Embed Size (px)
Citation preview

Wessel et Schmidt-Gollwitzer, Intrauterine death of one twin 467
J. Perinat. Med.16 (1988) 467
Intrauterine death of a single fetus in twin pregnancies
Jens Wessel1 and Karin Schmidt-Gollwitzer2
JFree University of Berlin, University Clinic Rudolf Virchow, Gynaecological ClinicCharlottenburg, Berlin, West Germany2Fa. Schering AG, Berlin, West Germany
1 Introduction
The intrauterine death of a single fetus in twinpregnancies is a rare event in obstetrics. Apartfrom individual case reports, the literature doesalso contain reports on larger study populations[1, 6, 8, 11]. Both the further management of thepregnancy taking into account the risk for thesurviving twin and the mother and the procedureto be employed at delivery are of particular clinicalinterest. Special account must be taken of thecauses which led to the intrauterine demise andthe neonatal period of the surviving twin must beclosely monitored. We report on our experience ofthis pathological course of pregnancy over the lastsix years.
Curriculum vitae
JENS WESSEL, M.D., wasborn 1953 in Lüneburg,Germany. He studied bio-logy and social affairs1973-1979 and medicine1979-1985. Until 1986 hewas research associate atthe Forensic Science Insti-tute of the Free Universityof Berlin. Doctoral thesis in1986. Since 1986 he hasbeen research associate atthe Universitäts-Frauenklinik Charlottenburg at the FreeUniversity of Berlin.
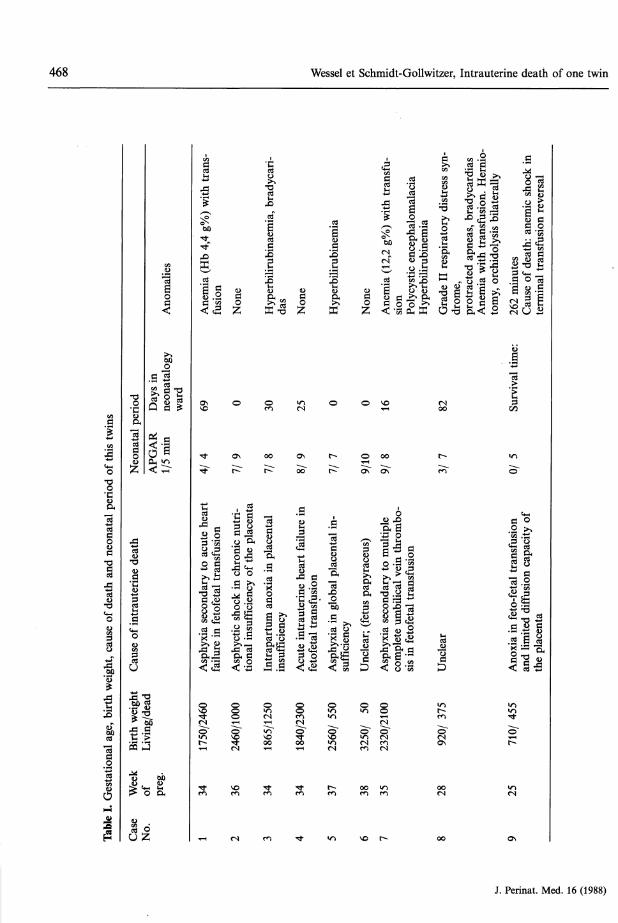
2 ResultsIn the period 1982-1987, our hospital encoun-tered nine twin pregnancies in which one of thetwins was dead at the time of delivery. The inci-dence is 0.10% referred to all births (n = 8.808) inthe six-year observation period, but 5.42% re-ferred to all twin births (n = 186). The maternalage was 33.1 years (age range 26—41 years). Sixwomen were para 1, two were para 2 and one waspara 3. The average age of the pregnancy at thetime of delivery was 33.4 weeks (25 — 38 weeks)(table I). An autopsy was performed on all thedead twins and the placentas were examined his-tologically.The birth weight of the surviving twin (table I) wasless than 1,000 g in two cases, between 1,500 and2,500 g in five and above 2,500 g in two cases.Course of the neonatal period: Cases 2, 5 and 6 didnot need to be transferred to the Department for
Neonatology, and the neonatal period was normalapart from hyperbilirubinaemia in Case No. 5.The other six newboras (< 35th week of preg-nancy) all required treatment and the neonatalperiod differed in each case (table I). Of the twinsborn live, one died (Case No. 9).Apart from the extreme immaturity at birth (25thweek of pregnancy), the cause of death was anemicshock secondary to terminal shunt reversal in fe-tofetal transfusion (table I).
The twins who died in utero were mostly hypo-trophic (Case Nos. 2, 3, 4, 8 and 9), although 2were eutrophic (Nos. 1 and 7).
Apart from Case No. 6 (fetus papyraceus), thereasons for the big differences in the weight of thetwins which died in utero were the different periodsof gestation and, in particular shifts of weightbetween the two twin partners in fetofetal trans-fusion.
1988 by Walter de Gruyter & Co. Berlin · New York
468 Wessel et Schmidt-Gollwitzer, Intrauterine death of one twin
.S'jsC/D
3's•βo•c&111
eigh
t, ca
use
of d
eath
£
05?
1ο1Λ1
Μ
iEH
Ό•g&3S§(U£
IdO
<
gsO.s 3
siS-ec? 0 hQ S g
fV>
< ·§2!OH «n
< ̂
1g
Caus
e of
intra
uter
i
ill='S -S«3
•a ωD
ί> ο α
J .£
11sO
° O
scd
1l<<a
s
*·τΓ
1
y to
acu
tetra
nsfu
sio]
Asp
hyxi
a se
cond
arfa
ilure
in fe
tofe
tal
l
£1sf•«-H
m
^
go
o
ON
r^
i!
chro
nic
nof
the
pla
Asp
hyct
ic s
hock
intio
nal
insu
fficie
ncy
11m
es
1Icd"
lirub
inae
mi
£PH
K ^
0m
00
r^
3"A_aΛ*
Intra
partu
m a
noxi
iin
suffi
cienc
y
(N
Ό00
m
m
go£
(N
ON
OO
.s8i^
Acu
te in
traut
erin
efe
tofe
tal
trans
fusio
i
Smo~S
m
^
lirub
inem
ia
^1K
o
ot^
.s
plac
enta
lA
sphy
xia
in g
loba
lsu
fficie
ncy
»n
|<N
m
«n
g*
0
0
ON~
1IgEi-Tcd
|
s5f(Nm
00m
VO
• CΈ &1 1 15 1 ί|^ o >^
i U is II tc- .a 5 ^cd t« ^B »— ι
1 α ^ & ^ ί<-^a o^
^O (NT-H 00
00 l>
ON m
D χ)U g2 °
Asp
hyxi
a se
cond
arco
mpl
ete
umbi
lical
sis in
feto
feta
l tr
n
Unc
lear
S »n
S ^o~ o~es °^
in oom (N
r- oo
g.S .g
Pf li||| uill II||| ||I
Λ "g cd o o 131 S 1 ^ ^ 1 Ί5 < 2 ^υΰ
i' '-
Id•fe^
00
•n
0"
α οo ^
1}"S '^
l ^ c d^T3 ^.S - g
lit§0~
^
es
ON
J. Perinat. Med. 16 (1988)
Wessel et Schmidt-Gollwitzer, Intrauterine death of one twin 469
The cause of intrauterine death was placental in-sufficiency in three cases and a fetofetal transfu-sion syndrome in another three. Heart failure infetofetal transfusion was the cause in Case No. 4,while the cause of death remained unclear in CaseNos. 6 and 8.Grade I maceration was seen in Case No. 1, GradeII in numbers 2 and 7, and Grade III in numbers4, 5 and 8. Two fetuses displayed no signs ofmaceration, one (Case No. 3) under the picture ofacute maternal pre-eclampsia, the other (CaseNo. 9) after unsuccessful tocolysis in prematurelabor pains in the 25th week of pregnacy (fetofetaltransfusion had been suspected since the 22ndweek on the basis of the echographic finding of adifference in growth).No malformations were observed in the twinswhich died in utero.
3 Method of delivery
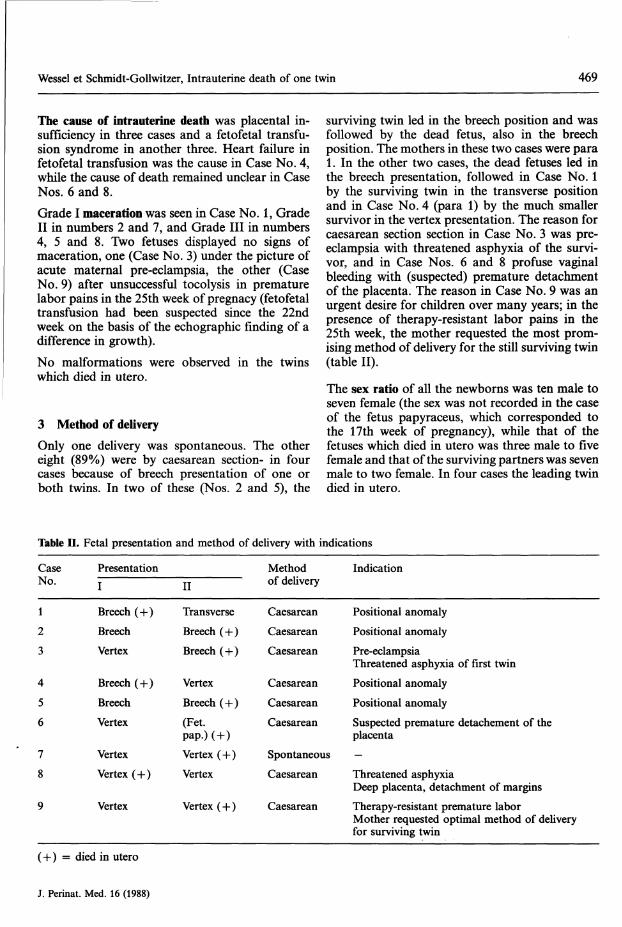
Only one delivery was spontaneous. The othereight (89%) were by caesarean section- in fourcases because of breech presentation of one orboth twins. In two of these (Nos. 2 and 5), the
surviving twin led in the breech position and wasfollowed by the dead fetus, also in the breechposition. The mothers in these two cases were para1. In the other two cases, the dead fetuses led inthe breech presentation, followed in Case No. 1by the surviving twin in the transverse positionand in Case No. 4 (para 1) by the much smallersurvivor in the vertex presentation. The reason forcaesarean section section in Case No. 3 was pre-eclampsia with threatened asphyxia of the survi-vor, and in Case Nos. 6 and 8 profuse vaginalbleeding with (suspected) premature detachmentof the placenta. The reason in Case No. 9 was anurgent desire for children over many years; in thepresence of therapy-resistant labor pains in the25th week, the mother requested the most prom-ising method of delivery for the still surviving twin(table II).
The sex ratio of all the newborns was ten male toseven female (the sex was not recorded in the caseof the fetus papyraceus, which corresponded tothe 17th week of pregnancy), while that of thefetuses which died in utero was three male to fivefemale and that of the surviving partners was sevenmale to two female. In four cases the leading twindied in utero.
Table Π. Fetal presentation and method of delivery with indications
CaseNo.
PresentationI II
Methodof delivery
Indication
1 Breech (+) Transverse Caesarean Positional anomaly2 Breech Breech (+) Caesarean Positional anomaly3 Vertex Breech (+) Caesarean Pre-eclampsia
Threatened asphyxia of first twin4 Breech (+) Vertex Caesarean Positional anomaly5 Breech Breech (+) Caesarean Positional anomaly6 Vertex (Fet. Caesarean Suspected premature detachement of the
pap.) (+) placenta7 Vertex Vertex (+) Spontaneous —8 Vertex (+) Vertex Caesarean Threatened asphyxia
Deep placenta, detachment of margins9 Vertex Vertex (+) Caesarean Therapy-resistant premature labor
Mother requested optimal method of deliveryfor surviving twin
(+) = died in utero
J. Perinat. Med. 16 (1988)
470 Wessel et Schmidt-Gollwitzer, Intrauterine death of one twin
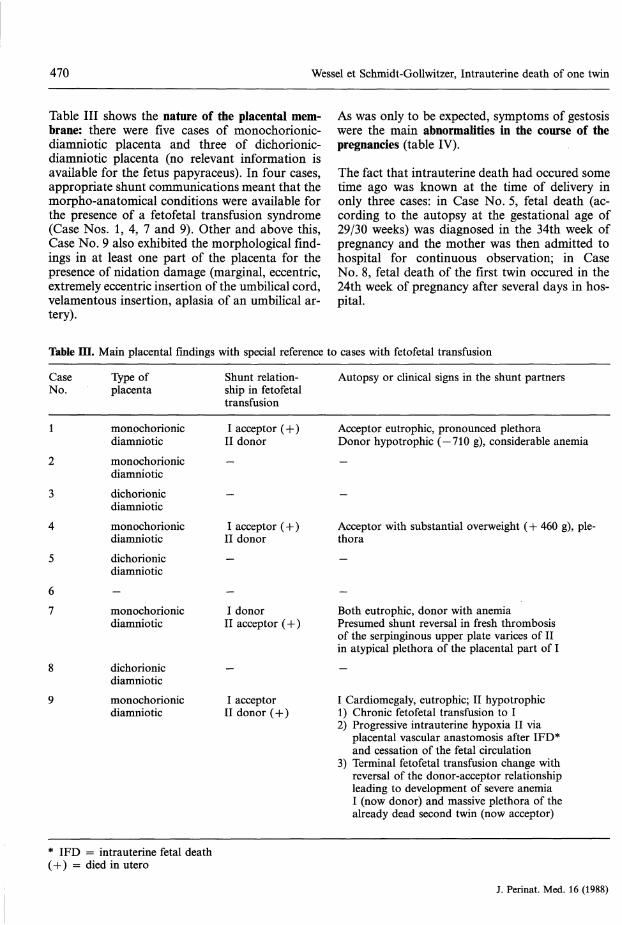
Table III shows the nature of the placental mem-brane: there were five cases of monochorionic-diamniotic placenta and three of dichorionic-diamniotic placenta (no relevant information isavailable for the fetus papyraceus). In four cases,appropriate shunt communications meant that themorpho-anatomical conditions were available forthe presence of a fetofetal transfusion syndrome(Case Nos. 1, 4, 7 and 9). Other and above this,Case No. 9 also exhibited the morphological find-ings in at least one part of the placenta for thepresence of nidation damage (marginal, eccentric,extremely eccentric insertion of the umbilical cord,velamentous insertion, aplasia of an umbilical ar-tery).
As was only to be expected, symptoms of gestosiswere the main abnormalities in the course of thepregnancies (table IV).
The fact that intrauterine death had occured sometime ago was known at the time of delivery inonly three cases: in Case No. 5, fetal death (ac-cording to the autopsy at the gestational age of29/30 weeks) was diagnosed in the 34th week ofpregnancy and the mother was then admitted tohospital for continuous observation; in CaseNo. 8, fetal death of the first twin occured in the24th week of pregnancy after several days in hos-pital.
Table ΠΙ. Main placental findings with special reference to cases with fetofetal transfusion
CaseNo.
Type ofplacenta
Shunt relation-ship in fetofetaltransfusion
Autopsy or clinical signs in the shunt partners
1
2
3
4
5
monpchorionicdiamnioticmonochorionicdiamnioticdichorionicdiamnioticmonochorionicdiamnioticdichorionic
I acceptor (+)II donor—
-
I acceptor (+)II donor
Acceptor eutrophic, pronounced plethoraDonor hypotrophic (— 710 g), considerable anemia—
-
Acceptor with substantial overweight (+ 460 g),thora
pie-
diamniotic
monochorionicdiamniotic
dichorionicdiamnioticmonochorionicdiamniotic
I donor Both eutrophic, donor with anemiaII acceptor (+) Presumed shunt reversal in fresh thrombosis
of the serpinginous upper plate varices of IIin atypical plethora of the placental part of I
I acceptor I Cardiomegaly, eutrophic; II hypotrophicII donor (+) 1) Chronic fetofetal transfusion to I
2) Progressive intrauterine hypoxia II viaplacental vascular anastomosis after IFD*and cessation of the fetal circulation
3) Terminal fetofetal transfusion change withreversal of the donor-acceptor relationshipleading to development of severe anemiaI (now donor) and massive plethora of thealready dead second twin (now acceptor)
* IFD = intrauterine fetal death(+) = died in utero
J. Perinat. Med. 16 (1988)
Wessel et Schmidt-Gollwitzer, Intrauterine death of one twin 471
Table IV. Events during the course of pregnancy
Case 31st week:No. 1 Pre-eclampsia, hydramniosCase 26th week:No. 3 Pre-eclampsia
32nd week:Pre-eclampsia33rd/34th week:Pre-eclampsia
Case 29th/31st week:No. 4 Premature labour (oral tocolysis)Case 14th week:No. 8 Imminent abortion
Urinary tract infection23rd week:Pre-eclampsia
Case 22nd week:No. 9 Pyelonephritis with urinary
stasis on right23rd week:Percutaneous nephrostomy right24th week:Premature labour (i. v. tocolysis, unsuccess-ful)
A gestationel age fo 28 weeks was reached underfurther hospitalized observation with the occur-ence of severe vaginal bleeding and signs of as-phyxia in the cardiotocogram (CTG); in the otherCase (No. 6, fetus papyraceus), the death of thefetus (gestational age corresponding to the 17thweek) was diagnosed in the 20th week of preg-nancy, but the mother was not admitted to hos-pital for observation. In four cases, the acute di-agnosis of intrauterine death of one of the fetusesdemanded curtailment of the period of hospital-ized observation because of prepathological CTGsigns from the surviving twin (Nos. 4 and 7),advanced gestational age (Nos. 2, 4 and 7) orunstoppable labor pains (Nos. 1 and 4).No complications secondary to the intrauterinefetal death were observed as regards maternal mor-bidity or the puerperium.
4 DiscussionIt is a well-known fact that twin pregnancies areassociated with more risks than single pregnancies.The mortality rate for twins is 3—4 times higherthan for single newborns and the morbidity rateis also increased, in particular because of the high
rate of premature births. The second twin is atparticular risk in this respect. The rate of intra-uterine deaths is also about 2 — 3 times higher thanthat for single pregnancies [8]. The intrauterinedemise of a twin raises diverse questions concern-ing the risk to the surviving twin and the motherand the method of delivery. The occurence of suchan event is rare, but the possibility of an increaseresulting from an above-average rate of twin preg-nancies in association with stimulation ovulationinduction or in vitro fertilization programs shouldbe kept in mind.
The incidence of 0.10% in our study populationreferred to all births is compatible with the figuresreported by LUMME and SAARIKOVSKI (0.03%) [8]and LITSCHGI and STUCKI (0.07%) [6]. Referred toall twin births in the observation period, we re-corded an incidence of 5.4% compared to valuesof 2.2% [8] and 6.8% [6].
At 33.1 years, the average maternal age was dis-tinctly higher than in the other studies (e.g. 28years in the study by LUMME and SAARIKOVSKI).
In agreement with other authors, the results ofour study show that the intrauterine death of atwin in itself does not expose the mother to anyincreased risk. However, the number of mothersin our study who were observed for a prolongedperiod after diagnosis of the intrauterine deathwas relatively small (n = 3, of whom 2 were hos-pitalized). Among others, SKELLY draws attentionto the risk of consumptive coagulopathy (with adecrease of fibrinogen, increase of break-downproducts of fibrinogen and reduced platelet count)which can be induced by thromboplastin absorp-tion from the tissue of the dead fetus or from theplacenta [13]. This clotting disorder usually occursa few weeks after the death: PRITCHARD [10] re-ported an incidence of 25% in the case of deadfetuses in single pregnancies retained for morethan 4—5 weeks. This risk appears to be muchlower in the case of a single fetal death in a twinpregnancy [13]. According to ROMERO et al., thematernal clotting status should nevertheless beclosely monitored and, if necessary, heparinizationperformed [12]. We performed prophylactic low-dose heparinization in one of our patients.
Of the surviving twins in utero, one died afterdelivery (11.1%); the gestational age in this casewas 25 weeks, the lowest in our study. Otherauthors report mortality rates of between 4.1%[8] and 23.1% [6].
J. Perinat. Med. 16 (1988)
472 Wessel et Schmidt-Gollwitzer, Intrauterine death of one twin
Three of the children in our study exhibited anAPGAR score of < 4 at 1 minute. In agreementwith RIEHN, it can be assumed that there is noassociation between the vitality of the survivingnewborn and the length of time between the in-trauterine death of the other twin and the delivery[11]. In analogy to single pregnancies or to twinpregnancies which are not complicated by the in-trauterine death of one of the twins, morbiditydepends mainly on the gestational age achieved;at an average of 33.4 weeks, this was compara-tively low in our study.
Therfe was no need to transfer the surviving part-ner to the neonatology deparment in cases inwhich a gestational age of at least 35 weeks hadbeen achieved.
At 89%, the high rate of caesarean section as themethod of delivery was striking. Other studygroups report rates of between 9% [11] and 93%[1]. The incidence of caesarean sections is largelydetermined by the obstetrician's attitude to thedelivery of breech presentations [8]: in our studypopulation, this positional anomaly was the soleindication in four cases. It was also the sole indi-cation for caesarean section in half of the casesreported by D'ALTON, while LITSCHGI and STUCKIperformed caesarean section in only one case ofbreech presentation. At the same time, the pro-portion of women with a longer period of hospi-talized supervision after diagnosis of the intra-uterine fetal death was considerably larger in thestudies with a low incidence of caesarean section.The greater readiness to deliver by caesarean sec-tion is more understandable in cases in whichintrauterine fetal death is diagnosed acutely andother risk factors such as profuse vaginal bleedingare present at the same time. Neither the survivingnor the dead twins displayed any congenital mal-formations in our study. LITSCHGI and STUCKI [6]reported just one case of hypospadia (in a studypopulation of 13 twin pairs), RIEHN [11] observedone case of hydrocephaly and one pair of twinswith thanatophoric dwarfism out of 11 pairs oftwins, while LUMME and SAARIKOVSKI [8] reporteda total of 6 (including multiple) malformations outof 24 pairs of twins.
The attending pediatricians interpreted the case ofpolycystic encephalomalacia (in the donor) as theconsequence of severe intrauterine hypoxia sec-ondary to fetofetal transfusion. An arterial occlu-sion due either to disseminated intravascular clot-ting in fetofetal exchange of thromboplastic ma-
terial of the dead fetus through vascular shunts orto embolisation of infarcted, necrotic bits of tissueis regarded as the cause of this encephalomalaciain surviving partners of monochorionic twins[3, 8].The incidence of fetus papyraceus with delivery ofthe living twin partner is reported as 1:12,000births or 1:184 twin pregnancies [9]. Most of thefetuses die in the second trimester [4, 7]. The con-dition arises as a result of compression of themummified fetus between the amnion and theuterine wall or the fetal partner over a sufficientlylong period, which explains why the conditionsdoes not occur in single pregnancies or when deathof a twin occurs at a later time (third trimester).A fetus papyraceus can develop in the case of bothmonochorionic and dichorionic placentas [7] aswell as in the fetofetal transfusion syndrome [5].
The incidence of monochorionic placentas in ourstudy is compatible with that reported by otherinvestigators: 5 of 9 cases, 4 of them with a feto-fetal transfusion syndrome. The acceptor died inutero in 3 cases, the donor in one. KLOOS andVOGEL make a distinction between a chronic fe-tofetal transfusion syndrome with early embryonalmanifestation (development of a holoacadius) anda late-embryonal/early-fetal manifestation afterformation of the vascular system of both twins.The latter generally leads to hypotrophy and ane-mia of the donor and to cardiomegaly and ple-thora of the acceptor. The date of manifestationfor the subchronic form is assumed to be a fewweeks before term; the diagnosis is made partlyon the basis of considerable anaemia of the donorwithout any distinct difference in the weights ofthe twins. In the acute form, the donor can sufferan acute hemorrhagic shock and the acceptor anacute load on the cardiac volume as a result of asudden transfer of blood. The development of afetus papyraceus in the fetofetal transfusion syn-drome is also possible [5].The transfusion syndromes reported here werechronic in three cases (Numbers 1, 4, and 9) andsubchronic in one (No. 7). A blood transfusionwas required in the neonatal period in the twochronic cases in which the donor survived (one ofthem with the remarkably low initial Hb value of4.4 g%). Case Numbers 7 and 9 suffered a reversalof the donor-acceptor relationship in terminalshunt reversal, presumably shortly before delivery.According to published experience, the procedureand timing for the termination of a pregnancy
J. Perinat. Med. 16 (1988)
Wessel et Schmidt-Gollwitzer, Intrauterine death of one twin 473
with a surviving twin are determined primarily bythe state of maturity of this child. The type ofplacenta should also be taken into account: if adizygotic situation is definitely present (ultrasounddemonstration of two placentas, different sexes),it can generally be assumed that there is no in-creased fetal risk, and the spontaneous onset oflabour can be awaited under monitoring of thefetal and maternal parameters. If a monochorionicsituation cannot be ruled out, there is an increasedrisk to the surviving twin through shunt commu-nications, which can lead to DIG induced deathor organ damage [2, 3].
The following general guidelines are proposed inthe event of the intrauterine death of a fetus in atwin pregnancy:
There is no directly associated increased risk tothe mother; the relevant parameters should bemonitored continuously to detect any disturbancesin the clotting system. The intrauterine death of
one twin is not an absolute indication for termi-nation of the pregnancy of the surviving partner.Thorough CTG and ultrasound monitoringshould be performed in order to detect any riskfactors which, in the case of a monochorionicplacenta, might develop for the survivor as a resultof a shunt reversal in a fetofetal transfusion syn-drome. This is also the only way in which thecondition of the surviving twin can be monitored,and it is this condition which — apart from com-plications (hemorrhage) which might occur at anytime — determines the time and method of deliv-ery. An attempt should always be made to achievepulmonary maturity through the attainment of anappropriate gestational age or by induction. Closesupervision of the condition of the mother andsurviving child is essential and the mother shouldbe admitted to hospital for this purpose. Ideally,it should be possible as a result to reduce theincidence of caesarean sections to that for uncom-plicated twin pregnancies.
AbstractThe paper reports on nine twin pregnancies in the years1982-1987 with the intrauterine death of a single fetus.The incidence of 0.10% is consistant with that reportedin other comparable studies.Evaluation of the causes of death shows a preponderanceof asphyxia. A fetofetal transfusion syndrome occurredin 4 cases. Eight of the pregnancies were terminated bycaesarean section. One of the surviving children died in
the neonatal period. The course of the neonatal periodin the other babies was determined mainly by the stateof maturity. No increased maternal morbidity was ob-served.On the basis of this and other experience described inthe literature, some general guidelines are proposed forthe management of the further pregnancy and deliveryin such high-risk cases.
Keywords: Intrauterine death of one twin, mode of delivery, neonatal morbidity, placentation, twin pregnancy.
Zusammenfassung
Intrauteriner Fruchttod eines Feten bei Zwillingsschwan-gerschaftenDer intrauterine Tod eines Feten bei Zwillingsschwan-gerschaften ist ein seltenes Ereignis in der Geburtshilfe.Dabei gilt das besondere klinische Interesse zum einender weiteren Führung der Schwangerschaft unter Ein-beziehung des Risikos für den überlebenden Feten wieauch der Mutter, zum anderen dem Entbindungsmodusfür den abgestorbenen Feten.Zwischen 1982 und 1987 wurden in unserer Klinik neunZwillingsschwangerschaften aufgenommen, bei denen je-weils ein Zwilling zum Zeitpunkt der Entbindung ab-gestorben war (entsprechend einer Inzidenz von 0,10%in Bezug auf alle Geburten bzw. 5,42% in Bezug aufZwillingsgeburten). Das durchschnittliche mütterlicheAlter betrug 33,1 Jahre. Das durchschnittliche Schwan-gerschaftsalter bei Entbindung lag bei 33,4 Wochen.
Alle toten Zwillingsfeten wurden obduziert sowie sämt-liche Plazenten histologisch untersucht.In zwei Fällen lag das Geburtsgewicht des überlebendenZwillings unter 1000g, in fünf Fällen zwischen 1500gund 2500 g und in zwei Fällen über 2500 g.Drei Neugeborene brauchten nicht auf eine neonatolo-gische Intensivstation verlegt zu werden. Die anderensechs Neugeborenen (unter 35 Schwangerschaftswochen)benötigten unterschiedlich lange eine neonatologischeIntensivüberwachung. Einer der lebendgeborenen Zwil-linge starb. In drei Fällen war die intrauterine Todes-ursache eine Plazentainsuffizienz, bei weiteren drei einfeto-fetales Transfusionssyndrom, in einem Fall Herz-versagen bei feto-fetaler Transfusion ind in zwei Fällenblieb die Todesursache ungeklärt.Bei den intrauterin abgestorbenen Zwillingen wurdenkeine Mißbildungen beobachtet.
J. Perinat. Med. 16 (1988)
474 Wessel et Schmidt-Gollwitzer, Intrauterine death of one twin
Eine Entbindung verlief spontan, während in acht Fällen(89%) eine Sectio caes area notwendig war.Die Geschlechtsverteilung aller Neugeborenen betrugzehn Jungen gegenüber sieben Mädchen, bei den in uteroverstorbenen Feten drei Jungen zu fünf Mädchen undbei den jeweils überlebenden Zwillingen sieben Jungenzu zwei Mädchen. In vier Fällen starb der führendeZwilling intrauterin ab.Zum Aufbau der Plazenta: in fünf Fällen handelte essich um eine monochoriatisch-diamniotische Plazentaund in drei Fällen um eine dichoriatisch-diamniotischePlazenta. Bei vier Fällen ließen sich Verbindungen imSinne von Shunts nachweisen als morphologisch-ana-tomische Voraussetzung für ein feto-fetales Transfu-sionssyndrom.Wie erwartet, waren Gestosesymptome die häufigstenKomplikationen bei den Schwangerschaftsverläufen.Nur in drei Fällen war bekannt, daß der intrauterineTod schon einige Zeit vor der Entbindung erfolgte.Hinsichtlich der mütterlichen Morbidität und des Wo-chenbetts war die Komplikationsrate nach einem intrau-terinen fetalen Tod nicht erhöht.Die Mortalitätsrate liegt bei Zwillingen 3—4fach höherals bei Einlingen. Auch die Morbidität ist erhöht, speziellwegen der häufigeren Frühgeburten. Dabei hat vor allemder zweite Zwilling ein höheres Risiko. Ein intrauterinerTod ereignet sich 3—4mal häufiger als bei Einzelschwan-gerschaften [8].Die in unserer Untersuchungsgruppe gefundene Inzidenzvon 0,10% ist mit der anderer Autoren vergleichbar.Mit 33,1 Jahren war das durchschnittliche mütterlicheAlter geringfügig höher als in anderen Studien.Von den lebendgeborenen Zwillingen starb einer postpartum (11,1%); er hatte mit 25 Schwangerschaftswo-chen das niedrigste Gestationsalter in unserem Kollektiv.Zwischen der Vitalität des überlebenden Neugeborenenund der Dauer zwischen intrauterinem Tod des anderenZwillings und der Entbindung gibt es keinen Zusam-menhang.Auffallend ist die mit 89% sehr hohe Sektiorate. DasVerhalten des Geburtshelfers bei Steißlagen bestimmt inweitem Maße die Inzidenz von Kaiserschnitten. In un-serem Kollektiv war in vier Fällen die Steißlage diealleinige Sektioindikation. Eine größere Bereitschaft zurSektio ist in den Fällen verständlich, wo ein intrauterinesfetales Absterben akut diagnostiziert wird und gleich-zeitig andere Symptome wie starke vaginale Blutungenauftreten. Weder die überlebenden noch die abgestor-benen Zwillinge zeigten irgendeine angeborene Mißbil-dung.Die Inzidenz von monochoriatrischen Plazenten in un-serer Studie ist vergleichbar mit den Zahlen andererAutoren: bei neun Fällen traten sie fünfmal auf, davon
lag in vier Fällen ein feto-fetales Transfusionssyndromvor. Dabei kam es beim Empfanger in drei Fällen zumintrauterinen Absterben, beim Spender in einem Fall.Bei 3 Fällen lag ein chronisches, in einem Fall ein sub-chronisches Transfusionssyndrom vor. In den zwei Fäl-len mit chronischem Transfusionssyndrom, wo der Spen-der überlebte, waren Bluttransfusionen erforderlich (ineinem Fall lag mit 4,4 g% ein initial sehr niedriger Hb-Wert vor).In Übereinstimmung mit den publizierten Erfahrungensind die Form und der Zeitpunkt für die Beendigungvon Schwangerschaften mit einem lebenden Zwilling inerster Linie durch den Reifestatus dieses Kindes be-stimmt. Auch der Plazentamorphologie sollte Rechnunggetragen werden: wenn definitiv eine dizygote Form vor-liegt (sonographischer Nachweis von zwei Plazenten,unterschiedliches Geschlecht), kann man davon ausge-hen, daß das fetale Risiko nicht erhöht ist. Unter Über-wachung fetaler und maternaler Parameter kann einspontanes Einsetzen der Wehentätigkeit abgewartet wer-den. Ist eine monochoriatische Form nicht auszuschlie-ßen, besteht ein erhöhtes Risiko für den überlebendenZwilling durch Shuntverbindungen, über die eine DICmit nachfolgendem Tod oder Organschädigung induziertwerden kann.Wir schlagen folgende allgemeine Richtlinien im Falledes intrauterinen Absterben eines Feten bei Zwillings-schwangerschaften vor:Es gibt kein mit dieser Situation direkt assoziiertes er-höhtes Risiko für die Mutter; die wichtigen Gerinnungs-parameter sollten kontinuierlich überwacht werden, umStörungen im Gerinnungssystem zu erfassen. Das in-trauterine Absterben eines Zwillings ist keine absoluteIndikation zur Beendigung der Schwangerschaft. Jedochsollte eine cardiotokographische und sonographischeÜberwachung erfolgen, um Risikofaktoren zu erkennen,die im Falle einer monochoriatischen Plazenta das Ri-siko für den überlebenden Zwilling in Form einer Shun-tumkehr bei feto-fetalem Transfusionssyndrom beinhal-ten. Cardiotokographie und Sonographie sind die ent-scheidenden Überwachungsmethoden beim überleben-den Zwillingsfeten, und sie bestimmen Form und Zeit-punkt der Entbindung, außer es kommt zu Komplika-tionen wie z. B. Blutungen, die jederzeit auftreten kön-nen. Man sollte immer versuchen, eine Lungenreife zuerzielen, entweder durch Abwarten bis zum adäquatenGestationsalter oder durch Induktion. Eine engmaschigeÜberwachung von Mutter und überlebendem Zwillingist essentiell. Daher sollte eine Einweisung in die Klinikerfolgen. Im Idealfall sollte es möglich sein, die Inzidenzvon Sectiones die der bei unkomplizierten Zwillings-schwangerschaften anzunähern.
Schlüsselwörter: Entbindungsmodus, intrauteriner Tod eines Zwillings, neonatale Morbidität, Plazentation, Zwil-lingschwangerschaft.
J. Perinat. Med. 16 (1988)
Wessel et Schmidt-Gollwitzer, Intrauterine death of one twin 475
Resume
Mort infra-uterine d'un des foetus au cours des grossessesgemellairesLa mort intra-uterine d'un fcetus au cours des grossessesgemellaires est rare en obstetrique. La prise en chargeulterieure de la grossesse en prenant en compte le risquepourle jumeau survivant et pour la mere ainsi que laconduite ä tenir pour Faccouchement sont d'un interetclinique particulier.Pendant la periode 1982-1987, il y a eu dans notrehopital 9 grossesses gemellaires au cours desquelles undes jumeaux etait mort au moment de l'accouchement(incidence de 0,1% de toutes les naissances, mais inci-dence de 5,42% de toutes les naissances gemellaires).L'äge maternel est de 33,1 ans. L'äge gestationnel moyenau moment de Faccouchement est de 33,4 semaines.Une autopsie a ete effectuee sur tous les jumeaux mortset les placentas ont ete examines en histologie.Le poids de naissance du jumeau survivant etait inferieurä 1000 g dans deux cas, compris entre 1500 et 2500gdans 5 cats superieur ä 2500 g dans 2 cas.Trois nouveaux-nes n'ont pas eu besoin d'etre transferesen neonatologie. Les six autres nouveaux-nes (< 35 se-maines de gestation) ont tous necessite un traitement etla periode neonatale a ete differente pour chaque cas.Parmi les jumeaux nes vivants, un est decode.Dans trois cas Finsuffisance placentaire etait la cause dela mort intra-uterine, dans trois autres cas c'etait unsyndrome de transfusion fceto-foetale, dans un cas unedefaillance cardiaque avec transfusion foeto-foetale, maisdans deux cas la cause de la mort n'est pas claire.On n'a pas observe de malformations chez les jumeauxmorts in utero.II n'y a eu qu'un seul accouchement spontane, les 8autres (89%) ont eu lieu par cesarienne.Le sex-ratio de tous les nouveaux-nes est de 10 gargonssur 7 filles, alors qu'il est de 3 gargons sur 5 filles pourles foetus morts in utero, et que le sex ratio des survivantsest de 7 gargons sur 2 filles. Dans 4 cas le deuxiemjumeau est mort in-utero.La nature des membranes est la suivante: dasn 5 cas ils'agissait de placenta monochorioniques-diamniotiqueset, dans 3 cas, de placentas dichorioniques-diamnio-tiques. Dans ce cas, la presence de communicationsvasculaires signifiaient qu'il existait des conditions ana-tomiques pour au'existe un syndrome de transfusionfoeto-foetale.Les symptomes de la gestose ont represente les anomaliesprincipales au cours de la grossesse comme il fallait s'yattendre.Le fait que la mort foetale soit survenue quelque tempsauparavant n'a ete decouvert au moment de Faccouche-ment que dans trois cas.On n'a pas observe de complications secondaires dues äla mort foetale intra-uterine en ce qui concerne la mor-bidite maternelle etle post-partum.Le taux de mortalite des jumeaux est 3 a 4 fois pluseleve que pour les nouveaux-nes uniques et la morbiditeest egalement augmentee tout particulierement en raison
du fort pourcentage d'accouchements prematures. En cesens, le second jumeau est tout particulierement ä risque.Le taux de morts intra-uterines est egalement 2 ä 3 foisplus eleve que pour les grossesses uniques [8).L'incidence de 0,1% dans notre population etudiee ense referant ä l'ensemble des naissances est compatibleavec les autres auteurs.Avec 33,1 ans, Fäge maternel moyen est nettement pluseleve que dans les autres etudes.Les resultats de notre etude montrent que la mort intra-uterine d'un jumeau n'expose pas en soi la mere a unrisque accru.Parmi les jumeaux survivants in utero, Fun est mortapres Faccouchement (11,1%); Fäge gestationnel de cecas etait de 25 semaines, le plus bas de notre etude.II n'y a pas de lesion entre la vitalite d'un nouveau-nesuivant et Fintervalle entre la mort intra-uterine deFautre jumeau et Faccouchement.Avec 89%, le taux eleve de cesarienne comme methoded'accouchement est frappent. L'incidence des cesariennesest grandement fondee sur Fattitude obstetricale faceaux presentations du siege: dans notre population, cettepresentation anormale a ete la seule indication dans cecas. On comprend mieux la plus grande facilite ä prati-quer une cesarienne dans les cas ou le diagnostic de mortfoetale intra-uterine est porte en urgence et lorsqued'autres facteurs de risque tel qu'un saignement vaginalabondant en meme temps. II n'y a pas eu de malfor-mations dans notre etude ni chez les jumeaux decedesni chez les survivants.L'incidence de placentas monochoriaux dans notre etudeest compatible avec ce qui est rapporte par les autresauteurs: 5 de nos 9 cas, 4 parmi eux avaient un syndromede transfusion foeto-foetale. Le receveur est mort in uterodans 3 cas, le donneur dans 1 cas.Les syndromes de transfusion rapportes ici etaient chro-niques dans 3 cas et subchronique 1 fois. Une transfusionsanguine a ete necessaire a la periode neonatale dans lesdeux cas chroniques chez lesquels le donneur a survecu(Fun des deux qui avait un taux initial particulierementbas d'hemoglobine ä 4,4%). En se fondant sur les ex-periences publiees, le mode et le moment de la termi-naison de la grossesse en cas de jumeau survivant sontdetermines avant tout par la maturite foetale. Le type deplacenta devrait egalement etre pris en compte: sexesdifferents), on peut estimer en regie generate qu'il n'y apas de risque foetal accru et que Fon peut attendre ledeclenchement spontane du travail en surveillant le foetuset les parametres maternels.Si Fone ne peut eliminer une grossesse monochoriale, ily a un risque accru pour le jumeau survivant du fait desshunts vasculaires qui peuvent entrainer la mort ou deslesions d'organes.Nous proposons les points generaux suivants commeguides en cas de mort intra-uterine d'un foetus en coursd'une grossesse gemellaire:II n'y a pas pour la mere de risque accru en liaisondirecte, les parametres adequats devraient etre surveilles
J. Perinat. Med. 16 (1988)
476 Wessel et Schmidt-Gollwitzer, Intrauterine death of one twin
regulierement pour depister toute perturbation de lacoagulation. La mort intra-uterine d'un jumeau n'estpas une indication absolue d'interruption de la grossessedu survivant. Neanmoins, il faut effectuer une surveil-lance CTC et echographique aim de depister les facteursde risque qui en cas de placenta monochorial pourraitapparaitre chez le survivant dans le cadre d'un syndromede transfusion foeto-foetale. II s'agit du seul mode desurveillance du bien etre du jumeau survivant et c'estjustement Petat du jumeau en dehors de complications
(hemorragies) qui peuvent survenir n'importe quand, quidetermine le moment et le mode d'accouchement.II faudrait toujours essayer d'obtenir la maturite pul-monaire fcetale en atteignant un age gestationnel appro-prie ou par induction. Une appreciation etroite de l'etatmaternel et de 1'enfant survivant est necessaire et la meredoit etre hospitalisee pour celä. Dans Fideal, il devraitetre possible de reduire l'incidence des cesariennes jus-qu'au taux des grossesses gemellaires non compliquees.
Mots-cles: Grossesse gemellaire, mort intra-uterine d'un jumeau, mode d'accouchement, placentation, morbiditeneonatale.
Acknowledgements: We are grateful to Prof. Dr. M. VOGEL (Department for Paidopathology and Placentology atthe Klinikum Charlottenburg) for the autopsy and placental findings.
References
[1] D'ALTON ME, ER NEWTON, CL CETRULO: Intra-uterine fetal demise in multiple gestation. Acta Ge-net Med Gemellol 33 (1984) 4349
[2] HAGAY ZJ, M MAZOR, JR LEIBERMANN: Multiplepregnancy complicated by a single intrauterine fetaldeath. Obstet Gynecol 66 (1985) 837-838 (Letter)
[3] HAGAY ZJ, M MAZOR, JR LEIBERMANN: Manage-ment and Outcome of Multiple Pregnancies Com-plicated by the Antenatal Death of One Fetus. JReprod Med 31 (1986) 717-720
[4] KINDRED JE: Twin pregnancies with one twinblighted: Reports of two cases with comparativestudy of cases in the literature. Am J Obstet Gy-necol 48 (1944) 642-682
[5] KLOOS K, M VOGEL: Pathologie der Perinatalper-iode. Georg Thieme Verlag Stuttgart 1974
[6] LITSCHGI M, D STUCKI: Verlauf von Zwillings-schwangerschaften nach intrauterinem Fruchttodeines Föten. Z Geburtsh u Perinat 184 (1980) 227-230
[7] LIVNAT EJ, L BURD, A CADKIN, P KEH, AB WARD:Fetus Papyraceus in Twin Pregnancy. Obstet Gy-necol 51 Suppl (1978) 415-455
[8] LUMME R, S SAARIKOVSKI: Antepartal fetal death ofone twin. Int J Gynecol Obstet 25 (1987) 331-336
[9] OTTOLENGHI-PETRI GF: Sopra un rarissiomo casodi gravidanza gemellare con un feto papiraceo econ inserzione velamentosa del funicolo del fetovivo. Ann Ost Gin Med Perm XCIII (1972) 173-199
[10] PRITCHARD JA: Fetal death in utero. Obstet Gyne-col 14(1959)573-580
[11] RIEHN A: Über das Risiko nach intrauterinemFruchttod eines Feten bei Zwillingsschwanger-schaft. Zbl Gynäkol 104 (1982) 1530-1536
[12] ROMERO R, T DUFFY, RL BERKOWITZ, E CHANG,JC HOBBINS: Prolongation of a preterm pregnancycomplicated by death of a single twin and dissem-inated intravascular coagulation. N Engl J Med 310(1984)772-774
[13] SKELLY H, M MARTIVATE, R NORMAN, G KENOYER,R MARTIN: Consumptive coagulopathy followingfetal death in a triplet pregnancy. Am J ObstetGynecol 142 (1982) 595-596
Received May 5, 1988. Accepted September 10,1988.Dr. Jens WesselUniversitätsfrauenklinik CharlottenburgPulsstr. 4-14D-1000 Berlin 19, West Germany
J. Perinat. Med. 16 (1988)






![Early intrauterine development of mixed giant … · Early intrauterine development of mixed giant ... but with intrauterine death at 29 weeks [5]. Fetal . Early intrauterine development](https://img.pdfslide.net/doc/110x75/5b63022f7f8b9ade588b8aac/early-intrauterine-development-of-mixed-giant-early-intrauterine-development.jpg)






![Research Article …downloads.hindawi.com/journals/jir/2012/928187.pdf · 2019-07-31 · intrauterine life [3, 4]. This passive immunity acquired by the fetus is crucial for the adaptation](https://img.pdfslide.net/doc/110x75/5e865aaf8ebd3a32064e5483/research-article-2019-07-31-intrauterine-life-3-4-this-passive-immunity-acquired.jpg)