Embed Size (px)
Citation preview

Interferon in Oncological Practice: Review of InterferonBiology, Clinical Applications, and Toxicities
ERIC JONASCH, FRANK G. HALUSKA
Massachusetts General Hospital, Boston, Massachusetts, USA
Key Words. Interferon · Cancer · Clinical applications · Toxicity · Management
ABSTRACT
For the past 40 years, various forms of interferon(IFN) have been evaluated as therapy in a number ofmalignant and non-malignant diseases. With the adventof gene cloning, large quantities of pure IFN becameavailable for clinical study. This paper reviews the biol-ogy, pharmacology, and clinical applications of IFN for-mulations most commonly used in oncology. It thenreviews the most common side effects seen in patientstreated with IFN, and makes recommendations for themanagement of IFN-induced toxicity.
The major oncological indications for IFN includemelanoma, renal cell carcinoma, AIDS-related Kaposi’ssarcoma, follicular lymphoma, hairy cell leukemia,
and chronic myelogenous leukemia. Unfortunately,IFN therapy is associated with significant toxicity,which can be divided into constitutional, neuropsychi-atric, hematologic, and hepatic effects. These toxicitieshave a major impact on the patient’s quality of life, andon the physician’s ability to optimally treat the patient.Careful attention to all aspects of patient care canresult in improved tolerability of this difficult butpromising therapy. Conclusion: a better understandingof IFN biology, indications, side effect profiles, and tox-icity management will aid in optimizing its use in thetreatment of patients with cancer. The Oncologist2001;6:34-55
The Oncologist 2001;6:34-55 www.TheOncologist.com
Correspondence: Eric Jonasch, M.D., Cox 640, Division of Hematology-Oncology, 55 Fruit Street, Boston, Massachusetts02114, USA. Telephone: 617-724-6582; Fax: 617-726-6974; e-mail: [email protected] Received March 31, 2000;accepted for publication October 3, 2000. ©AlphaMed Press 1083-7159/2001/$5.00/0
INTRODUCTION
In 1957 Isaacs and Lindeman described a factor that con-ferred the property of viral interference [1]. The term inter-feron (IFN) was coined to describe this new substance. Overthe next 40 years, the IFNs have been evaluated as therapeu-tic modalities in a large number of malignant and nonmalig-nant diseases. Research has revealed diverse mechanisms ofaction, including antiviral, immune-enhancing and cytostaticactivities.
In oncology, the IFNs are an important treatment for anumber of solid tumors and hematological malignancies.These include melanoma, renal cell carcinoma, AIDS-related Kaposi’s sarcoma (KS), follicular lymphoma, hairycell leukemia, and chronic myelogenous leukemia (CML).IFN therapy is associated with significant side effectswhich have an impact on the patient’s quality of life and thephysician’s ability to optimally treat the patient. An under-standing of IFN biology, interactions, indications for use,side-effect profiles, and the management of IFN toxicitieswill aid in the optimal application of these agents in themanagement of patients with cancer.
In this report, we review the classification of the IFNs andsummarize their major mechanisms of action. We thendescribe the indications for IFN therapy in oncological prac-tice and review the etiology and management of IFN-relatedside effects.
IFN CLASSIFICATION
After the discovery of IFN, initial attempts at purifica-tion were met with little success, defying efforts at classifi-cation. Early clinical trials used crude preparations that wereless than 1% IFN by weight [2]. It was only in 1978 andthereafter that IFN was purified to homogeneity in amountsthat allowed chemical and physical characterization. Theinitial nomenclature of α, β, and γ IFN was used to catego-rize the major HPLC peaks, but was quickly adopted to des-ignate leukocyte, fibroblast, and immune IFNs, respectively[2]. Table 1 summarizes some of the major properties of thevarious IFN subtypes.
In 1980, at a meeting jointly sponsored by the NationalInstitute of Allergy and Infectious Diseases and the WorldHealth Organization, nomenclature was formally adopted
by guest on Decem
ber 2, 2018http://theoncologist.alpham
edpress.org/D
ownloaded from

Jonasch, Haluska 35
classifying IFNs into three cate-gories based on antigenic speci-ficity. IFNs were categorized asalpha (α), beta (β), and gamma(γ), corresponding to the previ-ous designations of leukocyte,fibroblast and immune IFN [3].More recently, IFNs weredivided into two major sub-groups by virtue of their abilityto bind to common receptortypes [4-6]. Type I IFNs all bindto a type I IFN receptor, andinclude IFN-α, IFN-β, IFN-ω,and IFN-τ. IFN-γ is the sole typeII IFN, and binds to a distincttype II receptor [7].
Almost all cell types producetype I IFNs. The prototypicalproduction sites for IFN-α andIFN-β are leukocytes and fibro-blasts, respectively. Their induc-tion usually follows exposure toviruses, double-stranded RNA,polypeptides, and cytokines [8].The type II IFN-γ is produced inT cells and natural killer (NK)cells following a number ofimmunological stimuli, includ-ing T cell-specific antigens,staphylococcal enterotoxin A,and the combination of phytohemagglutinin and phorbolester [2, 8]. Unlike IFN-α and -β, it is not directly inducedin cells following viral infection.
BIOLOGICAL PROPERTIES OF IFNS
The IFNs possess a broad spectrum of activity and areinvolved in complex interactions. They display antiviral
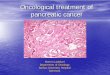
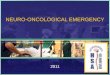
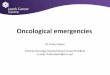
activity, impact cellular metabolism and differentiation, andpossess antitumor activity. The antitumor effects appear to bedue to a combination of direct antiproliferative, as well asindirect immune-mediated effects. Figure 1 summarizes theintracellular signaling, and Figures 2 and 3 summarize themajor effects of IFN-α and -γ on NK cells, antigen-presentingcells, macrophages, T cells, and tumor cells.
Table 1. IFN classification and properties
IFN IFN Receptor Prototypic Direct Anti- Stimulates MHC Stimulates MHC Stimulates NKType categories type cell of origin proliferative effects class I expression class II expression cell activation
Type I Alpha (α) I Leukocyte Yes Yes No Yes
Beta (β) I Fibroblast Yes Yes Slightly Yes
Omega (ω) I Leukocyte Yes Yes No Yes
Tao (τ) I OvineTrophoblast
Type II Gamma (γ) II T-cells Yes Yes Yes Less than type INK cells IFNs, delayed
P
PP
P P
P
P
P
P
P
P P
P
P
P
P
P
P
P
P
P
IFN
-AR
1
IFN
-AR
2
TY
K2
STA
T1
STA
T2
JAK
1IF
N-α
IFN
-γ
STA
T1
STA
T1
JAK
1JA
K1
JAK
2
IFN
-GR
2
IFN
-GR
2
IFN
-GR
1
IFN
-GR
1
STA
T1
STA
T1
STA
T1
STA
T1
GAS ISGISGISRE
STA
T1
STA
T2
ISG
F3γ
P
Cytoplasm
Nucleus
IFN
-γ
STA
T1
STA
T2
Figure 1. For the type I IFNs, there are two receptor subunits known, IFNAR-1 and IFNAR-2, which bind theJanus-activated kinase (Jak) molecules Tyk2 and Jak1, respectively. For IFN-γ, there are two receptor subunitsknown: IFNGR-1 and IFNGR-2, which associate with Jak1 and Jak2, respectively. Upon binding of IFN to its recep-tor, the receptor undergoes oligomerization, with transphosphorylation of Jaks followed by phosphorylation of thecytoplasmic tails of the receptor molecules. This provides a docking site for the signal transducers and activators oftranscription (Stats) which are then phosphorylated by the Jaks. The phosphorylated Stat dimers are released fromthe receptor molecules, and translocate to the nucleus, where they activate transcription of IFN-stimulated genes(ISGs). In the case of type I IFNs, ISGs can be identified by the presence of an IFN-stimulated response element(ISRE) in their promoter regions. Enhancers of IFN-γ-inducible genes contain a unique element called the IFN-γactivation site (GAS).
by guest on Decem
ber 2, 2018http://theoncologist.alpham
edpress.org/D
ownloaded from

36 Interferon in Oncological Practice
CURRENTLY AVAILABLE PREPARATIONS
The cloning of the IFN genes resulted in the availabil-ity of large quantities of pure IFN-α and -γ, allowing sub-stantive research to be done on the clinical efficacy of theIFNs in malignant and nonmalignant diseases. The clini-cal indications for the IFN subtypes are summarized inTable 2.
IFN-α2a (Roferon A; Roche Laboratories; Nutley, NJ)and IFN-α2b (Intron-A; Schering-Plough Corporation;
Kenilworth, NJ) are now produced by recombinant (r)DNAtechnology. The molecular sequences of the two rIFNs differfrom one another by a single amino acid at position 23 [9].IFN alfacon-1 (Infergen, Amgen; Thousand Oaks, CA) is arecombinant non-naturally occurring IFN, whose 166 amino-acid sequence was derived by scanning the sequences of sev-eral natural IFN-α subtypes and assigning the most frequentlyobserved amino acid in each corresponding position. Fouradditional changes were made to facilitate molecular con-struction. IFN-αn3 (Alferon N; Interferon Sciences Inc.;New Brunswick, NJ) is derived from human leukocytes.
T-cell
NK cell/macrophage
Tumorcell
Antiangiogenic
–Th1 differentiation
–Growth inhibition?
–MHC I expression
–Tumor-specific antigen–expression
–Adhesion molecule–expression
–Direct cytostatic–effects
–IFN-γ production
–Cellular cytotoxicity
–IL-1 production
–Proliferation
IFN-α
Figure 2. IFN-α possesses pleiotropic and potentially antagonistic activityin immune cells and tumors. Both stimulatory and inhibitory effects areseen in the T-cell population. A stimulatory effect is seen in natural killer(NK) cells and macrophages, which may be antagonized by the IFN-α medi-ated upregulation of major histocompatibility-1 (MHC1) in tumor cells.Direct cytostatic effects are seen in tumor cells, as well as upregulation oftumor-specific antigens and adhesion molecules. IFN-α may also haveantiangiogenic effects mediated indirectly by IFN-γ (Fig. 3).
T-cell
MacrophageAPC
Tumorcell
Antiangiogenic
Increased activation(in synergy with IL-2)
MHC class I upregulation
Decreased proliferation
Activation
MHC class IIupregulation
IFN-γ
Figure 3. IFN-γ is an activator of T-cells and macrophages, working in concertwith interleukin-2 (IL-2). IFN-γ is capable of upregulating both MHC classes Iand II, and has demonstrated direct inhibitory effects on tumor proliferation. IFN-γ is presumed to induce its antiangiogenic effects through the secretion of IFN-γinducible protein 10 (IP-10) and monokine induced by IFN-γ (MIG).
Table 2. IFN clinical indications
IFN type Trade name Manufacturing technique FDA-approved indications
IFN-α2a Roferon A rDNA NHLHairy cell leukemiaCMLAIDS-related KSChronic hepatitis C
IFN-α2b Intron A rDNA Follicular lymphomaHairy cell leukemiaAIDS-related KSMalignant melanomaCondyloma accuminataChronic hepatitis BChronic hepatitis C
IFN alfacon-1 Infergen rDNA Chronic hepatitis C
IFN-αn3 Alferon N Purified from human leukocytes Condyloma accuminata
IFN-β1a Avonex rDNA Relapsing-remitting MS (Chinese hamster ovary cells)
IFN-β1b Betaseron rDNA Relapsing-remitting MS(E. coli)
IFN-γ Actimmune rDNA Chronic granulomatous disease
by guest on Decem
ber 2, 2018http://theoncologist.alpham
edpress.org/D
ownloaded from

Jonasch, Haluska 37
IFNβ-1b is manufactured by bacterial fermentation of astrain of Escherichia coli that bears a genetically engineeredplasmid containing the gene for human IFN betaser17. Thenative gene was obtained from human fibroblasts and alteredin a way that substitutes serine for the cysteine residue foundat position 17 [10]. IFN-β1b has 165 amino acids and anapproximate molecular weight of 18,500 Da and does notinclude the carbohydrate side chains found in the naturalproduct. It is given s.c. every other day [11].
IFN-β1a (Avonex; Biogen Inc; Cambridge, MA) and IFN-β1b (Betaseron; Berlex; Richmond, CA) are recombinant proteins. IFN-β1a is a 166-amino acid glycoprotein with apredicted molecular weight of approximately 22,500 Da. Itis produced by mammalian cells (Chinese hamster ovarycells) into which the human IFN-β gene has been intro-duced. The amino acid sequence of IFN-β1a is identical tothat of natural human IFN-β. IFN-β1a is also U.S. Food andDrug Administration (FDA)-approved for treatment ofrelapsing-remitting multiple sclerosis (MS) to reduce fre-quency of relapses [12]. It may be preferable to IFN-β1bbecause of the convenience of weekly administration, therelative lack of injection site reactions, and lower incidenceof neutralizing antibodies.
IFN-γ (Actimmune; Genentech Inc; San Francisco, CA),is produced using rDNA technology. It is FDA-approved foruse in chronic granulomatous disease.
PHARMACOKINETICS
As with most peptides, oral delivery of the IFNs is notpractical due to proteolytic degradation. Subcutaneous andi.m. absorption of IFN-α and IFN-γ is >80%, and 30%-70%, respectively [13]. These routes of administrationresult in a protracted distribution phase, with maximalserum or plasma concentrations occurring after 1 to 8 h, fol-lowed by measurable concentrations for 4 to 24 h afterinjection for both IFN-α and -γ. After i.m. administration,IFN-β levels peak between 3 and 15 h, and then decline ata rate consistent with a 10-h elimination half-life. At thera-peutic dosages of 0.25 mg s.c., serum concentrations ofIFN-β are low or undetectable [14]. Intravenous adminis-tration of IFN-α or -β results in a biexponential decrease inserum concentration, and IFN-γ levels decline monoexpo-nentially. Terminal elimination half-lives range from 4-16 hfor IFN-α, 1-2 h for IFN-β and 25 to 35 min for IFN-γ [15-17]. Serum concentrations are generally measurable forbetween 8 and 24 h after i.v. injection of IFN-α and up to 4 h after i.v. injection of IFN-β and -γ.
The relationship between dose and biological responsevaries among disease types. A number of surrogate markershave been investigated to better define the dose-responserelationship of IFN. 2′5′ oligoadenylate synthetase (2-5A),
an enzyme induced by both IFN-α and -γ, is involved inIFN-mediated viral RNA degradation [18]. Introduction of2-5A into cells [19] or expression of 2-5A cDNA inhibitedcell growth rates [20]. Increased 2-5A levels were alsoshown to correlate with decreased cell cycling in mela-noma cell cultures treated with IFN [21], suggesting acausal role in its antiproliferative action. Using 2-5A activ-ity as a marker for response, a two- to sixfold increase in2-5A activity was seen over a 300-fold dose range i.m.using human lymphoblastoid IFN-α [22]. Other biologicalmarkers used to evaluate IFN response include neopterinand β2 microglobulin. Neopterin is a pteridine derivativeoriginally found in cultures of stimulated T lymphocytes[23] whose serum and urinary levels correlated with thera-peutic IFN dosages in the treatment of hairy cell leukemia[24, 25]. Small studies in melanoma [26-28] provide con-flicting data on the utility of neopterin levels in predictingresponse to immunotherapy. The human MxA protein is aGTPase with antiviral activity against orthomyxovirusesand certain other negative-strand DNA viruses [29].Unlike 2-5A, β2 microglobulin and neopterin, MxA geneexpression is induced solely by type I IFNs [30, 31], andholds promise for future cancer immunology studies. Inaggregate, these markers provide laboratory confirmationof immunological stimulation by IFN, but do not provideconsistent predictive information on the use of IFN therapyin cancer.
APPLICATION OF IFN THERAPY IN ONCOLOGICAL
PRACTICE
The IFNs have been used to treat a number of malig-nancies, with varying degrees of success. The followingsection summarizes the most common applications of IFNin current oncological practice.
Hairy Cell LeukemiaThe first report of IFN response in patients with hairy
cell leukemia was recorded in 1984 [32]. In this study,seven patients were treated with 3 × 106 U of partially puri-fied leukocyte IFN-α i.m. daily (qd). Three patients had acomplete remission (CR), four had a partial remission (PR),and remissions were maintained for 6 to 10 months. Subse-quently, 30 patients with hairy cell leukemia were treatedwith IFN-α2a, including seven who were previouslyuntreated. Nine (30%) CR and 17 (56%) PR were confirmedby bone marrow core biopsies. All patients’ peripheral bloodhematologic indices either improved or normalized [33]. Amulticenter phase II study of 64 patients published in 1986confirmed the drug’s efficacy in hairy cell leukemia [34].
IFN-α2a and 2b were FDA-approved for use in hairy cellleukemia in 1986. IFN-α is usually given over a two-year
by guest on Decem
ber 2, 2018http://theoncologist.alpham
edpress.org/D
ownloaded from

38 Interferon in Oncological Practice
period at 3 × 106 U/day. Unfortunately, upon cessation oftherapy, almost all patients will relapse. Although approvedfor use, IFN-α has been superceded by more effective thera-pies in hairy cell leukemia, including 2-deoxycoformycinand cladribine.
CML
Early StudiesPreclinical studies performed in the late 1970s sug-
gested IFN therapy had antiproliferative effects on granulo-cyte precursors [35]. In 1983, Talpaz et al. reported on sevenpatients with CML treated with IFN-α 9-15 × 106 U i.m. qd[36], five of whom developed a hematologic remission. In1986, the same group reported on 17 patients with early-phase CML who were treated with rIFN-α2a, 5 × 106 U/m2
i.m. qd [37]. Fourteen patients responded to the treatment,13 of whom had a complete hematologic remission (CHR)and one had a partial hematologic remission (PHR).Cytogenetic analysis revealed that 20%-25% of patientsexperienced long-term suppression of the Philadelphia (Ph)chromosome. At least 30 uncontrolled observational studieshave been published looking at the effect of IFN-α therapyon patients in chronic-phase CML [38]. These studies vary
greatly with respect to their reporting of outcome measures,and overall survival is often not recorded. Most studiesrecord an association between cytogenetic remission andimproved survival by landmark analysis*, with a minorityfailing to show such an association [39]. (*Landmark analy-sis is an assessment of outcome following the stratificationof patients according to a particular endpoint, in this case theachievement of cytogenetic remission.)
IFN MonotherapyIn 1994, the Italian Cooperative Group published a
study of 322 patients with untreated or minimally treatedCML randomized between IFN-α2a and conventionalchemotherapy [40]. The rate of karyotypic response was30% in the IFN group versus 5% in the chemotherapygroup. Median time to progression and overall survivalwere significantly longer in the IFN groups. Table 3 sum-marizes the five randomized studies comparing chemother-apy (busulfan and/or hydroxyurea) to IFN-α therapy[40-44]. Four of these studies conclude that IFN therapy isbetter than chemotherapy in patients with early chronic-phase CML [40-43]. In all but one of these studies, IFN wasgiven as monotherapy. The Benelux study [45] randomizedpatients to IFN plus hydroxyurea as needed to keep the
Table 3. CML: randomized studies
Author Year n Study Hematologic response (%) Medianpatients design CHR PHR survival (mos)
Broustet [44] 1991 30 IFN 53 N/A N/A
28 Hydroxurea 82 N/A N/A
Hehlmann [41] 1994 133 IFN 31 52 66*
186 Busulfan 23 69 45*
194 Hydroxyurea 39 51 56
Italian 1994 218 IFN CHR + PHR = 45% 72Cooperative 104 Hydroxyurea/ CHR + PHR = 46% 52Group [40] Busulfan (p = 0.002)
Allan [42] 1995 293 IFN 69 18 61
294 Hydroxyurea/ N/A N/A 41Busulfan (p = 0.0009)
Ohnishi [43] 1995 80 IFN 39 39 Not reached, but improved 79 Busulfan 54 43 survival in IFN arm (p = 0.029)
Benelux [45] 1998 100 IFN 62 N/A 64Hydroxyurea
95 Hydroxyurea 38 N/A 68 NS
Guilhot [50] 1997 361 IFN 55 N/A Not reached, but improvedHydroxyurea survival in IFN-cytarabine
360 IFN 66 N/A arm (p = 0.02)
HydroxyureaCytarabine (p = 0.003)
NS = not significant; *statistically significant
by guest on Decem
ber 2, 2018http://theoncologist.alpham
edpress.org/D
ownloaded from

Jonasch, Haluska 39
WBC count below 10 × 109 versus hydroxyurea alone, withno survival benefit noted in the IFN arm. Differences intrial design, inclusion criteria, treatment and documentationof response make direct comparisons between these trialsdifficult, but the evidence supports a benefit to IFN-α therapyin patients with early chronic-phase CML.
Combination TherapyIn the late 1980s, cytarabine (ara-C) was shown to sup-
press CML clones selectively in vitro [46] and demon-strated in vivo antitumor efficacy when given as a low-dosecontinuous infusion [47]. In 1992, Kantarjian et al. pub-lished a report on 60 patients with advanced phases of CMLwho received combination therapy with IFN-α 5 × 106
U/m2 daily, and low-dose ara-C 15 mg/m2 daily for twoweeks every four weeks until remission, then for one weekevery month as maintenance, compared to historical con-trols receiving IFN-α therapy alone. Patients receivingIFN-α plus ara-C had a better CHR rate compared withthose treated with IFN-α, a trend for better Ph suppressionand longer survival [48]. More recently, Kantarjian et al.compared 140 patients with chronic-phase CML receivingIFN-α at 5 × 106 and ara-C 10 mg daily to historical con-trols receiving IFN-α alone or IFN-α with intermittent ara-C [49]. The study group demonstrated a CHR in 92% ofpatients, with cytogenetic response in 74% of patients, 31%of which were complete, results that were significantly bet-ter than the control groups. The time to blastic transforma-tion and overall survival was the same as in the controlgroups. Several other observational studies report a poten-tial benefit to the combination of IFN and ara-C.Subsequently, a randomized study by Guilhot et al. indi-cated the 360 patients receiving IFN-α2b, hydroxyurea, andara-C demonstrated a significant improvement in overallsurvival and cytogenetic response when compared with 361patients receiving IFN-α2b and hydroxyurea alone [50](Table 3).
IFN-γIFN-γ has been used as therapy in chronic-phase CML.
In 1987, Kurzrock et al. reported that 6 of 30 patients withchronic-phase CML treated with rIFN-γ demonstrated CHR,and varying degrees of cytogenetic improvement [51].Subsequent studies using combinations of IFN-α and IFN-γfailed to show an improvement over treatment with IFN-αalone [52, 53], and IFN-γ is not recommended for treatmentof CML.
Bone Marrow Transplantation and IFNConcern has been raised about prior IFN-α therapy
having a negative influence on allogeneic bone marrow
transplant outcomes. Several recent studies have suggestedthis is not the case in patients who received a matched-related donor [54-56], but one report suggests adverse out-comes for patients who received a greater than six-monthcourse of IFN-α prior to undergoing a matched-unrelateddonor transplant [57].
SummaryThe major decision in otherwise healthy patients with
CML is whether to treat with IFN-α initially, or to proceedwith early allogeneic bone marrow transplantation. Outcomesafter transplantation reveal lower overall survival initiallywhen compared to IFN therapy, with a crossing-over of sur-vival curves at approximately seven years after diagnosis [38].There appears to be a survival plateau in the transplant patientpopulation, but not in the IFN-α-treated patient population.Unfortunately, most of the transplant data are nonrandomized,and there have been no direct valid comparisons between IFNtherapy and transplantation in CML. The recommendationsmade in an American Society of Hematology-sponsoredreview [38] do not strongly favor IFN-α therapy or allogeneicbone marrow transplantation therapy, but indicate that bothshould be considered. The patient’s age, stage of disease,comorbid conditions, and the patient’s and physician’s thresh-old for risk and treatment-related morbidity need to be takeninto consideration when making such a decision.
FOLLICULAR LYMPHOMA
IFN-α was first used in the treatment of patients with fol-licular lymphoma in the early 1980s [58]. Early-phase studiesshowed a 50% objective response rate. Subsequently, twophase III trials randomized patients between single alkylat-ing agents with or without IFN-α, demonstrating improvedremission duration, but no overall survival improvement [58-61]. In addition, two randomized phase III trials evaluated theaddition of IFN to combination cytoreductive chemotherapy[62, 63]. In only one of these studies was there an improvedmedian progression-free survival and overall survival in thegroup of patients receiving IFN [63].
The role of IFN-α as maintenance therapy for patientswith low-grade non-Hodgkin’s lymphoma (NHL) whoachieved tumor bulk reduction after cytoreductive chemo-therapy has also been evaluated [58, 64-69]. Most studiesdemonstrated an increased failure-free survival in patientson maintenance IFN, but no clear-cut increase in overallsurvival. One randomized study of IFN-α2b maintenancetherapy did reveal an overall survival advantage [69].
Based on the above studies, some authors recommendthat IFN-α therapy be used in combination with chemother-apy in clinically aggressive follicular NHL, and as mainte-nance therapy in patients with high tumor burden after
by guest on Decem
ber 2, 2018http://theoncologist.alpham
edpress.org/D
ownloaded from

40 Interferon in Oncological Practice
cytoreductive therapy [58]. These recommendations havenot been universally accepted. We recommend that IFN-αbe used in an investigational setting to better define its rolein the treatment of follicular lymphoma.
RENAL CELL CARCINOMA (RCC)IFN has been extensively used in the treatment of RRC.
Although there is no clear role for its use in the adjuvant set-ting, extensive work has been done to define its role in themanagement of metastatic disease. The following sectionssummarize these findings.
IFN MonotherapySingle-agent IFN has been used in over 50 clinical trials
in the treatment of metastatic RCC. Response rates in thesetrials range between 0% and 50%, with a mean of approxi-mately 15% for IFN-α and 10% for IFN-γ. There does notappear to be a clear dose-response curve in the treatment ofmetastatic RCC with rIFN-α2a or IFN-α2b [70]. Stratifi-cation of trials among those with average daily doses of <5,5-10 and >10 million units per day does not reveal any sta-tistically significant differences in outcome. A retrospectiveanalysis of prognostic markers of response suggested thatpretreatment nephrectomy and lung metastases as sole site ofmetastatic disease were markers for better outcome. Overallperformance status is another important prognostic factorpredicting response to therapy [71].
Several randomized studies have been published toquantify the benefit of IFN in metastatic RCC (Table 4A).The Medical Research Council Renal Cancer Collaboratorstrial randomized 350 patients with metastatic RCC betweenIFN-α2b and medroxyprogesterone acetate (MPA) [71]. Aninterim analysis was performed when time-to-progression
data were available for 335 patients, showing a statisticallysignificant improvement in median survival in favor of the IFNarm. Pyrhonen et al. prospectively randomized 160 patientswith locally advanced or metastatic RCC between vinblas-tine (VBL) alone and IFN-α2a plus VBL for 12 months oruntil progression of disease [72]. Both the response rates andmedian survival were superior in the IFN arm.
Role of NephrectomyThe benefit of preimmunotherapy nephrectomy was
addressed by the Southwest Oncology Group (SWOG) in arandomized trial designed to determine whether nephrec-tomy prior to systemic therapy with IFN prolonged survival(Table 4A). Patients with operable metastatic renal cancerwere randomized to two arms: immediate IFN therapy orradical nephrectomy followed by IFN therapy. BetweenJune 1991 and October 1998, 246 patients were random-ized. Median survival was significantly improved in thenephrectomy arm, but the response rate to IFN was a low4% in both arms, suggesting the survival advantage wasmainly due to surgical debulking, and not because surgeryimproved the efficacy of IFN therapy.
Combination with Interleukin 2 (IL-2)Subsequent efforts have been made to evaluate IFN
together with other biological response modifiers includingIL-2, or in combination with chemotherapeutic agents, in par-ticular 5-fluorouracil (5-FU). The combination of IFN-α andIL-2 has been extensively investigated in patients withmetastatic RCC. Phase I and II trials have demonstratedresponse rates of approximately 20%, with 5% CR [73].Treatment schedules, cytokine doses, patient selection criteriaand response criteria differ from study to study. Table 4B
Table 4A. RCC: randomized studies
Author Year n Study Response Medianpatients design rates (%) survival (mos)
IFN and Chemo- or Hormonal Therapy
MRC [71] 1999 174 IFN 10 MU s.c. tiw × 12 wks 14 6.0
176 MPA 300 mg PO qd × 12 wks 7 8.5*
Pyrhonen [72] 1999 81 VBL 0.1 mg/kg q 3 wks 2.5 8.7
79 VBL 0.1 mg/kg q 3 wks 16.5 15.6IFN 3 MU s.c. tiw wk 1 then (p = 0.0025) (p = 0.0049)IFn18 MU s.c. tiw
* statistically significant
IFN ± Nephrectomy
SWOG [156] 2000 123 Nephrectomy 4 8.1
123 Nephrectomy plus 4 12.5IFN 5 MU/m2 s.c. tiw until progression (p = 0.033)
by guest on Decem
ber 2, 2018http://theoncologist.alpham
edpress.org/D
ownloaded from

Jonasch, Haluska 41
summarizes seven randomized trials assessing the efficacy ofcombination cytokine therapy in metastatic RCC. In a phaseII trial, Atkins et al. randomly assigned patients to receivetreatment with either IL-2 alone or IL-2 and IFN-α. After 28patients were entered onto each arm, the IL-2/IFN arm wasclosed because of a failure to meet predetermined efficacy
criteria. An additional 43 patients (total 71) were assigned toreceive IL-2 alone. Responses were seen in 3 of 28 patients(11%) on IL-2/IFN-α and 12 of 71 patients (17%) on IL-2alone. The Groupe Français d’Immunotherapie randomized425 patients with metastatic RCC to a continuous i.v. infusionof IL-2, s.c. injections of IFN-α2a, or both [74]. Response
Table 4B. RCC: randomized studies
Author Year n Study Response Medianpatients design rates (%) survival (mos)
IFN and IL-2
Atkins [157] 1993 71 IL-2 0.6 MIU/kg i.v. q 8 h × 14 11 15.5days 1-5 and 15-19
28 IL-2 0.36 MIU/kg i.v. q 8 h × 14 17 16IFN 3 MU/m2 IV q 8 h × 14 NS NSdays 1-5 and 15-19
Lissoni [78] 1993 15 IL-2 3 MIU s.c. bid 5 days/wk × 6 wks 33 Survival at one
15 IL-2 3 MIU s.c. bid 5 days/wk × 6 wks 26 year: NS
IFN 5 MU/m2 s.c. tiw NS
Lummen [79] 1996 30 IFN-γ 200 µg s.c. q wk 0 13.0
30 IL-2 4.8 MIU/m2 s.c. qid days 1, 22 23 13.0IL-2 4.8 MIU/m2 s.c. bid days 2, 23IL-2 2.4 MIU/m2 s.c. bid days 3-5, 8-12, (p = 0.01) (p = 0.49)IL-2 15-19, 24-26, 29-33, 36-40
IFN 3 MU/m2 days 3, 5, 24, 26IFN 6 MU/m2 days 8, 10, 12, 15, 17,IFN 19, 29, 31, 33, 36, 38, 40
Negrier [74] 1998 138 IL-2 18 MIU/m2 qd CI 6.5 12days 1-5, 15-19 × 2 ; then days 1-5 q 3 wks
147 IFN 18 MU s.c. tiw × 10 wks 7.5 13
140 IL-2 18 MIU/m2 CI qd days 1-5, 15-19 × 2; 18.6 17then days 1-5 q 3 wk (p = 0.01) (p = 0.55)IFN 6 MU s.c. tiw in the wks IL-2 is given.
Jayson [77] 1998 29 IL-2 18 MIU s.c. days 1-5 × 3-4 wks 7 14.6
29 IL-2 18 MIU s.c. days 1-5 × 3-4 wks 0 12.5IFN 9 MU tiw × 3-4 wks (p = 0.98)
Boccardo [75] 1998 22 IL-2 18 MIU/m2 CI qd × days 1-4 wks 1,3, 22.7 307, 9, 13, 17, 21, 25
22 IFN 6 MU/m2 IM days 1, 3, 5 × 52 wks 9.0 18
22 IL-2 18 MIU/m2 CI qd × days 1-4 wks 1,5, 9, 9.0 1313, 17, 21 NS NS
IFN 6 MU/m2 i.m. days 1, 3, 5 wks 2-4, 6-8,10-12, 14-16, 18-20, 22-24
Henriksson [76] 1998 63 Tamoxifen 40 mg PO qd 3.2* 13.3
65 Tamoxifen 40 mg PO qd 7.7* 11.8
IL-2 4.8 MIU/m2 q 8 h days 1, 22 NSIL-2 4.8 MIU/m2 q 12 h days 2, 23IL-2 2.4 MIU/m2 q 12 h day 3-5, 8-12,IL-2 15-19, 24-26, 29-33, 36-40
IFN 3 MU/m2 days 3, 5, 24, 26,IFN 6 MU/m2 days 8, 10, 12, 15, 17,IFN 19, 29, 31, 33, 36, 38, 40
NS = not significant; *complete response only
by guest on Decem
ber 2, 2018http://theoncologist.alpham
edpress.org/D
ownloaded from

42 Interferon in Oncological Practice
rates and event-free survival rates were significantly betterin the combination therapy group, but overall survival rateswere not significantly different. The other randomized stud-ies assessing the role of combination IFN and IL-2 therapyfailed to demonstrate a survival advantage to this combina-tion when compared with cytokine monotherapy [75-79](Table 4B). In summary, as numerous studies have failed toshow a survival advantage for patients with metastatic RCCreceiving combination cytokine therapy, it cannot be rec-ommended as standard treatment.
Combination with IL-2 and 5-FUCombinations of IFN-α, IL-2, and 5-FU have been
evaluated in metastatic RCC. In vitro data suggestimproved efficacy of 5-FU when given in combination withIFN-α [80, 81]. An overall response rate of approximately30% has been seen in most studies [73, 82-90]. Two recentrandomized studies presented in abstract form address theefficacy of chemoimmunotherapy in metastatic RCC [91,92] (Table 4C). Negrier et al. randomized 131 patientsbetween IL-2, IFN and IL-2, IFN and 5-FU, and reported nosignificant difference in response between the two treatmentarms. Atzpodien et al. randomized patients betweenTamoxifen and IFN, IL-2 and i.v. 5-FU, and found a highlysignificant improvement in response rate and survival in thecombination therapy arm. The results from the Atzpodienstudy are encouraging, but in the absence of a confirmatorystudy, are insufficient to make IL-2, IFN, and 5-FU standardcare in metastatic RCC.
SummaryIn conclusion, IFN monotherapy in patients with metasta-
tic RCC provides a modest but significant prolongation of
survival with manageable side effects. A subset of patients,in particular those with good performance status, lung-onlydisease and resected primaries, may benefit from combina-tion chemoimmunotherapy, but more data are needed todetermine whether combination therapy is superior to IFNalone. At the current time, the best approach is to enterpatients into well-designed phase III trials that will helpanswer these questions.
MELANOMA
In 1980, Bart et al. reported on the inhibition of B16melanoma in vitro and in vivo by murine IFN [93]. Subsequentphase I studies using partially purified leukocyte IFN at dosesbelow 10 × 106 U/day resulted in few responses [94]. Otherreports using rIFN-α2a 12 × 106 U/m2 three times a week (tiw)[95], and 50 × 106 tiw i.m., respectively [96], for three monthsrevealed response rates at both dose levels of around 20%. IFNmonotherapy in patients with metastatic melanoma inducesresponses in approximately 15% and CR rates on the order of5% [97]. Predictors of favorable response were uninterruptedschedules of therapy regardless of route, with no clear advan-tage of lower or higher dosages in the range between 10 × 106
U/m2 and 50 × 106 U/m2 qd or tiw. Intermittent cyclic therapywas associated with a poorer outcome [97]. Suggestions ofresponse durability set IFN apart from DTIC as a therapy formetastatic melanoma [98].
Combination TherapyMore recently, IFN-α has been used in the context of com-
bination therapy for the treatment of metastatic melanoma.Numerous trials have been performed combining IFN withIL-2, with single-agent chemotherapy, and with Tamoxifen(Table 5A). The addition of IFN to IL-2 did not result in a
Table 4C. RCC: randomized studies
Author Year n Study Response Medianpatients design rates (%) survival (mos)
Chemoimmunotherapy
Negrier [91] 1997 70 IL-2 9 MIU s.c. days 1-6 wks 1, 3, 5, 7 1.4 N/AIFN 6 MU s.c. days 1, 3, 5 wks 1,3, 5, 7
61 IL-2 9 MIU s.c. days 1-6 wks 1, 3, 5, 7 8.2IFN 6 MU s.c. days 1, 3, 5 wks 1,3, 5, 75-FU 600 mg/m2 CI days 1-5 wks 1, 5 (p = 0.10)
Atzpodien [92] 1997 41 IL-2 10 MIU/m2 s.c. bid days 3-5 wks 39 >42 mos1, 4; 5 MIU/m2 s.c. days 1, 3, 5 wks 2,3IFN 6 MU/m2 s.c. day 1 wks 1, 4 anddays 1, 3, 5 wks 2, 3IFN 9 MU/m2 days 1, 3, 5 wks 5-85-FU 1,000 mg/m2 q wk wks 5-8
37 Tamoxifen 45 mg/m2 PO bid wks 1-8 0 14(p < 0.04)
by guest on Decem
ber 2, 2018http://theoncologist.alpham
edpress.org/D
ownloaded from

Jonasch, Haluska 43
significantly greater response rate or survival, with signifi-cantly more side effects [99]. An early study looking at thecombination of IFN and DTIC chemotherapy was promising[100], but subsequent investigations failed to demonstratean advantage to this combination [101-103].
Chemoimmunotherapy has been assessed in patientswith metastatic melanoma [104-109]. Table 5B summarizessome of the major studies looking at this treatment modality.Although increased response rates have been shown in mostof these trials, this has not translated into an increase in over-all survival. A recent abstract from the M.D. AndersonCancer Center randomized patients between cisplatin, VBLand DTIC (CVD) and CVD plus sequential infusion IL-2 andIFN therapy. This study demonstrated a survival improve-ment in the chemoimmunotherapy arm that approached sta-tistical significance [110]. The major question in treatingpatients with metastatic melanoma who are eligible for thesetrials is whether the severe toxicities encountered with
chemoimmunotherapy are worth the as-yet unproven survivalbenefits. The Eastern Cooperative Oncology Group (ECOG)3695/Cancer and Leukemia Group B (CALGB) 509802, astudy currently accruing patients and randomizing them toCVD or concomitant CVD plus IL-2 and IFN, will hopefullyprovide information to help answer this question.
Adjuvant TherapySeveral trials looked at the role of IFN-α in the adjuvant
setting for melanoma patients at high risk for relapse, includ-ing patients with deep primary lesions and those with lymphnode involvement [111-116]. Studies using relatively lowdoses of IFN (3 × 106 U tiw) failed to show an overall survivalbenefit in this patient group. In 1996, Kirkwood et al. pub-lished the results of ECOG 1684, which demonstrated both adisease-free and overall survival benefit for patients withstage III (lymph node-positive) melanoma treated with maxi-mally tolerated doses of IFN-α [113]. The regimen used in
Table 5A. Melanoma: randomized studies
Author Year n Study Response Medianpatients design rates (%) survival (mos)
IL-2 and IFN
Sparano [99] 1993 44 IL-2 6 MU/m2 q 8 h i.v. 14 doses days 1-5, 15-19 5 10.2
41 IL-2 4.5 MU/m2 i.v. q 8 h 14 doses days 1-5, 15-19 10 9.7IFN-α 3 MU/m2 i.v. q 8 h 14 doses days 1-5, 15-19 NS
IFN and chemotherapy
Falkson [100] 1991 31 DTIC 200 mg/m2 i.v. days 1-5 q 28 days 20 9.6
30 IFN-α 15 MU/m2 i.v. M-F × 3 wk, then 53 17.610 MU/m2 s.c tiw (p < 0.05) (p < 0.01)DTIC 200 mg/m2 i.v. days 1-5 q 28 d starting wk 4
Thomson [103] 1993 83 DTIC 800 mg/m2 i.v. q 21 days 17 7.8
87 DTIC (200-800 mg2) i.v. q 21 days 21 9.0IFN-α 9 MU s.c. qd NS NS
Bajetta [102] 1994 82 DTIC 800 mg/m2 i.v. q 21 days 20 11
76 DTIC 800 mg/m2 i.v. q 21 days 28 13IFN-α 3 MU s,c, tiw
84 DTIC 800 mg/m2 i.v. q 21 days 23 11IFN-α 3 MU IM days 1-3, 6 MU days 4-6 NS NSthen 9 MU IM qd
Falkson [101] 1998 69 DTIC 200 mg/m2 i.v. days 1-5 q 28 days 15 9.99
68 IFN 15 MU/m2 i.v. days 1-5 wks 1-3, then 21 9.3510 MU/m2 s.c. tiwDTIC 200 mg/m2 i.v. days 1-5 q 28 days,starting day 22
66 DTIC 200 mg/m2 i.v. days 1-5 q 28 days 19 9.54Tamoxifen 20 mg PO qdIFN 15 MU/m2 i.v. days 1-5 wks 1-3, then10 MU/m2 s.c. tiw
68 DTIC 200 mg/m2 i.v. days 1-5 q 28 days 18 7.97Tamoxifen 20 mg PO qd NS (p = 0.85)
NS = not significant
by guest on Decem
ber 2, 2018http://theoncologist.alpham
edpress.org/D
ownloaded from

44 Interferon in Oncological Practice
ECOG 1684 involved administration of IFN-α at 20 × 106 U/m2
i.v. qd for five days/week for four weeks, followed by 10 × 106
U/m2 s.c. tiw for 11 months. Based on the findings from thisstudy, the FDA approved the uses of IFN-α in stage III andstage IIB melanoma. The follow-up study ECOG 1690 showeda disease-free survival advantage in similar patient groups, butan overall survival advantage was not seen [114]. Of note, over-all survival of both the IFN and control groups in ECOG 1690is higher than the IFN arm in ECOG 1684. This may be due toa number of reasons, including patient crossover, or a favorablepatient cohort in the control arm of ECOG 1690. Results fromECOG 1694, which randomized patients between standardhigh-dose IFN and GM-K, a ganglioside vaccine developed atthe Memorial Sloan-Kettering Cancer Center, will be availablesoon. This study was closed prematurely, because a signifi-cantly greater number of relapses occurred in the vaccine arm.
SummaryAlthough concerns have been raised regarding the toxicity
of IFN therapy, the authors recommend its use in the adjuvant
setting. For stage IV disease, the role of IFN-α is less clear.The promising response rates of chemoimmunotherapy havenot translated into a hoped-for prolongation in survival.Nevertheless, in patients with good performance status, lowdisease burden and favorable disease sites (lung, skin),chemoimmunotherapy should be considered, preferably inthe setting of a clinical trial. Results from several studies willbe available in the near future to help clarify the role of IFNtherapy in both the adjuvant and metastatic settings.
KSIFN has been used in the treatment of HIV-associated
KS since 1981 [117]. Initial treatment regimens employeddoses in the 20 × 106 U/d range, which were associated withsignificant response rates, but also high levels of toxicity[118]. In subsequent studies [119], the probability ofresponding to therapy was correlated with CD4 count.Patients with CD4 counts greater than 400/mm3 responded,whereas none of those with CD4 counts of less than 150/mm3
had a response.
Table 5B. Melanoma: randomized studies
Author Year n Study Response Medianpatients design rates (%) survival (mos)
Chemoimmunotherapy
Keilholz [105] 1997 66 Starting d 3: IL-2 18 MIU/m2 i.v. CI over 6 h, 18 9IL-2then 18 MIU/m2 i.v. CI over 12 h, thenIL-218 MIU/m2 i.v. CI over 24 h, thenIL-24.5 MIU/m2 i.v. CI qd × 3 daysIFN-α 10 MU/m2 s.c. days 1-5
60 Starting d 3: IL-2 18 MIU/m2 i.v. CI over 6 h, 33 9IL-2then 18 MIU/m2 i.v. CI over 12 h, thenIL-218 MIU/m2 i.v. CI over 24 h, then (p = 0.04) NSIL-24.5 MIU/m2 i.v. CI qd × 3 daysIFN-α 10 MU/m2 s.c. days 1-5Cisplatin 100 mg/m2 day 1
Rosenberg [109] 1999 52 Cisplatin 25 mg/m2 i.v. days 2-4 and 23-25 27 15.8DTIC 220 mg/m2 i.v. days 2-4 and 23-25Tamoxifen 20 mg PO qd starting day 1
50 Cisplatin 25 mg/m2 i.v. days 2-4 and 23-25 44 10.7DTIC 220 mg/m2 i.v. days 2-4 and 23-25Tamoxifen 20 mg PO qd starting day 1IFN-α 6 MU/m2 s.c. days 5-8 and 26-29 (p = 0.071) (p = 0.052)IL-2 0.72 MIU/kg i.v. q 8 h days 5-8 and 26-29to patient tolerance
Eton [110] 2000 92 Cisplatin 20 mg/m2 i.v. qd days 1-4, 22-25 25 9.5DTIC 800 mg/m2 i.v. day 1, 22VBL 2 mg/m2 i.v. days 1-4, 22-25
91 Cisplatin 20 mg/m2 i.v. qd days 1-4, 22-25 48 11.8DTIC 800 mg/m2 i.v. day 1, 22VBL 1.5 mg/m2 i.v. days 1-4, 22-25 (p = 0.001) (p = 0.055)IL-2 9 MIU/m2 CI days 5-8, 17-20, 26-29IFN 5 MU/m2 s.c. days 5-9, 17-21, 26-30
NS = not significant; CI = continuous infusion
by guest on Decem
ber 2, 2018http://theoncologist.alpham
edpress.org/D
ownloaded from

Jonasch, Haluska 45
The combination of lower dosages of IFN-α and zidovu-dine (AZT) was found to be effective in treating HIV-associ-ated KS, including those with lower CD4 counts [120], butwith dose-limiting hematological side effects. In 1991,Scadden et al. reported that the use of GM-CSF as an adjunctto combination IFN-α/AZT therapy resulted in an improvedend-of-study absolute neutrophil count [121, 122]. Anotherreport indicated that although GM-CSF decreased the inci-dence of neutropenia in patients on IFN-α and AZT, otherIFN-related side effects precluded any dose escalation [123].More recently, Shepherd et al. reported on treatment of HIV-related KS with AZT and IFN-α at two dose levels. Allpatients received AZT 500 mg daily and were randomized toreceive IFN-α 1 × 106 U or 8 × 106 U s.c. qd. Response wasreported in 31% of high-dose therapy and 8% of low-dosetherapy patients (p = .011). Response at both dose levels washigher for patients with CD4 (+) counts greater than 150/mm3.The median time to progression was longer for patients in the8-million U arm (18 versus 13 weeks; p = .002). Both hema-tologic and nonhematologic toxicities were higher in the high-dose arm; 50 of 54 patients who received 8 × 106 U requireddose alterations in the first four months compared with only 19 of 53 patients who received 1 × 106 U (p = .0002) [124].
A phase I/II study assessed effectiveness of IFN-γ therapyin the treatment of HIV-associated KS, and showed clinicalresponse in 3 of 17 patients [125]. There does not appear to beany role for IFN-γ in the treatment of KS.
For widespread, symptomatic KS, combination cyto-toxic chemotherapy is usually the treatment of choice[126]. Paclitaxel has recently been evaluated in the treat-ment of AIDS-related KS demonstrating promising results[127, 128]. The exciting initial findings with paclitaxel willprompt direct comparisons between paclitaxel and IFN-α.Further study will allow us to determine the definitive rolefor IFN-α therapy in KS.
In summary IFN-α, either as monotherapy or in combi-nation with AZT, shows activity in HIV-positive patientsprovided they possess relatively elevated CD4 (+) lympho-cyte counts (i.e., greater than 150/mm3). For more advanceddisease, combination chemotherapy is currently the acceptedmeans of treatment for KS.
TOXICITIES
Treatment with IFN is always considered in the context ofits significant side-effect profile. Four major side effect groupsoccur: constitutional, neuropsychiatric, hematologic, andhepatic. These vary in degree, persistence and our ability tomanage them. Side effects can also be divided into those thatoccur acutely but decrease over time, and those that are chronic.The severity of many side effects appears to be directly relatedto the dose and duration of IFN therapy [129]. This section
summarizes the major types of toxicity and their etiology, andconcludes with proposed toxicity management guidelines.
Acute ToxicityToxicity can be divided into acute and chronic manifesta-
tions. In the acute setting, the patients experience fevers, chillsand rigors, usually between 3 and 6 h after receiving IFN.Patients may also experience headaches, myalgias, andmalaise. With prolonged and uninterrupted administration ofIFN, tolerance can develop to these symptoms. However,treatment breaks as short as a few days can result in the rede-velopment of rigors and chills. Transaminitis and neutropeniamay occur within the first few days of treatment, and can becontrolled by adjusting the IFN dose. Both resolve rapidlyupon cessation of treatment. If the transaminitis is not followedclosely, it can result in fatal hepatotoxicity [113].
Chronic ToxicityThe chronic symptoms experienced by patients on IFN
include fatigue (70%-100% of patients), anorexia (40%-70%),and neuropsychiatric symptoms (up to 30%). These symp-toms appear to be dose-related, and cumulative, worseningover time [9].
Mechanisms of ToxicityThe mechanisms of IFN-induced toxicity are unclear, but
are most likely multifactorial. These will be summarized inthe following section.
FatigueFatigue is the most common symptom associated with
chronic use of IFN-α, occurring in more than 70% of patients.It is frequently the dose-limiting toxicity [130]. The exact eti-ology of the fatigue is unclear, but there appears to be both apsychological and neuromuscular component [130, 131].Chronic fatigue generally worsens with continued therapy,does not exhibit tolerance, is dose-related, and does notrespond to therapy with steroids or antiinflammatory drugs.Little research has been done to analyze the neuromuscularaxis in patients on IFN to determine whether there are clearstructural or biochemical changes that can be quantified.Assessment with muscle biopsy and other diagnostic modali-ties has not been performed. Clearly, further study into the eti-ology of IFN-induced fatigue is needed to better manage thisprevalent and debilitating side effect. The first step will be tobuild into clinical trials an accurate, objective and reproducibleevaluation of patient fatigue.
Neurological ToxicitiesCentral nervous system toxicities include somnolence,
confusion, lethargy, dizziness, and impaired mental status
by guest on Decem
ber 2, 2018http://theoncologist.alpham
edpress.org/D
ownloaded from

46 Interferon in Oncological Practice
[9]. Peripheral nervous system toxicities include numbnessand tingling.
Duration of therapy appears to be the most importantfactor in determining the degree of cognitive impairment[132, 133]. Absolute dose appears to be less important.
Caraceni et al. evaluated neurotoxicities of 113 patientsreceiving IFN-α 3 × 106 U s.c. tiw for 36 months as part of arandomized trial. Particular emphasis was placed on the devel-opment of extrapyramidal signs and symptoms, psychiatricsymptoms, attention, memory, reasoning capability, psycho-logical adaptation, and quality of life [134]. Significant differ-ences between study and control groups included a higherincidence of action tremor in the treatment group. Cognitiveperformance did not differ between the two groups, but ahigher level of anxiety was recorded in the IFN group. In thequality-of-life assessment, there was a significantly greaternumber of patients who experienced fatigue.
Mood DisordersPatients with cancer in general have a higher risk of
developing clinical depression [133]. A significant minorityof patients on IFN therapy becomes depressed, in somecases leading to suicide. There are also several reports ofmania in patients on IFN [135-138]. Mood disorders canoccur in patients without predisposing factors or past historyof psychiatric problems.
In non-cancer patients, depression is associated with alter-ations in a number of bodily systems, including the endocrinesystem [133]. The mechanism by which IFN causes psychi-atric disturbances is poorly understood, and research into themechanisms underlying endogenous depression has beenperformed in patients receiving IFN to better understand theetiology of IFN-induced mood disturbances. Neuroendocrinedisturbances, including perturbation of the hypothalamic-thyroid-adrenal axis and alteration in dopamine and sero-tonin production have all been implicated [139], as havealterations in the secretion of secondary cytokines, espe-cially IL-1 [133].
Endocrine DysfunctionIn 1983, Ernstoff et al. reported that human leukocyte
IFN administration resulted in an increase in cortisol lev-els via adrenocorticotropic hormone (ACTH) stimulation[140]. More recent studies revealed that IFN-β and IFN-γboth induced ACTH, prolactin, growth hormone and corti-sol levels in patients [141], although other investigators didnot find any effect of IFN-β on anterior pituitary function[142]. An assessment of IFN-α-induced endocrine stimu-lation in patients with myeloproliferative disordersrevealed that on day 1 of therapy, a significant stimulationof the hypothalamic-pituitary axis was apparent, an effect
that had disappeared by the third week of therapy [143].The acute stimulatory effect of IFN-α on cortisol releaseappears to be mediated by the release of hypothalamiccorticotropin releasing hormone [143].
There have been reports of alterations in the levels of sexhormones during IFN therapy, and male sexual dysfunctiondoes occur [139]. The hypothalamic-pituitary-gonadal axiscan be suppressed during acute and chronic illness, and thiseffect appears to be cytokine-mediated [139]. Thus it is pos-sible that IFN-induced alteration in sex hormone levels ismediated via direct or indirect pathways.
Autoimmune-Mediated Thyroid DysfunctionThyroid dysfunction occurs in 8%-20% of patients
receiving IFN-α therapy [139]. Numerous studies report thedevelopment of overt or subclinical hyper- or hypothyroidismin patients on IFN-α for various malignancies [144-149]. Thepattern demonstrated by most patients is one of an autoim-mune thyroiditis, with a period of hyper- followed by hypo-thyroidism [139]. A few patients with hepatitis C havedeveloped symptoms of Grave’s disease while on IFN-α[139]. Investigation into etiologies of IFN-α-induced thy-roiditis suggests an indirect effect via activation of othercytokines, including IFN-γ. Preexisting autoimmune dis-ease or baseline serological abnormalities appear to predis-pose patients to developing overt autoimmune diseasewhile on IFN-α [147, 148]. Antithyroid antibodies occur inup to 16% of women and 1.5% to 3% of men in the generalpopulation, and individuals expressing baseline antithyroidantibodies have a 60% risk of developing clinical thyroiddisease during the course of therapy [139]. Treatment of MSpatients with IFN-β was shown to induce antithyroidautoantibodies and symptoms of overt hypothyroidism in asmall series of patients [150]. Treatment with IFN-γ para-doxically did not appear to induce the same number ofautoimmune side effects as IFN-α [151]. A recent studycorrelated the degree of autoimmune disease with improvedprognosis in renal cancer patients treated with IFN-α andIL-2, suggesting that autoimmune disease while on cytokinetherapy is a marker for breaking immunologic tolerance inpatients with cancer [152].
Although it is unclear how much of the IFN-mediatedtoxicity is due to endocrine dysfunction, a serum thyroidstimulating hormone (TSH) determination is indicated in apatient on IFN who complains of severe and persistentfatigue, cold sensitivity, or other symptoms suggestive ofhypothyroidism.
STUDIES AND SIDE-EFFECT PROFILES
Due to the variation in dosing and schedule, dose adjust-ment, duration of follow-up, data presentation, and disease
by guest on Decem
ber 2, 2018http://theoncologist.alpham
edpress.org/D
ownloaded from

Jonasch, Haluska 47
type in which IFN has been administered, it is difficult to make direct comparisons of side-effect profiles seen invarious studies.
Some general trends can be observed. In Table 6, sideeffects resulting from treatment of melanoma, NHL and KSwith high-dose levels of IFN (10 × 106 to 50 × 106 U/m2) arecompared. Fatigue symptoms at this dose level occur at levelsapproaching 90% in the studies that categorized this symptom.A very high incidence of fevers is also recorded. The one studythat categorized depression recorded a rate of 47%. Other sideeffects are difficult to compare due to the incompleteness of thedata, but in general it appears that the incidence of severe toxi-cities (grade III or greater) is much greater at these higher doses.
Table 7 summarizes the side-effect profiles of patientswho received IFN dosages in the range of 3 × 106 U to 5 × 106 U/m2 for a variety of cancers. Although direct com-parisons may not be quantitative, and several studies onlyrecorded the incidence of grade 3 and higher toxicities, ingeneral the degree of constitutional toxicities appears to beconsiderably lower than is seen in the studies with the higherdoses seen in Table 6, and the incidence of dose-limiting
hepatic, neuropsychiatric and hematologic toxicities appearsto be negligible.
QUALITY OF LIFE
Due to the substantial toxicities encountered during IFNtherapy, a number of groups have looked at the quality of lifeof patients undergoing IFN therapy. Cole et al. evaluated thequality of life of patients receiving high-dose IFN therapy inthe ECOG 1684 trial for stage III melanoma using theQuality-Adjusted Time Without Symptoms and Toxicity(Q-TWiST) methodology [153], which estimates the meantime spent in a series of clinical health states that differ interms of quality of life. Q-TWiST adjusts each time perioddepending on how much value the patient places on thequality of life of each health state [153]. Even if patientswere to place a very low value on the time spent on IFN,there would still be a net prolongation in overall survival onthe ECOG 1684 trial.
The same Q-TWiST methodology was used to evaluatethe quality-of-life-adjusted survival in the previously men-tioned trial randomizing patients to doxorubicin-based
Table 6. Summary of toxicities in patients receiving high-dose IFN for malignancies
Study Real [117] Creagan [96] Kirkwood [113] Creagan [116] Sertoli [159] Creagan [95] O’Connell [160]
Disease/stage Kaposi’s/HIV Melanoma IV Melanoma III Melanoma III Melanoma IV Melanoma IV NHL, CLL
Type/dose IFN-α2a 36 IFN-α2a 50 IFN-α2b 20 IFN-α2a 20 IFN-α2b IFN-α2a 12 IFN-α 12 MU IM qd MU/m2 i.m. MU/m2 IV MU/m2 i.m. tiw 10 MU/m2 i.m. MU/m2 i.m. MU/m2 i.m. tiw × 4 wks, then tiw × 12 wks 5 days/wk × 12 wks tiw tiw × 12 wks × 8 wks, then tiw × 4 wks, then until disease weekly if response,
10 MU/m2 s.c. progression and 25 MU/m2 tiw tiw × 11 mo × 4 wks if stable
disease
n patients on IFN 34 31 143 131 21 30 20
Degree of All Mod- All ≥Grade All ≥Grade All ≥Grade Mod- All Severeseverity Grades Severe Grades III Grades III Grades III Severe Grades
% % % % % % % % % % %
Constitutional 97 48Fatigue 88 87 89 20 100 43 50 90 10Anorexia 74 58 55 3 13 47 55 10Weight loss 13Fevers 94 83 24 100 10 80 85 5Myalgias 74 63 7 27Headache 62 44 5 45 0
Hepatic 64 16 N/A N/A 19 0 0 10 5
Neuropsychiatric 83 28 11 2 5 3Depression 21Dizziness/vertigo 47Confusion 23 15 5
5 5
Hematologic 64 24 N/A N/A 29 0Thrombocytopenia 35 0Anemialeukopenia 45 0 by guest on D
ecember 2, 2018
http://theoncologist.alphamedpress.org/
Dow
nloaded from

48 Interferon in Oncological Practice
combination chemotherapy with or without IFN-α2b forthe treatment of advanced follicular lymphoma [63, 154].An advantage in terms of quality-adjusted survival was seenin the patients receiving IFN regardless of the value placedon the time patients were undergoing IFN therapy [154].
Kilbridge et al. interviewed 107 patients with superficialmelanomas who did not require IFN therapy, asking themwhat value they place on a prolongation of life secondary toIFN therapy, were they to need it. The authors assessed patientpreference for a particular health state as a function of toxicityand outcome. A great majority of respondents indicatedthey preferred experiencing even severe treatment-relatedside effects for a gain in disease-free survival [155].
MANAGING IFN TOXICITY
Communication among all members of the treating teamis imperative in managing patients on IFN therapy. Eachteam member is in a position to obtain complementary infor-mation that, when put together, gives a complete picture ofthe patient’s side-effect profile. The following section willsummarize management of the major IFN side effects.
Constitutional Side EffectsConstitutional side effects are managed with copious
hydration and acetaminophen. Acetominophen is useful incontrolling the shakes, fevers and myalgias experienced by thepatient at the onset of therapy. Nonsteroidal anti-inflammatorymedications may be used if acetaminophen is not adequate in controlling these symptoms, but should be used only ifadequate control is not achieved with acetaminophen alone.
There is no recognized pharmacological antidote forIFN-induced fatigue. It is equally unclear what can be doneto alleviate this symptom short of dose decrement, or cessa-tion of treatment. Suggestions include mild exercise, goodnutritional intake, copious fluid ingestion, and stress man-agement techniques. The treating team needs to rememberthat a treatment-induced decrement in functional status can bea serious blow to a patient’s self-esteem and sense of indepen-dence [130], and that patients need encouragement and positivefeedback from their treating team. On the other hand, patientsalso need to be told that it is acceptable to draw on socialresources, which include family, friends, or hospital-basedsocial services if the patients feel they are unable to cope.
Table 7. Summary of toxicities in patients receiving low-dose IFN for malignancies
Study Real [117] Grob [158] Doveil [115] Ozer [39] Kantarjian [49]
Disease/stage Kaposi’s/HIV Melanoma II Melanoma III CML chronic-phase CML chronic-phase
Type/dose IFN IFN-α2a 3 IFN-α2a 3 Mu IFN-α2b 3 IFN-α2b 5 IFN-α 5MU i.m. qd s.c. tiw × 18 mos MU i.m. MU/m2 s.c. qd MU/m2 s.c.× 4 wks, then tiw × 12 qd + Ara-Ctiw until disease mos 10 mg s.c. qdprogression until progression
n patients on IFN 36 248 50 107 140
Degree of severity All Grades All Grades ≥Grade III ≥Grade III ≥Grade III ≥Grade III% % % % % %
ConstitutionalFatigue 83 48 <2 11Anorexia 39Weight Loss 11 11Fevers 42 4 18Myalgias 67 7Headache 42 33 <1
Hepatic N/A <1 0 13 1
Neuropsychiatric 0 4Depression 11 16 <1 4Dizziness/Vertigo 42 15 <0 11ConfusionAtaxia
Hematologic 0 0Thrombocytopenia 26Anemia 18Leukopenia <2 10
by guest on Decem
ber 2, 2018http://theoncologist.alpham
edpress.org/D
ownloaded from

Jonasch, Haluska 49
Mood DisordersForty percent of patients on IFN will experience some
degree of mood impairment, and up to 10% may becomeovertly depressed [113, 130]. It is important that the treatmentteam be aware of the potential for depression, and to incorpo-rate questions about the patient’s mood and emotional stateinto the patient’s routine evaluation. Early psychiatric referralis important, and IFN-related mood disorders can often bemanaged with measures similar to those used to treat endoge-nous depression. The occurrence of mania in patients on IFNalso needs to be kept in mind, especially after patientsundergo significant dose-reduction or treatment breaks [138].
The clinician’s natural instinct is to interdict the use of IFNin patients with any past history of depression, or a strong fam-ily history of mood disorders. We recommend that patientswith any of the above risk factors be evaluated prior to treat-ment by a psychiatrist versed in the assessment and manage-ment of cancer patients, and ideally with prior experience intreating IFN-related mood disorders [138]. These patientsshould not be denied treatment, but should be followed closelyfor signs of depression, with mood-related questions as part ofthe review of systems at each visit.
HepatotoxicityIn patients receiving high-dose i.v. IFN for stage III
melanoma, liver function tests (LFTs) need to be drawn atleast weekly, assessing for grade III transaminitis.Withholding treatment until LFTs decrease to a grade I tox-icity and restarting with a 30%-50% dose reduction is astandard approach. Recently, a report was published sug-gesting that less aggressive dose reduction can be per-formed with no decrease in patient safety or compliance[161]. Once a steady-state level of treatment is achieved,LFTs are fairly stable and assessment of liver function canbe decreased to monthly or bimonthy blood draws.
Hematologic ToxicityWeekly blood draws assessing for grade III neutropenia
need to be performed in patients receiving high-dose i.v.IFN. Dose-reduction algorithms are the same as those for
hepatotoxicity. In patients on s.c. IFN regimens, once asteady-state of treatment is established, neutrophil countsare fairly stable, although they may drift down further insome patients. In general, blood draws can be decreased toa monthly or even bimonthly schedule once stable dosingoccurs.
Endocrine ToxicityRecognition of the occurrence of hypothyroidism is
important in the management of patients on IFN. Initially,monthly TSH measurements should be performed, and ifthree sequential values are stable and within a normal range,bimonthly or quarterly evaluations may be sufficient.
SUMMARY AND RECOMMENDATIONS
IFN is a promising but incompletely understood anti-cancer agent. Clinical trials have established a number ofindications for the IFNs in both the hematological and solidtumor arenas, although the effectiveness of the IFNs is modestin most applications of the agent.
The side-effect profiles of the IFNs are substantial, and athigh doses, daunting, making the choice of IFN therapy onethat has to be weighed against the near certainty of a decrementin quality of life while on the agent. It is important that thetreating physician be aware of the four major categories of IFNtoxicity: constitutional, neuropsychiatric, hepatic, and hemato-logic. An ongoing dialogue must occur between the patientand the treating team to ensure that all aspects of IFN toxicityare addressed. A number of steps can be taken to minimize themorbidity of IFN therapy, resulting in an improvement in bothquality of life and patient compliance.
IFN has been FDA-approved for use in a number of clin-ical applications. Treatment with IFN outside of these recom-mendations should be performed in the context of a clinicaltrial designed to assess immunological endpoints and to care-fully measure type and degree of toxicities. Companion stud-ies designed to ask specific questions regarding the etiologyof IFN-induced toxicities should also be encouraged, as thisknowledge will be extremely useful in the evolution of IFN asa useful agent in the oncological armamentarium.
REFERENCES
1 Isaacs A, Lindenman J. Virus interference I. The interferon.Proc R Soc 1957;147:258-267.
2 Pestka S. The human interferon-alpha species and hybridproteins. Semin Oncol 1997;24(suppl 9):S9-4-S9-17.
3 Interferon nomenclature. Nature 1980;286:110.
4 Haque SJ, Williams BR. Signal transduction in the inter-feron system. Semin Oncol 1998;25(suppl 1):14-22.
5 Aguet M, Grobke M, Dreiding P. Various human interferon
alpha subclasses cross-react with common receptors: theirbinding affinities correlate with their specific biologicalactivities. Virology 1984;132:211-216.
6 Merlin G, Falcoff E, Aguet M. 125I-labelled human inter-ferons alpha, beta and gamma: comparative receptor-bindingdata. J Gen Virol 1985;66:1149-1152.
7 Pfeffer LM, Dinarello CA, Herberman RB et al. Biologicalproperties of recombinant alpha-interferons: 40th anniversaryof the discovery of interferons. Cancer Res 1998;58:2489-2499.
by guest on Decem
ber 2, 2018http://theoncologist.alpham
edpress.org/D
ownloaded from

50 Interferon in Oncological Practice
8 Sreevalsan T. Biological therapy with Interferon-alfa and beta:preclinical studies. In: DeVita VTJ, Hellman SMD, RosenbergSA, eds. Biologic Therapy of Cancer, Second Ed. Philadelphia:J.B. Lippincott Company, 1995;347-364.
9 Weiss K. Safety profile of interferon-alpha therapy. SeminOncol 1998;25(suppl 1):9-13.
10 Mark DF, Lu SD, Creasey AA et al. Site-specific mutagene-sis of the human fibroblast interferon gene. Proc Natl AcadSci USA 1984;81:5662-5666.
11 Witt PL, Storer BE, Bryan GT et al. Pharmacodynamics ofbiological response in vivo after single and multiple doses ofinterferon-beta. J Immunother 1993;13:191-200.
12 Jacobs LD, Cookfair DL, Rudick RA et al. Intramuscular inter-feron beta-1a for disease progression in relapsing multiple scle-rosis. The Multiple Sclerosis Collaborative Research Group(MSCRG) [published erratum appears in Ann Neurol1996;40:480]. Ann Neurol 1996;39:285-294.
13 Wills RJ. Clinical pharmacokinetics of interferons. ClinPharmacokinet 1990;19:390-399.
14 Goldstein D, Sielaff KM, Storer BE et al. Human biologicresponse modification by interferon in the absence of measur-able serum concentrations: a comparative trial of subcutaneousand intravenous interferon-beta serine. J Natl Cancer Inst1989;81:1061-1068.
15 Sarna G, Pertcheck M, Figlin R et al. Phase I study of recom-binant beta ser 17 interferon in the treatment of cancer. CancerTreat Rep 1986;70:1365-1372.
16 Rinehart JJ, Malspeis L, Young D et al. Phase I/II trial ofhuman recombinant interferon gamma in renal cell carcinoma.J Biol Response Mod 1986;5:300-308.
17 Shah I, Band J, Samson M et al. Pharmacokinetics and toleranceof intravenous and intramuscular recombinant alpha 2 interferonin patients with malignancies. Am J Hematol 1984;17:363-371.
18 Zhou A, Hassel BA, Silverman RH. Expression cloning of 2-5A-dependent RNAase: a uniquely regulated mediator ofinterferon action. Cell 1993;72:753-765.
19 Hovanessian AG, Wood JN. Anticellular and antiviraleffects of pppA(2′p5′A)n. Virology 1980;101:81-90.
20 Rysiecki G, Gewert DR, Williams BR. Constitutive expressionof a 2′,5′-oligoadenylate synthetase cDNA results in increasedantiviral activity and growth suppression. J Interferon Res1989;9:649-657.
21 Creasey AA, Eppstein DA, Marsh YV et al. Growth regula-tion of melanoma cells by interferon and (2′-5′)oligoadeny-late synthetase. Mol Cell Biol 1983;3:780-786.
22 Merritt JA, Ball LA, Sielaff KM et al. Modulation of 2′,5′-oligoadenylate synthetase in patients treated with alpha-inter-feron: effects of dose, schedule, and route of administration. J Interferon Res 1986;6:189-198.
23 Huber C, Fuchs D, Hausen A et al. Pteridines as a newmarker to detect human T cells activated by allogeneic ormodified self major histocompatibility complex (MHC)determinants. J Immunol 1983;130:1047-1050.
24 Gastl G, Aulitzky W, Tilg H et al. A biological approach tooptimize interferon treatment in hairy cell leukemia.Immunobiology 1986;172:262-268.
25 Huber C, Aulitzky W, Tilg H et al. Studies on the optimaldose and the mode of action of alpha-interferon in the treat-ment of hairy cell leukemia. Leukemia 1987;1:355-357.
26 Buzaid AC, Grimm EA, Ali-Osman F et al. Mechanism ofthe anti-tumour effect of biochemotherapy in melanoma:preliminary results. Melanoma Res 1994;4:327-330.
27 Anderson CM, Buzaid AC, Sussman J et al. Nitric oxide andneopterin levels and clinical response in stage III melanomapatients receiving concurrent biochemotherapy. Melanoma Res1998;8:149-155.
28 Bernengo MG, Quaglino P, Cappello N et al. Macrophage-mediated immunostimulation modulates therapeutic efficacyof interleukin-2 based chemoimmunotherapy in advancedmetastatic melanoma patients. Melanoma Res 2000;10:55-65.
29 Roers A, Hochkeppel HK, Horisberger MA et al. MxA geneexpression after live virus vaccination: a sensitive marker forendogenous type I interferon. J Infect Dis 1994;169:807-813.
30 Simon A, Fah J, Haller O et al. Interferon-regulated Mx genesare not responsive to interleukin-1, tumor necrosis factor, andother cytokines. J Virol 1991;65:968-971.
31 von Wussow P, Jakschies D, Hochkeppel HK et al. The humanintracellular Mx-homologous protein is specifically induced bytype I interferons. Eur J Immunol 1990;20:2015-2019.
32 Quesada JR, Reuben J, Manning JT et al. Alpha interferon forinduction of remission in hairy-cell leukemia. N Engl J Med1984;310:15-18.
33 Quesada JR, Hersh EM, Manning J et al. Treatment of hairycell leukemia with recombinant alpha-interferon. Blood1986;68:493-497.
34 Golomb HM, Jacobs A, Fefer A et al. Alpha-2 interferon ther-apy of hairy-cell leukemia: a multicenter study of 64 patients.J Clin Oncol 1986;4:900-905.
35 Verma DS, Spitzer G, Gutterman JU et al. Human leukocyteinterferon preparation blocks granulopoietic differentiation.Blood 1979;54:1423-1427.
36 Talpaz M, McCredie KB, Mavligit GM et al. Leukocyte inter-feron-induced myeloid cytoreduction in chronic myelogenousleukemia. Blood 1983;62:689-692.
37 Talpaz M, Kantarjian HM, McCredie K et al. Hematologicremission and cytogenetic improvement induced by recombinanthuman interferon alpha A in chronic myelogenous leukemia.N Engl J Med 1986;314:1065-1069.
38 Silver RT, Woolf SH, Hehlmann R et al. An evidence-basedanalysis of the effect of busulfan, hydroxyurea, interferon, andallogeneic bone marrow transplantation in treating the chronicphase of chronic myeloid leukemia: developed for theAmerican Society of Hematology. Blood 1999;94:1517-1536.
39 Ozer H, George SL, Schiffer CA et al. Prolonged subcutaneousadministration of recombinant alpha 2b interferon in patientswith previously untreated Philadelphia chromosome-positivechronic-phase chronic myelogenous leukemia: effect on remis-
by guest on Decem
ber 2, 2018http://theoncologist.alpham
edpress.org/D
ownloaded from

Jonasch, Haluska 51
sion duration and survival: Cancer and Leukemia Group Bstudy 8583. Blood 1993;82:2975-2984.
40 Interferon alfa-2a as compared with conventional chemother-apy for the treatment of chronic myeloid leukemia. The ItalianCooperative Study Group on Chronic Myeloid Leukemia. NEngl J Med 1994;330:820-825.
41 Hehlmann R, Heimpel H, Hasford J et al. Randomized com-parison of interferon-alpha with busulfan and hydroxyureain chronic myelogenous leukemia. The German CML StudyGroup. Blood 1994;84:4064-4077.
42 Allan NC, Richards SM, Shepherd PC. UK Medical ResearchCouncil randomised, multicentre trial of interferon- alpha n1for chronic myeloid leukaemia: improved survival irrespectiveof cytogenetic response. The UK Medical Research Council’sWorking Parties for Therapeutic Trials in Adult Leukaemia.Lancet 1995;345:1392-1397.
43 Ohnishi K, Ohno R, Tomonaga M et al. A randomized trialcomparing interferon-alpha with busulfan for newly diag-nosed chronic myelogenous leukemia in chronic phase. Blood1995;86:906-916.
44 Broustet A, Reiffers J, Marit G et al. Hydroxyurea versusinterferon alfa-2b in chronic myelogenous leukaemia: prelim-inary results of an open French multicentre randomized study.Eur J Cancer 1991;27(suppl 4):S18-S21.
45 Randomized study on hydroxyurea alone versus hydroxyureacombined with low-dose interferon-alpha 2b for chronicmyeloid leukemia. The Benelux CML Study Group. Blood1998;91:2713-2721.
46 Sokal JE, Leong SS, Gomez GA. Preferential inhibition bycytarabine of CFU-GM from patients with chronic granulocyticleukemia. Cancer 1987;59:197-202.
47 Robertson MJ, Tantravahi R, Griffin JD et al. Hematologicremission and cytogenetic improvement after treatment of sta-ble-phase chronic myelogenous leukemia with continuous infu-sion of low-dose cytarabine. Am J Hematol 1993;43:95-102.
48 Kantarjian HM, Keating MJ, Estey EH et al. Treatment ofadvanced stages of Philadelphia chromosome-positivechronic myelogenous leukemia with interferon-alpha andlow-dose cytarabine. J Clin Oncol 1992;10:772-778.
49 Kantarjian HM, O’Brien S, Smith TL et al. Treatment ofPhiladelphia chromosome-positive early chronic phase chronicmyelogenous leukemia with daily doses of interferon alphaand low-dose cytarabine. J Clin Oncol 1999;17:284-292.
50 Guilhot F, Chastang C, Michallet M et al. Interferon alfa-2bcombined with cytarabine versus interferon alone in chronicmyelogenous leukemia. French Chronic Myeloid LeukemiaStudy Group. N Engl J Med 1997;337:223-229.
51 Kurzrock R, Talpaz M, Kantarjian H et al. Therapy of chronicmyelogenous leukemia with recombinant interferon-gamma.Blood 1987;70:943-947.
52 Kloke O, Wandl U, Opalka B et al. A prospective randomizedcomparison of single-agent interferon (IFN)-alpha with thecombination of IFN-alpha and low-dose IFN-gamma in chronicmyelogenous leukaemia. Eur J Haematol 1992;48:93-98.
53 Wandl UB, Opalka B, Kloke O et al. Treatment of chronicmyelogenous leukemia with different cytokines. Semin Oncol1992;19(suppl 4):88-94.
54 Rodriguez J, Cortes J, Smith T et al. Determinants of prog-nosis in late chronic-phase chronic myelogenous leukemia. J Clin Oncol 1998;16:3782-3787.
55 Tomas JF, Lopez-Lorenzo JL, Requena MJ et al. Absence ofinfluence of prior treatment with interferon on the outcome ofallogeneic bone marrow transplantation for chronic myeloidleukemia. Bone Marrow Transplant 1998;22:47-51.
56 Zuffa E, Bandini G, Bonini A et al. Prior treatment withalpha-interferon does not adversely affect the outcome ofallogeneic BMT in chronic phase chronic myeloid leukemia.Haematologica 1998;83:231-236.
57 Morton AJ, Gooley T, Hansen JA et al. Association betweenpretransplant interferon-alpha and outcome after unrelateddonor marrow transplantation for chronic myelogenousleukemia in chronic phase. Blood 1998;92:394-401.
58 Ozer H, Wiernik PH, Giles F et al. Recombinant interferon-alpha therapy in patients with follicular lymphoma [publishederratum appears in Cancer 1998;83:593]. Cancer 1998;82:1821-1830.
59 Price CG, Rohatiner AZ, Steward W et al. Interferon-alpha 2bin the treatment of follicular lymphoma: preliminary results ofa trial in progress. Ann Oncol 1991;2(suppl 2):141-145.
60 Rohatiner A, Crowther D, Radford J et al. The role of inter-feron in follicular lymphoma. Proc Am Soc Clin Oncol1996;15:418.
61 Peterson BA, Petroni GR, Oken MM et al. Cyclophos-phamide versus cyclophosphamide plus interferon alfa-2b infollicular low-grade lymphomas: an intergroup phase III trial(CALGB 8691 and EST 7486). Proc Am Soc Clin Oncol1997;16:14a.
62 Smalley RV, Andersen JW, Hawkins MJ et al. Interferon alfacombined with cytotoxic chemotherapy for patients with non-Hodgkin’s lymphoma. N Engl J Med 1992;327:1336-1341.
63 Solal-Celigny P, Lepage E, Brousse N et al. Doxorubicin-con-taining regimen with or without interferon alfa-2b foradvanced follicular lymphomas: final analysis of survival andtoxicity in the Groupe d’Etude des Lymphomes Folliculaires86 Trial. J Clin Oncol 1998;16:2332-2338.
64 McLaughlin P, Cabanillas F, Hagemeister FB et al. CHOP-Bleo plus interferon for stage IV low-grade lymphoma. AnnOncol 1993;4:205-211.
65 Hiddemann W, Unterhalt M, Koch P et al. New aspects in thetreatment of advanced low-grade non-Hodgkin’s lymphomas:prednimustine/mitoxantrone versus cyclophosphamide/vincris-tine/prednisone followed by interferon alfa versus observationonly—a preliminary update of the German Low-Grade Lym-phoma Study Group. Semin Hematol 1994;31(suppl 3):32-35.
66 Unterhalt M, Herrmann R, Tiemann M et al. Prednimustine,mitoxantrone (PmM) vs cyclophosphamide, vincristine, pred-nisone (COP) for the treatment of advanced low-grade non-Hodgkin’s lymphoma. German Low-Grade Lymphoma StudyGroup. Leukemia 1996;10:836-843.
by guest on Decem
ber 2, 2018http://theoncologist.alpham
edpress.org/D
ownloaded from

52 Interferon in Oncological Practice
67 Unterhalt M, Herrmann R, Nahler M et al. Significant prolon-gation of disease-free survival in advanced low grade non-Hodgkin’s lymphomas (NHL) by interferon alfa maintenance.Blood 1995;86:439a.
68 Hagenbeek A, Carde P, Somers R et al. Interferon-alfa-2a vscontrol as maintenance therapy for low grade non-Hodgkin’slymphoma: results from a prospective randomized clinicaltrial. Proc Am Soc Clin Oncol 1995;14:386.
69 Aviles A, Duque G, Talavera A et al. Interferon alpha 2b asmaintenance therapy in low grade malignant lymphomaimproves duration of remission and survival. Leuk Lymphoma1996;20:495-499.
70 Savage PD, Muss HB. Renal cell cancer. In: De Vita VT Jr,Hellman S, Rosenberg SA, eds. Biologic Therapy of CancerSecond Ed. Philadelphia: J.B. Lippincott Company,1995;373-387.
71 Interferon-alpha and survival in metastatic renal carcinoma:early results of a randomised controlled trial. Medical ResearchCouncil Renal Cancer Collaborators. Lancet 1999;353:14-17.
72 Pyrhonen S, Salminen E, Ruutu M et al. Prospective ran-domized trial of interferon alfa-2a plus vinblastine versusvinblastine alone in patients with advanced renal cell cancer.J Clin Oncol 1999;17:2859-2867.
73 Bukowski RM. Natural history and therapy of metastaticrenal cell carcinoma: the role of interleukin-2. Cancer1997;80:1198-1220.
74 Negrier S, Escudier B, Lasset C et al. Recombinant humaninterleukin-2, recombinant human interferon alfa-2a, or both inmetastatic renal-cell carcinoma. Groupe Francais d’Immuno-therapie. N Engl J Med 1998;338:1272-1278.
75 Boccardo F, Rubagotti A, Canobbio L et al. Interleukin-2,interferon-alpha and interleukin-2 plus interferon-alpha inrenal cell carcinoma. A randomized phase II trial. Tumori1998;84:534-539.
76 Henriksson R, Nilsson S, Colleen S et al. Survival in renalcell carcinoma—a randomized evaluation of tamoxifen vsinterleukin 2, alpha-interferon (leucocyte) and tamoxifen. BrJ Cancer 1998;77:1311-1317.
77 Jayson GC, Middleton M, Lee SM et al. A randomized phaseII trial of interleukin 2 and interleukin 2- interferon alpha inadvanced renal cancer. Br J Cancer 1998;78:366-369.
78 Lissoni P, Barni S, Ardizzoia A et al. A randomized study oflow-dose interleukin-2 subcutaneous immunotherapy versusinterleukin-2 plus interferon-alpha as first line therapy formetastatic renal cell carcinoma. Tumori 1993;79:397-400.
79 Lummen G, Goepel M, Mollhoff S et al. Phase II study of inter-feron-gamma versus interleukin-2 and interferon-alpha 2b inmetastatic renal cell carcinoma. J Urol 1996;155:455-458.
80 Houghton JA, Morton CL, Adkins DA et al. Locus of the inter-action among 5-fluorouracil, leucovorin, and interferon-alpha2a in colon carcinoma cells. Cancer Res 1993;53:4243-4250.
81 Morita T, Tokue A. Biomodulation of 5-fluorouracil byinterferon-alpha in human renal carcinoma cells: relation-ship to the expression of thymidine phosphorylase. CancerChemother Pharmacol 1999;44:91-96.
82 Lopez Hanninen E, Kirchner H, Atzpodien J. Interleukin-2based home therapy of metastatic renal cell carcinoma: risksand benefits in 215 consecutive single institution patients. J Urol 1996;155:19-25.
83 Hofmockel G, Langer W, Theiss M et al. Immunochemo-therapy for metastatic renal cell carcinoma using a regimenof interleukin-2, interferon-alpha and 5-fluorouracil. J Urol1996;156:18-21.
84 Sella A, Kilbourn RG, Gray I et al. Phase I study of inter-leukin-2 combined with interferon-alpha and 5-fluorouracilin patients with metastatic renal cell cancer. Cancer Biother1994;9:103-111.
85 Dutcher J, Logan T, Gordon M et al. 5FU + subcutaneous (SC)interleukin-2 (IL2) plus SC Intron (IFN) in metastatic renal cellcancer (RCC) patients (pts). A CWG study. Proc Am Soc ClinOncol 1996:272a.
86 Sella A, Zukiwski A, Robinson E et al. Interleukin-2 (IL-2)with interferon-α (IFN-α) and 5-fluorouracil (5-FU) in patients(pts) with metastatic renal cell carcer (RCC). Proc Am SocClin Oncol 1994:237a.
87 Gitlitz B, Dolan N, Pierce W et al. Fluoropyrimidines plus inter-leukin-2 and inteferon-α in the treatment of metastatic renal cellcarcinoma: the UCLA Kidney Cancer Program. Proc Am SocClin Oncol 1996:248a.
88 Olencki T, Bukowski R, Budd G et al. Phase I/II trial ofsimultaneously administered rIL-2/rHuIFNα2a and 5-FU inpatients (pts) with metastatic renal cell carcinoma (RCC).Proc Am Soc Clin Oncol 1996:263.
89 Ellerhorst JA, Sella A, Amato RJ et al. Phase II trial of 5-flu-orouracil, interferon-alpha and continuous infusion inter-leukin-2 for patients with metastatic renal cell carcinoma.Cancer 1997;80:2128-2132.
90 Tourani JM, Pfister C, Berdah JF et al. Outpatient treatmentwith subcutaneous interleukin-2 and interferon alfa administra-tion in combination with fluorouracil in patients with metastaticrenal cell carcinoma: results of a sequential nonrandomizedphase II study. Subcutaneous Administration PropeukinProgram Cooperative Group. J Clin Oncol 1998;16:2505-2513.
91 Négrier S, Escudier B, Douillard J et al. Randomized studyof interleukin-2 (IL2) and interferon (IFN) with or without5-FU (FUCY study) in metastatic renal cell carcinoma(MRCC). Proc Am Soc Clin Oncol 1997;16.
92 Atzpodien J, Kirchner H, Franzke A et al. Results of a random-ized clinical trial comparing SC interleukin-2, SC alpha-2a-interferon, and IV bolus 5-fluorouracil against oral tamoxifen inprogressive metastatic renal cell carcinoma patients. Proc AmSoc Clin Oncol 1997;16:32a.
93 Bart RS, Porzio NR, Kopf AW et al. Inhibition of growth ofB16 murine malignant melanoma by exogenous interferon.Cancer Res 1980;40:614-619.
94 Krown SE, Burk MW, Kirkwood JM et al. Human leukocyte(alpha) interferon in metastatic malignant melanoma: theAmerican Cancer Society phase II trial. Cancer Treat Rep1984;68:723-726.
by guest on Decem
ber 2, 2018http://theoncologist.alpham
edpress.org/D
ownloaded from

Jonasch, Haluska 53
95 Creagan ET, Ahmann DL, Green SJ et al. Phase II study oflow-dose recombinant leukocyte A interferon in dissemi-nated malignant melanoma. J Clin Oncol 1984;2:1002-1005.
96 Creagan ET, Ahmann DL, Green SJ et al. Phase II study ofrecombinant leukocyte A interferon (rIFN-alpha A) in dis-seminated malignant melanoma. Cancer 1984;54:2844-2849.
97 Kirkwood JM. Interferon therapy: melanoma. In: DeVitaVT, Hellman S, Rosenberg SA, eds. Biologic Therapy ofCancer, Second Ed. Philadelphia: J.B. Lippincott Company,1995;388-411.
98 Agarwala SS, Kirkwood JM. Interferons in melanoma. CurrOpin Oncol 1996;8:167-174.
99 Sparano JA, Fisher RI, Sunderland M et al. Randomizedphase III trial of treatment with high-dose interleukin-2 eitheralone or in combination with interferon alfa-2a in patientswith advanced melanoma. J Clin Oncol 1993;11:1969-1977.
100 Falkson CI, Falkson G, Falkson HC. Improved results withthe addition of interferon alfa-2b to dacarbazine in the treat-ment of patients with metastatic malignant melanoma. J ClinOncol 1991;9:1403-1408.
101 Falkson CI, Ibrahim J, Kirkwood JM et al. Phase III trial ofdacarbazine versus dacarbazine with interferon alpha- 2b versusdacarbazine with tamoxifen versus dacarbazine with interferonalpha-2b and tamoxifen in patients with metastatic malignantmelanoma: an Eastern Cooperative Oncology Group study. J Clin Oncol 1998;16:1743-1751.
102 Bajetta E, Di Leo A, Zampino MG et al. Multicenter random-ized trial of dacarbazine alone or in combination with two dif-ferent doses and schedules of interferon alfa-2a in the treatmentof advanced melanoma. J Clin Oncol 1994;12:806-811.
103 Thomson DB, Adena M, McLeod GR et al. Interferon-alpha 2adoes not improve response or survival when combined withdacarbazine in metastatic malignant melanoma: results of amulti-institutional Australian randomized trial. Melanoma Res1993;3:133-138.
104 Legha SS, Ring S, Bedikian A et al. Treatment of metastaticmelanoma with combined chemotherapy containing cisplatin,vinblastine and dacarbazine (CVD) and biotherapy using inter-leukin-2 and interferon-alpha. Ann Oncol 1996;7:827-835.
105 Keilholz U, Goey SH, Punt CJ et al. Interferon alfa-2a andinterleukin-2 with or without cisplatin in metastatic melanoma:a randomized trial of the European Organization for Researchand Treatment of Cancer Melanoma Cooperative Group. J ClinOncol 1997;15:2579-2588.
106 Buzaid AC, Bedikian A, Houghton AN. Systemic chemother-apy and biotherapy. In: Balch CM, Houghton AM, Sober AJ etal., eds. Cutaneous Melanoma, Third Ed. St. Louis: QualityMedical Publishing, Inc., 1998;405-418.
107 Legha SS, Ring S, Papadopoulos N et al. A prospective evalu-ation of a triple-drug regimen containing cisplatin, vinblastine,and dacarbazine (CVD) for metastatic melanoma. Cancer1989;64:2024-2029.
108 Legha SS, Buzaid AC. Role of recombinant interleukin-2 incombination with interferon-alfa and chemotherapy in the treat-
ment of advanced melanoma. Semin Oncol 1993;20(suppl9):27-32.
109 Rosenberg SA, Yang JC, Schwartzentruber DJ et al.Prospective randomized trial of the treatment of patientswith metastatic melanoma using chemotherapy with cis-platin, dacarbazine, and tamoxifen alone or in combinationwith interleukin-2 and interferon alfa-2b. J Clin Oncol1999;17:968-975.
110 Eton O, Legha S, Bedikian A et al. Phase III randomized trialof cisplatin, vinblastine and dacarbazine (CVD) plusInterleukin-2 (IL2) and Interferon-alpha-2b (INF) versusCVD in patients (Pts) with metastatic melanoma. Proc AmSoc Clin Oncol 2000;19:2174.
111 Kokoschka EM, Trautinger F, Knobler RM et al. Long-termadjuvant therapy of high-risk malignant melanoma with inter-feron alpha 2b. J Invest Dermatol 1990;95(suppl 6):193S-197S.
112 Pehamberger H, Soyer HP, Steiner A et al. Adjuvant inter-feron alfa-2a treatment in resected primary stage II cutaneousmelanoma. Austrian Malignant Melanoma CooperativeGroup. J Clin Oncol 1998;16:1425-1429.
113 Kirkwood JM, Strawderman MH, Ernstoff MS et al. Interferonalfa-2b adjuvant therapy of high-risk resected cutaneousmelanoma: the Eastern Cooperative Oncology Group Trial EST1684. J Clin Oncol 1996;14:7-17.
114 Kirkwood JM, Ibrahim J, Sondak V et al. Preliminary analy-sis of the E1690/S9111/C9190 intergroup postoperativeadjuvant trial of high-and low-dose IFNa2b (HDI and LDI)in high-risk primary or lymph node metastatic melanoma.Proc Am Soc Clin Oncol 1999;18:537a.
115 Doveil GC, Fierro MT, Novelli M et al. Adjuvant therapy ofstage IIIb melanoma with interferon alfa-2b: clinical andimmunological relevance. Dermatology 1995;191:234-239.
116 Creagan ET, Dalton RJ, Ahmann DL et al. Randomized, sur-gical adjuvant clinical trial of recombinant interferon alfa-2ain selected patients with malignant melanoma. J Clin Oncol1995;13:2776-2783.
117 Real FX, Oettgen HF, Krown SE. Kaposi’s sarcoma and theacquired immunodeficiency syndrome: treatment with highand low doses of recombinant leukocyte A interferon. J ClinOncol 1986;4:544-551.
118 Krown SE, Real FX, Cunningham-Rundles S et al. Preliminaryobservations on the effect of recombinant leukocyte A inter-feron in homosexual men with Kaposi’s sarcoma. N Engl J Med1983;308:1071-1076.
119 Lane HC, Kovacs JA, Feinberg J et al. Anti-retroviral effectsof interferon-alpha in AIDS-associated Kaposi’s sarcoma.Lancet 1988;2:1218-1222.
120 Krown SE. Approaches to interferon combination therapy in the treatment of AIDS [discussion 38-41]. Semin Oncol1990;17(suppl 1):11-15.
121 Scadden DT, Bering HA, Levine JD et al. GM-CSF as an alter-native to dose modification of the combination zidovudine andinterferon-alpha in the treatment of AIDS-associated Kaposi’ssarcoma. Am J Clin Oncol 1991;14(suppl 1):S40-S44.
by guest on Decem
ber 2, 2018http://theoncologist.alpham
edpress.org/D
ownloaded from

54 Interferon in Oncological Practice
122 Scadden DT, Bering HA, Levine JD et al. Granulocyte-macrophage colony-stimulating factor mitigates the neutropeniaof combined interferon alfa and zidovudine treatment ofacquired immune deficiency syndrome-associated Kaposi’s sar-coma [published erratum appears in J Clin Oncol 1992;10:346].J Clin Oncol 1991;9:802-808.
123 Krown SE, Paredes J, Bundow D et al. Interferon-alpha,zidovudine, and granulocyte-macrophage colony-stimulat-ing factor: a phase I AIDS Clinical Trials Group study inpatients with Kaposi’s sarcoma associated with AIDS. J ClinOncol 1992;10:1344-1351.
124 Shepherd FA, Beaulieu R, Gelmon K et al. Prospective random-ized trial of two dose levels of interferon alfa with zidovudine forthe treatment of Kaposi’s sarcoma associated with humanimmunodeficiency virus infection: a Canadian HIV ClinicalTrials Network study. J Clin Oncol 1998;16:1736-1742.
125 Heagy W, Groopman J, Schindler J et al. Use of IFN-gammain patients with AIDS. J Acquir Immune Defic Syndr1990;3:584-590.
126 Northfelt DW. Treatment of Kaposi’s sarcoma. Currentguidelines and future perspectives. Drugs 1994;48:569-582.
127 Welles L, Saville MW, Lietzau J et al. Phase II trial withdose titration of paclitaxel for the therapy of human immun-odeficiency virus-associated Kaposi’s sarcoma. J Clin Oncol1998;16:1112-1121.
128 Gill PS, Tulpule A, Espina BM et al. Paclitaxel is safe andeffective in the treatment of advanced AIDS-related Kaposi’ssarcoma. J Clin Oncol 1999;17:1876-1883.
129 Borden EC, Parkinson D. A perspective on the clinical effec-tiveness and tolerance of interferon-alpha. Semin Oncol1998;25(suppl 1):3-8.
130 Dalakas MC, Mock V, Hawkins MJ. Fatigue: definitions,mechanisms, and paradigms for study. Semin Oncol1998;25(suppl 1):48-53.
131 Dean GE, Spears L, Ferrell BR et al. Fatigue in patients withcancer receiving interferon alpha. Cancer Pract 1995;3:164-172.
132 Pavol MA, Meyers CA, Rexer JL et al. Pattern of neurobe-havioral deficits associated with interferon alfa therapy forleukemia. Neurology 1995;45:947-950.
133 Valentine AD, Meyers CA, Kling MA et al. Mood and cog-nitive side effects of interferon alfa therapy. Semin Oncol1998;25(suppl 1):39-47.
134 Caraceni A, Gangeri L, Martini C et al. Neurotoxicity of inter-feron alfa in melanoma therapy: results from a randomizedcontrolled trial. Cancer 1998;83:482-489.
135 Adams F, Fernandez F, Mavligit G. Interferon induced organicmental disorders associated with unsuspected pre-existing neurologic abnormalities. J Neurooncol 1988;6:355-359.
136 Carpiniello B, Orru MG, Baita A et al. Mania induced bywithdrawal of treatment with interferon alfa [letter]. ArchGen Psychiatry 1998;55:88-89.
137 Strite D, Valentine AD, Meyers CA. Manic episode in two
patients treated with inteferon alfa. J Neuropsychiatry ClinNeurosci 1997;9:273-276.
138 Greenberg DB, Jonasch E, Gadd MA et al. Adjuvant therapyof melanoma with interferon-alpha-2b is associated withmania and bipolar syndromes. Cancer 2000;89:356-362.
139 Jones TH, Wadler S, Hupart KH. Endocrine-mediated mech-anisms of fatigue during treatment with interferon-alpha.Semin Oncol 1998;25(suppl 1):54-63.
140 Ernstoff MS, Fusi S, Kirkwood JM. Parameters of interferonaction: I. Immunological effects of whole cell leukocyte inter-feron (IFN-alpha) in phase I-II trials. J Biol Response Mod1983;2:528-539.
141 Nolten WE, Goldstein D, Lindstrom M et al. Effects ofcytokines on the pituitary-adrenal axis in cancer patients. J Interferon Res 1993;13:349-357.
142 Yamada S, Takada K, Tsuchida S et al. A study of anteriorpituitary hormones secretion in patients with glioma receivinginterferon-beta treatment. Endocr J 1996;43:335-338.
143 Gisslinger H, Svoboda T, Clodi M et al. Interferon-alpha stim-ulates the hypothalamic-pituitary-adrenal axis in vivo and invitro. Neuroendocrinology 1993;57:489-495.
144 Burman P, Totterman TH, Oberg K et al. Thyroid autoimmu-nity in patients on long term therapy with leukocyte-derivedinterferon. J Clin Endocrinol Metab 1986;63:1086-1090.
145 Oberg K, Norheim I, Lind E et al. Treatment of malignant car-cinoid tumors with human leukocyte interferon: long-termresults. Cancer Treat Rep 1986;70:1297-1304.
146 Scalzo S, Gengaro A, Boccoli G et al. Primary hypothy-roidism associated with interleukin-2 and interferon alpha-2therapy of melanoma and renal carcinoma. Eur J Cancer1990;26:1152-1156.
147 Conlon KC, Urba WJ, Smith JW II et al. Exacerbation ofsymptoms of autoimmune disease in patients receivingalpha-interferon therapy. Cancer 1990;65:2237-2242.
148 Gisslinger H, Gilly B, Woloszczuk W et al. Thyroid autoimmu-nity and hypothyroidism during long-term treatment with recom-binant interferon-alpha. Clin Exp Immunol 1992;90:363-367.
149 Sacchi S, Kantarjian H, O’Brien S et al. Immune-mediated andunusual complications during interferon alfa therapy in chronicmyelogenous leukemia. J Clin Oncol 1995;13:2401-2407.
150 Rotondi M, Oliviero A, Profice P et al. Occurrence of thyroidautoimmunity and dysfunction throughout a nine-month fol-low-up in patients undergoing interferon-beta therapy formultiple sclerosis. J Endocrinol Invest 1998;21:748-752.
151 Kung AW, Jones BM, Lai CL. Effects of interferon-gammatherapy on thyroid function, T-lymphocyte subpopulationsand induction of autoantibodies. J Clin Endocrinol Metab1990;71:1230-1234.
152 Franzke A, Peest D, Probst-Kepper M et al. Autoimmunityresulting from cytokine treatment predicts long-term survivalin patients with metastatic renal cell cancer. J Clin Oncol1999;17:529-533.
by guest on Decem
ber 2, 2018http://theoncologist.alpham
edpress.org/D
ownloaded from

153 Cole BF, Gelber RD, Kirkwood JM et al. Quality-of-life-adjusted survival analysis of interferon alfa-2b adjuvanttreatment of high-risk resected cutaneous melanoma: anEastern Cooperative Oncology Group study. J Clin Oncol1996;14:2666-2673.
154 Cole BF, Solal-Celigny P, Gelber RD et al. Quality-of-life-adjusted survival analysis of interferon alfa-2b treatment foradvanced follicular lymphoma: an aid to clinical decisionmaking. J Clin Oncol 1998;16:2339-2344.
155 Kilbridge KL, Nease RF, Sober AJ et al. Patient utilities foradjuvant Interferon (IFN) treatment for high-risk melanoma.Proc Am Soc Clin Oncol 1999:411a.
156 Flanigan RC, Blumenstein BA, Salmon SE et al. Cytoreductionnephrectomy in metastatic renal cancer: the results ofSouthwest Oncology Group Trial 8949. Proc Am Soc ClinOncol 2000:3.
157 Atkins MB, Sparano J, Fisher RI et al. Randomized phase IItrial of high-dose interleukin-2 either alone or in combination
with interferon alfa-2b in advanced renal cell carcinoma. J ClinOncol 1993;11:661-670.
158 Grob JJ, Dreno B, de la Salmoniere P et al. Randomised trialof interferon alpha-2a as adjuvant therapy in resected primarymelanoma thicker than 1.5 mm without clinically detectablenode metastases. French Cooperative Group on Melanoma.Lancet 1998;351:1905-1910.
159 Sertoli MR, Bernengo MG, Ardizzoni A et al. Phase II trial ofrecombinant alpha-2b interferon in the treatment of metastaticskin melanoma. Oncology 1989;46:96-98.
160 O’Connell MJ, Colgan JP, Oken MM et al. Clinical trial ofrecombinant leukocyte A interferon as initial therapy for favor-able histology non-Hodgkin’s lymphomas and chronic lym-phocytic leukemia. An Eastern Cooperative Oncology Grouppilot study. J Clin Oncol 1986;4:128-136.
161 Jonasch E, Kumar UN, Linette GP et al. Adjuvant high-doseinterferon alfa-2b in patients with high-risk melanoma [inProcess Citation]. Cancer J Sci Am 2000;6:139-145.
Jonasch, Haluska 55
Wagon Wheel, Massachusetts
©A
rthur
T. S
karin
, M.D
.
by guest on Decem
ber 2, 2018http://theoncologist.alpham
edpress.org/D
ownloaded from