Embed Size (px)
Citation preview

Research ArticleChanges in Mitral Annular Ascent withWorsening Echocardiographic Parameters ofLeft Ventricular Diastolic Function
Paula M Hernaacutendez Burgos1 and Angel Loacutepez-Candales2
1University of Puerto Rico School of Medicine PO Box 365067 San Juan PR 00936-5067 USA2Cardiovascular Medicine Division University of Puerto Rico School of Medicine Medical Sciences CampusPO Box 365067 San Juan PR 00936-5067 USA
Correspondence should be addressed to Angel Lopez-Candales candales33gmailcom
Received 2 December 2015 Revised 4 February 2016 Accepted 8 February 2016
Academic Editor Michael S Firstenberg
Copyright copy 2016 P M Hernandez Burgos and A Lopez-Candales This is an open access article distributed under the CreativeCommons Attribution License which permits unrestricted use distribution and reproduction in any medium provided theoriginal work is properly cited
Background While the mitral annular plane systolic excursion (MAPSE) has been suggested as a surrogate measurement ofleft ventricular ejection fraction less is known about the relative value of mitral annular ascent (MAa) Methods Our databasewas queried for complete transthoracic echocardiograms performed for any clinical indication Baseline echocardiographicmeasurements were compared to determine any correlation between MAa and traditional Echo-Doppler echocardiographicmeasures to characterize left ventricular diastolic dysfunction (LVDD) Results Patients with normal LV diastolic function wereyounger (41plusmn13 years) than patients with LVDD (stage 1 61plusmn13 years stage 2 57plusmn14 years and stage 3 66plusmn17 years 119901 = 0156)LV ejection fraction decreased in patients with stage 2 LVDD (63 plusmn 17) and was further reduced in patients with stage 3 LVDD(28 plusmn 21 119901 = 0003) Discussion While a vigorous MAa excursion was seen in patients with stage 1 LVDD MAa significantlydecreased in stage 2 and stage 3 LVDD patients Our results highlight the importance of atrioventricular coupling as MAa motionseems to reflect changes in left atrial pressure Additional studies are now required to better examine atrioventricular interactionsand electromechanical coupling that might improve our assessment of LV diastolic function
1 Introduction
Measuring the maximal descent of the mitral annulus duringsystole commonly referred to asmitral annular plane systolicexcursion (MAPSE) has been suggested as a surrogatemeasurement of left ventricular ejection fraction (LVEF) [1ndash4] In contrast less is known about the relative value ofmitral annular ascent (MAa) that occurs late in LV diastoleparticularly after atrial contraction while in normal sinusrhythm
Given the temporal relation of the mechanical events inlate diastole we sought to determine if there was any corre-lation between MAa and traditional Echo-Doppler echocar-diographic measures to characterize left ventricular diastolicdysfunction (LVDD) currently used as recommended byboth the American Society of Echocardiography (ASE) andEuropean Association of Echocardiography [5ndash7]
2 Methods
For this retrospective study our echocardiographic databasewas queried for complete transthoracic echocardiogramsperformed for any clinical indication at the University ofCincinnati College of Medicine Main University HospitalEchocardiography Laboratory Inclusion variables includenormal sinus rhythm at the time of the examination goodvisualization of both the LA and LV endocardium andcomplete spectral Doppler study with M-mode tracings andtissue Doppler interrogation of the lateral portion of the MAwith clear signals in all studies [5] In contrast data frompatients with frequent premature or atrial contraction beatsprevious myocardial infarction valve disease worse thanmild pulmonary hypertension previous cardiac surgery leftbundle branch block pericardial disease or the presence ofa pacer or defibrillator wire were not included LV diastolic
Hindawi Publishing CorporationScientificaVolume 2016 Article ID 6303815 4 pageshttpdxdoiorg10115520166303815
2 Scientifica
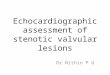
Figure 1 Representative M-mode tracing showing maximal mitralannular plane systolic motion MA ascent (MAa) was measured asthe distance of the annulus traversed from the end of diastasis untilthe end of atrial contraction (white arrow) from the imaginary linedrawn (dotted white line) that represents annular motion duringdiastasis with the sharp ascent (downward slope) towards the atriaafter atrial contraction Please note that typically several lines arealways seen when performing M-mode of the MA due to thecontribution of chordal structures However since these imageshave the same frequency their reflected images maintain the samedistance Usually the most reflective echo-bright image should beused for the purpose of measurements as shown in this figureMAPSE is also shown
function was classified as normal (0) impaired relaxation(1) pseudonormal (2) and restrictive pattern (3) followingpublished recommendations as suggested by Nagueh andassociates [5]
Two-dimensional echocardiographic studies were per-formed using commercially available systems (Vivid 7 andVivid 9 GE Medical Systems Milwaukee WI USA) Basedon previous findings by our laboratory pulsed-wave tissueDoppler imaging (TDI) was only performed on the lateralportion of the MA for assessing maximal MA excursionand MAa [3 4] MAa was measured as the distance of thelateral annulus traversed from the end of diastasis until theend of atrial contraction (Figure 1) [4] Echocardiographicparameters were calculated using the commercially availablesoftware Merge Cardio Workstation and determined by asingle observer All continuous data are presented as meanplusmn standard deviation and categorical data as frequenciesBaseline characteristics were compared between groups usinganalysis of variance (ANOVA) and Fisherrsquos exact test for con-tinuous and categorical data respectively Echocardiographicmeasurements were compared using two-tailed unpaired 119905-test assuming unequal variances In order to assess repro-ducibility of MAa measurements the intraclass correlationcoefficient was used
Study approval was obtained from the University ofCincinnati IRB office (Protocol number 12061302) and sincethis was a retrospective study there was no need for writtenconsent
3 Results
The main echocardiographic data from 150 patients per-formed for any clinical indication was collected and includedfor final analysis as shown in Table 1 Patients with normal LV
diastolic function were younger (41 plusmn 13 years) than patientswith LVDD (stage 1 61 plusmn 13 stage 2 57 plusmn 14 and stage 366 plusmn 17 years 119901 = 0156)
Evaluation of LV systolic function demonstrated that LVejection fraction began decreasing in patients with stage 2LVDD (63 plusmn 17) and was further reduced in those patientswith stage 3 LVDD (28 plusmn 21 119901 = 0003)
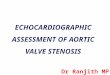
When evaluating other echocardiographic parameterswe found the traditional MV EA ratio pattern with worsen-ing LVDD(Figure 2(a)) aswell as an increase in both LVmassindex (Figure 2(b)) and left atrial volume index (Figure 2(c))with worsening LVDD parameters
Furthermore mean and standard deviation values forMAa lateral MA TDI A1015840 and MVMA TDI E1015840 values forthe study population according to LV diastolic function areshown in Table 2
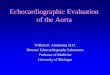
A representative image showing the changes in MAaexcursion with regard to LV diastolic function is shown inFigure 3
Finally interrater agreement (120581 Kappa) value assess-ment was used to measure variability in terms of MAameasurements The strength of the agreement was moderate(120581 = 0546 standard error = 0158 and 95 CI = 0237to 0855) when two untrained observers reproduced MAameasurements and was very good (120581 = 0985 standard error= 0094 and 95CI = 0711 to 1000) if a trained observer wasperforming these measurements
4 Discussion
For the first time to our knowledge an apparent relationshipbetween MAa motion and LVDD was identified Specificallya vigorous MAa excursion was exclusively seen in patientswith stage 1 LVDD when compared to the rest of the studiedpopulation including patients with normal LV diastolicfunction Moreover MAa significantly decreased in stage 2LVDD patients while the lowest MAa values were seen instage 3 LVDD patients
LV relaxation is known to occurwith a concomitant activemovement of the MA away from the apex [5] The velocityof this MA motion has been demonstrated to correlate wellwith how fast the LV fills and relaxes [6ndash10] but the effectof LV diastole with regard to the late MAa component hadnever been examined From a mechanistic point of viewthe first question would be why to consider this late MAaascent motion of the annulus with regard to LV diastole Inprinciple this portion of MA motion should correspond toLV compliance Hence problems with increased left atrialpressurewould bemainly seen during this portion of diastoleConsequently by examining this relationship we would beexploring novel information not previously investigated andalso developing a new venue for examining the axiome-chanical relationship known to exist between left atria andventricle (atrioventricular interactions) all throughout thecardiac cycle
The following are the most important limitations thatneed to be addressed retrospective nature of the studysmall number of patients included into the final analysisexclusion of other pathological events that could affect MAa
Scientifica 3
Table 1 Clinical indication to perform echocardiogram
Main indications LVDDD 0 LVDD 1 LVDD 2 LVDD 3Hypertension 2 23 22 0Postcerebrovascular accident 4 8 0 0Pulmonary causes 5 5 0 0Renal causes 3 9 7 2Coronary disease 0 5 3 0Heart failure 0 0 8 0Other 21 5 0 18
Table 2 Results for MAa lateral MA TDI A1015840 and MVMA TDI E1015840 values for the study population according to LV diastolic function
Variables LVDD 0(119873 = 35)
LVDD 1(119873 = 55)
LVDD 2(119873 = 40)
LVDD 3(119873 = 20) ANOVA
Lateral MA TDI A1015840 8 plusmn 2 11 plusmn 3 7 plusmn 3 4 plusmn 2 001MV EMA TDI E1015840 ratio 56 plusmn 26 94 plusmn 48 151 plusmn 72 210 plusmn 146 lt0001MAa 046 plusmn 013 061 plusmn 014 041 plusmn 013 018 plusmn 05 lt0001
LVDD 3LVDD 2LVDD 1LVDD 00
05
1
15
2
25
3
35
4
45
5
MV
EA
ratio
(a)LVDD 3LVDD 2LVDD 1LVDD 0
0
20
40
60
80
100
120
140
160
180LV
MI
(b)
LVDD 3LVDD 2LVDD 1LVDD 00
10
20
30
40
50
60
LAV
I
(c)
Figure 2 (a) Box plot showingMVEA ratiomean and standard deviation values for each stage of LV diastolic function (b) Box plot showingLV mass index (LVMI) mean and standard deviation values for each stage of LV diastolic function (c) Box plot showing left atrial volumeindex (LAVI) mean and standard deviation values for each stage of LV diastolic function
measurements and lack of speckle-tracking imaging Inaddition we did not include data of MAa measurementsduring exercise particularly when there are a significantnumber of patients that are diagnosed with LVDD duringexercise [11] However the main goal was attained Finallyonly the lateral portion of theMAwas used tomeasureTDIE1015840velocity in order to assess global LV diastolic function Sincethis was the first attempt in correlating MAa excursion withdiastolic MA velocities it would make sense to only use the
lateral portion MA which is known to move the fastest andhas the greatest overall displacement [7 8]
Even though we are not proposing the use of MAa asadditional measure to asses LVDD our results highlightthe importance of atrioventricular coupling as MAa motionseems to reflect changes in LA pressure known to occur withworsening LVDDThis perhaps suggests the need for a morecomprehensive integration of atrioventricular interactionswhen assessing LV diastolic function
4 Scientifica
(a) (b) (c)
Figure 3 MAa M-mode images are shown to demonstrate the observed differences in MAa (a) shows the M-mode tracing that is arepresentative MAa image of a patient with stage 1 LVDD (b) demonstrates a representative MAa of a patient with stage 2 LVDD and (c) anMAa tracing of a patient with stage 3 LVDD Solid lines represent site of measurement while the arrows represent actual MAameasure Pleasenote the relative magnitude of each MAa by the size of the arrow
Competing Interests
The authors declare that they have no competing interests
References
[1] J Matos I Kronzon G Panagopoulos and G Perk ldquoMitralannular plane systolic excursion as a surrogate for left ven-tricular ejection fractionrdquo Journal of the American Society ofEchocardiography vol 25 no 9 pp 969ndash974 2012
[2] W Adel A M Roushdy and M Nabil ldquoMitral annular planesystolic excursion-derived ejection fraction a simple and validtool in adult males with left ventricular systolic dysfunctionrdquoEchocardiography vol 33 no 2 pp 179ndash184 2016
[3] R Bazaz K Edelman B Gulyasy and A Lopez-Candales ldquoEvi-dence of robust coupling of atrioventricular mechanical func-tion of the right side of the heart insights fromM-mode analysisof annular motionrdquo Echocardiography vol 25 no 6 pp 557ndash561 2008
[4] A Lopez-Candales N Rajagopalan B Gulyasy K Edelmanand R Bazaz ldquoComparative echocardiographic analysis ofmitral and tricuspid annularmotion differences explained withproposed anatomic-structural correlatesrdquo Echocardiographyvol 24 no 4 pp 353ndash359 2007
[5] J KOh S-J Park and S FNagueh ldquoEstablished andnovel clin-ical applications of diastolic function assessment by echocar-diographyrdquo Circulation Cardiovascular Imaging vol 4 no 4pp 444ndash455 2011
[6] S F Nagueh C P Appleton T C Gillebert et al ldquoRecommen-dations for the evaluation of left ventricular diastolic functionby echocardiographyrdquo European Journal of Echocardiographyvol 10 no 2 pp 165ndash193 2009
[7] W J Paulus C Tschope J E Sanderson et al ldquoHow to diagnosediastolic heart failure a consensus statement on the diagnosisof heart failure with normal left ventricular ejection fraction
by the Heart Failure and Echocardiography Associations of theEuropean Society of Cardiologyrdquo European Heart Journal vol28 no 20 pp 2539ndash2550 2007
[8] RM LangM Bierig R B Devereux et al ldquoRecommendationsfor chamber quantification a report from the American Societyof Echocardiographyrsquos guidelines and standards committee andthe Chamber Quantification Writing Group developed in con-junction with the European Association of Echocardiographya branch of the European Society of Cardiologyrdquo Journal of theAmerican Society of Echocardiography vol 18 no 12 pp 1440ndash1463 2005
[9] S R Ommen R A Nishimura C P Appleton et al ldquoClin-ical utility of Doppler echocardiography and tissue Dopplerimaging in the estimation of left ventricular filling pressuresa comparative simultaneous Doppler-catheterization studyrdquoCirculation vol 102 no 15 pp 1788ndash1794 2000
[10] D-W Sohn I-H Chai D-J Lee et al ldquoAssessment of mitralannulus velocity by Doppler tissue imaging in the evaluationof left ventricular diastolic functionrdquo Journal of the AmericanCollege of Cardiology vol 30 no 2 pp 474ndash480 1997
[11] Y T Tan F Wenzelburger E Lee et al ldquoReduced left atrialfunction on exercise in patients with heart failure and normalejection fractionrdquo Heart vol 96 no 13 pp 1017ndash1023 2010
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

2 Scientifica
Figure 1 Representative M-mode tracing showing maximal mitralannular plane systolic motion MA ascent (MAa) was measured asthe distance of the annulus traversed from the end of diastasis untilthe end of atrial contraction (white arrow) from the imaginary linedrawn (dotted white line) that represents annular motion duringdiastasis with the sharp ascent (downward slope) towards the atriaafter atrial contraction Please note that typically several lines arealways seen when performing M-mode of the MA due to thecontribution of chordal structures However since these imageshave the same frequency their reflected images maintain the samedistance Usually the most reflective echo-bright image should beused for the purpose of measurements as shown in this figureMAPSE is also shown
function was classified as normal (0) impaired relaxation(1) pseudonormal (2) and restrictive pattern (3) followingpublished recommendations as suggested by Nagueh andassociates [5]
Two-dimensional echocardiographic studies were per-formed using commercially available systems (Vivid 7 andVivid 9 GE Medical Systems Milwaukee WI USA) Basedon previous findings by our laboratory pulsed-wave tissueDoppler imaging (TDI) was only performed on the lateralportion of the MA for assessing maximal MA excursionand MAa [3 4] MAa was measured as the distance of thelateral annulus traversed from the end of diastasis until theend of atrial contraction (Figure 1) [4] Echocardiographicparameters were calculated using the commercially availablesoftware Merge Cardio Workstation and determined by asingle observer All continuous data are presented as meanplusmn standard deviation and categorical data as frequenciesBaseline characteristics were compared between groups usinganalysis of variance (ANOVA) and Fisherrsquos exact test for con-tinuous and categorical data respectively Echocardiographicmeasurements were compared using two-tailed unpaired 119905-test assuming unequal variances In order to assess repro-ducibility of MAa measurements the intraclass correlationcoefficient was used
Study approval was obtained from the University ofCincinnati IRB office (Protocol number 12061302) and sincethis was a retrospective study there was no need for writtenconsent
3 Results
The main echocardiographic data from 150 patients per-formed for any clinical indication was collected and includedfor final analysis as shown in Table 1 Patients with normal LV
diastolic function were younger (41 plusmn 13 years) than patientswith LVDD (stage 1 61 plusmn 13 stage 2 57 plusmn 14 and stage 366 plusmn 17 years 119901 = 0156)
Evaluation of LV systolic function demonstrated that LVejection fraction began decreasing in patients with stage 2LVDD (63 plusmn 17) and was further reduced in those patientswith stage 3 LVDD (28 plusmn 21 119901 = 0003)
When evaluating other echocardiographic parameterswe found the traditional MV EA ratio pattern with worsen-ing LVDD(Figure 2(a)) aswell as an increase in both LVmassindex (Figure 2(b)) and left atrial volume index (Figure 2(c))with worsening LVDD parameters
Furthermore mean and standard deviation values forMAa lateral MA TDI A1015840 and MVMA TDI E1015840 values forthe study population according to LV diastolic function areshown in Table 2
A representative image showing the changes in MAaexcursion with regard to LV diastolic function is shown inFigure 3
Finally interrater agreement (120581 Kappa) value assess-ment was used to measure variability in terms of MAameasurements The strength of the agreement was moderate(120581 = 0546 standard error = 0158 and 95 CI = 0237to 0855) when two untrained observers reproduced MAameasurements and was very good (120581 = 0985 standard error= 0094 and 95CI = 0711 to 1000) if a trained observer wasperforming these measurements
4 Discussion
For the first time to our knowledge an apparent relationshipbetween MAa motion and LVDD was identified Specificallya vigorous MAa excursion was exclusively seen in patientswith stage 1 LVDD when compared to the rest of the studiedpopulation including patients with normal LV diastolicfunction Moreover MAa significantly decreased in stage 2LVDD patients while the lowest MAa values were seen instage 3 LVDD patients
LV relaxation is known to occurwith a concomitant activemovement of the MA away from the apex [5] The velocityof this MA motion has been demonstrated to correlate wellwith how fast the LV fills and relaxes [6ndash10] but the effectof LV diastole with regard to the late MAa component hadnever been examined From a mechanistic point of viewthe first question would be why to consider this late MAaascent motion of the annulus with regard to LV diastole Inprinciple this portion of MA motion should correspond toLV compliance Hence problems with increased left atrialpressurewould bemainly seen during this portion of diastoleConsequently by examining this relationship we would beexploring novel information not previously investigated andalso developing a new venue for examining the axiome-chanical relationship known to exist between left atria andventricle (atrioventricular interactions) all throughout thecardiac cycle
The following are the most important limitations thatneed to be addressed retrospective nature of the studysmall number of patients included into the final analysisexclusion of other pathological events that could affect MAa
Scientifica 3
Table 1 Clinical indication to perform echocardiogram
Main indications LVDDD 0 LVDD 1 LVDD 2 LVDD 3Hypertension 2 23 22 0Postcerebrovascular accident 4 8 0 0Pulmonary causes 5 5 0 0Renal causes 3 9 7 2Coronary disease 0 5 3 0Heart failure 0 0 8 0Other 21 5 0 18
Table 2 Results for MAa lateral MA TDI A1015840 and MVMA TDI E1015840 values for the study population according to LV diastolic function
Variables LVDD 0(119873 = 35)
LVDD 1(119873 = 55)
LVDD 2(119873 = 40)
LVDD 3(119873 = 20) ANOVA
Lateral MA TDI A1015840 8 plusmn 2 11 plusmn 3 7 plusmn 3 4 plusmn 2 001MV EMA TDI E1015840 ratio 56 plusmn 26 94 plusmn 48 151 plusmn 72 210 plusmn 146 lt0001MAa 046 plusmn 013 061 plusmn 014 041 plusmn 013 018 plusmn 05 lt0001
LVDD 3LVDD 2LVDD 1LVDD 00
05
1
15
2
25
3
35
4
45
5
MV
EA
ratio
(a)LVDD 3LVDD 2LVDD 1LVDD 0
0
20
40
60
80
100
120
140
160
180LV
MI
(b)
LVDD 3LVDD 2LVDD 1LVDD 00
10
20
30
40
50
60
LAV
I
(c)
Figure 2 (a) Box plot showingMVEA ratiomean and standard deviation values for each stage of LV diastolic function (b) Box plot showingLV mass index (LVMI) mean and standard deviation values for each stage of LV diastolic function (c) Box plot showing left atrial volumeindex (LAVI) mean and standard deviation values for each stage of LV diastolic function
measurements and lack of speckle-tracking imaging Inaddition we did not include data of MAa measurementsduring exercise particularly when there are a significantnumber of patients that are diagnosed with LVDD duringexercise [11] However the main goal was attained Finallyonly the lateral portion of theMAwas used tomeasureTDIE1015840velocity in order to assess global LV diastolic function Sincethis was the first attempt in correlating MAa excursion withdiastolic MA velocities it would make sense to only use the
lateral portion MA which is known to move the fastest andhas the greatest overall displacement [7 8]
Even though we are not proposing the use of MAa asadditional measure to asses LVDD our results highlightthe importance of atrioventricular coupling as MAa motionseems to reflect changes in LA pressure known to occur withworsening LVDDThis perhaps suggests the need for a morecomprehensive integration of atrioventricular interactionswhen assessing LV diastolic function
4 Scientifica
(a) (b) (c)
Figure 3 MAa M-mode images are shown to demonstrate the observed differences in MAa (a) shows the M-mode tracing that is arepresentative MAa image of a patient with stage 1 LVDD (b) demonstrates a representative MAa of a patient with stage 2 LVDD and (c) anMAa tracing of a patient with stage 3 LVDD Solid lines represent site of measurement while the arrows represent actual MAameasure Pleasenote the relative magnitude of each MAa by the size of the arrow
Competing Interests
The authors declare that they have no competing interests
References
[1] J Matos I Kronzon G Panagopoulos and G Perk ldquoMitralannular plane systolic excursion as a surrogate for left ven-tricular ejection fractionrdquo Journal of the American Society ofEchocardiography vol 25 no 9 pp 969ndash974 2012
[2] W Adel A M Roushdy and M Nabil ldquoMitral annular planesystolic excursion-derived ejection fraction a simple and validtool in adult males with left ventricular systolic dysfunctionrdquoEchocardiography vol 33 no 2 pp 179ndash184 2016
[3] R Bazaz K Edelman B Gulyasy and A Lopez-Candales ldquoEvi-dence of robust coupling of atrioventricular mechanical func-tion of the right side of the heart insights fromM-mode analysisof annular motionrdquo Echocardiography vol 25 no 6 pp 557ndash561 2008
[4] A Lopez-Candales N Rajagopalan B Gulyasy K Edelmanand R Bazaz ldquoComparative echocardiographic analysis ofmitral and tricuspid annularmotion differences explained withproposed anatomic-structural correlatesrdquo Echocardiographyvol 24 no 4 pp 353ndash359 2007
[5] J KOh S-J Park and S FNagueh ldquoEstablished andnovel clin-ical applications of diastolic function assessment by echocar-diographyrdquo Circulation Cardiovascular Imaging vol 4 no 4pp 444ndash455 2011
[6] S F Nagueh C P Appleton T C Gillebert et al ldquoRecommen-dations for the evaluation of left ventricular diastolic functionby echocardiographyrdquo European Journal of Echocardiographyvol 10 no 2 pp 165ndash193 2009
[7] W J Paulus C Tschope J E Sanderson et al ldquoHow to diagnosediastolic heart failure a consensus statement on the diagnosisof heart failure with normal left ventricular ejection fraction
by the Heart Failure and Echocardiography Associations of theEuropean Society of Cardiologyrdquo European Heart Journal vol28 no 20 pp 2539ndash2550 2007
[8] RM LangM Bierig R B Devereux et al ldquoRecommendationsfor chamber quantification a report from the American Societyof Echocardiographyrsquos guidelines and standards committee andthe Chamber Quantification Writing Group developed in con-junction with the European Association of Echocardiographya branch of the European Society of Cardiologyrdquo Journal of theAmerican Society of Echocardiography vol 18 no 12 pp 1440ndash1463 2005
[9] S R Ommen R A Nishimura C P Appleton et al ldquoClin-ical utility of Doppler echocardiography and tissue Dopplerimaging in the estimation of left ventricular filling pressuresa comparative simultaneous Doppler-catheterization studyrdquoCirculation vol 102 no 15 pp 1788ndash1794 2000
[10] D-W Sohn I-H Chai D-J Lee et al ldquoAssessment of mitralannulus velocity by Doppler tissue imaging in the evaluationof left ventricular diastolic functionrdquo Journal of the AmericanCollege of Cardiology vol 30 no 2 pp 474ndash480 1997
[11] Y T Tan F Wenzelburger E Lee et al ldquoReduced left atrialfunction on exercise in patients with heart failure and normalejection fractionrdquo Heart vol 96 no 13 pp 1017ndash1023 2010
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

Scientifica 3
Table 1 Clinical indication to perform echocardiogram
Main indications LVDDD 0 LVDD 1 LVDD 2 LVDD 3Hypertension 2 23 22 0Postcerebrovascular accident 4 8 0 0Pulmonary causes 5 5 0 0Renal causes 3 9 7 2Coronary disease 0 5 3 0Heart failure 0 0 8 0Other 21 5 0 18
Table 2 Results for MAa lateral MA TDI A1015840 and MVMA TDI E1015840 values for the study population according to LV diastolic function
Variables LVDD 0(119873 = 35)
LVDD 1(119873 = 55)
LVDD 2(119873 = 40)
LVDD 3(119873 = 20) ANOVA
Lateral MA TDI A1015840 8 plusmn 2 11 plusmn 3 7 plusmn 3 4 plusmn 2 001MV EMA TDI E1015840 ratio 56 plusmn 26 94 plusmn 48 151 plusmn 72 210 plusmn 146 lt0001MAa 046 plusmn 013 061 plusmn 014 041 plusmn 013 018 plusmn 05 lt0001
LVDD 3LVDD 2LVDD 1LVDD 00
05
1
15
2
25
3
35
4
45
5
MV
EA
ratio
(a)LVDD 3LVDD 2LVDD 1LVDD 0
0
20
40
60
80
100
120
140
160
180LV
MI
(b)
LVDD 3LVDD 2LVDD 1LVDD 00
10
20
30
40
50
60
LAV
I
(c)
Figure 2 (a) Box plot showingMVEA ratiomean and standard deviation values for each stage of LV diastolic function (b) Box plot showingLV mass index (LVMI) mean and standard deviation values for each stage of LV diastolic function (c) Box plot showing left atrial volumeindex (LAVI) mean and standard deviation values for each stage of LV diastolic function
measurements and lack of speckle-tracking imaging Inaddition we did not include data of MAa measurementsduring exercise particularly when there are a significantnumber of patients that are diagnosed with LVDD duringexercise [11] However the main goal was attained Finallyonly the lateral portion of theMAwas used tomeasureTDIE1015840velocity in order to assess global LV diastolic function Sincethis was the first attempt in correlating MAa excursion withdiastolic MA velocities it would make sense to only use the
lateral portion MA which is known to move the fastest andhas the greatest overall displacement [7 8]
Even though we are not proposing the use of MAa asadditional measure to asses LVDD our results highlightthe importance of atrioventricular coupling as MAa motionseems to reflect changes in LA pressure known to occur withworsening LVDDThis perhaps suggests the need for a morecomprehensive integration of atrioventricular interactionswhen assessing LV diastolic function
4 Scientifica
(a) (b) (c)
Figure 3 MAa M-mode images are shown to demonstrate the observed differences in MAa (a) shows the M-mode tracing that is arepresentative MAa image of a patient with stage 1 LVDD (b) demonstrates a representative MAa of a patient with stage 2 LVDD and (c) anMAa tracing of a patient with stage 3 LVDD Solid lines represent site of measurement while the arrows represent actual MAameasure Pleasenote the relative magnitude of each MAa by the size of the arrow
Competing Interests
The authors declare that they have no competing interests
References
[1] J Matos I Kronzon G Panagopoulos and G Perk ldquoMitralannular plane systolic excursion as a surrogate for left ven-tricular ejection fractionrdquo Journal of the American Society ofEchocardiography vol 25 no 9 pp 969ndash974 2012
[2] W Adel A M Roushdy and M Nabil ldquoMitral annular planesystolic excursion-derived ejection fraction a simple and validtool in adult males with left ventricular systolic dysfunctionrdquoEchocardiography vol 33 no 2 pp 179ndash184 2016
[3] R Bazaz K Edelman B Gulyasy and A Lopez-Candales ldquoEvi-dence of robust coupling of atrioventricular mechanical func-tion of the right side of the heart insights fromM-mode analysisof annular motionrdquo Echocardiography vol 25 no 6 pp 557ndash561 2008
[4] A Lopez-Candales N Rajagopalan B Gulyasy K Edelmanand R Bazaz ldquoComparative echocardiographic analysis ofmitral and tricuspid annularmotion differences explained withproposed anatomic-structural correlatesrdquo Echocardiographyvol 24 no 4 pp 353ndash359 2007
[5] J KOh S-J Park and S FNagueh ldquoEstablished andnovel clin-ical applications of diastolic function assessment by echocar-diographyrdquo Circulation Cardiovascular Imaging vol 4 no 4pp 444ndash455 2011
[6] S F Nagueh C P Appleton T C Gillebert et al ldquoRecommen-dations for the evaluation of left ventricular diastolic functionby echocardiographyrdquo European Journal of Echocardiographyvol 10 no 2 pp 165ndash193 2009
[7] W J Paulus C Tschope J E Sanderson et al ldquoHow to diagnosediastolic heart failure a consensus statement on the diagnosisof heart failure with normal left ventricular ejection fraction
by the Heart Failure and Echocardiography Associations of theEuropean Society of Cardiologyrdquo European Heart Journal vol28 no 20 pp 2539ndash2550 2007
[8] RM LangM Bierig R B Devereux et al ldquoRecommendationsfor chamber quantification a report from the American Societyof Echocardiographyrsquos guidelines and standards committee andthe Chamber Quantification Writing Group developed in con-junction with the European Association of Echocardiographya branch of the European Society of Cardiologyrdquo Journal of theAmerican Society of Echocardiography vol 18 no 12 pp 1440ndash1463 2005
[9] S R Ommen R A Nishimura C P Appleton et al ldquoClin-ical utility of Doppler echocardiography and tissue Dopplerimaging in the estimation of left ventricular filling pressuresa comparative simultaneous Doppler-catheterization studyrdquoCirculation vol 102 no 15 pp 1788ndash1794 2000
[10] D-W Sohn I-H Chai D-J Lee et al ldquoAssessment of mitralannulus velocity by Doppler tissue imaging in the evaluationof left ventricular diastolic functionrdquo Journal of the AmericanCollege of Cardiology vol 30 no 2 pp 474ndash480 1997
[11] Y T Tan F Wenzelburger E Lee et al ldquoReduced left atrialfunction on exercise in patients with heart failure and normalejection fractionrdquo Heart vol 96 no 13 pp 1017ndash1023 2010
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

4 Scientifica
(a) (b) (c)
Figure 3 MAa M-mode images are shown to demonstrate the observed differences in MAa (a) shows the M-mode tracing that is arepresentative MAa image of a patient with stage 1 LVDD (b) demonstrates a representative MAa of a patient with stage 2 LVDD and (c) anMAa tracing of a patient with stage 3 LVDD Solid lines represent site of measurement while the arrows represent actual MAameasure Pleasenote the relative magnitude of each MAa by the size of the arrow
Competing Interests
The authors declare that they have no competing interests
References
[1] J Matos I Kronzon G Panagopoulos and G Perk ldquoMitralannular plane systolic excursion as a surrogate for left ven-tricular ejection fractionrdquo Journal of the American Society ofEchocardiography vol 25 no 9 pp 969ndash974 2012
[2] W Adel A M Roushdy and M Nabil ldquoMitral annular planesystolic excursion-derived ejection fraction a simple and validtool in adult males with left ventricular systolic dysfunctionrdquoEchocardiography vol 33 no 2 pp 179ndash184 2016
[3] R Bazaz K Edelman B Gulyasy and A Lopez-Candales ldquoEvi-dence of robust coupling of atrioventricular mechanical func-tion of the right side of the heart insights fromM-mode analysisof annular motionrdquo Echocardiography vol 25 no 6 pp 557ndash561 2008
[4] A Lopez-Candales N Rajagopalan B Gulyasy K Edelmanand R Bazaz ldquoComparative echocardiographic analysis ofmitral and tricuspid annularmotion differences explained withproposed anatomic-structural correlatesrdquo Echocardiographyvol 24 no 4 pp 353ndash359 2007
[5] J KOh S-J Park and S FNagueh ldquoEstablished andnovel clin-ical applications of diastolic function assessment by echocar-diographyrdquo Circulation Cardiovascular Imaging vol 4 no 4pp 444ndash455 2011
[6] S F Nagueh C P Appleton T C Gillebert et al ldquoRecommen-dations for the evaluation of left ventricular diastolic functionby echocardiographyrdquo European Journal of Echocardiographyvol 10 no 2 pp 165ndash193 2009
[7] W J Paulus C Tschope J E Sanderson et al ldquoHow to diagnosediastolic heart failure a consensus statement on the diagnosisof heart failure with normal left ventricular ejection fraction
by the Heart Failure and Echocardiography Associations of theEuropean Society of Cardiologyrdquo European Heart Journal vol28 no 20 pp 2539ndash2550 2007
[8] RM LangM Bierig R B Devereux et al ldquoRecommendationsfor chamber quantification a report from the American Societyof Echocardiographyrsquos guidelines and standards committee andthe Chamber Quantification Writing Group developed in con-junction with the European Association of Echocardiographya branch of the European Society of Cardiologyrdquo Journal of theAmerican Society of Echocardiography vol 18 no 12 pp 1440ndash1463 2005
[9] S R Ommen R A Nishimura C P Appleton et al ldquoClin-ical utility of Doppler echocardiography and tissue Dopplerimaging in the estimation of left ventricular filling pressuresa comparative simultaneous Doppler-catheterization studyrdquoCirculation vol 102 no 15 pp 1788ndash1794 2000
[10] D-W Sohn I-H Chai D-J Lee et al ldquoAssessment of mitralannulus velocity by Doppler tissue imaging in the evaluationof left ventricular diastolic functionrdquo Journal of the AmericanCollege of Cardiology vol 30 no 2 pp 474ndash480 1997
[11] Y T Tan F Wenzelburger E Lee et al ldquoReduced left atrialfunction on exercise in patients with heart failure and normalejection fractionrdquo Heart vol 96 no 13 pp 1017ndash1023 2010
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom