Embed Size (px)
Citation preview

Available online at www.sciencedirect.com
Journal of Electromyography and Kinesiology 19 (2009) e353–e361
www.elsevier.com/locate/jelekin
Reliability of a new virtual reality test to measurecervicocephalic kinaesthesia
Michael Kramer a, Marina Honold a, Kathrin Hohl b, Ulrich Bockholt c,Alexander Rettig c, Martin Elbel a, Christoph Dehner a,*
a Department of Trauma, Hand, Plastic and Reconstructive Surgery, Ulm University, Ulm, Germanyb Institute for Biometry, Ulm University, Ulm, Germany
c Fraunhofer Institute for Computer Graphics, Darmstadt, Germany
Received 15 December 2007; received in revised form 20 May 2008; accepted 21 May 2008
Abstract
The aim of this study was to investigate the cervicocephalic kinaesthesia of healthy subjects for gender and age effects and its reliabilityin a new virtual reality test procedure. 57 healthy subjects (30 male, 27 females; 18-64 years) were immersed into a virtual 3D scene via aheadmounted display, which generated specific head movements. The joint repositioning error was determined in a static and dynamictest at the times T0, T1 (T0 + 10 minutes) and T2 (T0 + 24 hours). The intrasession reliability (T0-T1) and the intersession reliability (T0-T2) were analysed. In both tests no gender- or age-specific effects were found. In the overall group the means of the static test were 6.2�-6.9� and of the dynamic test were 4.5�-4.9�. The intratest difference in the static test was -0.16� and the intertest difference was 0.47�. Theintratest difference in the dynamic test was 0.42� and the intertest difference was 0.37�. The static and dynamic test was reproducible inhealthy subjects, with minor deviations, irrespective of gender and age. The smaller interindividual differences in the dynamic test couldbe beneficial in the comparison of healthy individuals and individuals with cervical spine disorders.� 2008 Elsevier Ltd. All rights reserved.
Keywords: Cervical spine; Proprioception; Joint repositioning error
1. Introduction
Besides the execution of voluntary head movements(Takebe et al., 1974; Conley et al., 1997; Sommerich etal., 2000), the main function of the cervical spine is the sta-tic and dynamic stabilisation of the head in space (Crom-well et al., 2001; Cromwell et al., 2001). This is necessaryin order to enable optimal function of the sense organslocated in the head. For example, a still head positionmakes it easier to fix the gaze on an object, and optimisesthe influence of the equilibrium sense on locomotion.
The balance of the head is ensured by complex neuro-physiological regulation and control mechanisms betweenthe sense organs of the head and the neck muscles. In par-
1050-6411/$ - see front matter � 2008 Elsevier Ltd. All rights reserved.
doi:10.1016/j.jelekin.2008.05.005
* Corresponding author.E-mail address: [email protected] (C. Dehner).
ticular, proprioceptive, visual, and vestibular effects play arole. As regards the visual effects, eye movements as aresult of afferent information from the neck muscles (cerv-ico-ocular reflex) have been demonstrated (Barlow andFreedman, 1980), as have muscle reactions to visual stimuli(Keshner et al., 1995). Also, activating and inhibiting stim-uli from the vestibular system – the so-called ‘‘vestibulocol-lic reflex” – have been verified (Wilson et al., 1995; Shinodaet al., 1997). Furthermore, proprioceptive afferents frommuscle spindles and sense organs of the neck muscles inturn lead to specific reflex responses (cervicocollic reflex)of other neck muscles that are involved in maintainingthe balance of the head (Peterson et al., 1985; Goldbergand Peterson, 1986; Dutia, 1988; Richmond and Loeb,1992).
The above-mentioned visual, vestibular, and proprio-ceptive control systems are coordinated in the upper

e354 M. Kramer et al. / Journal of Electromyography and Kinesiology 19 (2009) e353–e361
cervical spine (Taylor and McCloskey, 1988). This inter-action is called cervicocephalic kinaesthesia (CK)(Barnes, 1979; Heikkila and Astrom, 1996; Heikkilaand Wenngren, 1998; Kristjansson et al., 2001). In pop-ulations with chronic neck pain (Revel et al., 1991) andpatients with chronic whiplash associated disorders (Hei-kkila and Astrom, 1996; Loudon et al., 1997; Heikkilaand Wenngren, 1998; Treleaven et al., 2003; Kristjanssonet al., 2004), a reduced CK was observed when comparedto healthy subjects (Glencross and Thornton, 1981; Lep-hart et al., 1997). Disturbances of the CK can have anadverse effect on daily, occupational, and sports activities(Taylor and McCloskey, 1988; Loudon et al., 1997).These studies have greatly changed the understandingof the cervical spine, which had long been focused onmechanics, and have shown that clinical importance mustbe attached to the neurophysiological properties of thecervical spine.
To date, joint repositioning error (JRE) has been stud-ied as a quantitative measure of CK in three different testprocedures. The ‘‘head repositioning test” (HRT) by Revelet al. (1991) measures the ability of a subject to relocate thehead to the neutral position after a movement of the cervi-cal spine. However, it could be demonstrated that peoplecan perform common movements which are stored inlong-term memory even without proprioceptive informa-tion (Rothwell et al., 1982; Gandevia et al., 1992; Nougieret al., 1996). Relocating to neutral head position, isassumed to be such a memory stored movement task(Kristjansson et al., 2001), which is why the HRT is a ques-tionable test for CK.
The HRT was later augmented by Loudon et al. (1997)who replaced the neutral position with an arbitrary headposition as the target in their ‘‘head to target test” (HTT).However, this poses technical difficulties concerning thespecification of the target positions. In previous studies,the subject’s head was guided to the target position intwo ways. Some authors Loudon et al. (1997); Lee et al.(2006) used the examiner’s hands to position the head.With this method, additional sensory information is deliv-ered via the skin surface by the examiner’s hands (McNairand Heine, 1999; Ulkar et al., 2004). By eliminating theforce of gravity and specifying the direction of movement,the examiner also changes the perception of the sense ofeffort, which can change the ability to relocate positions(Winter et al., 2005; Walsh et al., 2006). One study (Krist-jansson et al., 2001) used a monitor that displayed a spec-ified target point which the subject had to locate him/herself. With this technique, the results are not influencedby the examiner, however, they are reduced to a smallrange of motion due to the size of the monitor. Further,it could be shown that deafferented patients can suffi-ciently control simple single joint movements solely bylong-term memory (Gandevia et al., 1992; Nougier etal., 1996). These results raise doubts about the validityof a test using a simple motion task to detect a proprio-ceptive deficit. A test using a more complex motion task
may therefore be more appropriate to detect propriocep-tive deficits.
Kristjansson et al. (2004) developed such a test proce-dure in which the subject has to follow a moving targeton a computer screen by moving his/her head. Directionand speed vary unpredictably, so that this complex motionpattern cannot be controlled without proprioceptiveinformation.
Furthermore the reliability of all tests was either notinvestigated at all, (Heikkila and Wenngren, 1998; Rixand Bagust, 2001; Treleaven et al., 2003; Treleaven et al.,2006), not satisfactorily met (Strimpakos et al., 2006) ornot adequately described from a statistical point of view(Revel et al., 1991; Loudon et al., 1997; Kristjansson etal., 2004; Lee et al., 2006).
The objective of this study was to develop a new measur-ing instrument for CK that is independent of examinerinfluences and allows examination of CK within the entirerange of motion. A new virtual reality test procedure wasdeveloped for this purpose. During the test, the subject isimmersed into a virtual scene via a head-mounted display(HMD). In this scene, the subject performs a conventionalHTT under static conditions and a new more complexdynamic test.
As a first step, we wanted to gain experience concerningthe practicability, age and gender dependence and reliabil-ity of the two virtual reality tests in healthy individuals inorder to answer the following questions:
1. Does the gender or age of healthy subjects have an effecton the JRE in a static and in a dynamic virtual realitytest?
2. How good is the reliability of the JRE of healthy sub-jects in a static virtual reality test?
3. How good is the reliability of the JRE of healthy sub-jects in a dynamic virtual reality test?
2. Material and methods
2.1. Subjects
Volunteers (57) – 30 male and 27 female healthy subjects withages of 18–64 years – were enrolled in the study. Written consentfor participation was obtained from all subjects, along withwritten approval from the ethics committee for the conduct of thestudy. Freedom from pain and unrestricted mobility of the cer-vical spine were prerequisites for participation. Past injuries ofthe cervical spine, cranium, or eyes, neurological symptoms, orprevious cervical spine surgery were exclusion criteria and led tothe exclusion of four subjects from the study. The participantswere instructed not to engage in any strenuous physical activitiesfrom two days before the initial measurement until the lastmeasurement, in order to rule out a possible influence of musclefatigue. The median age of the males (n = 30) was 27.5 years(minimum 18 years/maximum 64 years) and the median age ofthe females (n = 27) was 25 years (minimum 18 years/ maximum52 years). Each subject participated in three measurements at thetime T0, at the time T1 (T0 + 10 min) and at the time T2(T0 + 24 h).

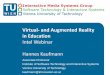
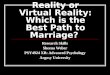
Fig. 2. Virtual scene as seen by the participant. In the static test the globeleads the subject’s head to a specific position. In the dynamic test theparticipant has to follow the moving globe with the white rhomb.
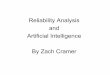
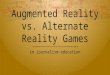
Fig. 3. Diagram of the field of vision in the static test. The outer linedelineates the field of vision at maximal range of motion. The areahighlighted in grey corresponds to the field of vision between 50% and 80%
M. Kramer et al. / Journal of Electromyography and Kinesiology 19 (2009) e353–e361 e355
2.2. Experimental design
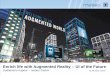
The subject was seated upright on a chair in a darkened,soundproofed room (Fig. 1). During the test, the subjects wereasked to follow a visual target in a virtual scene. The subjects wereimmersed into the virtual outer space environment via a head-mounted display (HMD) equipped with a motion tracking system(Fig. 2). The subjects were then asked to follow the paths ofmotion of a virtual planet in this virtual outer space environment.For this task, the subject had to try to track the virtual globe asclosely as possible with a white diamond whose position in thevirtual scene corresponded to the head position (Fig. 2). A fixedeye position was maintained due to the short distance between thesubject’s eyes and the monitors in the HMD, so this task couldonly be accomplished with head movements. A 3Space Fastraksystem (Polhemus Incorporated, Colchester, Vermont, USA.) wasused for head movement tracking (Fig. 1). This system’s accuracyfor the measurement of orientations is 0.2� (Percy and Hindel,1989).
2.3. Measurement technique and data recording
Before each measurement, the field of vision of the subject wasdetermined in flexion, extension, right and left rotation, and thepositions halfway between each of these directions and the next.The field of vision in the HMD was divided into eight sectors, onebetween each pair of adjacent directions (Fig. 3). Each subjectcompleted one practice run of each test before the data wererecorded.
Two different tests were performed
(a) Static head to target test to assess the sense of position.(b) Dynamic test to assess the visually triggered sense of
motion.
2.3.1. Static test
At the beginning of the test, the head was in neutral position.The globe started from this position and led the subject’s head toa specific position within Sector 1. The software selected a pre-defined and constant position at an arbitrary location between
Fig. 1. Photo of the experimental setup demonstrating a measuringprocedure.
range of motion. The numbers define the eight different measuring areas.
50% and 80% of the field of vision. The specified target was thesame at each measuring time (T0, T1, T2) for each subject. Theglobe stayed at this end point for three seconds, after which it ledthe subject’s head back to the neutral position. The globe thendisappeared and the subject was asked to find the end positionagain without visual guidance (Fig. 3). The difference between theactual and required head position values was determined. It wasrepresented as angles and called ‘‘static joint repositioning error”
(SJRE). This process was repeated one time for each of the eightsectors and the median of the SJREs of all eight sectors wascalculated (SJREMed).
2.3.2. Dynamic test
In this test, the globe travels along a path shaped like a figureeight on its side. To make the test less predictable, four standar-dised speed changes were included in each figure-eight task. Whilethe subject followed the specified target, the angle between theactual and required head position was determined every 1/100 sthroughout the motion cycle. This angle was called ‘‘dynamic

Table 1Joint repositioning error in the static and dynamic test in all subjects
T0 T1 T2
Mean (�) SD (�) Mean (�) SD (�) Mean (�) SD (�)
SJREMed 6.7 2.6 6.9 2.6 6.2 2.4DJREMed 4.9 1.6 4.5 1.3 4.6 1.4DJRE5% 1.7 0.9 1.5 0.8 1.4 0.7DJRE95% 9.8 2.9 8.7 2.3 8.7 2.4
T0: initial measurement; T1: measurement at T0 + 10 min; T2: measure-ment at T0 + 24 h; SD: standard deviation; SJRE: static joint reposi-tioning error; DJRE: dynamic joint repositioning error; Med: Median; 5%:5%-percentile; 95%: 95%-percentile; The p-values range between 0.10 and1.00.
Table 2Joint repositioning error in the static and dynamic test separated for malesand females
Males n = 30 Females n = 27
Mean (�) SD (�) Mean (�) SD (�)
Static
T0 SJREMed 6.3 2.6 7.1 2.7T1 SJREMed 6.7 2.8 7.0 2.4T2 SJREMed 6.0 2.0 6.4 2.8
Dynamic
T0 DJRE5% 1.6 0.7 1.7 1.1T0 DJREMed 4.6 1.1 5.3 1.9T0 DJRE95% 8.9 1.8 10.8 3.6T1 DJRE5% 1.5 0.9 1.4 0.8T1 DJREMed 4.4 1.3 4.6 1.3T1 DJRE95% 8.3 2.0 9.1 2.6T2 DJRE5% 1.3 0.7 1.6 0.7T2 DJREMed 4.4 1.3 4.8 1.5T2 DJRE95% 7.9 2.0 9.6 2.5
T0: initial measurement; T1: measurement at T0 + 10 min; T2: measure-ment at T0 + 24 h; SD: standard deviation; SJRE: static joint reposi-tioning error; DJRE: dynamic joint repositioning error; Med: Median; 5%:5%-percentile; 95%: 95%-percentile. The p-values range between 0.15 and1.00.
e356 M. Kramer et al. / Journal of Electromyography and Kinesiology 19 (2009) e353–e361
joint repositioning error‘‘ (DJRE). The median (DJREMed) andthe 5% (DJRE5%) and 95% (DJRE95%) percentiles of theapproximately 700 DJRE values were determined for each sub-ject. We regard the DJRE as a measure of CK. This parameter isprobably influenced by visual, proprioceptive and vestibularafferents.
2.4. Statistical analysis
The above-mentioned parameters were presented withmean ± standard deviation (SD). Intraindividual changes of theparameter between T0 and T1 or T0 and T2 were analyzed usingthe paired t test (significance level p < 0.05). Furthermore theparameters were investigated for gender- and age-specific effects.For this purpose, the subjects were divided into three age cate-gories: 18–29 years = age category I (n = 38), 30–45 years = agecategory II (n = 9), and 46–64 years = age category III (n = 10).A one-way ANOVA with JRE as dependent variable and age,respectively, gender as independent variable was performed ateach time point and for each testing method. The p-values (sig-nificance level p < 0.05) have been adjusted according to themethod of Bonferroni–Holm.
The intrasession reliability was described by comparing thetimes T0 and T1 and the intersession reliability was described bycomparing the times T0 and T2. A repeated measures ANOVAwas performed with the JRE as the dependent variable and timeand subject as independent variables as well as the interaction oftime and subject for the calculation of the intracategory correla-tion coefficient (ICC (3.1)) and the 95% confidence interval (CI)(Shrout and Fleiss, 1979). Bland & Altman plots (Bland andAltman, 1986) (see Appendix) were additionally generated for agraphic representation of the variance of the JREs. Based on thisthe mean and the standard deviation of the differences betweenthe T0 and T1 (or T2) values of a parameter, the 95% CI, theupper limit (UL) (= mean + 1.96 � SD), and the lower limit (LL)(= mean � 1.96 � SD), were calculated for the static and dynamictests and listed in tables.
3. Results
The procedure took between 8:32 min and 11:14 min attime T0 and between 4:02 min and 4:32 min at times T1and T2. None of the subjects complained about anyinconveniences.
The means of the SJREMed, DJREMed DJRE5% andDJRE95% of all subjects did not differ significantly betweenthe three time points of measurement (Table 1). No genderor age effect on the SJRE and DJRE was found (Tables 2and 3).
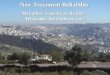
Both the ICC values and the Bland & Altman plots indi-cated a slightly better intrasession than intersession reliabil-ity in both tests. While the ±2SD range of the deviation ofthe SJREMed between T0 and T1 is 8.82�, this range is only5.64� for the DJREMed. Between T0 and T2, the ±2SDrange of the deviation of the SJREMed is 10.13� while thatof the DJREMed is 6.01�. When considering the ICCs, thereliability of the static test (T0 � T1: 0.63 and T1 � T2:0.48) was higher than that of the dynamic test (T0 � T1:0.50 and T1 � T2: 0.46). Table 4 lists the values obtainedfrom the Bland & Altman plots and the ICCs for the static
test. Table 5 shows the values of the dynamic test. Figs. 4and 5 show the Bland & Altman plots for the SJREMed
and for the DJREMed, respectively.
4. Discussion
The results of this study show that the subjects’ genderor age did not have any effect on the SJRE or DJRE. Theseresults coincide with those of earlier studies which alsofailed to find a gender (Heikkila and Astrom, 1996) orage effect (Heikkila and Wenngren, 1998; Rix and Bagust,2001) on the JRE.
The results of our static test, which corresponds to anHTT, are compared with those of previous studies in Table6. The means of the SJRE of all studies range from 0.73� to7.19�, and all studies have comparable SDs. As neither agenor gender effects on the JRE have been observed in the lit-erature to date, the differences cannot be explained by thecomposition of the study populations but are more likely

Table 3Joint repositioning error in the static and dynamic test separated for three age categories
Age category I 18–29 years n = 38 Age category II 30–45 years n = 9 Age category III 46–64 years n = 10
Mean (�) SD (�) Mean (�) SD (�) Mean (�) SD (�)
Static
T0 SJREMed 6.6 2.1 7.4 4.4 6.5 2.7T1 SJREMed 6.2 1.8 8.2 4.5 8.1 2.4T2 SJREMed 5.8 2.0 6.9 2.7 7.3 3.3
Dynamic
T0 DJRE5% 1.6 0.9 1.6 0.6 1.8 1.1T0 DJREMed 4.7 1.5 5.6 1.4 5.1 1.8T0 DJRE95% 9.5 2.6 10.7 2.7 10.3 4.3T1 DJRE5% 1.4 0.8 1.8 1.1 1.3 0.5T1 DJREMed 4.4 1.3 4.9 1.7 4.6 1.0T1 DJRE95% 8.5 2.3 9.2 2.9 8.7 1.9T2 DJRE5% 1.4 0.7 1.6 0.9 1.5 0.6T2 DJREMed 4.4 1.3 5.1 1.9 4.7 1.3T2 DJRE95% 8.5 2.1 10.0 3.1 8.5 2.6
T0: initial measurement; T1: measurement at T0 + 10 min; T2: measurement at T0 + 24 h; SD: standard deviation; SJRE: static joint repositioning error;DJRE: dynamic joint repositioning error; Med: Median; 5%: 5%-percentile; 95%: 95%-percentile. The p-values range between 0.76 and 1.00.
Table 4Intracategory correlation coefficients and Bland & Altman plots for the joint repositioning error in the static test
ICC Bland & Altman
ICC (�) 95% CI (�) Mean (�) 95% CI Mean (�) SD (�) LL (�) UL (�)
T0 � T1SJREMed 0.63 0.45–0.77 �0.16 �0.76–0.44 2.25 �4.57 4.25
T0 � T2SJREMed 0.48 0.25–0.65 0.47 �0.21–1.16 2.58 �4.59 5.54
ICC: intracategory correlation coefficient; 95% CI: 95% confidence interval; SD: standard deviation; LL: lower limit (= mean � 1.96 � SD); UL: upperlimit (UL) (= mean + 1.96 � SD); T0: initial measurement; T1: measurement at T0 + 10 min; T2: measurement at T0 + 24 h; SJRE: static joint reposi-tioning error; Med: Median.
Table 5Intracategory correlation coefficients and Bland & Altman plots for the joint repositioning error in the dynamic test
ICC Bland & Altman
ICC (�) 95% CI (�) Mean (�) 95% CI Mean (�) SD (�) LL (�) UL (�)
T0 � T1DJRE5% 0.31 0.05–0.52 0.18 �0.09–0.45 1.02 �1.81 2.17DJREMed 0.50 0.25–0.66 0.42 0.04–0.80 1.44 �2.40 3.24DJRE95% 0.42 0.12–0.57 1.13 0.38–1.88 2.83 �4.42 6.68
T0 � T2DJRE5% 0.13 �0.15–0.36 0.21 �0.07–0.49 1.05 �1.84 2.27DJREMed 0.46 0.21–0.63 0.37 �0.04–0.77 1.54 �2.64 3.37DJRE95% 0.51 0.23–0.64 1.07 0.37–1.78 2.65 �4.12 6.26
ICC: intracategory correlation coefficient; 95% CI: 95% confidence interval; SD: standard deviation; LL: lower limit (= mean � 1.96 � SD); UL: upperlimit (UL) (= mean + 1.96 � SD); T0: initial measurement; T1: measurement at T0 + 10 min; T2: measurement at T0 + 24 h; DJRE: dynamic jointrepositioning error; Med: Median.
M. Kramer et al. / Journal of Electromyography and Kinesiology 19 (2009) e353–e361 e357
the result of the different test procedures. Kristjansson etal. (2001) showed that the JRE in an HTT is more thantwice as large as in an HRT. Consequently, modificationsof the test setting appear to have a considerable effect onthe JRE. A direct comparison of the absolute JRE valuesbetween studies is thus only possible if the test conditionsare identical.
Based on the maximal individual deviations (5.54�)observed in the intrasession and intersession comparisons(see Table 4) in the static test and an estimated range ofmotion of 120�–180� for right/left rotation and 100�–60�for flexion/extension, the individual difference betweentwo time points is between 3.1% and 5.5% of the maximalrange of motion. In the study conducted by Strimpakos,

Fig. 4. Bland & Altman plots of the static test. Panel A – intrasession reliability (T0 � T1) and Panel B – intersession reliability (T0 � T2). SJRE: staticjoint repositioning error; Med: median; SD: standard deviation; T0: initial measurement; T1: measurement at T0 + 10 min; T2: measurement at T0 + 24 h.
Fig. 5. Bland & Altman plots of the dynamic test. Panel A – intrasession reliability (T0 � T1) and Panel B – intersession reliability (T0 � T2). DJRE:dynamic joint repositioning error; Med: median; SD: standard deviation; T0: initial measurement; T1: measurement at T0 + 10 min; T2: measurement atT0 + 24 h.
Table 6Comparison of the joint repositioning error, intracategory correlation coefficients and Bland & Altman plots under static test conditions
Author Test n SJRE T0 SJRE T2 ICC Bland and Altman
Mean SD Mean SD Mean SD
Revel et al. (1991) HRT 30 3.37–3.5 0.73–0.82 – – – – –Kristjansson et al. (2001) HRT 20 2.16–3.54 1.36–2.75 2.26–3.55 1.18–2.61 0.35–0.82 IncompleteLoudon et al. (1997) HTT 11 0.73–1.57 1.55–2.77 – – – – –Kristjansson et al. (2001) HTT 20 5.03–7.19 3.37–3.87 5.39–5.81 3.71–4.20 0.69–0.74 IncompleteStrimpakos et al. (2006) HTT 35 2.2-4.4* 1.7–4.0* 1.7–4.5* 1.8–3.2* �0.01–0.35 – –Our results HTT 57 6.7 2.6 6.2 2.4 0.48 0.47 2.58
SJRE: static joint repositioning error; T0: initial measurement; T2: measurement at T0 + 24 h; ICC: intracategory correlation coefficient; HRT: headrepositioning test; HTT: head to target test; SD: standard deviation; –: no data available; * These values have been taken from the graphs of thepublication and are thus not completely accurate.
e358 M. Kramer et al. / Journal of Electromyography and Kinesiology 19 (2009) e353–e361
the greatest intersession differences (only reported for theinter-examiner test) are observed in rotation (�8.5�),the second greatest are observed in flexion (�6�), and thesmallest are observed in lateral flexion (�2�). As the range
of motion for rotation is greater than the range of motionin flexion/extension and this in turn is greater than in lat-eral flexion, a dependence of the JRE on the range ofmotion can be assumed. The fluctuations of the SJREs in

Table 7Comparison of the joint repositioning error, intracategory correlation coefficients and Bland & Altman plots under dynamic test conditions
Author n DJRE T0 DJRE T2 ICC Bland and Altman
Mean SD Mean SD Mean SD
Kristjansson et al. (2004) 10 3.97–4.24 mm 0.93–1.10 mm 3.90–4.11 mm 1.05–1.17 mm 0.60–0.77 mm 0.01 mm 0.64 mmOur results 57 5.4� 1.4� 4.8� 1.5� 0.46 0.37� 1.54�
DJRE: dynamic joint repositioning error; T0: initial measurement; T2: measurement at T0 + 24 h; ICC: intracategory correlation coefficient; SD: standarddeviation.
M. Kramer et al. / Journal of Electromyography and Kinesiology 19 (2009) e353–e361 e359
previous studies (Table 6) could, at least partly, beexplained by this relation. This observation requires fur-ther investigations; however, if such a relation was con-firmed in future studies, an interpretation of the SJREwould hardly be possible without data on the field of visionand the specified target angle.
It is not possible to compare the intrasession reliabilityof the SJRE with that of other studies, as the intrasessionreliability has not been investigated in previous studies.Up to now, the intersession reliability has only been inves-tigated in very small populations.In most of these studies, itis not defined which type of ICC has been calculated sothat the comparison of ICC values is hardly possible (seealso Table 6).
A dynamic test has only been described in one previousstudy which was conducted by Kristjansson et al. (2004).Table 7 shows the results of this study in comparison withour results. In the Kristjansson study, the subjects trackeda black target dot with a blue dot on a remote computermonitor. Using an HMD, as in our study, constituted animportant improvement under dynamic test conditions.As the distance between the eyes and the monitor is verysmall with the HMD, it is not possible to follow the targetwith eye movements in the current study. With the conven-tional technique in the Kristjansson study, however, eyemovements are possible and could cause a systematic error.
In view of these results, the dynamic test could be ofclinical interest, as the DJREMed has a smaller interindivid-ual variance at all measuring times and lower SDs as com-pared to the SJREMed. The Bland & Altman plots show anupper limit between repeated measurements of 337�, corre-sponding to an error of 1.9–3.4% of maximal range ofmotion. A smaller variance of the DJREMed within a pop-ulation of healthy subjects is also evident in the Kristjans-son study (Kristjansson et al., 2004) and is an importantcharacteristic if the parameter is to be used for the distinc-tion between healthy individuals and patients.
So far, it could be shown that tests which place lesserdemands on the proprioceptive system (HRT) have betterICC values than more proprioceptively demanding tests(HTT) (Kristjansson et al., 2001). While HRT and HTTcan distinguish between healthy individuals and patientswith neck problems (Revel et al., 1991; Heikkila andAstrom, 1996; Loudon et al., 1997; Heikkila and Wenn-gren, 1998; Treleaven et al., 2003), Kristjansson’s dynamictest has not yet been investigated for this ability. The abil-ity to distinguish between healthy and diseased individuals
could depend on the demands placed on the proprioceptivesystem. Mean JRE in people with neck pain is 1.4- to 1.7-fold higher compared to healthy controls measured with anHRT (Heikkila and Astrom, 1996; Heikkila and Wenn-gren, 1998). This difference seems to be more than double(2.9-fold) in an HTT (Loudon et al., 1997). Due to the con-stant change in speed and direction of motion in a veryshort time, the demand placed on the proprioceptive sys-tem by our dynamic test is probably greater as comparedto an HTT. Due to this fact the dynamic test could possiblyattain higher specificity and sensitivity in the comparison ofneck pain patients with a normal population. But this ques-tion has to be the issue of further studies.
The ICCs and the Bland & Altman plots always yieldedcontrasting results in our study. When considering theICCs, the reliability of the static test was higher than thatof the dynamic test. The Bland & Altman plots, on theother hand, indicated that the differences in the DJREbetween two measuring times were smaller as comparedto the SJRE, from which a better reproducibility of theDJRE can be deduced as compared to the SJRE. A similardiscrepancy in results between ICCs and plotting of thesame data has been observed before by Kristjansson etal. (2004). The fact that the ICCs and the Bland & Altmanplots can lead to contradictory statements is explained bythe mathematical calculation of the ICC and the data pre-sentation of the Bland & Altman plots (see Appendix). Itshows the importance of not using ICCs as the only reli-ability measure for repeated measures in clinical researchbecause a single number can not demonstrate as much asa visual demonstration of the data. Various authors there-fore recommend that the ICC should never be consideredalone to prevent any misinterpretation of results (Krist-jansson et al., 2001; Lee et al., 2006; Strimpakos et al.,2006). Therefore in case of contradictory results betweenICC and the Bland & Altman plots, one should not relyon ICC values and rather have a look at the more detailedinformation of the plots. The plots show small discrepan-cies between repeated measurements and therefore a goodreliability of SJRE and even a better reliability of DJRE.
The procedure presented makes it possible to gain infor-mation about the position and movement control of thecervical spine in a very short time. The advantages com-pared to currently used techniques are that the virtual real-ity technique allows the specification of target points in theentire range of motion of the cervical spine without anyexaminer effect on proprioceptive perception.

e360 M. Kramer et al. / Journal of Electromyography and Kinesiology 19 (2009) e353–e361
The practicability and reliability of both tests have beendemonstrated. Whether one of them will have true signifi-cance for clinical routine now depends on how well theycan distinguish between healthy individuals and popula-tions with neck disorders. This will have to be investigatedin further studies.
Acknowledgement
The experiments comply with the current laws of Ger-many and were performed inclusive of ethics approval.
Appendix
ICC(3.1)
ICCð3:1Þ ¼ BMS� EMS
BMSþ ðk � 1Þ � EMS
BMS (‘‘between target mean square”) represents the vari-ance of the results between subjects and EMS (‘‘residualmean square error”) represents the variance of the mea-sured values of an individual subject. The parameter k rep-resents the number of measuring times (Shrout and Fleiss,1979). With two measuring times, the following equation isobtained for the calculation of the ICC(3.1):
ICCð3:1Þ ¼ BMS� EMS
BMSþ EMS
If the variance of the measured values between subjects andthe variance within a subject are similarly high, this resultsin a small ICC (Rankin and Stokes, 1998). If both quanti-ties are small, the reliability is good; however, the calcula-tion results in a small ICC(3.1) value.
Bland & Altman plots
To assess reliability in detail, a plot of the differencebetween two measurements against their mean of eachsubject was suggested by Bland and Altman (1986). Themean of the measurements should be close to zerobecause otherwise the first measurement would affectthe second or the process of measurement would alterthe quantity. The advantage of this plot over a simpleplot of the measurements of one time point against theother time point is that between-measurement differenceswill be easier to assess. The Bland & Altman plot showsclearly if the difference of measurements of a subject withgreater JRE is also greater than for a subject with smallerJRE. The plot shows a good reliability if the mean of thepoints is close to zero and the variance of the differencesis small.
References
Barlow D, Freedman W. Cervico-ocular reflex in the normal adult. ActaOtolaryngol 1980;89(5–6):487–96.
Barnes GR. Vestibulo-ocular function during co-ordinated head and eyemovements to acquire visual targets. J Physiol 1979;287:127–47.
Bland JM, Altman DG. Statistical methods for assessing agreementbetween two methods of clinical measurement. Lancet 1986;1(8476):307–10.
Conley MS, Stone MH, Nimmons M, Dudley GA. Resistance trainingand human cervical muscle recruitment plasticity. J Appl Physiol1997;83(6):2105–11.
Cromwell RL, Newton RA, Carlton LG. Horizontal plane head stabil-ization during locomotor tasks. J Mot Behav 2001;33(1):49–58.
Cromwell RL, Aadland-Monahan TK, Nelson AT, Stern-Sylvestre SM,Seder B. Sagittal plane analysis of head, neck, and trunk kinematicsand electromyographic activity during locomotion. J Orthop SportsPhys Ther 2001;31(5):255–62.
Dutia MB. Interaction between vestibulocollic and cervicocollic reflexes:automatic compensation of reflex gain by muscle afferents. Prog BrainRes 1988;76:173–80.
Gandevia SC, McCloskey DI, Burke D. Kinaesthetic signals and musclecontraction. Trends Neurosci 1992;15(2):62–5.
Glencross D, Thornton E. Position sense following joint injury. J SportsMed Phys Fitness 1981;21(1):23–7.
Goldberg J, Peterson BW. Reflex and mechanical contributions to headstabilization in alert cats. J Neurophysiol 1986;56(3):857–75.
Heikkila H, Astrom PG. Cervicocephalic kinesthetic sensibility in patientswith whiplash injury. Scand J Rehabil Med 1996;28(3):133–8.
Heikkila HV, Wenngren BI. Cervicocephalic kinesthetic sensibility, activerange of cervical motion, and oculomotor function in patients withwhiplash injury. Arch Phys Med Rehabil 1998;79(9):1089–94.
Keshner EA, Cromwell RL, Peterson BW. Mechanisms controllinghuman head stabilization. II. Head–neck characteristics duringrandom rotations in the vertical plane. J Neurophysiol 1995;73(6):2302–12.
Kristjansson E, Dall’Alba P, Jull G. Cervicocephalic kinaesthesia:reliability of a new test approach. Physiother Res Int 2001;6(4):224–35.
Kristjansson E, Hardardottir L, Asmundardottir M, Gudmundsson K. Anew clinical test for cervicocephalic kinesthetic sensibility: ‘‘the fly”.Arch Phys Med Rehabil 2004;85(3):490–5.
Lee HY, Teng CC, Chai HM, Wang SF. Test–retest reliability ofcervicocephalic kinesthetic sensibility in three cardinal planes. ManTher 2006;11(1):61–8.
Lephart SM, Pincivero DM, Giraldo JL, Fu FH. The role of proprio-ception in the management and rehabilitation of athletic injuries.Am JSports Med 1997;25(1):130–7.
Loudon JK, Ruhl M, Field E. Ability to reproduce head position afterwhiplash injury. Spine 1997;22(8):865–8.
McNair PJ, Heine PJ. Trunk proprioception: enhancement throughlumbar bracing. Arch Phys Med Rehabil 1999;80(1):96–9.
Nougier V, Bard C, Fleury M, Teasdale N, Cole J, Forget R, et al. Controlof single-joint movements in deafferented patients: evidence foramplitude coding rather than position control. Exp Brain Res1996;109(3):473–82.
Percy M, Hindel R. New method for non-invasive three-dimensionalmeasurements of human back movement. ClinBiomech 1989;4:73–9.
Peterson BW, Goldberg J, Bilotto G, Fuller JH. Cervicocollic reflex: itsdynamic properties and interaction with vestibular reflexes. J Neuro-physiol 1985;54(1):90–109.
Rankin G, Stokes M. Reliability of assessment tools in rehabilitation: anillustration of appropriate statistical analyses. Clin Rehabil1998;12(3):187–99.
Revel M, Andre-Deshays C, Minguet M. Cervicocephalic kinestheticsensibility in patients with cervical pain. Arch Phys Med Rehabil1991;72(5):288–91.
Richmond FJ, Loeb GE. Electromyographic studies of neck muscles in theintact cat. II. Reflexes evoked by muscle nerve stimulation. Exp BrainRes 1992;88(1):59–66.
Rix GD, Bagust J. Cervicocephalic kinesthetic sensibility in patients withchronic, nontraumatic cervical spine pain. Arch Phys Med Rehabil2001;82(7):911–9.

M. Kramer et al. / Journal of Electromyography and Kinesiology 19 (2009) e353–e361 e361
Rothwell JC, Traub MM, Day BL, Obeso JA, Thomas PK, Marsden CD.Manual motor performance in a deafferented man. Brain 1982;105(3):515–42.
Shinoda Y, Sugiuchi Y, Futami T, Ando N, Yagi J. Input patterns andpathways from the six semicircular canals to motoneurons of neckmuscles. II. The longissimus and semispinalis muscle groups. JNeurophysiol 1997;77(3):1234–58.
Shrout PE, Fleiss JL. Intraclass Correlations: Uses in assessing raterreliability. Psychol. Bull. 1979;86(2):420–8.
Sommerich CM, Joines SM, Hermans V, Moon SD. Use of surfaceelectromyography to estimate neck muscle activity. J ElectromyogrKinesiol 2000;10(6):377–98.
Strimpakos N, Sakellari V, Gioftsos G, Kapreli E, Oldham J. Cervicaljoint position sense: an intra- and inter-examiner reliability study. GaitPosture 2006;23(1):22–31.
Takebe K, Vitti M, Basmajian JV. The functions of semispinalis capitisand splenius capitis muscles: an electromyographic study. Anat Rec1974;179(4):477–80.
Taylor JL, McCloskey DI. Proprioception in the neck. Exp Brain Res1988;70(2):351–60.
Treleaven J, Jull G, Sterling M. Dizziness and unsteadiness followingwhiplash injury: characteristic features and relationship with cervicaljoint position error. J Rehabil Med 2003;35(1):36–43.
Treleaven J, Jull G, LowChoy N. The relationship of cervical jointposition error to balance and eye movement disturbances in persistentwhiplash. Man Ther 2006;11(2):99–106.
Ulkar B, Kunduracioglu B, Cetin C, Guner RS. Effect of positioning andbracing on passive position sense of shoulder joint. Br J Sports Med2004;38(5):549–52.
Walsh LD, Allen TJ, Gandevia SC, Proske U. Effect of eccentric exerciseon position sense at the human forearm in different postures. J ApplPhysiol 2006;100(4):1109–16.
Wilson VJ, Boyle R, Fukushima K, Rose PK, Shinoda Y, Sugiuchi Y,Uchino Y. The vestibulocollic reflex. J Vestib Res 1995;5(3):147–70.
Winter JA, Allen TJ, Proske U. Muscle spindle signals combine withthe sense of effort to indicate limb position. J Physiol 2005;568(3):1035–46.
Michael Kramer was born in 1967 in Pforz-heim, South Germany. He studied Medicine atthe University of Ulm, Germany and passedparts of the studies in Zurich, Switzerland andDurban, South Africa. In 1996 he started towork at the Department of Surgery andmeanwhile specialized in Traumasurgery. Sincemore than 15 years he is studying chronic painsyndromes and functional disorders of thespine. The main effort of his studies is focusedon neck muscle function and whiplash associ-ated disorders.
Marina Honold was born in 1984 in Ulm, South
Germany. She studied Physiotherapy at theEuropa Fachhochschule Fresenius (EFF) inIdstein and received her Bachelor of Science in2007. The subject of her thesis was Reliabilityof a New Virtual Reality Test to MeasureCervicocephalic Kinaesthesia. Currently (sinceOctober 2007) she is working at a physiother-apy practice in Ulm while also being enrolled ina interdisciplinary part-time Master’s programat the EFF. Her perspective graduation date isMarch 2010, when she will receive a Master’sdegree in Therapy Sciences.
Kathrin Hohl, born 1978 in Hamburg, studiedbusiness mathematics in Ulm and Missouri-Rolla, USA. Since 2003 she works as a bio-statistician at the University of Ulm. Shereceived her PhD in 2007. The subject of herthesis was imputation of missing data.
Dr. Ulrich Bockholt received his diploma degreein Mathematics from the University Mainz
(Germany) in 1997 and his doctoral degreefrom the Darmstadt University of Technologyin 2003. Since 1997 he is working in projects inthe field of surgical simulation and medicalvisualization. Today Ulrich Bockholt is leadingthe Department ‘‘Virtual & Augmented Real-ity” at the Fraunhofer Institute for ComputerGraphics (Fraunhofer-IGD) in Darmstadt(Germany).Alexander Rettig was born in 1969 in Munich,South Germany. He studied Mathematics at
the Technical University Darmstadt. 1998 hebecame researcher in the area of virtual realityat the Fraunhofer Institute for ComputerGraphics and specialized in force feedbacksystems. Since 2005 he is working as freelanceron projects about applications of virtual realityin medicine with special interest in trainingsystems.Martin Elbel was born in 1973 in Ulm SouthGermany. He studied Medicine at the Univer-
sity of Ulm, Germany. Since 2003 he worked atthe Department of Surgery in Ulm, includingone year at the Orthopaedic Department. Hisstudies are focused on whiplash injuries and thecorresponding car crash analysis since 5 years.Christoph Dehner was born in Goppingen,South Germany in 1976. He studied Medicine
at the University of Ulm, Germany. In 2003 hestarted his work at the Department of Trauma,Hand, Plastic and Reconstructive Surgery atthe University Hospital of Ulm. Since that hehas been studying intensively the muscle func-tion of the cervical spine. Furthermore he hasbeen involved in the development of newdiagnostic and therapeutic tools investigatingwhiplash associated disorders.