-
7/30/2019 Lecture 19 - Respiration 2 - Mechanics of
Breathing
1/35
Dr. Christina [email protected]
PHY2021Mechanics of Breathing
http://www.google.com.sg/url?sa=i&rct=j&q=old+pictures+paintings+of+respiratory+system&source=images&cd=&cad=rja&docid=8XdAzm7byEcWJM&tbnid=7FuR29Z95rBMTM:&ved=0CAUQjRw&url=http%3A%2F%2Flapetitemort73.blogspot.com%2F2009_03_01_archive.html&ei=Fq42UYStPIGpkwXcp4GwCg&bvm=bv.43287494,d.bmk&psig=AFQjCNH7vAOSQaj7lI6QNH5dLynGrw1ygA&ust=1362623969056948
-
7/30/2019 Lecture 19 - Respiration 2 - Mechanics of
Breathing
2/35
Volume, pressure and airflow changes during respiratory
cycle
Mechanical relationship between lung and chest wall:
Generation of pressure gradient between atmosphere and
alveoli
Muscles of respiration
Airway resistance; Stability of alveoli; Pulmonary
Surfactant
Role of lung compliance during breathing
Essential Reading: Vanders (11th ed) Chapter 13, p 44356
Key Learning Outcomes
After this lecture and with further reading you will be able to
describe:
Lung Volumes and Capacities
A brief review of major respiratory disorders that change
themechanics of the respiratory system
-
7/30/2019 Lecture 19 - Respiration 2 - Mechanics of
Breathing
3/35
1. Ventilation: Exchange of air between
atmosphere & alveoli by bulk flow
2. Exchange of O2 & CO2 between alveolar
air & blood in lung capillaries by diffusion
5. Cellular utilization of O2 & production
of CO2
3. Transport of O2 &CO2 through pulmonary
& systemic circulation by bulk flow
4. Exchange of O2 & CO2 between blood
in tissue capillaries & cells in tissues
by diffusion
Steps in Ventilation
-
7/30/2019 Lecture 19 - Respiration 2 - Mechanics of
Breathing
4/35
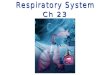
The respiratory system
Chest is a closed container.
Closed at top by muscle&
connective tissue.
Closed at sides by ribs & muscle
Sealed at bottom by diaphragm
-
7/30/2019 Lecture 19 - Respiration 2 - Mechanics of
Breathing
5/35
Boyles law: P1V1=P2V2
Volumes and pressures are related!
The pressure of a gas is inversely related to the volume of its
container.
A decrease in thoracic volume leads to an increase in
pressure.
As the chest is a closed container, an increase in thoracic
volume will
lead to a decrease in pressure.
-
7/30/2019 Lecture 19 - Respiration 2 - Mechanics of
Breathing
6/35
Quiet Inspiration
The diaphragm and external intercostal muscles contract
External intercostal muscles elevate the rib cage the
sternum
moves anteriorly
Diaphragm flattens and moves inferiorly
Volume and Pressure (within the thoracic cavity and the
lungs)
-
7/30/2019 Lecture 19 - Respiration 2 - Mechanics of
Breathing
7/35
Lung expansion relies on intrapleural pressure.
How does increasing and decreasing thoracic
volume alter lung volume?
Intrapleural space
Visceral pleura
Parietal pleura
Small changes in this pressure work to couple
changes in thoracic volume with changes in
lung volume!
The lungs are only attached at the hilus!
Lung expansion following increased thoracic
volumes is dependent on intrapleural pressure.
Consequently, due to elastic recoil of the lung
during expiration, lungs collapse away from the
chest wall this draws chest wall in!
At rest, the lungs want to collapse, but chestwall wants to
expand. This creates a sub-
atmospheric intrapleural pressure.
-
7/30/2019 Lecture 19 - Respiration 2 - Mechanics of
Breathing
8/35
Pressure differences involved in ventilation
Palv
Intrapleural FluidLung wall
Chest wall
Pip
Atmosphere
Patm
Palv < PatmPalv > Patm
Ptp = Palv - Pip
Pcw = Pip -Patm
Patm
Prs= Palv- Patm
Opposes inward elastic recoil of the lung
Opposes out ward elastic recoil of chest wall
Determines air flow
-
7/30/2019 Lecture 19 - Respiration 2 - Mechanics of
Breathing
9/35
Inspiration as chest wall expands, Pip
(Boyles law)
Palv
Intrapleural Fluid
Lung wall
Chest wall
Pip
Ptp Pip Lung expands
Palv Air flows inward
Ptp = Palv - Pip
Air flows inward
Greater than inward elastic recoil force
-
7/30/2019 Lecture 19 - Respiration 2 - Mechanics of
Breathing
10/35
Expiration Decrease firing of phrenic nerve and
intercostal nerve respiratory muscles
relax Chest recoils back to originalposition smaller thoracic
volume
Palv
Intrapleural Fluid
Lung wall
Chest wall
Pip
Ptp Pip Lung recoils
Palv Air flows out
Ptp = Palv - Pip
Air flows outward
Lower than inward elastic recoil force
-
7/30/2019 Lecture 19 - Respiration 2 - Mechanics of
Breathing
11/35
Quiet Expiration
Expiration is due to passive recoil
During quiet breathing, expiration is passive process
(no muscle contraction)
-
7/30/2019 Lecture 19 - Respiration 2 - Mechanics of
Breathing
12/35
Stable Balance Between Breaths
Intrapleural space
Alveolus
Chest wall
Elastic recoil of lung Elastic recoil of chest wall
Patm= 0mmHg
Palv = 0mmHg
Ptp = Palv - Pip= 4mmHg
Pcw = Pip - Patm= - 4 mmHg
Pip= - 4mmHg
Prs= Palv - Patm = 0 mmHg
No
Flow
-
7/30/2019 Lecture 19 - Respiration 2 - Mechanics of
Breathing
13/35
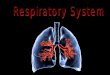
Respiratory Cycle & Pressure Changes
Inspiration Expiration
2
- 2
- 4
- 6
0
0
0.5
4 secTime
Pressuresduringbreathing(m
mHg)
Breathvolume(L)
End of Expiration
Mid Inspiration
End Inspiration
Mid Expiration
1
2
3
4
Patm = 0
Palv = 0
Nofl
ow
Ptp = 4Pip = - 4
Palv
Pip
Ptp
Airflow
Patm = 0
Palv = -1
Palv - Patm = -1
Ptp = Patm Pip = 7
Recoil
Pip
= - 6
Pip
= - 7
Recoil
Patm = 0Noflow
Palv = 0
Palv - Patm = 0
Ptp = Patm Pip = 5
Pip = - 5
Recoil
Ptp = Patm Pip = 6
Airflow
Patm = 0
Palv = 1
Palv - Patm = 1
-
7/30/2019 Lecture 19 - Respiration 2 - Mechanics of
Breathing
14/35
Deep Breathing
Inspiration involvescontraction of extramuscles to elevateribs:
scalenes,pectoralis minor, &
sternocleidomastoidmuscles
Expiration involvescontraction ofinternal intercostals&
abdominal muscles
-
7/30/2019 Lecture 19 - Respiration 2 - Mechanics of
Breathing
15/35
Physical Aspects of Ventilation
Ventilation results from pressure differences induced
by changes in lung volumes
Air moves from higher to lower pressure
Compliance, elasticity, & surface tension
of lungs influence ease of ventilation
-
7/30/2019 Lecture 19 - Respiration 2 - Mechanics of
Breathing
16/35
Compliance
Magnitude of change in lung volumeproduced by a given change in
Ptp
How easily lung expands with pressure
Major determinants: - Elasticity
- Surface tension
Is reduced by factors that cause resistanceto stretching
-
7/30/2019 Lecture 19 - Respiration 2 - Mechanics of
Breathing
17/35
Elasticity Tendency to return to initial size after
distension
Due to high content of elastin proteins
Elastic tension increases during inspiration &is reduced by
recoil during expiration
Elastic Recoil
- return to the original dimension driven by the
elastic tension generated during stretching.
-
7/30/2019 Lecture 19 - Respiration 2 - Mechanics of
Breathing
18/35
Surface tension (& elasticity) are forces that promote
alveolar
collapse & resist stretching
Surface tension of H2O tends to collapse alveoli (attractive
forcesbetween liquid molecules is greater than forces between
liquid and
gas molecules)
Smaller alveoli tend to collapse more than larger ones
Law of Laplace relationship between pressure (P), surface
tension
(T), and the radius (r) of an alveolus : P = 2T/r
Surface tension
Pressure needed to
keep a sphere shape=
2x Surface tension
radius
-
7/30/2019 Lecture 19 - Respiration 2 - Mechanics of
Breathing
19/35
Pulmonary surfactant
Produced by alveoli type II cells
Function:
- reduce surface tension during expiration
- consequently increasing the lung compliance
(decreasing the work of breathing).
- Prevents alveoli from collapse
- Preventing fluid accumulation in the alveoli
- host defense mechanism against infection
and inflammation
Surfactant
H2O molecules
Alveolar wall
-
7/30/2019 Lecture 19 - Respiration 2 - Mechanics of
Breathing
20/35
Surface tension & surfactant
Surfactant reduces surface tension
Surfactant production starts in late gestation
Secreted by type II alveolar cells
Surfactant (a mixture of phospholipids & proteins)
Diplamitoyl phosphatidyl choline (DPPC) Hydrophobic tail,
hydrophillic head
R l f f t t i h t i
-
7/30/2019 Lecture 19 - Respiration 2 - Mechanics of
Breathing
21/35
Role of surfactant in hysteresis
Hysteresis
Surface tension forces
overcome by surface film
pressure (prevent collapse)
Surface tension forces
overcome by surface film
pressure
(prevent collapse)
Alveolus expands.
Not enough surfactant
molecules to totally resist
surface tension forces.- Difficult to expand
More surfactant molecules
produced.
Alveolus expands easily
Alveolus starting to decrease in
size but surfactant moleculesprevent this.
Surfactant molecules pushed
out of film allowing alveolusto decrease easily
surfactant
water
alveolus
-
7/30/2019 Lecture 19 - Respiration 2 - Mechanics of
Breathing
22/35
Resistance =
Airway resistance - effect of radius on airflow
radius 4
constant x lengthOhms and Poiseuilles Laws combined:
Halve airway radius = 16 xs increase in resistance (e.g.
asthma)
Double the length = doubles the resistance
Factors affecting airway radii (resistance):
- physical - Trans pulmonary pressure (Ptp)- elastic connective
fibers
- Intrapleural pressure (Pip)
- neuro-endocrine influence the airway smooth muscle-
epinephrine - relaxes smooth muscles
- leukotrines - contract smooth muscles
-
7/30/2019 Lecture 19 - Respiration 2 - Mechanics of
Breathing
23/35
Airway resistance (RAW)
Raw > in medium-sized
bronchi, not small bronchioles
Example cross-sectional areas
Trachea = 2.5cm
2
Terminal bronchioles = 240cm2
The medium-sized bronchi (over
2mm) around the 7th generation
have the highest resistance
This is because the small airways
are so numerous and, existing in
parallel, have a large total cross-
sectional area
Importantly, the low resistance of the small airways makes them
a
silent zone on auscultation
Early obstructive (emphysema) disease affects these vessels
first,
but is hard to detect.
-
7/30/2019 Lecture 19 - Respiration 2 - Mechanics of
Breathing
24/35
Measuring lung function
-
7/30/2019 Lecture 19 - Respiration 2 - Mechanics of
Breathing
25/35
Measurement of Lung volumes and capacities
Spirometer - for measuring lung volumes & capacities
- also inspiratory and expiratory flow rates
Spirogram
-
7/30/2019 Lecture 19 - Respiration 2 - Mechanics of
Breathing
26/35
Spirogram
Measure changes in lung volumeduring breathing.
Can also be used to measure flow rates (L/sec) - inspiratory or
expiratory.
Cannot measure the absolute gas volumein the lungs
- need Helium dilution or plethysmography.
Lung volumes - related to gender, height, weight, age.
- also affected by lung diseases.
Tid l V l ( i t b thi )
-
7/30/2019 Lecture 19 - Respiration 2 - Mechanics of
Breathing
27/35
Tidal Volume (quiet breathing)
Each breath is ~500 ml
- Most of this reaches the alveoli
In each breath, ~350 ml reaches
the alveoli and ~150 ml stays in
the airways (ie. dead space).Anatomical dead space is the
air
in conducting airways (~150 ml).
At end of normal expiration, there
~2.5 L in the Lungs:
ie. they are never empty.
(values are for typical young adult male)
-
7/30/2019 Lecture 19 - Respiration 2 - Mechanics of
Breathing
28/35
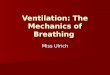
Tidal volume
500ml
LUNG VOLUMES
Inspiratory
reserve
volume
Expiratory reservevolume
Residua
l
Volume
(1.2L)
Dead space
(airways)
Lung volumes and capacities
-
7/30/2019 Lecture 19 - Respiration 2 - Mechanics of
Breathing
29/35
Lung volumes and capacities
Expiratory Reserve Volume (ERV)
Amount of expired air during forced expiration after quiet
breathingResidual Volume (RV)
Amount of air remain in lungs after maximal expiration
Tidal Volume (TV)
Amount of air that goes in/out of lungs for each
inspiration/expiration
Inspiratory Reserve Volume (IRV)
Amount of inspired air more than TV during maximal
inspiration
Vital Capacity (VC)
Total amount of air that is maximally expired after maximum
inspiration
= IRV + TV + ERV
Lung Volumes & Capacitiescontinue
-
7/30/2019 Lecture 19 - Respiration 2 - Mechanics of
Breathing
30/35
Lung Volumes & Capacities
Inspiratory Capacity (IC)
Total amount of air that is maximally inspired after normal
expiration
IC = IRV + TVFunctional Residual Capacity (FRC)
Total amount of residual air in the lungs after normal
expiration
FRC = ERV + RV
Total Lung Capacity (TLC)
Total amount of air in the lungs after maximal inspiration
TLC = IRV + TV + ERV + RV
RV & FRC
cannot be measured byspirometer
RV & FRC is measurable
by N2 wash-out technique
-
7/30/2019 Lecture 19 - Respiration 2 - Mechanics of
Breathing
31/35
Pulmonary Ventilation
Minute ventilation Volume of air breathed per minute
(litres/min)
MV = Tidal Volume (mL/breath) x Respiratory rate (breaths
/min)
eg: 12 breaths/min x 500 ml = 6 litres/min
Alveolar minute ventilation = breath/min x (TV DeadSpace
Volume)
Maximum voluntary ventilation
= maximum minute ventilation
(i.e maximum breathing effort)
Depends on muscular effort and airway resistance
Ob t ti l di
-
7/30/2019 Lecture 19 - Respiration 2 - Mechanics of
Breathing
32/35
Obstructive lung disease1- Asthma.Chronic inflammation of
airways and hypersensitivity to allergens.
Increased tone of airway smooth muscle and excessive mucus
secretion.
2- Chronic bronchitis.Increase in mucus secretion and
inflammation of airway walls.
3- Emphysema.Destruction of alveolar walls reduce the
radial traction of airways and therefore
the airway resistance is abnormally high.
Obstructive lung diseases - airway resistance is abnormally
increased.
N E
Lung volumes and work of breathing
-
7/30/2019 Lecture 19 - Respiration 2 - Mechanics of
Breathing
33/35
Lung volumes and work of breathing
Diseases/conditions
affecting themRESTRICTIVE
Pulmonary fibrosis, chest
burns, diaphragm in obesity
and pregnancy, muscleweakness
OBSTRUCTIVE
Asthma, COPD,
Bronchiectasis, bronchitis,
tumours
Work aspects of breathing
Work to expand the chest
FEV1 is severely decreased:
FEV1/FVC = < 80%
FEV1 and FVC are decreased. But:
FEV1/FVC = about 80% (normal)Airway resistance
- Work to move air into the lungs
S i t Fl l
-
7/30/2019 Lecture 19 - Respiration 2 - Mechanics of
Breathing
34/35
Spirometry: Flow-volume curves
Respiratory Physiology. John West. Chapter 10; page 160
-
7/30/2019 Lecture 19 - Respiration 2 - Mechanics of
Breathing
35/35
Reading...
Recommended reading
Vanders (chapter 13) p443-56
Silverton (chapter 17) p 568-574, p 578-589
Other very very useful information...!
Ward JPT Respiratory System at a Glance (chapters 1-3, 20)
Marieb & Hoehn Human Anatomy & Physiology7th Ed
(chapter 22)