Embed Size (px)
Citation preview

Oxygen lowers intraocular pressurePamela F. Gallin-Cohen, Steven M. Podos, and Michael E. Yablonski
A significant decrease in intraocular pressure was demonstrated in 14 patients as atmosphericpressure was increased at intervals of 0.5 atmospheric pressure up to 3 atmospheres within ahyperbaric chamber. Nine of these patients had the identical protocol repeated in room air atatmospheric pressure without a significant change in intraocular pressure. Administration of100% O2 at 15 L/min by partial rebreathing face mask to these patients using the same protocolat atmospheric pressure resulted in a significant decrease in intraocular pressure. The results inthe oxygen and hyperbaric groups were not statistically different. While in the hyperbaricchamber, scleral rigidity increased uniformly, outflow facility decreased significantly, andkeratometry readings remained unchanged. A significant decrease in intraocular pressure oc-curred in 20 rabbits that received 100% oxygen by partial rebreathing face mask for 180minutes. Arterial blood gases were obtained at 0, 90, and 180 min in seven rabbits. The pH andpCO2 did not change significantly; however, pO2 was markedly elevated. Increased oxygenconcentration was felt to be responsible for the decrease in intraocular pressure and. thechanges in other parameters observed in patients and rabbits.
Key words: glaucoma, oxygen, intraocular pressure, hyperbaric chamber,keratometry, pseudofacility
A t increased atmospheric pressure, Prae-torius1 found a decrease in the outflow facilityof rabbits without an alteration of intraocularpressure (Schiotz). Kalthoff and John2 did notfind a change in the intraocular pressure ofdivers following 8m dives. However, a rapidrise in atmospheric pressure caused a de-crease in intraocular pressure in a patientwith chronic glaucoma simplex.2 Beehler andassociates3 found that hypotony was thesequel to retinal detachments following 145hr of oxygen administration.
The purpose of this experiment was to in-
From the Department of Ophthalmology, Mount SinaiSchool of Medicine of The City University of NewYork, New York, N. Y.
This study was supported in part by U. S. Public HealthService Grants EY-01661 and EY-01867.
Submitted for publication Feb. 6, 1979.Reprint requests: Dr. Pamela F. Gallin-Cohen, De-
partment of Ophthalmology, Mount Sinai School ofMedicine of the City University of New York, OneGustave L. Levy Place, New York, N. Y. 10029.
vestigate the effect of increasing atmosphericpressure and oxygen on the intraocular pres-sure in humans and rabbits.
Materials and methods
Humans. Fourteen volunteers with normal ocu-lar examinations had Goldmann applanation to-nometry measured bilaterally at 1 atmosphere(atm) (room air). They were then placed inthe Union Carbide Hyperbaric Chamber at TheMount Sinai Medical Center, in which the pres-sure was progressively increased from 1.0 atm to1.5, 2, 2.5, and 3 atm. At each interval, intraocularpressure was measured in only one eye, while at 1and 3 atm it was measured bilaterally. The mini-mum time interval between successive applana-tion measurements was 5 min. The mean time(±SD) from onset of increased atmospheric pres-sure to intraocular pressure measurement at 3 atmwas 38.3 ± 10.0 min. At 3 atm, tonography andkeratometiy were performed.
Each patient went into the hyperbaric chamberon only one occasion. All other room air mea-surements were obtained on other days. Nine ofthe above patients had the applanation protocol
0146-0404/80/010043+06$00.60/0 © 1980 Assoc. for Res. in Vis. and Ophthal., Inc. 43

44 Gallin-Cohen, Podos, and YablonskiInvest. Ophthalmol. Vis. Set.
January 1980
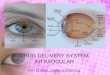
Fig. 1. The administration of oxygen to rabbits by pediatric partial rebreathing face mask.
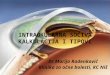
" 0 0.5 1.0 1.5 2.0 2.5 3.0ATMOSPHERES
Fig. 2. The change in intraocular pressure withincreasing atmospheric pressure in 14 patients.
repeated in room air at a similar time within 1 hr ofbaseline applanation intraocular pressure mea-surement and with identical time intervals and thesame eyes as within the chamber.
On a different day, at atmospheric conditions,the same nine patients breathed 100% oxygen bypartial rebreathing face mask at 15 L/min. A por-table oxygen tank was used with 6 ft connectiontubing (Vs inch diameter) and Puritan humidifier,This resulted in a 90% to 95% oxygen delivery,as measured by oxygen analyzer. Intraocular pres-sure was measured following the identical protocol.
On another day, 14 of the patients had tonog-raphy (Alcon), and in 12 patients keratometry wasperformed on the same eye as within the chamberbut at 1 atm (room air).
Analysis was carried out on the same nine pa-tients within three distinct environments.
1. Hyperbaric group. These patients wereplaced within a hyperbaric chamber in which at-mospheric pressure was increased from 1 to 3 atmat 0.5 atm increments (3 atm pressure, 520 mmHg, partial pressure oxygen).
2. Control group. Intraocular pressure was ob-tained at room air within an office (1 atm pressure,22.8% oxygen, 173 mm Hg, partial pressureoxygen).
3. Oxygen group. Face mask oxygen was ad-ministered to patients within an office (1 atm pres-sure, 100% oxygen administration with 90%to 95%delivery, 722 mm Hg, partial pressure oxygen).Times were standardized with respect to the ap-planations within the chamber. Time 1 representsthe time within the control or oxygen groupsequivalent to the applanation at 1 atm within thehyperbaric chamber. Similarly, time 3 is the timeequivalent to the applanation at 3 atm pressurewithin the chamber.
The mean time until the "3 atm" reading ofintraocular pressure in these three groups was38.5 ± 8.8 min.

Volume 19Number 1 Oxygen lowers intraocular pressure 45
Table I. Effect of atmospheric pressure and oxygen on intraocularpressure (mm Hg) in humans
Hyperbaric chamber(14 subjects)
Room air(9 subjects)
Control100% O2
1 Atm
15.3 ± 2.1
Time 1\
15.2 ± 1.614.8 ± 2.8
1 >/> Atm
13.9 ± 2.2
Time 1V4
14.3 ± 1.413.4 ± 3.2
2 Atm
13.1 ± 1.8
Time 2
14.6 ± 1.613.4 ±3.1
2ViAtm
13.0 ± 1.7
Time 2M>
14.8 ± 1.612.8 ± 3.4
3 Atm
12.3 ± 1.7*
Time 3
15.0 ± 1.7$12.7 ± 3.0*
*Significant difference between IOP at last measurement and first measurement (paired t test; p < 0.001).tTime is that of IOP measurement corresponding to similar time while in hyperbaric chamber at various atmospheres.(Significant difference between (a) control IOP at time 3 and 3 atm. (p < 0.001); (b) control IOP at time 3 and 100% oxygen at time 3(p < 0.025).
Table II. Effect of atmospheric pressure on ocular parameters in humans
IOP Applanation (mm Hg)Other eye*
IOP Schi0tz (mm Hg)tOutflow facility (ml/mm/mm Hg)tOcular rigidity (/xl"1)Keratometry
No. patients
12
14141412
I Atm
14.8 ± 2.3
14.0 ± 1.90.34 ± 0.15
0.019 ± 0.00543.7 ± 1.5
3 Atm
11.9 ± 1.7
11.3 ± 1.40.24 ± 0.10
0.023 ± 0.00543.9 ± 1.7
P*
<0.001
<0.001<0.020<0.001>0.050
Values at 1 and 3 Atm are mean ± S.D.*Eye receiving applanation tonometry only at 1 Atm and 3 Atm.t Corrected for scleral rigidity.(Significant difference of values at 1 and 3 Atm, by paired t test.
Rabbits. Face mask oxygen was administered to20 rabbits. Intraocular pressure was measured atthe baseline (—15, -10, - 5 , and 0 min) and dur-ing oxygen administration at 30 min intervals for180 min using a calibrated pneumotonograph.One hundred percent oxygen was delivered at 15L/min through 6 ft connection tubing (Vs inch di-ameter) using a Puritan humidifier and thepediatric size of the partial rebreathing face maskused previously (Fig. 1). The above sequence ofintraocular pressure measurement was also fol-lowed for a "control group" of six rabbits which didnot receive oxygen.
During this study, arterial blood gas composi-tion was determined by the withdrawal of 4 ml ofarterial blood into a heparinized syringe at 0, 90,and 180 min from the ear artery. The blood wasplaced on ice and blood gas determination madewithin 15 min using an ABL-2 machine. Despite20 attempts, only seven complete sets of gaseswere obtained due to severe peripheral vasocon-striction during oxygen administration.
Results
Humans. When the intraocular pressurewas repetitively measured at 0.5 atmosphericpressure intervals in 14 patients within thehyperbaric chamber, it showed a significant
Table III. Effect of face mask oxygen onintraocular pressure in rabbits
Minutes
0*90
180
IOP (mean ±
Oxygen (40 eyes)
24.3 ± 2.321.6 ± 2.9t21.9 ± 2.9t
SD) (mm Hg)
Control (12 eyes)
25.5 ± 1.925.7 ± 1.824.8 ± 1.5
*Mean value of pressures at —15, —10, —5, and 0 min.tSignificant difference between 0 min and 90 or 180 min meanreadings (paired t test, p < 0.001).
(p < 0.001) decrease from 15.3 ± 2 . 1 mmHg at 1 atm to 12.3 ± 1 . 7 mm Hg at 3 atm(Table I, Fig. 2). The intraocular pressure ofthe fellow eye was measured at 1 and 3 atm.It decreased from 14.8 ± 2 . 3 mm Hg (1 atm)to 11.9 ± 1 . 7 mm Hg (3 atm). There was nosignificant difference between the decreasein the eye subjected to repetitive pressuremeasurements and the fellow eye receivingbaseline and final pressure measurements.
Comparisons between the baseline intra-ocular pressure in the control, oxygen, andhyperbaric groups (see Methods) were notstatistically different. There was no statis-tically significant change of intraocular pres-

46 Gallin-Cohen, Podos, and Yablonski Invest. Ophthalmol. Vis. Sci.January 1980
Table IV. Effect
Minutes of oxygen
090
180
of face mask oxygen onpH (mean ± SD)
7.44 ± 0.027.42 ± 0.057.40 ± 0.05
arterial blood gas in sevenpO2(mean ± SD)
91.3 ± 22.1426.3 ± 99.4*427.8 ± 97.1*
rabbits
pCO2 (mean
37.6 ± 538.6 ± 437.4 ± 5
± SD)
598
••Significant difference between 0 min and 90 or 180 min mean readings (paired t test, p < 0.001).
sure in the control group, 15.2 ± 1.6mmHgat time 1 and 15.0 ± 1.7 at time 3. However,the intraocular pressure of the control groupat time 3 was significantly (p < 0.001) higherthan that of the hyperbaric group at 3 atm(Table I).
There was a significant (p < 0.001) de-crease in intraocular pressure from time 1 totime 3 within the oxygen group. The controlgroup and oxygen group intraocular pres-sures differed significantly at time 3 (p <0.025). There was no statistically significantdifference between the intraocular pressureof the patients within the hyperbaricchamber at 3 atm and the oxygen group attime 3.
Ocular rigidity was calculated for each eyeat 1 and 3 atm by the method of Friedenwald,as described in Becker and Shaffer.4 Scleralrigidity increased significantly (p < 0.001)from 0.019 ± 0.005 at 1 atm to 0.023 ±0.005 at 3 atm (Table II). Mean outflow facil-ity corrected for scleral rigidity, as above, de-creased significantly (p < 0.02) from 0.34 ±0.15 ml/min/mm Hg at room air to 0.24 ±0.10 ml/min/mm Hg at 3 atm (Table II). Thechange in keratometry readings from 1 atm to3 atm was not statistically significant. At 1atm the mean was 43.73 ± 1.46 diopters, incomparison to 43.92 ± 1.70 diopters at 3atm. The keratometry readings of a steel ballwere the same at 1 atm and 3 atm.
Rabbits. The intraocular pressure of 40rabbit eyes (20 rabbits) showed a significantdecrease (p < 0.001), from 24.3 ± 2.3 mmHg at the baseline to 21.9 ± 2.9 mm Hg at180 min of oxygen administration (Table III).The intraocular pressure in 12 control rabbiteyes did not change significantly at 90 or180 min.
Blood gases were obtained at 0, 90, and180 min in seven rabbits (Table IV). No sta-
tistically significant change in pH was seen.The pO2 increased significantly (p < 0.001)from 91.3 ± 22.1 at the baseline to 426.3 ±99.4 at 90 min and 427.8 ± 97.1 at 180 min.The pCO2 remained unchanged with meanvalues of 37.6 ± 5.5 at the baseline, 38.6 ±4.9 at 90 min, and 37.4 ± 5.8 at 180 min.
Discussion
An increase of atmospheric pressure from 1to 3 atm within the hyperbaric chambercaused a significant decrease in human ap-planation intraocular pressure. This was incontrast to the findings of Praetorius,1 whodid not note a change in the Schi0tz pres-sures of rabbits at 3 and 4 atm.
Moses,5 Bynke and associates,6 and Wilke7
reported decreases of 2 to 3 mm Hg in appla-nation tonometry values following five to sixrepetitive applanation readings at 1 min in-tervals. In our study, the minimum time in-terval between applanations was 5 min. Nosignificant differences between the decreasesin intraocular pressure were demonstrablebetween the eye receiving repetitive pres-sures and the eye receiving only baseline andfinal measurements. Therefore, the effect ofrepeated applanation tonometry cannot ac-count for the observed effect of the decreasein intraocular pressure.
Welsh and associates8 have reported in-creases of 0.75 to 1.0 diopter in the kera-tometry readings of Navy divers (and a steelball) within a hyperbaric chamber at 4 and 5atm. In contrast, our keratometry readingsdid not change. Welsh and associates8 at-tributed the keratometry changes to a changein the refractive index of the air. Structuralchanges within the keratometer were ruledout by Bausch and Lomb engineers (personalcommunication). However, Welsh and asso-ciates8 did not consider the effect of tern-

Volume 19Number 1 Oxygen lowers intraocular pressure 47
perature, which reached 130° F within thechamber. The Mount Sinai hyperbaricchamber was continuously air-conditioned.The lack of change in cornea curvature isconsistent with the concept that slowly in-creasing atmospheric pressure rapidly equil-ibrates throughout the entire body, causinglittle demonstrable change in the contour ofthe globe.
The significant decrease in intraocularpressure demonstrated in 40 rabbit eyes re-ceiving face mask oxygen at room air confirmsthe results in humans. The change in IOPwas significant at 90 and 180 min. As in thepatient control group, there was no signif-icant decrease in the intraocular pressure ofthe control rabbits.
Although oxygen is probably responsiblefor the decrease in intraocular pressure dem-onstrated within the hyperbaric chamber andwith face mask oxygen at room air, the effectsof arterial pH and carbon dioxide are notknown. Intracerebral vasoconstriction occurswithin the hyperbaric chamber9"11; however,the individual effect of increasing oxygen ordecreasing carbon dioxide is debated. Mar-cus and associates12 demonstrated a decreasein intraocular pressure associated with a pHchange secondary to increasing partial pres-sure of carbon dioxide. It is possible that ourpatient data might have been produced byincreasing oxygen or a change in carbondioxide.
While the question of the effect of CO2 andpH on intraocular pressure in the patientswithin the chamber and with face mask O2
was unanswered in the patient population, itwas clearly elucidated in the rabbit group.Although the pH decreased approximately0.04, this was not a statistically significant de-crease. The oxygen increased to a pO2 of 427mm Hg, consistent with the oxygen adminis-tration. It is important to note that the pCO2
did not change significantly. Thus the factorresponsible for the change in intraocularpressure in rabbits is probably the oxygen.
Scleral rigidity recalculated according tothe formula of Friedenwald4 increased uni-formly from 1 atm to 3 atm. The total outflowfacility decreased significantly at 3 atm in
comparison to 1 atm. The decrease in outflowfacility was consistent with the data of Prae-torius.1 He did not measure scleral rigidity.
Barany13 and Goldmann14- 15 indicated thatan apparent increase in scleral rigidity anddecrease in total outflow facility is possibledue to a relative decrease in choroidal bloodvolume. The effects of oxygen on retinal ves-sels have been observed in man. Fundusphotos showed retinal vasoconstriction due toincreased oxygen and no change followinghypocarbia.16 Similar results (constrictiondue to hyperoxygenation) have been re-ported,17"19 although Duke-Elder20 did notnote any change after 5 min. Only Beehlerand associates3 directly described oxygen andintraocular pressure. Following 145 hr ofconstant oxygen administration in dogs atroom air, retinal detachments were followedby hypotony. Therefore a decrease in cho-roidal volume, secondary to an oxygen-in-duced vasoconstriction, could yield the aboveobservation of increased scleral rigidity anddecreased total facility of outflow.
We conclude that the increased oxygenconcentration is responsible for the changesin tonography parameters and the decreasein intraocular pressure observed in humansubjects and rabbits. The exact mechanism ofthe decrease in pressure is not clear. A con-traction of the choroidal volume at a rate ofabout 40% of the normal secretory rate wouldyield the observed decrease in intraocularpressure; however, it seems unlikely thatsuch a contraction of the choroid would stillbe occurring after 38 min in the human ex-periments and after 180 min in the rabbitexperiments. Either a 40% decrease in therate of aqueous humor formation or an ap-proximately 3 mm Hg fall in episcleral ve-nous pressure would account for the ob-served fall in intraocular pressure. Directmeasurements of aqueous flow and episcleralvenous pressure are necessary to evaluatethese two possible mechanisms.
We thank Doctor J. Jacobson, Chief of Vascular Sur-gery, for his suggestions and use of the hyperbaricchamber; D. Mandell, R. N., Director of OphthalmologyClinics; and Colette Severin and Maria Perez.

48 Gallin-Cohen, Podos, and Yablonski Invest. Ophthalmol. Vis. Sci.January 1980
REFERENCES1. Praetorius, G.H.M.: The effect of increased baro-
metric pressure on intraocular pressure and aqueousdynamics: A preliminary report, S. Afr. Med. J.42:1254, 1968.
2. Kalthoff, H., and John, S.: Verhalten des augenin-nendruckes beim schnorcheln und tauchen, Klin.Monatsbl. Augenheilkunde 168:253, 1976.
3. Beehler, C.C., Newton, N.L., Culver, J., et al.:Retinal detachment in adult dogs resulting fromoxygen toxicity, Arch. Ophthalmol. 71:665, 1964.
4. Kolker, A., and Hetherington, J.: Becker-ShaffersDiagnosis and Therapy of the Glaucomas, St. Louis,1976, The C.V. Mosby Co., pp. 26, 124-125, 457-461.
5. Moses, R.A.: Repeated applanation tonometry,Ophthalmologica 142:663, 1961.
6. Bynke, H., Krakau, C.E.T., and Wilke, K.: Re-peated applanation tonometry in optic atrophy, ActaOphthalmol. 50:240, 1972.
7. Wilke, K.: Effects of repeated tonometry: Genuineand sham measurements, Acta. Ophthalmol. 50:574, 1972.
8. Welsh, K., Bennett, Q., and Kislin, B.: Effects ofhyperbaric air pressure on keratometry, Am. J. Op-tom. Physiol. Opt. 52:192, 1975.
9. Sukoff, M., Hollin, S., and Jacobson, J.: The pro-tective effect of hyperbaric oxygenation in experi-mentally produced cerebral edema and compres-sion, Surgery 62:40, 1967.
10. Harper, A.M., Jacobson, I., and McDowall, D.G.:In Ledingham, Iain McA., editor: The Effect of Hy-perbaric Oxygen on the Blood Flow through theCerebral Cortex, 2nd International Congress onHyperbaric Oxygenation, Baltimore, Md., 1965,The Williams & Wilkins Co., pp. 184-191.
11. Bergofsky, E.H., Wang, M., Yamaki, T., and Jacob-son, J.: Tissue oxygen and carbon dioxide tensions
during hyperbaric oxygen, J. Am. Med. Assoc.189:841, 1964.
12. Marcus, D.F., Krupin, T., Podos, S.M., andBecker, B.: The effect of exercise on intraocularpressure, I. Human beings, INVEST. OPHTHALMOL.
9:749, 1970.
13. Barany, E.H.: Pseudofacility and uveoscleral out-flow routes. In Glaucoma Symposium, Tutzing Cas-tle, 1966, Basel, 1967, S. Karger AG, pp. 27-57.
14. Goldmann, H.: Discussion of Barany, E. H.: Pseu-dofacility and uveoscleral outflow routes. In Glau-coma Symposium, Tutzing Castle, 1966, Basel,1967, S. Karger AG, pp. 40-57.
15. Goldmann, H.: On pseudofacility in vascular dis-eases in ophthalmology, Bibl. Ophthalmol. 76:1,1968.
16. Saltzman, H., Anderson, B., Hart, L., et al.: InLedingham, Iain, McA., editor: The Retinal Vascu-lar and Functional Response to Hyperbaric Oxy-genation in Normal Subjects and in Patients withRetinal Vascular Disease, 2nd International Con-gress on Hyperbaric Oxygenation, Baltimore, Md.,1965, The Williams & Wilkins, Co., pp. 202-211.
17. Frayser, R., and Hickham, J.B.: Retinal vascular re-sponse to breathing increased carbon dioxide andoxygen concentrations, INVEST. OPHTHALMOL. 3:
427, 1964.18. Dollery, C.T., Hill, D., Mialer, C , and Ramalho,
P.: Response of retinal blood vessels to changes inrespiratory gas pressures, J. Physiol. 177:70, 1965.
19. Cusick, P.L., Benson, O.O., and Boothby, W.M.:Effect of anoxia and of high concentrations of oxygenon retinal vessels, Proc. Staff Meeting, Mayo Clinic15:500, 1940.
20. Duke-Elder, S., cited by Campbell, A.J., and Hill,L.: Concerning the amount of nitrogen gas in thetissues and its removal by breathing almost pureoxygen, J. Physiol. 71:309, 1931.