Embed Size (px)
Citation preview

8/12/2019 Melanoma Sentinel Node
http://slidepdf.com/reader/full/melanoma-sentinel-node 1/63
MELANOMA
Sentinel Lymph Node Evaluation:
Update
Kim James Charney, MD

8/12/2019 Melanoma Sentinel Node
http://slidepdf.com/reader/full/melanoma-sentinel-node 2/63
Conflict of Interest
None

8/12/2019 Melanoma Sentinel Node
http://slidepdf.com/reader/full/melanoma-sentinel-node 3/63
Objectives
Sentinel lymph node (SLN) biopsy conceptand technique
Impact of SLN metastasis on recurrence andsurvival in melanoma
Implication of isolated SLN tumor cells inmelanoma
SLN tumor burden
Necessity of completion lymph node
dissection (CLND) Candidates for SLN biopsy

8/12/2019 Melanoma Sentinel Node
http://slidepdf.com/reader/full/melanoma-sentinel-node 4/63
Stage I & II
85% of newly diagnosed patients

8/12/2019 Melanoma Sentinel Node
http://slidepdf.com/reader/full/melanoma-sentinel-node 5/63
Surgical Management of Stage I and II
Goals
Accurate Staging
Assess risk for recurrence Recommendation for therapy
Durable Local/Regional Control
Cure
Minim ize Morb idi ty
8/12/2019 Melanoma Sentinel Node
http://slidepdf.com/reader/full/melanoma-sentinel-node 6/63
Stage I and II Primary MelanomaComponents of Treatment
Wide Excision
Margins appropriate for thickness
Regional Nodes?

8/12/2019 Melanoma Sentinel Node
http://slidepdf.com/reader/full/melanoma-sentinel-node 7/63
Lymph Node Involvement and
Melanoma
Regional nodes, most common site of first
recurrence
>50% chance for distant relapse
15-50% chance for in-basin failure after lymph node
dissection for palpable disease

8/12/2019 Melanoma Sentinel Node
http://slidepdf.com/reader/full/melanoma-sentinel-node 8/63
Approach to the Clinically Negative
Regional Basin
Observation-----------------------Therapeutic Dissection
ELND Intermediate thickness
Selective lymphadenectomy Lymphatic mapping and sentinel lymph node biopsy
Only pt’s with metastases are dissected

8/12/2019 Melanoma Sentinel Node
http://slidepdf.com/reader/full/melanoma-sentinel-node 9/63
Morton, DL, et al. Arch Surg . 1992; 127:392-399

8/12/2019 Melanoma Sentinel Node
http://slidepdf.com/reader/full/melanoma-sentinel-node 10/63
Sentinel Node BiopsyPublished Findings
SLN identification rate: 99% Dual modality technique
Blue dye
Radio-colloid injections and gamma probe
Accurately stages regional nodal basin Concomitant ELND:FNR < 5%
Follow-up of SLN-neg. patients: ~3% will develop nodaldisease
Facilitates the use of sensitive pathologic techniques

8/12/2019 Melanoma Sentinel Node
http://slidepdf.com/reader/full/melanoma-sentinel-node 11/63
Sentinel Node Biopsy
Goals
Improve disease outcome for node positive
patients
Regional control
Survival
Prevent the development of clinical nodal involvement
Minimally invasive approach to nodal staging

8/12/2019 Melanoma Sentinel Node
http://slidepdf.com/reader/full/melanoma-sentinel-node 12/63
StagingPrognostic Relevance

8/12/2019 Melanoma Sentinel Node
http://slidepdf.com/reader/full/melanoma-sentinel-node 13/63
2010 AJCC StagingChanges
Stage I and II (clinically localized) Thickness
Ulceration
Mitotic Rate >1/mm2
SLN status?
Stage III (regional) Nodes
In-transit disease
Ulceration
Stage IV (distant) Site
LDH

8/12/2019 Melanoma Sentinel Node
http://slidepdf.com/reader/full/melanoma-sentinel-node 14/63
0 1 2 3 4 5 6 7 8
1.0
0.9
0.8
0.7
0.6
0.5
0.4
0.3
0.2
0.1
9 10 11 1312 14 15
(1)
(3)(5)
(7)
Survival, years
P r o p o r t i o n S u r v i v
i n g
(2)
(4)
(6)
(8)
Balch CM, et al. J Clin Oncol . 2001;19(16):3622-3634.
Non-ulcerated
Ulcerated
AJCC MELANOMA STAGING DATABASESurvival Curves for Stage I & II
Ia
Ib
IIa
IIb
IIc

8/12/2019 Melanoma Sentinel Node
http://slidepdf.com/reader/full/melanoma-sentinel-node 15/63
Incidence of SLN MetastasesMDACC Database
Tumor Total No. Positive SLN
Thickness Patients All non-Ulcerated ulcerated
(mm) (N) (%) (%) (%)
< 1.00 326 4.2 3.9 12.5
1.01-2.00 490 11.4 10.8 21.22.01-4.00 310 28.5 23.1 37.0
4.01+ 190 45.5 34.2 55.4
Total 1316 17.4 11.9 37.0
Ross, MI. Clin Cancer Res. 2006;12: 2312s-2319s.

8/12/2019 Melanoma Sentinel Node
http://slidepdf.com/reader/full/melanoma-sentinel-node 16/63
2008 AJCC Melanoma Database Stage I
Survival Rates for T1 Patients (0.01-1.00 mm)
According to MR (per mm2)
Survival Rate
Thickness MR 5-Year 10-Year n
(mm)
0.01-0.50 <1.0 99% 97% 1,194
0.01-0.50 >1.0 97% 95% 327
0.51-1.00 <1.0 98% 93% 1,472
0.51-1.00 >1.0 94% 87% 1,868
2009 staging rule: T1b melanomas defined as
≤1.0 mm with ulceration or >1 mitosis / mm2
The original source for this material is the AJCC Cancer Staging Manual, Seventh Edition (2010)
published by Springer Science and Business Media LLC, www.springerlink.com.

8/12/2019 Melanoma Sentinel Node
http://slidepdf.com/reader/full/melanoma-sentinel-node 17/63
Impact of MR on SLN Positivity
Currently, the T1b designation is used for staging interms of survival
Is not itself a criterion to perform SLNB
Evolving data suggests that MR may be predictive of
occult regional nodal disease
Andtbacka RH et al: SLNB in thin melanoma
Suggests that SLNB is appropriate for patients with T1b
melanomas, including those defined by MR
Await publication of a larger analysis of patients with
thin melanoma
Andtbacka RH, Gershenwald JE. JNCCN. 2009;7:308-317.
8/12/2019 Melanoma Sentinel Node
http://slidepdf.com/reader/full/melanoma-sentinel-node 18/63
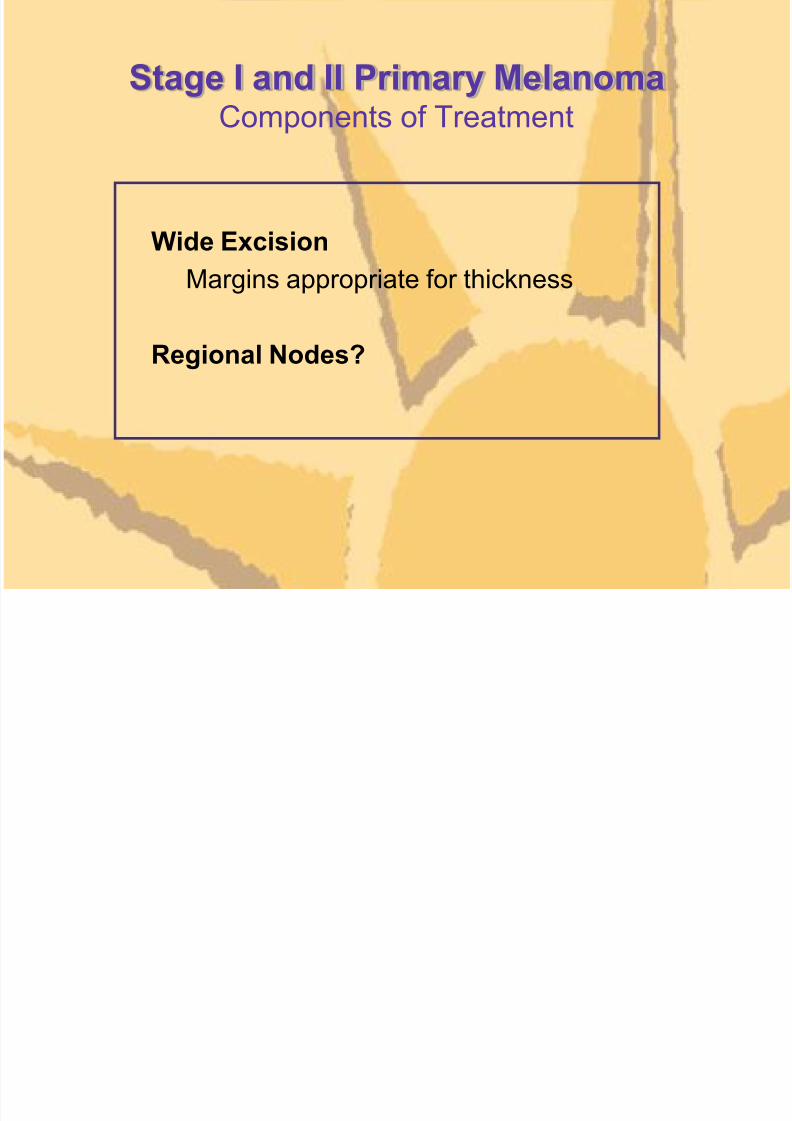
Prognostic Factors Influencing
Disease-Specific Survival _____________________________________________________________________________
Multiple covariate
Prognostic Factor Univariate Hazard Ratio p-value
Age NS - NS
Sex NS - NS
Axial location .03 - NSTumor thickness <.0001 1.1 .04
Clark level > III .001 2.3 .01
Ulceration <.0001 3.3 <.0001
SLN status <.0001 6.5 <.0001
_____________________________________________________________________________
Several large single institution and multi-center databases provide consistent findings

8/12/2019 Melanoma Sentinel Node
http://slidepdf.com/reader/full/melanoma-sentinel-node 19/63
Disease-Specific Survival by
SLN Status
Morton DL, et al. N Engl J Med. 2006; 355: 1307-1317
Most powerful predictor of survival

8/12/2019 Melanoma Sentinel Node
http://slidepdf.com/reader/full/melanoma-sentinel-node 20/63
Does early treatment of lymph node
disease improve survival?

8/12/2019 Melanoma Sentinel Node
http://slidepdf.com/reader/full/melanoma-sentinel-node 21/63
Randomized Surgical Trials Comparing
ELND vs. Nodal Observation
Pt’s. Thickness Site
WHO Program
Trial #1 533 All Extremities
Trial #14 227 >1.5mm Trunk
Mayo Clinic 171 All Extremities
Trunk
Intergroup Melanoma Trial 737 1-4mm All
Not all patients benefit

8/12/2019 Melanoma Sentinel Node
http://slidepdf.com/reader/full/melanoma-sentinel-node 22/63
Long Term Results of ELND Trials
2 contemporary ELND trials with survival benefits for patients with
microscopic disease

8/12/2019 Melanoma Sentinel Node
http://slidepdf.com/reader/full/melanoma-sentinel-node 23/63
Survival According to Status of Regional Nodes
Cascinelli. Lancet 1998
German Retrospective Review

8/12/2019 Melanoma Sentinel Node
http://slidepdf.com/reader/full/melanoma-sentinel-node 24/63
German Retrospective Review
Impact of Sentinel Node Biopsy on Survival
for Node-Positive Patients
Kretschmer et al, Eur J Cancer . 2004; 212-218.
SLNE: Sentinel Lymph Node positive Elective node dissection
DLND: Delayed Lymph Node Dissection
8/12/2019 Melanoma Sentinel Node
http://slidepdf.com/reader/full/melanoma-sentinel-node 25/63
ELND Trial OutcomesConclusions
No overall survival benefit
Early dissection has no impact on the natural history of primary
melanoma
Incidence of node positive patients too low to adequately test the
hypothesis
Survival benefit observed in the node positive and other stratified
subgroups

8/12/2019 Melanoma Sentinel Node
http://slidepdf.com/reader/full/melanoma-sentinel-node 26/63
MSLT-I: Immediate vs. Delayed CLND
for Nodal MetastasesBiopsy-proven Melanoma > 1mm
Randomized
60% 40%
WEX + SNB WEX + Watch & Wait Observation
A: Comparison of al l randomized patients
SN(-) SN(+) Nodal
Recurrence
Observation Immediate CLND Delayed CLND
B: Comparison of randomized patients with
SN occult vs. palpable nodal metastases
Morton DL, et al. N Engl J Med. 2006; 355: 1307-1317

8/12/2019 Melanoma Sentinel Node
http://slidepdf.com/reader/full/melanoma-sentinel-node 27/63
MSLT-15-year Survival Benefit Estimates
Based on previous trial observations
WHO: 20% survival advantage in the microscopic node positive
German multi-center trial: 15% benefit in SLN positive group
Assuming 20% incidence of node positivity
Overall 3%-4% survival benefit
8/12/2019 Melanoma Sentinel Node
http://slidepdf.com/reader/full/melanoma-sentinel-node 28/63
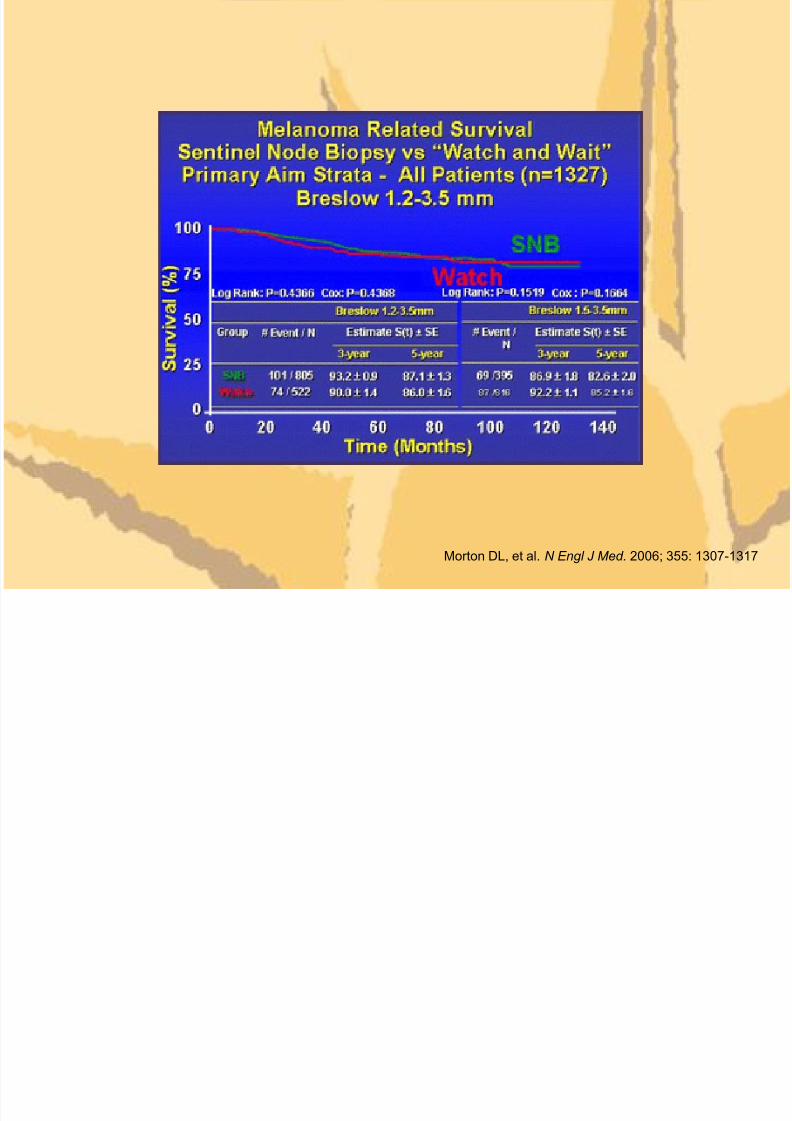
Morton DL, et al. N Engl J Med. 2006; 355: 1307-1317

8/12/2019 Melanoma Sentinel Node
http://slidepdf.com/reader/full/melanoma-sentinel-node 29/63
5-year disease-free survival 73.1% vs 78.3%, p=0.009
• Median follow-up 59.8 months
• 26.8% patients on observation arm with relapse at any
site
• 20.7% patients on sentinel node biopsy arm with
relapse at any site
Morton et al. N Engl J Med. 2006;355:1307
Impact of Sentinel Node Biopsy on
Relapse-Free Survival

8/12/2019 Melanoma Sentinel Node
http://slidepdf.com/reader/full/melanoma-sentinel-node 30/63
MSLT-I: Immediate vs. Delayed CLND
for Nodal MetastasesBiopsy-proven Melanoma > 1mm
Randomized
60% 40%
WEX + SNB WEX + Watch & Wait Observation
A: Comparison of al l randomized patients
SN(-) SN(+) Nodal
Recurrence
Observation Immediate CLND Delayed CLND
B: Comparison of randomized patients with
SN occult vs. palpable nodal metastases
Morton DL, et al. N Engl J Med. 2006; 355: 1307-1317

8/12/2019 Melanoma Sentinel Node
http://slidepdf.com/reader/full/melanoma-sentinel-node 31/63
Stage Progression to More Advanced Nodal Disease
Among “Watch and Wait” Patients vs. SNB
0
1
2
3
4
Rx
0%
10%
20%
30%
40%
50%
60%
70%
% S
N B ( + ) o r N o d a l R
e c u r .
M
e a n # P o s .
N o d e s
1.6
SNB
3.4
Watch
N1 N2 N3
> 4 Nodes
67%
41%
28%
32%
5%
27%
SNB
Watch
SNB
Watch
SNB
Watch
1 Node 2-3 Nodes
AJCC N Stage
P=0.0001

8/12/2019 Melanoma Sentinel Node
http://slidepdf.com/reader/full/melanoma-sentinel-node 32/63
Randomizat ion
SLNB OBS
P= 0.004multivariate model adjusted for known prognostic factors
+ - - +
Early TLND
72% 5-year survival
Delayed TLND
52% 5-year survival
MSLT-I: Impact of Sentinel Node Biopsy on
Survival for Node-Positive PatientsA ll 2001 Patien ts
Morton DL, et al. N Engl J Med. 2006; 355: 1307-1317

8/12/2019 Melanoma Sentinel Node
http://slidepdf.com/reader/full/melanoma-sentinel-node 33/63
MSLT-1 Node + SubgroupsReasons for Survival Differences
False positive SLN's
SLN group prognostically more favorable
Early dissection prevents regional progression and
distant dissemination

8/12/2019 Melanoma Sentinel Node
http://slidepdf.com/reader/full/melanoma-sentinel-node 34/63
False Positive SLN?

8/12/2019 Melanoma Sentinel Node
http://slidepdf.com/reader/full/melanoma-sentinel-node 35/63
Incidence of SN Metastases at SNB vs. Clinical Nodal
Recurrence following “Watch and Wait”
0.0%
10.0%
20.0%
30.0%
40.0%
1.2-3.5 >3.5 Overall
SNB
Watch
% N
o d e ( + ) o r N o d a
l R e c u r r e n c e
Breslow Thickness (mm)
P=0.8329
16.2 16.4
35.2 35.5
19.8 20.3

8/12/2019 Melanoma Sentinel Node
http://slidepdf.com/reader/full/melanoma-sentinel-node 36/63
Cumulative Incidence of Regional
Node Metastasis
Morton et al. N Engl J Med. 2007;356:418-421

8/12/2019 Melanoma Sentinel Node
http://slidepdf.com/reader/full/melanoma-sentinel-node 37/63
AJCC 2009 Stage III Changes
Concept of ITCs as node-negative disease [N0(i+)] no longer used
Scheri et al: 214 SLN+ patients, 57 had ITCs (≤ 0.2 mm) CLND 6 (12%) additional + nodes, 5-yr melanoma-specific survival LOWER
in ITC+ patients than SLN- patients (89% vs 94%, P =.02)
Akkooi et al: 388 SLN+ patients, 40 (10%) had metastases <0.1 mm 1 (3%) with additional + nodes, 5-yr OS 91% = to SLN- patients
Bottom line: It remains unclear whether ITCs in the regional
nodes are of clinical significance BUT, concept of “clinically insignificant nodal disease” unproven
Scheri RP et al. Ann Surg Oncol. 2007;14:2861-2866.
van Akkooi ACJ et al. Ann Surg. 2008;248:949-955.

8/12/2019 Melanoma Sentinel Node
http://slidepdf.com/reader/full/melanoma-sentinel-node 38/63
Microscopic metastases will become
Macroscopic

8/12/2019 Melanoma Sentinel Node
http://slidepdf.com/reader/full/melanoma-sentinel-node 39/63
Do the AJCC staging criteria apply to
patients with microscopic SLN tumor
burden?
R i d AJCC St i S t

8/12/2019 Melanoma Sentinel Node
http://slidepdf.com/reader/full/melanoma-sentinel-node 40/63
Revised AJCC Staging System
Stage III Changes
Independent Prognostic Factors
AJCC Cox Model – 1151 Stage III Patients
Variable Chi Square P-Value Risk Ratio
Number of (+) 57.6 <0.00001 1.26
Nodes
Tumor Burden 40.3 <0.00001 1.79
Ulcer + 23.3 <0.00001 1.58
6th Edition - 2002
Balch CM et al. J Clin Oncol. 2001; 19(16):3622-3634.

8/12/2019 Melanoma Sentinel Node
http://slidepdf.com/reader/full/melanoma-sentinel-node 41/63
Disease-Specific Survival Total # Positive NodesSLN Positive Patients Only
Gershenwald JE et al. WHO 6th World Congress on Melanoma; September 2005; Vancouver, BC.

8/12/2019 Melanoma Sentinel Node
http://slidepdf.com/reader/full/melanoma-sentinel-node 42/63
Disease-Specific Survival by Ulceration
SLN Positive Patients Only
Gershenwald et al, Ann Surg Oncol. 2000;7:160

8/12/2019 Melanoma Sentinel Node
http://slidepdf.com/reader/full/melanoma-sentinel-node 43/63
Di S ifi S i l b T B d

8/12/2019 Melanoma Sentinel Node
http://slidepdf.com/reader/full/melanoma-sentinel-node 44/63
Disease-Specific Survival by Tumor Burden
Largest Focus SLN-Positive Patients Only
Gershenwald JE et al. WHO 6th World Congress on Melanoma; September 2005; Vancouver, BC.

8/12/2019 Melanoma Sentinel Node
http://slidepdf.com/reader/full/melanoma-sentinel-node 45/63
Survival According to Tumor Burden in
SLN’s
Ross MI. New AJCC Recommendations for Melanoma Staging. Presented at: 33rd ESMO Congress Satellite
Symposium: Current Trends in Melanoma Management ; September 14, 2008; Stockholm, Sweden.

8/12/2019 Melanoma Sentinel Node
http://slidepdf.com/reader/full/melanoma-sentinel-node 46/63
Prognostic Factors Influencing DSS
SNL Positive Patients Only
Multiple covariate
Prognostic Factor Hazard Ratio p-value
Ulceration 2.04 .01
Total Positive Nodes
1 1.0 -
2 1.46 .25
3+ 2.10 .045
Largest SLN metastatic focus
< 2mm 1.0 -
>2 & < 8mm 2.51 .004
> 8mm 2.91 .01

8/12/2019 Melanoma Sentinel Node
http://slidepdf.com/reader/full/melanoma-sentinel-node 47/63
Copyright ©2004 American Cancer Society
From Balch, C. M. et al.
CA Cancer J Clin 2004;54:131-149.
Fifteen-year Survival Curves for the Stage Groupings of Patients with RegionalMetastatic Melanoma (Stage III)

8/12/2019 Melanoma Sentinel Node
http://slidepdf.com/reader/full/melanoma-sentinel-node 48/63
Completion Node Dissection for
Positive Sentinel Nodes:Is i t necessary?
Staging
Survival
Regional Control

8/12/2019 Melanoma Sentinel Node
http://slidepdf.com/reader/full/melanoma-sentinel-node 49/63
Regional Recurrence After Surgery
Alone
Regional
Reference Failure Rate
Fuhrmann,2001 28%
Kretschmer, 2001 34%Lee, 2000 30% Weighted average:
Shen, 2000 14%
Hughes, 2000 25% 692 failures/3350 patients=
Monsour, 1993 52%
Miller, 1992 12% 21%
O’Brien, 1991 24%
Calabro, 1989 17%
Bowsher, 1986 15%
Byers, 1986 16%

8/12/2019 Melanoma Sentinel Node
http://slidepdf.com/reader/full/melanoma-sentinel-node 50/63
Risk Factors for Regional Recurrence
After Surgery Alone
Regional
Characteristic Failure Rate References
Extracapsular extension 31% - 63% Lee, Calabro, Shen, Monsour
>4 involved lymph nodes 22% - 63% Lee, Calabro, Miller, Kretschmer
Lymph node >3 cm 42% - 80% Lee
Cervical ln location 33% - 50% Lee, Bowsher, Monsour
30% - 50% if high-risk features present

8/12/2019 Melanoma Sentinel Node
http://slidepdf.com/reader/full/melanoma-sentinel-node 51/63
In-Basin FailureSelective Lymphadenectomy vs. ELND
(Node Positive Only)
0
1
2
3
4
56
7
8
9
ELND SLN
Slingluff, 1994 MDACC Study, 2003
% N
o d a l F
a i l u r e

8/12/2019 Melanoma Sentinel Node
http://slidepdf.com/reader/full/melanoma-sentinel-node 52/63
Rational For Completion Dissection
Avoid the development of palpable nodal disease
- residual microscopic disease in non-sentinel nodes
Staging- total number of nodes involved prognostically relevant
- may influence recommendations for adjuvant therapy
Incidence of non-sentinel node involvement under-estimated
- based on routine pathologic techniques

8/12/2019 Melanoma Sentinel Node
http://slidepdf.com/reader/full/melanoma-sentinel-node 53/63
Reasons Against Routine Use of
Completion Dissections
Incidence of non-sentinel node involvement is only 10%-20%
- unnecessary cost and morbidity in patients without additional
microscopic disease
No proven survival benefit for node dissection
Incidence of nodal failure after SLN biopsy

8/12/2019 Melanoma Sentinel Node
http://slidepdf.com/reader/full/melanoma-sentinel-node 54/63
A selective approach to completion
dissection is rational.

8/12/2019 Melanoma Sentinel Node
http://slidepdf.com/reader/full/melanoma-sentinel-node 55/63
Recommendations
CLND for a positive SLN is the standard of care
Omission of CLND should only occur as part of a
clinical trial

8/12/2019 Melanoma Sentinel Node
http://slidepdf.com/reader/full/melanoma-sentinel-node 56/63
SLN BiopsyIndispensable Staging Procedure?
Effectively identifies microscopic disease/Promotes early node
dissection
survival benefit
optimizes regional control
Identifies patients who benefit most with adjuvant therapy
Facilitates careful pathologic scrutiny
Node negative patients spared toxicity
Critical prognostic information
Stratification criteria for clinical trials

8/12/2019 Melanoma Sentinel Node
http://slidepdf.com/reader/full/melanoma-sentinel-node 57/63
Candidates for SLN Biopsy
Incidence of Positive SLN:

8/12/2019 Melanoma Sentinel Node
http://slidepdf.com/reader/full/melanoma-sentinel-node 58/63
Incidence of Positive SLN:
AJCC Stage Grouping
0
10
20
30
40
50
60
P e r c e n t P o s i t i v e S L N
3.9%
11.4%
22.1%
35.3%
55.4%
Ia Ib IIa IIb IIc
AJCC Stage

8/12/2019 Melanoma Sentinel Node
http://slidepdf.com/reader/full/melanoma-sentinel-node 59/63
Melanoma Lymphatic MappingPreoperative Eligibility
Primary tumor criteria
> 1mm Breslow thickness
< 1mm MR: present (Ib)
Ulceration (Ib)
Clark Level IV/V Vertical growth phase?
Age?
After a wide excision?
Ambiguous diagnosis of melanocytic lesion?
Pure Desmoplastic melanoma?
National Comprehensive Cancer Network (NCCN) Clinical Practice Guidelines in Oncology for
Melanoma. V1.2010
Balch CM et al. J Clin Oncol. 2009;27(6):6199-6206.

8/12/2019 Melanoma Sentinel Node
http://slidepdf.com/reader/full/melanoma-sentinel-node 60/63
Who Should Undergo SLNB?
National Comprehensive Cancer Network, 2011 Consider SLNB for high risk Ia melanoma
Discuss and offer SLNB for stage Ib, stage II CM
SLNB important staging tool, but impact on overall survival
unclear
AJCC Recommendations Microstaging of all primary melanomas
Pathologic nodal staging for stage Ib-IIc
National Comprehensive Cancer Network Clinical Practice Guidelinesin Oncology Melanoma. V. 3.2011
AJCC Cancer Staging Manual, Seventh Edition (2010) publishedby Springer Science and Business Media LLC, www.springerlink.com.

8/12/2019 Melanoma Sentinel Node
http://slidepdf.com/reader/full/melanoma-sentinel-node 61/63
SLN Biopsy
Standard of Care?
Discuss with patients:
accuracy of SLN biopsy
predicted risk for microscopic nodal disease
potential risks and benefits
how the information will impact therapy
Currently offered as standard of care for patientswith Ib-IIc and selectively for Ia.

8/12/2019 Melanoma Sentinel Node
http://slidepdf.com/reader/full/melanoma-sentinel-node 62/63
Thank You

8/12/2019 Melanoma Sentinel Node
http://slidepdf.com/reader/full/melanoma-sentinel-node 63/63