Embed Size (px)
Citation preview
Management of withdrawal
Prof.Dr.Aznan Lelo,PhD,SpFK
Dr.Datten Bangun MSc,SpFK
Dept.Farmakologi & Terapeutik
Fak.Kedokteran
U S U
Withdrawal Syndrome
The characteristic group of signs and
symptoms that typically develop after :
= a rapid or
= marked decrease or
= discontinuation of a substance of
The characteristic group of signs and
symptoms that typically develop after :
= a rapid or
= marked decrease or
= discontinuation of a substance of = discontinuation of a substance of
dependence,
which may or may not be clinically significantly of life threatening.
= discontinuation of a substance of
dependence,
which may or may not be clinically significantly of life threatening.
Withdrawal Syndrome
Withdrawal severity and duration depend on several factors:
1. Nature of substance2. Half-life and duration of action3. Length of time substance used3. Length of time substance used4. Amount used5. Use of other substances 6. Presence of other medical and psychiatric
conditions 7. Individual biopsychosocial variables
Alcohol Withdrawal

Delirium TremensDelirium Tremens
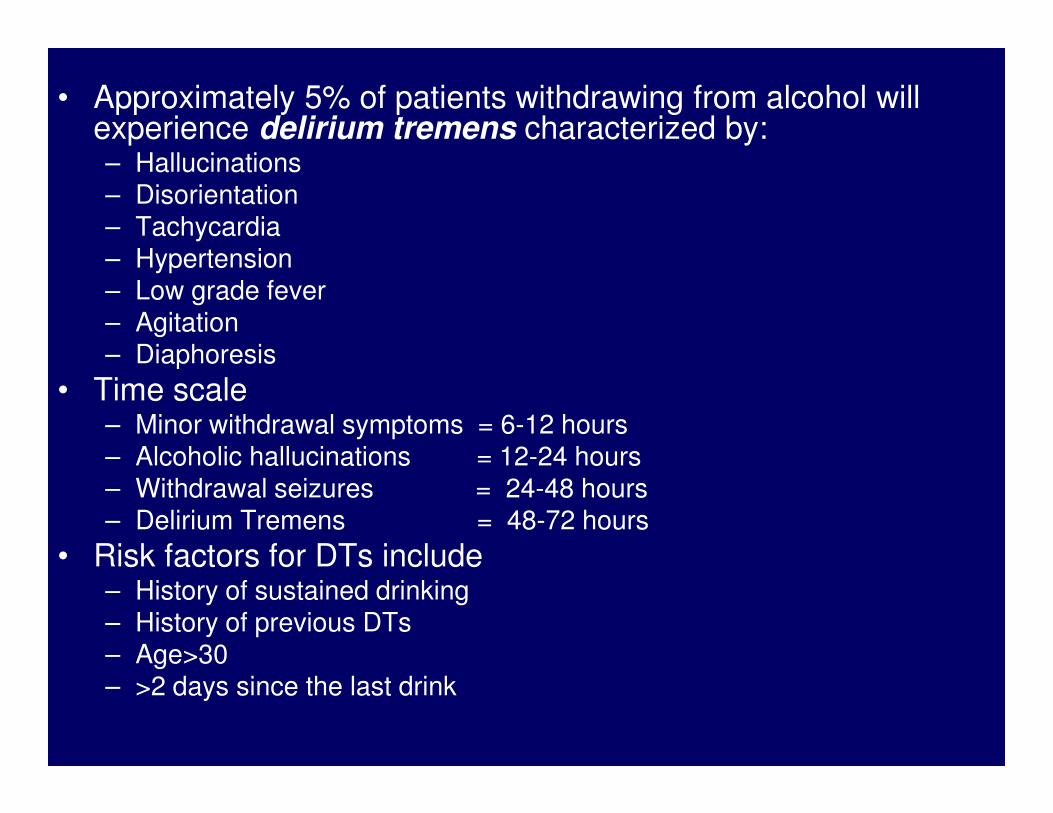
• Approximately 5% of patients withdrawing from alcohol will experience delirium tremens characterized by:– Hallucinations– Disorientation– Tachycardia– Hypertension– Low grade fever– Agitation– Diaphoresis
• Time scale• Time scale– Minor withdrawal symptoms = 6-12 hours– Alcoholic hallucinations = 12-24 hours– Withdrawal seizures = 24-48 hours– Delirium Tremens = 48-72 hours
• Risk factors for DTs include– History of sustained drinking– History of previous DTs– Age>30– >2 days since the last drink
3
4
0
00
5
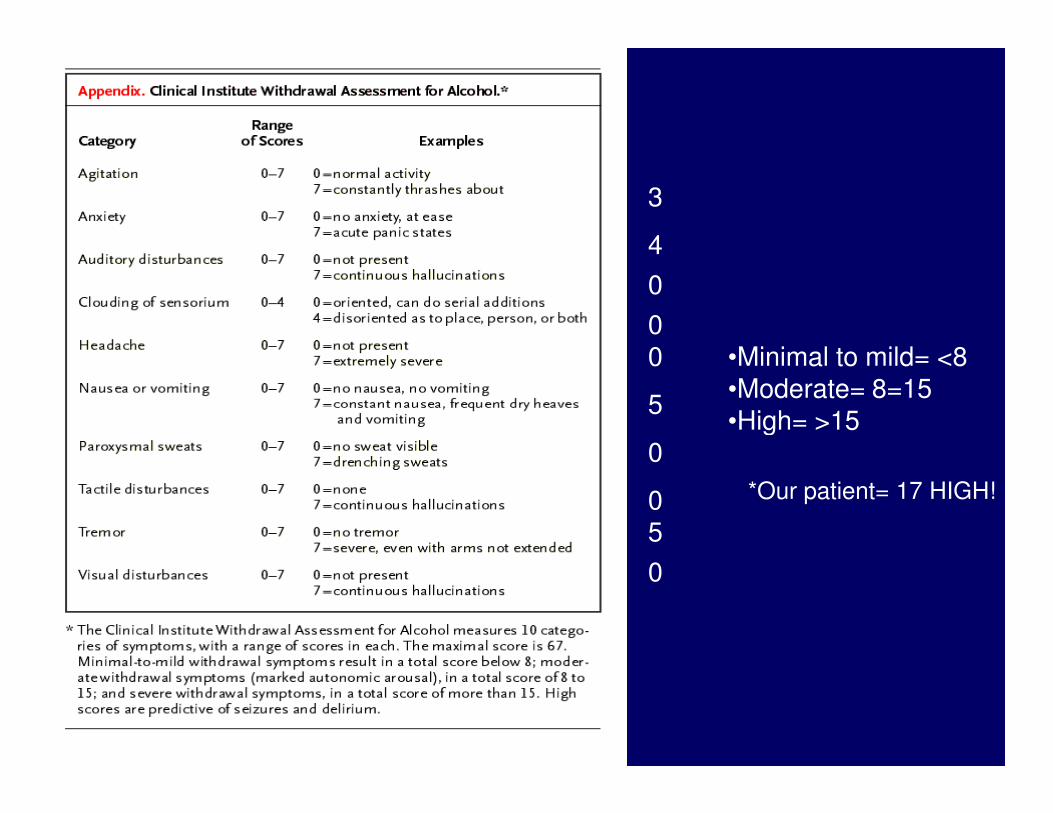
•Minimal to mild= <8•Moderate= 8=15•High= >15
*Our patient= 17 HIGH!
5
0
05
0
•High= >15
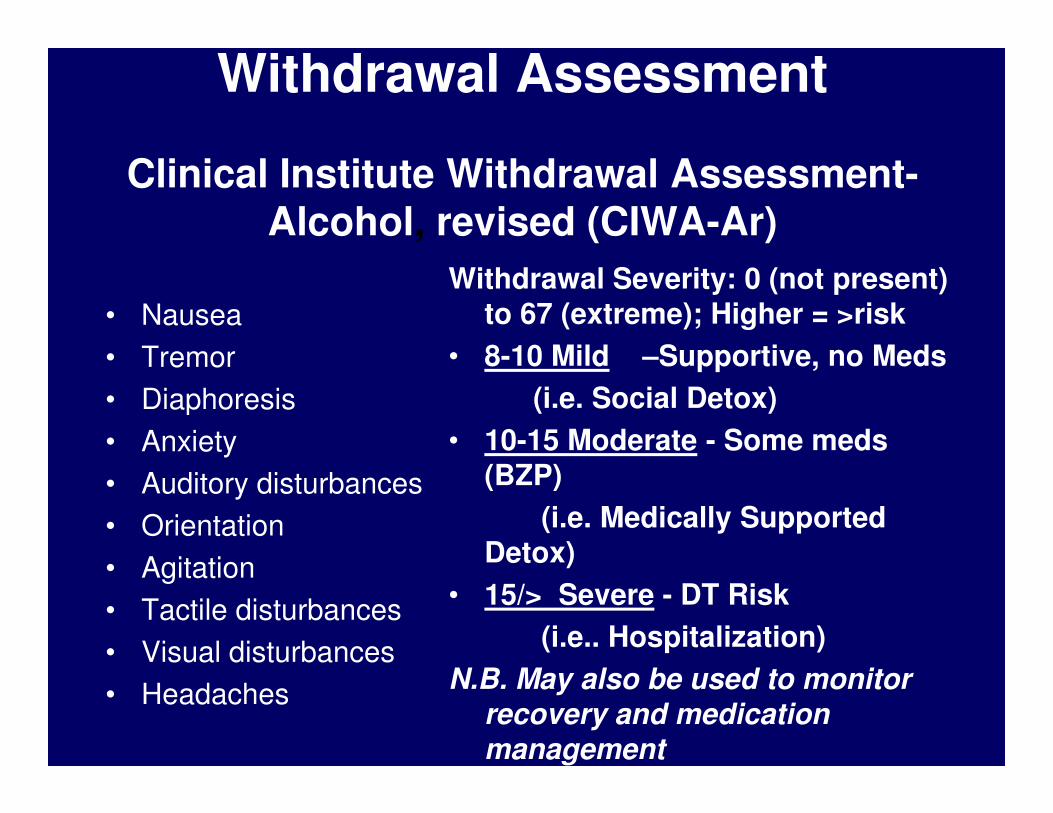
Withdrawal Assessment
Clinical Institute Withdrawal Assessment-Alcohol, revised (CIWA-Ar)
• Nausea
• Tremor
• Diaphoresis
Withdrawal Severity: 0 (not present)
to 67 (extreme); Higher = >risk
• 8-10 Mild –Supportive, no Meds
(i.e. Social Detox)• Diaphoresis
• Anxiety
• Auditory disturbances
• Orientation
• Agitation
• Tactile disturbances
• Visual disturbances
• Headaches
(i.e. Social Detox)
• 10-15 Moderate - Some meds
(BZP)
(i.e. Medically Supported
Detox)
• 15/> Severe - DT Risk
(i.e.. Hospitalization)
N.B. May also be used to monitor
recovery and medication
management
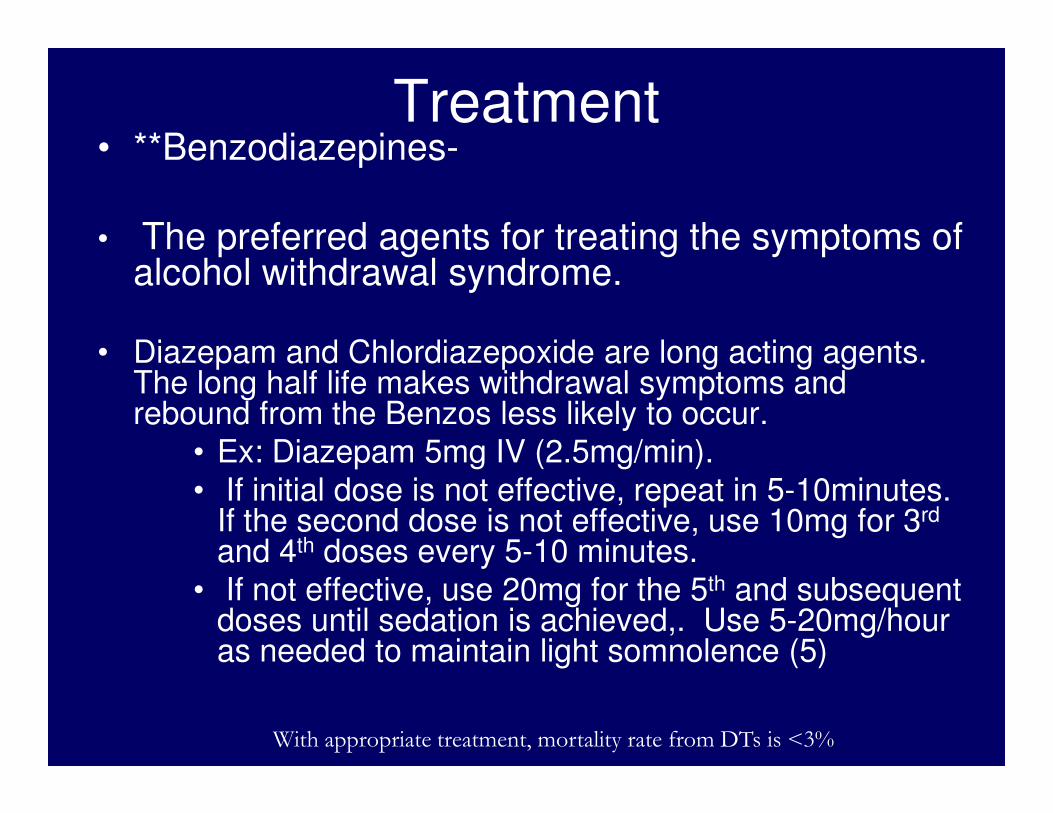
Treatment• **Benzodiazepines-
• The preferred agents for treating the symptoms of alcohol withdrawal syndrome.
• Diazepam and Chlordiazepoxide are long acting agents. The long half life makes withdrawal symptoms and rebound from the Benzos less likely to occur.rebound from the Benzos less likely to occur.
• Ex: Diazepam 5mg IV (2.5mg/min).
• If initial dose is not effective, repeat in 5-10minutes. If the second dose is not effective, use 10mg for 3rd
and 4th doses every 5-10 minutes.
• If not effective, use 20mg for the 5th and subsequent doses until sedation is achieved,. Use 5-20mg/hour as needed to maintain light somnolence (5)
With appropriate treatment, mortality rate from DTs is <3%
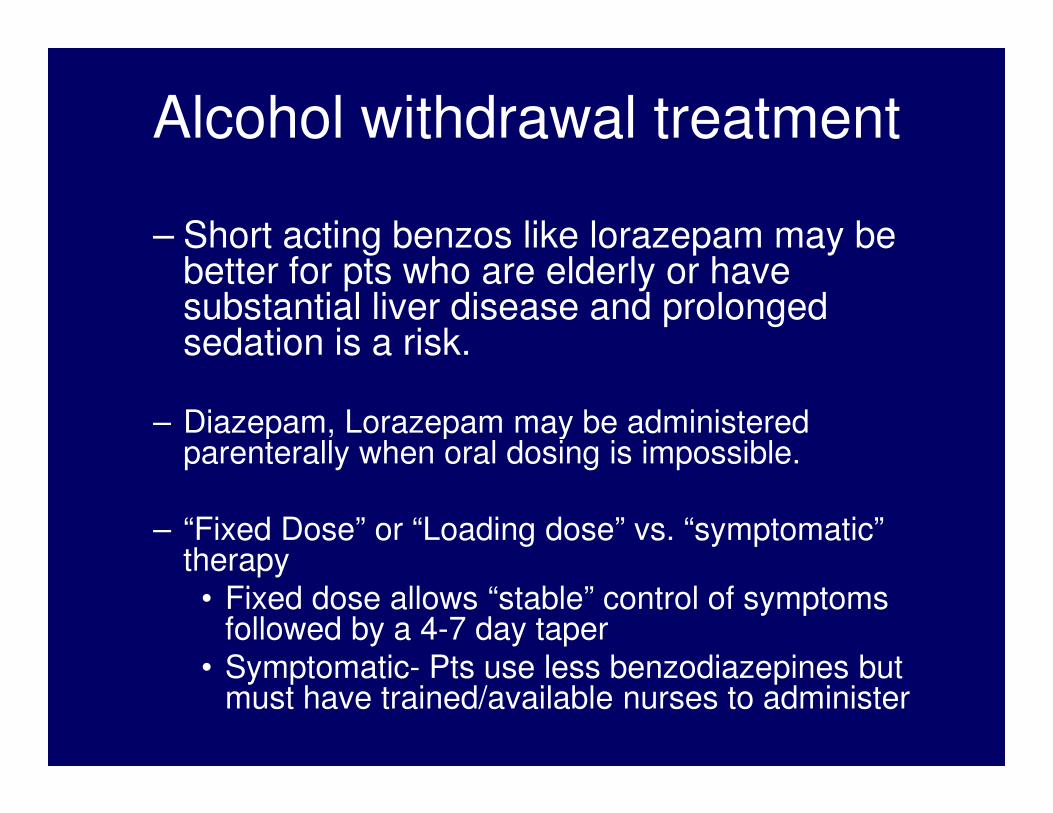
Alcohol withdrawal treatment
– Short acting benzos like lorazepam may be better for pts who are elderly or have substantial liver disease and prolonged sedation is a risk.
– Diazepam, Lorazepam may be administered – Diazepam, Lorazepam may be administered parenterally when oral dosing is impossible.
– “Fixed Dose” or “Loading dose” vs. “symptomatic” therapy
• Fixed dose allows “stable” control of symptoms followed by a 4-7 day taper
• Symptomatic- Pts use less benzodiazepines but must have trained/available nurses to administer
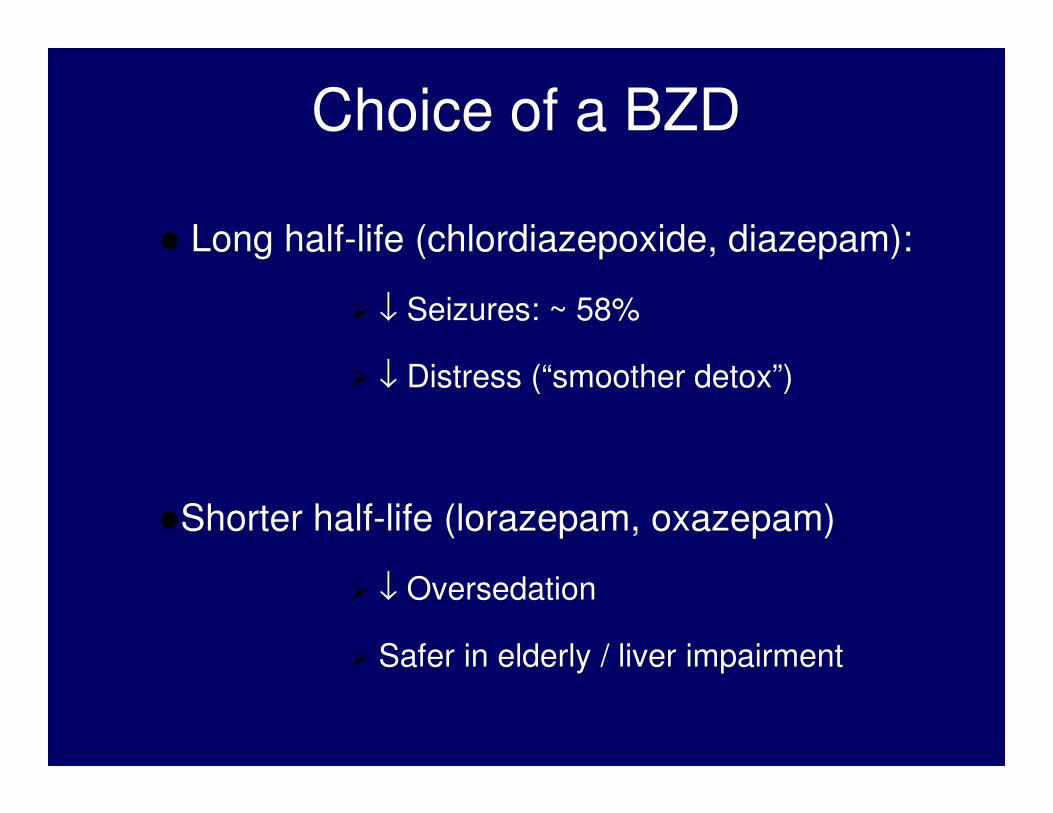
Choice of a BZD
� Long half-life (chlordiazepoxide, diazepam):
� ↓ Seizures: ~ 58%
� ↓ Distress (“smoother detox”)
�Shorter half-life (lorazepam, oxazepam)
� ↓ Oversedation
� Safer in elderly / liver impairment
Alcohol withdrawal treatment
• B-Blockers in conjunction with benzos to control persistent HTN and tachycardia. There is no evidence these improve outcome.
• Carbamazepine can be used to treat the seizures, this is done more in Europe than in the US.
• Haldol can be used to treat agitation and hallucinations
• Nutrition support: Thiamine to avoid Wernicke-Korskoff, Mg supplementation, folate if needed.
• Acamprosate, disulfiram appropriate for abstinence therapy NOT withdrawal
Detoxification
Alcohol Withdrawal• Autonomic dysfunction-Insomnia-Anxiety• Onset 8+ hrs, Peak 48hrs, Diminished 5dys,
Duration 3-6 months • Withdrawal Syndromes:• Withdrawal Syndromes:1. Mild, moderate or life-threatening severity
(increased severity with BAL>100mg/dl)2. 3% Withdrawal Seizures (w/in 48hrs of abstinence)3. Delirium Tremens (DTs) – Medical Emergency!
(w/in 48-72hrs of abstinence)(4-5% Prev., M&M<5% w/o tx, <1% w/tx)
Sample Medication Protocol
Days 1-2 : Lorezepan 1-2 mg three times a day
Days 3-4: Lorezepam 1-2 mg twice daily
Day 5: Lorezepam 1-2mg, daily
*Adjust dosage and duration for intoxication or prolonged withdrawalor prolonged withdrawal
• Adjunctive treatments:1. Seizure history: Tegretol 200mg/Neurontin 400mg (5dy
taper)
2. Sympathetic activity: Clonidine 0.1-0.2q8hrs (3-5dys)
3. Fluids, MVI, Thiamine
4. Manage co-morbid conditions
Carbamazepine and Valproate
• Effective in:� Mild to moderate AW / protracted AW
�↓↓↓↓ distress and faster return to work
� No abuse potential / alcohol interactions
� No toxicity in 7-day trials
• Limitations:� Not better than BZDs
� ↑↑↑↑ Side effects
� ↑↑↑↑ Cost
� Limited data in AW seizures/delirium
Other Agents
• Antipsychotics:� ↑↑↑↑ seizures, ↓↓↓↓ agitation
• ββββ-Adrenergic antagonists and clonidine:
� ↓↓↓↓ Autonomic activity, may hide impending � ↓↓↓↓ Autonomic activity, may hide impending seizures
• Magnesium:
� ↓↓↓↓ levels in AW, supplement does not ↓↓↓↓ severity
• Ethyl Alcohol:
� No evidence of efficacy, toxic + expensive
Nonpharmacological Treatment
• Quiet environment
• Nutrition and hydration:
� Oral thiamine (prevents Wernicke-Korsakoff) / folic acidacid
� Oral fluids / electrolytes
• Orientation to reality
• Brief interventions / motivate to change
• Referral to AA / relapse prevention tx.
Conclusions
• AW common complication in AD patients
• Clinicians must screen for AD / AW
• During AW, ↑ excitatory neurotramsmission• During AW, ↑ excitatory neurotramsmission
• If untreated AW can be deadly or lead to morbidity
• BZD most effective, safest and cheapest treatment
BENZODIAZEPINES
General Consideration
Sedative-hypnotic (Benzodiazepine) Detoxification
• Symptoms similar to alcohol but no objective measure/scoring system
• High risk of delirium, seizures and death • High risk of delirium, seizures and death requires treatment
• Sub-clinical symptoms may persist for months
• Tolerance develops within 3-4 weeks of regular use
• Onset of withdrawal symptoms determined by half-life of compound
Benzodiazepine
Detoxification guidelines:
• Slow-tapering of the compound or use of a longer acting benzodiazepine recommended
(i.e., Clonazepam TID with 10% tapering (i.e., Clonazepam TID with 10% tapering daily)
• Sedatives for insomnia (i.e. antidepressants)
• Avoid beta blockers (mask symptoms)
• Anti-seizure medications adjusted and monitored
General Consideration
Detoxification
• Symptoms similar to alcohol but no objective measure/scoring system
• High risk of delirium, seizures and death ---����requires treatment
Sedative-hypnotic (Benzodiazepine)
requires treatment
• Sub-clinical symptoms may persist for months
• Tolerance develops within 3-4 weeks of regular use
• Onset of withdrawal symptoms determined by half-life of compound
Barbiturate withdrawal
Symptoms may range from rebound insomnia
(from hypnotic doses) to delirium and seizures
(from higher doses) similar to those of alcohol
withdrawal
Management involves substitution of a long-
acting benzodiazepine (diazepam) to reduce
severity of symptoms and aid in slow and
careful tapering off of offending barbiturate
POPPY PLANTSPOPPY PLANTSOPIATE/OPIOID
Opiate Indications for Use
1. Addiction Maintenance Therapy
– Methadone (Pure Mu Opioid Agonist)
– Naltrexone (Opioid Antagonist)
– Buprenorphine (Opioid Agonist-– Buprenorphine (Opioid Agonist-
Antagonist)
– (N.B. LAMM now Minimally Available)
2. Pain Management
Opiate Withdrawal Syndrome
1. Not life threatening, Extremely uncomfortable
2. Symptom onset and duration, half-life
• Nausea and/vomiting
• Diarrhea
• Weakness
• Dilated Pupils
• Goose bumps2. Symptom onset and
duration, half-life dependent
3. Common Sns & Sxs:
• Yawning
• Sweating
• Tearing
• Abdominal Cramps
• Goose bumps
• Muscle twitching aches and pain
• Anxiety
• Insomnia
• Increased pulse
• Increased Resp rate
• Elevated Blood pressure
Opiate Detoxification
Key Considerations:
• Medical Detoxification = Standard of Care
• Methadone short-term substitution therapy = the preferred method of therapy = the preferred method of detoxification, but…
• Goal of treatment = reducing withdrawal discomforts, with or without Methadone or Narcotic Substitution
Opiate Detoxification
Levels of Care
• Inpatient Setting
1. Duration: 4-7 days
2. Usual dose to suppress
symptoms: 30-40mg/day
Methadone
• Outpatient Setting1. 21 day protocol
sufficient for most stable, motivated patients
2. 180 day protocol, done Methadone
3. Immediate Referral to
drug-free treatment
setting
4. Clonidine (Catapres) can
be considered an
effective alternative
treatment for inpatient
opioid detoxification but
not outpatient
2. 180 day protocol, done within an opioid agonist therapy program, should be considered to work on patients’ early recovery problems, while stabilized on relatively low dose (50-60mg) Methadone
Opiate Detoxification
Advantages of Methadone• Daily dosing due to 24 hour half-life, requiring
slower tapering schedule
• Long half-life safe for all opiates
• Safe in pregnancy• Safe in pregnancy
• May be used in combination with other medications for co-occurring disorders or mild withdrawal symptoms
• Decreases morbidity and mortality, hepatic damage, and HIV
• Exception: licensing requirements, very addictive
Opiate Detoxification
Methadone Guidelines:
• Stabilize Withdrawal: 5-10 mg prn every 4-6 hours to control objective signs of withdrawalwithdrawal
• Monitor respiratory depression and excessive sedation until stabilized
• Detoxification: Reduce by 10%/day after stabilized for 2-3 days
• Clonidine 0.1-0.2mg/day for duration
Opiate Detoxification
Pharmacological Guidelines (cont.)
Adjunctive Treatments• Nonsteroidal Anti-inflammatory Agents for pain and
fever (i.e. Tylenol, Aleve)• Alpha-adrenergic blocker for sympathetic
hyperactivity such blood pressure, nausea, vomiting, diarrhea, cramps and sweating hyperactivity such blood pressure, nausea, vomiting, diarrhea, cramps and sweating (i.e. Clonidine/Catapres)
• Antidiarreals and anti-emetics to control gastrointestinal symptoms (i.e. Bentyl, Phenergan)
• Antidepressants/Antipsychotic for dysphoria, anxiety and insomnia (i.e. Trazedone/Elavil/Seroquel with/without Lexapro)
• Psychotropics for co-morbid psychiatric conditions along with medications for medical conditions
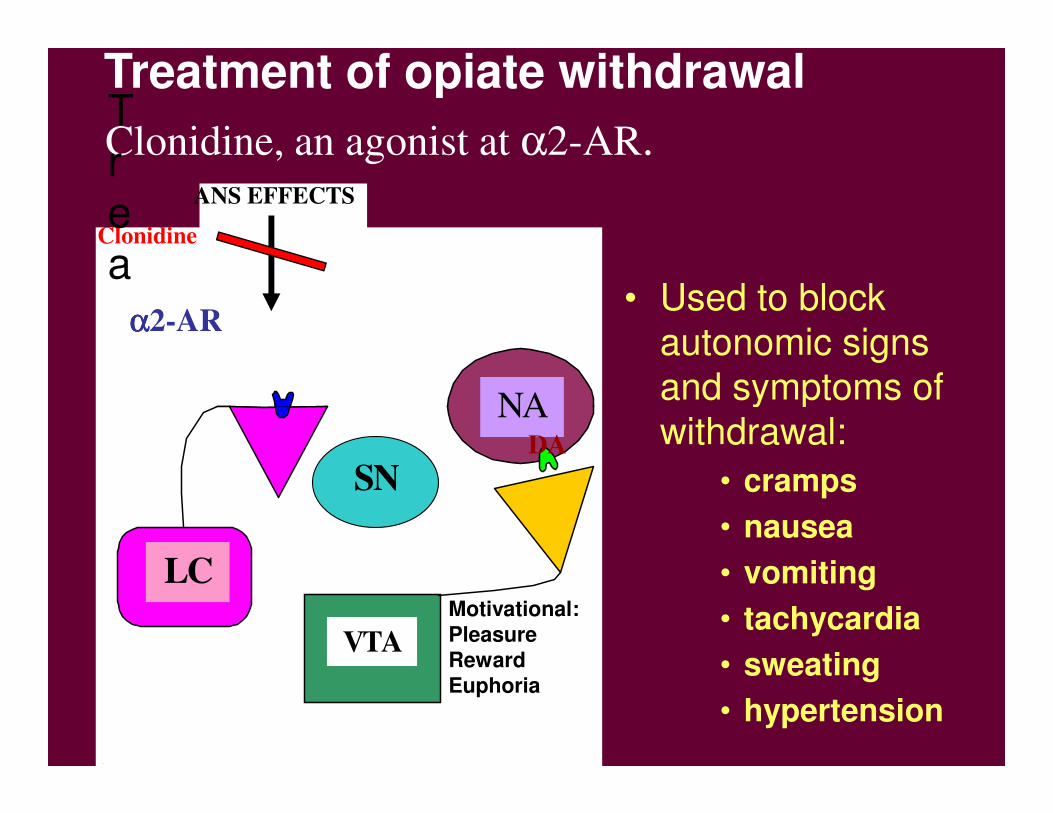
• Used to block
autonomic signs
and symptoms of
NA
ANS EFFECTS
Clonidine
NE
αααα2-AR
Clonidine, an agonist at α2-AR.Trea
Treatment of opiate withdrawal
and symptoms of
withdrawal:
• cramps
• nausea
• vomiting
• tachycardia
• sweating
• hypertension
SN
VTA
LC
NA
Motivational:
Pleasure
Reward
Euphoria
DA
Opiate Detoxification
Buprenorphine
• History: October 2000amended Control Substance Act: 30 patient/MD max for opioid dependence treatment, with DEA waiver; Goal: accessibility, expanded treatment capacity
• Partial mu agonist antagonist: ceiling effect • Partial mu agonist antagonist: ceiling effect (safer), sublingual absorption, Suboxone preferred
• Dosing instructions dependent on half-life of substituted opiate
• Average tolerable maintenance dose is 4-32 mg SL/day to every 3rd day
• Detox at 10%/day as tolerated
Medically-Assisted Withdrawal (Detoxification)
• Outpatient and inpatient withdrawal are both
possible
• How is it done?
– Switch to longer-acting opioid (e.g.,
buprenorphine)
• Taper off over a period of time (a few days to weeks depending upon the program)
• Use other medications to treat withdrawal symptoms
– Use clonidine and other non-narcotic medications
to manage symptoms during withdrawal
naloxone (Narcan)
• Competes for opiate receptor sites
• Has a shorter duration of action than narcotics, so it must be given repeatedly
The Clinical Assessment
The diagnosis of dependence is made through a careful patient history and physical examination, focusing on the following information:
• Drug type, route and duration of use, symptoms with cessation and last use
• Risk factors, symptoms and previous testing for blood-bourn pathogens
• Past Medical History and review of symptoms of chronic use such • Past Medical History and review of symptoms of chronic use such as malnutrition, tuberculosis infection, trauma, endocarditis, and sexually transmitted diseases
• Physical Examination to include vital signs, and cardiac status for evidence of fever, heart murmur, or hemodynamic instability; exam should focus on skin areas for scarring, atrophy, infection
• Laboratory Evaluation should include a complete blood count, comprehensive chemistry panel, HIV testing, EKG, Chest x-ray, screening for STD’s
• Urine Drug Screens and Breath Analysis (Alcohol)
Detoxification
The physiological process of withdrawal
from a substance of dependence
which requires medication management, careful monitoring, and careful monitoring, and
the availability of lifesaving emergency interventions.
β-Adrenoceptor and Dopamine Receptor Agonists
• Dobutamine
• Dopamine
Mechanism of Action:
Dobutamine
• Stimulation of cardiac β1−−−−adrenoceptors: ↑inotropy > ↑ chronotropy
• peripheral vasodilatation
• ↑ myocardial oxygen demand
Mechanism of Action: Dopamine
• Stimulation of peripheral postjunctional D1 and prejunctional D2 receptorsD2 receptors
• Splanchnic and renal vasodilatation
Therapeutic Use
• Dobutamine: management of acute
failure only
• Dopamine: restore renal blood in
acute failure
Adverse Effects
• Dobutamine
– Tolerance
– Tachycardia
• Dopamine• Dopamine
– tachycardia
– arrhythmias
– peripheral vasoconstriction