Embed Size (px)
Citation preview

8/9/2019 Renal Tumors in Adults
http://slidepdf.com/reader/full/renal-tumors-in-adults 1/23
Pathology of Renal Tumors in Adults
Dr Manoj Jain
Pathology of Renal Tumors
Gaya Prasad Memorial Pathology Symposium
APCON 2005, Indore; 2nd December, 2005 1
Pathology of Renal Tumors in Adults
Dr Manoj Jain
Associate Professor, Department of Pathology
Sanjay Gandhi Postgraduate Institute of Medical Sciences, Lucknow
Renal neoplasms are a distinct group of tumors, based on histologic, cytogenetic and molecularstudies and account for approximately 2.5-3% of all solid neoplasm. Conventionally pediatricand adult renal tumors are distinguished due to distinct clinico-pathological features, biological
behavior and treatment modalities. The majority of adult renal neoplasms are of epithelial origin
and are malignant.
Renal tumors can be differentiated based on their cells of origin (Table 1). Approximately 85%
are comprised of renal cell carcinoma (RCC). The old classification of “renal carcinomas” as
clear cell, granular cell and sarcomatoid carcinoma is now no longer used as many biologicallydistinct tumor subgroups were clubbed with similar looking histologcal features (Table 2).
Apart from the histological and immunohistochemical features, renal tumors are divided intodistinct histologic subtypes with characteristic cytogenetic alterations. Recently described Xp 11
translocation group of renal tumors with papillary architecture and low grade malignant potential
are distinguished by molecular studies. WHO 2004 classification of renal neoplasm also takesmolecular genetics in to account (Table 2).
Table. 1: Cell of Origin of Renal TumorsCell of Origin Tumor
Renal tubules Adenoma, adenocarcinoma
Embryonic tissue Mesoblastic nephroma, Wilms tumor
Mesenchymal tissue Angiomyolipoma, medullary Ca, interstitial cell tumour
Epithelium of renal pelvis Urothelial CarcinomaOthers Juxtaglomerular cell tumour
Table 2.
Differential Diagnosis of Renal Epithelial Cell Neoplasm “Granular” Features Sarcomatoid Features Papillary or Tubulopapillary Features
Clear Cell RCC Clear Cell RCC Clear Cell RCC
Chromophobe RCC Papillary RCC Chromophobe RCC
Papillary RCC Chromophobe RCC Papillary RCC
Oncocytoma Collecting Duct Ca Collecting Duct Ca
Mucinous Tubular and
Spindle cell Ca
Urothelial Ca

8/9/2019 Renal Tumors in Adults
http://slidepdf.com/reader/full/renal-tumors-in-adults 2/23
Pathology of Renal Tumors in Adults
Dr Manoj Jain
Pathology of Renal Tumors
Gaya Prasad Memorial Pathology Symposium
APCON 2005, Indore; 2nd December, 2005 2
Table 3: Classification of Renal Tumors in Adults (non-urothelial) (WHO 2004) Renal Epithelial Tumors Non-epithelial tumors
Benign Benign
Renal oncocytoma Renomedullary interstitial cell tumor
(medullary fibroma)
Papillary/tubulopapillary adenoma Angiomyolipoma
Metanephric adenoma Juxtaglomerular cell tumorMetanephric adenofibroma Metanephric stromal tumor
Malignant Solitary fibrous tumor
Clear cell (conventional) renal cell carcinoma Lipoma
Papillary renal cell carcinoma Leiomyoma
Chromophobe renal cell carcinoma Hemangioma
Collecting duct carcinoma Lymphangioma
Medullary carcinoma Malignant
Mucinous tubular and spindle cell carcinoma Leiomyosarcoma
Xp11 translocation carcinoma Rhabdosarcoma
Renal cell carcinoma, unclassified Synovial sarcoma
Liposarcoma
Tumor of undetermined malignant potential Miscellaneous tumors Multi-locular cystic renal cell carcinoma Carcinoid tumor
Mixed epithelial and stromal tumors Primitive neuroectodermal tumor
Mixed epithelial and stromal tumor Small cell carcinoma
Cystic nephroma Metastatic tumors
Hematopoeitic tumors
Table 4: American Joint Committee on Cancer staging of Renal Cell Carcinoma (2002)Stage Charateristics
Primary Tumor (T)
TX Primary tumor cannot be assessed
T0 No evidence of primary tumor
T1a Confined to kidney (≤4.0cm) T1b Confined to kidney (>4.0 cm and ≤7.0cm)
T2 Confined to kidney (>7.0 cm)
T3a Tumor directly invades adrenal gland or perirenal or renal sinus fat but not
beyond Gerota's fascia
T3b Tumor grossly extends into the renal vein or its segmental (muscle-containing)
branches, or vena cava below the diaphragm
T3c Tumor grossly extends into vena cava above diaphragm or invades the wall of
the vena cava
T4 Tumor invades beyond Gerota's fascia
Regional Lymph Nodes (N)
NX Regional lymph nodes cannot be assessed
N0 No regional lymph node metastasis
N1 Metastasis in a single regional lymph node
N2 Metastases in more than one regional lymph node
Distant Metastasis (M)
MX Distant metastasis cannot be assessed
M0 No distant metastasis
M1 Distant metastasis

8/9/2019 Renal Tumors in Adults
http://slidepdf.com/reader/full/renal-tumors-in-adults 3/23
Pathology of Renal Tumors in Adults
Dr Manoj Jain
Pathology of Renal Tumors
Gaya Prasad Memorial Pathology Symposium
APCON 2005, Indore; 2nd December, 2005 3
StagingThe TNM staging proposed by UICC/AJCC (most recently modified in 2002) is widely used
(Table 4). The changes in the current AJCC 2002 compared to the previous staging are
• pT1 tumors divided into pT1a (up to 4 cm in size) and pT1b (more than 4 cm up to 7 cm in
size)
• Stage pT3a includes tumors invading into renal sinus fat
•
Stage pT3b includes tumors with gross involvement of segmental (muscle-containing)
‘branches’ of renal vein.
Grading• Fuhrman’s nuclear grading system is the most popular and clinically useful (Table 5)
• Tumors are graded according to the highest nuclear grade present, even when focal
• For practical purposes, if nucleoli are not apparent at low magnification (x100), either grade
1 or 2 if nucleoli easily identified at high magnification (x400), grade 2, otherwise grade 1easily identifiable nucleoli at low magnification, grades 3 or 4 marked nuclear
pleomorphism- Grade 4, otherwise grade 3.
•
Nuclear grading of chromophobe and papillary RCC are of limited or no use.
Table 5: Histological Grading of Renal Cell CarcinomaGrade Nuclear features
1 Round, uniform nuclei approximately 10µ in diameter with minute or absent nucleoli
2 The nuclei have slightly irregular contours and are approximately 15 µ in diameter with
inconspicuous nucleoli which could be seen at 400x
3 Moderately to markedly irregular nuclear contours and diameters of nuclei is
approximately 20µ with large nucleoli visible at 100x
4 Nuclei similar to those of grade 3 but also multilobular or multiple nuclei or bizarre nuclei
and heavy clumps of chromatin
Malignant Epithelial Neoplasms:
Clear Cell (Conventional) Renal Cell Carcinoma
• Comprises 60-65% of renal cell neoplasms with age range of 34 to 90 years. Only occasional
cases occur in children and young adults.
• Charecterzied by 3p losses and mutations in VHL gene in virtually all cases of VHLsyndrome. Somatic mutations/hypermethylations found in 75-80% of sporadic tumors
• Clear cell RCC are bilateral in 3.5%, and multifocal in 11%. Hereditary cases arise at an
early age and often bilateral/multifocal, usually in fourth and fifth decade.
•
Combination of hematuria, abdominal pain, and a palpable mass (“classical triad”) at presentation in few cases (<10%). 50% or more diagnosed as incidental renal mass using
modern imaging techniques for unrelated conditions.
• Grossly classic cases are golden yellow on cut section due to intracytoplasmic lipid; higher-grade tumors have more varied appearance. Cystic change and necrosis frequent, some
tumors extensively cystic. Gross renal vein invasion occurs in 30%.
• On microscopic examination, characteristically the tumor cells are arranged in solid aciniseparated by delicate, arborizing fibrovascular septa; in others solid sheet-like, cystic,

8/9/2019 Renal Tumors in Adults
http://slidepdf.com/reader/full/renal-tumors-in-adults 4/23
Pathology of Renal Tumors in Adults
Dr Manoj Jain
Pathology of Renal Tumors
Gaya Prasad Memorial Pathology Symposium
APCON 2005, Indore; 2nd December, 2005 4
papillary or pseudo- papillary, tubular and sarcomatoid growth patterns. Low-grade lesions
usually have acinar growth whereas higher-grade areas more often solid, pseudopapillary orsarcomatoid. Majority have a mixture of clear or granular-eosinophilic cells. Grade 1 lesions
invariably found with clear cytoplasm and higher-grade lesions more often have variably
eosinophilic cytoplasm. Necrosis and focal hemorrhage are frequently present. Calcificationis found in 10% and osseous metaplasia in 4% cases. Sarcomatoid areas denote grade 4
disease.• Clear cell RCC metastasizing to unusual and uncommon sites not infrequent, and patients
sometimes present with such unusual metastases
• Some tumors may be confused with papillary or chromophobe RCC, although, thoroughmicroscopic examination reveals areas with classic histological features; immunostains for
CK7 and Racemase frequently expressed by papillary RCC and usually not by clear cell
RCC. Adrenocortical carcinoma is differentiated from clear cell RCC as it is not reactivewith EMA and rarely positive for CK and express Inhibin and Melan-A (A103).
• Disease-free and overall survival correlate with grade and stage. 5 and 10 year disease
specific survivals 76 and 70%.
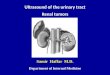
Fig 1 (A & B). Gross morphology of Clear Cell Renal Cell Carcinoma

8/9/2019 Renal Tumors in Adults
http://slidepdf.com/reader/full/renal-tumors-in-adults 5/23
Pathology of Renal Tumors in Adults
Dr Manoj Jain
Pathology of Renal Tumors
Gaya Prasad Memorial Pathology Symposium
APCON 2005, Indore; 2nd December, 2005 5
Fig 2. (A & B). Microphotographs of Clear Cell Renal Cell Carcinoma
Fig 3. Microphotograph of Clear Cell RCCwith clear cell and granular cell areas
Multilocular Cystic Renal Cell Carcinoma
• Rare variant (3 to 6%) of clear cell RCC; no reported cases progressed.
• Grossly, well-circumscribed, multicystic mass; cysts separated by thin fibrous septa, and
containing serous or bloody fluid or clots. No solid or expansile masses of tumor present.

8/9/2019 Renal Tumors in Adults
http://slidepdf.com/reader/full/renal-tumors-in-adults 6/23
Pathology of Renal Tumors in Adults
Dr Manoj Jain
Pathology of Renal Tumors
Gaya Prasad Memorial Pathology Symposium
APCON 2005, Indore; 2nd December, 2005 6
• Microscopically, the thin fibrous septa lined by one or more layers of neoplastic clear cells
with Furhman grade 1 or 2 nuclei. Small collections of tumor cells always present within the
fibrous septa or in the tumor capsule, but no expansile masses of tumor seen.
• Differential diagnoses include cystic nephroma, and extensively cystic clear cell RCC. Ifexpansile tumor masses in the septa diagnosis of clear cell RCC should be considered.
Fig 4 (A & B). Gross and microphotographs of multilocular cystic RCC
Papillary Renal Cell Carcinoma (PRCC)
• Comprises 7 to 15% of renal cell neoplasms with age at presentation from 3rd to 8th decadesand male to female ration of 2.5:1. PRCC are most common tumors with bilateral occurance,
as well as, multifocal disease.
• Among all renal epithelial tumors, PRCC most likely to have a fibrous capsule. Gross
necrosis, hemorrhage and gross cystic change are common. Tumors containing abundantfoamy macrophages appear tan to yellow on cut surface and those with intratumoral
hemorrhage dark tan to brown.
• Microscopically, a broad morphologic spectrum; classical papillary pattern with discrete
papillary fronds lined by neoplastic epithelial cells with a central fibrovascular core. SomePRCCs may have trabecular and solid areas and closely packed papillae, masking their true
growth pattern; others with tubular and/or glomeruloid features. Sarcomatoid features, when present, denotes a sign of aggressive disease. The percentage of papillary architecture alone
not used to determine whether a tumor is a PRCC or not.
• The predominant cell type in a tumor either basophilic or eosinophilic, but many with
combination of both; tumor cells with clear cytoplasm, almost always a focal finding; nuclearfeatures ranging from small with inconspicuous nucleoli (generally in basophilic areas) to

8/9/2019 Renal Tumors in Adults
http://slidepdf.com/reader/full/renal-tumors-in-adults 7/23
Pathology of Renal Tumors in Adults
Dr Manoj Jain
Pathology of Renal Tumors
Gaya Prasad Memorial Pathology Symposium
APCON 2005, Indore; 2nd December, 2005 7
large with prominent nucleoli (generally in eosinophilic areas). Necrosis with cystic change,
psammoma bodies and foamy macrophages in fibrovascular stalk are commonly present.Cytoplasmic hemosiderin deposition more often found in eosinophilic tumors.
• Prognosis intermediate between clear cell RCC and chromophobe RCC; reported 5-year
disease free survival of 79% to 92%. Role of Fuhrman grading controversial, tumors with
eosinophilic cytoplasm are usually high grade and basophilic tumors are usually low grade.
Proposed subtyping into type 1 and type 2 (WHO), based on architecture and cytologicfeatures; some genetic and survival differences between the two groups reported. Type 2
tumor having more plemorphism and poorer prognosis.
• PRCC may be confused with clear cell RCC exhibiting a papillary or pseudopapillarygrowth, and with collecting duct carcinoma. P sammoma bodies, hemosiderin deposition
within tumor cells, and fibrovascular cores containing foamy macrophages more likely in
PRCC than clear cell. CK 7 and Racemase immunoreactivity and if needed, moleculargenetics, can be used to resolve difficult cases. Collecting duct carcinoma may have a
papillary growth pattern, but centered in the medulla, virtually always high grade, invariably
invade into adjacent renal parenchyma, are associated with a desmoplastic stroma, and showintracytoplasmic and luminal mucin, reactivity for CEA, the lectins peanut and soybean
agglutinins, Ulex europaeus, and high molecular weight cytokeratin.
Fig 5. (A & B). Gross photograph of Papillary Renal Cell Carcinoma

8/9/2019 Renal Tumors in Adults
http://slidepdf.com/reader/full/renal-tumors-in-adults 8/23
Pathology of Renal Tumors in Adults
Dr Manoj Jain
Pathology of Renal Tumors
Gaya Prasad Memorial Pathology Symposium
APCON 2005, Indore; 2nd December, 2005 8
Fig 6. (A & B). Microphotographs of Papillary Renal Cell Carcinoma (Type I & Type 2)
Chromophobe Renal Cell Carcinoma (CRCC)
• CRCC first recognized in humans in 1985, leading to and serving as the foundation for the
current classification of renal tumors; stage for stage, significantly better prognosis than clear
cell RCC; 6% to 11% of renal epithelial tumors; age and sex distribution similar to clear cellRCC. Majority are asymptomatic; approximately 11% are bilateral.
• On gross examination cut surface is usually homogenous beige or pale-tan, but may be dark brown (eosinophilic variants). Central scar found in 7-15% and largest mean size of all renal
epithelial tumors. 1/4th cases have gross hemorrhage or necrosis. Gross cysts are rare, gross
renal vein involvement and perirenal adipose tissue invasion occasionally present (Table 6).
• Microscopically, predominantly solid growth pattern, with thin incomplete, fibrousseptations. Tubular, trabecular, cystic, and sarcomatoid patterns found in a few. Necrosis and
calcification frequently found. Cells are predominantly large round to polygonal with well-
defined cell borders and pale (translucent and finely reticulated) cytoplasm in the “classical”
variant, in some cases (eosinophilic variants) cells have predominantly dense eosinophilic
cytoplasm, however, combination of both cell types in variable proportions in virtually alltumors. Nuclei are typically hyperchromatic, with irregular, wrinkled nuclear membrane in
variable proportions, and characteristic perinuclear cytoplasmic clarity (halos), at least focal,in each case. Cell membranes appear prominent due to cytoplasmic organelles pushed to the
periphery of the cytoplasm. Binucleate cells present in all cases. Mitotic activity is very low,
except in sarcomatoid areas.
• Diffuse, reticular positivity with Hale’s colloidal iron stain very characteristic; however, thestain highly fastidious and procedure-dependant.

8/9/2019 Renal Tumors in Adults
http://slidepdf.com/reader/full/renal-tumors-in-adults 9/23
Pathology of Renal Tumors in Adults
Dr Manoj Jain
Pathology of Renal Tumors
Gaya Prasad Memorial Pathology Symposium
APCON 2005, Indore; 2nd December, 2005 9
• Prognosis much better than other types of RCC; 5 and 10 year disease specific survivals
close to 95 and 90%; rare classical CRCC metastasize and kill the patient, but tumors with a
sarcomatoid component the most likely to behave in an aggressive fashion
Fig 7. (A & B) Gross and microphotographs of Chromophobe Renal Cell Carcinoma
Collecting Duct Carcinoma (CDC)
•
Comprises <1% of renal epithelial tumors; occur at any age (13 to 83 yrs), but, in general,
tend to present in younger patients. Hematuria, pain, weight loss and the presence of a palpable mass the most common presentation. >50% have metastases at time of presentation.
• Grossly most CDCs are centered in the medulla, usually poorly circumscribed. Cut surface is
solid, tan-white and firm but may show cysts, hemorrhage and necrosis.
• The histological features of classic tumors -multinodularity, and neoplastic ducts, tubules,
and papillae in a fibrotic, desmoplastic stroma. Tumor cells have eosinophilic, basophilic or
amphophilic cytoplasm, high grade nuclei and prominent nucleoli. Some cases show focallyor predominantly sarcomatoid areas. Acute or chronic inflammatory cells usually abundant in
the stroma. The papillae found rarely, if ever, with foamy macrophages and psammoma
bodies are rare. Characteristically, adjacent renal tubules are dysplastic, cytoplasmic/luminalmucin frequently found.
• Classic cases characterized by aggressive behavior; >50% present with metastatic diseaseand most die within 24 months of presentation; nodal, osseous, and visceral metastases
common. Metastases to bone is usually osteoblastic.
• Differential diagnoses include PRCC (see PRCC), medullary carcinoma and, more
commonly, pelvicalyceal urothelial carcinoma invading the renal parenchyma; distinguishing between high-grade urothelial carcinoma and CDC more difficult as both may be associated

8/9/2019 Renal Tumors in Adults
http://slidepdf.com/reader/full/renal-tumors-in-adults 10/23
Pathology of Renal Tumors in Adults
Dr Manoj Jain
Pathology of Renal Tumors
Gaya Prasad Memorial Pathology Symposium
APCON 2005, Indore; 2nd December, 2005 10
with an inflamed, desmoplastic stroma and may show dysplasia in adjacent renal tubules;
both may have a tubular/tubulopapillary pattern of growth and a similar immunophenotype;cytoplasmic mucin may be seen in urothelial tumors as well. Best way to resolve the issue is
by looking for in situ urothelial carcinoma; molecular studies may also be of diagnostic
utility.
Fig 8. (A & B) Gross and microphotographs of Collecting Duct Carcinoma
Medullary Carcinoma• Highly aggressive tumors predominantly affecting young African-American patients; usually
medulla centered; mean age of 22 years (range, 11 to 39 years), rare cases in older patients.
Almost all with sickle cell trait, rarely with SS or SC disease.
• Morphologically, many features similar to high-grade CDC; tumors composed of cells withhigh-grade nuclei arranged in solid nests or irregular tubules; microcystic or reticular growth
reminiscent of yolk sac tumors or adenoid cystic carcinoma present.Many tumoral/non-
tumoral blood vessels contain irregular or sickled red blood cells.
• Most cases with metastases at presentation; mean survival approximately 4 months.
Renal Cell Carcinoma, Unclassified
•
Includes the renal carcinomas not fitting into any of the above-described categories; thus,tumors of unrecognizable cell or architectural types, or those with apparent composites of the
recognized types all included in this category.
• Form up to 6% of all renal epithelial tumors; many tumors of high cytoarchitectural gradeand aggressive behavior, but, by definition, not limited to only such aggressive tumors.

8/9/2019 Renal Tumors in Adults
http://slidepdf.com/reader/full/renal-tumors-in-adults 11/23
Pathology of Renal Tumors in Adults
Dr Manoj Jain
Pathology of Renal Tumors
Gaya Prasad Memorial Pathology Symposium
APCON 2005, Indore; 2nd December, 2005 11
Recently described rare renal tumors
Renal Tumors Of Birt-Hogg-Dubé Syndrome
• Usually multifocal and bilateral renal tumors in the autosomal-dominant, Birt-Hogg-Dubé
syndrome. Most tumors have oncocytic features, and usually either CRCC, renaloncocytoma, or tumors with hybrid features of renal oncocytoma and CRCC; rare clear cell
(conventional) RCCs also described.
Mucinous Tubular and Spindle Cell Carcinoma (Low-Grade Biphasic RCC of Possible
Collecting Duct/ Loop of Henle Origin)
• Recently described tumor, unique renal neoplasm being less aggressive in spite of a spindle
cell component that mimics a low-grade sarcoma. Most cases occur in females with age
ranges of 17-78 years (average, 53 years).
• Grossly, well-circumscribed with a tan white cut surface; usually medulla-centered.
• Microscopically, elongated, interconnected tubules many appearing straight and with slit-likelumina, solid compressed cord-like structures, and prominent low-grade spindle cell areas.
Papillary areas and cysts not identified, stroma characteristically, and at least focally,
myxoid, and usually with some inflammatory cell infiltrates.
• Ultrastructural evaluation done on a few cases shows close resemblance to the normal loop of
Henle.
Translocation Associated Carcinomas
• Recently recognized carcinomas, usually in children and young adults; rarely in older people;
Xp11.2 translocations: 2 broad types; t(X;1) mostly with translocations of TFE3 and PRCCgenes, and t(X;17) mostly with Alveolar Soft Part Sarcoma-like translocations involving
TFE3 and ASPL3 genes; another group with t(6;11) involving TFEB gene
• Each group with unique and distinctive morphology, including combination of clear cell and
papillary/pseudopapillary features
Benign Epithelial Neoplasms Renal Oncocytoma
• Commonest benign renal tumor, incidence varies 3-7% of all renal neoplasms and most cases
of oncocytoma are discovered incidentally during the work-up of non-urologic conditions.
• On gross examination oncocytomas are well-circumscribed, pale-yellow to mahogany-brown
in color. Central stellate scar in 33% (similar scars also seen in other low-grade tumors).
Focal hemorrhage may be present, but gross necrosis rare. 15% oncocytoma are multifocaland 4% are bilateral.
•
Histologically, pure population of oncocytes arranged in organoid/nested, tubulocystic ormixtures of these patterns. Nuclei are round and uniform. Foci with pleomorphic and
hyperchromatic nuclei suggesting degenerative change and focal smaller cell populationwith scant cytoplasm (“oncoblasts”) are common. Focal clear cell change, usually in areas of
stromal hyalinization may be present. Mitotic activity is very rare.
• Frequent genetic change is loss of chromosome 1& Y and less frequent change is
translocation involving chromosome 9& 11[t(9;11)(p23;q13)].

8/9/2019 Renal Tumors in Adults
http://slidepdf.com/reader/full/renal-tumors-in-adults 12/23
Pathology of Renal Tumors in Adults
Dr Manoj Jain
Pathology of Renal Tumors
Gaya Prasad Memorial Pathology Symposium
APCON 2005, Indore; 2nd December, 2005 12
Fig 9. (A & B). Gross and Microphotographs of Renal Oncocytoma
Table 6: Distinguishing features of Renal Oncocytoma and Chromophobe RCC Features Oncocytoma Chromophobe RCC
Gross
Color Brown Red (mahogany) Yellow-Tan
Central Scar Coommon Less common
Cellular
Architecture Nested & Tubular Solid Sheets
Necrosis Absent Common
Cytoplasm Absent Present
Perinuclar halo Absent Present
Nuclear
Shape Round Irregular, cleaved
Hyperchromatic Atypical Common Less common Nucleoli Common Small/ absent
Binucleate Common Always
EM Mitochondria Microvescile & mitochondria
Hales colloidal Iron Negative / Luminal Diffuse/ granular

8/9/2019 Renal Tumors in Adults
http://slidepdf.com/reader/full/renal-tumors-in-adults 13/23
Pathology of Renal Tumors in Adults
Dr Manoj Jain
Pathology of Renal Tumors
Gaya Prasad Memorial Pathology Symposium
APCON 2005, Indore; 2nd December, 2005 13
Papillary/Tubulopapillary Adenoma
• Microscopic lesions up to 5 mm, morphologically similar to low-grade papillary RCC.
• Present in cases of papillary RCC with multifocal disease or as incidental finding innephrectomy specimen.
• Histologially presence of clear cell RCC features are not compatible with diagnosis ofadenoma.
•
Cytogenetic abnormality reveal trisomies of chromosomes 7 and 17, and loss of chromosomeY common.
Fig 10. Photomicrograph of Tubulopapillary Adenoma in case of chronic pyelonephritis
Metanephric Tumors (Metanephric Adenoma, Metanephric Adenofibroma And
Metanephric Stromal Tumor)
• Metanephric tumors are relatively recently described benign tumors with age range of 1-9thdecades and female to male ratio of 2:1.
• Metanephric adenoma and metanephric adenofibroma are well-circumscribed, non-encapsulated tumors and are sharply demarcated from the surrounding renal parenchyma.
Areas of necrosis, hemorrhage, cystic degeneration, and gross calcifications not uncommon.
• Histologically metanephric adenoma have tightly packed small tubules, focal papillary orglomeruloid components, and microcalcifications including psammoma bodies. Cytoplasm is
scant with often overlapping small nuclei with inconspicuous nucleoli and rare mitotic
figures. Multifocality is very rare.
• Metanephric adenofibroma is a biphasic neoplasm with epithelial component similar to
metanephric adenoma and mesenchymal component of bland fibroblast-like cells arranged ininterlacing fascicles.
• Metanephric stromal tumor is a spindle cell lesion with characteristic histologic featuresincluding alternating high and low cellularity, onion-skin cuffing around entrapped renal

8/9/2019 Renal Tumors in Adults
http://slidepdf.com/reader/full/renal-tumors-in-adults 14/23
Pathology of Renal Tumors in Adults
Dr Manoj Jain
Pathology of Renal Tumors
Gaya Prasad Memorial Pathology Symposium
APCON 2005, Indore; 2nd December, 2005 14
tubules, heterologous differentiation (glial or cartilaginous), and vascular alterations
(including angiodysplasia)
• Differential diagnosis: Epithelial- predomint Wilms tumor and solid variant of papillaryRCC
Fig 11 (A & B). Microphotographs of Metanephric Adenoma
Fig 12 Microphotograph of Metanephric Adenofibroma

8/9/2019 Renal Tumors in Adults
http://slidepdf.com/reader/full/renal-tumors-in-adults 15/23

8/9/2019 Renal Tumors in Adults
http://slidepdf.com/reader/full/renal-tumors-in-adults 16/23
Pathology of Renal Tumors in Adults
Dr Manoj Jain
Pathology of Renal Tumors
Gaya Prasad Memorial Pathology Symposium
APCON 2005, Indore; 2nd December, 2005 16
• On Gross examination AML have generally pushing borders; color and consistency reflect
relative proportion of adipose tissue and smooth muscle. Majority are unilateral and unifocal,
presence of bilateral or multifocal tumors, or tumors with epithelioid histology stronglysuggest T S.
• Histologically AML are composed of adipose tissue, smooth muscle, and vasculature in
variable proportions. Smooth muscle component may show sheets of epithelioid cells with
abundant pink granular cytoplasm. AML have thickened and hyalinized vessels and eccentriclumens with smooth muscle cells often appear to originate and radiate from vessel walls.
• The recently described epithelioid variant of angiomyolipoma (Renal Epithelioid Oxiphilic
Neoplasm-REON/Perivascular Epithelioid Cell Tumor-PECOMA) composed either
exclusively or predominantly of polygonal cells with densely eosinophilic cytoplasm.
Variable degree of nuclear atypia, focal cytoplasmic clearing and extensive intratumoralhemorrhage and necrosis are common in such tumors.
• IHC show positivity for HMB-45, A-103 (Melan-A/MART-1) and smooth muscle actin.
• EM reveals spherical structures with internal lamellations, consistent with aberrant
melanosomes, in a few cases rare type-2 premelanosomes and rhomboid crystals may be present.
•
Majority AML are benign and primary complication include retroperitoneal hemorrhage
usually in >4 cm tumors. Epithelioid variant of AMl with pleomorphic monotypic featuresmimicking high-grade or sarcomatous RCC tend to behave in more aggressive fashion.
• Angiomyolipomas involving non-contiguous sites like regional lymph nodes considered to
represent multifocal disease.
Fig 13. Gross and photomicrograph of angimyolipoma

8/9/2019 Renal Tumors in Adults
http://slidepdf.com/reader/full/renal-tumors-in-adults 17/23
Pathology of Renal Tumors in Adults
Dr Manoj Jain
Pathology of Renal Tumors
Gaya Prasad Memorial Pathology Symposium
APCON 2005, Indore; 2nd December, 2005 17
Mesenchymal Neoplasms
• A wide variety of mesenchymal neoplasms rarely occur in the adult kidney and benign
tumors include lipoma, leiomyoma, solitary fibrous tumor, schwannoma, neurofibroma,myxoma, hemangioma, and lymphangioma
• Primary renal sarcomas comprise roughly 1% of all renal neoplasms; majority of these are
leiomyosarcomas; other sarcomas described include liposarcoma, rhabdomyosarcomas,
malignant fibrous histiocytoma, fibrosarcoma, osteosarcoma, mesenchymal chondrosarcoma,chondrosarcoma, malignant mesenchymoma, and angiosarcoma. Consideration should be
given to sarcomatoid renal cell carcinoma or direct infiltration from the retroperitoneum
before making the diagnosis of any primary renal sarcoma.
Fig 14 . Photomicrograph of leiomysarcoma of kidney
Fig 14 . Photomicrograph of Lymphoma of kidney

8/9/2019 Renal Tumors in Adults
http://slidepdf.com/reader/full/renal-tumors-in-adults 18/23
Pathology of Renal Tumors in Adults
Dr Manoj Jain
Pathology of Renal Tumors
Gaya Prasad Memorial Pathology Symposium
APCON 2005, Indore; 2nd December, 2005 18
Suggested Reading: Introduction
1. Storkel S, Eble JN, Adlakha K, Amin M, Blute ML, Bostwick DG, Darson M, Delahunt
B, Iczkowski K. Classification of renal cell carcinoma: Workgroup No. 1. Union
Internationale Contre le Cancer (UICC) and the American Joint Committee on Cancer(AJCC). Cancer 1997;80:987-9.
2.
World Health Organization Classification of Tumours- Pathology and Genetics: Tumoursof the Urinary System and Male Genital Organs. Eds. Eble JN, Sauter G, Epstein,
Sesterhenn IA. IARC Press, Lyon, 2004.3. Fleming S. The impact of genetics on the classification of renal carcinoma.
Histopathology 1993;22:89-92.
4. Kovacs G. Molecular differential pathology of renal cell tumours. Histopathology1993;22:1-8.
5. Bodmer D, van den Hurk W, van Groningen JJ, Eleveld MJ, Martens GJ, Weterman MA,
van Kessel AG. Understanding familial and non-familial renal cell cancer. Hum MolGenet. 2002;11:2489-98.
6. Parkin DM, Pisani P, Ferlay J. Estimates of the worldwide incidence of eighteen major
cancers in 1985. Int J Cancer. 1993;54:594-606.7. Cancer Incidence, Mortality and Prevalence Worldwide, Version 1.0. IARC Cancer Base
No. 5. Lyon, IARC Press, 2001.8. Adult Renal Tumors by Reutor EV, Tickoo SK; in Sternberg’s Diagnostic Surgical
Pathology Vol 3, 4th Edn (2004) by LippincottvWilliams & Wilkins.
9. Renal Tumors, Clinics in Laboratory Medicine; June 2005, Vol 25, No. 210.
Srivastava A, Mandhani A, Kapoor R, Jain M, Dubey D, Srivastava A, Raghavendra M,Kumar A. Prognosticfactors in patients with renal cell carcinoma: is TNM (1997) staging
relevant in Indian subpopulation? Indian J Cancer. 2004 Jul-Sep;41(3):99-103.
Malignant Epithelial Renal Tumors
11.
Green F, Page D, Fleming I, Fritz A, Balch C, Haller D, Morrow M. AJCC cancerstaging manual. 6th ed: Springer; 2002.
12. Medeiros LJ, Jones EC, Aizawa S, Aldape HC, Cheville JC, Goldstein NS, Lubensky IA,
Ro J, Shanks J, Pacelli A, Jung SH. Grading of renal cell carcinoma: Workgroup No. 2.
Union Internationale Contre le Cancer and the American Joint Committee on Cancer(AJCC). Cancer 1997;80:990-1.
13. VE Reuter, SK Tickoo. Adult renal tumors. In: Sternberg’s Diagnostic Surgical
Pathology. 4th edition. Eds. Mills SE, Carter D, Greenson JK, Oberman HA, Reuter VE,
Stoler MH. Lippincott Williams and Wilkins, Philadelphia. 2004. pp. 1955-2000.14. Lohse CM, Blute ML, Zincke H, Weaver AL, Cheville JC. Comparison of standardized
and nonstandardized nuclear grade of renal cell carcinoma to predict outcome among
2,042 patients. Am J Clin Pathol. 2002 Dec;118(6):877-86.15. Linehan WM, Lerman MI, Zbar B. Identification of the von Hippel-Lindau (VHL) gene.
Its role in renal cancer. JAMA 1995;273:564-70.
16. Zbar B. Von Hippel-Lindau disease and sporadic renal cell carcinoma. Cancer Surv.1995;25:219-32.
17. Porena M, Vespasiani G, Rosi P, Costantini E, Virgili G, Mearini E, Micali F.
Incidentally detected renal cell carcinoma: role of ultrasonography. J Clin Ultrasound.
1992;20:395-400.

8/9/2019 Renal Tumors in Adults
http://slidepdf.com/reader/full/renal-tumors-in-adults 19/23
Pathology of Renal Tumors in Adults
Dr Manoj Jain
Pathology of Renal Tumors
Gaya Prasad Memorial Pathology Symposium
APCON 2005, Indore; 2nd December, 2005 19
18. Thompson IM, Peek M. Improvement in survival of patients with renal cell carcinoma--
the role of the serendipitously detected tumor. J Urol. 1988;140:487-90.
19. Murad T, Komaiko W, Oyasu R, Bauer K. Multilocular cystic renal cell carcinoma. Am J
Clin Pathol. 1991;95:633-7.20. Nassir A, Jollimore J, Gupta R, Bell D, Norman R. Multilocular cystic renal cell
carcinoma: a series of 12 cases and review of the literature. Urology 2002;60:421-7.21. Papillary renal cell carcinoma
22. Amin MB, Corless CL, Renshaw AA, Tickoo SK, Kubus J, Schultz DS. Papillary(chromophil) renal cell carcinoma: histomorphologic characteristics and evaluation of
conventional pathologic prognostic parameters in 62 cases. Am J Surg Pathol.
1997;21:621-35.23. Weiss LM, Gelb AB, Medeiros LJ. Adult renal epithelial neoplasms. Am J Clin Pathol.
1995;103:624-35.
24. Kovacs G. Papillary renal cell carcinoma. A morphologic and cytogenetic study of 11cases. Am J Pathol. 1989;134:27-34.
25. Delahunt B, Eble JN. Papillary renal cell carcinoma: a clinicopathologic and
immunohistochemical study of 105 tumors. Mod Pathol. 1997;10:537-44.26. Delahunt B, Eble JN, McCredie MR, Bethwaite PB, Stewart JH, Bilous AM.
Morphologic typing of papillary renal cell carcinoma: comparison of growth kinetics and patient survival in 66 cases. Hum Pathol. 2001;32:590-5.
27. Sanders ME, Mick R, Tomaszewski JE, Barr FG. Unique patterns of allelic imbalance
distinguish type 1 from type 2 sporadic papillary renal cell carcinoma. Am J Pathol.
2002;161:997-1005. Chromophobe renal cell carcinoma28. Thoenes W, Storkel S, Rumpelt HJ. Human chromophobe cell renal carcinoma.
Virchows Arch B Cell Pathol Incl Mol Pathol. 1985;48:207-17.
29. Thoenes W, Storkel S, Rumpelt HJ, Moll R, Baum HP, Werner S. Chromophobe cellrenal carcinoma and its variants--a report on 32 cases. J Pathol. 1988;155:277-87.
30.
Akhtar M, Kardar H, Linjawi T, McClintock J, Ali MA. Chromophobe cell carcinoma ofthe kidney. A clinicopathologic study of 21 cases. Am J Surg Pathol. 1995;19:1245-56.
31. Crotty TB, Farrow GM, Lieber MM. Chromophobe cell renal carcinoma:
clinicopathological features of 50 cases. J Urol. 1995;154:964-7.
32. Bugert P, Gaul C, Weber K, Herbers J, Akhtar M, Ljungberg B, Kovacs G. Specificgenetic changes of diagnostic importance in chromophobe renal cell carcinomas. Lab
Invest. 1997;76:203-8.
33. Kovacs A, Kovacs G. Low chromosome number in chromophobe renal cell carcinomas.
Genes Chromosomes Cancer. 1992;4:267-8.34. Tickoo SK, Amin MB. Discriminant nuclear features of renal oncocytoma and
chromophobe renal cell carcinoma. Analysis of their potential utility in the differential
diagnosis. Am J Clin Pathol. 1998;110:782-7.35. Tickoo SK, Amin MB, Zarbo RJ. Colloidal iron staining in renal epithelial neoplasms,
including chromophobe renal cell carcinoma: emphasis on technique and patterns of
staining. Am J Surg Pathol. 1998;22:419-24.36. Tickoo SK, Amin MB, Zarbo RJ. Colloidal iron staining in renal epithelial neoplasms,
including chromophobe renal cell carcinoma: emphasis on technique and patterns of
staining. Am J Surg Pathol. 1998;22:419-24.

8/9/2019 Renal Tumors in Adults
http://slidepdf.com/reader/full/renal-tumors-in-adults 20/23

8/9/2019 Renal Tumors in Adults
http://slidepdf.com/reader/full/renal-tumors-in-adults 21/23
Pathology of Renal Tumors in Adults
Dr Manoj Jain
Pathology of Renal Tumors
Gaya Prasad Memorial Pathology Symposium
APCON 2005, Indore; 2nd December, 2005 21
55. Srigley JR, Kapusta L, Reuter V, Amin M, Grignon DG, Eble JN, Weber A, Moch H.
Phenotypic, molecular and ultrastructural studies of a novel low grade renal epithelialneoplasm possibly related to the loop of Henle. Mod Pathol. 2002;12:182A.
56. Argani P, Ladanyi M. Recent advances in pediatric renal neoplasia. Adv Anat Pathol.
2003 Sep;10(5):243-60.
Benign Epithelial Tumors57. Davis CJ, Jr., Mostofi FK, Sesterhenn I, Ho CK. Renal oncocytoma. Clinicopathological
study of 166 patients. J Urogen Pathol. 1991;1:41-52.58. Amin MB, Crotty TB, Tickoo SK, Farrow GM. Renal oncocytoma: a reappraisal of
morphologic features with clinicopathologic findings in 80 cases. Am J Surg Pathol.
1997;21:1-12.59. Perez-Ordonez B, Hamed G, Campbell S, Erlandson RA, Russo P, Gaudin PB, Reuter
VE. Renal oncocytoma: a clinicopathologic study of 70 cases. Am J Surg Pathol.
1997;21:871-83.60. Amin MB, Tamboli P, Javidan J, Stricker H, de-Peralta Venturina M, Deshpande A,
Menon M. Prognostic impact of histologic subtyping of adult renal epithelial neoplasms:
an experience of 405 cases. Am J Surg Pathol. 2002;26:281-91.61. Fuzesi L, Gunawan B, Braun S, Boeckmann W. Renal oncocytoma with a translocation
t(9;11)(p23;q13). J Urol. 1994;152:471-2.62. Neuhaus C, Dijkhuizen T, van den Berg E, Storkel S, Stockle M, Mensch B, Huber C,
Decker HJ. Involvement of the chromosomal region 11q13 in renal oncocytoma: case
report and literature review. Cancer Genet Cytogenet. 1997;94:95-8.
63. Tickoo SK, Lee MW, Eble JN, Amin M, Christopherson T, Zarbo RJ, Amin MB.Ultrastructural observations on mitochondria and microvesicles in renal oncocytoma,
chromophobe renal cell carcinoma, and eosinophilic variant of conventional (clear cell)
renal cell carcinoma. Am J Surg Pathol. 2000;24:1247-56.64. Argani P, Beckwith JB. Metanephric stromal tumor: report of 31 cases of a distinctive
pediatric renal neoplasm. Am J Surg Pathol. 2000;24:917-26.65. Davis CJ, Jr., Barton JH, Sesterhenn IA, Mostofi FK. Metanephric adenoma.
Clinicopathological study of fifty patients. Am J Surg Pathol. 1995;19:1101-14.
66. Gatalica Z, Grujic S, Kovatich A, Petersen RO. Metanephric adenoma: histology,
immunophenotype, cytogenetics, ultrastructure. Mod Pathol. 1996;9:329-33.67.
Kuroda N, Tol M, Hiroi M, Enzan H. Review of metanephric adenoma of the kidney with
focus on clinical and pathobiological aspects. Histol Histopathol. 2003;18:253-7.
68. Stumm M, Koch A, Wieacker PF, Phillip C, Steinbach F, Allhoff EP, Buhtz P, Walter H,
Tonnies H, Wirth J. Partial monosomy 2p as the single chromosomal anomaly in a caseof renal metanephric adenoma. Cancer Genet Cytogenet. 1999;115:82-5.
69. Jain M, Rastogi A, Gupta RK. Atypical Metanephric Adenoma- a case report and review
of literature. International Urol & Nephrol (2005) ACCEPTED FOR PUBLICATION.
Other Renal Tumors
70. Durham JR, Bostwick DG, Farrow GM, Ohorodnik JM. Mesoblastic nephroma of
adulthood. Report of three cases. Am J Surg Pathol. 1993;17:1029-38.
71. Levin NP, Damjanov I, Depillis VJ. Mesoblastic nephroma in an adult patient: recurrence
21 years after removal of the primary lesion. Cancer 1982;49:573-7.

8/9/2019 Renal Tumors in Adults
http://slidepdf.com/reader/full/renal-tumors-in-adults 22/23
Pathology of Renal Tumors in Adults
Dr Manoj Jain
Pathology of Renal Tumors
Gaya Prasad Memorial Pathology Symposium
APCON 2005, Indore; 2nd December, 2005 22
72. Prats Lopez J, Palou Redorta J, Morote Robles J, Martinez Perez E, Ruiz Marcellan C.
Leiomyomatous renal hamartoma in an adult. Eur Urol. 1988;14:80-2.73. Adsay NV, Eble JN, Srigley JR, Jones EC, Grignon DJ. Mixed epithelial and stromal
tumor of the kidney. Am J Surg Pathol. 2000;24:958-70.
74. Pierson CR, Schober MS, Wallis T, Sarkar FH, Sorensen PH, Eble JN, Srigley JR, JonesEC, Grignon DJ, Adsay V. Mixed epithelial and stromal tumor of the kidney lacks the
genetic alterations of cellular congenital mesoblastic nephroma. Hum Pathol.2001;32:513-20.
75. Gupta NP, Singh BP, Raina V, Gupta SD. Primitive neuroectodermal kidney tumor: 2case reports and review of the literature. J Urol. 1995;153:1890-2.
76. Marley EF, Liapis H, Humphrey PA, Nadler RB, Siegel CL, Zhu X, Brandt JM, Dehner
LP. Primitive neuroectodermal tumor of the kidney--another enigma: a pathologic,immunohistochemical, and molecular diagnostic study. Am J Surg Pathol. 1997;21:354-
9.
77. Parham DM, Roloson GJ, Feely M, Green DM, Bridge JA, Beckwith JB. Primarymalignant neuroepithelial tumors of the kidney: a clinicopathologic analysis of 146 adult
and pediatric cases from the National Wilms' Tumor Study Group Pathology Center. Am
J Surg Pathol. 2001;25:133-46.78. Jimenez RE, Folpe AL, Lapham RL, Ro JY, O'Shea PA, Weiss SW, Amin MB. Primary
Ewing's Sarcoma/Primitive Neuroectodermal Tumor of the Kidney: A Clinicopathologicand Immunohistochemical Analysis of 11 Cases. Am J Surg Pathol. 2002;26:320-7.
79. Quezado M, Benjamin DR, Tsokos M. EWS/FLI-1 fusion transcripts in three peripheral
primitive neuroectodermal tumors of the kidney. Hum Pathol. 1997;28:767-71.
80. Gupta RK, Soni SM, Joshi VV, Cartun R, Kumar A, Jain M. Primary PNET of kidney:report of two cases and review of literature. Indian J Cancer. 2000 Dec; 37(4):184-9.
81. Farrow GM, Harrison EG, Jr., Utz DC, Jones DR. Renal angiomyolipoma. A
clinicopathologic study of 32 cases. Cancer 1968;22:564-70.82. Stone CH, Lee MW, Amin MB, Yaziji H, Gown AM, Ro JY, Tetu B, Paraf F, Zarbo RJ.
Renal angiomyolipoma: further immunophenotypic characterization of an expandingmorphologic spectrum. Arch Pathol Lab Med. 2001;125:751-8
83. Bernstein J, Robbins TO. Renal involvement in tuberous sclerosis. Ann N Y Acad Sci.
1991;615:36-49.
84. Bonetti F, Pea M, Martignoni G, Doglioni C, Zamboni G, Capelli P, Rimondi P, AndrionA. Clear cell ("sugar") tumor of the lung is a lesion strictly related to angiomyolipoma--
the concept of a family of lesions characterized by the presence of the perivascular
epithelioid cells (PEC). Pathology 1994;26:230- 6.254.
85. Hruban RH, Bhagavan BS, Epstein JI. Massive retroperitoneal angiomyolipoma. A lesionthat may be confused with well-differentiated liposarcoma. Am J Clin Pathol.
1989;92:805-8.
86.
Eble JN, Amin MB, Young RH. Epithelioid angiomyolipoma of the kidney: a report offive cases with a prominent and diagnostically confusing epithelioid smooth muscle
component. Am J Surg Pathol. 1997;21:1123-30.
87. Martignoni G, Pea M, Bonetti F, Brunelli M, Eble JN. Oncocytoma-likeangiomyolipoma. A clinicopathologic and immunohistochemical study of 2 cases. Arch
Pathol Lab Med. 2002;126:610-2.

8/9/2019 Renal Tumors in Adults
http://slidepdf.com/reader/full/renal-tumors-in-adults 23/23
Pathology of Renal Tumors in Adults
Dr Manoj Jain
Pathology of Renal Tumors
G P d M i l P th l S i
88. Zavala-Pompa A, Folpe AL, Jimenez RE, Lim SD, Cohen C, Eble JN, Amin MB.
Immunohistochemical study of microphthalmia transcription factor and tyrosinase inangiomyolipoma of the kidney, renal cell carcinoma, and renal and retroperitoneal
sarcomas: comparative evaluation with traditional diagnostic markers. Am J Surg Pathol.
2001;25:65-70.89. Jungbluth AA, Busam KJ, Gerald WL, Stockert E, Coplan KA, Iversen K, MacGregor
DP, Old LJ, Chen YT. A103: An anti-melan-a monoclonal antibody for the detection ofmalignant melanoma in paraffinembedded tissues. Am J Surg Pathol. 1998;22:595-602.
90. Ro JY, Ayala AG, el-Naggar A, Grignon DJ, Hogan SF, Howard DR. Angiomyolipomaof kidney with lymph node involvement. DNA flow cytometric analysis. Arch Pathol Lab
Med. 1990;114:65-7.
91. Ferry JA, Malt RA, Young RH. Renal angiomyolipoma with sarcomatous transformationand pulmonary metastases. Am J Surg Pathol. 1991;15:1083-8.
92. Cibas ES, Goss GA, Kulke MH, Demetri GD, Fletcher CD. Malignant epithelioid
angiomyolipoma ('sarcoma ex angiomyolipoma') of the kidney: a case report and reviewof the literature. Am J Surg Pathol. 2001;25:121-6.
93. Elehence V, Mehta B, Jain M, Gupta RK. Renal Angiomyolipoma: A Clincopathological
study of eleven cases. Indian J Cancer. 2002; 39(2):16-2194. Dineen MK, Venable DD, Misra RP. Pure intrarenal lipoma--report of a case and review
of the literature. J Urol. 1984;132:104-7.95. Ligato S, Ro JY, Tamboli P, Amin MB, Ayala AG. Benign tumors and tumor-like lesions
of the adult kidney. Part I: Benign renal epithelial neoplasms. Adv Anat Pathol. 1999;6:1-
11.
96. Farrow GM, Harrison EG, Jr., Utz DC, ReMine WH. Sarcomas and sarcomatoid andmixed malignant tumors of the kidney in adults. I. Cancer. 1968;22:545-50.
97. Farrow GM, Harrison EG, Jr., Utz DC. Sarcomas and sarcomatoid and mixed malignant
tumors of the kidney in adults. II. Cancer 1968;22:551-5.98. Srinivas V, Sogani PC, Hajdu SI, Whitmore WF, Jr. Sarcomas of the kidney. J Urol.
1984;132:13-6.
Address for Correspondence:
Dr Manoj Jain
Associate Professor Department of Pathology
Sanjay Gandhi Postgraduate
Institute of Medical Sciences Lucknow- 226014
Email: [email protected]







![4- GU Onc351[1] Semester/Surgery/22- Common...Adrenal Tumors. Renal Tumors. Renal Tumors Benign tumours of the kidney are rare All renal neoplasms should be regarded as potentially](https://img.pdfslide.net/doc/110x75/5f0983b17e708231d4273048/4-gu-onc3511-semestersurgery22-common-adrenal-tumors-renal-tumors-renal.jpg)