloma Blood Cancer J 2015 [cited 2018 Feb 3] 5 e296 Available fromhttpwwwnaturecomdoifinder101038bcj201520
57 Dimopoulos MA Cheung MC Roussel M et al Impact of renal impair-ment on outcomes with lenalidomide and dexamethasone treatment in theFIRST trial a randomized open-label phase 3 trial in transplant-ineligiblepatients with multiple myeloma Haematologica [Internet] 2016 [cited2018 Jul 7] 101 363ndash370 Available from httpwwwncbinlmnihgovpubmed26659916
58 Ponisch W Andrea M Wagner I et al Successful treatment of patientswith newly diagnoseduntreated multiple myeloma and advanced renalfailure using bortezomib in combination with bendamustine and predni-sone J Cancer Res Clin Oncol 2012 [cited 2018 Jul 2] 138 1405ndash1412Available from httpwwwncbinlmnihgovpubmed22526157
59 Perry M Delarche A Ribes D et al Rituximab-cyclophosphamide-dexa-methasone is highly effective in patients with monoclonal Ig deposit-related glomerulopathy and indolent non-Hodgkin lymphomas Am JHematol 2014 [cited 2018 Jul 1] 89 969ndash973 Available from httpdoiwileycom101002ajh23798
60 Dimopoulos M Weisel K van de Donk Nwcj et al Pomalidomide pluslow-dose dexamethasone in patients with relapsedrefractory multiple my-eloma and renal impairment results from a Phase II trial J Clin Oncol2018 36 2035ndash2043
61 Fervenza FC Canetta PA Barbour SJ et al A multicenter randomized con-trolled trial of rituximab versus cyclosporine in the treatment of idiopathicmembranous nephropathy (MENTOR) Nephron [Internet] 2015 [cited2017 Dec 25] 130 159ndash168 Available from httpwwwncbinlmnihgovpubmed26087670
62 Dimopoulos MA Richardson PG Schlag R et al VMP (bortezomib mel-phalan and prednisone) is active and well tolerated in newly diagnosedpatients with multiple myeloma with moderately impaired renal functionand results in reversal of renal impairment cohort analysis of the Phase IIIVISTA study JCO 2009 [cited 2017 Dec 8] 27 6086ndash6093 Available fromhttpwwwncbinlmnihgovpubmed19858394
63 Morabito F Gentile M Mazzone C et al Safety and efficacy ofbortezomib-melphalan-prednisone-thalidomide followed by bortezomib-thalidomide maintenance (VMPT-VT) versus bortezomib-melphalan-prednisone (VMP) in untreated multiple myeloma patients with renal im-pairment Blood [Internet] 2011 [cited 2017 Dec 9] 118 5759ndash5766Available from httpwwwncbinlmnihgovpubmed21951682
64 Moreau P Masszi T Grzasko N et al Oral ixazomib lenalidomide anddexamethasone for multiple myeloma N Engl J Med 2016 [cited 2018 Apr27] 374 1621ndash1634 Available from httpwwwnejmorgdoi101056NEJMoa1516282
65 Nordstrom BL Knopf KB Teltsch DY et al The safety of bendamustine inpatients with chronic lymphocytic leukemia or non-Hodgkin lymphomaand concomitant renal impairment a retrospective electronic medical re-cord database analysis Leuk Lymphoma [Internet] 2014 [cited 2017 Dec13] 55 1266ndash1273 Available from httpwwwncbinlmnihgovpubmed23987821
66 Roussou M Kastritis E Christoulas D et al Reversibility of renal failure innewly diagnosed patients with multiple myeloma and the role of novelagents Leuk Res [Internet] 2010 [cited 2017 Dec 15] 34 1395ndash1397Available from httpwwwncbinlmnihgovpubmed20510452
67 Tosi P Zamagni E Tacchetti P et al Thalidomide-dexamethasone as in-duction therapy before autologous stem cell transplantation in patientswith newly diagnosed multiple myeloma and renal insufficiency BiolBlood Marrow Transplant [Internet] 2010 [cited 2018 Apr 27] 161115ndash1121 Available from httpwwwncbinlmnihgovpubmed20197100
68 Dimopoulos M Alegre A Stadtmauer EA et al The efficacy and safety oflenalidomide plus dexamethasone in relapsed andor refractory multiplemyeloma patients with impaired renal function Cancer [Internet] 2010116 3807 [cited 2017 Dec 15] Available from httpwwwncbinlmnihgovpubmed20564094
69 Siegel DS Weisel KC Dimopoulos MA et al Pomalidomide plus low-dosedexamethasone in patients with relapsedrefractory multiple myeloma andmoderate renal impairment a pooled analysis of three clinical trials LeukLymphoma [Internet] 2016 [cited 2017 Dec 15] 57 2833ndash2838 Availablefrom httpwwwncbinlmnihgovpubmed27267105
70 Dimopoulos MA Goldschmidt H Niesvizky R et al Carfilzomib or borte-zomib in relapsed or refractory multiple myeloma (ENDEAVOR) an in-terim overall survival analysis of an open-label randomised phase 3 trialLancet Oncol [Internet] 2017 [cited 2017 Dec 6] 18 1327ndash1337 Availablefrom httpwwwncbinlmnihgovpubmed28843768
71 Telio D Shepherd J Forrest D et al High-dose melphalan followed byauto-SCT has favorable safety and efficacy in selected patients with lightchain deposition disease and light and heavy chain deposition diseaseBone Marrow Transplant 2012 [cited 2017 Dec 8] 47 453ndash455 Availablefrom httpwwwnaturecomdoifinder101038bmt201187
72 Batalini F Econimo L Quillen K et al High-dose melphalan and stem celltransplantation in patients on dialysis due to immunoglobulin light-chainamyloidosis and monoclonal immunoglobulin deposition disease BiolBlood Marrow Transplant [Internet] 2018 [cited 2017 Dec 25] 24127ndash132 Available from httpwwwncbinlmnihgovpubmed28865972
73 Kourelis TV Nasr SH Dispenzieri A et al Outcomes of patients with renalmonoclonal immunoglobulin deposition disease Am J Hematol 2016[cited 2018 Jul 2] 91 1123ndash1128 Available from httpwwwncbinlmnihgovpubmed27501122
74 Pozzi C DrsquoAmico M Fogazzi GB et al Light chain deposition disease withrenal involvement clinical characteristics and prognostic factors Am JKidney Dis [Internet] 2003 [cited 2018 Jun 23] 42 1154ndash1163 Availablefrom httpwwwncbinlmnihgovpubmed14655186
75 Song M-K Chung J-S Shin H-J et al Cyclophosphamide-containing regi-men (TCD) is superior to melphalan-containing regimen (MPT) in elderlymultiple myeloma patients with renal impairment Ann Hematol
Clinical implication of monoclonal gammopathies 11Downloaded from httpsacademicoupcomndtadvance-article-abstractdoi101093ndtgfy2595086133by gueston 29 August 2018
[Internet] 2012 [cited 2017 Dec 9] 91 889ndash896 Available from httpwwwncbinlmnihgovpubmed22237937
76 Specter R Sanchorawala V Seldin DC et al Kidney dysfunction duringlenalidomide treatment for AL amyloidosis Nephrol Dial Transplant[Internet] 2011 [cited 2018 Jul 7] 26 881ndash886 Available from httpwwwncbinlmnihgovpubmed20693160
77 Li Y Wang X OrsquoMara E et al Population pharmacokinetics of pomalido-mide in patients with relapsed or refractory multiple myeloma with variousdegrees of impaired renal function CPAA 2017 [cited 2018 Feb 4] 9133ndash145 Available from httpwwwncbinlmnihgovpubmed29184451
78 Kastritis E Gavriatopoulou M Roussou M et al Addition of cyclophos-phamide and higher doses of dexamethasone do not improve outcomes ofpatients with AL amyloidosis treated with bortezomib Blood Cancer J2017 [cited 2017 Dec 15] 7 e570 Available from httpwwwncbinlmnihgovpubmed28622303
79 Venner CP Gillmore JD Sachchithanantham S et al A matched compari-son of cyclophosphamide bortezomib and dexamethasone (CVD) versusrisk-adapted cyclophosphamide thalidomide and dexamethasone (CTD)in AL amyloidosis Leukemia [Internet] 2014 [cited 2018 Jul 5] 282304ndash2310 Available from httpwwwncbinlmnihgovpubmed25027514
80 Palladini G Sachchithanantham S Milani P et al A European collabora-tive study of cyclophosphamide bortezomib and dexamethasone inupfront treatment of systemic AL amyloidosis Blood [Internet] 2015[cited 2017 Dec 9] 126 612ndash615 Available from httpwwwncbinlmnihgovpubmed25987656
81 Kopel T Kaufman JS Hamburg N et al Endothelium-dependent and -in-dependent vascular function in advanced chronic kidney disease CJASN2017 [cited 2018 Apr 18] 12 1588ndash1594 Available from httpcjasnasnjournalsorglookupdoi102215CJN12811216
82 Palladini G Milani P Foli A et al A Phase 2 trial of pomalidomide anddexamethasone rescue treatment in patients with AL amyloidosis Blood[Internet] 2017 [cited 2018 Apr 26] 129 2120ndash2123 Available fromhttpwwwncbinlmnihgovpubmed28130212
83 Hegenbart U Bochtler T Benner A et al Lenalidomidemelphalandexa-methasone in newly diagnosed patients with immunoglobulin light chainamyloidosis results of a prospective phase 2 study with long-term followup Haematologica [Internet] 2017 [cited 2017 Dec 26] 102 1424ndash1431Available from httpwwwncbinlmnihgovpubmed28522573
84 Palladini G Milani P Foli A et al Oral melphalan and dexamethasonegrants extended survival with minimal toxicity in AL amyloidosis long-term results of a risk-adapted approach Haematologica [Internet] 2014[cited 2017 Dec 15] 99 743ndash750 Available from httpwwwncbinlmnihgovpubmed24213149
85 Payet J Livartowski J Kavian N et al Type I cryoglobulinemia in multiplemyeloma a rare entity analysis of clinical and biological characteristics ofseven cases and review of the literature Leuk Lymphoma [Internet] 201354 767ndash777 Available from httpwwwtandfonlinecomdoifull103109104281942012671481
86 Terpos E Kleber M Engelhardt M et al European Myeloma Networkguidelines for the management of multiple myeloma-related complica-tions Haematologica [Internet] 2015 [cited 2017 Dec 4] 100 1254ndash1266Available from httpwwwncbinlmnihgovpubmed26432383
87 Chanan-Khan AA Kaufman JL Mehta J et al Activity and safety of borte-zomib in multiple myeloma patients with advanced renal failure a multi-center retrospective study Blood [Internet] 2007 [cited 2018 Jul 2] 1092604ndash2606 Available from httpwwwncbinlmnihgovpubmed17138816
88 Dimopoulos MA Roussou M Gkotzamanidou M et al The role of novelagents on the reversibility of renal impairment in newly diagnosed symp-tomatic patients with multiple myeloma Leukemia 2013 27 423ndash429
89 Kouroukis TC Baldassarre FG Haynes AE et al Bortezomib in multiplemyeloma systematic review and clinical considerations Curr Oncol(Toronto Ont) [Internet] 2014 [cited 2017 Dec 4] 21 e573ndashe603Available from httpwwwncbinlmnihgovpubmed25089109
90 Zhu W Chen W Bortezomib-based treatment for multiple myelomapatients with renal impairment a systematic review and meta-analysis ofobservational studies Medicine [Internet] 2016 95 e5202 Available fromhttpwwwncbinlmnihgovpmcarticlesPMC5120900
91 Dimopoulos MA Terpos E Chanan-Khan A et al Renal impairment inpatients with multiple myeloma a consensus statement on behalf of theInternational Myeloma Working Group JCO 2010 28 4976ndash4984
92 Chauvet S Fremeaux-Bacchi V Petitprez F et al Treatment of B-cell disor-der improves renal outcome of patients with monoclonal gammopathyndashassociated C3 glomerulopathy Blood [Internet] 2017 [cited 2017 Oct 26]129 1437ndash1447 Available from httpwwwncbinlmnihgovpubmed28069603
93 Cohen C Royer B Javaugue V et al Bortezomib produces high hematolog-ical response rates with prolonged renal survival in monoclonal immuno-globulin deposition disease Kidney Int [Internet] 2015 [cited 2017 Dec25] 88 1135ndash1143 Available from httpwwwncbinlmnihgovpubmed26176826
94 Ziogas DC Kastritis E Terpos E et al Hematologic and renal improve-ment of monoclonal immunoglobulin deposition disease after treatmentwith bortezomib-based regimens Leuk Lymphoma [Internet] 2017 [cited2017 Dec 25] 58 1832ndash1839 Available from httpwwwncbinlmnihgovpubmed27967286
95 Milani P Merlini G Palladini G Novel therapies in light chain amyloid-osis Kidney Int Rep [Internet] 2018 [cited 2018 Jul 4] 3 530ndash541 Availablefrom httpwwwncbinlmnihgovpubmed29854961
96 Spizzo G Mitterer M Gunsilius E Bortezomib for the treatment of refrac-tory Type-1 cryoglobulinaemia Br J Haematol [Internet] 2010 [cited 2018Jul 7] 150 235ndash237 Available from httpdoiwileycom101111j1365-2141201008184x
97 Talamo G Claxton D Tricot G et al Response to bortezomib in refractoryType I cryoglobulinemia Am J Hematol 2008 [cited 2018 Jul 7] 83883ndash884 Available from httpwwwncbinlmnihgovpubmed18756542
98 Dimopoulos MA Roussou M Gavriatopoulou M et al Cardiac and renalcomplications of carfilzomib in patients with multiple myeloma BloodAdv 2017 [cited 2017 Dec 6] 1 449ndash454 Available from httpwwwbloodadvancesorglookupdoi101182bloodadvances2016003269
99 Strati P Nasr SH Leung N et al Renal complications in chronic lympho-cytic leukemia and monoclonal B-cell lymphocytosis the Mayo Clinic ex-perience Haematologica [Internet] 2015 [cited 2018 Jul 3] 100 1180ndash1188Available from httpwwwncbinlmnihgovpubmed26088927
100 Salama AD Pusey CD Drug insight rituximab in renal disease and trans-plantation Nat Clin Pract Nephrol [Internet] 2006 [cited 2017 Dec 8] 2221ndash230 Available from httpwwwnaturecomdoifinder101038ncpneph0133
101 Jillella AP Dainer PM Kallab AM et al Treatment of a patient with end-stage renal disease with rituximab pharmacokinetic evaluation suggestsrituximab is not eliminated by hemodialysis Am J Hematol 2002 [cited2018 Jul] 71 219ndash222 Available from httpwwwncbinlmnihgovpubmed12410580
102 Guiard E Karras A Plaisier E et al Patterns of noncryoglobulinemic glo-merulonephritis with monoclonal Ig deposits correlation with IgG sub-class and response to rituximab Clin J Am Soc Nephrol 2011 6 1609ndash1616
103 Ribes D Hachem HEL Oberic L et al Bendamustine plus rituximab forindolent B-cell lymphoma of renal significance Am J Hematol 2018 93356ndash362
104 Darwish M Bond M Hellriegel E et al Pharmacokinetic and pharmacody-namic profile of bendamustine and its metabolites Cancer ChemotherPharmacol 2015 [cited 2017 Dec 15] 75 1143ndash1154 Available from httpwwwncbinlmnihgovpubmed25829094
105 Ponisch W Moll B Bourgeois M et al Bendamustine and prednisone incombination with bortezomib (BPV) in the treatment of patients with re-lapsed or refractory multiple myeloma and light chain-induced renal fail-ure J Cancer Res Clin Oncol [Internet] 2013 [cited 2018 Jul 2] 1391937ndash1946 Available from httpwwwncbinlmnihgovpubmed24046251
106 Mateos M-V Dimopoulos MA Cavo M et al Daratumumab plus bortezo-mib melphalan and prednisone for untreated myeloma N Engl J Med2018 378 518ndash528
107 Rocchi S Tacchetti P Pantani L et al Safety and efficacy of daratumumabin dialysis-dependent renal failure secondary to multiple myelomaHaematologica [Internet] 2018 [cited 2018 Jul 2] 103 e277ndashe278 Availablefrom httpwwwncbinlmnihgovpubmed29622654
12 K Batko et alDownloaded from httpsacademicoupcomndtadvance-article-abstractdoi101093ndtgfy2595086133by gueston 29 August 2018
108 Anand S Miller D Chipman G Morris D Srinivas S Daratumumab forsevere refractory proliferative glomerulonephritis with monoclonal im-mune deposits (PGNMID) ATC Abstr [Internet] 2017 [cited 2018 Jul 3]Available from httpsatcmeetingabstractscomabstractdaratumumab-for-severe-refractory-proliferative-glomerulonephritis-with-monoclonal-immune-deposits-pgnmid
109 Leung N Lager DJ Gertz MA et al Long-term outcome of renal transplan-tation in light-chain deposition disease Am J Kidney Dis [Internet] 2004[cited 2018 Feb 9] 43 147ndash153 Available from httpwwwncbinlmnihgovpubmed14712438
110 Lorenz EC Sethi S Leung N et al Recurrent membranoproliferative glo-merulonephritis after kidney transplantation Kidney Int [Internet] 2010[cited 2018 Feb 9] 77 721ndash728 Available from httpwwwncbinlmnihgovpubmed20130531
111 Leung N Nasr SH A patient with abnormal kidney function and a mono-clonal light chain in the urine Clin J Am Soc Nephrol 2016 11 1073ndash1082
112 Cibeira MT Sanchorawala V Seldin DC et al Outcome of AL amyloidosisafter high-dose melphalan and autologous stem cell transplantation long-term results in a series of 421 patients Blood [Internet] 2011 [cited 2018Feb 3] 118 4346ndash4352 Available from httpwwwncbinlmnihgovpubmed21828140
113 Gertz MA Lacy MQ Dispenzieri A et al Autologous stem cell transplantfor immunoglobulin light chain amyloidosis a status report LeukLymphoma [Internet] 2010 [cited 2018 Feb 3] 51 2181ndash2187 Availablefrom httpwwwncbinlmnihgovpubmed20958232
114 Leung N Kumar SK Glavey SV et al The impact of dialysis on the survivalof patients with immunoglobulin light chain (AL) amyloidosis undergoingautologous stem cell transplantation Nephrol Dial Transplant 2016 [cited2018 Jul 7] 31 1284ndash1289 Available from httpsacademicoupcomndtarticle-lookupdoi101093ndtgfv328
115 Badros A Barlogie B Siegel E et al Results of autologous stem cell trans-plant in multiple myeloma patients with renal failure Br J Haematol 2001[cited 2018 Jul 7] 114 822ndash829 Available from httpwwwncbinlmnihgovpubmed11564069
116 Soltero L Carbajal H Xu J et al Initial survival data of kidney transplantpatients with pre-transplant monoclonal gammopathy Clin Transplant[Internet] 2012 [cited 2018 Feb 3] 26 300ndash304 Available from httpwwwncbinlmnihgovpubmed22044717
117 Jimenez-Zepeda VH Heilman RL Engel RA et al Monoclonal gammopathyof undetermined significance does not affect outcomes in patients undergoingsolid organ transplants Transplantation [Internet] 2011 [cited 2018 Feb 3]92 570ndash574 Available from httpwwwncbinlmnihgovpubmed21712755
118 Naina HVK Harris S Dispenzieri A et al Long-term follow-up of patientswith monoclonal gammopathy of undetermined significance after kidney
transplantation Am J Nephrol 2012 [cited 2018 Feb] 35 365ndash371Available from httpwwwncbinlmnihgovpubmed22473253
119 Bansal T Garg A Snowden JA et al Defining the role of renal transplanta-tion in the modern management of multiple myeloma and other plasmacell dyscrasias Nephron Clin Pract [Internet] 2012 [cited 2018 Feb 3] 120c228 wwwkargercom
120 Hassoun H Flombaum C DrsquoAgati VD et al High-dose melphalan andauto-SCT in patients with monoclonal Ig deposition disease Bone MarrowTransplant 2008 [cited 2018 Feb 3] 42 405ndash412 Available from httpwwwncbinlmnihgovpubmed18574442
121 Herrmann SMS Gertz MA Stegall MD et al Long-term outcomes ofpatients with light chain amyloidosis (AL) after renal transplantation withor without stem cell transplantation Nephrol Dial Transplant [Internet]2011 [cited 2018 Feb 3] 26 2032ndash2036 Available from httpwwwncbinlmnihgovpubmed21543655
122 Lorenz EC Gertz MA Fervenza FC et al Long-term outcome of autolo-gous stem cell transplantation in light chain deposition disease NephrolDial Transplant [Internet] 2008 [cited 2018 Jul 5] 23 2052ndash2057 Availablefrom httpwwwncbinlmnihgovpubmed18178602
123 Merhi B Patel N Bayliss G et al Proliferative glomerulonephritis withmonoclonal IgG deposits in two kidney allografts successfully treated withrituximab Clin Kidney J [Internet] 2017 [cited 2018 Feb 10] 10 405ndash410Available from httpsacademicoupcomckjarticle-lookupdoi101093ckjsfx001
124 Barbour SJ Beaulieu MC Zalunardo NY et al Proliferative glomerulone-phritis with monoclonal IgG deposits secondary to chronic lymphocyticleukemia Report of two cases Nephrol Dial Transplant [Internet] 2011[cited 2018 Feb 10] 26 2712ndash2714 Available from httpsacademicoupcomndtarticle-lookupdoi101093ndtgfr251
125 Zand L Lorenz EC Cosio FG et al Clinical findings pathology and out-comes of C3GN after kidney transplantation J Am Soc Nephrol [Internet]2014 [cited 2018 Jul 5] 25 1110ndash1117 Available from httpwwwncbinlmnihgovpubmed24357668
126 Alfano G Fontana F Colaci E et al Monoclonal gammopathy of undeter-mined significance after kidney transplantation Transplantation [Internet]2017 [cited 2017 Oct 24] 101 e337ndashe342 Available from httpwwwncbinlmnihgovpubmed28731904
127 Bancu I Ca~nas L Juega FJ et al Outcomes of monoclonal gammopathyof undetermined significance in patients who underwent kidneytransplantation Transplant Proc [Internet] 2015 [cited 2018 Feb 10] 472344ndash2345 Available from httpwwwncbinlmnihgovpubmed26518922
Received 2632018 Editorial decision 1472018
Clinical implication of monoclonal gammopathies 13Downloaded from httpsacademicoupcomndtadvance-article-abstractdoi101093ndtgfy2595086133by gueston 29 August 2018

suppressed [24 109 110] The current treatment paradigm inMGRS is to achieve a complete HR as a means of improvingpost-transplant outcome and preventing recurrence [71 72111] Cibeira et al [112] report that in 340 AL amyloidosispatients subject to SCT 43 attained CR improving long-termOS and organ response (OR) In recent years the treatment-re-lated mortality (TRM) has decreased from 138 between 1994and 2003 to 56 between 2004 and 2008 In part this probablyreflects the experience of established centres however with ac-cess to novel agents there are other options for treatmentCardiac involvement should be screened for in LCDD due to ahigh TRM (23) with SCT as opposed to non-cardiac patients[32] PS does not indicate treatment failure and significantlyincreases survival compared with patients lacking response[113]
A study in AL amyloidosis patients associated the need fordialysis within 30 days of SCT with highest early death risk andTRM Patients with both eGFRlt40 mLmin173 m2 and se-rum albumin lt25 mgdL had a 438 and 281 risk of requir-ing dialysis and chance of TRM respectively Identifying andscreening for such risk factors should improve the feasibility ofSCT in MGRS conditions [114] In a study of 36 patients withAL amyloidosisMIDD who were dialysis dependent for ESRDCR was reached in 53 at 1 year post SCT with an 8 TRM[72] Achievement of dialysis independence was possible inpatients receiving a Ktx after successful SCT Similarly a studyin MM with RI found no impact on survival for patients whowere dialysis dependent [115] Further research is required toevaluate risk factors and establish whether select ESRD patientsmay benefit from SCT
Literature reports are conflicting on the approach to Ktx inMGUS [116ndash118] Bansal et al [119] reflect that a select groupof plasma dyscrasia patients should be considered for Ktx espe-cially those subject to dialysis-associated complications In ALand MIDD patients achieving haematological CR have beenreported with successful Ktx [120 121] Monoclonal gammop-athy in the setting of Ktxs is presented in Table 3 In summaryprimary disease activity organ function and patient perfor-mance should dictate selection for Ktx We propose an algo-rithm for diagnostic and therapeutic treatment of MGRS(Figure 1)
C O N C L U S I O N
With under-recognition of the wide spectrum of MGRS accu-rate classification evidence-based therapy and expert estab-lished management is required Renal involvement in MGRSresults from the direct deposition of monoclonal protein and itslight- or heavy-chain fragments in the kidney IFE microscopyis essential to identify the offending monoclonal protein and itsrenal tissue distribution In selected cases MS is of valueMGRS therapy is directed to eliminate the clonal plasma cell orB-cell population Adverse events particular to the chosen drugshould complement the patient profile Early detection diagno-sis and chemotherapy may improve kidney function It shouldbe stressed that both the renal pathology and the underlyinghaematological disorders influence the management and
prognosis of MGRS Upon achieving HR ASCT and Ktx shouldbe considered as therapy endpoints in MGRS
C O N F L I C T O F I N T E R E S T S T A T E M E N T
None declared
R E F E R E N C E S
1 Kyle RA Monoclonal gammopathy of undetermined significance NaturalHistory in 241 Cases Am J Med [Internet] 1978 [cited 2017 Oct 24] 64814ndash826 Available from httpwwwncbinlmnihgovpubmed645746
2 Leung N Bridoux F Hutchison CA et al Monoclonal gammopathy of re-nal significance when MGUS is no longer undetermined or insignificantBlood [Internet] 2012 [cited 2017 Oct 24] 120 4292ndash4295 Available fromhttpwwwncbinlmnihgovpubmed23047823
3 Kyle RA Therneau TM Rajkumar SV et al Prevalence of monoclonalgammopathy of undetermined significance N Engl J Med [Internet] 2006[cited 2017 Oct 24] 354 1362ndash1369 Available from httpwwwncbinlmnihgovpubmed16571879
4 Landgren O Graubard BI Kumar S et al Prevalence of myeloma precur-sor state monoclonal gammopathy of undetermined significance in 12372individuals 10ndash49 years old a population-based study from the NationalHealth and Nutrition Examination Survey Blood Cancer J 2017 7 e618[cited 2018 Feb 9] 7 Available from httpwwwncbinlmnihgovpubmed29053158
5 Landgren O Graubard BI Katzmann JA et al Racial disparities in theprevalence of monoclonal gammopathies a population-based study of12 482 persons from the National Health and Nutritional ExaminationSurvey Leukemia [Internet] 2014 28 1537ndash1542 [cited 2018 Jun 22]Available from httpwwwncbinlmnihgovpubmed24441287
6 Cabrera Q Macro M Hebert B et al Epidemiology of monoclonal gamm-opathy of undetermined significance (MGUS) the experience from thespecialized registry of hematologic malignancies of Basse-Normandie(France) Cancer Epidemiol [Internet] 2014 38 354ndash356 [cited 2017 Oct24] Available from httpwwwncbinlmnihgovpubmed24880205
7 Therneau TM Kyle RA Melton LJ et al Incidence of monoclonal gamm-opathy of undetermined significance and estimation of duration beforefirst clinical recognition Mayo Clin Proc [Internet] 2012 [cited 2017 Dec23] 87 1071ndash1079 Available from httpwwwncbinlmnihgovpubmed22883742
8 Kyle RA Larson DR Therneau TM et al Long-term follow-up of mono-clonal gammopathy of undetermined significance N Engl J Med 2018[cited 2018 Apr 23] 378 241ndash249 Available from httpwwwncbinlmnihgovpubmed29342381
9 Dispenzieri A Katzmann JA Kyle RA et al Prevalence and risk of progres-sion of light-chain monoclonal gammopathy of undetermined significancea retrospective population-based cohort study Lancet [Internet] 2010[cited 2018 Feb 9] 375 1721ndash1728 Available from httpwwwncbinlmnihgovpubmed20472173
10 Steiner N Gobel G Suchecki P et al Monoclonal gammopathy of renalsignificance (MGRS) increases the risk for progression to multiple mye-loma an observational study of 2935 MGUS patients Oncotarget[Internet] 2018 [cited 2018 Apr 27] 9 2344ndash2356 Available from httpwwwncbinlmnihgovpubmed29416776
11 Dhodapkar MV Sexton R Waheed S et al Clinical genomic andimaging predictors of myeloma progression from asymptomaticmonoclonal gammopathies (SWOG S0120) Blood [Internet] 2014[cited 2018 Jun 22] 123 78ndash85 Available from httpwwwncbinlmnihgovpubmed24144643
12 Zand L Kattah A Fervenza FC et al C3 glomerulonephritis associatedwith monoclonal gammopathy a case series Am J Kidney Dis [Internet]2013 [cited 2017 Dec 29] 62 506ndash514 Available from httpwwwncbinlmnihgovpubmed23623956
13 Rajkumar SV Dimopoulos MA Palumbo A et al International MyelomaWorking Group updated criteria for the diagnosis of multiple myelomaLancet Oncol [Internet] 2014 [cited 2018 Jun 23] 15 e538ndashe548 Availablefrom httplinkinghubelseviercomretrievepiiS1470204514704425
Clinical implication of monoclonal gammopathies 9Downloaded from httpsacademicoupcomndtadvance-article-abstractdoi101093ndtgfy2595086133by gueston 29 August 2018
14 Ravindran A Bartley AC Holton SJ et al Prevalence incidence and sur-vival of smoldering multiple myeloma in the United States Nat PublishingGroup [Internet] 2016 6 2018ndash2023 [cited Jun] Available from httpswwwncbinlmnihgovpmcarticlesPMC5098258pdfbcj2016100apdf
15 Fermand J-P Bridoux F Kyle RA et al How I treat monoclonal gammop-athy of renal significance (MGRS) Blood [Internet] 2013 [cited 2017 Oct27] 122 3583ndash3590 Available from httpwwwncbinlmnihgovpubmed24108460
16 Bridoux F Leung N Hutchison CA et al Diagnosis of monoclonal gamm-opathy of renal significance Kidney Int [Internet] 2015 [cited 2017 Oct24] 87 698ndash711 Available from httpwwwncbinlmnihgovpubmed25607108
17 Kristinsson SY Bjorkholm M Andersson TM-L et al Patterns of survivaland causes of death following a diagnosis of monoclonal gammopathy ofundetermined significance a population-based study Haematologica[Internet] 2009 [cited 2018 Feb] 94 1714ndash1720 Available from httpwwwncbinlmnihgovpubmed19608666
18 Dimopoulos MA Delimpasi S Katodritou E et al Significant improve-ment in the survival of patients with multiple myeloma presenting with se-vere renal impairment after the introduction of novel agents Ann Oncol[Internet] 2014 [cited 2018 Apr 23] 25 195ndash200 Available from httpsacademicoupcomannoncarticle-lookupdoi101093annoncmdt483
19 Correia SO Santos S Malheiro J et al Monoclonal gammopathy of renalsignificance diagnostic workup WJN 2017 [cited 2017 Oct 27] 6 72ndash78Available from httpwwwncbinlmnihgovpubmed28316940
20 Lin J Markowitz GS Valeri AM et al Renal monoclonal immunoglobulindeposition disease the disease spectrum J Am Soc Nephrol [Internet] 2001[cited 2018 Jun 23] 12 1482ndash1492 Available from httpwwwncbinlmnihgovpubmed11423577
21 Sethi S Zand L Leung N et al Membranoproliferative glomerulonephritissecondary to monoclonal gammopathy Clin J Am Soc Nephrol [Internet]2010 [cited 2017 Dec 8] 5 770ndash782 Available from httpwwwncbinlmnihgovpubmed20185597
22 Bhutani G Nasr SH Said SM et al Hematologic characteristics of prolifer-ative glomerulonephritides with nonorganized monoclonal immunoglobu-lin deposits Mayo Clin Proc [Internet] 2015 [cited 2018 Jun 23] 90587ndash596 Available from httpwwwncbinlmnihgovpubmed25939936
23 Cohen C El-Karoui K Alyanakian M-A et al Light and heavy chain depo-sition disease associated with CH1 deletion Clin Kidney J [Internet] 2015[cited 2017 Oct 26] 8 237ndash239 Available from httpwwwncbinlmnihgovpubmed25815184
24 Nasr SH Valeri AM Cornell LD et al Renal monoclonal immunoglobulindeposition disease a report of 64 patients from a single institution Clin JAm Soc Nephrol [Internet] 2012 [cited 2018 Feb 9] 7 231ndash239 Availablefrom httpwwwncbinlmnihgovpubmed22156754
25 Sicard A Karras A Goujon J-M et al Light chain deposition disease with-out glomerular proteinuria a diagnostic challenge for the nephrologistNephrol Dial Transplant [Internet] 2014 [cited 2018 Jul 7] 29 1894ndash1902Available from httpwwwncbinlmnihgovpubmed24619059
26 Haas M A reevaluation of routine electron microscopy in the examinationof native renal biopsies J Am Soc Nephrol [Internet] 1997 8 70ndash76Available from httpwwwncbinlmnihgovpubmed9013450
27 Stokes MB Valeri AM Herlitz L et al Light chain proximal tubulopathyclinical and pathologic characteristics in the modern treatment era J AmSoc Nephrol [Internet] 2016 [cited 2018 Jun 23] 27 1555ndash1565 Availablefrom httpwwwncbinlmnihgovpubmed26374607
28 Larsen CP Messias NC Walker PD et al Membranoproliferative glomeru-lonephritis with masked monotypic immunoglobulin deposits Kidney Int[Internet] 2015 [cited 2018 Feb 10] 88 867ndash873 Available from httpwwwncbinlmnihgovpubmed26154922
29 Eirin A Irazabal MV Gertz MA et al Clinical features of patients with im-munoglobulin light chain amyloidosis (AL) with vascular-limited deposi-tion in the kidney Nephrol Dial Transplant [Internet] 2012 [cited 2018Feb 10] 27 1097ndash1101 Available from httpwwwncbinlmnihgovpubmed22067518
30 Alonso-Titos J Perea-Ortega L Sola E et al C3 glomerulonephritis associ-ated with monoclonal gammopathy of renal significance case report BMCNephrol 2018 Jul 6] 19 129 Available from httpwwwncbinlmnihgovpubmed29884135
31 Sayed RH Wechalekar AD Gilbertson JA et al Natural history and out-come of light chain deposition disease Blood [Internet] 2015 [cited 2017Dec 8] 126 2805ndash2810 Available from httpwwwncbinlmnihgovpubmed26392598
32 Mohan M Buros A Mathur P et al Clinical characteristics and prognosticfactors in multiple myeloma patients with light chain deposition diseaseAm J Hematol 2017 [cited 2018 Jul 7] 92 739ndash745 Available from httpwwwncbinlmnihgovpubmed28383130
33 Vignon M Cohen C Faguer S et al The clinicopathologic characteristicsof kidney diseases related to monotypic IgA deposits Kidney Int [Internet]2017 [cited 2018 Jul] 91 720ndash728 Available from httpwwwncbinlmnihgovpubmed28069266
34 Best Rocha A Larsen CP Membranous glomerulopathy with light chain-restricted deposits a clinicopathological analysis of 28 cases Kidney IntRep [Internet] 2017 [cited 2018 Jul 6] 2 1141ndash1148 Available from httpwwwncbinlmnihgovpubmed29270522
35 Nasr SH Valeri AM Sethi S et al Clinicopathologic correlations in multi-ple myeloma a case series of 190 patients with kidney biopsies Am JKidney Dis [Internet] 2012 [cited 2017 Oct 26] 59 786ndash794 Availablefrom httpwwwncbinlmnihgovpubmed22417785
36 Glavey SV Leung N Monoclonal gammopathy the good the bad and theugly Blood Rev [Internet] 2016 [cited 2017 Dec 24] 30 223ndash231 Availablefrom httpwwwsciencedirectcomsciencearticlepiiS0268960X15000946bb0130
37 Katzmann JA Kyle RA Benson J et al Screening panels for detection ofmonoclonal gammopathies Clin Chem [Internet] 2009 [cited 2017 Oct25] 55 1517ndash1522 Available from httpwwwncbinlmnihgovpubmed19520758
38 Yadav P Leung N Sanders PW et al The use of immunoglobulin lightchain assays in the diagnosis of paraprotein-related kidney disease KidneyInt [Internet] 2015 [cited 2018 Feb 9] 87 692ndash697 Available from httpwwwncbinlmnihgovpubmed25296094
39 Sugihara H Chihara D Seike K et al Percentage of urinary albumin excre-tion and serum-free light-chain reduction are important determinants ofrenal response in myeloma patients with moderate to severe renal impair-ment Blood Cancer J [Internet] 2014 [cited 2018 Jun 24] 4 e235 Availablefrom httpwwwncbinlmnihgovpubmed25083819
40 Leung N Gertz M Kyle RA et al Urinary albumin excretion patterns ofpatients with cast nephropathy and other monoclonal gammopathy-related kidney diseases Clin J Am Soc Nephrol [Internet] 2012 [cited 2018Jun 24] 7 1964ndash1968 Available from httpwwwncbinlmnihgovpubmed23024162
41 Ciocchini M Arbelbide J Musso CG Monoclonal gammopathy of renalsignificance (MGRS) the characteristics and significance of a new meta-entity Int Urol Nephrol [Internet] 2017 [cited 2017 Oct 26] 492171ndash2175 Available from httpwwwncbinlmnihgovpubmed28425076
42 Sethi S Rajkumar SV DrsquoAgati VD The complexity and heterogeneity ofmonoclonal immunoglobulinndashassociated renal diseases J Am Soc Nephrol2018 29 1810ndash1823
43 Hutchison CA Harding S Hewins P et al Quantitative assessment of se-rum and urinary polyclonal free light chains in patients with chronic kid-ney disease Clin J Am Soc Nephrol [Internet] 2008 [cited 2017 Dec 25] 31684ndash1690 Available from httpwwwncbinlmnihgovpubmed18945993
44 Jurczyszyn A Ochrem B Abnormal serum free light chain ratio does notalways indicate monoclonal gammopathy Polskie Archiwum MedycynyWewnetrznej [Internet] 2015 [cited 2017 Dec 29] 125 502ndash504 Availablefrom httpwwwncbinlmnihgovpubmed26266682
45 Singh G Serum free light chain assay and jk ratio performance inpatients with monoclonal gammopathy-high false negative rate for jk ra-tio J Clin Med Res 2017 [cited 2018 Jun 25] 9 46ndash57 Available fromhttpwwwncbinlmnihgovpubmed27924175
46 Fulton RB Fernando SL Serum free light chain assay reduces the need forserum and urine immunofixation electrophoresis in the evaluation ofmonoclonal gammopathy Ann Clin Biochem [Internet] 2009 [cited 2018Jun 25] 46 407ndash412 Available from httpwwwncbinlmnihgovpubmed19641008
10 K Batko et alDownloaded from httpsacademicoupcomndtadvance-article-abstractdoi101093ndtgfy2595086133by gueston 29 August 2018
47 Levinson SS Urine immunofixation electrophoresis remains importantand is complementary to serum free light chain Clin Chem Lab Med[Internet] 2011 [cited 2018 Jun 25] 49 1801ndash1804 Available from httpwwwncbinlmnihgovpubmed21663562 [CrossRef][Mismatch]
48 Lee WS Singh G Serum free light chains in neoplastic monoclonal gam-mopathies relative under-detection of lambda dominant KappaLambdaratio and underproduction of free lambda light chains as compared tokappa light chains in patients with neoplastic monoclonal gammopathiesJ Clin Med Res 2018 [cited 2018 Jun 25] 10 562ndash569 Available fromhttpwwwncbinlmnihgovpubmed29904440
49 Xu B Tang Y Zhou J et al Disease spectrum of abnormal serum free lightchain ratio and its diagnostic significance Oncotarget [Internet] 2017[cited 2017 Dec 29] 8 82268ndash82279 Available from httpwwwncbinlmnihgovpubmed29137262
50 Koo EH Shin J Jang HR et al Diagnostic performances of M-protein testsaccording to the clinical presentations of kidney disease Eur J Intern Med[Internet] 2016 [cited 2018 Feb 9] 33 88ndash92 Available from httpwwwncbinlmnihgovpubmed27421913
51 Gumber R Cohen JB Palmer MB et al A clone-directed approach mayimprove diagnosis and treatment of proliferative glomerulonephritis withmonoclonal immunoglobulin deposits Kidney Int [Internet] 2018 94199ndash205 Available from httpsdoiorg101016jkint201802020
52 Leung N Barnidge DR Hutchison CA Laboratory testing in monoclonalgammopathy of renal significance (MGRS) Clin Chem Lab Med [Internet]2016 [cited 2017 Oct 25] 54 929ndash937 Available from httpwwwncbinlmnihgovpubmed27107835 [CrossRef][Mismatch]
53 Ramirez-Alvarado M Ward CJ Huang BQ et al Differences in immuno-globulin light chain species found in urinary exosomes in light chain amy-loidosis (AL) PLoS ONE [Internet] 2012 [cited 2018 Jul 7] 7 e38061Available from httpwwwncbinlmnihgovpubmed22723846
54 Hogan JJ Weiss BM Bridging the divide an onco-nephrologic approachto the monoclonal gammopathies of renal significance Clin J Am SocNephrol [Internet] 2016 [cited 2017 Oct 26] 11 1681ndash1691 Availablefrom httpwwwncbinlmnihgovpubmed27416775
55 Vij R Mazumder A Klinger M et al Deep sequencing reveals myelomacells in peripheral blood in majority of multiple myeloma patients ClinLymphoma Myeloma Leuk [Internet] 2014 [cited 2017 Oct 25] 14131ndash139e1 Available from httpwwwncbinlmnihgovpubmed24629890
56 Gonsalves WI Leung N Rajkumar SV et al Improvement in renal func-tion and its impact on survival in patients with newly diagnosed multiplemyeloma Blood Cancer J 2015 [cited 2018 Feb 3] 5 e296 Available fromhttpwwwnaturecomdoifinder101038bcj201520
57 Dimopoulos MA Cheung MC Roussel M et al Impact of renal impair-ment on outcomes with lenalidomide and dexamethasone treatment in theFIRST trial a randomized open-label phase 3 trial in transplant-ineligiblepatients with multiple myeloma Haematologica [Internet] 2016 [cited2018 Jul 7] 101 363ndash370 Available from httpwwwncbinlmnihgovpubmed26659916
58 Ponisch W Andrea M Wagner I et al Successful treatment of patientswith newly diagnoseduntreated multiple myeloma and advanced renalfailure using bortezomib in combination with bendamustine and predni-sone J Cancer Res Clin Oncol 2012 [cited 2018 Jul 2] 138 1405ndash1412Available from httpwwwncbinlmnihgovpubmed22526157
59 Perry M Delarche A Ribes D et al Rituximab-cyclophosphamide-dexa-methasone is highly effective in patients with monoclonal Ig deposit-related glomerulopathy and indolent non-Hodgkin lymphomas Am JHematol 2014 [cited 2018 Jul 1] 89 969ndash973 Available from httpdoiwileycom101002ajh23798
60 Dimopoulos M Weisel K van de Donk Nwcj et al Pomalidomide pluslow-dose dexamethasone in patients with relapsedrefractory multiple my-eloma and renal impairment results from a Phase II trial J Clin Oncol2018 36 2035ndash2043
61 Fervenza FC Canetta PA Barbour SJ et al A multicenter randomized con-trolled trial of rituximab versus cyclosporine in the treatment of idiopathicmembranous nephropathy (MENTOR) Nephron [Internet] 2015 [cited2017 Dec 25] 130 159ndash168 Available from httpwwwncbinlmnihgovpubmed26087670
62 Dimopoulos MA Richardson PG Schlag R et al VMP (bortezomib mel-phalan and prednisone) is active and well tolerated in newly diagnosedpatients with multiple myeloma with moderately impaired renal functionand results in reversal of renal impairment cohort analysis of the Phase IIIVISTA study JCO 2009 [cited 2017 Dec 8] 27 6086ndash6093 Available fromhttpwwwncbinlmnihgovpubmed19858394
63 Morabito F Gentile M Mazzone C et al Safety and efficacy ofbortezomib-melphalan-prednisone-thalidomide followed by bortezomib-thalidomide maintenance (VMPT-VT) versus bortezomib-melphalan-prednisone (VMP) in untreated multiple myeloma patients with renal im-pairment Blood [Internet] 2011 [cited 2017 Dec 9] 118 5759ndash5766Available from httpwwwncbinlmnihgovpubmed21951682
64 Moreau P Masszi T Grzasko N et al Oral ixazomib lenalidomide anddexamethasone for multiple myeloma N Engl J Med 2016 [cited 2018 Apr27] 374 1621ndash1634 Available from httpwwwnejmorgdoi101056NEJMoa1516282
65 Nordstrom BL Knopf KB Teltsch DY et al The safety of bendamustine inpatients with chronic lymphocytic leukemia or non-Hodgkin lymphomaand concomitant renal impairment a retrospective electronic medical re-cord database analysis Leuk Lymphoma [Internet] 2014 [cited 2017 Dec13] 55 1266ndash1273 Available from httpwwwncbinlmnihgovpubmed23987821
66 Roussou M Kastritis E Christoulas D et al Reversibility of renal failure innewly diagnosed patients with multiple myeloma and the role of novelagents Leuk Res [Internet] 2010 [cited 2017 Dec 15] 34 1395ndash1397Available from httpwwwncbinlmnihgovpubmed20510452
67 Tosi P Zamagni E Tacchetti P et al Thalidomide-dexamethasone as in-duction therapy before autologous stem cell transplantation in patientswith newly diagnosed multiple myeloma and renal insufficiency BiolBlood Marrow Transplant [Internet] 2010 [cited 2018 Apr 27] 161115ndash1121 Available from httpwwwncbinlmnihgovpubmed20197100
68 Dimopoulos M Alegre A Stadtmauer EA et al The efficacy and safety oflenalidomide plus dexamethasone in relapsed andor refractory multiplemyeloma patients with impaired renal function Cancer [Internet] 2010116 3807 [cited 2017 Dec 15] Available from httpwwwncbinlmnihgovpubmed20564094
69 Siegel DS Weisel KC Dimopoulos MA et al Pomalidomide plus low-dosedexamethasone in patients with relapsedrefractory multiple myeloma andmoderate renal impairment a pooled analysis of three clinical trials LeukLymphoma [Internet] 2016 [cited 2017 Dec 15] 57 2833ndash2838 Availablefrom httpwwwncbinlmnihgovpubmed27267105
70 Dimopoulos MA Goldschmidt H Niesvizky R et al Carfilzomib or borte-zomib in relapsed or refractory multiple myeloma (ENDEAVOR) an in-terim overall survival analysis of an open-label randomised phase 3 trialLancet Oncol [Internet] 2017 [cited 2017 Dec 6] 18 1327ndash1337 Availablefrom httpwwwncbinlmnihgovpubmed28843768
71 Telio D Shepherd J Forrest D et al High-dose melphalan followed byauto-SCT has favorable safety and efficacy in selected patients with lightchain deposition disease and light and heavy chain deposition diseaseBone Marrow Transplant 2012 [cited 2017 Dec 8] 47 453ndash455 Availablefrom httpwwwnaturecomdoifinder101038bmt201187
72 Batalini F Econimo L Quillen K et al High-dose melphalan and stem celltransplantation in patients on dialysis due to immunoglobulin light-chainamyloidosis and monoclonal immunoglobulin deposition disease BiolBlood Marrow Transplant [Internet] 2018 [cited 2017 Dec 25] 24127ndash132 Available from httpwwwncbinlmnihgovpubmed28865972
73 Kourelis TV Nasr SH Dispenzieri A et al Outcomes of patients with renalmonoclonal immunoglobulin deposition disease Am J Hematol 2016[cited 2018 Jul 2] 91 1123ndash1128 Available from httpwwwncbinlmnihgovpubmed27501122
74 Pozzi C DrsquoAmico M Fogazzi GB et al Light chain deposition disease withrenal involvement clinical characteristics and prognostic factors Am JKidney Dis [Internet] 2003 [cited 2018 Jun 23] 42 1154ndash1163 Availablefrom httpwwwncbinlmnihgovpubmed14655186
75 Song M-K Chung J-S Shin H-J et al Cyclophosphamide-containing regi-men (TCD) is superior to melphalan-containing regimen (MPT) in elderlymultiple myeloma patients with renal impairment Ann Hematol
Clinical implication of monoclonal gammopathies 11Downloaded from httpsacademicoupcomndtadvance-article-abstractdoi101093ndtgfy2595086133by gueston 29 August 2018
[Internet] 2012 [cited 2017 Dec 9] 91 889ndash896 Available from httpwwwncbinlmnihgovpubmed22237937
76 Specter R Sanchorawala V Seldin DC et al Kidney dysfunction duringlenalidomide treatment for AL amyloidosis Nephrol Dial Transplant[Internet] 2011 [cited 2018 Jul 7] 26 881ndash886 Available from httpwwwncbinlmnihgovpubmed20693160
77 Li Y Wang X OrsquoMara E et al Population pharmacokinetics of pomalido-mide in patients with relapsed or refractory multiple myeloma with variousdegrees of impaired renal function CPAA 2017 [cited 2018 Feb 4] 9133ndash145 Available from httpwwwncbinlmnihgovpubmed29184451
78 Kastritis E Gavriatopoulou M Roussou M et al Addition of cyclophos-phamide and higher doses of dexamethasone do not improve outcomes ofpatients with AL amyloidosis treated with bortezomib Blood Cancer J2017 [cited 2017 Dec 15] 7 e570 Available from httpwwwncbinlmnihgovpubmed28622303
79 Venner CP Gillmore JD Sachchithanantham S et al A matched compari-son of cyclophosphamide bortezomib and dexamethasone (CVD) versusrisk-adapted cyclophosphamide thalidomide and dexamethasone (CTD)in AL amyloidosis Leukemia [Internet] 2014 [cited 2018 Jul 5] 282304ndash2310 Available from httpwwwncbinlmnihgovpubmed25027514
80 Palladini G Sachchithanantham S Milani P et al A European collabora-tive study of cyclophosphamide bortezomib and dexamethasone inupfront treatment of systemic AL amyloidosis Blood [Internet] 2015[cited 2017 Dec 9] 126 612ndash615 Available from httpwwwncbinlmnihgovpubmed25987656
81 Kopel T Kaufman JS Hamburg N et al Endothelium-dependent and -in-dependent vascular function in advanced chronic kidney disease CJASN2017 [cited 2018 Apr 18] 12 1588ndash1594 Available from httpcjasnasnjournalsorglookupdoi102215CJN12811216
82 Palladini G Milani P Foli A et al A Phase 2 trial of pomalidomide anddexamethasone rescue treatment in patients with AL amyloidosis Blood[Internet] 2017 [cited 2018 Apr 26] 129 2120ndash2123 Available fromhttpwwwncbinlmnihgovpubmed28130212
83 Hegenbart U Bochtler T Benner A et al Lenalidomidemelphalandexa-methasone in newly diagnosed patients with immunoglobulin light chainamyloidosis results of a prospective phase 2 study with long-term followup Haematologica [Internet] 2017 [cited 2017 Dec 26] 102 1424ndash1431Available from httpwwwncbinlmnihgovpubmed28522573
84 Palladini G Milani P Foli A et al Oral melphalan and dexamethasonegrants extended survival with minimal toxicity in AL amyloidosis long-term results of a risk-adapted approach Haematologica [Internet] 2014[cited 2017 Dec 15] 99 743ndash750 Available from httpwwwncbinlmnihgovpubmed24213149
85 Payet J Livartowski J Kavian N et al Type I cryoglobulinemia in multiplemyeloma a rare entity analysis of clinical and biological characteristics ofseven cases and review of the literature Leuk Lymphoma [Internet] 201354 767ndash777 Available from httpwwwtandfonlinecomdoifull103109104281942012671481
86 Terpos E Kleber M Engelhardt M et al European Myeloma Networkguidelines for the management of multiple myeloma-related complica-tions Haematologica [Internet] 2015 [cited 2017 Dec 4] 100 1254ndash1266Available from httpwwwncbinlmnihgovpubmed26432383
87 Chanan-Khan AA Kaufman JL Mehta J et al Activity and safety of borte-zomib in multiple myeloma patients with advanced renal failure a multi-center retrospective study Blood [Internet] 2007 [cited 2018 Jul 2] 1092604ndash2606 Available from httpwwwncbinlmnihgovpubmed17138816
88 Dimopoulos MA Roussou M Gkotzamanidou M et al The role of novelagents on the reversibility of renal impairment in newly diagnosed symp-tomatic patients with multiple myeloma Leukemia 2013 27 423ndash429
89 Kouroukis TC Baldassarre FG Haynes AE et al Bortezomib in multiplemyeloma systematic review and clinical considerations Curr Oncol(Toronto Ont) [Internet] 2014 [cited 2017 Dec 4] 21 e573ndashe603Available from httpwwwncbinlmnihgovpubmed25089109
90 Zhu W Chen W Bortezomib-based treatment for multiple myelomapatients with renal impairment a systematic review and meta-analysis ofobservational studies Medicine [Internet] 2016 95 e5202 Available fromhttpwwwncbinlmnihgovpmcarticlesPMC5120900
91 Dimopoulos MA Terpos E Chanan-Khan A et al Renal impairment inpatients with multiple myeloma a consensus statement on behalf of theInternational Myeloma Working Group JCO 2010 28 4976ndash4984
92 Chauvet S Fremeaux-Bacchi V Petitprez F et al Treatment of B-cell disor-der improves renal outcome of patients with monoclonal gammopathyndashassociated C3 glomerulopathy Blood [Internet] 2017 [cited 2017 Oct 26]129 1437ndash1447 Available from httpwwwncbinlmnihgovpubmed28069603
93 Cohen C Royer B Javaugue V et al Bortezomib produces high hematolog-ical response rates with prolonged renal survival in monoclonal immuno-globulin deposition disease Kidney Int [Internet] 2015 [cited 2017 Dec25] 88 1135ndash1143 Available from httpwwwncbinlmnihgovpubmed26176826
94 Ziogas DC Kastritis E Terpos E et al Hematologic and renal improve-ment of monoclonal immunoglobulin deposition disease after treatmentwith bortezomib-based regimens Leuk Lymphoma [Internet] 2017 [cited2017 Dec 25] 58 1832ndash1839 Available from httpwwwncbinlmnihgovpubmed27967286
95 Milani P Merlini G Palladini G Novel therapies in light chain amyloid-osis Kidney Int Rep [Internet] 2018 [cited 2018 Jul 4] 3 530ndash541 Availablefrom httpwwwncbinlmnihgovpubmed29854961
96 Spizzo G Mitterer M Gunsilius E Bortezomib for the treatment of refrac-tory Type-1 cryoglobulinaemia Br J Haematol [Internet] 2010 [cited 2018Jul 7] 150 235ndash237 Available from httpdoiwileycom101111j1365-2141201008184x
97 Talamo G Claxton D Tricot G et al Response to bortezomib in refractoryType I cryoglobulinemia Am J Hematol 2008 [cited 2018 Jul 7] 83883ndash884 Available from httpwwwncbinlmnihgovpubmed18756542
98 Dimopoulos MA Roussou M Gavriatopoulou M et al Cardiac and renalcomplications of carfilzomib in patients with multiple myeloma BloodAdv 2017 [cited 2017 Dec 6] 1 449ndash454 Available from httpwwwbloodadvancesorglookupdoi101182bloodadvances2016003269
99 Strati P Nasr SH Leung N et al Renal complications in chronic lympho-cytic leukemia and monoclonal B-cell lymphocytosis the Mayo Clinic ex-perience Haematologica [Internet] 2015 [cited 2018 Jul 3] 100 1180ndash1188Available from httpwwwncbinlmnihgovpubmed26088927
100 Salama AD Pusey CD Drug insight rituximab in renal disease and trans-plantation Nat Clin Pract Nephrol [Internet] 2006 [cited 2017 Dec 8] 2221ndash230 Available from httpwwwnaturecomdoifinder101038ncpneph0133
101 Jillella AP Dainer PM Kallab AM et al Treatment of a patient with end-stage renal disease with rituximab pharmacokinetic evaluation suggestsrituximab is not eliminated by hemodialysis Am J Hematol 2002 [cited2018 Jul] 71 219ndash222 Available from httpwwwncbinlmnihgovpubmed12410580
102 Guiard E Karras A Plaisier E et al Patterns of noncryoglobulinemic glo-merulonephritis with monoclonal Ig deposits correlation with IgG sub-class and response to rituximab Clin J Am Soc Nephrol 2011 6 1609ndash1616
103 Ribes D Hachem HEL Oberic L et al Bendamustine plus rituximab forindolent B-cell lymphoma of renal significance Am J Hematol 2018 93356ndash362
104 Darwish M Bond M Hellriegel E et al Pharmacokinetic and pharmacody-namic profile of bendamustine and its metabolites Cancer ChemotherPharmacol 2015 [cited 2017 Dec 15] 75 1143ndash1154 Available from httpwwwncbinlmnihgovpubmed25829094
105 Ponisch W Moll B Bourgeois M et al Bendamustine and prednisone incombination with bortezomib (BPV) in the treatment of patients with re-lapsed or refractory multiple myeloma and light chain-induced renal fail-ure J Cancer Res Clin Oncol [Internet] 2013 [cited 2018 Jul 2] 1391937ndash1946 Available from httpwwwncbinlmnihgovpubmed24046251
106 Mateos M-V Dimopoulos MA Cavo M et al Daratumumab plus bortezo-mib melphalan and prednisone for untreated myeloma N Engl J Med2018 378 518ndash528
107 Rocchi S Tacchetti P Pantani L et al Safety and efficacy of daratumumabin dialysis-dependent renal failure secondary to multiple myelomaHaematologica [Internet] 2018 [cited 2018 Jul 2] 103 e277ndashe278 Availablefrom httpwwwncbinlmnihgovpubmed29622654
12 K Batko et alDownloaded from httpsacademicoupcomndtadvance-article-abstractdoi101093ndtgfy2595086133by gueston 29 August 2018
108 Anand S Miller D Chipman G Morris D Srinivas S Daratumumab forsevere refractory proliferative glomerulonephritis with monoclonal im-mune deposits (PGNMID) ATC Abstr [Internet] 2017 [cited 2018 Jul 3]Available from httpsatcmeetingabstractscomabstractdaratumumab-for-severe-refractory-proliferative-glomerulonephritis-with-monoclonal-immune-deposits-pgnmid
109 Leung N Lager DJ Gertz MA et al Long-term outcome of renal transplan-tation in light-chain deposition disease Am J Kidney Dis [Internet] 2004[cited 2018 Feb 9] 43 147ndash153 Available from httpwwwncbinlmnihgovpubmed14712438
110 Lorenz EC Sethi S Leung N et al Recurrent membranoproliferative glo-merulonephritis after kidney transplantation Kidney Int [Internet] 2010[cited 2018 Feb 9] 77 721ndash728 Available from httpwwwncbinlmnihgovpubmed20130531
111 Leung N Nasr SH A patient with abnormal kidney function and a mono-clonal light chain in the urine Clin J Am Soc Nephrol 2016 11 1073ndash1082
112 Cibeira MT Sanchorawala V Seldin DC et al Outcome of AL amyloidosisafter high-dose melphalan and autologous stem cell transplantation long-term results in a series of 421 patients Blood [Internet] 2011 [cited 2018Feb 3] 118 4346ndash4352 Available from httpwwwncbinlmnihgovpubmed21828140
113 Gertz MA Lacy MQ Dispenzieri A et al Autologous stem cell transplantfor immunoglobulin light chain amyloidosis a status report LeukLymphoma [Internet] 2010 [cited 2018 Feb 3] 51 2181ndash2187 Availablefrom httpwwwncbinlmnihgovpubmed20958232
114 Leung N Kumar SK Glavey SV et al The impact of dialysis on the survivalof patients with immunoglobulin light chain (AL) amyloidosis undergoingautologous stem cell transplantation Nephrol Dial Transplant 2016 [cited2018 Jul 7] 31 1284ndash1289 Available from httpsacademicoupcomndtarticle-lookupdoi101093ndtgfv328
115 Badros A Barlogie B Siegel E et al Results of autologous stem cell trans-plant in multiple myeloma patients with renal failure Br J Haematol 2001[cited 2018 Jul 7] 114 822ndash829 Available from httpwwwncbinlmnihgovpubmed11564069
116 Soltero L Carbajal H Xu J et al Initial survival data of kidney transplantpatients with pre-transplant monoclonal gammopathy Clin Transplant[Internet] 2012 [cited 2018 Feb 3] 26 300ndash304 Available from httpwwwncbinlmnihgovpubmed22044717
117 Jimenez-Zepeda VH Heilman RL Engel RA et al Monoclonal gammopathyof undetermined significance does not affect outcomes in patients undergoingsolid organ transplants Transplantation [Internet] 2011 [cited 2018 Feb 3]92 570ndash574 Available from httpwwwncbinlmnihgovpubmed21712755
118 Naina HVK Harris S Dispenzieri A et al Long-term follow-up of patientswith monoclonal gammopathy of undetermined significance after kidney
transplantation Am J Nephrol 2012 [cited 2018 Feb] 35 365ndash371Available from httpwwwncbinlmnihgovpubmed22473253
119 Bansal T Garg A Snowden JA et al Defining the role of renal transplanta-tion in the modern management of multiple myeloma and other plasmacell dyscrasias Nephron Clin Pract [Internet] 2012 [cited 2018 Feb 3] 120c228 wwwkargercom
120 Hassoun H Flombaum C DrsquoAgati VD et al High-dose melphalan andauto-SCT in patients with monoclonal Ig deposition disease Bone MarrowTransplant 2008 [cited 2018 Feb 3] 42 405ndash412 Available from httpwwwncbinlmnihgovpubmed18574442
121 Herrmann SMS Gertz MA Stegall MD et al Long-term outcomes ofpatients with light chain amyloidosis (AL) after renal transplantation withor without stem cell transplantation Nephrol Dial Transplant [Internet]2011 [cited 2018 Feb 3] 26 2032ndash2036 Available from httpwwwncbinlmnihgovpubmed21543655
122 Lorenz EC Gertz MA Fervenza FC et al Long-term outcome of autolo-gous stem cell transplantation in light chain deposition disease NephrolDial Transplant [Internet] 2008 [cited 2018 Jul 5] 23 2052ndash2057 Availablefrom httpwwwncbinlmnihgovpubmed18178602
123 Merhi B Patel N Bayliss G et al Proliferative glomerulonephritis withmonoclonal IgG deposits in two kidney allografts successfully treated withrituximab Clin Kidney J [Internet] 2017 [cited 2018 Feb 10] 10 405ndash410Available from httpsacademicoupcomckjarticle-lookupdoi101093ckjsfx001
124 Barbour SJ Beaulieu MC Zalunardo NY et al Proliferative glomerulone-phritis with monoclonal IgG deposits secondary to chronic lymphocyticleukemia Report of two cases Nephrol Dial Transplant [Internet] 2011[cited 2018 Feb 10] 26 2712ndash2714 Available from httpsacademicoupcomndtarticle-lookupdoi101093ndtgfr251
125 Zand L Lorenz EC Cosio FG et al Clinical findings pathology and out-comes of C3GN after kidney transplantation J Am Soc Nephrol [Internet]2014 [cited 2018 Jul 5] 25 1110ndash1117 Available from httpwwwncbinlmnihgovpubmed24357668
126 Alfano G Fontana F Colaci E et al Monoclonal gammopathy of undeter-mined significance after kidney transplantation Transplantation [Internet]2017 [cited 2017 Oct 24] 101 e337ndashe342 Available from httpwwwncbinlmnihgovpubmed28731904
127 Bancu I Ca~nas L Juega FJ et al Outcomes of monoclonal gammopathyof undetermined significance in patients who underwent kidneytransplantation Transplant Proc [Internet] 2015 [cited 2018 Feb 10] 472344ndash2345 Available from httpwwwncbinlmnihgovpubmed26518922
Received 2632018 Editorial decision 1472018
Clinical implication of monoclonal gammopathies 13Downloaded from httpsacademicoupcomndtadvance-article-abstractdoi101093ndtgfy2595086133by gueston 29 August 2018

14 Ravindran A Bartley AC Holton SJ et al Prevalence incidence and sur-vival of smoldering multiple myeloma in the United States Nat PublishingGroup [Internet] 2016 6 2018ndash2023 [cited Jun] Available from httpswwwncbinlmnihgovpmcarticlesPMC5098258pdfbcj2016100apdf
15 Fermand J-P Bridoux F Kyle RA et al How I treat monoclonal gammop-athy of renal significance (MGRS) Blood [Internet] 2013 [cited 2017 Oct27] 122 3583ndash3590 Available from httpwwwncbinlmnihgovpubmed24108460
16 Bridoux F Leung N Hutchison CA et al Diagnosis of monoclonal gamm-opathy of renal significance Kidney Int [Internet] 2015 [cited 2017 Oct24] 87 698ndash711 Available from httpwwwncbinlmnihgovpubmed25607108
17 Kristinsson SY Bjorkholm M Andersson TM-L et al Patterns of survivaland causes of death following a diagnosis of monoclonal gammopathy ofundetermined significance a population-based study Haematologica[Internet] 2009 [cited 2018 Feb] 94 1714ndash1720 Available from httpwwwncbinlmnihgovpubmed19608666
18 Dimopoulos MA Delimpasi S Katodritou E et al Significant improve-ment in the survival of patients with multiple myeloma presenting with se-vere renal impairment after the introduction of novel agents Ann Oncol[Internet] 2014 [cited 2018 Apr 23] 25 195ndash200 Available from httpsacademicoupcomannoncarticle-lookupdoi101093annoncmdt483
19 Correia SO Santos S Malheiro J et al Monoclonal gammopathy of renalsignificance diagnostic workup WJN 2017 [cited 2017 Oct 27] 6 72ndash78Available from httpwwwncbinlmnihgovpubmed28316940
20 Lin J Markowitz GS Valeri AM et al Renal monoclonal immunoglobulindeposition disease the disease spectrum J Am Soc Nephrol [Internet] 2001[cited 2018 Jun 23] 12 1482ndash1492 Available from httpwwwncbinlmnihgovpubmed11423577
21 Sethi S Zand L Leung N et al Membranoproliferative glomerulonephritissecondary to monoclonal gammopathy Clin J Am Soc Nephrol [Internet]2010 [cited 2017 Dec 8] 5 770ndash782 Available from httpwwwncbinlmnihgovpubmed20185597
22 Bhutani G Nasr SH Said SM et al Hematologic characteristics of prolifer-ative glomerulonephritides with nonorganized monoclonal immunoglobu-lin deposits Mayo Clin Proc [Internet] 2015 [cited 2018 Jun 23] 90587ndash596 Available from httpwwwncbinlmnihgovpubmed25939936
23 Cohen C El-Karoui K Alyanakian M-A et al Light and heavy chain depo-sition disease associated with CH1 deletion Clin Kidney J [Internet] 2015[cited 2017 Oct 26] 8 237ndash239 Available from httpwwwncbinlmnihgovpubmed25815184
24 Nasr SH Valeri AM Cornell LD et al Renal monoclonal immunoglobulindeposition disease a report of 64 patients from a single institution Clin JAm Soc Nephrol [Internet] 2012 [cited 2018 Feb 9] 7 231ndash239 Availablefrom httpwwwncbinlmnihgovpubmed22156754
25 Sicard A Karras A Goujon J-M et al Light chain deposition disease with-out glomerular proteinuria a diagnostic challenge for the nephrologistNephrol Dial Transplant [Internet] 2014 [cited 2018 Jul 7] 29 1894ndash1902Available from httpwwwncbinlmnihgovpubmed24619059
26 Haas M A reevaluation of routine electron microscopy in the examinationof native renal biopsies J Am Soc Nephrol [Internet] 1997 8 70ndash76Available from httpwwwncbinlmnihgovpubmed9013450
27 Stokes MB Valeri AM Herlitz L et al Light chain proximal tubulopathyclinical and pathologic characteristics in the modern treatment era J AmSoc Nephrol [Internet] 2016 [cited 2018 Jun 23] 27 1555ndash1565 Availablefrom httpwwwncbinlmnihgovpubmed26374607
28 Larsen CP Messias NC Walker PD et al Membranoproliferative glomeru-lonephritis with masked monotypic immunoglobulin deposits Kidney Int[Internet] 2015 [cited 2018 Feb 10] 88 867ndash873 Available from httpwwwncbinlmnihgovpubmed26154922
29 Eirin A Irazabal MV Gertz MA et al Clinical features of patients with im-munoglobulin light chain amyloidosis (AL) with vascular-limited deposi-tion in the kidney Nephrol Dial Transplant [Internet] 2012 [cited 2018Feb 10] 27 1097ndash1101 Available from httpwwwncbinlmnihgovpubmed22067518
30 Alonso-Titos J Perea-Ortega L Sola E et al C3 glomerulonephritis associ-ated with monoclonal gammopathy of renal significance case report BMCNephrol 2018 Jul 6] 19 129 Available from httpwwwncbinlmnihgovpubmed29884135
31 Sayed RH Wechalekar AD Gilbertson JA et al Natural history and out-come of light chain deposition disease Blood [Internet] 2015 [cited 2017Dec 8] 126 2805ndash2810 Available from httpwwwncbinlmnihgovpubmed26392598
32 Mohan M Buros A Mathur P et al Clinical characteristics and prognosticfactors in multiple myeloma patients with light chain deposition diseaseAm J Hematol 2017 [cited 2018 Jul 7] 92 739ndash745 Available from httpwwwncbinlmnihgovpubmed28383130
33 Vignon M Cohen C Faguer S et al The clinicopathologic characteristicsof kidney diseases related to monotypic IgA deposits Kidney Int [Internet]2017 [cited 2018 Jul] 91 720ndash728 Available from httpwwwncbinlmnihgovpubmed28069266
34 Best Rocha A Larsen CP Membranous glomerulopathy with light chain-restricted deposits a clinicopathological analysis of 28 cases Kidney IntRep [Internet] 2017 [cited 2018 Jul 6] 2 1141ndash1148 Available from httpwwwncbinlmnihgovpubmed29270522
35 Nasr SH Valeri AM Sethi S et al Clinicopathologic correlations in multi-ple myeloma a case series of 190 patients with kidney biopsies Am JKidney Dis [Internet] 2012 [cited 2017 Oct 26] 59 786ndash794 Availablefrom httpwwwncbinlmnihgovpubmed22417785
36 Glavey SV Leung N Monoclonal gammopathy the good the bad and theugly Blood Rev [Internet] 2016 [cited 2017 Dec 24] 30 223ndash231 Availablefrom httpwwwsciencedirectcomsciencearticlepiiS0268960X15000946bb0130
37 Katzmann JA Kyle RA Benson J et al Screening panels for detection ofmonoclonal gammopathies Clin Chem [Internet] 2009 [cited 2017 Oct25] 55 1517ndash1522 Available from httpwwwncbinlmnihgovpubmed19520758
38 Yadav P Leung N Sanders PW et al The use of immunoglobulin lightchain assays in the diagnosis of paraprotein-related kidney disease KidneyInt [Internet] 2015 [cited 2018 Feb 9] 87 692ndash697 Available from httpwwwncbinlmnihgovpubmed25296094
39 Sugihara H Chihara D Seike K et al Percentage of urinary albumin excre-tion and serum-free light-chain reduction are important determinants ofrenal response in myeloma patients with moderate to severe renal impair-ment Blood Cancer J [Internet] 2014 [cited 2018 Jun 24] 4 e235 Availablefrom httpwwwncbinlmnihgovpubmed25083819
40 Leung N Gertz M Kyle RA et al Urinary albumin excretion patterns ofpatients with cast nephropathy and other monoclonal gammopathy-related kidney diseases Clin J Am Soc Nephrol [Internet] 2012 [cited 2018Jun 24] 7 1964ndash1968 Available from httpwwwncbinlmnihgovpubmed23024162
41 Ciocchini M Arbelbide J Musso CG Monoclonal gammopathy of renalsignificance (MGRS) the characteristics and significance of a new meta-entity Int Urol Nephrol [Internet] 2017 [cited 2017 Oct 26] 492171ndash2175 Available from httpwwwncbinlmnihgovpubmed28425076
42 Sethi S Rajkumar SV DrsquoAgati VD The complexity and heterogeneity ofmonoclonal immunoglobulinndashassociated renal diseases J Am Soc Nephrol2018 29 1810ndash1823
43 Hutchison CA Harding S Hewins P et al Quantitative assessment of se-rum and urinary polyclonal free light chains in patients with chronic kid-ney disease Clin J Am Soc Nephrol [Internet] 2008 [cited 2017 Dec 25] 31684ndash1690 Available from httpwwwncbinlmnihgovpubmed18945993
44 Jurczyszyn A Ochrem B Abnormal serum free light chain ratio does notalways indicate monoclonal gammopathy Polskie Archiwum MedycynyWewnetrznej [Internet] 2015 [cited 2017 Dec 29] 125 502ndash504 Availablefrom httpwwwncbinlmnihgovpubmed26266682
45 Singh G Serum free light chain assay and jk ratio performance inpatients with monoclonal gammopathy-high false negative rate for jk ra-tio J Clin Med Res 2017 [cited 2018 Jun 25] 9 46ndash57 Available fromhttpwwwncbinlmnihgovpubmed27924175
46 Fulton RB Fernando SL Serum free light chain assay reduces the need forserum and urine immunofixation electrophoresis in the evaluation ofmonoclonal gammopathy Ann Clin Biochem [Internet] 2009 [cited 2018Jun 25] 46 407ndash412 Available from httpwwwncbinlmnihgovpubmed19641008
10 K Batko et alDownloaded from httpsacademicoupcomndtadvance-article-abstractdoi101093ndtgfy2595086133by gueston 29 August 2018
47 Levinson SS Urine immunofixation electrophoresis remains importantand is complementary to serum free light chain Clin Chem Lab Med[Internet] 2011 [cited 2018 Jun 25] 49 1801ndash1804 Available from httpwwwncbinlmnihgovpubmed21663562 [CrossRef][Mismatch]
48 Lee WS Singh G Serum free light chains in neoplastic monoclonal gam-mopathies relative under-detection of lambda dominant KappaLambdaratio and underproduction of free lambda light chains as compared tokappa light chains in patients with neoplastic monoclonal gammopathiesJ Clin Med Res 2018 [cited 2018 Jun 25] 10 562ndash569 Available fromhttpwwwncbinlmnihgovpubmed29904440
49 Xu B Tang Y Zhou J et al Disease spectrum of abnormal serum free lightchain ratio and its diagnostic significance Oncotarget [Internet] 2017[cited 2017 Dec 29] 8 82268ndash82279 Available from httpwwwncbinlmnihgovpubmed29137262
50 Koo EH Shin J Jang HR et al Diagnostic performances of M-protein testsaccording to the clinical presentations of kidney disease Eur J Intern Med[Internet] 2016 [cited 2018 Feb 9] 33 88ndash92 Available from httpwwwncbinlmnihgovpubmed27421913
51 Gumber R Cohen JB Palmer MB et al A clone-directed approach mayimprove diagnosis and treatment of proliferative glomerulonephritis withmonoclonal immunoglobulin deposits Kidney Int [Internet] 2018 94199ndash205 Available from httpsdoiorg101016jkint201802020
52 Leung N Barnidge DR Hutchison CA Laboratory testing in monoclonalgammopathy of renal significance (MGRS) Clin Chem Lab Med [Internet]2016 [cited 2017 Oct 25] 54 929ndash937 Available from httpwwwncbinlmnihgovpubmed27107835 [CrossRef][Mismatch]
53 Ramirez-Alvarado M Ward CJ Huang BQ et al Differences in immuno-globulin light chain species found in urinary exosomes in light chain amy-loidosis (AL) PLoS ONE [Internet] 2012 [cited 2018 Jul 7] 7 e38061Available from httpwwwncbinlmnihgovpubmed22723846
54 Hogan JJ Weiss BM Bridging the divide an onco-nephrologic approachto the monoclonal gammopathies of renal significance Clin J Am SocNephrol [Internet] 2016 [cited 2017 Oct 26] 11 1681ndash1691 Availablefrom httpwwwncbinlmnihgovpubmed27416775
55 Vij R Mazumder A Klinger M et al Deep sequencing reveals myelomacells in peripheral blood in majority of multiple myeloma patients ClinLymphoma Myeloma Leuk [Internet] 2014 [cited 2017 Oct 25] 14131ndash139e1 Available from httpwwwncbinlmnihgovpubmed24629890
56 Gonsalves WI Leung N Rajkumar SV et al Improvement in renal func-tion and its impact on survival in patients with newly diagnosed multiplemyeloma Blood Cancer J 2015 [cited 2018 Feb 3] 5 e296 Available fromhttpwwwnaturecomdoifinder101038bcj201520
57 Dimopoulos MA Cheung MC Roussel M et al Impact of renal impair-ment on outcomes with lenalidomide and dexamethasone treatment in theFIRST trial a randomized open-label phase 3 trial in transplant-ineligiblepatients with multiple myeloma Haematologica [Internet] 2016 [cited2018 Jul 7] 101 363ndash370 Available from httpwwwncbinlmnihgovpubmed26659916
58 Ponisch W Andrea M Wagner I et al Successful treatment of patientswith newly diagnoseduntreated multiple myeloma and advanced renalfailure using bortezomib in combination with bendamustine and predni-sone J Cancer Res Clin Oncol 2012 [cited 2018 Jul 2] 138 1405ndash1412Available from httpwwwncbinlmnihgovpubmed22526157
59 Perry M Delarche A Ribes D et al Rituximab-cyclophosphamide-dexa-methasone is highly effective in patients with monoclonal Ig deposit-related glomerulopathy and indolent non-Hodgkin lymphomas Am JHematol 2014 [cited 2018 Jul 1] 89 969ndash973 Available from httpdoiwileycom101002ajh23798
60 Dimopoulos M Weisel K van de Donk Nwcj et al Pomalidomide pluslow-dose dexamethasone in patients with relapsedrefractory multiple my-eloma and renal impairment results from a Phase II trial J Clin Oncol2018 36 2035ndash2043
61 Fervenza FC Canetta PA Barbour SJ et al A multicenter randomized con-trolled trial of rituximab versus cyclosporine in the treatment of idiopathicmembranous nephropathy (MENTOR) Nephron [Internet] 2015 [cited2017 Dec 25] 130 159ndash168 Available from httpwwwncbinlmnihgovpubmed26087670
62 Dimopoulos MA Richardson PG Schlag R et al VMP (bortezomib mel-phalan and prednisone) is active and well tolerated in newly diagnosedpatients with multiple myeloma with moderately impaired renal functionand results in reversal of renal impairment cohort analysis of the Phase IIIVISTA study JCO 2009 [cited 2017 Dec 8] 27 6086ndash6093 Available fromhttpwwwncbinlmnihgovpubmed19858394
63 Morabito F Gentile M Mazzone C et al Safety and efficacy ofbortezomib-melphalan-prednisone-thalidomide followed by bortezomib-thalidomide maintenance (VMPT-VT) versus bortezomib-melphalan-prednisone (VMP) in untreated multiple myeloma patients with renal im-pairment Blood [Internet] 2011 [cited 2017 Dec 9] 118 5759ndash5766Available from httpwwwncbinlmnihgovpubmed21951682
64 Moreau P Masszi T Grzasko N et al Oral ixazomib lenalidomide anddexamethasone for multiple myeloma N Engl J Med 2016 [cited 2018 Apr27] 374 1621ndash1634 Available from httpwwwnejmorgdoi101056NEJMoa1516282
65 Nordstrom BL Knopf KB Teltsch DY et al The safety of bendamustine inpatients with chronic lymphocytic leukemia or non-Hodgkin lymphomaand concomitant renal impairment a retrospective electronic medical re-cord database analysis Leuk Lymphoma [Internet] 2014 [cited 2017 Dec13] 55 1266ndash1273 Available from httpwwwncbinlmnihgovpubmed23987821
66 Roussou M Kastritis E Christoulas D et al Reversibility of renal failure innewly diagnosed patients with multiple myeloma and the role of novelagents Leuk Res [Internet] 2010 [cited 2017 Dec 15] 34 1395ndash1397Available from httpwwwncbinlmnihgovpubmed20510452
67 Tosi P Zamagni E Tacchetti P et al Thalidomide-dexamethasone as in-duction therapy before autologous stem cell transplantation in patientswith newly diagnosed multiple myeloma and renal insufficiency BiolBlood Marrow Transplant [Internet] 2010 [cited 2018 Apr 27] 161115ndash1121 Available from httpwwwncbinlmnihgovpubmed20197100
68 Dimopoulos M Alegre A Stadtmauer EA et al The efficacy and safety oflenalidomide plus dexamethasone in relapsed andor refractory multiplemyeloma patients with impaired renal function Cancer [Internet] 2010116 3807 [cited 2017 Dec 15] Available from httpwwwncbinlmnihgovpubmed20564094
69 Siegel DS Weisel KC Dimopoulos MA et al Pomalidomide plus low-dosedexamethasone in patients with relapsedrefractory multiple myeloma andmoderate renal impairment a pooled analysis of three clinical trials LeukLymphoma [Internet] 2016 [cited 2017 Dec 15] 57 2833ndash2838 Availablefrom httpwwwncbinlmnihgovpubmed27267105
70 Dimopoulos MA Goldschmidt H Niesvizky R et al Carfilzomib or borte-zomib in relapsed or refractory multiple myeloma (ENDEAVOR) an in-terim overall survival analysis of an open-label randomised phase 3 trialLancet Oncol [Internet] 2017 [cited 2017 Dec 6] 18 1327ndash1337 Availablefrom httpwwwncbinlmnihgovpubmed28843768
71 Telio D Shepherd J Forrest D et al High-dose melphalan followed byauto-SCT has favorable safety and efficacy in selected patients with lightchain deposition disease and light and heavy chain deposition diseaseBone Marrow Transplant 2012 [cited 2017 Dec 8] 47 453ndash455 Availablefrom httpwwwnaturecomdoifinder101038bmt201187
72 Batalini F Econimo L Quillen K et al High-dose melphalan and stem celltransplantation in patients on dialysis due to immunoglobulin light-chainamyloidosis and monoclonal immunoglobulin deposition disease BiolBlood Marrow Transplant [Internet] 2018 [cited 2017 Dec 25] 24127ndash132 Available from httpwwwncbinlmnihgovpubmed28865972
73 Kourelis TV Nasr SH Dispenzieri A et al Outcomes of patients with renalmonoclonal immunoglobulin deposition disease Am J Hematol 2016[cited 2018 Jul 2] 91 1123ndash1128 Available from httpwwwncbinlmnihgovpubmed27501122
74 Pozzi C DrsquoAmico M Fogazzi GB et al Light chain deposition disease withrenal involvement clinical characteristics and prognostic factors Am JKidney Dis [Internet] 2003 [cited 2018 Jun 23] 42 1154ndash1163 Availablefrom httpwwwncbinlmnihgovpubmed14655186
75 Song M-K Chung J-S Shin H-J et al Cyclophosphamide-containing regi-men (TCD) is superior to melphalan-containing regimen (MPT) in elderlymultiple myeloma patients with renal impairment Ann Hematol
Clinical implication of monoclonal gammopathies 11Downloaded from httpsacademicoupcomndtadvance-article-abstractdoi101093ndtgfy2595086133by gueston 29 August 2018
[Internet] 2012 [cited 2017 Dec 9] 91 889ndash896 Available from httpwwwncbinlmnihgovpubmed22237937
76 Specter R Sanchorawala V Seldin DC et al Kidney dysfunction duringlenalidomide treatment for AL amyloidosis Nephrol Dial Transplant[Internet] 2011 [cited 2018 Jul 7] 26 881ndash886 Available from httpwwwncbinlmnihgovpubmed20693160
77 Li Y Wang X OrsquoMara E et al Population pharmacokinetics of pomalido-mide in patients with relapsed or refractory multiple myeloma with variousdegrees of impaired renal function CPAA 2017 [cited 2018 Feb 4] 9133ndash145 Available from httpwwwncbinlmnihgovpubmed29184451
78 Kastritis E Gavriatopoulou M Roussou M et al Addition of cyclophos-phamide and higher doses of dexamethasone do not improve outcomes ofpatients with AL amyloidosis treated with bortezomib Blood Cancer J2017 [cited 2017 Dec 15] 7 e570 Available from httpwwwncbinlmnihgovpubmed28622303
79 Venner CP Gillmore JD Sachchithanantham S et al A matched compari-son of cyclophosphamide bortezomib and dexamethasone (CVD) versusrisk-adapted cyclophosphamide thalidomide and dexamethasone (CTD)in AL amyloidosis Leukemia [Internet] 2014 [cited 2018 Jul 5] 282304ndash2310 Available from httpwwwncbinlmnihgovpubmed25027514
80 Palladini G Sachchithanantham S Milani P et al A European collabora-tive study of cyclophosphamide bortezomib and dexamethasone inupfront treatment of systemic AL amyloidosis Blood [Internet] 2015[cited 2017 Dec 9] 126 612ndash615 Available from httpwwwncbinlmnihgovpubmed25987656
81 Kopel T Kaufman JS Hamburg N et al Endothelium-dependent and -in-dependent vascular function in advanced chronic kidney disease CJASN2017 [cited 2018 Apr 18] 12 1588ndash1594 Available from httpcjasnasnjournalsorglookupdoi102215CJN12811216
82 Palladini G Milani P Foli A et al A Phase 2 trial of pomalidomide anddexamethasone rescue treatment in patients with AL amyloidosis Blood[Internet] 2017 [cited 2018 Apr 26] 129 2120ndash2123 Available fromhttpwwwncbinlmnihgovpubmed28130212
83 Hegenbart U Bochtler T Benner A et al Lenalidomidemelphalandexa-methasone in newly diagnosed patients with immunoglobulin light chainamyloidosis results of a prospective phase 2 study with long-term followup Haematologica [Internet] 2017 [cited 2017 Dec 26] 102 1424ndash1431Available from httpwwwncbinlmnihgovpubmed28522573
84 Palladini G Milani P Foli A et al Oral melphalan and dexamethasonegrants extended survival with minimal toxicity in AL amyloidosis long-term results of a risk-adapted approach Haematologica [Internet] 2014[cited 2017 Dec 15] 99 743ndash750 Available from httpwwwncbinlmnihgovpubmed24213149
85 Payet J Livartowski J Kavian N et al Type I cryoglobulinemia in multiplemyeloma a rare entity analysis of clinical and biological characteristics ofseven cases and review of the literature Leuk Lymphoma [Internet] 201354 767ndash777 Available from httpwwwtandfonlinecomdoifull103109104281942012671481
86 Terpos E Kleber M Engelhardt M et al European Myeloma Networkguidelines for the management of multiple myeloma-related complica-tions Haematologica [Internet] 2015 [cited 2017 Dec 4] 100 1254ndash1266Available from httpwwwncbinlmnihgovpubmed26432383
87 Chanan-Khan AA Kaufman JL Mehta J et al Activity and safety of borte-zomib in multiple myeloma patients with advanced renal failure a multi-center retrospective study Blood [Internet] 2007 [cited 2018 Jul 2] 1092604ndash2606 Available from httpwwwncbinlmnihgovpubmed17138816
88 Dimopoulos MA Roussou M Gkotzamanidou M et al The role of novelagents on the reversibility of renal impairment in newly diagnosed symp-tomatic patients with multiple myeloma Leukemia 2013 27 423ndash429
89 Kouroukis TC Baldassarre FG Haynes AE et al Bortezomib in multiplemyeloma systematic review and clinical considerations Curr Oncol(Toronto Ont) [Internet] 2014 [cited 2017 Dec 4] 21 e573ndashe603Available from httpwwwncbinlmnihgovpubmed25089109
90 Zhu W Chen W Bortezomib-based treatment for multiple myelomapatients with renal impairment a systematic review and meta-analysis ofobservational studies Medicine [Internet] 2016 95 e5202 Available fromhttpwwwncbinlmnihgovpmcarticlesPMC5120900
91 Dimopoulos MA Terpos E Chanan-Khan A et al Renal impairment inpatients with multiple myeloma a consensus statement on behalf of theInternational Myeloma Working Group JCO 2010 28 4976ndash4984
92 Chauvet S Fremeaux-Bacchi V Petitprez F et al Treatment of B-cell disor-der improves renal outcome of patients with monoclonal gammopathyndashassociated C3 glomerulopathy Blood [Internet] 2017 [cited 2017 Oct 26]129 1437ndash1447 Available from httpwwwncbinlmnihgovpubmed28069603
93 Cohen C Royer B Javaugue V et al Bortezomib produces high hematolog-ical response rates with prolonged renal survival in monoclonal immuno-globulin deposition disease Kidney Int [Internet] 2015 [cited 2017 Dec25] 88 1135ndash1143 Available from httpwwwncbinlmnihgovpubmed26176826
94 Ziogas DC Kastritis E Terpos E et al Hematologic and renal improve-ment of monoclonal immunoglobulin deposition disease after treatmentwith bortezomib-based regimens Leuk Lymphoma [Internet] 2017 [cited2017 Dec 25] 58 1832ndash1839 Available from httpwwwncbinlmnihgovpubmed27967286
95 Milani P Merlini G Palladini G Novel therapies in light chain amyloid-osis Kidney Int Rep [Internet] 2018 [cited 2018 Jul 4] 3 530ndash541 Availablefrom httpwwwncbinlmnihgovpubmed29854961
96 Spizzo G Mitterer M Gunsilius E Bortezomib for the treatment of refrac-tory Type-1 cryoglobulinaemia Br J Haematol [Internet] 2010 [cited 2018Jul 7] 150 235ndash237 Available from httpdoiwileycom101111j1365-2141201008184x
97 Talamo G Claxton D Tricot G et al Response to bortezomib in refractoryType I cryoglobulinemia Am J Hematol 2008 [cited 2018 Jul 7] 83883ndash884 Available from httpwwwncbinlmnihgovpubmed18756542
98 Dimopoulos MA Roussou M Gavriatopoulou M et al Cardiac and renalcomplications of carfilzomib in patients with multiple myeloma BloodAdv 2017 [cited 2017 Dec 6] 1 449ndash454 Available from httpwwwbloodadvancesorglookupdoi101182bloodadvances2016003269
99 Strati P Nasr SH Leung N et al Renal complications in chronic lympho-cytic leukemia and monoclonal B-cell lymphocytosis the Mayo Clinic ex-perience Haematologica [Internet] 2015 [cited 2018 Jul 3] 100 1180ndash1188Available from httpwwwncbinlmnihgovpubmed26088927
100 Salama AD Pusey CD Drug insight rituximab in renal disease and trans-plantation Nat Clin Pract Nephrol [Internet] 2006 [cited 2017 Dec 8] 2221ndash230 Available from httpwwwnaturecomdoifinder101038ncpneph0133
101 Jillella AP Dainer PM Kallab AM et al Treatment of a patient with end-stage renal disease with rituximab pharmacokinetic evaluation suggestsrituximab is not eliminated by hemodialysis Am J Hematol 2002 [cited2018 Jul] 71 219ndash222 Available from httpwwwncbinlmnihgovpubmed12410580
102 Guiard E Karras A Plaisier E et al Patterns of noncryoglobulinemic glo-merulonephritis with monoclonal Ig deposits correlation with IgG sub-class and response to rituximab Clin J Am Soc Nephrol 2011 6 1609ndash1616
103 Ribes D Hachem HEL Oberic L et al Bendamustine plus rituximab forindolent B-cell lymphoma of renal significance Am J Hematol 2018 93356ndash362
104 Darwish M Bond M Hellriegel E et al Pharmacokinetic and pharmacody-namic profile of bendamustine and its metabolites Cancer ChemotherPharmacol 2015 [cited 2017 Dec 15] 75 1143ndash1154 Available from httpwwwncbinlmnihgovpubmed25829094
105 Ponisch W Moll B Bourgeois M et al Bendamustine and prednisone incombination with bortezomib (BPV) in the treatment of patients with re-lapsed or refractory multiple myeloma and light chain-induced renal fail-ure J Cancer Res Clin Oncol [Internet] 2013 [cited 2018 Jul 2] 1391937ndash1946 Available from httpwwwncbinlmnihgovpubmed24046251
106 Mateos M-V Dimopoulos MA Cavo M et al Daratumumab plus bortezo-mib melphalan and prednisone for untreated myeloma N Engl J Med2018 378 518ndash528
107 Rocchi S Tacchetti P Pantani L et al Safety and efficacy of daratumumabin dialysis-dependent renal failure secondary to multiple myelomaHaematologica [Internet] 2018 [cited 2018 Jul 2] 103 e277ndashe278 Availablefrom httpwwwncbinlmnihgovpubmed29622654
12 K Batko et alDownloaded from httpsacademicoupcomndtadvance-article-abstractdoi101093ndtgfy2595086133by gueston 29 August 2018
108 Anand S Miller D Chipman G Morris D Srinivas S Daratumumab forsevere refractory proliferative glomerulonephritis with monoclonal im-mune deposits (PGNMID) ATC Abstr [Internet] 2017 [cited 2018 Jul 3]Available from httpsatcmeetingabstractscomabstractdaratumumab-for-severe-refractory-proliferative-glomerulonephritis-with-monoclonal-immune-deposits-pgnmid
109 Leung N Lager DJ Gertz MA et al Long-term outcome of renal transplan-tation in light-chain deposition disease Am J Kidney Dis [Internet] 2004[cited 2018 Feb 9] 43 147ndash153 Available from httpwwwncbinlmnihgovpubmed14712438
110 Lorenz EC Sethi S Leung N et al Recurrent membranoproliferative glo-merulonephritis after kidney transplantation Kidney Int [Internet] 2010[cited 2018 Feb 9] 77 721ndash728 Available from httpwwwncbinlmnihgovpubmed20130531
111 Leung N Nasr SH A patient with abnormal kidney function and a mono-clonal light chain in the urine Clin J Am Soc Nephrol 2016 11 1073ndash1082
112 Cibeira MT Sanchorawala V Seldin DC et al Outcome of AL amyloidosisafter high-dose melphalan and autologous stem cell transplantation long-term results in a series of 421 patients Blood [Internet] 2011 [cited 2018Feb 3] 118 4346ndash4352 Available from httpwwwncbinlmnihgovpubmed21828140
113 Gertz MA Lacy MQ Dispenzieri A et al Autologous stem cell transplantfor immunoglobulin light chain amyloidosis a status report LeukLymphoma [Internet] 2010 [cited 2018 Feb 3] 51 2181ndash2187 Availablefrom httpwwwncbinlmnihgovpubmed20958232
114 Leung N Kumar SK Glavey SV et al The impact of dialysis on the survivalof patients with immunoglobulin light chain (AL) amyloidosis undergoingautologous stem cell transplantation Nephrol Dial Transplant 2016 [cited2018 Jul 7] 31 1284ndash1289 Available from httpsacademicoupcomndtarticle-lookupdoi101093ndtgfv328
115 Badros A Barlogie B Siegel E et al Results of autologous stem cell trans-plant in multiple myeloma patients with renal failure Br J Haematol 2001[cited 2018 Jul 7] 114 822ndash829 Available from httpwwwncbinlmnihgovpubmed11564069
116 Soltero L Carbajal H Xu J et al Initial survival data of kidney transplantpatients with pre-transplant monoclonal gammopathy Clin Transplant[Internet] 2012 [cited 2018 Feb 3] 26 300ndash304 Available from httpwwwncbinlmnihgovpubmed22044717
117 Jimenez-Zepeda VH Heilman RL Engel RA et al Monoclonal gammopathyof undetermined significance does not affect outcomes in patients undergoingsolid organ transplants Transplantation [Internet] 2011 [cited 2018 Feb 3]92 570ndash574 Available from httpwwwncbinlmnihgovpubmed21712755
118 Naina HVK Harris S Dispenzieri A et al Long-term follow-up of patientswith monoclonal gammopathy of undetermined significance after kidney
transplantation Am J Nephrol 2012 [cited 2018 Feb] 35 365ndash371Available from httpwwwncbinlmnihgovpubmed22473253
119 Bansal T Garg A Snowden JA et al Defining the role of renal transplanta-tion in the modern management of multiple myeloma and other plasmacell dyscrasias Nephron Clin Pract [Internet] 2012 [cited 2018 Feb 3] 120c228 wwwkargercom
120 Hassoun H Flombaum C DrsquoAgati VD et al High-dose melphalan andauto-SCT in patients with monoclonal Ig deposition disease Bone MarrowTransplant 2008 [cited 2018 Feb 3] 42 405ndash412 Available from httpwwwncbinlmnihgovpubmed18574442
121 Herrmann SMS Gertz MA Stegall MD et al Long-term outcomes ofpatients with light chain amyloidosis (AL) after renal transplantation withor without stem cell transplantation Nephrol Dial Transplant [Internet]2011 [cited 2018 Feb 3] 26 2032ndash2036 Available from httpwwwncbinlmnihgovpubmed21543655
122 Lorenz EC Gertz MA Fervenza FC et al Long-term outcome of autolo-gous stem cell transplantation in light chain deposition disease NephrolDial Transplant [Internet] 2008 [cited 2018 Jul 5] 23 2052ndash2057 Availablefrom httpwwwncbinlmnihgovpubmed18178602
123 Merhi B Patel N Bayliss G et al Proliferative glomerulonephritis withmonoclonal IgG deposits in two kidney allografts successfully treated withrituximab Clin Kidney J [Internet] 2017 [cited 2018 Feb 10] 10 405ndash410Available from httpsacademicoupcomckjarticle-lookupdoi101093ckjsfx001
124 Barbour SJ Beaulieu MC Zalunardo NY et al Proliferative glomerulone-phritis with monoclonal IgG deposits secondary to chronic lymphocyticleukemia Report of two cases Nephrol Dial Transplant [Internet] 2011[cited 2018 Feb 10] 26 2712ndash2714 Available from httpsacademicoupcomndtarticle-lookupdoi101093ndtgfr251
125 Zand L Lorenz EC Cosio FG et al Clinical findings pathology and out-comes of C3GN after kidney transplantation J Am Soc Nephrol [Internet]2014 [cited 2018 Jul 5] 25 1110ndash1117 Available from httpwwwncbinlmnihgovpubmed24357668
126 Alfano G Fontana F Colaci E et al Monoclonal gammopathy of undeter-mined significance after kidney transplantation Transplantation [Internet]2017 [cited 2017 Oct 24] 101 e337ndashe342 Available from httpwwwncbinlmnihgovpubmed28731904
127 Bancu I Ca~nas L Juega FJ et al Outcomes of monoclonal gammopathyof undetermined significance in patients who underwent kidneytransplantation Transplant Proc [Internet] 2015 [cited 2018 Feb 10] 472344ndash2345 Available from httpwwwncbinlmnihgovpubmed26518922
Received 2632018 Editorial decision 1472018
Clinical implication of monoclonal gammopathies 13Downloaded from httpsacademicoupcomndtadvance-article-abstractdoi101093ndtgfy2595086133by gueston 29 August 2018

47 Levinson SS Urine immunofixation electrophoresis remains importantand is complementary to serum free light chain Clin Chem Lab Med[Internet] 2011 [cited 2018 Jun 25] 49 1801ndash1804 Available from httpwwwncbinlmnihgovpubmed21663562 [CrossRef][Mismatch]
48 Lee WS Singh G Serum free light chains in neoplastic monoclonal gam-mopathies relative under-detection of lambda dominant KappaLambdaratio and underproduction of free lambda light chains as compared tokappa light chains in patients with neoplastic monoclonal gammopathiesJ Clin Med Res 2018 [cited 2018 Jun 25] 10 562ndash569 Available fromhttpwwwncbinlmnihgovpubmed29904440
49 Xu B Tang Y Zhou J et al Disease spectrum of abnormal serum free lightchain ratio and its diagnostic significance Oncotarget [Internet] 2017[cited 2017 Dec 29] 8 82268ndash82279 Available from httpwwwncbinlmnihgovpubmed29137262
50 Koo EH Shin J Jang HR et al Diagnostic performances of M-protein testsaccording to the clinical presentations of kidney disease Eur J Intern Med[Internet] 2016 [cited 2018 Feb 9] 33 88ndash92 Available from httpwwwncbinlmnihgovpubmed27421913
51 Gumber R Cohen JB Palmer MB et al A clone-directed approach mayimprove diagnosis and treatment of proliferative glomerulonephritis withmonoclonal immunoglobulin deposits Kidney Int [Internet] 2018 94199ndash205 Available from httpsdoiorg101016jkint201802020
52 Leung N Barnidge DR Hutchison CA Laboratory testing in monoclonalgammopathy of renal significance (MGRS) Clin Chem Lab Med [Internet]2016 [cited 2017 Oct 25] 54 929ndash937 Available from httpwwwncbinlmnihgovpubmed27107835 [CrossRef][Mismatch]
53 Ramirez-Alvarado M Ward CJ Huang BQ et al Differences in immuno-globulin light chain species found in urinary exosomes in light chain amy-loidosis (AL) PLoS ONE [Internet] 2012 [cited 2018 Jul 7] 7 e38061Available from httpwwwncbinlmnihgovpubmed22723846
54 Hogan JJ Weiss BM Bridging the divide an onco-nephrologic approachto the monoclonal gammopathies of renal significance Clin J Am SocNephrol [Internet] 2016 [cited 2017 Oct 26] 11 1681ndash1691 Availablefrom httpwwwncbinlmnihgovpubmed27416775
55 Vij R Mazumder A Klinger M et al Deep sequencing reveals myelomacells in peripheral blood in majority of multiple myeloma patients ClinLymphoma Myeloma Leuk [Internet] 2014 [cited 2017 Oct 25] 14131ndash139e1 Available from httpwwwncbinlmnihgovpubmed24629890
56 Gonsalves WI Leung N Rajkumar SV et al Improvement in renal func-tion and its impact on survival in patients with newly diagnosed multiplemyeloma Blood Cancer J 2015 [cited 2018 Feb 3] 5 e296 Available fromhttpwwwnaturecomdoifinder101038bcj201520
57 Dimopoulos MA Cheung MC Roussel M et al Impact of renal impair-ment on outcomes with lenalidomide and dexamethasone treatment in theFIRST trial a randomized open-label phase 3 trial in transplant-ineligiblepatients with multiple myeloma Haematologica [Internet] 2016 [cited2018 Jul 7] 101 363ndash370 Available from httpwwwncbinlmnihgovpubmed26659916
58 Ponisch W Andrea M Wagner I et al Successful treatment of patientswith newly diagnoseduntreated multiple myeloma and advanced renalfailure using bortezomib in combination with bendamustine and predni-sone J Cancer Res Clin Oncol 2012 [cited 2018 Jul 2] 138 1405ndash1412Available from httpwwwncbinlmnihgovpubmed22526157
59 Perry M Delarche A Ribes D et al Rituximab-cyclophosphamide-dexa-methasone is highly effective in patients with monoclonal Ig deposit-related glomerulopathy and indolent non-Hodgkin lymphomas Am JHematol 2014 [cited 2018 Jul 1] 89 969ndash973 Available from httpdoiwileycom101002ajh23798
60 Dimopoulos M Weisel K van de Donk Nwcj et al Pomalidomide pluslow-dose dexamethasone in patients with relapsedrefractory multiple my-eloma and renal impairment results from a Phase II trial J Clin Oncol2018 36 2035ndash2043
61 Fervenza FC Canetta PA Barbour SJ et al A multicenter randomized con-trolled trial of rituximab versus cyclosporine in the treatment of idiopathicmembranous nephropathy (MENTOR) Nephron [Internet] 2015 [cited2017 Dec 25] 130 159ndash168 Available from httpwwwncbinlmnihgovpubmed26087670
62 Dimopoulos MA Richardson PG Schlag R et al VMP (bortezomib mel-phalan and prednisone) is active and well tolerated in newly diagnosedpatients with multiple myeloma with moderately impaired renal functionand results in reversal of renal impairment cohort analysis of the Phase IIIVISTA study JCO 2009 [cited 2017 Dec 8] 27 6086ndash6093 Available fromhttpwwwncbinlmnihgovpubmed19858394
63 Morabito F Gentile M Mazzone C et al Safety and efficacy ofbortezomib-melphalan-prednisone-thalidomide followed by bortezomib-thalidomide maintenance (VMPT-VT) versus bortezomib-melphalan-prednisone (VMP) in untreated multiple myeloma patients with renal im-pairment Blood [Internet] 2011 [cited 2017 Dec 9] 118 5759ndash5766Available from httpwwwncbinlmnihgovpubmed21951682
64 Moreau P Masszi T Grzasko N et al Oral ixazomib lenalidomide anddexamethasone for multiple myeloma N Engl J Med 2016 [cited 2018 Apr27] 374 1621ndash1634 Available from httpwwwnejmorgdoi101056NEJMoa1516282
65 Nordstrom BL Knopf KB Teltsch DY et al The safety of bendamustine inpatients with chronic lymphocytic leukemia or non-Hodgkin lymphomaand concomitant renal impairment a retrospective electronic medical re-cord database analysis Leuk Lymphoma [Internet] 2014 [cited 2017 Dec13] 55 1266ndash1273 Available from httpwwwncbinlmnihgovpubmed23987821
66 Roussou M Kastritis E Christoulas D et al Reversibility of renal failure innewly diagnosed patients with multiple myeloma and the role of novelagents Leuk Res [Internet] 2010 [cited 2017 Dec 15] 34 1395ndash1397Available from httpwwwncbinlmnihgovpubmed20510452
67 Tosi P Zamagni E Tacchetti P et al Thalidomide-dexamethasone as in-duction therapy before autologous stem cell transplantation in patientswith newly diagnosed multiple myeloma and renal insufficiency BiolBlood Marrow Transplant [Internet] 2010 [cited 2018 Apr 27] 161115ndash1121 Available from httpwwwncbinlmnihgovpubmed20197100
68 Dimopoulos M Alegre A Stadtmauer EA et al The efficacy and safety oflenalidomide plus dexamethasone in relapsed andor refractory multiplemyeloma patients with impaired renal function Cancer [Internet] 2010116 3807 [cited 2017 Dec 15] Available from httpwwwncbinlmnihgovpubmed20564094
69 Siegel DS Weisel KC Dimopoulos MA et al Pomalidomide plus low-dosedexamethasone in patients with relapsedrefractory multiple myeloma andmoderate renal impairment a pooled analysis of three clinical trials LeukLymphoma [Internet] 2016 [cited 2017 Dec 15] 57 2833ndash2838 Availablefrom httpwwwncbinlmnihgovpubmed27267105
70 Dimopoulos MA Goldschmidt H Niesvizky R et al Carfilzomib or borte-zomib in relapsed or refractory multiple myeloma (ENDEAVOR) an in-terim overall survival analysis of an open-label randomised phase 3 trialLancet Oncol [Internet] 2017 [cited 2017 Dec 6] 18 1327ndash1337 Availablefrom httpwwwncbinlmnihgovpubmed28843768
71 Telio D Shepherd J Forrest D et al High-dose melphalan followed byauto-SCT has favorable safety and efficacy in selected patients with lightchain deposition disease and light and heavy chain deposition diseaseBone Marrow Transplant 2012 [cited 2017 Dec 8] 47 453ndash455 Availablefrom httpwwwnaturecomdoifinder101038bmt201187
72 Batalini F Econimo L Quillen K et al High-dose melphalan and stem celltransplantation in patients on dialysis due to immunoglobulin light-chainamyloidosis and monoclonal immunoglobulin deposition disease BiolBlood Marrow Transplant [Internet] 2018 [cited 2017 Dec 25] 24127ndash132 Available from httpwwwncbinlmnihgovpubmed28865972
73 Kourelis TV Nasr SH Dispenzieri A et al Outcomes of patients with renalmonoclonal immunoglobulin deposition disease Am J Hematol 2016[cited 2018 Jul 2] 91 1123ndash1128 Available from httpwwwncbinlmnihgovpubmed27501122
74 Pozzi C DrsquoAmico M Fogazzi GB et al Light chain deposition disease withrenal involvement clinical characteristics and prognostic factors Am JKidney Dis [Internet] 2003 [cited 2018 Jun 23] 42 1154ndash1163 Availablefrom httpwwwncbinlmnihgovpubmed14655186
75 Song M-K Chung J-S Shin H-J et al Cyclophosphamide-containing regi-men (TCD) is superior to melphalan-containing regimen (MPT) in elderlymultiple myeloma patients with renal impairment Ann Hematol
Clinical implication of monoclonal gammopathies 11Downloaded from httpsacademicoupcomndtadvance-article-abstractdoi101093ndtgfy2595086133by gueston 29 August 2018
[Internet] 2012 [cited 2017 Dec 9] 91 889ndash896 Available from httpwwwncbinlmnihgovpubmed22237937
76 Specter R Sanchorawala V Seldin DC et al Kidney dysfunction duringlenalidomide treatment for AL amyloidosis Nephrol Dial Transplant[Internet] 2011 [cited 2018 Jul 7] 26 881ndash886 Available from httpwwwncbinlmnihgovpubmed20693160
77 Li Y Wang X OrsquoMara E et al Population pharmacokinetics of pomalido-mide in patients with relapsed or refractory multiple myeloma with variousdegrees of impaired renal function CPAA 2017 [cited 2018 Feb 4] 9133ndash145 Available from httpwwwncbinlmnihgovpubmed29184451
78 Kastritis E Gavriatopoulou M Roussou M et al Addition of cyclophos-phamide and higher doses of dexamethasone do not improve outcomes ofpatients with AL amyloidosis treated with bortezomib Blood Cancer J2017 [cited 2017 Dec 15] 7 e570 Available from httpwwwncbinlmnihgovpubmed28622303
79 Venner CP Gillmore JD Sachchithanantham S et al A matched compari-son of cyclophosphamide bortezomib and dexamethasone (CVD) versusrisk-adapted cyclophosphamide thalidomide and dexamethasone (CTD)in AL amyloidosis Leukemia [Internet] 2014 [cited 2018 Jul 5] 282304ndash2310 Available from httpwwwncbinlmnihgovpubmed25027514
80 Palladini G Sachchithanantham S Milani P et al A European collabora-tive study of cyclophosphamide bortezomib and dexamethasone inupfront treatment of systemic AL amyloidosis Blood [Internet] 2015[cited 2017 Dec 9] 126 612ndash615 Available from httpwwwncbinlmnihgovpubmed25987656
81 Kopel T Kaufman JS Hamburg N et al Endothelium-dependent and -in-dependent vascular function in advanced chronic kidney disease CJASN2017 [cited 2018 Apr 18] 12 1588ndash1594 Available from httpcjasnasnjournalsorglookupdoi102215CJN12811216
82 Palladini G Milani P Foli A et al A Phase 2 trial of pomalidomide anddexamethasone rescue treatment in patients with AL amyloidosis Blood[Internet] 2017 [cited 2018 Apr 26] 129 2120ndash2123 Available fromhttpwwwncbinlmnihgovpubmed28130212
83 Hegenbart U Bochtler T Benner A et al Lenalidomidemelphalandexa-methasone in newly diagnosed patients with immunoglobulin light chainamyloidosis results of a prospective phase 2 study with long-term followup Haematologica [Internet] 2017 [cited 2017 Dec 26] 102 1424ndash1431Available from httpwwwncbinlmnihgovpubmed28522573
84 Palladini G Milani P Foli A et al Oral melphalan and dexamethasonegrants extended survival with minimal toxicity in AL amyloidosis long-term results of a risk-adapted approach Haematologica [Internet] 2014[cited 2017 Dec 15] 99 743ndash750 Available from httpwwwncbinlmnihgovpubmed24213149
85 Payet J Livartowski J Kavian N et al Type I cryoglobulinemia in multiplemyeloma a rare entity analysis of clinical and biological characteristics ofseven cases and review of the literature Leuk Lymphoma [Internet] 201354 767ndash777 Available from httpwwwtandfonlinecomdoifull103109104281942012671481
86 Terpos E Kleber M Engelhardt M et al European Myeloma Networkguidelines for the management of multiple myeloma-related complica-tions Haematologica [Internet] 2015 [cited 2017 Dec 4] 100 1254ndash1266Available from httpwwwncbinlmnihgovpubmed26432383
87 Chanan-Khan AA Kaufman JL Mehta J et al Activity and safety of borte-zomib in multiple myeloma patients with advanced renal failure a multi-center retrospective study Blood [Internet] 2007 [cited 2018 Jul 2] 1092604ndash2606 Available from httpwwwncbinlmnihgovpubmed17138816
88 Dimopoulos MA Roussou M Gkotzamanidou M et al The role of novelagents on the reversibility of renal impairment in newly diagnosed symp-tomatic patients with multiple myeloma Leukemia 2013 27 423ndash429
89 Kouroukis TC Baldassarre FG Haynes AE et al Bortezomib in multiplemyeloma systematic review and clinical considerations Curr Oncol(Toronto Ont) [Internet] 2014 [cited 2017 Dec 4] 21 e573ndashe603Available from httpwwwncbinlmnihgovpubmed25089109
90 Zhu W Chen W Bortezomib-based treatment for multiple myelomapatients with renal impairment a systematic review and meta-analysis ofobservational studies Medicine [Internet] 2016 95 e5202 Available fromhttpwwwncbinlmnihgovpmcarticlesPMC5120900
91 Dimopoulos MA Terpos E Chanan-Khan A et al Renal impairment inpatients with multiple myeloma a consensus statement on behalf of theInternational Myeloma Working Group JCO 2010 28 4976ndash4984
92 Chauvet S Fremeaux-Bacchi V Petitprez F et al Treatment of B-cell disor-der improves renal outcome of patients with monoclonal gammopathyndashassociated C3 glomerulopathy Blood [Internet] 2017 [cited 2017 Oct 26]129 1437ndash1447 Available from httpwwwncbinlmnihgovpubmed28069603
93 Cohen C Royer B Javaugue V et al Bortezomib produces high hematolog-ical response rates with prolonged renal survival in monoclonal immuno-globulin deposition disease Kidney Int [Internet] 2015 [cited 2017 Dec25] 88 1135ndash1143 Available from httpwwwncbinlmnihgovpubmed26176826
94 Ziogas DC Kastritis E Terpos E et al Hematologic and renal improve-ment of monoclonal immunoglobulin deposition disease after treatmentwith bortezomib-based regimens Leuk Lymphoma [Internet] 2017 [cited2017 Dec 25] 58 1832ndash1839 Available from httpwwwncbinlmnihgovpubmed27967286
95 Milani P Merlini G Palladini G Novel therapies in light chain amyloid-osis Kidney Int Rep [Internet] 2018 [cited 2018 Jul 4] 3 530ndash541 Availablefrom httpwwwncbinlmnihgovpubmed29854961
96 Spizzo G Mitterer M Gunsilius E Bortezomib for the treatment of refrac-tory Type-1 cryoglobulinaemia Br J Haematol [Internet] 2010 [cited 2018Jul 7] 150 235ndash237 Available from httpdoiwileycom101111j1365-2141201008184x
97 Talamo G Claxton D Tricot G et al Response to bortezomib in refractoryType I cryoglobulinemia Am J Hematol 2008 [cited 2018 Jul 7] 83883ndash884 Available from httpwwwncbinlmnihgovpubmed18756542
98 Dimopoulos MA Roussou M Gavriatopoulou M et al Cardiac and renalcomplications of carfilzomib in patients with multiple myeloma BloodAdv 2017 [cited 2017 Dec 6] 1 449ndash454 Available from httpwwwbloodadvancesorglookupdoi101182bloodadvances2016003269
99 Strati P Nasr SH Leung N et al Renal complications in chronic lympho-cytic leukemia and monoclonal B-cell lymphocytosis the Mayo Clinic ex-perience Haematologica [Internet] 2015 [cited 2018 Jul 3] 100 1180ndash1188Available from httpwwwncbinlmnihgovpubmed26088927
100 Salama AD Pusey CD Drug insight rituximab in renal disease and trans-plantation Nat Clin Pract Nephrol [Internet] 2006 [cited 2017 Dec 8] 2221ndash230 Available from httpwwwnaturecomdoifinder101038ncpneph0133
101 Jillella AP Dainer PM Kallab AM et al Treatment of a patient with end-stage renal disease with rituximab pharmacokinetic evaluation suggestsrituximab is not eliminated by hemodialysis Am J Hematol 2002 [cited2018 Jul] 71 219ndash222 Available from httpwwwncbinlmnihgovpubmed12410580
102 Guiard E Karras A Plaisier E et al Patterns of noncryoglobulinemic glo-merulonephritis with monoclonal Ig deposits correlation with IgG sub-class and response to rituximab Clin J Am Soc Nephrol 2011 6 1609ndash1616
103 Ribes D Hachem HEL Oberic L et al Bendamustine plus rituximab forindolent B-cell lymphoma of renal significance Am J Hematol 2018 93356ndash362
104 Darwish M Bond M Hellriegel E et al Pharmacokinetic and pharmacody-namic profile of bendamustine and its metabolites Cancer ChemotherPharmacol 2015 [cited 2017 Dec 15] 75 1143ndash1154 Available from httpwwwncbinlmnihgovpubmed25829094
105 Ponisch W Moll B Bourgeois M et al Bendamustine and prednisone incombination with bortezomib (BPV) in the treatment of patients with re-lapsed or refractory multiple myeloma and light chain-induced renal fail-ure J Cancer Res Clin Oncol [Internet] 2013 [cited 2018 Jul 2] 1391937ndash1946 Available from httpwwwncbinlmnihgovpubmed24046251
106 Mateos M-V Dimopoulos MA Cavo M et al Daratumumab plus bortezo-mib melphalan and prednisone for untreated myeloma N Engl J Med2018 378 518ndash528
107 Rocchi S Tacchetti P Pantani L et al Safety and efficacy of daratumumabin dialysis-dependent renal failure secondary to multiple myelomaHaematologica [Internet] 2018 [cited 2018 Jul 2] 103 e277ndashe278 Availablefrom httpwwwncbinlmnihgovpubmed29622654
12 K Batko et alDownloaded from httpsacademicoupcomndtadvance-article-abstractdoi101093ndtgfy2595086133by gueston 29 August 2018
108 Anand S Miller D Chipman G Morris D Srinivas S Daratumumab forsevere refractory proliferative glomerulonephritis with monoclonal im-mune deposits (PGNMID) ATC Abstr [Internet] 2017 [cited 2018 Jul 3]Available from httpsatcmeetingabstractscomabstractdaratumumab-for-severe-refractory-proliferative-glomerulonephritis-with-monoclonal-immune-deposits-pgnmid
109 Leung N Lager DJ Gertz MA et al Long-term outcome of renal transplan-tation in light-chain deposition disease Am J Kidney Dis [Internet] 2004[cited 2018 Feb 9] 43 147ndash153 Available from httpwwwncbinlmnihgovpubmed14712438
110 Lorenz EC Sethi S Leung N et al Recurrent membranoproliferative glo-merulonephritis after kidney transplantation Kidney Int [Internet] 2010[cited 2018 Feb 9] 77 721ndash728 Available from httpwwwncbinlmnihgovpubmed20130531
111 Leung N Nasr SH A patient with abnormal kidney function and a mono-clonal light chain in the urine Clin J Am Soc Nephrol 2016 11 1073ndash1082
112 Cibeira MT Sanchorawala V Seldin DC et al Outcome of AL amyloidosisafter high-dose melphalan and autologous stem cell transplantation long-term results in a series of 421 patients Blood [Internet] 2011 [cited 2018Feb 3] 118 4346ndash4352 Available from httpwwwncbinlmnihgovpubmed21828140
113 Gertz MA Lacy MQ Dispenzieri A et al Autologous stem cell transplantfor immunoglobulin light chain amyloidosis a status report LeukLymphoma [Internet] 2010 [cited 2018 Feb 3] 51 2181ndash2187 Availablefrom httpwwwncbinlmnihgovpubmed20958232
114 Leung N Kumar SK Glavey SV et al The impact of dialysis on the survivalof patients with immunoglobulin light chain (AL) amyloidosis undergoingautologous stem cell transplantation Nephrol Dial Transplant 2016 [cited2018 Jul 7] 31 1284ndash1289 Available from httpsacademicoupcomndtarticle-lookupdoi101093ndtgfv328
115 Badros A Barlogie B Siegel E et al Results of autologous stem cell trans-plant in multiple myeloma patients with renal failure Br J Haematol 2001[cited 2018 Jul 7] 114 822ndash829 Available from httpwwwncbinlmnihgovpubmed11564069
116 Soltero L Carbajal H Xu J et al Initial survival data of kidney transplantpatients with pre-transplant monoclonal gammopathy Clin Transplant[Internet] 2012 [cited 2018 Feb 3] 26 300ndash304 Available from httpwwwncbinlmnihgovpubmed22044717
117 Jimenez-Zepeda VH Heilman RL Engel RA et al Monoclonal gammopathyof undetermined significance does not affect outcomes in patients undergoingsolid organ transplants Transplantation [Internet] 2011 [cited 2018 Feb 3]92 570ndash574 Available from httpwwwncbinlmnihgovpubmed21712755
118 Naina HVK Harris S Dispenzieri A et al Long-term follow-up of patientswith monoclonal gammopathy of undetermined significance after kidney
transplantation Am J Nephrol 2012 [cited 2018 Feb] 35 365ndash371Available from httpwwwncbinlmnihgovpubmed22473253
119 Bansal T Garg A Snowden JA et al Defining the role of renal transplanta-tion in the modern management of multiple myeloma and other plasmacell dyscrasias Nephron Clin Pract [Internet] 2012 [cited 2018 Feb 3] 120c228 wwwkargercom
120 Hassoun H Flombaum C DrsquoAgati VD et al High-dose melphalan andauto-SCT in patients with monoclonal Ig deposition disease Bone MarrowTransplant 2008 [cited 2018 Feb 3] 42 405ndash412 Available from httpwwwncbinlmnihgovpubmed18574442
121 Herrmann SMS Gertz MA Stegall MD et al Long-term outcomes ofpatients with light chain amyloidosis (AL) after renal transplantation withor without stem cell transplantation Nephrol Dial Transplant [Internet]2011 [cited 2018 Feb 3] 26 2032ndash2036 Available from httpwwwncbinlmnihgovpubmed21543655
122 Lorenz EC Gertz MA Fervenza FC et al Long-term outcome of autolo-gous stem cell transplantation in light chain deposition disease NephrolDial Transplant [Internet] 2008 [cited 2018 Jul 5] 23 2052ndash2057 Availablefrom httpwwwncbinlmnihgovpubmed18178602
123 Merhi B Patel N Bayliss G et al Proliferative glomerulonephritis withmonoclonal IgG deposits in two kidney allografts successfully treated withrituximab Clin Kidney J [Internet] 2017 [cited 2018 Feb 10] 10 405ndash410Available from httpsacademicoupcomckjarticle-lookupdoi101093ckjsfx001
124 Barbour SJ Beaulieu MC Zalunardo NY et al Proliferative glomerulone-phritis with monoclonal IgG deposits secondary to chronic lymphocyticleukemia Report of two cases Nephrol Dial Transplant [Internet] 2011[cited 2018 Feb 10] 26 2712ndash2714 Available from httpsacademicoupcomndtarticle-lookupdoi101093ndtgfr251
125 Zand L Lorenz EC Cosio FG et al Clinical findings pathology and out-comes of C3GN after kidney transplantation J Am Soc Nephrol [Internet]2014 [cited 2018 Jul 5] 25 1110ndash1117 Available from httpwwwncbinlmnihgovpubmed24357668
126 Alfano G Fontana F Colaci E et al Monoclonal gammopathy of undeter-mined significance after kidney transplantation Transplantation [Internet]2017 [cited 2017 Oct 24] 101 e337ndashe342 Available from httpwwwncbinlmnihgovpubmed28731904
127 Bancu I Ca~nas L Juega FJ et al Outcomes of monoclonal gammopathyof undetermined significance in patients who underwent kidneytransplantation Transplant Proc [Internet] 2015 [cited 2018 Feb 10] 472344ndash2345 Available from httpwwwncbinlmnihgovpubmed26518922
Received 2632018 Editorial decision 1472018
Clinical implication of monoclonal gammopathies 13Downloaded from httpsacademicoupcomndtadvance-article-abstractdoi101093ndtgfy2595086133by gueston 29 August 2018

[Internet] 2012 [cited 2017 Dec 9] 91 889ndash896 Available from httpwwwncbinlmnihgovpubmed22237937
76 Specter R Sanchorawala V Seldin DC et al Kidney dysfunction duringlenalidomide treatment for AL amyloidosis Nephrol Dial Transplant[Internet] 2011 [cited 2018 Jul 7] 26 881ndash886 Available from httpwwwncbinlmnihgovpubmed20693160
77 Li Y Wang X OrsquoMara E et al Population pharmacokinetics of pomalido-mide in patients with relapsed or refractory multiple myeloma with variousdegrees of impaired renal function CPAA 2017 [cited 2018 Feb 4] 9133ndash145 Available from httpwwwncbinlmnihgovpubmed29184451
78 Kastritis E Gavriatopoulou M Roussou M et al Addition of cyclophos-phamide and higher doses of dexamethasone do not improve outcomes ofpatients with AL amyloidosis treated with bortezomib Blood Cancer J2017 [cited 2017 Dec 15] 7 e570 Available from httpwwwncbinlmnihgovpubmed28622303
79 Venner CP Gillmore JD Sachchithanantham S et al A matched compari-son of cyclophosphamide bortezomib and dexamethasone (CVD) versusrisk-adapted cyclophosphamide thalidomide and dexamethasone (CTD)in AL amyloidosis Leukemia [Internet] 2014 [cited 2018 Jul 5] 282304ndash2310 Available from httpwwwncbinlmnihgovpubmed25027514
80 Palladini G Sachchithanantham S Milani P et al A European collabora-tive study of cyclophosphamide bortezomib and dexamethasone inupfront treatment of systemic AL amyloidosis Blood [Internet] 2015[cited 2017 Dec 9] 126 612ndash615 Available from httpwwwncbinlmnihgovpubmed25987656
81 Kopel T Kaufman JS Hamburg N et al Endothelium-dependent and -in-dependent vascular function in advanced chronic kidney disease CJASN2017 [cited 2018 Apr 18] 12 1588ndash1594 Available from httpcjasnasnjournalsorglookupdoi102215CJN12811216
82 Palladini G Milani P Foli A et al A Phase 2 trial of pomalidomide anddexamethasone rescue treatment in patients with AL amyloidosis Blood[Internet] 2017 [cited 2018 Apr 26] 129 2120ndash2123 Available fromhttpwwwncbinlmnihgovpubmed28130212
83 Hegenbart U Bochtler T Benner A et al Lenalidomidemelphalandexa-methasone in newly diagnosed patients with immunoglobulin light chainamyloidosis results of a prospective phase 2 study with long-term followup Haematologica [Internet] 2017 [cited 2017 Dec 26] 102 1424ndash1431Available from httpwwwncbinlmnihgovpubmed28522573
84 Palladini G Milani P Foli A et al Oral melphalan and dexamethasonegrants extended survival with minimal toxicity in AL amyloidosis long-term results of a risk-adapted approach Haematologica [Internet] 2014[cited 2017 Dec 15] 99 743ndash750 Available from httpwwwncbinlmnihgovpubmed24213149
85 Payet J Livartowski J Kavian N et al Type I cryoglobulinemia in multiplemyeloma a rare entity analysis of clinical and biological characteristics ofseven cases and review of the literature Leuk Lymphoma [Internet] 201354 767ndash777 Available from httpwwwtandfonlinecomdoifull103109104281942012671481
86 Terpos E Kleber M Engelhardt M et al European Myeloma Networkguidelines for the management of multiple myeloma-related complica-tions Haematologica [Internet] 2015 [cited 2017 Dec 4] 100 1254ndash1266Available from httpwwwncbinlmnihgovpubmed26432383
87 Chanan-Khan AA Kaufman JL Mehta J et al Activity and safety of borte-zomib in multiple myeloma patients with advanced renal failure a multi-center retrospective study Blood [Internet] 2007 [cited 2018 Jul 2] 1092604ndash2606 Available from httpwwwncbinlmnihgovpubmed17138816
88 Dimopoulos MA Roussou M Gkotzamanidou M et al The role of novelagents on the reversibility of renal impairment in newly diagnosed symp-tomatic patients with multiple myeloma Leukemia 2013 27 423ndash429
89 Kouroukis TC Baldassarre FG Haynes AE et al Bortezomib in multiplemyeloma systematic review and clinical considerations Curr Oncol(Toronto Ont) [Internet] 2014 [cited 2017 Dec 4] 21 e573ndashe603Available from httpwwwncbinlmnihgovpubmed25089109
90 Zhu W Chen W Bortezomib-based treatment for multiple myelomapatients with renal impairment a systematic review and meta-analysis ofobservational studies Medicine [Internet] 2016 95 e5202 Available fromhttpwwwncbinlmnihgovpmcarticlesPMC5120900
91 Dimopoulos MA Terpos E Chanan-Khan A et al Renal impairment inpatients with multiple myeloma a consensus statement on behalf of theInternational Myeloma Working Group JCO 2010 28 4976ndash4984
92 Chauvet S Fremeaux-Bacchi V Petitprez F et al Treatment of B-cell disor-der improves renal outcome of patients with monoclonal gammopathyndashassociated C3 glomerulopathy Blood [Internet] 2017 [cited 2017 Oct 26]129 1437ndash1447 Available from httpwwwncbinlmnihgovpubmed28069603
93 Cohen C Royer B Javaugue V et al Bortezomib produces high hematolog-ical response rates with prolonged renal survival in monoclonal immuno-globulin deposition disease Kidney Int [Internet] 2015 [cited 2017 Dec25] 88 1135ndash1143 Available from httpwwwncbinlmnihgovpubmed26176826
94 Ziogas DC Kastritis E Terpos E et al Hematologic and renal improve-ment of monoclonal immunoglobulin deposition disease after treatmentwith bortezomib-based regimens Leuk Lymphoma [Internet] 2017 [cited2017 Dec 25] 58 1832ndash1839 Available from httpwwwncbinlmnihgovpubmed27967286
95 Milani P Merlini G Palladini G Novel therapies in light chain amyloid-osis Kidney Int Rep [Internet] 2018 [cited 2018 Jul 4] 3 530ndash541 Availablefrom httpwwwncbinlmnihgovpubmed29854961
96 Spizzo G Mitterer M Gunsilius E Bortezomib for the treatment of refrac-tory Type-1 cryoglobulinaemia Br J Haematol [Internet] 2010 [cited 2018Jul 7] 150 235ndash237 Available from httpdoiwileycom101111j1365-2141201008184x
97 Talamo G Claxton D Tricot G et al Response to bortezomib in refractoryType I cryoglobulinemia Am J Hematol 2008 [cited 2018 Jul 7] 83883ndash884 Available from httpwwwncbinlmnihgovpubmed18756542
98 Dimopoulos MA Roussou M Gavriatopoulou M et al Cardiac and renalcomplications of carfilzomib in patients with multiple myeloma BloodAdv 2017 [cited 2017 Dec 6] 1 449ndash454 Available from httpwwwbloodadvancesorglookupdoi101182bloodadvances2016003269
99 Strati P Nasr SH Leung N et al Renal complications in chronic lympho-cytic leukemia and monoclonal B-cell lymphocytosis the Mayo Clinic ex-perience Haematologica [Internet] 2015 [cited 2018 Jul 3] 100 1180ndash1188Available from httpwwwncbinlmnihgovpubmed26088927
100 Salama AD Pusey CD Drug insight rituximab in renal disease and trans-plantation Nat Clin Pract Nephrol [Internet] 2006 [cited 2017 Dec 8] 2221ndash230 Available from httpwwwnaturecomdoifinder101038ncpneph0133
101 Jillella AP Dainer PM Kallab AM et al Treatment of a patient with end-stage renal disease with rituximab pharmacokinetic evaluation suggestsrituximab is not eliminated by hemodialysis Am J Hematol 2002 [cited2018 Jul] 71 219ndash222 Available from httpwwwncbinlmnihgovpubmed12410580
102 Guiard E Karras A Plaisier E et al Patterns of noncryoglobulinemic glo-merulonephritis with monoclonal Ig deposits correlation with IgG sub-class and response to rituximab Clin J Am Soc Nephrol 2011 6 1609ndash1616
103 Ribes D Hachem HEL Oberic L et al Bendamustine plus rituximab forindolent B-cell lymphoma of renal significance Am J Hematol 2018 93356ndash362
104 Darwish M Bond M Hellriegel E et al Pharmacokinetic and pharmacody-namic profile of bendamustine and its metabolites Cancer ChemotherPharmacol 2015 [cited 2017 Dec 15] 75 1143ndash1154 Available from httpwwwncbinlmnihgovpubmed25829094
105 Ponisch W Moll B Bourgeois M et al Bendamustine and prednisone incombination with bortezomib (BPV) in the treatment of patients with re-lapsed or refractory multiple myeloma and light chain-induced renal fail-ure J Cancer Res Clin Oncol [Internet] 2013 [cited 2018 Jul 2] 1391937ndash1946 Available from httpwwwncbinlmnihgovpubmed24046251
106 Mateos M-V Dimopoulos MA Cavo M et al Daratumumab plus bortezo-mib melphalan and prednisone for untreated myeloma N Engl J Med2018 378 518ndash528
107 Rocchi S Tacchetti P Pantani L et al Safety and efficacy of daratumumabin dialysis-dependent renal failure secondary to multiple myelomaHaematologica [Internet] 2018 [cited 2018 Jul 2] 103 e277ndashe278 Availablefrom httpwwwncbinlmnihgovpubmed29622654
12 K Batko et alDownloaded from httpsacademicoupcomndtadvance-article-abstractdoi101093ndtgfy2595086133by gueston 29 August 2018
108 Anand S Miller D Chipman G Morris D Srinivas S Daratumumab forsevere refractory proliferative glomerulonephritis with monoclonal im-mune deposits (PGNMID) ATC Abstr [Internet] 2017 [cited 2018 Jul 3]Available from httpsatcmeetingabstractscomabstractdaratumumab-for-severe-refractory-proliferative-glomerulonephritis-with-monoclonal-immune-deposits-pgnmid
109 Leung N Lager DJ Gertz MA et al Long-term outcome of renal transplan-tation in light-chain deposition disease Am J Kidney Dis [Internet] 2004[cited 2018 Feb 9] 43 147ndash153 Available from httpwwwncbinlmnihgovpubmed14712438
110 Lorenz EC Sethi S Leung N et al Recurrent membranoproliferative glo-merulonephritis after kidney transplantation Kidney Int [Internet] 2010[cited 2018 Feb 9] 77 721ndash728 Available from httpwwwncbinlmnihgovpubmed20130531
111 Leung N Nasr SH A patient with abnormal kidney function and a mono-clonal light chain in the urine Clin J Am Soc Nephrol 2016 11 1073ndash1082
112 Cibeira MT Sanchorawala V Seldin DC et al Outcome of AL amyloidosisafter high-dose melphalan and autologous stem cell transplantation long-term results in a series of 421 patients Blood [Internet] 2011 [cited 2018Feb 3] 118 4346ndash4352 Available from httpwwwncbinlmnihgovpubmed21828140
113 Gertz MA Lacy MQ Dispenzieri A et al Autologous stem cell transplantfor immunoglobulin light chain amyloidosis a status report LeukLymphoma [Internet] 2010 [cited 2018 Feb 3] 51 2181ndash2187 Availablefrom httpwwwncbinlmnihgovpubmed20958232
114 Leung N Kumar SK Glavey SV et al The impact of dialysis on the survivalof patients with immunoglobulin light chain (AL) amyloidosis undergoingautologous stem cell transplantation Nephrol Dial Transplant 2016 [cited2018 Jul 7] 31 1284ndash1289 Available from httpsacademicoupcomndtarticle-lookupdoi101093ndtgfv328
115 Badros A Barlogie B Siegel E et al Results of autologous stem cell trans-plant in multiple myeloma patients with renal failure Br J Haematol 2001[cited 2018 Jul 7] 114 822ndash829 Available from httpwwwncbinlmnihgovpubmed11564069
116 Soltero L Carbajal H Xu J et al Initial survival data of kidney transplantpatients with pre-transplant monoclonal gammopathy Clin Transplant[Internet] 2012 [cited 2018 Feb 3] 26 300ndash304 Available from httpwwwncbinlmnihgovpubmed22044717
117 Jimenez-Zepeda VH Heilman RL Engel RA et al Monoclonal gammopathyof undetermined significance does not affect outcomes in patients undergoingsolid organ transplants Transplantation [Internet] 2011 [cited 2018 Feb 3]92 570ndash574 Available from httpwwwncbinlmnihgovpubmed21712755
118 Naina HVK Harris S Dispenzieri A et al Long-term follow-up of patientswith monoclonal gammopathy of undetermined significance after kidney
transplantation Am J Nephrol 2012 [cited 2018 Feb] 35 365ndash371Available from httpwwwncbinlmnihgovpubmed22473253
119 Bansal T Garg A Snowden JA et al Defining the role of renal transplanta-tion in the modern management of multiple myeloma and other plasmacell dyscrasias Nephron Clin Pract [Internet] 2012 [cited 2018 Feb 3] 120c228 wwwkargercom
120 Hassoun H Flombaum C DrsquoAgati VD et al High-dose melphalan andauto-SCT in patients with monoclonal Ig deposition disease Bone MarrowTransplant 2008 [cited 2018 Feb 3] 42 405ndash412 Available from httpwwwncbinlmnihgovpubmed18574442
121 Herrmann SMS Gertz MA Stegall MD et al Long-term outcomes ofpatients with light chain amyloidosis (AL) after renal transplantation withor without stem cell transplantation Nephrol Dial Transplant [Internet]2011 [cited 2018 Feb 3] 26 2032ndash2036 Available from httpwwwncbinlmnihgovpubmed21543655
122 Lorenz EC Gertz MA Fervenza FC et al Long-term outcome of autolo-gous stem cell transplantation in light chain deposition disease NephrolDial Transplant [Internet] 2008 [cited 2018 Jul 5] 23 2052ndash2057 Availablefrom httpwwwncbinlmnihgovpubmed18178602
123 Merhi B Patel N Bayliss G et al Proliferative glomerulonephritis withmonoclonal IgG deposits in two kidney allografts successfully treated withrituximab Clin Kidney J [Internet] 2017 [cited 2018 Feb 10] 10 405ndash410Available from httpsacademicoupcomckjarticle-lookupdoi101093ckjsfx001
124 Barbour SJ Beaulieu MC Zalunardo NY et al Proliferative glomerulone-phritis with monoclonal IgG deposits secondary to chronic lymphocyticleukemia Report of two cases Nephrol Dial Transplant [Internet] 2011[cited 2018 Feb 10] 26 2712ndash2714 Available from httpsacademicoupcomndtarticle-lookupdoi101093ndtgfr251
125 Zand L Lorenz EC Cosio FG et al Clinical findings pathology and out-comes of C3GN after kidney transplantation J Am Soc Nephrol [Internet]2014 [cited 2018 Jul 5] 25 1110ndash1117 Available from httpwwwncbinlmnihgovpubmed24357668
126 Alfano G Fontana F Colaci E et al Monoclonal gammopathy of undeter-mined significance after kidney transplantation Transplantation [Internet]2017 [cited 2017 Oct 24] 101 e337ndashe342 Available from httpwwwncbinlmnihgovpubmed28731904
127 Bancu I Ca~nas L Juega FJ et al Outcomes of monoclonal gammopathyof undetermined significance in patients who underwent kidneytransplantation Transplant Proc [Internet] 2015 [cited 2018 Feb 10] 472344ndash2345 Available from httpwwwncbinlmnihgovpubmed26518922
Received 2632018 Editorial decision 1472018
Clinical implication of monoclonal gammopathies 13Downloaded from httpsacademicoupcomndtadvance-article-abstractdoi101093ndtgfy2595086133by gueston 29 August 2018

108 Anand S Miller D Chipman G Morris D Srinivas S Daratumumab forsevere refractory proliferative glomerulonephritis with monoclonal im-mune deposits (PGNMID) ATC Abstr [Internet] 2017 [cited 2018 Jul 3]Available from httpsatcmeetingabstractscomabstractdaratumumab-for-severe-refractory-proliferative-glomerulonephritis-with-monoclonal-immune-deposits-pgnmid
109 Leung N Lager DJ Gertz MA et al Long-term outcome of renal transplan-tation in light-chain deposition disease Am J Kidney Dis [Internet] 2004[cited 2018 Feb 9] 43 147ndash153 Available from httpwwwncbinlmnihgovpubmed14712438
110 Lorenz EC Sethi S Leung N et al Recurrent membranoproliferative glo-merulonephritis after kidney transplantation Kidney Int [Internet] 2010[cited 2018 Feb 9] 77 721ndash728 Available from httpwwwncbinlmnihgovpubmed20130531
111 Leung N Nasr SH A patient with abnormal kidney function and a mono-clonal light chain in the urine Clin J Am Soc Nephrol 2016 11 1073ndash1082
112 Cibeira MT Sanchorawala V Seldin DC et al Outcome of AL amyloidosisafter high-dose melphalan and autologous stem cell transplantation long-term results in a series of 421 patients Blood [Internet] 2011 [cited 2018Feb 3] 118 4346ndash4352 Available from httpwwwncbinlmnihgovpubmed21828140
113 Gertz MA Lacy MQ Dispenzieri A et al Autologous stem cell transplantfor immunoglobulin light chain amyloidosis a status report LeukLymphoma [Internet] 2010 [cited 2018 Feb 3] 51 2181ndash2187 Availablefrom httpwwwncbinlmnihgovpubmed20958232
114 Leung N Kumar SK Glavey SV et al The impact of dialysis on the survivalof patients with immunoglobulin light chain (AL) amyloidosis undergoingautologous stem cell transplantation Nephrol Dial Transplant 2016 [cited2018 Jul 7] 31 1284ndash1289 Available from httpsacademicoupcomndtarticle-lookupdoi101093ndtgfv328
115 Badros A Barlogie B Siegel E et al Results of autologous stem cell trans-plant in multiple myeloma patients with renal failure Br J Haematol 2001[cited 2018 Jul 7] 114 822ndash829 Available from httpwwwncbinlmnihgovpubmed11564069
116 Soltero L Carbajal H Xu J et al Initial survival data of kidney transplantpatients with pre-transplant monoclonal gammopathy Clin Transplant[Internet] 2012 [cited 2018 Feb 3] 26 300ndash304 Available from httpwwwncbinlmnihgovpubmed22044717
117 Jimenez-Zepeda VH Heilman RL Engel RA et al Monoclonal gammopathyof undetermined significance does not affect outcomes in patients undergoingsolid organ transplants Transplantation [Internet] 2011 [cited 2018 Feb 3]92 570ndash574 Available from httpwwwncbinlmnihgovpubmed21712755
118 Naina HVK Harris S Dispenzieri A et al Long-term follow-up of patientswith monoclonal gammopathy of undetermined significance after kidney
transplantation Am J Nephrol 2012 [cited 2018 Feb] 35 365ndash371Available from httpwwwncbinlmnihgovpubmed22473253
119 Bansal T Garg A Snowden JA et al Defining the role of renal transplanta-tion in the modern management of multiple myeloma and other plasmacell dyscrasias Nephron Clin Pract [Internet] 2012 [cited 2018 Feb 3] 120c228 wwwkargercom
120 Hassoun H Flombaum C DrsquoAgati VD et al High-dose melphalan andauto-SCT in patients with monoclonal Ig deposition disease Bone MarrowTransplant 2008 [cited 2018 Feb 3] 42 405ndash412 Available from httpwwwncbinlmnihgovpubmed18574442
121 Herrmann SMS Gertz MA Stegall MD et al Long-term outcomes ofpatients with light chain amyloidosis (AL) after renal transplantation withor without stem cell transplantation Nephrol Dial Transplant [Internet]2011 [cited 2018 Feb 3] 26 2032ndash2036 Available from httpwwwncbinlmnihgovpubmed21543655
122 Lorenz EC Gertz MA Fervenza FC et al Long-term outcome of autolo-gous stem cell transplantation in light chain deposition disease NephrolDial Transplant [Internet] 2008 [cited 2018 Jul 5] 23 2052ndash2057 Availablefrom httpwwwncbinlmnihgovpubmed18178602
123 Merhi B Patel N Bayliss G et al Proliferative glomerulonephritis withmonoclonal IgG deposits in two kidney allografts successfully treated withrituximab Clin Kidney J [Internet] 2017 [cited 2018 Feb 10] 10 405ndash410Available from httpsacademicoupcomckjarticle-lookupdoi101093ckjsfx001
124 Barbour SJ Beaulieu MC Zalunardo NY et al Proliferative glomerulone-phritis with monoclonal IgG deposits secondary to chronic lymphocyticleukemia Report of two cases Nephrol Dial Transplant [Internet] 2011[cited 2018 Feb 10] 26 2712ndash2714 Available from httpsacademicoupcomndtarticle-lookupdoi101093ndtgfr251
125 Zand L Lorenz EC Cosio FG et al Clinical findings pathology and out-comes of C3GN after kidney transplantation J Am Soc Nephrol [Internet]2014 [cited 2018 Jul 5] 25 1110ndash1117 Available from httpwwwncbinlmnihgovpubmed24357668
126 Alfano G Fontana F Colaci E et al Monoclonal gammopathy of undeter-mined significance after kidney transplantation Transplantation [Internet]2017 [cited 2017 Oct 24] 101 e337ndashe342 Available from httpwwwncbinlmnihgovpubmed28731904
127 Bancu I Ca~nas L Juega FJ et al Outcomes of monoclonal gammopathyof undetermined significance in patients who underwent kidneytransplantation Transplant Proc [Internet] 2015 [cited 2018 Feb 10] 472344ndash2345 Available from httpwwwncbinlmnihgovpubmed26518922
Received 2632018 Editorial decision 1472018
Clinical implication of monoclonal gammopathies 13Downloaded from httpsacademicoupcomndtadvance-article-abstractdoi101093ndtgfy2595086133by gueston 29 August 2018