Embed Size (px)
Citation preview

Nephritic Edema
By Neil A. Kurtzman
Nephritic edema results from the primary retention of salt. Acute glomerulonephritis is the prototypical form of the
disorder. The stimulus for the salt retention arises within the kidney by an unknown mechanism, As effective
arterial blood volume (EABV) was normal at the start of the disease process, it becomes expanded as salt and
water are added to it. The pathophysiological sequelae of this process are compared with ihose which follow the
salt retention of congestive heart failure {CHF), The latter is a syndrome in which salt retention is secondary, driven
by the contraction of EABV which is at the heart of CHF. Finally, mechanisms responsible for the salt retention of
nephrosis are considered. lt is possible, and even likely, that most patients with nephrotic edema have primary salt
retention, rather than secondary edema. lf this view is correct, salt is retained not because of urinary protein loss
and its consequent hypoalbuminemia, but rather because of the glomerulopathy which caused the syndrome in the
first place.Copyright @ 2001 by W.B. Saunders Company
rFHg TOPIC OF this review is something of a
I ooo. relation. The most recent edition (the
sixthj of Brenner and Rector's The Kidney does not
mention it in its chapter on edema and barely refers
to it in the chapter on glomeruionephritis. The
reasons for this snub are not immediately apparent,
but may be symptomatic of the decline of organ
physiology in the age of exons, to the antiquity of
much of the relevant work on the subject, to the
infrequency of nephritrc edema's occurerce in the
developed world, and to simple inadvertence,
The edema of renal disease has long been clas-
sified into 2 types, nephritic and nephrotic. The
former exemplihed by salt-retaining glomerulone-
phritis, the latter typically attributed to the hy-
poalbuminemia characteristic of the nephrotic syn-
drome. In this article I will compare the features of
nephritic edema to those seen in congestive heart
failure (CHF). I will then consider in which cate-
gory to place the patient with nbphrotic syndrome.
The edema of heart, kidney, and liver disease is
the result of renal salt retention. The failure of a
normal tadney to excrete appropriate amounts of
sait in patients with CHF and cirrhosis has in-
trigued clinicians and renal physiologists for more
than half a century. Petersr reasoned that CHF
must induce volume contraction and introduced the
concept of effective arterial blood volume (EABV)
into the clinical consciousness. He proposed that
EABV was contracted in CHF and that the relent-
less salt retention so often a feature of that malady
was an appropriate, although maladaptive, re-
sponse by the kidney. In other words, the kidney
was a dumb beast just carrying out orders -
volume contracted, salt retained. A mechanrsm
useful when absolute volume was diminished
could cause lethal edema when the heart failed'
EABV is not a measurable entity. Its state must
be infened. It does not necessarily correiate with
blood volume, extracelluar volume, or interstitial
volume. Failure to distinguish between effective
and absoiute volume has caused much medical
mischief. For example, finding an increased total
blood volume in patients with advanced liver dis-
ease tells us nothing about their EABVs.2 Table 1
lists some of the features of patients with a con-
tracted EABV. The essence of a contracted EABV
is arterial underfilling that results in impaired or-
gan perfusion. If the patient has dianhea, his total
blood volume is likely decreased; if organ isch-
emia is secondary to CHF, the patient wiil proba-
bly have an increase in total blood volume al-
though EABV is contracted. The kidney responds
to voiume contraction by increasing reabsorption
and reieasing renin, hence reduced salt excretion, a
high urea to creatinine ratio, decreased urate ex-
cretion, and secondary hyperaldosteronism charac-
teristic of states of both absolute and effective
volume contraction. Vasopressin release also in-
creases because it too is sensitive to volume.
Expansion of EABV will have opposite effects.
The markers of volume will be oppositely ex-
pressed. The urea to creatinine ratio will fall' Like-
wise, renin, aldosterone, and vasopressin will de-
crease. The blood pressure which decreases when
volume is contracted may rise to life-threatening
From the Department of Internal Medicine, Texas Tech Uni'
versity Health Sciences Center,
Lubbock, TX.
Addres,s reprint requests to NeiI A Kurtzman, MD, University
Distinguished Professor, Department of Internal Medicine,
Texas Tech University Health Sciences Center, 3601 4'h Street'
Lubbock TX 79430.
Copyright @ 2001 by W.B. Saunders Company
027 0 -929 5 /0 I /2 I 0 3 - 0007 $3 5. 00/0
doi : 1 0. 1 0 5 j/snep.200 1. 2 1 6 5 3
Semlnars in Nephrology, Vol 21, No 3 (May)' 2001:pp 257-261 257
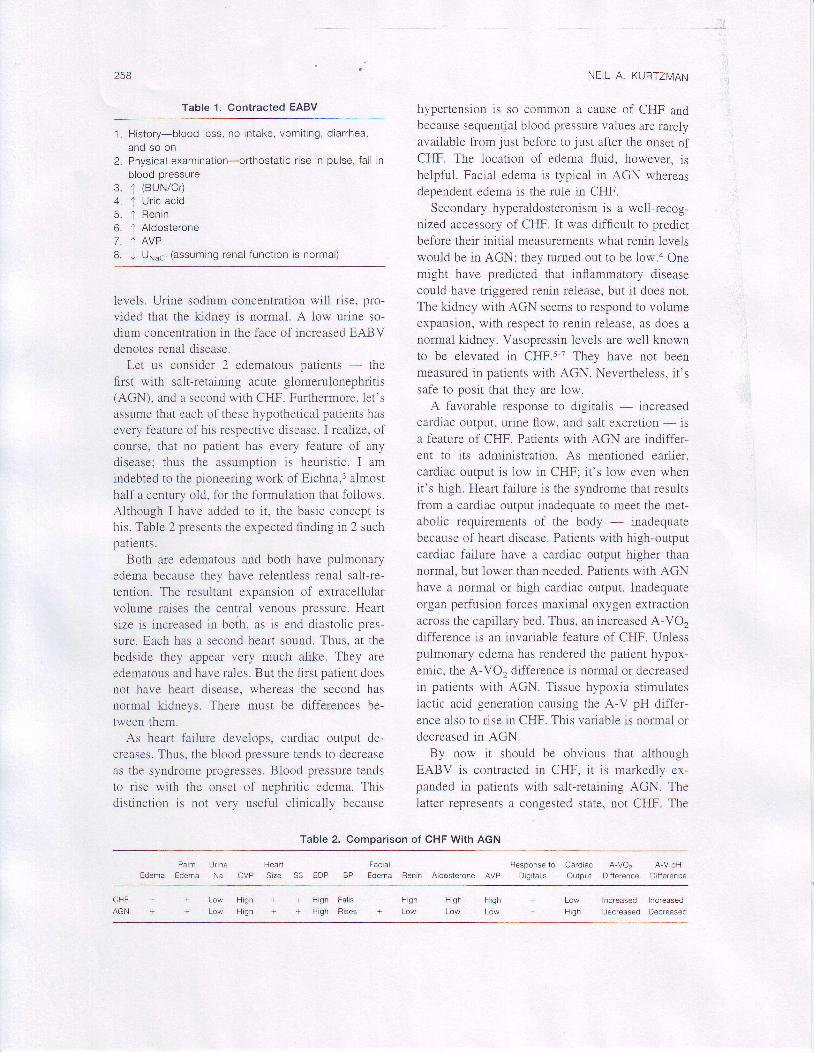
Table 1. Contracted EABV
1. History-blood loss, no intake, vomit ing, diarrhea,and so on
2. Physical examination-orlhostat ic r ise in pulse, fal l inblood pressure
3. t (BUN/Cr)4. ' l Uric acid5 . I Ren in6. J Aldosterone7. t AVPB. J Unrucr (assuming renal function is normal)
levels. Urine sodium concentration will rise, pro-vided that the krdney is normal. A low urine so-dium concentration in the face of increased EABVdenotes renal disease.
Let us consider 2 edematous patients - thefirst with salt-retaining acute glomeruionephritis(AGN), and a second with CHF. Furthermore, let'sassume that each of these hypothetical patients hasevery feature of his respective disease. I realize, ofcourse, that no patient has every feature of anydisease; thus the assumption is heuristic. I amindebted to the pioneering work of Eichna,3 aimosthalf a century old, for the formulation that follows.Although I have added to it, the basic concept ishis. Table 2 presents the expected finding in 2 suchpatients.
Both are edematous and both have pulmonaryedema because they have relentless renal salt-re-tention. The resultant expansion of extracellularvolume raises the central venous Dressure. Heartsize is increased in boih. as is eni diastolic pres-sure. Each has a second heart sound. Thus, at thebedside they appear very much alike. They areedematous and have rales. But the iirst patient doesnot have heart disease, whereas the second hasuormal kidneys. There must be differences be-tween them.
As heart failure develops, cardiac output de-creases. Thus, the blood pressure tends to decreaseas the syndrome progresses. Blood pressure tendsto rise with the onset of nephritic edema. Thisdistinction is not very useful clinically because
NEIL A. KURTZMAN
hypertension is so common a cause of CHF andbecause sequentjal blood pressure values are rareiyavailable from just before to just after the onset ofCHF. The location of edema fluid, however, ishelpful. Faciai edema is typical in AGN whereasdependent edema is the rule in CHF.
Secondary hyperaldosteronism is a well-recog-nized accessory of CHF. It was difficult to predictbefore their initiai measurements what renin levelswould be in AGN; they turned out to be low.a Onemight have predicted that inflammatory diseasecould have triggered renin release, but it does not.The ledney with AGN seems to respond to volumeexpansion, with respect to renin release, as does anormal ladney. Vasopressin levels are well knownto be eievated in CHF.5-7 They have not beenmeasured in patients with AGN. Nevertheless, it'ssafe to posit that they are low.
A favorable response to digitalis - increasedcardiac output, urine flow, and salt excretion - rsa feature of CHF. Patients with AGN are indiffer-ent to its administration. As mentioned earlier,cardiac output is low in CHF; it's low even whenit's high, Heart failure is the syndrome that resultsliom a cardiac outpllt inadequate to meet the met-abolic requirements of the body - inadequatebecause of heart disease. Patients with high-oLrtputcardiac failure have a cardiac output higher thannormal, but lower than needed. Patients with AGNhave a normal or high cardiac output. Inadequateorgan perfusion fbrces maximal oxygen extractronacross the capillary bed. Thus, an increased A-VO2difference is an invariable I'eature of CHF. Unlesspulmonary edema has rendered the patient hypox-emic, the A-VO2 difference is norrnal or decreasedin patients with AGN. Tissue hypoxia stimulateslactic acid generation causing the A-V pH diifer-ence also to rise in CHF. This variable is normal ordecreased in AGN.
By now it should be obvious that althoughEABV is contracted in CHF, it is markedly ex-panded in patients with salt-retaining AGN. Thelatter represents a congested state, not CHF. The
Table 2. Comparison of CHF With AGN
PalmEdema Edema
Heart
Size 53 EDP
un neNa CVP
Faclal
BP Edema Renin Aldosterone AVP
Response lo Cardiac A-VO2 A-V pHDigitalis Output Diiference Difference
Low IncreasedH i d h n a . / a . c A d
tncreaseo
Decreased
H i q h H i g h H i g h- Low Low Low
+ + L o w H i g h + + H i g h+ + L o w H i g h + + H i g h
FallsRises
C H F
AGN
NEPHRITIC EDEMA
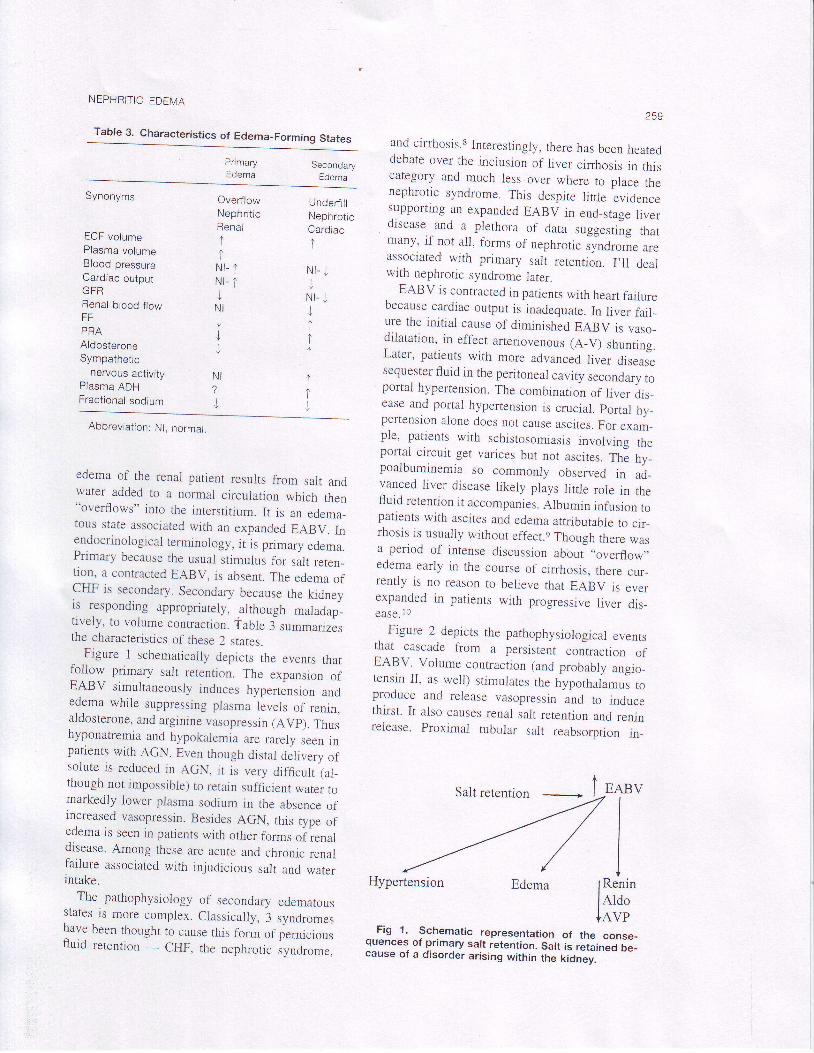
Table 3. Characteristics of Edema_Forming States
259
and cirrhosis.8 Interestingly, there has been heateddebate over the inclusion of liver cinhosis rn thiscategory and much less over where to place thenephrotic syndrome. This despite little evidencesupporring an expanded EABV in end_stage liverdisease and a plethora of data suggesd;g thatmany, if not ail, forms of nephrotic ,yna.o*. ur.associated with primary salt retention. I,ll deatwith nephrotic syndrome later.
EABV is contracted in patients with heart failurebecause cardiac output is inadequate In liver farl-ure the initial cause of diminished EABV is vaso_dilatation, in effect arteriovenous (A_V) shuntrng.Later, patients with more advanced liver diseasesequester ffuid in the peritoneal cavity secondary toportal hypertension. The combination of liver dis_ease and portal hypertension is crucial. portal hy_pertension alone does nor cause ascrtes. For exam_ple, patients with schistosomiasis involving theportai circuit get varices but not ascites. fh-e fry_poalbuminemia so commonly observed in ad_vanced liver disease likely plays little role in thefluid retention it accompanies. Albumin infusion ropatients with ascites and edema attributable to cir_rhosis is usualiy without effect.e Though there wasa period of intense discussion abbui ,,overflow,,edema early in the course of cirrhosis, there cur_rently is no reason to believe that EABV is everexpanded in patients with progressive liver dis_ease.1o
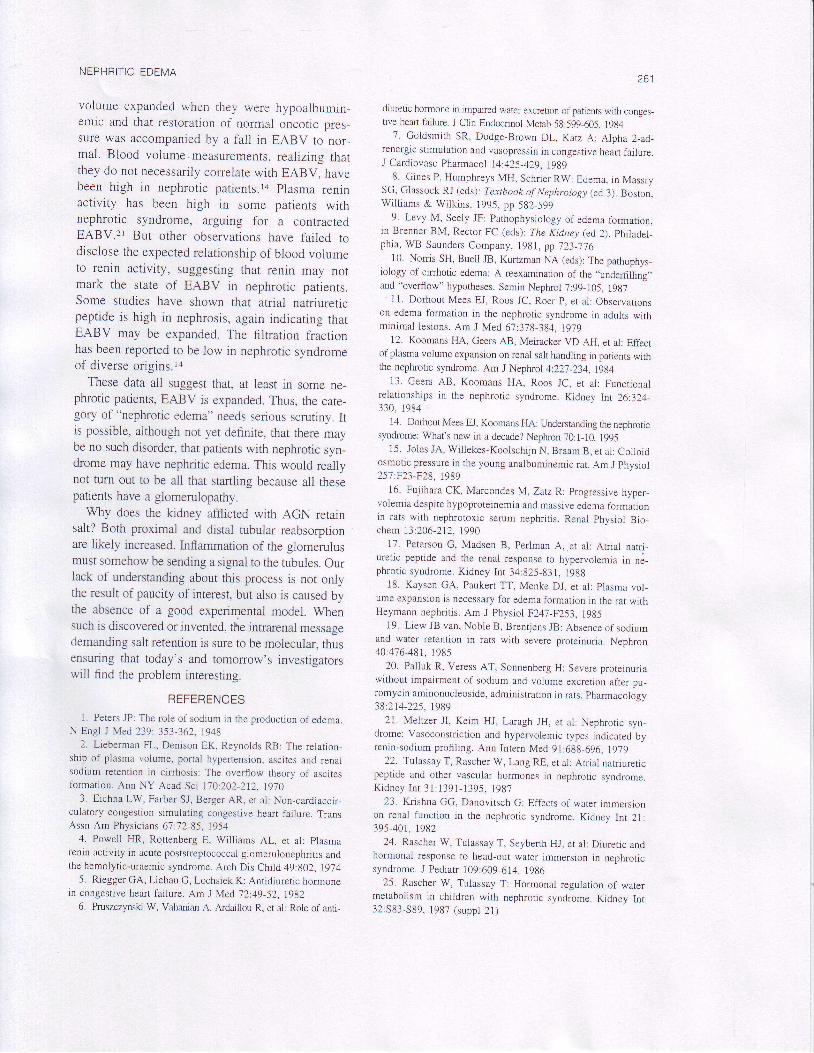
_ Figure 2 depicts the pathophysiological events
that cascade from a perslstent contraction ofEABV. Volume contracrion (and probably angro_tensin II, as well) srimuiares the hypothaia.u, toproduce and release vasopressin and to inducethirst. It also causes renal salt retention and renrnrelease. Proximal tubular sait reabsorption in_
PrimaryEdema
SecondaryEdema
Synonyms
ECF volumePlasma volumeBlood pressureCardiac outputGFRRenal blood f lowFFPRAAldosteroneSympathetic
nervous activityPlasma ADHFractional sodium
OverflowNephrit icRenal
tINr- 1Nl- tjN IJJJ
Underf i l lNephroticCardiac
1
N I - JI
N I - JJItt
1It
NI1
J
Abbreviation: Nl, normal.
edema of the renai patient results from salt andwater added to a normal circulation which then"overflows" into the interstitium. It is an edema_tous state associated with an expanded EABV. Inendocrinological terminology, it is primary edema.Primary because the usual stimuiui for salt reten_tion, a contracted EABV, is absent. The edema ofCHF is secondary. Secondary because the kidneyis responding appropriately, although maiadap_tively, to volume conracrion. table isummarrzesthe characteristics of these 2 states.
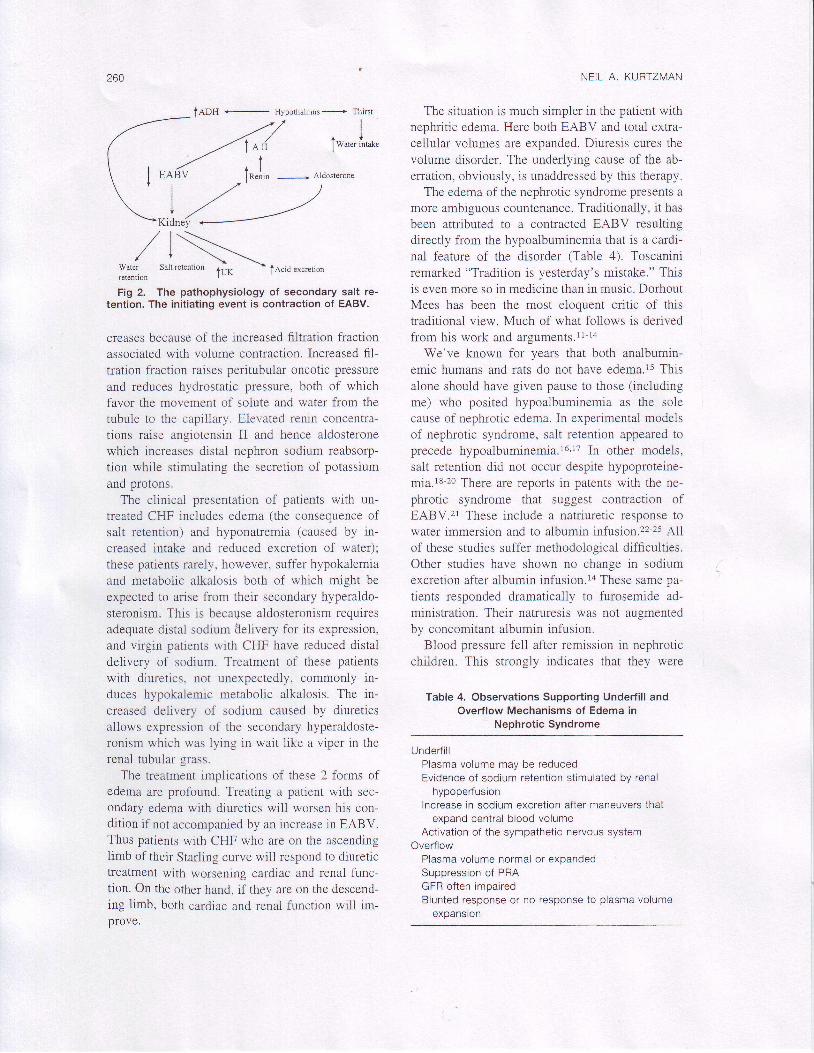
Figure I schematically depicts the evenrs thatfoliow primary salt retention. The expansion ofEABV simultaneously induces hypertension andedema whiie suppressing plasma levels of renrn,aldosterone, and arginine vasopressin (AVp). Thushyponatremia and hypokalemia are rarely seen inpatienrs with AGN. Even though disral d;Uvery ofsolute is reduced in AGN, it is very difficutt (al-though not impossible) to retain sufficient water romarkedly lower plasma sodium in the absence ofincreased vasopressin. Besides AGN, this type ofedema is seen in parients with other fbrms oi renatdisease. Among these are acute and chronic renalfailure associated with injudicious salt and waterintake.
The pathophysiology of secondary edematousstates is more complex. Classically, 3 syndromesnave been thought to cause this form of perniciousfluid retention - CHF, the nephrotic syndrome,
Saltretention - I
Hypertension Edema
I_
Fig 1. Schematic representation of the conse_quences of primary salt retention. Satt is reta;nJ Oe_cause of a disorder arising within the kiOnly.
EABV,TIII
ReninAldoAVP
tADH
260
,/ | -'---'--/ | \-.--,-
r' i \ --r._
Water Salt rerenrion tUf
- tA.id .*.r.non
retenllon
Fig 2. The pathophysiology of secondary salt re-tention. The initiating event is contraction of EABV.
creases because of the increased filtration fractronassociated with volume contraction. Increased fil-tration fraction raises peritubular oncotic pressure
and reduces hydrostatic pressure, both of whichfavor the movement of solute and water from thetubule to the capillary. Elevated renin concentra-tions raise angiotensin II and hence aldosteronewhich increases distal nephron sodium reabsorp-tion while stimulating the secretion of potassiumand protons.
The clinical presentation of patients with un-treated CHF includes edema (the consequence ofsalt retention) and hyponatremia (caused by in-creased intake and reduced excretion of water);these patients rarely. however, suffer hypokalemiaand metabolic alkalosis both of which might beexpected to arise from their secondary hyperaldo-steronism. This is because aldosteronism requiresadequate distal sodium Selivery for its expression,and virgin patients with CHF have reduced distaldelivery of sodium. Treatment of chese patientswith diuretics. not unexpectedly, commonly in-duces hypokalemic metabolic alkalosis. The in-creased delivery of sodium caused by diureticsallows expression of the secondary hyperaldoste-ronism which was lying in wait like a viper in therenal tubular grass.
The treatment implications of these 2 forms ofedema are profound. Treating a patient with sec-ondary edema with diuretics will worsen his con-dition if not accompanied by an increase in EABV.Thus patients with CHF who are on the ascendingiimb of their Starling curve will respond to diuretictreatment with worsening cardiac and renal func-tion. On the other hand, if they are on the descend-ing limb, both cardiac and renal function will im-Drove.
NEIL A, KURTZMAN
The situation is much simpler in the patient withnephritic edema. Here both EABV and total extra-cellular volumes are expanded. Djuresis cures thevolume disorder. The underlying cause of the ab-erration, obviously, is unaddressed by this therapy.
The edema of the nephrotic syndrome presents amore ambiguous countenance. Traditionally, it hasbeen attributed to a contracted EABV resultingdirectly from the hypoalbuminemia that is a cardi-nal f'eature of the disorder (Table 4). Toscaniniremarked "Tradition is yesterday's mistake." Thisis even more so in medicine than in music. DorhoutMees has been the most eloquent critic of thistraditional view. Much of what follows is derivedfrom his work and arguments.lr-14
We've known for years that both analbumin-emic humans and rats do not have edema.rs Thisalone should have given pause to those (including
me) who posited hypoalbuminemia as the solecause of nephrotic edema. In experimental modelsof nephrotic syndrome, salt retention appeared toprecede hypoaibumrnemia.l6,rT In other models,salt retention did not occur despite hypoproteine-mia.18-20 There are reports in patents with the ne-phrotic syndrome that suggest contraction ofEABV.2l These include a natriuretic response towater immersion and to albumin infusion.z2-25 Allof these studies suffer methodological difficulties.Other studies have shown no change in sodiumexcretion after albumin infusion.la These same pa-tients responded drarnatically to furosemide ad-ministration. Their natruresis was not augmentedby concomitant aibumin infusion.
Blood pressure feil after remission in nephroticchildren. This strongly indicates that they were
Table 4. Observations Supporting Underfill andOverflow Mechanisms of Edema in
Nephrotic Syndrome
Undedil lPlasma volume may be reducedEvidence of sodium retention stimulated by renal
hypoperfusionIncrease in sodium excretion after maneuvers that
expand central blood volumeActivation of the sympathetic nervous system
OverflowPlasma volume normal or expandedSuppression of PRAGFR often impairedBlunted response or no response to plasma volume
expansion
-,L"2
NEPHRITIC EDEMA
volume expanded when they were hypoalbumin-emic and that restoration of normal oncotic pres-sure was accompanied by a fall in EABV to nor_mal. Blood volume measurements, realizing thatthey do not necessarily correlate with EABV, havebeen high in nephrotic patients.la plasma renrnactivity has been high in some patients withnephrotic syndrome, arguing for a contractedEABV.2l But other observations have failed todisclose the expected relationship of blood volumeto renin activity, suggesting that renin may notmark the srate of EABV in nephrotic patients.Some studies have shown that atrial natriuretrcpeptide is high in nephrosis, again indicating thatEABV may be expanded. The filtration fractionhas been reported to be low in nephrotic svndromeof diverse origins.ra
These data all suggest that, at least in some ne-phrotic patients, EABV is expanded. Thus, the cate-gory of "nephrotic edema" needs serious scrutiny. Itis possible, although not yet definite, that there maybe no such disorder, that patients with nephrotic syn-drome may have nephritic edema. This would reallynot turn out to be all that startling because all thesepatients have a glomerulopathy.
Why does the kidney afflicted with AGN retarnsalt? Both proximal and distal tubular reabsorptionare likely increased. Inflammation of the glomerulusmust somehow be sending a signal to the fubules. Ourlack of understanding about this process is not onlythe result of pauciry of interest, but also is caused bythe absence of a good experimental model. Whensuch is discovered or invented, the intrarenal messagedemanding salt retention is sure to be molecular, thusensuring that today's and tomorrow's investigatorswill find the problem interesting.
REFERENCES
l. Peters JP: The role of sodium in the productlon of edema.N Engl J Med239:353-362,1948
2. Lieberman FL, Denison EK, Reynolds RB: The relation-ship of plasma volume, portal hypertension, ascites and renalsodium retention in cirrhosis: The overflow theory of ascitesformation. Ann NY Acad Sci 1'10:202-212, l9i0
3. Eichna LW, Farber SJ, Berger AR, et al: Non-cardiaccir-culatory congestion simulating congestive heart failure. TransAssn Am Physicians 6'7:'12-85, 1954
4. Poweil HR, Rottenberg E, Williams AL, et al: plasma
renin activity in acute poststreptococcal glomerulonephritis andthe hemolytic-uraemic syndrome. Arch Drs Child 49:802, 1974
5. Riegger GA, Liebau G, Lochsiek K: Anridiuretic hormonetn congestive heart taiiure. Am J Med 72:49-52, l9B2
6. Pruszczynski W, Vahanian A, Ardaillou R, et al: Role of antr-
z o l
druretic hormone in impated water excretion of patients with conges_rive hean tallure. J Clin Endocrinol Metab 5g:599-605, 19g4
7. Goldsmrrh SR, Dodge-Brown DL, Katz A: Alpha 2_ad-renergic stimulation and vasopressin in congestive heart tailure.J Cardiovasc Pharmacol 14:425-429, l9g9
8. Gines P, Humphreys MH, Schrier RW: Edema, in MassrySC, Glassock RJ (eds): Textbook of NephroLogy (ed 3). Boston,Wi l l iams & Wi lk ins, 1995, pp 582-599
9. Levy M, Seely JF: Pathophysiology of edema tbrmatron,in Brenner BM, Rector FC (eds): The Ki&tey (ed 2). philadet-phia, WB Saunders Company, 1981, pp j23- j . /6
10. Norris SH, Buell JB, Kurtzman NA (eds): The pathopnys-iology of crnhotic edema: A reexamrnarion of the ,,underfilling,'
and "overflow" hypotheses. Semin Nephrol 7:99-105, l9g711. Dorhout Mees EJ, Roos JC, Roer p, et al: Observations
on edema fbrmation rn the nephrotic syndrome in adults wrthminimal lesions. Am J Med 67:378-384. lgig
12. Koomans HA, Geers AB, Meiracker VD AH, et al: Effectof plasma volume exparsion on renal salt handling in patients withthe nephrotrc synfuome. Am J Neptuol 4:22'l-234, I9g4
13. Geers AB, Koomans HA, Roos JC, et al: Functionalrelationships in the nephrotrc syndrome. Kidney Int 26:324_330, 1984
1 4. Dorhout Mees EI, Koomans FIA: Understandrng the nephrotrcsyndrome: What's new n a decade? Nephron 70:l-10, 1995
15. Joles JA, Willekes-Koolschijn N, Braan B, et al: Colloidosmotic pressure in the young analbuminemic rat. Am J phvsiol257:F23-F28, 1989
16. Fujihara CK, Marcondes M, Zatz R: progressive hyper_volemia despite hypoproteinemia and massive edema format.ionin rats wirh nephrotoxic serum nephritis. Renal physiol Bio_chem 13:206-212, 1990
17. Peterson C, Madsen B, Perlman A,.et al: Atrial natri_uretic peptide and the renal response to hypervolemia in ne_phrot ic syndrome. Kidney Int 34:825-83i , 19gg
18. Kaysen GA, Paukert TT, Menke DJ, et al: plasma vol-ume expansion is necessary for edema lbrmatron in the rat withHeymann nephritis. Am J Physiol FZ47-F253, Igg5
19. Liew JB van, Noble B, Brentjens JB: Absence of sodiumand water retention in rats with severe proteinuria. Nephron40 :476 -481 , I 985
20, Palluk R, Veress AT, Sonnenberg H: Severe proteinuriawithout impairment of sodium and volume excretion after pu_romycin aminonucleoside, administration in rats, pharmacolosv
38:214-225.198921. Meltzer JI, Keim HJ, Laragh JH, et al: Nephrotic syn-
drome: Vasoconstriction and hypervolemic types indicated byrenin-sodium proflling. Ann Inrern Med 91:688-696, 1979
22. Tulassay T, Rascher W, Lang RE, et al: Atrial natriureticpeptide and other vascular hormones in nephrotic syndrome.K idney I n t 31 :1391 -1395 , 1987
23. Krishna GG, Danovitsch G: Effects of warer immersionon renal function in the nephrotic syndrome. Kidney Int 21:395-40t, 1982
24. Rascher W, Tulassay T, Seyberth HJ, et al: Diuretic andhormonal response to head-out water immersion in nephroticsyndrome. J Pediaf 109:609-614. 1986
25. Rascher W, Tulassay T: Hormonal reguiation of watermetabolism in chiidren with nephrotic syndrome. Kidney Int32:S83-S89, 1987 (suppt 21)