Embed Size (px)
Citation preview

Management of Extremity Fractures
Bucky Boaz, ARNP-C

Upper Extremity Fractures
• Commonly encountered in Family Practice
• Ranked 14th out of top 20 diagnoses
• 6% to 15% of orthopedic problems encountered in Family Practice
• Most common injuries are fractures of fingers, radius, metacarpals, toes, and fibula
• Many can be managed by Family Practice

Metacarpal Fractures
• Second most common fracture in primary care
• Classified according to location:– Head
– Neck
– Shaft
– Base

Metacarpal Fractures
• Most fractures of MC head are comminuted and need ortho referral
• Acute mgt:– Immobilize in ulnar or
radial gutter splint– Ice– Elevation– Analgesia
• Ortho evaluation within 1 week of injury

Metacarpal Fractures
• Fractures of MC neck result from direct impact (punching)
• Boxer’s Fracture• Head of MC is displaced
volarly• Tenderness and swelling
over dorsum of hand• Possible pseudocrawling
– Hyperextension at MCP and flexion at PIP
– Dorsal angulation > 40º

Metacarpal Fractures
• Radiographs AP, lat and oblique views
• Degree of angulation on lateral view– Expected 15º
– Subtract from visualized angulation
– More distal greater allowed
– Deformity better tolerated in 4th or 5th digits

Metacarpal Fractures
• Management– Splint:
• MCP 70º to 90º of flexion
• Use radial or ulnar gutter
– Reduction:• Pseudocrawling• 4th MC > 30º• 5th MC > 40º• May not improve
outcome
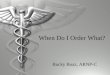
Ulnar Gutter Splint

Metacarpal Fractures
• Reduction– Hematoma or ulnar
nerve block
– 90-90 method:• MCP, PIP, DIP joints
flexed 90º
• Volar-directed pressure over fracture site
• Immob with wrist extension 30º and MCP flexed to 90º

Metacarpal Fractures
• Nondisplaced fractures of 2nd and 3rd MCs follow up x-ray within 4-5 days
• Fractures to 4th or 5th MCs follow up x-ray 7-10 days
• Any change, ortho referral
• No contact sports for 4-6 weeks after immobilization
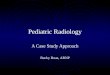
Fracture 4th metacarpal

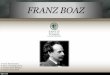
Wrist Anatomy
A. Metacarpals and phalangesB. TrapeziumC. CarplesD. Scaphoid (navicular)E. Distal radiusF. LunateG. TriquetriumH. PisiformI. CapitateJ. HamateK. Trapezoid

Wrist Anatomy
A. Radial styloid
B. Extensor pollicis brevis
C. Anatomic snuffbox
D. Extensor pollicis longus
E. Lister’s tubercle
F. Dorsal wrist depression
G. Ulnar styloid
Dorsal Anatomic Landmarks

Wrist Anatomy
A. Radial styloid
B. Scaphoid tubercle
C. Carpal tunnel
D. Hamulus
E. Pisiform
Volar anatomic landmarks

Scaphoid Fracture
• Most commonly fractured carpal bone– 70% - 80% of all carpal
bone injuries
– 8% of all sports-related fractures
• Spans both carpal rows
• Susceptible to injury when stress applied to dorsiflexed wrist

Scaphoid Fracture
• Patients will complain of wrist pain– Particularly over
anatomic snuff box
• Swelling• Motion is commonly
limited

Scaphoid Fracture
• Radiographs need to include scaphoid view– Elongates the scaphoid
along its long axis
– At least 10%-20% false negative on x-ray

Scaphoid Fracture
• Anatomical Importance:– Blood supply from a
branch of radial artery enters the distal pole
– Retrograde blood flow– Fractures at risk of
nonunion or AVN• Proximal• Oblique• displaced

Scaphoid Fracture
• Examination– Anatomic snuff box
swelling or pain on palpation
– Pronation and ulnar deviation exacerbates pain
– Axial loading exacerbates pain
– Pronation/supination against resistance exacerbates pain (supination more specific)

Scaphoid Fracture
• Management– Immobilize even if x-
rays negative if warranted
– Immobilization with thumb spica
– Ortho referral

Colles’ Fracture
• Most common fracture of the distal radius
• Results from a fall on an outstretched hand (FOOSH)
• Dorsal swelling
• Eccymosis
• “Silver fork” deformity of the hand and wrist

Colles’ Fracture
• Radiographs– (AP, lat, & oblique)– Apex volar fracture
with dorsal comminution and shortening of the radius
• Typically occurs within 2cm of distal radius articular surface

Colles’ Fracture
• Definitive care may be provided by primary care provider– Reduction of fracture
– Splinting
• Ortho referral• Inter-articular fracture
needs ortho follow up

Smith’s Fracture
• Less common fracture of distal radius
• Unstable fracture
• Distal fragment is displaced volarly and proximally (apex dorsal)
• Direct blow to dorsum of the wrist
• Splint and immediate ortho referral

Galeazzi’s Fracture
• Radial shaft fracture at junction of middle and distal thirds with disruption of distal radioulnar joint
• Fall on extended pronated wrist
• Suspect if tenderness at distal radius and distal radial ulnar joint (DRUJ) disruption

Galeazzi’s Fracture
• Radiographic:– Transverse or oblique
fracture at junction of middle and distal thirds seen on AP view
– Widening of DRUJ on AP view
– Fracture of base of the ulnar styloid
– Radial shortening > 5mm
– Dislocation of radius relative to ulna on lat view

Monteggia’s Fracture
• Fracture of ulnar shaft with dislocation of radial head
• Fall on outstretched, extended, and pronated elbow is usual mechanism
• Radial head may be palpated in antecubital fossa
• Radial nerve neuropraxia

Monteggia’s Fracture
• Radiographic:– Ulnar fracture
– Dislocation of radial head
– High index of suspension required

Radial Head Fracture
• Result from FOOSH or valgus compressive force
• May occur in elbow dislocation
• Swelling lat aspect• Limited ROM• Maximal tenderness
over radial head

Radial Head Fracture
• Radiographic:– AP and lat– Fat pad may be only
clue• (occurs as a result of
distension of the capsule by an intra-articular hemarthrosis)
– Large sail shape abnormal
– Posterior abnormal

Radial Head Fracture
• Treatment non-displaced fracture:
• Immob in long-arm posterior splint with elbow flexed 90º.
• Ice and elevation for 48 hours
• Analgesia• Forearm rotation out of
splint 3-5 days• 1 week – sling for
comfort only• Active ROM

Radial Head Fracture• Most common complication
– 10º to 15º limit to ROM– Does not limit function
• Immediate ortho referral criteria:– fracture dislocation– brachial artery or nerve injury– 2mm displacement– 1/3 of articulating surface– Angulated > 30º– Depressed > 3mm– Severely comminuted

Distal Humeral Fracture
• Described as:– Supracondylar
– Transcondylar
– Intercondylar
• Hyperextension of elbow during FOOSH
• AP and lat views sufficient

Distal Humeral Fracture
• Helpful landmark on lat view is extension of anterior humeral line through the capitellum– Line should transect
middle of capitellum– Supracondylar fracture
• Transects anterior third• Falls completely
anterior

Distal Humeral Fracture
• Most important aspect:– Assess neurovascular – All three major nerves of arm or brachial artery
may be injured– Immediate referral for any compromise
• Long-arm posterior splint arm flexed 90º

Clavicle Fracture
• Approx 5% of all primary care fractures
• Typical mechanism of injury– FOOSH– Fall onto shoulder– Direct clavicle trauma
• Patient complains of pain with any shoulder movement and holds arm against chest

Clavicle Fracture
• Physical exam– Edema
– Point tenderness over fracture site
– May have crepitus
– Possible fragment motion
– Possible eccymosis
– Possible tenting of skin
– Careful, passive range of motion should be tolerated
– Motor strength should be intact

Clavicle Fracture
• Radiographic:– AP and 45º cephalic tilt
views
– Medial portion often displaced upwards
• Treatment:– Reduction of motion
– Less than 45º abduction
– Sling or figure eight
– Continue until no crepitus or pain over site. (4-8w)

Clavicle Fracture
• Avoid contact sports or risk of falls for 6 additional weeks
• Ortho referral:– Neurovascular compromise
– Open fracture
– Integrity of skin in jeopardy
– Uncontrolled deformity
– Cosmesis
– Nonunion after 12 weeks

Lower Extremity Fractures
• Examination for:– presence of gross deformity– Loss of pulses– Impaired neurologic function distal to injury
• Ankle injuries account for 10% of all ER x-rays

Fractures of Tibial Shaft
• Most commonly fractured long bone
• Associated with complications
• Time to union:– 20 wks rods
– 14.7 wks cast
– 13 wks ORIF (higher rate of complications)

Fractures of Tibial Shaft
• Radiologic:– Cross-table lat and AP
– Immobilize prior to x-rays if obvious fracture
• Analgesia• Assessment of knee
and ankle

Fractures of Tibial Shaft
• Immobilization– Long or medium posterior splint with
application of stirrups
• Elevation and ice
• Immediate ortho referral

Proximal and Midshaft Fibular Fractures
• Fibula not significantly involved in weight bearing
• Prox fib attachment site for lateral collateral ligament and biceps femoris
• Examine to rule out Maisonneuve fracture

Proximal and Midshaft Fibular Fractures
• Proximal fibular fractures indicate knee instability until proven otherwise
• May be associated with peroneal nerve injury
• Test dorsiflexion and sensation of 1st web space

Proximal and Midshaft Fibular Fractures
• Radiographic:– Lateral and AP views
– Look for tibial plateau fracture
• Treatment– In sensory or motor
disfunction, post splint and ortho follow-up

Proximal and Midshaft Fibular Fractures
• Treatment:– Small avulsion and
nondisplaced fractures of fib neck, knee immob and crutches
– Hinged knee brace when comfortable
– 4-6 wks protection from lateral motion

Ankle Fractures
• Most common lower-extremity fracture
• 15% of patients examined for ankle injury will have a fracture
• Successful management requires determination of stable vs unstable

Ankle Fractures
• The bones and ligaments of the ankle form a ring around the ankle mortis
• For instability to occur, ligamentous injury or fracture must include both medial and lateral sides of the ring
• Isolated distal fib or tib fractures are stable if no ligamentous instability on opposite side of ring

Ankle Fractures
Original Ottawa Ankle Rules Refined Ankle/Foot Rules
Age>55 No age limits
Unable to bear weight (4 steps) both immediately and in ER
Inability to bear weight (4 steps) both immediately and in ER
Bone tenderness (at the posterior edge or top of either malleolus)
Bone tenderness (at the posterior edge or top of either malleolus)
Bone tenderness of the navicular, the cuboid, base of the fifth metatarsal
Bone tenderness of the navicular or the base of the fifth metatarsal
Pain in the midfoot Pain in the midfoot
Evolution of the Ottawa Ankle Rules

Ankle Fractures
• Three bones make up the ankle joint:1. Distal tibia2. Distal fibula3. Talus
• Relationship of the tibial plafond (joint surface) to the talus in important for ankle stability
• Determining ankle position during injury can assist in assessment

Ankle Fractures
• Medial complex injuries occur from eversion force
• Lateral complex injuries occur from inversion force– Most common ankle injury
• Posterior malleolus injury is found with a combination of forces

Ankle Fractures
• Radiographic:– AP, lat, and mortise
views
– Mortise view consists of:A. Medial clear space
B. Tibular/fibular clear space
C. Tibular/fibular overlap
D. Lateral clear space

Ankle Fractures
• 5 most commonly missed foot and ankle fractures: (FLOAT)– Fifth metatarsal base
– Lateral process of talus
– Os trigone (post mall)
– Anterior process of calcaneous
– Talar dome

Ankle Fractures
• Danis-Weber Classification of Fibular Fractures – Type A are horizontal
avulsion fractures found below the mortise
– Type B starts at the level of the mortise (stable or unstable depending on ligaments)
– Type C fracture is above the level of the mortise and disrupts the ligaments between the fibula and tibia

Ankle Fractures
• Treatment:– Analgesia– Immobilization– Primary care can treat Danis-
Weber A
• Ortho referral– Displacement > 2mm– Danis-Weber B and C– Trimalleolar (involving both
medial and lateral malleoli and posterior lip of tibial plafond)
– Mortise view >5mm medial clear space

Fractures of the Fifth Metatarsal
• Most common fracture to base of Fifth metatarsal is results from inversion ankle injury
• The peroneus brevis tendon insertion causes an avulsion of the proximal portion
• Physical exam should include palpation over the base of the fifth metatarsal for all ankle injuries

Fractures of the Fifth Metatarsal
• Types of fifth metatarsal fractures:– Avulsion fracture
– Jones fracture (Metaphyseal- diaphyseal junction)
– Apophysis

Fractures of the Fifth Metatarsal
• Nondisplaced tuberosity fractures:– Wooden postop shoe– Weight bearing as tolerated
for 2-4 weeks– Displaced >3mm ortho
referral
• Jones fracture– Posterior splint– Ortho referral
• All displaced Jones fractures and intraarticular tuberosity fractures should be referred

Questions?