-
7/28/2019 NEPHRITIC/NEPHROTIC SYNDROME.
1/37
NEPHRITIC/NEPHROTICSYNDROMESBY
DR. SAMUEL.N UWAEZUOKE,MB;BS. FWACP (Paed), Dip Th.
SENIOR LECTURER/CONSULTANTPAEDIATRICIAN
-
7/28/2019 NEPHRITIC/NEPHROTIC SYNDROME.
2/37
OUTLINE
GENERAL CONSIDERATIONS
DEFINITION
AETIOLOGY
CLINICAL FEATURES
LABORATORY EVALUATION
TREATMENT
DIFFERENTIAL DIAGNOSIS
PROGNOSIS
-
7/28/2019 NEPHRITIC/NEPHROTIC SYNDROME.
3/37
NEPHRITIC SYNDROME
-SYNONYMS INCLUDE
ACUTE GLOMERULONEPHRITIS
ACUTE NEPHRITIS
ACUTE NEPHRITIC SYNDROME
-
7/28/2019 NEPHRITIC/NEPHROTIC SYNDROME.
4/37
GENERAL CONSIDERATIONS
EACH KIDNEY HAS ABOUT ONE MILLIONNEPHRONS- THE FUNCTIONAL
UNIT
THE NEPHRON RECEIVES BLOOD THROUGHTHE AFFERENT ARTERIOLE
THE AFFERENT ARTERIOLE FORMS THECAPILLARY TUFTS OR
GLOMERULUS-
REUNITE TO FORM THE EFFERENT ARTERIOLE
-
7/28/2019 NEPHRITIC/NEPHROTIC SYNDROME.
5/37
GENERAL CONSIDERATIONS
THE MAJOR ELEMENTS OF RENALFUNCTION INCLUDE GLOMERULAR
ULTRAFILTRATION, TUBULAR REABSORPTIONAND TUBULAR SECRETION
GLOMERULAR CAPILLARY HYDROSTATICPRESSURE GENERATES AN ALMOST
PROTEIN-FREE FILTRATE OF PLASMA INTOTHE BOWMANS CAPSULE
-
7/28/2019 NEPHRITIC/NEPHROTIC SYNDROME.
6/37
GENERAL CONSIDERATIONS
GLOMERULAR FILTRATION RATE(GFR) ISMAINLY DETERMINED BY THE
RELATIVE
DEGREE OF CONSTRICTION OF AFFERENTAND EFFERENT ARTERIOLE
ANGIOTENSIN II CAUSES A PREFRENTIALCONSTRICTION OF EFFERENT
ARTERIOLE
RAISING THE GLOMERULAR CAPILLARYPRESSURE AND INCREASE IN
GFR.
-
7/28/2019 NEPHRITIC/NEPHROTIC SYNDROME.
7/37
DEFINTION
-A RENAL PATHOLOGY CHARACTERIZED BYABRUPT ONSET OF
HAEMATURIA(VARIABLE DEGREES)OEDEMA
HYPERTENSION
OLIGURIA
-FOLLOWING INFECTION WITH A VARIETY OFORGANISMS ESPECIALLY
BETA-HAEMOLYTICSTREPTOCOCCI
-
7/28/2019 NEPHRITIC/NEPHROTIC SYNDROME.
8/37
Aetiology of acute nephriticsyndrome
POST INFECTIOUS
Streptococci, staphylococci ,treponemapallidum, salmonella
typhi, leptospirosis.
Plasmodium malariae, toxoplasma.
Hepatitis B and C , cytomegalovirus,parvovirus, Ebstein Barr
virus
Infections of shunts, prostheses, bacterialendocarditis
-
7/28/2019 NEPHRITIC/NEPHROTIC SYNDROME.
9/37
Aetiology of acute nephriticsyndrome
SYSTEMIC VASCULITIS
Henoch Schonlein purpura, Systemic lupus
erythematosusMicroscopic polyarteritis, Wegeners
granulomatosis
OTHERS
Membranoproliferative glomerulonephritis Ig A nephropathy
Acute interstitial nephritis
-
7/28/2019 NEPHRITIC/NEPHROTIC SYNDROME.
10/37
PATHOGENESIS
-POST STREPTOCOCCAL ACUTEGLOMERULONEPHRITIS ( PSGN )
AS THE PROTOTYPE OF AGN REMAINS THE COMMONEST CAUSE IN
DEVELOPING COUNTRIES
OFTEN FOLLOWS PHARYNGITIS, IMPETIGO
OR RARELY A MIDDLE EAR INFECTIONCAUSED BY GROUP A
BETA-HEMOLYTICSTREPTOCOCCI
-
7/28/2019 NEPHRITIC/NEPHROTIC SYNDROME.
11/37
PATHOGENESIS The nephritogenic strains of streptococci are
capable of producing AGN
These include several protein M-types such as4,12,25 and 49
Host factors, genetically determined, areimportant in the
formation of antibodies tostreptococcal antigens
Glomerular injury in PSGN results fromdeposition of immune
complexes in theglomerular capillaries
-
7/28/2019 NEPHRITIC/NEPHROTIC SYNDROME.
12/37
PATHOGENESIS Nephritogenic antigens derived from
streptococci may bind directly to sub-
epithelial glomerular sites Antibodies formed against these
antigens
combine(immune complexes) and result in aninflammatory
response
Activation of complement, infiltration of
neutrophils, proliferation of glomerular cellsand expansion of
mesangial matrixfollow(glomerular injury).
-
7/28/2019 NEPHRITIC/NEPHROTIC SYNDROME.
13/37
CLINICAL FEATURES
History of sore throat or pyoderma(impetigenous lesions) is
noted in most
cases Latent period in the history of sore throat is
7 to 14 days while that of pyoderma is 2 to4 weeks
Peak age incidence : 5 to 12 years. Rarebelow the age of 3
years
A male preponderance is reported
-
7/28/2019 NEPHRITIC/NEPHROTIC SYNDROME.
14/37
CLINICAL FEATURES
Gross hematuria and mild facial edemaare the most common
presenting features
Urine usually cola coloured or reddishbrown
Oliguria ( less than 0.5ml-1ml/kg/hour )orsometimes anuria
Hypertension(from volume overload) maylead to headache
-
7/28/2019 NEPHRITIC/NEPHROTIC SYNDROME.
15/37
CLINICAL FEATURES
Atypical presentations (complications ofAGN) include
- Acute pulmonary edema
- Hypertensive encephalopathy(even atcomparatively lower BP
levels)
- Acute renal failure
- Nephrotic syndrome( so-called nephriticnephrotic syndrome)
-
7/28/2019 NEPHRITIC/NEPHROTIC SYNDROME.
16/37
LABORATORY INVESTIGATIONS
Urinalysis- mild proteinuria
Urine microscopy- dysmorphic red cells,
red cell casts, and neutrophils. Hyalineand granular casts may
also be seen.
Serum electrolyte, urea and creatinine-elevated urea/creatinine,
hyperkalemia,metabolic acidosis( in patients with ARF ).
Hematology- anemia due tohemodilution
-
7/28/2019 NEPHRITIC/NEPHROTIC SYNDROME.
17/37
LABORATORY INVESTIGATIONS
Imaging study(Chest X-ray)- may showcardiomegaly and pulmonary
congestion
Serology ( ASO titre and C3 levels)-elevated ASO titre within 3
to 5 weeksafter streptococcal infection, anddecreased serum C3
levels
Renal biopsy- not required in typical casesbut indicated under
special conditions
-
7/28/2019 NEPHRITIC/NEPHROTIC SYNDROME.
18/37
Indications for renal biopsy inAGN
Associated systemic features like fever, rash,joint pain, heart
disease.
Normal ASO titre and C3 levels Mixed picture of AGN and
Nephrotic
syndrome
Delayed cases of resolution
-oliguria, hypertension and/or azotemia beyond
2 weeks, gross hematuria past 3-4 weeks, lowC3 levels past 6-8
weeks and microscopichematuria/proteinuria beyond 6-12 months
-
7/28/2019 NEPHRITIC/NEPHROTIC SYNDROME.
19/37
TREATMENT
GENERAL MEASURES
- Fluid balance : strict input/output if oliguria is
present, daily weight measurement.- Diet : restriction of sodium
intake in all children
with edema or hypertension, restriction of
foods high in potassium until oliguria resolves
- Bed rest: if hypertension, edema or cardiacfailure are
present
-
7/28/2019 NEPHRITIC/NEPHROTIC SYNDROME.
20/37
TREATMENT
Drug treatment:
- Eradication of streptococcal infections
using penicillin or alternativelyerythromycin.
- Intravenous furosemide(1mg/kg) foredema and circulatory
congestion
- For hypertension, the use of vasodilators(hydralazine,
nifedipine, ACEI) may beeffective
-
7/28/2019 NEPHRITIC/NEPHROTIC SYNDROME.
21/37
DIFFERENTIAL DIAGNOSIS
Acute interstitial nephritis
Shunt nephritis
Nephritis in SBE
Glomerulonephritis associated withhepatitis B or C
Ig A nephropathy
-
7/28/2019 NEPHRITIC/NEPHROTIC SYNDROME.
22/37
Prognosis
Most cases resolve within the first week
Gross hematuria rapidly clears but
microscopic hematuria may be detectedfor 6 to 12 months
The long-term prognosis of PSGN inchildren is excellent
Even those with severe diseasecompletely recover
-
7/28/2019 NEPHRITIC/NEPHROTIC SYNDROME.
23/37
NEPHROTIC SYNDROME
-
7/28/2019 NEPHRITIC/NEPHROTIC SYNDROME.
24/37
NEPHROTIC SYNDROME
Not a distinct renal disease
A clinical and biochemical state that maydevelop during the
course of severaldifferent renal diseases of known andunknown
aetiology
-
7/28/2019 NEPHRITIC/NEPHROTIC SYNDROME.
25/37
CAUSES/ CLASSIFICATION
CONGENITAL :
- FINNISH TYPE (AUTOSOMAL RECESSIVE)
- MICROCYSTIC KIDNEY DISEASE(CONGENITAL NEPHROSIS)
- INTRAUTERINE INFECTIONS SUCH ASSYPHILIS, CMV, TOXOPLASMA
ACQUIRED :IDIOPATHIC OR PRIMARY ANDSECONDARY
-
7/28/2019 NEPHRITIC/NEPHROTIC SYNDROME.
26/37
CAUSES/CLASSIFICATION PRIMARY / IDIOPATHIC: Minimal change
nephropathy (MCN), Mesangial proliferative
GN, Focal segmental glomerulosclerosis
(FSG),Membranoproliferative GN (MPGN), andMembranous
nephropathy
SECONDARY: Systemic lupuserythematosus(SLE),
Henoch-Schonleinpurpura (HSP), amyloidosis, hepatitis B, HIV,
P.malariae, SCD, Bee stings, Gold salts/ heavymetals such as
mercury etc.
-
7/28/2019 NEPHRITIC/NEPHROTIC SYNDROME.
27/37
Minimal change nephroticsyndrome( MCNS)
Occurs in about 85% of children withidiopathic nephrotic
syndrome
Often steroid responsive
Onset usually between the age of 2-6years
More common in boys
Hypertension, hematuria and raised urealevels are rare
-
7/28/2019 NEPHRITIC/NEPHROTIC SYNDROME.
28/37
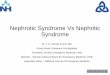
PATHOGENESIS OF NEPHROTICSYNDROME
Increasedglomerular
permeability
Gross proteinuria
Hypoalbuminaemia
hyperlipidaemia
Reduced oncoticpressure
Diminished effectiveplasma volume
Oedema- due tosalt/water retention
-
7/28/2019 NEPHRITIC/NEPHROTIC SYNDROME.
29/37
Clinical features of MCNS Insidious onset with periorbital
swelling and
facial puffiness
Swelling gradually increases to involve theextremities and
abdomen and if untreated
may become massive resulting in anasarca
May occasionally be associated with gross
hematuria and oliguria ( mixed picture of
nephrotic syndrome and acute nephritis)
-
7/28/2019 NEPHRITIC/NEPHROTIC SYNDROME.
30/37
LABORATORY EVALUATION Urinalysis : dipstick test(3+/4+), spot
urine test or
protein/creatinine concentrations (ratios
-
7/28/2019 NEPHRITIC/NEPHROTIC SYNDROME.
31/37
TREATMENT Initial episode:
- Control of massive edema and infection
before starting steroid therapy- Oral prednisolone 2mg/kg in 2
to 3 divided
doses for 6weeks and single morning dose
alternate days for the next 6 weeks
- Prolonging the treatment for 6 months mayresult in a longer
remission and fewer relapses
-
7/28/2019 NEPHRITIC/NEPHROTIC SYNDROME.
32/37
TREATMENT PATTERN OF RESPONSE TO STEROID THERAPY:
Remission: Protein-free urine(urine proteinnegative or trace)
for 3 consecutive days
Relapse: Proteinuria(urine protein 3+ or more)for 3 consecutive
days
Frequent relapser: 2 or more relapses within 6months of initial
episode or more than 3relapses within any 12 month period
Steroid dependent: 2 consecutive relapsesduring alt. day pred.
or within 2 weeks ofstopping therapy
-
7/28/2019 NEPHRITIC/NEPHROTIC SYNDROME.
33/37
TREATMENT
ALTERNATIVE OR ADJUNCT DRUGS USED INFREQUENT RELAPSES AND
STEROID
DEPENDENCE INCLUDE; LEVAMISOLE
CYCLOPHOSPHAMIDE
CYCLOSPORINE A
-
7/28/2019 NEPHRITIC/NEPHROTIC SYNDROME.
34/37
TREATMENT Use of ACEI : Enalapril, Lisinopril ( anti-
proteinuric effect)
Management of edema: diuretics,intravenous albumin or pooled
plasmatransfusion
Dietary management: high biologicalvalue protein, salt
restriction, supplementsof vitamins and micronutrients
Management of complications
-
7/28/2019 NEPHRITIC/NEPHROTIC SYNDROME.
35/37
Complications of Nephroticsyndrome
Infections : peritonitis, cellulitis
Hypovolemia
Thromboembolism
Hyperlipidemia
-
7/28/2019 NEPHRITIC/NEPHROTIC SYNDROME.
36/37
DIFFERENTIAL DIAGNOSIS
Angioneurotic edema
Protein-losing enteropathy
Chronic liver disease
Malnutrition with edema
Congestive heart failure
-
7/28/2019 NEPHRITIC/NEPHROTIC SYNDROME.
37/37
Prognosis
The final outcome of steroid sensitivenephrotic syndrome is
excellent
Most patients stop getting relapsesbetween the ages of 14 to 20
years
Fully recover without any residualdysfunction
Some may continue to have relapses intoadulthood