Embed Size (px)
Citation preview
MECHANISMS OF FAILURE IN THE REPAIR OF LARGE RETINAL TEARS
HARVEY LINCOFF, M.D., INGRID KREISSIG, M.D., AND FRANK LAFRANCO, M.D.
New York, New York
The purpose of this paper is to describe the mechanisms of failure in the repair of large horseshoe tears and to contrast them with the results obtained in the treatment of retinal dialyses of equivalent size.
MATERIAL AND METHODS
We examined the preoperative drawings of the last 1,650 consecutive patients admitted to New York Hospital for repair of retinal detachment to find those patients with retinal breaks greater than 60 degrees. Fifty-one patients with large breaks in one eye and five patients with large breaks in both eyes were identified (Table 1). For the purposes of analysis, we separated the patients into two groups: (1) those whose retinas were torn in two dimensions, anteroposteriorly and circumferentially (typically horseshoe tears); and (2) patients whose retinas were torn only circumferentially (all dialyses).
The patients with horseshoe tears are further subdivided into those whose tears had circumferential lengths less than and greater than 70 degrees. The patients with dialyses are divided into those with tears less than and greater than 90 degrees. The division of horseshoe type tears at 70 degrees and dialyses at 90 degrees is not arbitrary, but reflects limits for various therapeutic approaches.
Large horseshoe tears—The surgical management of large horseshoe tears changed over the 11 years of the series. Initially, they were treated with cryopexy
From the Department of Ophthalmology, New York Hospital-Cornell Medical Center (Drs. Lincoff and LaFranco), and the Universitaets-Augenklinik, Bonn, West Germany (Dr. Kreissig).
Reprint requests to Harvey Lincoff, M.D., New York Hospital, Department of Ophthalmology, 525 East 68th St., New York, NY 10021.
TABLE 1 DISTRIBUTION OF LARGE TEARS
Type No.
Horseshoe 60° to 70° 10 > 70° 20
Dialyses 60° to 90° 23 >90° 8
Total 61
and encircling elements oriented to the posterior edge of the break. The intention was to wall the break away, to confine it to the periphery. Intravitreal air was subsequently added to press out leaking folds on the buckle. We abandoned the encircling structure when we realized that it augmented retinal folds.1·2 In recent years, large tears, up to 70 degrees in circumferential dimension, have been treated with radial buckles, often without drainage of subretinal fluid. Tears of more than 70 degrees are treated initially with cryopexy, drainage, and an intravitreal air or large molecule gas injection3
aimed at reducing the problem to a point where it becomes amenable to conventional buckling.
Dialyses—The management of dialyses has undergone only minor changes by comparison. They have been treated with circumferential buckles throughout. The length of the buckles has been shortened through the years and the drainage of subretinal fluid has been omitted for tears up to 90 degrees.
RESULTS
We performed 100 operations on 61 eyes with tears greater than 60 degrees in circumferential dimension. The results
501
502 AMERICAN JOURNAL OF OPHTHALMOLOGY OCTOBER, 1977
TABLE 2 ANATOMICAL RESULTS
Type of Tear
Horseshoe 60° to 70° >70° Total
Dialvses 60° to 90° >90° Total
No.
10 20 30
23 8
31
Reattached
7 10 17
23 7
30
are shown in Tables 2 and 3. When the patients are divided into those treated at the beginning of the series and those treated later, a therapeutic direction is indicated.
Horseshoe tears—Of ten tears between 60 and 70 degrees, six were treated early in the series with circumferential or encircling buckles and two failed to reat-tach. Of four treated with radial buckles, one failed after two months because of massive preretinal retraction. There were 20 eyes with tears of more than 70 degrees. Fourteen were treated early in the series with long circumferential or encircling structures and ten failed. Six tears treated later in the series reattached with gas tamponade alone or with subsequent radial or short circumferential buckles. One of these failed with massive preretinal retraction in the fourth postoperative week.
TABLE 3 FUNCTIONAL RESULTS IN
4 7 EYES REATTACHED
Final Macula Attached Macula Detached Visual Acuity Preoperatively Preoperatively
6/6-6/12 (20/20-20/40)
6/15-6/22 (20/50-20/70)
6/24-6/120 (20/80-20/400)
19
0
11
Dialyses—All of 23 dialyses between 60 and 90 degrees responded favorably to circumferential buckles, 17 without drainage of subretinal fluid. Of the eight dialyses greater than 90 degrees, three reattached with circumferential buckles alone and four of the remaining five with the addition of drainage and gas injections.
DISCUSSION
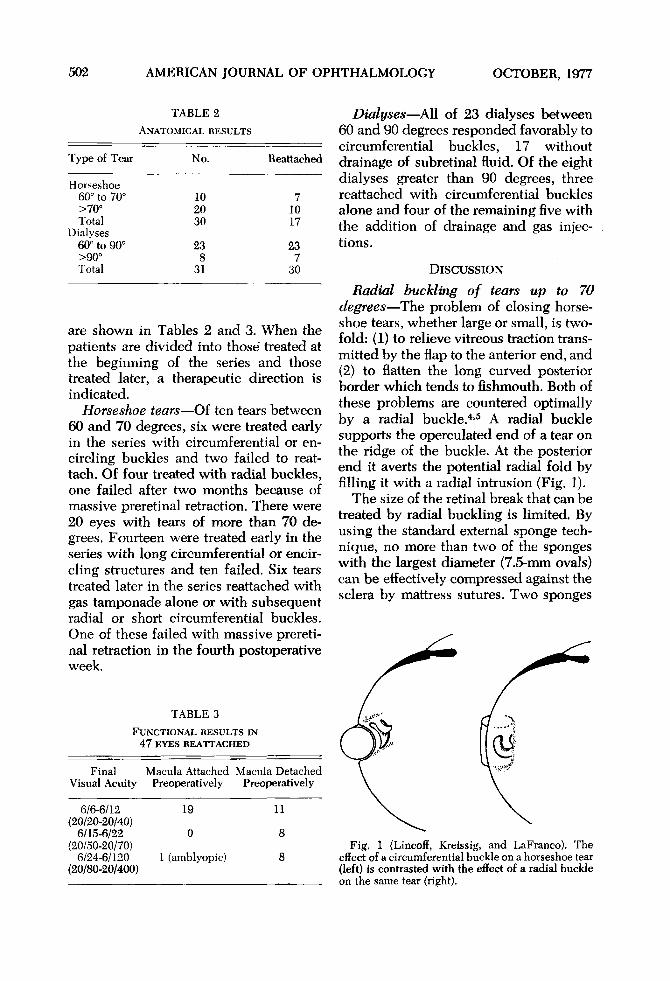
Radial buckling of tears up to 70 degrees—The problem of closing horseshoe tears, whether large or small, is twofold: (1) to relieve vitreous traction transmitted by the flap to the anterior end, and (2) to flatten the long curved posterior border which tends to fishmouth. Both of these problems are countered optimally by a radial buckle.4·5 A radial buckle supports the operculated end of a tear on the ridge of the buckle. At the posterior end it averts the potential radial fold by filling it with a radial intrusion (Fig. 1).
The size of the retinal break that can be treated by radial buckling is limited. By using the standard external sponge technique, no more than two of the sponges with the largest diameter (7.5-mm ovals) can be effectively compressed against the sclera by mattress sutures. Two sponges
1 (amblyopic) Fig. 1 (Lincoff, Kreissig, and LaFranco). The
effect of a circumferential buckle on a horseshoe tear (left) is contrasted with the effect of a radial buckle on the same tear (right).
VOL. 84, NO. 4 LARGE RETINAL TEARS 503
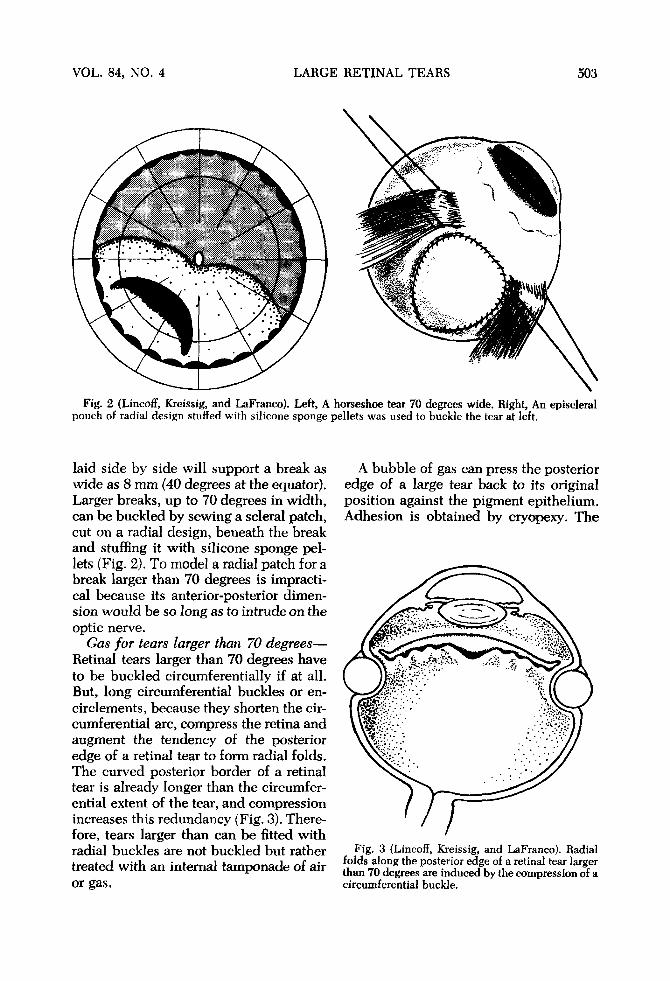
Fig. 2 (Lincoff, Kreissig, and LaFranco). Left, A pouch of radial design stuffed with silicone sponge
laid side by side will support a break as wide as 8 mm (40 degrees at the equator). Larger breaks, up to 70 degrees in width, can be buckled by sewing a scierai patch, cut on a radial design, beneath the break and stuffing it with silicone sponge pellets (Fig. 2). To model a radial patch for a break larger than 70 degrees is impractical because its anterior-posterior dimension would be so long as to intrude on the optic nerve.
Gas for tears larger than 70 degrees— Retinal tears larger than 70 degrees have to be buckled circumferentially if at all. But, long circumferential buckles or encirclements, because they shorten the circumferential arc, compress the retina and augment the tendency of the posterior edge of a retinal tear to form radial folds. The curved posterior border of a retinal tear is already longer than the circumferential extent of the tear, and compression increases this redundancy (Fig. 3). Therefore, tears larger than can be fitted with radial buckles are not buckled but rather treated with an internal tamponade of air or gas.
horseshoe tear 70 degrees wide. Right, An episeleral pellets was used to buckle the tear at left.
A bubble of gas can press the posterior edge of a large tear back to its original position against the pigment epithelium. Adhesion is obtained by cryopexy. The
Fig. 3 (Lincoff, Kreissig, and LaFranco). Radial folds along the posterior edge of a retinal tear larger than 70 degrees are induced by the compression of a circumferential buckle.
504 AMERICAN JOURNAL OF OPHTHALMOLOGY OCTOBER, 1977
anterior edge, operculated and under traction, however, remains elevated within the gas bubble or is only temporarily flattened while the gas is present. To confine the anterior detachment, lines of cryopexy are extended anteriorly on either side of the break to a latitude beyond the pull of the operculum, or to the ora serrata, if the ora serrata is close upon the break.
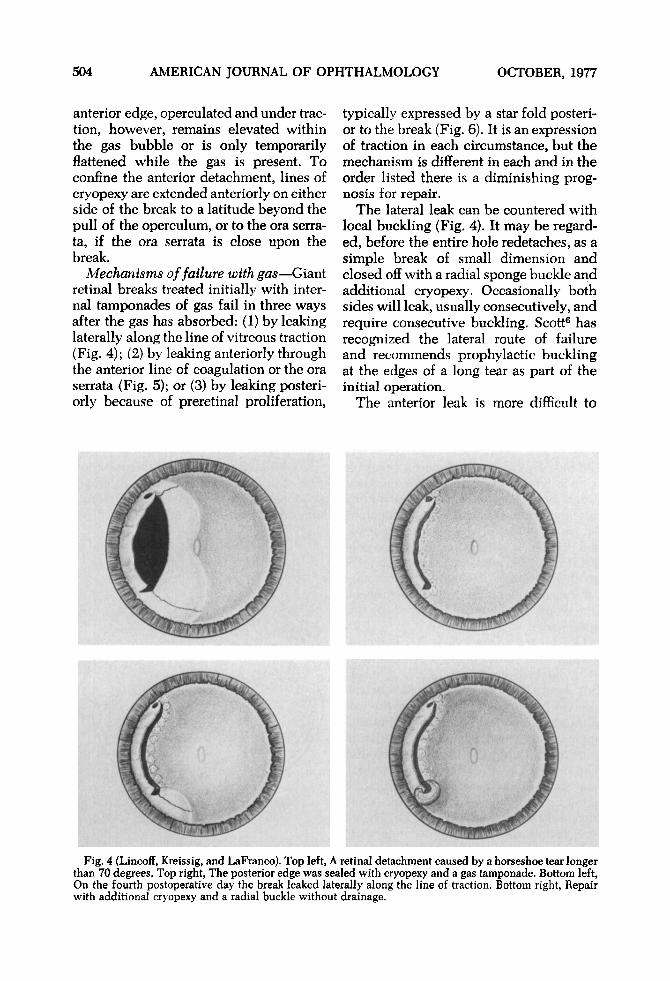
Mechanisms of failure with gas—Giant retinal breaks treated initially with internal tamponades of gas fail in three ways after the gas has absorbed: (1) by leaking laterally along the line of vitreous traction (Fig. 4); (2) by leaking anteriorly through the anterior line of coagulation or the ora serrata (Fig. 5); or (3) by leaking posteriorly because of preretinal proliferation,
Fig. 4 (Lincoff, Kreissig, and LaFranco). Top left, than 70 degrees. Top right, The posterior edge was s On the fourth postoperative day the break leaked li with additional cryopexy and a radial buckle witho
typically expressed by a star fold posterior to the break (Fig. 6). It is an expression of traction in each circumstance, but the mechanism is different in each and in the order listed there is a diminishing prognosis for repair.
The lateral leak can be countered with local buckling (Fig. 4). It may be regarded, before the entire hole redetaehes, as a simple break of small dimension and closed off with a radial sponge buckle and additional cryopexy. Occasionally both sides will leak, usually consecutively, and require consecutive buckling. Scott6 has recognized the lateral route of failure and recommends prophylactic buckling at the edges of a long tear as part of the initial operation.
The anterior leak is more difficult to
retinal detachment caused by a horseshoe tear longer Jed with cryopexy and a gas tamponade. Bottom left, irally along the line of traction. Bottom right, Repair drainage.
VOL. 84, NO. 4 LARGE RETINAL TEARS 505
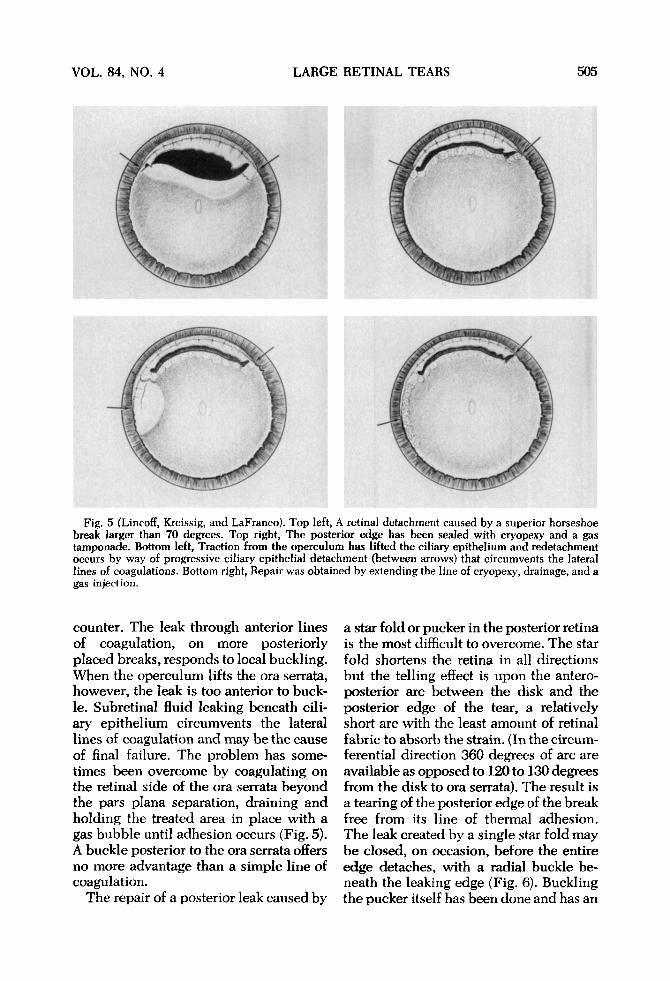
Fig. 5 (Lincoff, Kreissig, and LaFranco). Top left, A retinal detachment caused by a superior horseshoe break larger than 70 degrees. Top right, The posterior edge has been sealed with cryopexy and a gas tamponade. Bottom left, Traction from the operculum has lifted the ciliary epithelium and redetachment occurs by way of progressive ciliary epithelial detachment (between arrows) that circumvents the lateral lines of coagulations. Bottom right, Repair was obtained by extending the line of cryopexy, drainage, and a gas injection.
counter. The leak through anterior lines of coagulation, on more posteriorly placed breaks, responds to local buckling. When the operculum lifts the ora serrata, however, the leak is too anterior to buckle. Subretinal fluid leaking beneath ciliary epithelium circumvents the lateral lines of coagulation and may be the cause of final failure. The problem has sometimes been overcome by coagulating on the retinal side of the ora serrata beyond the pars plana separation, draining and holding the treated area in place with a gas bubble until adhesion occurs (Fig. 5). A buckle posterior to the ora serrata offers no more advantage than a simple line of coagulation.
The repair of a posterior leak caused by
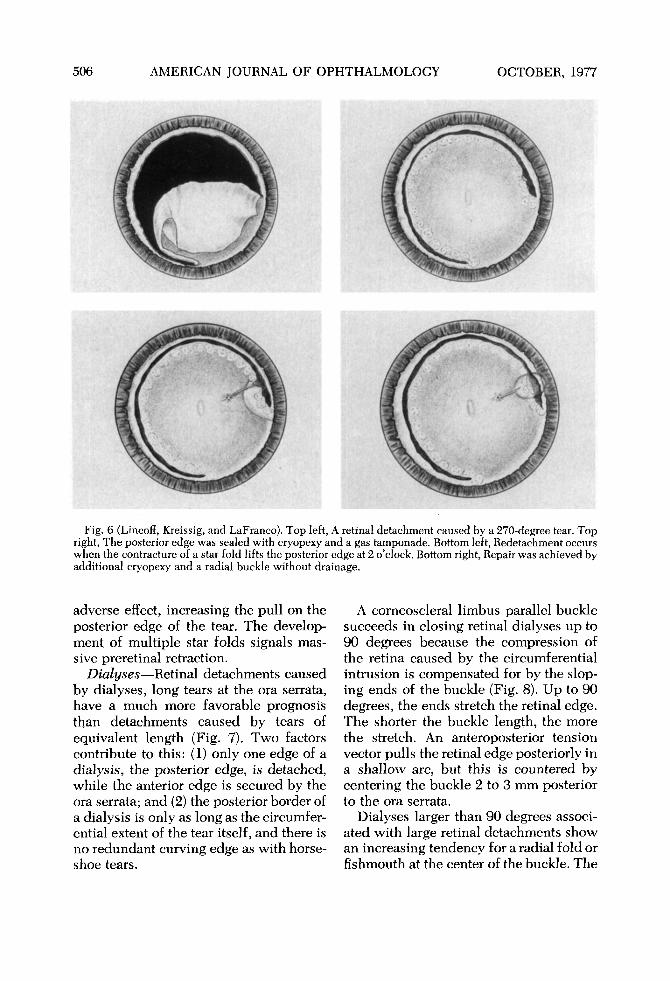
a star fold or pucker in the posterior retina is the most difficult to overcome. The star fold shortens the retina in all directions but the telling effect is upon the antero-posterior arc between the disk and the posterior edge of the tear, a relatively short arc with the least amount of retinal fabric to absorb the strain. (In the circumferential direction 360 degrees of arc are available as opposed to 120 to 130 degrees from the disk to ora serrata). The result is a tearing of the posterior edge of the break free from its line of thermal adhesion. The leak created by a single star fold may be closed, on occasion, before the entire edge detaches, with a radial buckle beneath the leaking edge (Fig. 6), Buckling the pucker itself has been done and has an
506 AMERICAN JOURNAL OF OPHTHALMOLOGY OCTOBER, 1977
Fig. 6 (Lincoff, Kreissig, and LaFranco). Top left, A retinal detachment caused by a 270-degree tear. Top right, The posterior edge was sealed with cryopexy and a gas tamponade. Bottom left, Redetachment occurs when the contracture of a star fold lifts the posterior edge at 2 o'clock. Bottom right, Repair was achieved by additional cryopexy and a radial buckle without drainage.
adverse effect, increasing the pull on the posterior edge of the tear. The development of multiple star folds signals massive preretinal retraction.
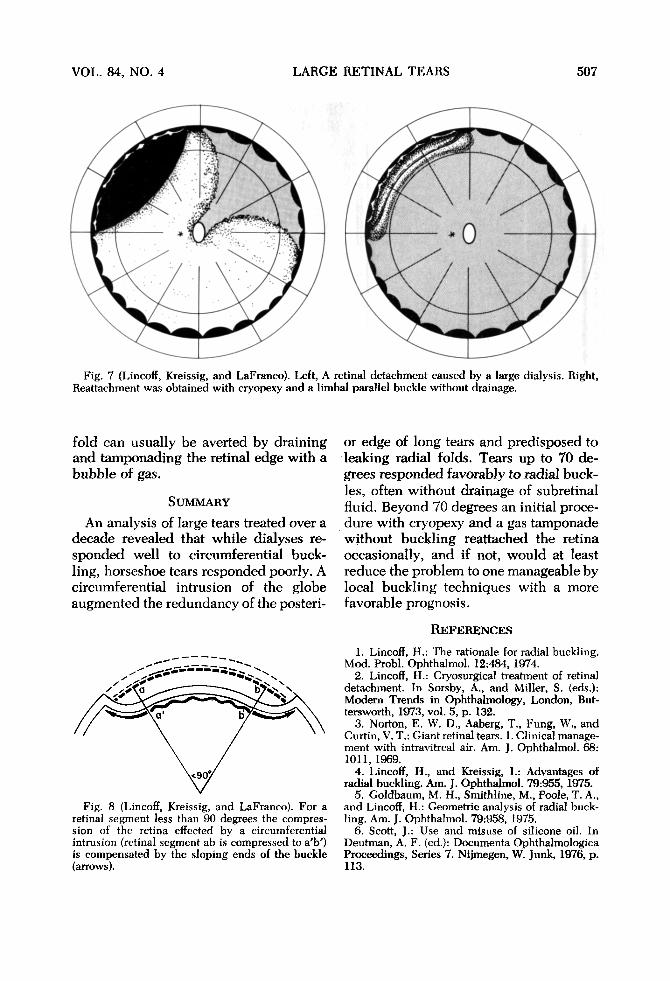
Dialyses—Retinal detachments caused by dialyses, long tears at the ora serrata, have a much more favorable prognosis than detachments caused by tears of equivalent length (Fig. 7). Two factors contribute to this: (1) only one edge of a dialysis, the posterior edge, is detached, while the anterior edge is secured by the ora serrata; and (2) the posterior border of a dialysis is only as long as the circumferential extent of the tear itself, and there is no redundant curving edge as with horseshoe tears.
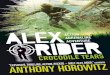
A corneoscleral limbus parallel buckle succeeds in closing retinal dialyses up to 90 degrees because the compression of the retina caused by the circumferential intrusion is compensated for by the sloping ends of the buckle (Fig. 8). Up to 90 degrees, the ends stretch the retinal edge. The shorter the buckle length, the more the stretch. An anteroposterior tension vector pulls the retinal edge posteriorly in a shallow arc, but this is countered by centering the buckle 2 to 3 mm posterior to the ora serrata.
Dialyses larger than 90 degrees associated with large retinal detachments show an increasing tendency for a radial fold or fishmouth at the center of the buckle. The
VOL. 84, NO. 4 LARGE RETINAL TEARS 507
Fig. 7 (Lincoff, Kreissig, and LaFranco). Left, A retinal detachment caused by a large dialysis. Right, Reattachment was obtained with cryopexy and a limbal parallel buckle without drainage.
fold can usually be averted by draining and tamponading the retinal edge with a bubble of gas.
SUMMARY
An analysis of large tears treated over a decade revealed that while dialyses responded well to circumferential buckling, horseshoe tears responded poorly. A circumferential intrusion of the globe augmented the redundancy of the posteri-
Fig. 8 (Lincoff, Kreissig, and LaFranco). For a retinal segment less than 90 degrees the compression of the retina effected by a circumferential intrusion (retinal segment ab is compressed to a'b') is compensated by the sloping ends of the buckle (arrows).
or edge of long tears and predisposed to leaking radial folds. Tears up to 70 degrees responded favorably to radial buckles, often without drainage of subretinal fluid. Beyond 70 degrees an initial procedure with cryopexy and a gas tamponade without buckling reattached the retina occasionally, and if not, would at least reduce the problem to one manageable by local buckling techniques with a more favorable prognosis.
REFERENCES 1. Lincoff, H.: The rationale for radial buckling.
Mod. Probi. Ophthalmol. 12:484, 1974. 2. Lincoff, H.: Cryosurgical treatment of retinal
detachment. In Sorsby, A., and Miller, S. (eds.): Modern Trends in Ophthalmology, London, But-tersworth, 1973, vol. 5, p. 132.
3. Norton, E. W. D., Aaberg, T., Fung, W., and Curtin, V. T.: Giant retinal tears. 1. Clinical management with intravitreal air. Am. J. Ophthalmol. 68: 1011, 1969.
4. Lincoff, H., and Kreissig, I.: Advantages of radial buckling. Am. J. Ophthalmol. 79:955, 1975.
5. Goldbaum, M. H., Smithline, M., Poole, T. A., and Lincoff, H.: Geometric analysis of radial buckling. Am. J. Ophthalmol. 79:958, 1975.
6. Scott, J.: Use and misuse of silicone oil. In Deutman, A. F. (ed.): Documenta Ophthalmologica Proceedings, Series 7. Nijmegen, W. Junk, 1976, p. 113.


![$PQZSJHIU …ousar.lib.okayama-u.ac.jp/files/public/5/56175/...rhages, retinal pigment epithelial tears, and/or chorio-capillaris atrophy [9-11]. The risk of serious complica-tions](https://img.pdfslide.net/doc/110x75/5e274ba9c8f801547e287b2d/pqzsjhiu-ousarlibokayama-uacjpfilespublic556175-rhages-retinal-pigment.jpg)












![Blood, Sweat & Tears - [Book] the Best of Blood, Sweat & Tears](https://img.pdfslide.net/doc/110x75/577c780e1a28abe0548e8be9/blood-sweat-tears-book-the-best-of-blood-sweat-tears.jpg)











