Embed Size (px)
DESCRIPTION
kesehatan anak
Citation preview

04/22/2304/22/23 04:4004:40 [email protected] [email protected] 11
Pediatric Solid TumorsPediatric Solid Tumors
Bambang SudarmantoHematology-oncology working groupKariadi Hospital SemarangIndonesia

04/22/2304/22/23 04:4004:40 [email protected] [email protected] 22

04/22/2304/22/23 04:4004:40 [email protected] [email protected] 33
Pediatric TumorsPediatric Tumors
Kariadi Hospital is referall hospital Central Kariadi Hospital is referall hospital Central Java and part of BorneoJava and part of Borneo
Class of patients: Jamkesmas (poor Class of patients: Jamkesmas (poor people), Askes (health insurance), privatepeople), Askes (health insurance), private
Many are treated in Private HospitalsMany are treated in Private Hospitalsmany hospitals do not treat children with many hospitals do not treat children with
cancercancer

04/22/2304/22/23 04:4004:40 [email protected] [email protected] 44
Pediatric Solid Tumors (<14)Pediatric Solid Tumors (<14)
9,000 new cases, 1500 deaths of pediatric 9,000 new cases, 1500 deaths of pediatric cancers annually in the U.S.cancers annually in the U.S.
Cancer- 2nd leading cause of death in Cancer- 2nd leading cause of death in children (1children (1stst infections) infections)
1/3 deaths from leukemia1/3 deaths from leukemiaCNS tumors most frequent SOLID tumors CNS tumors most frequent SOLID tumors
in pediatric populationin pediatric population Indonesia data not viable (Semarang?)Indonesia data not viable (Semarang?)

04/22/2304/22/23 04:4004:40 [email protected] [email protected] 55
Pediatric solid tumorsPediatric solid tumors
Childhood cancer Childhood cancer requires multidisciplinary treatment groupsrequires multidisciplinary treatment groups
emotional needs of patient/familyemotional needs of patient/familynutritional needsnutritional needscoordinated care- medical, surgical, oncology, coordinated care- medical, surgical, oncology,
nursing, social services, therapists, educators nursing, social services, therapists, educators

04/22/2304/22/23 04:4004:40 [email protected] [email protected] 66
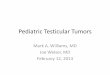
Distribution of Childhood CancerDistribution of Childhood Cancer
CNS18%
Liver1%
Other8%
Leukemia33%Retina
3%Germ Cell3%
Bone5%
Wilm's Tumor
6%
Hodgkin's5% NHL
3%
NBL8%
Soft Tissue Sarcoma
7%

04/22/2304/22/23 04:4004:40 [email protected] [email protected] 77
Thyroglossal Duct Cyst
Infectious/Inflammatory
Neoplasms
Pediatric Neck Mass
Congenital Acquired
Branchial cleft cyst
Cystic hygroma
Dermoid cyst

04/22/2304/22/23 04:4004:40 [email protected] [email protected] 88
Congenital MassesCongenital Masses
Thyroglossal duct Thyroglossal duct cystscysts
Branchial cleft cystsBranchial cleft cysts Lymphatic Lymphatic
malformationsmalformations HemangiomasHemangiomas TeratomasTeratomas Dermoid cystsDermoid cysts
LaryngocelesLaryngoceles Thymic cystsThymic cysts Vascular Vascular
malformationsmalformations SCM tumors of SCM tumors of
infancyinfancy Plunging ranulasPlunging ranulas

04/22/2304/22/23 04:4004:40 [email protected] [email protected] 99
Acquired MassesAcquired Masses
InfectiousInfectiousBacterialBacterialViralViralFungalFungalSialadenitisSialadenitis
InflammatoryInflammatoryKawasakiKawasakiSinus HistiocytosisSinus HistiocytosisDrug-induced Drug-induced
lymphadenopathylymphadenopathySarcoidosisSarcoidosis

04/22/2304/22/23 04:4004:40 [email protected] [email protected] 1111
Abdominal massesAbdominal masses
HistoryHistorySymptomsSymptoms
abdominal discomfort, increased abdominal abdominal discomfort, increased abdominal size or assymptomaticsize or assymptomatic
Presence of systemic symptomsPresence of systemic symptomsbone pain, limping, malaise, feverbone pain, limping, malaise, fever
Other symptomsOther symptomshematuriahematuria

04/22/2304/22/23 04:4004:40 [email protected] [email protected] 1212
Abdominal massesAbdominal masses
Physical findingsPhysical findingsPresence of abdominal massPresence of abdominal mass
upper abdomen or lower abdomenupper abdomen or lower abdomenOther associated physical findingsOther associated physical findings
other masses: orbitalother masses: orbitalbruisesbruiseshypertensionhypertensionpainpain

04/22/2304/22/23 04:4004:40 [email protected] [email protected] 1313
Abdominal MassAbdominal Mass
Differential diagnosis Differential diagnosis depends on locationdepends on location
Upper abdominal Upper abdominal massmass NeuroblastomaNeuroblastoma Wilm’s tumorWilm’s tumor HepatoblastomaHepatoblastoma RhabdomyosarcomaRhabdomyosarcoma Germ cell tumorGerm cell tumor LymphomaLymphoma

04/22/2304/22/23 04:4004:40 [email protected] [email protected] 1414
Abdominal MassAbdominal Mass
Differential diagnosis Differential diagnosis (cont)(cont)
Lower abdominal/pelvic Lower abdominal/pelvic massmass NeuroblastomaNeuroblastoma RhabdomyosarcomaRhabdomyosarcoma Germ cell tumorGerm cell tumor LymphomaLymphoma Ewing’s sarcomaEwing’s sarcoma

04/22/2304/22/23 04:4004:40 [email protected] [email protected] 1515
Abdominal MassesAbdominal MassesLaboratory evaluationLaboratory evaluation Bone marrow aspirateBone marrow aspirate
neuroblastoma, lymphoma, neuroblastoma, lymphoma, rhabdomyosarcoma or rhabdomyosarcoma or Ewing’s sarcoma Ewing’s sarcoma
CSF tapCSF tap if lymphoma is a if lymphoma is a
considerationconsideration

04/22/2304/22/23 04:4004:40 [email protected] [email protected] 1616
Abdominal massesAbdominal masses
Radiologic work-upRadiologic work-up Abdominal/pelvic ultrasoundAbdominal/pelvic ultrasound
useful screening test: helps define location and useful screening test: helps define location and quality (solid or cystic)quality (solid or cystic)
not useful to assess for retroperitoneal adenopathynot useful to assess for retroperitoneal adenopathy
Computed tomographyComputed tomography location of masslocation of mass presence of calcificationpresence of calcification obstructive signs obstructive signs

04/22/2304/22/23 04:4004:40 [email protected] [email protected] 1717
Wilm’s TumorWilm’s Tumor
Accounts for 6% childhood malignanciesAccounts for 6% childhood malignanciesMedian age at diagnosis 3 yearsMedian age at diagnosis 3 yearsMetastasizes to lung and lymph nodesMetastasizes to lung and lymph nodes
70% patients present with localized disease70% patients present with localized disease

04/22/2304/22/23 04:4004:40 [email protected] [email protected] 1818
Wilm’s Tumor: Signs & SymptomsWilm’s Tumor: Signs & Symptoms
Most commonly Most commonly presents as painless presents as painless abdominal massabdominal mass
Hypertension (20-Hypertension (20-30%)30%)
Pain (20-30%)Pain (20-30%) Hematuria (25%)Hematuria (25%)

04/22/2304/22/23 04:4004:40 [email protected] [email protected] 1919
Wilm’s TumorWilm’s Tumor
Diagnosis:Diagnosis:UltrasoundUltrasoundCTCT
Lymph node and lung metsLymph node and lung metsRight sided tumors- liver metsRight sided tumors- liver metsMets to bone and brain possible with some Mets to bone and brain possible with some
histologieshistologies

04/22/2304/22/23 04:4004:40 [email protected] [email protected] 2020
Wilm’s Tumor: Staging Wilm’s Tumor: Staging SystemSystem
StageStage DefinitionDefinition
II Tumor limited to kidney, completely excisedTumor limited to kidney, completely excised
IIII Tumor extends beyond the kidney, completely Tumor extends beyond the kidney, completely resected; no residual tumor beyond resection marginsresected; no residual tumor beyond resection margins
IIIIII Residual non-hematogenous tumor confined to Residual non-hematogenous tumor confined to abdomenabdomen
IVIV Hematogenous metastasesHematogenous metastases
VV Bilateral renal involvementBilateral renal involvement

04/22/2304/22/23 04:4004:40 [email protected] [email protected] 2121
Bilateral Wilm’sBilateral Wilm’s

04/22/2304/22/23 04:4004:40 [email protected] [email protected] 2222
Survival by Stage and HistologySurvival by Stage and Histology
Histology/stage # pts 2 yr-s* 4 yr-s*
FH/I 546 98 97
II 281 96 94
III 290 91 88
IV 126 88 82
UH/I 20 89 89
UH/II-IV 40 56 54* survival

04/22/2304/22/23 04:4004:40 [email protected] [email protected] 2323
Wilm’s tumorWilm’s tumor
Treatment:Treatment:Remove kidney- nephrectomyRemove kidney- nephrectomy
Lymph nodes biopsiedLymph nodes biopsiedCan spread also through bloodCan spread also through bloodTumor spill is possible- abdominal cavity is at riskTumor spill is possible- abdominal cavity is at risk
Chemo and RT- sometimes preop to reduce Chemo and RT- sometimes preop to reduce tumor spill tumor spill
RT late stages, residual dx, LN mets, RT late stages, residual dx, LN mets, bilateral dx, lung metsbilateral dx, lung mets

04/22/2304/22/23 04:4004:40 [email protected] [email protected] 2424
Wilm’s TumorWilm’s Tumor
ChemoChemo Actinomycin-DActinomycin-D Added vincristine, Adriamycin- 80-100% cure ratesAdded vincristine, Adriamycin- 80-100% cure rates Mets = 70% cure rateMets = 70% cure rate

04/22/2304/22/23 04:4004:40 [email protected] [email protected] 2525
Wilms Tumor: Prognosis & Future DirectionsWilms Tumor: Prognosis & Future Directions
Prognostic factors: stage and histologyPrognostic factors: stage and histologyFuture directionsFuture directions
Minimize therapy for favorable histology Minimize therapy for favorable histology patientspatients
Identify biologic factors predictive of outcomeIdentify biologic factors predictive of outcome Intensify therapy for patients with unfavorable Intensify therapy for patients with unfavorable
histologyhistology

04/22/2304/22/23 04:4004:40 [email protected] [email protected] 2626
Pediatric Brain Tumors(CNS Tumor)

04/22/2304/22/23 04:4004:40 [email protected] [email protected] 2727
Brain tumors: pediatric vs. adultBrain tumors: pediatric vs. adult Adults: 70% of tumors are supratentorialAdults: 70% of tumors are supratentorial
meningiomameningioma pituitary adenomapituitary adenoma High grade astrocytomaHigh grade astrocytoma
Anaplastic astrocytoma (grade III)Anaplastic astrocytoma (grade III) Glioblastoma multiforme (grade IV astrocytoma)Glioblastoma multiforme (grade IV astrocytoma)
Pediatric: 70% in posterior fossaPediatric: 70% in posterior fossa pilocytic astrocytoma (cerebellar astrocytoma)pilocytic astrocytoma (cerebellar astrocytoma) medulloblastoma medulloblastoma

04/22/2304/22/23 04:4004:40 [email protected] [email protected] 2828
CNS TUMORSCNS TUMORSMost common solid tumors in childrenMost common solid tumors in children22ndnd most frequent (16.6% of all childhood most frequent (16.6% of all childhood
malignancies)malignancies) Incidence has increased over the past 2 Incidence has increased over the past 2
decades decades Leading cause of cancer death in childrenLeading cause of cancer death in childrenResult in more morbidity than any other Result in more morbidity than any other
malignancy in childhoodmalignancy in childhoodMetastatic brain cases are rareMetastatic brain cases are rare

04/22/2304/22/23 04:4004:40 [email protected] [email protected] 2929
CNS TUMORSCNS TUMORS
Signs & SymptomsSigns & Symptoms (related to the location, histologic grade (related to the location, histologic grade
of tumor & age of child)of tumor & age of child)GeneralGeneral-Headache-Headache-Seizures-Seizures-Mental status changes-Mental status changes-Increased intracranial Pressure (ICP)-Increased intracranial Pressure (ICP)

Astrocytoma Astrocytoma
- high grade- high grade
- low grade- low gradeMedulloblastomaMedulloblastomaBenign tumor : adenomaBenign tumor : adenoma
04/22/2304/22/23 04:4004:40 [email protected] [email protected] 3030

04/22/2304/22/23 04:4004:40 [email protected] [email protected] 3131
MedulloblastomasMedulloblastomas
25% of all childhood brain tumors25% of all childhood brain tumors Occurs in the posterior fossaOccurs in the posterior fossa
Arises in the midline of the cerebellum and spreads to the in the Arises in the midline of the cerebellum and spreads to the in the 4th ventricle and brain stem4th ventricle and brain stem
High propensity to spread through CSFHigh propensity to spread through CSF 2-12 yr old2-12 yr old
peaks at 5 yr oldpeaks at 5 yr old Rare in adultsRare in adults arises from primitive neuroepithelial cellsarises from primitive neuroepithelial cells histologically cells appear as small, round, blue cells histologically cells appear as small, round, blue cells
forming pseudorosettes. Purple friable tumorforming pseudorosettes. Purple friable tumor

04/22/2304/22/23 04:4004:40 [email protected] [email protected] 3232
medulloblastomasmedulloblastomas
invasion of the fourth ventricle causes sx invasion of the fourth ventricle causes sx CSF does not flow causing hydrocephalusCSF does not flow causing hydrocephalusheadaches early- morning vomit get progressively headaches early- morning vomit get progressively
worseworseAtaxiaAtaxiacranial nerve abnormalities from invasion of the cranial nerve abnormalities from invasion of the
brain stembrain stemStaging correlates with survivalStaging correlates with survivalCT/MRI, myelography of entire CNS necessary CT/MRI, myelography of entire CNS necessary

04/22/2304/22/23 04:4004:40 [email protected] [email protected] 3333
MedulloblastomasMedulloblastomas Can develop mets in boneCan develop mets in bone Neurosurgery is first treatmentNeurosurgery is first treatment
remove gross diseaseremove gross disease ventricular shunts are discouraged because of possible ventricular shunts are discouraged because of possible
seeding into peritoneal cavityseeding into peritoneal cavity
CSI- Craniospinal IrradiationCSI- Craniospinal Irradiation postop- RTpostop- RT lateral- opposed brain fieldslateral- opposed brain fields
cover retroorbitally through mid-cervical cordcover retroorbitally through mid-cervical cord The divergence of the spinal field determines the collimator The divergence of the spinal field determines the collimator
twisttwist

04/22/2304/22/23 04:4004:40 [email protected] [email protected] 3434
CSI- Craniospinal IrradiationCSI- Craniospinal Irradiation Depending on the length of the spine, two spinal fields Depending on the length of the spine, two spinal fields
may be necessarymay be necessary Whole spine is treated- down to S2 or S3Whole spine is treated- down to S2 or S3 Electrons are used many times to avoid treating Electrons are used many times to avoid treating
anterior structuresanterior structures Gaps (photons) between fields are featheredGaps (photons) between fields are feathered Some institutions are encouraging a small gap Some institutions are encouraging a small gap
between lateral brain fields and the upper spinal fieldbetween lateral brain fields and the upper spinal field See page 326 RedSee page 326 Red

04/22/2304/22/23 04:4004:40 [email protected] [email protected] 3535
CSI -Craniospinal IrradiationCSI -Craniospinal Irradiation
Immobilization importantImmobilization importantWhat position?What position?Anesthesia may be necessaryAnesthesia may be necessary
RT Doses:RT Doses:1.5 Gy day to 36 Gy1.5 Gy day to 36 GyBoost to posterior fossa area- 54 Gy @ 1.8 Boost to posterior fossa area- 54 Gy @ 1.8
daydayChemo investigationChemo investigation

04/22/2304/22/23 04:4004:40 [email protected] [email protected] 3636
RetinoblastomasRetinoblastomas
Most common intraocular tumor in childrenMost common intraocular tumor in children200 U.S. annually (Indonesia: no data) 200 U.S. annually (Indonesia: no data) Most occur 6 mos-4yrs oldMost occur 6 mos-4yrs oldHereditary risk factors- 10% of casesHereditary risk factors- 10% of cases
Can be bilateral- 35% casesCan be bilateral- 35% casesRarely curativeRarely curative

04/22/2304/22/23 04:4004:40 [email protected] [email protected] 3737
RetinoblastomasRetinoblastomas
Discovered by light reflexDiscovered by light reflexWhite vs. redWhite vs. red
Ophthalmologist examOphthalmologist examNo biopsyNo biopsy
Avoid possibility of vitreous seedingAvoid possibility of vitreous seedingCT: detect extraocular extensionCT: detect extraocular extension

04/22/2304/22/23 04:4004:40 [email protected] [email protected] 3838
RetinoblastomasRetinoblastomas
CSF diseaseCSF diseaseAssessed by lumbar punctureAssessed by lumbar puncture
Bone marrow may be biopsedBone marrow may be biopsedStaging systems developedStaging systems developed
Preferred treatments outlined Preferred treatments outlined Predict success ratesPredict success ratesMost commonMost common
Reese-EllsworthReese-Ellsworth

04/22/2304/22/23 04:4004:40 [email protected] [email protected] 3939
RetinoblastomasRetinoblastomas
Treatment TechniquesTreatment TechniquesPhotocoagulationPhotocoagulationCryosurgeryCryosurgery
Small tumors not near optic disc and maculaSmall tumors not near optic disc and macula
EnucleationEnucleationUnilateral diseaseUnilateral diseaseSacrifices globeSacrifices globe

04/22/2304/22/23 04:4004:40 [email protected] [email protected] 4040
RetinoblastomasRetinoblastomas
Treatment Techniques:Treatment Techniques:SurgerySurgeryRadiation ImplantsRadiation Implants
RTRT Inoperable or bilateral dxInoperable or bilateral dxSpare lens and corneaSpare lens and corneaTreat retinaTreat retina

04/22/2304/22/23 04:4004:40 [email protected] [email protected] 4141
RetinoblastomasRetinoblastomas
Treatment Method: if disseminated dxTreatment Method: if disseminated dxChemo Chemo
Good response expectedGood response expectedVAC- Vincristine, Adriamycin, cyclophosphamideVAC- Vincristine, Adriamycin, cyclophosphamideOPEC- vincristine, cisplatin, etoposide, OPEC- vincristine, cisplatin, etoposide,
cyclophosphamidecyclophosphamide

04/22/2304/22/23 04:4004:40 [email protected] [email protected] 4242
RetinoblastomasRetinoblastomas
Late Effects of TreatmentLate Effects of TreatmentEnucleationEnucleation
Several prosthetics will be needed as child growsSeveral prosthetics will be needed as child grows
RTRTFacial growth affectedFacial growth affectedSmall orbitsSmall orbitsBlind spotsBlind spotsRadiation retinitis, and dry eyesRadiation retinitis, and dry eyes2nd malignancy2nd malignancy

04/22/2304/22/23 04:4004:40 [email protected] [email protected] 4343
Neuroblastomas
500 cases annually U.S.500 cases annually U.S.2nd most common pediatric solid tumor-2nd most common pediatric solid tumor-
after brain tumorsafter brain tumorsAge range- newborns-several yrs oldAge range- newborns-several yrs oldMedian age 2 yrs oldMedian age 2 yrs old

04/22/2304/22/23 04:4004:40 [email protected] [email protected] 4444
NeuroblastomasNeuroblastomas
Occur mainly in the abdomenOccur mainly in the abdomen Originate in adrenal gland or paraspinal gangliaOriginate in adrenal gland or paraspinal ganglia
Lethargic, ill appearing child under 2 with Lethargic, ill appearing child under 2 with abdominal mass is commonabdominal mass is common
Spinal cord invasion will promote neurological sxSpinal cord invasion will promote neurological sx Horner’s syndrome present with upper Horner’s syndrome present with upper
sympathetic ganglia involvementsympathetic ganglia involvement Flushing, diarrheaFlushing, diarrhea

04/22/2304/22/23 04:4004:40 [email protected] [email protected] 4545
NeuroblastomasNeuroblastomas
Many children present with metsMany children present with mets Children older than 18 months have 70% Children older than 18 months have 70%
chance of developing metschance of developing mets CT- chest, abd (US)CT- chest, abd (US)
Lungs and liver assessedLungs and liver assessed MRI spineMRI spine Bone marrow biopsyBone marrow biopsy Bone scanBone scan

04/22/2304/22/23 04:4004:40 [email protected] [email protected] 4646
NeuroblastomasNeuroblastomas
PrognosisPrognosisDependent on age at presentationDependent on age at presentation< 1 yr old disease may regress if acute sx are < 1 yr old disease may regress if acute sx are
managedmanaged Treatment TechniquesTreatment Techniques
RT and chemo- low cureRT and chemo- low cureSurgery if no mets- high cure rateSurgery if no mets- high cure rateChemo and BMTChemo and BMTRT- palliationRT- palliation

04/22/2304/22/23 04:4004:40 [email protected] [email protected] 4848
LymphomasLymphomas
33rdrd most common cancer in children. 60% are most common cancer in children. 60% are NHL; 40% Hodgkins disease NHL; 40% Hodgkins disease
Extranodal disease is common in children with Extranodal disease is common in children with 1/3 rd involving the mediastinum, abdomen or 1/3 rd involving the mediastinum, abdomen or head and neckhead and neck
Multi agent chemotherapy is the mainstay of Multi agent chemotherapy is the mainstay of treatment, surgery and radiotherapytreatment, surgery and radiotherapy
Anticipation and treatment of complications is Anticipation and treatment of complications is extremely important (lysis tumor syndrome, SVC extremely important (lysis tumor syndrome, SVC syndrome)syndrome)

04/22/2304/22/23 04:4004:40 [email protected] [email protected] 4949
Non Hodgkins lymphomaNon Hodgkins lymphoma
NHL result from malignant proliferation of NHL result from malignant proliferation of cells of lymphocytic ar histiocytic linage.cells of lymphocytic ar histiocytic linage.
Generally restricted to lymphoid tissue Generally restricted to lymphoid tissue such as lymphnodes and spleen such as lymphnodes and spleen
NHL categorized as low, intermediate and NHL categorized as low, intermediate and high grade on the base of their clinical high grade on the base of their clinical aggressiveness.aggressiveness.

04/22/2304/22/23 04:4004:40 [email protected] [email protected] 5050
Non Hodgkins lymphomaNon Hodgkins lymphoma
Epidemiology :Epidemiology : peak is between 5-15 years median age 9 peak is between 5-15 years median age 9
years; male preponderance , 3:1years; male preponderance , 3:1 Increase risk include patient with immunologic Increase risk include patient with immunologic
defect (AIDS, etc), immunosuppresive therapy defect (AIDS, etc), immunosuppresive therapy (post transplant)(post transplant)
EBV is almost invariably associated with the EBV is almost invariably associated with the African Burkitt’s lymphomaAfrican Burkitt’s lymphoma

04/22/2304/22/23 04:4004:40 [email protected] [email protected] 5151
Non Hodgkins lymphomaNon Hodgkins lymphoma
Clinical feature:Clinical feature: are varied depend on the location of the tumor, the are varied depend on the location of the tumor, the
extent of the disease (stage) and histologic subtypeextent of the disease (stage) and histologic subtype Extranodal involvement :Extranodal involvement : Mediastinum: may produce SVC syndromeMediastinum: may produce SVC syndrome Abdomen: ileocaecal region, appendix, colon and Abdomen: ileocaecal region, appendix, colon and
retroperitoneal area. Cayse pain, vomiting, retroperitoneal area. Cayse pain, vomiting, intussuception, ascites, obstructiveintussuception, ascites, obstructive
Head and neck: enlargement of cervical node, paritis, Head and neck: enlargement of cervical node, paritis, tonsilar hyperthropy; jaw swellingtonsilar hyperthropy; jaw swelling

04/22/2304/22/23 04:4004:40 [email protected] [email protected] 5252
Non Hodgkins lymphomaNon Hodgkins lymphoma
Diagnosis and staging: Diagnosis and staging: History and physical examHistory and physical examBlood count, BMA and BiopsyBlood count, BMA and BiopsyLDH levelLDH levelEvaluation of liver test (bil, SGOT/SGPT; Evaluation of liver test (bil, SGOT/SGPT;
alkphospatase)alkphospatase)Chest radiography; USG; CT Scan abdomenChest radiography; USG; CT Scan abdomenAdequate surgical biopsyAdequate surgical biopsy

04/22/2304/22/23 04:4004:40 [email protected] [email protected] 5353
Non Hodgkins lymphomaNon Hodgkins lymphoma
Staging:Staging:Stage I: a single tumor (extranodal) or single Stage I: a single tumor (extranodal) or single
anatomic areawith exclusion of mediastinum anatomic areawith exclusion of mediastinum and abdomenand abdomen
Stage II: stage I + two or more nodal area on Stage II: stage I + two or more nodal area on the same side of diaphragnathe same side of diaphragna
Satege III: stage II + all extensive node Satege III: stage II + all extensive node enlargementenlargement
Stage IV: stage III + with initial involvement of Stage IV: stage III + with initial involvement of CNS or bone marrow or both CNS or bone marrow or both

04/22/2304/22/23 04:4004:40 [email protected] [email protected] 5454
Non Hodgkins lymphomaNon Hodgkins lymphoma
Principal therapy :Principal therapy :Multi agent chemotherapy : CHOPMulti agent chemotherapy : CHOP
Anticipation and treatment of complication:Anticipation and treatment of complication:Two complication : Two complication :
- Arising Space occupying tumor:- Arising Space occupying tumor:
intrathoracic complicationintrathoracic complicationpericardial effusionpericardial effusion
- Metabolic complication of chemotherapy:Metabolic complication of chemotherapy:
tumor lysis syndrometumor lysis syndrome
Management of relaps Management of relaps

04/22/2304/22/23 04:4004:40 [email protected] [email protected] 5555
Bone tumorsBone tumors
Benign and malignant tumorBenign and malignant tumorFracture pathologicFracture pathologicPlain radiography is lytic bone lesion; Plain radiography is lytic bone lesion;
cortical destructions soft tissue extension.cortical destructions soft tissue extension.Two most common cancers of bone : Two most common cancers of bone :
osteosarcoma and Ewing sarcoma and the osteosarcoma and Ewing sarcoma and the fascinating group of disorders known as fascinating group of disorders known as histiocytosis histiocytosis

04/22/2304/22/23 04:4004:40 [email protected] [email protected] 5656
OsteosarcomaOsteosarcoma
Epidemioloy and etiology:Epidemioloy and etiology:Most frequent adolescent and young adultsMost frequent adolescent and young adultsAnnual 600 new cases in USAAnnual 600 new cases in USACorrelated with radiation exposureCorrelated with radiation exposure Incidence increase among survival Incidence increase among survival
retinoblastoma (Rb) and p53 tumor supressor retinoblastoma (Rb) and p53 tumor supressor gen. gen.

04/22/2304/22/23 04:4004:40 [email protected] [email protected] 5757
OsteosarcomaOsteosarcoma
Pathology:Pathology:Clinical history and radiographic appereance Clinical history and radiographic appereance
of bone lesionof bone lesionCorrect diagnosis requires of bone biopsyCorrect diagnosis requires of bone biopsy
Biology : Biology : Genetic alteration occur in the tumor Genetic alteration occur in the tumor
suppresor genes p53 and Rb to play suppresor genes p53 and Rb to play important role in tumorogenesisimportant role in tumorogenesis

04/22/2304/22/23 04:4004:40 [email protected] [email protected] 5858
OsteosarcomaOsteosarcoma
Pathology:Pathology:Clinical history and radiographic appereance Clinical history and radiographic appereance
of bone lesionof bone lesionCorrect diagnosis requires of bone biopsyCorrect diagnosis requires of bone biopsy
Biology : Biology : Genetic alteration occur in the tumor Genetic alteration occur in the tumor
suppresor genes p53 and Rb to play suppresor genes p53 and Rb to play important role in tumorogenesisimportant role in tumorogenesis

04/22/2304/22/23 04:4004:40 [email protected] [email protected] 5959
OsteosarcomaOsteosarcoma
Clinical presentation:Clinical presentation: Painful hard of the bonePainful hard of the bone History of trauma History of trauma Osteosarcoma can occur in any body but usually Osteosarcoma can occur in any body but usually
develop in metaphysis of long bone, common site is develop in metaphysis of long bone, common site is distal femur; proximal humerus, distal femur; proximal humerus,
Systemic symptom are fever, night sweats, weight Systemic symptom are fever, night sweats, weight loss.loss.
Metastatic disease: other bone; pulmonary; soft tissueMetastatic disease: other bone; pulmonary; soft tissue

04/22/2304/22/23 04:4004:40 [email protected] [email protected] 6060
OsteosarcomaOsteosarcoma
Diagnosis and staging:Diagnosis and staging:Plain radiography lytic and/or sclerotic bone Plain radiography lytic and/or sclerotic bone
abnormalityabnormalityA “sunburst” appearance A “sunburst” appearance Cortical distruction and periosteal reactionCortical distruction and periosteal reactionMRI and biopsyMRI and biopsy

04/22/2304/22/23 04:4004:40 [email protected] [email protected] 6161
OsteosarcomaOsteosarcoma
Treatment : local control of tumor and systemic Treatment : local control of tumor and systemic therapy to eradicated microscopic metastasis therapy to eradicated microscopic metastasis disease at distant sitesdisease at distant sites Preoperative chemotherapy : reduced tumor bulk; Preoperative chemotherapy : reduced tumor bulk;
prognostic implication; making surgical resection prognostic implication; making surgical resection easiereasier
HDX MTX; doxorubicin and cisplatinHDX MTX; doxorubicin and cisplatin Post operative chemotherapy 12 monthPost operative chemotherapy 12 month Non metastatic disease : 60 -65% to be cured Non metastatic disease : 60 -65% to be cured
Metastatic diseases indicated poor prognosisMetastatic diseases indicated poor prognosis

04/22/2304/22/23 04:4004:40 [email protected] [email protected] 6262
Ewing sarcomaEwing sarcoma
Ewing sarcoma is one of a group of Ewing sarcoma is one of a group of tumors referred to as the Ewing sarcoma tumors referred to as the Ewing sarcoma family tumors (ESFT): Ewing sarcoma of family tumors (ESFT): Ewing sarcoma of bone; soft tissue Ewing sarcoma and bone; soft tissue Ewing sarcoma and peripheral primitive neuro ectodermal peripheral primitive neuro ectodermal tumor (PNET)tumor (PNET)
Arise from share the same chromossomal Arise from share the same chromossomal abnormality abnormality

04/22/2304/22/23 04:4004:40 [email protected] [email protected] 6363
Ewing sarcomaEwing sarcoma
Epidemiology and etiologyEpidemiology and etiologyLess than 20 years at diagnosisLess than 20 years at diagnosisAnnual incidence 2.7 case permillionAnnual incidence 2.7 case permillionThe cause of ESFT is unknown, unrelated The cause of ESFT is unknown, unrelated
with radiationwith radiationPathology and biology:Pathology and biology:

04/22/2304/22/23 04:4004:40 [email protected] [email protected] 6464
Soft Tissue SarcomasSoft Tissue Sarcomas
Arise from mesenchymal tissueArise from mesenchymal tissueCan arise anywhere in bodyCan arise anywhere in bodyWide variety of histologiesWide variety of histologies
Most common 60 %Most common 60 %RhabdomyosarcomasRhabdomyosarcomasUndifferentiated Undifferentiated

04/22/2304/22/23 04:4004:40 [email protected] [email protected] 6565
Soft Tissue SarcomasSoft Tissue Sarcomas
Diagnosis and StagingDiagnosis and StagingDepends on area involvedDepends on area involvedH&N, genitourinary, extremities and trunkH&N, genitourinary, extremities and trunk
A large painless mass- extremityA large painless mass- extremityPainful orbitPainful orbit
In genitourinary areas- urinary problems In genitourinary areas- urinary problems (male)(male)
Exophytic mass vaginaExophytic mass vaginaMets to lung and bone marrow most commonMets to lung and bone marrow most common

04/22/2304/22/23 04:4004:40 [email protected] [email protected] 6666
Soft Tissue SarcomasSoft Tissue Sarcomas
StagingStagingPhysical examPhysical examUSUSCT or MRICT or MRIBM biopsy/Chest CT (mets)BM biopsy/Chest CT (mets)Stage and histology dictate txStage and histology dictate tx

04/22/2304/22/23 04:4004:40 [email protected] [email protected] 6767
StagingStaging
TreatmentTreatment SurgerySurgery
First choice is removalFirst choice is removal RTRT
Improves local control, spare organsImproves local control, spare organs Field covers entire muscular compartmentField covers entire muscular compartment 50.4 Gy 1.8 Gy fx50.4 Gy 1.8 Gy fx Shield growth platesShield growth plates Spare BM in pelvis if possibleSpare BM in pelvis if possible BrachyBrachy
Chemo- resected/nonresected tumorsChemo- resected/nonresected tumors Vincristine and actinomycin-DVincristine and actinomycin-D

04/22/2304/22/23 04:4004:40 [email protected] [email protected] 6868
Unusual Childhood TumorsUnusual Childhood Tumors
Germ Cell TumorsGerm Cell Tumors Can occur anywhere in the midline from CNS to Can occur anywhere in the midline from CNS to
ovaries and testesovaries and testes Sacrococcygeal teratomas often seen in newbornsSacrococcygeal teratomas often seen in newborns NonseminomasNonseminomas
Embryonal carcinomaEmbryonal carcinoma ChoriocarcinomaChoriocarcinoma Yolk-sac tumorsYolk-sac tumors These often produce AFP, HCG chemical markersThese often produce AFP, HCG chemical markers
Seminoma- dysgerminomaSeminoma- dysgerminoma

04/22/2304/22/23 04:4004:40 [email protected] [email protected] 6969
Unusual Childhood TumorsUnusual Childhood Tumors
Liver tumorsLiver tumors Appear much like Wilm’s tumor or Appear much like Wilm’s tumor or
neuroblastomaneuroblastoma CT or US will differentiateCT or US will differentiate
Hepatoblastoma- under 2 yrs oldHepatoblastoma- under 2 yrs old Hepatocellular carcinoma- after 10 yrs old, multifocalHepatocellular carcinoma- after 10 yrs old, multifocal Surgery- primary txSurgery- primary tx
Chemo- often usedChemo- often used RT- rarely usedRT- rarely used Poor survival ratesPoor survival rates

04/22/2304/22/23 04:4004:40 [email protected] [email protected] 7070
Unusual Childhood TumorsUnusual Childhood Tumors
Histiocytosis X syndromesHistiocytosis X syndromes Spectrum of diseaseSpectrum of disease Involves Langerhan’s cellsInvolves Langerhan’s cells
Miscellaneous TumorsMiscellaneous Tumors Nasopharyngeal angiofibromasNasopharyngeal angiofibromas Undifferentiated nasopharyngealUndifferentiated nasopharyngeal Thyroid tumors- benign and malignant, Iodine 131-Thyroid tumors- benign and malignant, Iodine 131-
ablationablation Keloids or fibromasKeloids or fibromas Kaposi’s sarcomaKaposi’s sarcoma

04/22/2304/22/23 04:4004:40 [email protected] [email protected] 7171
Pediatric Patients- Special Pediatric Patients- Special ConsiderationsConsiderations
Extra Time NeededExtra Time NeededAnesthesiaAnesthesiaPsychosocial needs of family- jobs/homePsychosocial needs of family- jobs/home
Understanding/compassionate therapistUnderstanding/compassionate therapist
Use of rewards- stickers/toysUse of rewards- stickers/toysProtocolsProtocols
Info sent for immediate reviewInfo sent for immediate reviewCareful adherence to guidelines importantCareful adherence to guidelines important