Embed Size (px)
Citation preview

Management of Upper Extremity Arterial and
Venous Occlusive DiseasesCLAUDIE SHEAHAN MD
PROFESSOR OF CLINICAL SURGERYLSU SCHOOL OF MEDICINE

Upper extremity arterial disease
• Rare – less than 5% of PVD• Dutch study –
– Prevalence 2.3% diabetics – 0% non-diabetics

Clinical Presentation
• Episodic - Spastic• Claudication• Tissue loss

History and Physical
• Symptoms c/w connective tissue disorders– Arthralgias– Dysphagia– Sclerodactyly– Xeropthalmia– Xerostomia




History and Physical
Also look for signs of• Malignancy• Hypothyroidism• Frostbite• Trauma• Vibrating tools• Drug use

Examination
• Color change• Digital pitting• Digital ulcer • Gangrene

Exam
• Palpation of pulses• Auscultation for bruits• Adsons maneuvers-should be
done sitting• Allens test

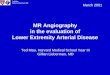
Allen’s test
Collateral flow across the palmar arch

Cold provocation testing
Low specificity and reproducibility

Cardiac echo
Look for embolization
potential

X-Rays
• Cervical rib• Soft tissue atrophy• Distal phalangeal tuft
reabsorption

Biopsy
• Skin for vasculitis• SSc atrophy of epidermis and adnexal fat• Arteritis- wall necrosis

Vascular lab• Multiple level segmental
pressures • Multiple level pulse volume
plethysmography (PVR)• Digital pressures /PPG• ABI• DBI (digital brachial index) ≥0.75

Vascular lab
• Demonstrate symmetry – Between arms– Lower extremities
• Gradient 30-50 mmHg with subclavian artery occlusion
• Digital plethysmography for differentiating vasospasm vs occlusive lesion

Angiography
• Aortic arch: atherosclerosis, ulceration, aneurysms
• TOS maneuvers • Retrograde flow in vertebral
“Subclavian Steal”• Vasodilators, hand warming,
magnified view

Angiography in collagen vascular diseases
• Absence of calcium• Total occlusion vs string • Multiple segmental lesions • Less developed collaterals

Upper extremity arterial disease
Occlusive vs. Spastic

Raynaud's Syndrome
•Vasospastic•Primary•Raynaud’s Disease
•Idiopathic
•Obstructive•Secondary•Raynaud’s Phenomena

Primary Raynaud’s
• Exaggerated response to cold, emotional stimuli
• 3 stages: White, Blue, Red• 15-20min episodes• Pain usually absent • Thermal threshold varies 17-26°C

Primary Raynaud’s
• Most common• Benign• Does not lead to severe ischemia

Secondary Raynaud’s
• More likely to progress to severe occlusive lesions within the digital arteries
• Rest pain and ulceration• Associated with Systemic Sclerosis SLE, RA, mixed collagen disease

Epidemiology
• Mostly women• Median age onset 14• Prevalence varies with climate• Study from Portland 30%
incidence• Higher risk in first degree
relative

Pathophysiology
“Local asphyxia of the extremities" was a result of "increased irritability of the central parts of the cord presiding over the vascular innervation"
-Maurice Raynaud 1862

Pathophysiology
“Local fault”
-Sir Thomas Lewis 1930

Bloodwork
• CBC• ESR/CRP• ANA• Biochemical profile• Thyroid function• RF• CXR/thoracic outlet

Nailfold Capilloroscopy
• Early manifestation of scleroderma
• Dilated capillaries, areas of avascularity

Nailfold Capilloroscopy
• Nailfold capillaries lie parallel rather than ꓕ
• Abnormalities not present in vasospastic disease
• Independent predictor for SScdevelopment

1° vs 2° Raynaud's
• Digital ischemia may precede systemic manifestations of these secondary diseases, makes diagnosis more difficult
• % of patients who go on to develop secondary Raynaud’s

Management of Primary Raynaud’s
• Cold avoidance, Gloves• Stop smoking• Stop beta blockers• Stop ergot preparations
(migraine therapy)• Biofeedback doesn’t work

Medical management of Raynaud's
First line therapy – calcium channel blockers
–Procardia XL (nifedipine) 30-60mg qd to bid–Norvasc (amlodipine) 5-10mg qd

Medical management of Raynaud's
Second line therapy with proven efficacy• Angiotensin II RCP blockade (losartan) • ACE Inhibitors (enalopril)• (Prozac) Fluoxetine• Alpha blockers (prazosin)

Alpha blockers reserpine

Medical management of Raynaud's
• Topical vasodilators (GTN)• IV prostanoid (Iloprost)• Endothelin RCP antagonist (Bosentan) • +/- antiplatelets

PDE5 Inhibitors
• Increase availability of NO• Second choice for secondary Raynaud's• Sildenafil (Viagra) 20-25 mg TID

Raynaud's syndrome disordersless than 1% of all Raynaud's
• Immunological and connective tissue disorders– Scleroderma– Mixed CT disease– RA– SLE– Dermatomyositis– Polymyositis– Hep B antigen induced vasculitis– Sjogrens syndrome– Drug induced vasculitis– Hypersensitivity angiitis– Undifferentiated CT disease– Antiphospholipid syndrome
• Obstructive arterial diseases– Atherosclerosis– buergers syndrome– TOS
• Environmental conditions– Vibration injury– Direct arterial trauma– Cold injury
• Drug induced Raynaud's syndrome without vasculitis– Ergot– B blockers– Cytotoxic drugs– OCPS
• Miscellaneous– Vinyl chloride disease– CRF– Cold agglutinins– Cryoglobulinemia– Neoplasia– Neurologic disorders– Endocrine disorders

Small Vessel Occlusion
Mechanism of obstruction is variable–Autoimmune vasculitis - widespread digital and
palmar artery occlusions

Small Vessel Occlusion
Vibrating tools- fibrotic form of
palmar and digital artery obstruction
- presumably shear stress

Small Vessel Occlusion
Pathophysiology–Hypercoagulable states–Embolic–Atherosclerotic–Renal failure

Small vessel occlusion
Gangrene • Usually occlusive disease-either digital or palmar arch. • BUT a proximal embolizing or obstructing lesion should be
looked for• Process of digital gangrene is different from necrosis-it is not
suppurative but a process of desication and mummification

Medical management
• No abx ointment-will dessicate
• Occasional suppurativeprocess requires iv abx, possible debridement
• Auto-amputation

Surgical therapy
• Cervical thoracic sympathectomy results are too short
• Perineural neurectomy• Fat grafting• Botox• Occasionally PTA

Surgical therapy
• Amputation rarely indicated• Spinal cord stimulation

Scleroderma
• Raynaud's phenomena present in 95% pts
• 40-50% pts will have a digital ulcer in their lifetime

Hypothenar Hammer Syndrome
• Male• Sudden onset• Unilateral

Hypothenar Hammer Syndrome
• Visible/palpable mass by hypothenar eminence due to ulnar artery aneurysm
• Aneurysm may embolize• May also present with thrombosis

Hypothenar Hammer Syndrome

Vasculitis of Malignancy
• Hairy cell leukemia– Systemic necrotizing vasculitis
• “Paraneoplastic” vasculitides• Vasculitis with solid tumors

Drug Abuse Vasculitis
• IVDA of meth or cocaine is associated with pan arteritis
• Accidental arterial injection • Treatment
– Heparin, debridement

Antiphospholipid Syndrome
• Acquired autoimmune disorder• Recurrent arterial and venous thrombosis – anywhere• Thrombotic events treated with anticoagulation

Ergotism
• Most cases due to ergot alkaloid treatments
• Can cause severe spasm of digital vessels - gangrene

Thromboangiitis Obliterans (TO)
• Formerly known as Buerger’s• Segmental medium and small vessel occlusion • Arms and legs• 40-50% pts have history of superficial migratory
thrombophlebitis, Raynaud’s or both

Thromboangiitis Obliterans (TO)
• USA• 10% isolated UE involvement• 30-40% UE and LE involvement• 50% LE

Thromboangiitis Obliterans (TO)
Arterial wall inflammatory infiltrate
Etiology unknown – Tobacco is permissive, probably
causative

Diagnosis
Essential Criteria• Onset of sx <45
• Tobacco use
• No disease proximal to popliteal artery
• No disease proximal to distal brachial artery
• Objective documentation distal occlusive disease
Supportive Criteria• Superficial thrombophlebitis
• Raynaud’s
• UE involvement

Differential Diagnosis
Must exclude:• Proximal embolic source• Trauma and local lesion• Autoimmune disease• Hypercoagulable state• Atherosclerosis• Atherosclerotic risk factors (DM, HTN, Hyperlipidemia)

Angiography
• Symmetric
• Radial or ulnar occlusion
• Segmental rather than diffuse
• Extensive digital and palmar artery occlusive disease

Treatment
• Stop smoking• Palliative• Remissions related to resumption of smoking• Limb salvage not as good as with atherosclerosis• Normal life expectancy, no coronary involvement

Large Vessel Arteritis
• Giant Cell• Radiation induced

Giant Cell Arteritis
Systemic GCA (temporal arteritis) vs. Takayasu’s arteritis

Giant Cell Arteritis
Systemic GCA (temporal arteritis)• Usually carotid artery branches
• But any branches
• Most often complaint is severe pain along course of temporal artery
• Women older than 50

Systemic GCA
Diagnosis• Biopsy
• Duplex may be helpful
Treatment• Prompt steroid therapy
• MTX
• Cyclosporin, Azathioprine
• TNF inhibitors
• Pyrimidine synthesis inhibitors

Takayasu’s Arteritis
• Younger patients, female more often
• Smooth tapered stenosis of subclavian, axillary, brachial
• Can cause stenosis of aorta and its branches, main difference is pulmonary artery involvement
• Thoracic aortic aneurysm 17x risk
• AAA 2.4x risk

Takayasu’s Arteritis
Pediatric
• Not as strong sex predilection
• Heart failure is common
• 75% survival at 20 yrs, heart failure driven
• HTN
• Also, myocarditis, coronary artery involvement, valvular involvement, pulmonary involvement

Takayasu’s Arteritis
• Two stages of illness– Acute – Chronic
• Same medications used as temporal arteritis
• Results not as consistent as with TA

Surgical Intervention
• Best done in quiescent (chronic) state
• Symptomatic stenosis
• Aneurysmal lesions

Surgical Intervention
• Successful surgery requires bypass to normal artery
• Continue steroid therapy
• PTA higher restenosis rate than expected, 90%

Surveillance
• Follow ESR, CRP
• PET-CT scan

Upper Extremity Acute Arterial Insufficiency
50% - embolization• mostly cardiac• also aneurysm brachiocephalic/subclavian
25% - primary arterial thrombosis25% - iatrogenic
• ABGs• A lines• AVF creation

Upper Extremity Acute Arterial Insufficiency
• Embolization is associated with 25% mortality–Recurrence and embolization to other vascular beds
• Renal, Mesenteric, Cerebral

Revascularization
• Thrombectomy• Endovascular• Combined

Repetitive Trauma
• Quadrilateral space syndrome-axillary artery injury
• Humeral head syndrome- post humeral circumflex artery injury
• Both lead to embolization• Common in throwing athletes

Large Vessel Occlusive Disease
• Atherosclerosis- most common
• Same risk factors as lower extremity
• Diabetes, renal failure lesions may involve large and small vessels

Large Vessel Occlusive Disease
AneurysmSubclavian and axillary – most common

Iatrogenic venous disease
• Trauma• IV access• PICC lines• Dialysis catheters

COVID 19 – Acute Limb Ischemia
• Thrombotic etiology predominates
• Can occur in pts receiving thromboprophylaxis

COVID 19- Acute Limb Ischemia
• Risk factors – Older age– Obesity– Cardiovascular comorbidities
• More typically affects patients with severe COVID-19
• Occurs five to seven days after respiratory decompensation

COVID 19 – Acute Limb Ischemia
• Thrombosis of large or medium-sized arteries have all been reported.
• Small vessel thrombosis leading to digital gangrene is often associated with the administration of vasopressor agents.

COVID 19 – Acute Limb Ischemia
• About 20 percent of patients who present with COVID-19 related ALI have few or no respiratory symptoms.
• Furthermore, ALI can occur during the recovery phase following infection of any severity.