Embed Size (px)
Citation preview

9/15/2019
1
Dana Scharfenberg MN, RN, OCN, CPAN
PSONS Fundamentals of Oncology Fall 2019
Oncologic Emergencies Defined
Cancer-related disorders that require emergency medical or surgical care.
Oncologic emergencies can occur upon diagnosis, throughout treatment, or during end-stage disease. They may be caused by the malignancy, the treatment, or a combination of both.
Objectives
Introduce emergencies that can occur in patients diagnosed with cancer (focused on MSCC, SVCS, DIC, and sepsis)
Identify risks associated with oncologic emergencies
Recognize associated signs and symptoms
Discuss pathophysiology
Learn diagnostic evaluations
Review nursing management and therapeutic interventions
Structural Emergencies
Metabolic Emergencies
Metastatic Spinal Cord Compression (MSCC)
Superior Vena Cava (SVC) Syndrome
Increased Intracranial
Pressure (ICP)
Cardiac Tamponade
Tumor Lysis Syndrome (TLS)
SIRS/Sepsis/Septic Shock
Disseminated Intravascular Coagulation (DIC)
Thrombosis
Hypercalcemia
Inappropriate Antidiuretic Hormone Secretion (SIADH)
Hypersensitivity Reactions (HSRs)
Anaphylaxis

9/15/2019
2
Metastatic Spinal Cord Compression MSCC “ … occurs when tumor invades or extends into the epidural
space or pathologically collapsed vertebral fragments impinge on the
spinal cord”; but can also be a hematoma or abscess (Kaplan, 2018).
MSCC is seen in up to 5% of cancer patients
Commonly Associated Cancers: Tumors that metastasize to the bone:
breast, lung, prostate, kidney, lymphoma, multiple myeloma
Signs and Symptoms: Back pain (earliest symptom for most), motor
weakness, sensory impairment, autonomic dysfunction, and paraplegia
Management: Corticosteroids, radiation, and/ or surgery like
decompression surgery and spine stabilization
Diagnostic test: non-contrast
MRI or biopsy (consider holding
steroids till after a biopsy)
MSCC can lead to permanent
neurological dysfunction;
however, 80-90% of patients
who are ambulatory at time of
treatment retain function.
*Early recognition matters!

9/15/2019
3
MSCC Check your MSCC knowledge
Which of the following is NOT a treatment approach to managing MSCC?
A. High dose steroids
B. Diphenhydramine
C. Surgery
D. Chemotherapy
E. Antineoplastic agents
Superior Vena Cava Syndrome (SVCS) Occurs when a tumor compresses or invades the SVC or a
thrombus develops within it causing decreased blood return to the
heart.
Risk Factors and Commonly Associated Cancers: intervascular
devices or chest malignancies like lung, lymphoma, or breast.
Signs and Symptoms: dyspnea, facial swelling, venous distention
of the neck, arm swelling, veins prominent cutaneous veins,
cyanosis
Management: Control disease if possible (chemotherapy, radiation
or surgery), hydration, HOB 45, corticosteroids, oxygen, diuretics,
surgical bypass, clot removal with stenting, or thrombolytic therapy.

9/15/2019
4
Diagnostic test: Chest CT
“Chest computed
tomography with contrast
… reveals tumor location,
level of invasion, and
presence of a thrombus” (Kaplan, 2018)
Check your SVCS knowledge
What is the most common symptom associated with SVCS?
A. Face swelling
B. Cyanosis
C. Dyspnea
D. Venous distention

9/15/2019
5
Increased Intracranial Pressure (ICP) Risk Factors and Commonly Associated Cancers: Increased ICP can be caused by tumors that start in the brain or cancer that metastasizes to the brain. Cancer that spreads from the lung, breast, kidney or skin (melanoma) is more likely to cause increased ICP.
Signs and Symptoms: headache is the most common symptom of increased ICP. It is often worse in the morning or after strenuous activity. Additional signs: Nausea, vomiting, dizziness, behavior changes, poor memory, restlessness, nervous system problems (including weakness, numbness, vision problems, coordination problems, loss of muscle strength, paralysis or difficulty speaking, lowered consciousness, including drowsiness, lack of energy, confusion or coma.
ICP Later signs develop as ICP increases. The following signs of
increased ICP are called Cushing triad.
high blood pressure with an increasing difference between the
top (systolic) and bottom (diastolic) blood pressure readings
slow pulse rate
abnormal respirations
Diagnostic tests: if increased ICP is suspected: CT scan of the
head, MRI of the head, a lumbar puncture, or spinal tap
Management: increase HOB 30-45, radiation therapy or
intrathecal chemotherapy via an ommaya reservoir to treat the tumor, bore hole, CSF shunt, corticosteroids, antibiotics.

9/15/2019
6
Cardiac Tamponade and Pericardial Effusion Pericardial effusion is an abnormal accumulation of fluid in the pericardial space. This excess fluid can progress to cardiac tamponade, a critical condition restricting the ventricles from filling properly.
Risk Factors: infection, inflammation, malignancy, or autoimmune disorder. Acute and chronic GVHD. Can occur with any antineoplastic treatment, but is most common with Cyclophosphamide.
Associated Cancers: lung, breast, lymphoma, leukemia, and melanoma
Cardiac Tamponade and Pericardial Effusion
Signs and Symptoms: chest pain, tachypnea, dyspnea, tachycardia, hypotension, widening pulse pressure, edema, distended jugular veins, increased venous pressure
Diagnostic tests: Echocardiogram or chest X-ray
Management: O2, monitor VS, telemetry, cardiac medication (B blocker, ACE inhibitors, calcium channel blockers), diuretics, corticosteroids, drainage of excess pericardial fluid
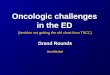
Tumor Lysis Syndrome (TLS)
TLS is more common in malignancies with high tumor burden or rapidly proliferating cells.
Tumor lysis syndrome (TLS) is caused when tumor cells die and massive quantities of intracellular contents release potassium, phosphates, and nucleic acids into the bloodstream. High levels of both uric acid and phosphate increase the severity of acute kidney injury because uric acid precipitates readily in the presence of calcium phosphate crystals.

9/15/2019
7
Tumor Lysis Syndrome (TLS) Commonly Associated Cancers: Leukemia, high grade lymphomas (NHL, ALL, AML, Burkett's lymphoma)
Signs and Symptoms: 25% increased from baseline phosphorus, potassium, and uric acid. 25% decrease in calcium. Nausea, vomiting, diarrhea, anorexia, lethargy, hematuria, heart failure, cardiac dysrhythmias, seizures, muscle cramps, tetany, syncope, and possible sudden death
Management: IV Fluids, allopurinol, rasburicase, diuretics, and dialysis in extreme cases
K+
PO4-
K+ PO4-
PO4- K+
Nucleic Acids
Nucleic Acids
Hypoxanthine Xanthine
Uric Acid
Xanthine Oxidase (Liver)
PO4
- PO4- PO4-
K+
K+
K+
PO4- Ca++ K+ Uric Acid
Urine of a patient with ALL and TLS

9/15/2019
8
TLS Onset:
Duration:
Usually within 6-72 hours after initiation of antineoplastic therapy
May persist for 5-7 days post-therapy
TLS Prevention
Vigorous Hydration – IV Normal saline or 5% dextrose; initially receive 2 to
3 L/m2 per day of IV fluid (or 200 mL/kg per day in children weighing ≤10 kg)
– Begin 24 – 48 hours prior to therapy
– Ensure urine output >150 – 200 ml/hr.
Allopurinol prevents uric acid build up. Oral dose in adults 200 -600mg/m2 day; IV 200-400mg/m2/day. In children, dose is 50 to 100 mg/m2 Q8H (maximum 300 mg/m2 per day) or 10 mg/kg per day in divided doses every eight hours. Reduced dose by 50 percent in the setting of acute kidney injury.
TLS Clinical Presentation
Early – nonspecific vague symptoms (nausea, vomiting, muscle cramps, lethargy), low urine output Late – cardiac dysthymias, seizures, organ failure
Detected in blood chemistries
Monitor serial lab values (Q4-Q12) – Serum potassium, phosphorous, ionized calcium, uric
acid, CBC – Renal function studies – BUN & creatinine
TLS Treatment Diuresis
– Typically used if urine output is not maintained by hydration
alone
– Loop or osmotic diuretics
Rasburicase – Reduces pre-existing hyperuricemia rapidly
breaking down serum uric acid. Dose is usually 0.15 – 0.2mg/kg
(3mg – 7.5mg). Starts working within 4 hours. Contraindicated
with G6PD deficiency.
Dialysis when other treatments are not effectively managing
symptoms or if the patient has kidney damage

9/15/2019
9
Metabolic Abnormality
Management
Hyperkalemia Mild (Potassium<6.5 mEq/L):
Sodium polystyrene sulfonate orally or by enema
Potassium >6.5 mEq/L or cardiac changes:
IV calcium gluconate or calcium carbonate
IV sodium bicarbonate, hypertonic glucose & insulin accompanied by sodium polystyrene sulfonate
Loop diuretics & aggressive hydration
Hyper-phosphatemia
• Phosphate-binding agents
• Aluminum-containing antacids
• Hypertonic glucose plus insulin
• Aggressive hydration
Hypocalemia
• Appropriate management of hyperphosphatemia
• IV calcium gluconate or calcium chloride to treat arrhythmias
Check your TLS knowledge
TLS prevention and intervention includes
which of the following?
A. Hydration
B. Recognition of high risk patients
C. Pharmacologic methods
D. Frequent monitoring of electrolytes
E. All of the above
TLS Nursing Implications
• Know if your patient is at risk for TLS
• Know you hospital policy and implement TLS protocol
• Review G6PD level
• Thorough physical assessment
• Educate the patient and caregiver about TLS; provide emotional support
• Maintain aggressive hydration
• Maintain UO >150mL/hr (give loop or osmotic diuretics as ordered)
• Monitor electrolytes (Q4-Q12 hours) – Note uric acid samples should be analyzed within 1 hour to avoid sample degradation.
SIRS/Sepsis/Septic Shock Systemic inflammatory response syndrome (SIRS) is an inflammatory state affecting the whole body. It is defined as the presence of 2 or more of the following:
Fever >38°C (100.4°F) or hypothermic <36°C (96.8°F)
HR >90 beats/minute
Respiratory rate >20 breaths per minute or arterial carbon dioxide tension (PaCO2) of less than 32 mm Hg
Abnormal white blood cell count: >12,000/µL or < 4,000/µL or >10% immature [band] forms

9/15/2019
10
Potential
insults
Systemic
inflammatory
response
syndrome
(SIRS)
Occurs on a continuum
SIRS
Sepsis
Severe Sepsis
SEPTIC SHOCK! (Maloney, 2016)
SIRS/Sepsis/Septic Shock
SIRS: Clinical response to an insult with the presence ≥ 2 of the following: temp >38C or <36C, HR>90, RR>20, abnormal WBC
Sepsis: SIRS + confirmed infection
Severe Sepsis: Sepsis + sepsis-induced organ dysfunction or tissue hypo perfusion (hypotension, elevated lactate, low UO)
Septic Shock: Severe sepsis + refractory hypotension
SIRS/Sepsis/Septic Shock
• Neutropenic (ANC <500)
• Infection
• Medical devices
• Mucositis
• Hospitalization
• Corticosteroids or other
immunosuppressants
Risk Factors:
• Splenectomy
• Age >60
• Poor nutritional status
• Concurrent
immunosuppressive
disease
• Type of malignancy
(Maloney, 2016)
SIRS/Sepsis/Septic Shock

9/15/2019
11
Sepsis
• confusion, agitation
• tachycardia, hypotension
• tachypnea, hypoxia on
RA, decreased breath
sounds
• decreased UO
• warm, dry, flushed skin
• nausea/vomiting
• fever
Clinical Presentation:
Septic shock
• obtunded, coma
• arrhythmias, tachycardia,
hypotensive
• SOB, decreased breath sounds,
crackles/wheezes, ARDS,
pulmonary edema
• oliguria or anuria, ARF
• cold, pale, mottled skin
• decreased GI motility, jaundice
• fever
(Maloney, 2016)
SIRS/Sepsis/Septic Shock
SIRS/Sepsis/Septic Shock The key to saving lives is T.I.M.E. For every hour treatment is delayed, the risk of death increases by as much as 8%. T.I.M.E. is a memory aid, developed by Sepsis Alliance, to help individuals remember the signs and symptoms of sepsis and the urgent need for medical treatment when they are present. T.I.M.E. stands for: T – TEMPERATURE that’s abnormal I – Signs of an INFECTION M – MENTAL DECLINE E – Feeling EXTREMELY ILL

9/15/2019
12
Septic shock
• elevated LFTs
• increased BUN and/or
creatinine
• decreased hematocrit
and/or hemoglobin
• hypoglycemia
Laboratory manifestations:
Sepsis
• hyperglycemia
• leukocytosis
• long PT and aPTT
• decreased fibrinogen
and platelets
• Elevated lactate
• + blood cultures
• WBCs in urine
(Maloney, 2016)
SIRS/Sepsis/Septic Shock Diagnostics: • BMP • CBC • Coagulation studies • Lactate • ABGs • Cultures (blood, sputum, vaginal, urine, stool,
wound) • CXR if respiratory symptoms present • Anything else to help determine potential site
of infection?
SIRS/Sepsis/Septic Shock
• Screen for sepsis
• Obtain blood cultures (maybe pan
cultures) and lactate level
• Assess organ function(give O2 if
needed)
• Administer broad-spectrum
antibiotics within 1 hour
• Administer at least 30 mL/kg of IV
crystalloid fluid within the first
3 hrs (goal MAP ≥65)
• If needed, give antipyretic after
drawing cultures
• Assess source
• If MAP ≥65 after giving IVF,
administer vasopressor (vasopressin,
norepinephrine, Dopamine,
Epinephrine, Phenylephrine) for
hypotension unrelieved by
crystalloids
• Measure central venous pressure
(goal 8-12mmHg) and venous
oxygen saturation ScvO2 ≥70
• Re-measure lactate
• U.O. 0.5mL/kg/hr
Dellinger, RP et al (2013).

9/15/2019
13
Sepsis case study - 49 year old male
49 year old male diagnosed with DLBCL and received RICE conditioning chemotherapy presented to the clinic for his daily assessment and lab draws (CBC with differentials and CMP). He ambulated with a steady, strong, independent gait. Daily weight 70.3kg. Vital signs are: 36.6C/70/16 BP 130/80 O2 sat 97% on RA, denies pain, denies GI symptoms. After his assessment and lab draws, he went home with his wife who is a nurse.
Later his labs return and he is newly neutropenic with an ANC of 260.
What should your first actions be?
Sepsis case study -49 year old male
Was the provider notified?
Check to see if prophylactic antibiotics were ordered.
Call the patient and have him come back to the clinic to start the prophylactic antibiotics.
Sepsis case study -49 year old male
19:10 The patient’s wife called and said he had a fever of 100.8F. The Hospital Oncology nurse encouraged the wife to bring him in to our ER ASAP. The wife and patient refused. He felt he just needed a little sleep and then would be better.
21:00 The patient’s wife called again. This time the patient’s temperature was 102.0F, still very tired, “a little confused”, and so weak he could not walk. The Hospital Oncology nurse encouraged the wife to call 911 and have the ambulance bring him in to our ER ASAP.
The wife called 911 and the patient was taken to a hospital that does not manage patient’s who receive marrow transplants. 23:00 He was intubated. 04:30 the next day he died.
What went well? What could have been improved?

9/15/2019
14
Test your knowledge.
Which of the following oncologic emergencies is a potential complication of septic shock?
A. Increased intracranial pressure
B. Disseminated intravascular coagulation
C. Tumor lysis syndrome
D. Anaphylaxis/hypersensitivity
SIRS/Sepsis/Septic Shock Disseminated Intravascular Coagulation (DIC)
Definition: Generalized activation of the hemostatic system, which results in widespread overstimulation of normal coagulation in the microvasculature and the simultaneous consumption of coagulation factors and platelets. DIC is never a primary diagnosis. It ALWAYS is a symptom of an underlying disease. Anti-neoplastic therapies increase the risk for bleeding by damaging normal tissues. Radiation therapy and steroid treatment can cause blood vessels to become fragile and more prone to injury.
(Maloney, 2016; Viele 2008)
DIC
Diseases and conditions can disrupt the body's normal blood clotting process and lead to disseminated intravascular coagulation (DIC) includes:
• Sepsis (an infection in the bloodstream)
• Surgery and trauma
• Cancer
• Serious complications of pregnancy and childbirth
• Examples of less common causes of DIC are bites from poisonous snakes (such as rattlesnakes and other vipers), frostbite, and burns.
The two types of DIC are acute and chronic. Acute DIC begins with clotting in the small blood vessels and quickly leads to serious bleeding. Chronic DIC causes blood clotting, but it usually doesn't lead to bleeding. Cancer is the most common cause of chronic DIC.
DIC Cancer and Cancer Related Risk Factors: sepsis, acute leukemia, TLS, trauma, liver disease, and vascular abnormalities, hemolytic transfusion reactions or massive blood transfusions
Signs and Symptoms: Most patients with DIC bleed from at least three unrelated sites. Subtle signs and symptoms of thrombi include red, indurated areas found in multiple organ sites. Possible fever, hypoxia, hypotension, proteinuria, acidosis.
Diagnostic tests: CBC, maybe a blood smear, PTT, PT, serum fibrinogen, fibrinogen degradation products (D-dimer assay). DIC is almost always associated with increased fibrinolysis.
Treatment: Treat the underlying cause! Use of heparin and platelets are provider dependent.

9/15/2019
15
Petechiae vs. purpura Basic pathophysiology:
• Over activation of coagulation cascade from certain proteins
can be intrinsic (blood vessel damage)
can be extrinsic (tissue damage)
• Clots begin to form and are deposited throughout the body’s
vasculature
• Because of excessive clotting, clotting factors and platelets
are all used up!
• This means there is no more clotting factors and platelets
for normal clotting anymore, which allows for abnormal
bleeding! (Maloney, 2016; Viele, 2008)
DIC
DIC DIC Nursing Management
• Early identification and notification
• Draw labs as ordered
• Monitor vital signs
• Monitor the patient’s daily weight
• Monitor intake & output
• Prevent dehydration
• Provide a calm environment for the patient and family

9/15/2019
16
Thrombosis
“…venous thromboembolism is five times greater in patients
with cancer than in the general population.” (Kaplan, 2019)
Therapies associated with higher risk: thalidomide,
lenalidomide, and bevacizumab
Clinical Manifestations:
DVT (swelling, warmth, localized pain, limb color changes)
PE (dyspnea, pleuritic pain, tachypnea, tachycardia,
anxiety)
Virchow's triad
Thrombosis
Diagnostic tests:
DVT - D-dimer, venous duplex ultrasound, CT scan
PE – CT scan, pulmonary angiogram,
ventilation/perfusion scan
Treatment: low molecular weight heparin,
unfractionated heparin, factor Xa inhibitors (e.g.
rivaroxaban, apixaban and edoxaban), prophylaxis (e.g.
SCDs, TED hose, IVF)
Hypercalcemia of Malignancy (HCM)
HCM is experienced by 20% to 30% of cancer patients at some point
during the course of the disease.
Risk Factors and Commonly Associated Cancers: tumors
associated with bone metastasis; such as lung, breast, and multiple
myeloma
Signs and Symptoms: kidney changes and CNS changes, confusion,
lethargy, depression, muscle weakness, seizures, coma
Management: treatment of the underlying malignancy with surgery or
chemotherapy is the most effective way to manage HCM. Can also
use normal saline followed by forced diuresis; bisphosphonate therapy
(alendronate, pamidronate, zoledronic acid), calcitonin, corticosteroids.

9/15/2019
17
HCM – Bones, Stones, Groans, and Moans
The cornerstone of initial management of HCM is hydration with IV normal
saline (NaCl 0.9%), since almost all patients with hypercalcemia have
intravascular volume depletion.
HCM
Hypercalcemia is classified according to severity, and measurements of serum calcium levels may differ between laboratories.
Normal level: 8.5 to 10.5 milligrams per deciliter (mg/dL)
mild hypercalcemia is approximately 10.5 to 11.9 mg/dL; usually no symptoms
moderate hypercalcemia, 12.0 to 13.9 mg/dL; may cause anorexia, polyuria, polydipsia, nausea, vomiting, and constipation
severe hypercalcemia, ≥14.0 mg/dL; weakness, difficulty concentrating, confusion, stupor, and coma

9/15/2019
18
Inappropriate Antidiuretic Hormone Secretion (SIADH) Hyponatremia is the most frequent electrolyte disorder and the SIADH
accounts for approximately one-third of all cases and should be treated to
cure symptoms.
Signs and Symptoms:
Mild: May be asymptomatic; may experience fatigue, anorexia, difficulty
concentrating, weakness, muscle cramps, or weight gain
Moderate: thirst, impaired taste, confusion, lethargy, N/V, diarrhea,
oliguria, incontinence, depressed deep tendon reflexes, personality
changes
Severe: seizures, coma
Management: Eliminate or control disease if possible, mild fluid restriction,
IV furosemide, monitor labs, measure urine specific gravity Q4h-Q8h, if
severe may give 3% normal saline IV cautiously.
Hypersensitivity Reactions (HSRs) A hypersensitivity reaction is defined as an exaggerated immune response that results in local tissue injury or changes throughout the body in response to an antigen or foreign substance. Most coincide with chemotherapy drug administration. The likelihood of hypersensitivity reactions increases with repeated exposure to L-asparaginase, platinum compounds, and epipodophyllotoxins.
Antineoplastic agents are the 3rd leading cause of fatal drug related HSRs.
Commonly Associated Chemotherapy Agents: L-asparaginase, Taxanes, platinum compounds, Epipodophyllotoxins
Risk Factors: female, hx of allergies, hx of contrast reaction, prior exposure to drug, IV route

9/15/2019
19
Kaplan, 2019
Hypersensitivity
Prevention: Skin testing frequently is performed before administration of drugs that have a high likelihood of causing hypersensitivity reactions. Patients often are able to tolerate a re-challenge of an agent if they are pre-medicated with a corticosteroid and an antihistamine even if they previously have experienced hypersensitivity reactions.
Management: O2, epinephrine, type 1 histamine antagonist, type 2 histamine antagonist, dopamine, corticosteroids, albuterol, atropine, lidocaine, IVF (NS or LR)
Hypersensitivy reactions are often the result of a non–immune-mediated release of histamine or cytokines, because many patients can tolerate re-exposure to the drug if it is re-administered slowly after pretreatment with steroids and antihistamines
Anaphylaxis Anaphylaxis is an immunologically mediated event, most commonly associated with production of IgE antibodies; occurs within minutes or hours of exposure to offending agent.
Risk Factors: new medication (-mabs and DMSO are higher risk)
Signs and Symptoms: Urticaria, pruritus, facial edema, SOB, wheezing, systolic blood pressure < 90 mm Hg (or a 30% decrease)
Management: Stop infusion, administer antihistamines and O2. Consider IVF, acetaminophen, monitor VS, 12 lead ECG, corticosteroids, atropine or epinephrine for severe reactions.
* Keep emergency equipment at bedside should cardiorespiratory support be needed.
Kaplan, 2019

9/15/2019
20
Nursing Implications/ Clinical Pearls • Patient and family education
• Provide emotional support
• Know how to complete a good physical assessment
• Communicate concerns and observations to provider
• Give medications as ordered
• Know the location of emergency medications and your unit crash cart
• Know your institution’s policies and practices
•Early recognition may save a life!
Resources
SVCS
https://www.cancer.net/coping-with-cancer/physical-emotional-and-social-effects-cancer/managing-physical-side-effects/superior-vena-cava-syndrome
Sepsis
http://www.survivingsepsis.org/Pages/default.aspx
https://www.ncbi.nlm.nih.gov/pubmed/26903335
https://www.cdc.gov/sepsis/clinicaltools/index.html
DIC
https://www.nhlbi.nih.gov/health-topics/disseminated-intravascular-coagulation
References
• Allen, A., Mekoba, B., & Adigun, M. (2015). Oncologic Emergencies: Hypercalcemia of Malignancy and Tumor Lysis Syndrome. Specialty and Oncology, (40)5, 3-7.
• Dellinger, RP et al (2013). Surviving sepsis campaign: International guidelines for management of severe sepsis and septic shock, 2012. Intensive Care Medicine, 39, 165-228.
• Demshar, R., Vanek, R., and Mazanec, P. (2012). Cardiac, Hemorrhagic, and Coagulopathic Oncologic Emergencies: What nurses need to Know. Oncology Times, Nursing Hem/Onc Spotlight Series #9, (34)6, 2-8.
• Gobel, B.H. (2005). Chemotherapy-Induced Hypersensitivity Reactions. Oncology Nursing Forum, (32)5, 1027-1035.
• Kaplan, M. (2018). Understanding and Managing Oncologic Emergencies: A resource for nurses. (3rd ed). Pittsburgh, PA. Oncology Nursing Society.
• Maloney, K. W. (2016). Metabolic Emergencies (J. M. Brant, F. A. Conde, & M. G. Saria, Eds.). In J. K. Itano (Ed.), Core Curriculum for Oncology Nursing (5th ed., pp. 478-494). St. Louis, MO: Elsevier.
• McAdams, F.W. & Burgunder, M.R. (2013). Transplant Treatment Course and Acute Complications. In S.A. Ezzone (Ed). Hematopoietic Stem Cell Transplantation: A Manual for Nursing Practice. Pittsburgh, PA: Oncology Nursing Society.
• Lindsey, H. (2011). Structural & Metabolic Oncologic Emergencies: Early Recognition Crucial. Oncology Times, Nursing Hem/Onc Spotlight Series #5, (33)2, 6-8.

9/15/2019
21
References • Patchel, R.A., Tibbs, P.A., Regine, W.F., Payne, R., Saris, S., Kryscio, R.J., Mohiuddin, &
M., Young, B. (2005). Direct decompressive surgical resection in the treatment of spinal cord compression caused by metastatic cancer: a randomised trial. Lancet. (366)9486, 607-688.
• Pirschel, C. (2018) Oncology Nurses’ Role in Recognizing and Addressing Oncologic Emergencies: A matter of life or death https://voice.ons.org/news-and-views/oncology-nurses-role-in-recognizing-and-addressing-oncologic-emergencies Retrieved Aug 8, 2019
• Theis, J. (2014). Oncologic Emergencies in Pediatric Patients: What Oncology Nurses Need to Know. Oncology Times (36)7, 2-4.
• Vogel, W. H. (2016). Structural Emergencies (J. M. Brant, F. A. Conde, & M. G. Saria, Eds.). In J. K. Itano (Ed.), Core Curriculum for Oncology Nursing (5th ed., pp. 495-508). St. Louis, MO: Elsevier.
• Wudel, J. & Nesbit, J. (2001). Superior vena cava syndrome. Current Treatment Options Oncology, (2)1, 77-91.