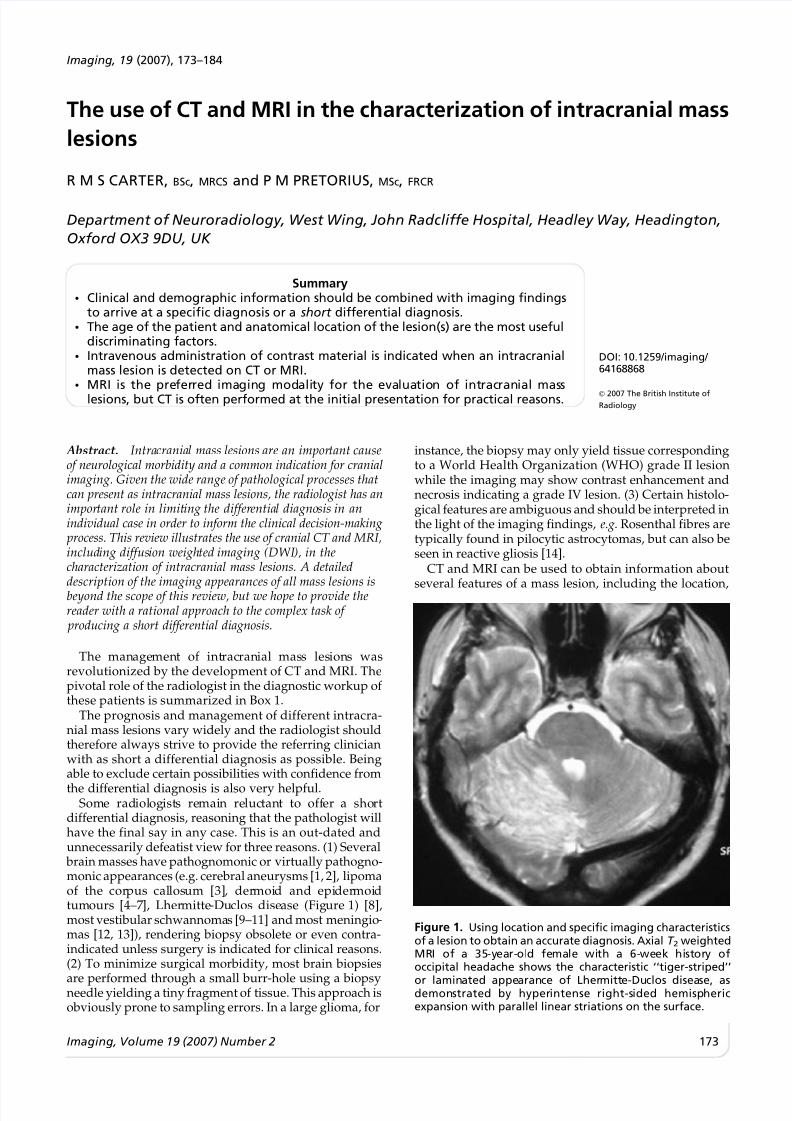
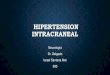
The use of CT and MRI in the characterization of intracranial mass lesions R M S CARTER, BSc, MRCS and P M PRETORIUS, MSc, FRCR Department of Neuroradiology, West Wing, John Radcliffe Hospital, Headley Way, Headington, Oxford OX3 9DU, UKSummary N Clinical and demographic information should be combined with imaging findings to arrive at a specific diagnosis or a shortdifferential diagnosis. N The age of the patient and anatomical location of the lesion(s) are the most useful discriminating factors. N Intravenous administration of contrast material is indicated when an intracranial mass lesion is detected on CT or MRI. N MRI is the preferred imaging modali ty for the evaluation of intracranial mass lesions, but CT is often performed at the initial presentation for practical reasons. DOI: 10.1259/imaging/64168868 ’ 2007 The British Institute of Radiology Abstract. Intra crania l mass lesions are an impor tant cause of neurological morbidity and a common indication for cranial imaging. Given the wide range of pathological processes that can present as intracranial mass lesions, the radiologist has an impor tant role in limit ing the differ entia l diagno sis in an individual case in order to inform the clinical decision-making process. This review illustrates the use of cranial CT and MRI, includ ing diffus ion weigh ted imaging (DWI ), in the characterization of intracranial mass lesions. A detailed description of the imaging appearances of all mass lesions is beyond the scope of this review, but we hope to provide the reader with a rational approach to the complex task ofproducing a short differential diagnosis. The man age ment of int rac ran ial mas s les ion s was revolutionized by the development of CT and MRI. The pivotal role of the radiologist in the diagnostic workup ofthese patients is summarized in Box 1. The prognosis and management of different intracra- nial mass lesions vary widely and the radiologist should therefore always strive to provide the referring clinician with as short a differential diagnosis as possible. Being able to exclude certain possibilities with confidence from the differential diagnosis is also very helpful. Some rad iol ogists remain reluc tan t to off er a sho rt differential diagnosis, reasoning that the pathologist will have the final say in any case. This is an out-dated and unnecessarily defeatist view for three reasons. (1) Several brain masses have pathognomonic or virtually pathogno- monic appearances (e.g. cerebral aneurysms [1, 2], lipoma of the cor pus cal los um [3] , der moi d and epi der moi d tumours [4–7 ], Lher mitte -Du clos dise ase (Fig ure 1) [8], most vestibular schwannoma s [9–11] and most meningio - mas [12, 13]), rendering biopsy obsolete or even contra- indicated unless surgery is indicated for clinical reasons. (2) To minimize surgical morbidity, most brain biopsies are performed through a small burr-hole using a biopsy needle yielding a tiny fragment of tissue. This approach is obviously prone to sampling errors. In a large glioma, for instance, the biopsy may only yield tissue corresponding to a World Health Organization (WHO) grade II lesion while the imaging may show contrast enhancement and necrosis indicating a grade IV lesion. (3) Certain histolo- gical features are ambiguous and should be interpreted in the light of the imaging findings, e.g. Rosenthal fibres are typically found in pilocytic astrocytomas, but can also be seen in reactive gliosis [14]. CT and MRI can be used to obtain information about several features of a mass lesion, including the location, Figure 1. Using location and specific imaging characteristics of a lesion to obtain an accurate diagnosis. Axial T2 weighted MRI of a 35-year- ol d female wi th a 6-week hi st ory of occipital headache shows the characteristic ‘‘tiger-striped’’ or lamin ated appearance of Lher mitt e-Du clos disea se, as demonstrated by hyperintense right-sided hemispheric expansion with parallel linear striations on the surface. Imaging, 19 (2007), 173–184 Imaging, Volume 19 (2007) Number 2 173