Embed Size (px)
Citation preview

Retinal Detachment after Branch Retinal Vein Occlusion
Influence of the Type of Break on the Outcome of Vitreous Surgery
Yasushi Ikuno, MD, 1,2 Yasuo T ano, MD,z John Michael Lewis, MD,z Tsunehiko Ikeda, MD,3 Yukihiro Sato, MD4
Background: Branch retinal vein occlusion (BRVO) is occasionally complicated by two types of retinal breaks (retinal holes without vitreous traction or retinal traction tears) that may lead to a rhegmatogenous retinal detachment (RRO). The authors describe surgical results of vitrectomy for RRO after BRVO and investigate whether there is any difference between clinical features or surgical results from eyes with the two types of retinal breaks.
Patients and Methods: The authors retrospectively studied 25 patients (25 eyes) who underwent vitrectomy for RRO after BRVO. Twelve of 25 eyes (48%) had a detachment secondary to one or more retinal holes (group I), and 13 of the eyes (52%) had one or more retinal tears (group II).
Results: Seventeen of the eyes (68%) achieved total retinal reattachment after the initial surgery; 22 (88%) did so by the time of final examination. Patients with retinal holes achieved more favorable final vision than those with retinal tears (P = 0.0391). A higher rate of preoperative macular detachment (P = 0.0112) and a higher rate of recurrent retinal detachment after initial vitrectomy (P = 0.0302) were the factors associated with the reduced final visual acuity in patients with retinal tears. The increased rate of recurrent retinal detachment in patients with retinal tears was associated with a higher rate of existing preretinal neovascular membranes (P = 0.0112) and a trend toward an increased incidence of intraoperative iatrogenic retinal breaks.
Conclusion: Among patients who undergo vitrectomy for RRO after BRVO, better surgical results are expected in eyes with retinal holes without vitreous traction than in those with retinal traction tears. This difference is thought to be due to the difference in vitreoretinal anatomy between eyes with the two types of retinal breaks. Ophthalmology 1997; 104:27-32
Branch retinal vein occlusion (BRVO) often leads to reduced visual acuity due to macular edema, l surface wrin-
Originally received: March 6, 1996. Revision accepted: August 8, 1996.
I Division of Ophthalmology, Osaka National Hospital, Osaka, Japan.
2 Department of Ophthalmology, Osaka University Medical School, Osaka, Japan.
kling retinopathy,2 or serous retinal detachment?.4 Neovascularization is also relatively common and, as a result, vitreous hemorrhage1.2 or traction retinal detachment may develop.s Midperipheral retinal photocoagulation is available to prevent retinal neovascularization,6 and vitrectomy is a useful treatment for vitreous hemorrhage.7
3 Department of Ophthalmology, Kyoto Prefectural University of Medicine, Kyoto, Japan.
4 Department of Ophthalmology, Surugadai Hospital of Nihon University, Tokyo, Japan.
Reprint requests to Yasushi !kuno, MD, Department of Ophthalmology, Osaka University Medical School, 2-2 Yamadaoka, Suita 565 Japan.
Rhegmatogenous retinal detachment (RRD) is another potential complication of BRVO that may result in visual IOSS,8-16 although it is less common than vitreous hemorrhage. Rhegmatogenous retinal detachment has been reported to occur in 2% to 3% of patients with BRVO.2.13
Two different types of retinal breaks have been described in these patients: retinal holes without vitreous traction8.9
27

Ophthalmology Volume 104, Number I, January 1997
and retinal tears with vitreous traction. lO•ll Retinal holes
are believed to be caused by cystic retinal changes,8 or chorioretinal occlusion.9 Retinal traction tears are believed to be caused by neovascularization and consequent contraction of the vitreous.lo,11
Clinical features of RRD after BRVO have been described by several investigators,12-16 and a few patients have been treated successful1y with vitrectomy and gas tamponade. 14,16 However, previous reports included small numbers of patients, and the majority of the reported cases were treatable with photocoagulation only. Thus, surgical results of vitrectomy for BRVO-related RRD remain uncertain.
We have reviewed our results of a series of 25 eyes that underwent vitrectomy for RRD after BRVO. We describe clinical characteristics and surgical results, and analyze the differences between these two types of retinal breaks (retinal holes without vitreous traction and retinal traction tears), comparing clinical features, final visual outcome, anatomic success, and complications after vitrectomy.
Patients and Methods
Patients
We reviewed the records of all eyes (25 eyes of 25 patients) that underwent primary vitrectomy for RRD caused by posterior retinal breaks in the tributary area of an occluded branch retinal vein at the Osaka National Hospital (Osaka, Japan) or the Surugadai Hospital of Nihon University (Tokyo, Japan) between July 1985 and December 1994. Vitrectomy was performed by four of the authors (YI, YT, TI, and YS), all of whom have extensive experience in vitreoretinal surgery. We included eyes both with and without vitreous hemorrhage preoperatively. There were 18 men and 7 women, ranging in age from 46 to 78 years (59.8 ± 7.9, mean ± standard deviation). The superior temporal vein was occluded in 16 eyes (64%), the inferior temporal vein in 8 eyes (32%), and a nasal vein in one eye (4%).
The indication for vitrectomy was a retinal detachment involving the macula, or a progressive extramacular retinal detachment, associated with a posterior retinal break within the area of retina drained by the obstructed vessel. A posterior break was defined as any break located within the vascular arcades, or no more than 2 disc diameters from the vascular arcades. In six eyes with severe vitreous hemorrhage obscuring the fundus, the diagnosis was made from ultrasonographic examination results. Patients with RRD resulting from an anterior retinal break after BRVO were treated with scleral buckling only and were not included in the study. Patients with diabetes or a history of vitrectomy or scleral buckling were also excluded.
Eyes were divided into two groups based on the type of retinal break, which was determined preoperatively by biomicroscopic examination at the slit lamp. In some eyes with severe preoperative vitreous hemorrhage, the type of break was determined intraoperatively after removal of the blood. Eyes with retinal holes, defined as round retinal breaks without vitreous traction on the detached
28
retina, were included in group I. Eyes with retinal tears, defined as slit-shaped or horseshoe retinal breaks associated with persistent vitreous traction on the detached retina, were included in group II. Twelve of 25 eyes (48%) had retinal holes, and 13 eyes (52%) had retinal tears. There were no eyes with both retinal holes and retinal tears.
Follow-up after final vitrectomy was at least 6 months and ranged from 6 to 72 months (29.6 ± 17.7, mean ± standard deviation). We recorded the following information: 1) preoperative characteristics, including best-corrected visual acuity and the status of the iris, lens, vitreous, and retina; 2) details of the operation, including the vitreoretinal relationship and the incidence of complications; 3) best-corrected visual acuity and anatomic status at the final examination; and 4) any postoperative complications.
Surgical Technique
A three-port vitrectomy system was used. A core vitrectomy was performed first, and any vitreous opacity was removed. If a preretinal neovascular membrane was present, it was segmented or delaminated with transvitreal scissors and forceps. When the vitreous gel was adherent to the retinal surface around the break, the posterior vitreous was separated gently from the inner retinal surface. After complete release of vitreous traction, pneumatic reattachment was performed with simultaneous aspiration of subretinal fluid via a small, blunt-tipped needle, followed by transvitreal photocoagulation to surround the retinal break and any iatrogenic retinal breaks. Then either perftuoropropane or sulfur hexafluoride was injected to provide postoperative gas tamponade. Avascular epiretinal membranes that appeared to affect visual function also were peeled from the retinal surface in three eyes in group I. An encircling band was placed in 13 eyes (group I, 6 eyes; group II, 7 eyes) to decrease traction of the anterior vitreous, and pars plana lensectomy was performed in 2 eyes (group I, 1 eye; group II, 1 eye) in which cataract obscured visualization of the fundus. Silicone oil tamponade was performed during reoperation in six group II eyes with recurrent retinal detachments.
Statistical Analysis
Mann-Whitney U test, chi-square test, and Fisher's exact test were performed to compare preoperative patient data, complications, and surgical results of patients with retinal holes and retinal tears.
Results
Preoperative Characteristics
Preoperative data for patients with retinal holes (group I) and retinal tears (group II) are summarized in Table 1. Preoperative visual acuity was reduced to worse than 20/ 200 in 16 of 25 eyes because of one or more of the following factors: macular detachment (17 eyes), vitreous

Ikuno et al . Retinal Vein Occlusion
Table l. Patient Data
Type of Retinal Break
Group I (retinal hole) Group II (retinal tear) Factor (n = 12) (n = 13) p
Age (yrs) Mean ± SD 57.3 ± 7.7 61.4 ± 8.1 NS* Range 46-71 49-78
Follow-up period (mas) Mean ± SD 26.4 ± 20.1 32.5 ± 15.4 NS* Range 6-72 10-70
No. (%) No. (%)
Sex Male 8 (67) 10 (77) Female 4 (33) 3 (23) NSt
Preoperative visual acuity VA ~ 20/200 4 (33) 5 (38) VA < 20/200 8 (67) 8 (62) NSt
Preoperative vitreous hemorrhage None or mild 10 (83) 9 (69) Severe 2 (17) 4 (31) NSt
Preoperative photocoagulation of the mid peripheral retina
Absent II (92) 9 (69) Present 1 (8) 4 (31) NSt
Preoperative status of the macula Detached 5 (42) 12 (92) Attached 7 (58) 1 (8) 0.01I2t+
Detachment area ~l quadrant 3 (25) 7 (54) < 1 quadrant 9 (75) 6 (46) NSt
No. of retinal breaks 1 7 (58) 9 (69) 2 4 (33) 2 (15) ~3 1 (8) 2 (15) NS§
Preretinal neovascular membrane Absent II (92) 5 (38) Present 1 (8) 8 (62) 0.01l2t+
Large retinal break (> I DD) Absent II (92) 8 (62) Present I (8) 5 (38) NSt
SD = standard deviation; V A = visual acuity; NS = not significant; DD = disc diameter.
* Based on Mann-Whitney U test.
t Based on Fisher's exact test.
* Significant.
§ Based on chi-square test.
opacity or hemorrhage (6 eyes), epiretinal membrane (3 eyes), and macular ischemia or edema resulting from vein occlusion (5 eyes). No significant differences in patient age, gender, preoperative visual acuity, preoperative vitreous hemorrhage, preoperative photocoagulation of the mid peripheral retina, rate of large retinal breaks (larger than 1 disc diameter), number of retinal breaks, retinal detachment area, or follow-up period were found between the two groups. Group II eyes were found to have a higher rate of neovascular membranes (P = 0.0112) and preoperative macular detachment (P = 0.0112).
Complications
Intraoperative and postoperative complications are shown in Table 2. Intraoperative complications included iatrogenic retinal break in 7 of the 25 eyes (28%) and severe preretinal bleeding in 1 eye (4%). Postoperative complications that required further vitrectomy included recurrent retinal detachment in eight eyes (32%) and recurrent vitreous hemorrhage in two eyes (8%). One eye had recurrent vitreous hemorrhage and recurrent retinal detachment simultaneously. The cause of recurrent retinal detachment
29

Ophthalmology Volume 104, Number 1, January 1997
Table 2. Complications
Total (n = 25)
Complication
Intraoperative Iatrogenic retinal break Severe bleeding
Postoperative Recurrent retinal detachment Proliferative vitreoretinopathy:j: Recurrent vitreous hemorrhage Cataract formation or progression Epimacular membrane formation Corneal opacification Open-angle glaucoma
NS = not significant.
* Based on Fisher's exact test.
t Significant.
:j: Grade C or D.
No.
7 1
8 6 2 2 2 2 1
§ Six of eight eyes with recurrent retinal detachment had PVR.
II Both eyes had undergone silicone oil tamponade.
(%)
(28) (4)
(32) (24)§ (8) (8) (8) (8)11 (4)
was reopening of pre-existing retinal breaks in two eyes (25%) and proliferative vitreoretinopathy in six eyes (75%). The interval from initial surgery to repeat vitrectomy for recurrent retinal detachment ranged from 0.7 to 3 months (1.5 ± 0.6 months, mean ± standard deviation). Other postoperative complications were cataract formation in two eyes (8%), epimacular membrane formation in two eyes (8%), corneal opacification in two eyes (8%), and open angle glaucoma in one eye (4%). Both eyes in which corneal opacification developed had undergone silicone oil tamponade for recurrent detachment.
Recurrent retinal detachment occurred in 1 of 12 group I eyes (8%), and 7 of 13 group II eyes (54%, P = 0.0302). The rate of postoperative proliferative vitreoretinopathy was higher in group II eyes (P = 0.0149). Intraoperative iatrogenic retinal breaks also were more common in group II eyes (46% versus 8%), but this difference did not reach statistical significance because of the small number of eyes involved (P = 0.0730). No differences were found between the two groups regarding such complications as severe bleeding, recurrent vitreous hemorrhage, cataract fonnation or progression, epimacular membrane fonnation, corneal opacification, or open-angle glaucoma.
Final Outcome
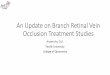
Figure 1 shows the best-corrected preoperative and final visual acuity. Of the 25 study eyes, 8 (32%) attained final visual acuity of 20/40 or better and 20 eyes (80%) had final visual acuity of 20/200 or better. Five eyes (20%) had a final visual acuity of 20/400 or worse and four eyes (16%) had final visual acuity of 21200 or worse. Visual acuity improved by two or more lines in 18 eyes (72%),
30
Type of Retinal Break
Group I (retinal Group II (retinal hole) (n = 12) tear) (n = 13)
No. (%) No. (%) p*
1 (8) 6 (46) 0.0730 0 (0) 1 (8) NS
1 (8) 7 (54) 0.0302t 0 (0) 6 (46) 0.0149t 0 (0) 2 (15) NS 2 (17) 0 (0) NS 2 (17) 0 (0) NS 0 (0) 2 (15) NS 1 (8) 0 (0) NS
worsened by two or more lines in three eyes (12%), and remained unchanged in four eyes (16%) postoperatively.
Anatomic success and visual acuity at final examination for the two groups are compared in Table 3. The final anatomic success rate was 100% for group I eyes and 77% for group II eyes. This difference did not reach statistical significance. The final retinal status in three group II eyes that did not attain total retinal reattachment was combined rhegmatogenous and tractional total retinal detachment in two of three eyes (67%) and partial traction detachment involving the macula in one eye (33%), de-
?;> ·s al ] .;;:
~ it
20120
20/200
21200 -
CF
HM
LP • •
• o Group I
• GroupII
NLP~---.--~ __ ---.---.----~---.----NLP LP HM CF 21200 20/200 20/20
Preoperative visual acuity
Figure 1. The preoperative and final visual acuity for each of the 25 eyes. CF = counting fingers; HM = hand motions; LP = light perception; NLP = no light perception.

Ikuno et al . Retinal Vein Occlusion
Table 3. Anatomic Success Rate and Final Visual Acuities
Type of Retinal Break
Group I (retinal hole) (n = 12)
Group II (retinal tear) (n = 13)
Factor No.
Final status of the retina Totally reattached 12 Partially reattached or detached a
Final visual acuity VA 2: 20/200 12 VA < 20/200 a
VA = visual acuity; NS = not significant.
* Based on Fisher's exact test.
t Significant.
spite repeat vitreous surgery in all three eyes. At the final examination, all 12 group I eyes (100%) achieved a visual acuity of better than 201200, and 8 of 13 group II eyes (62%) had a visual acuity of better than 20/200 (P =
0.0391). The cause for a final visual acuity of 201200 or worse was persistent macular detachment in three eyes (60%) and chronic macular degenerative change in two eyes (40%).
Discussion
We have demonstrated our surgical results for a series of patients receiving vitrectomy for RRD after BRVO. In this study, 22 of 25 eyes (88%) attained total retinal reattachment and 20 eyes (80%) achieved visual acuity better than 201200 at final examination. Our visual results are comparable to the natural history of the disease in patients not developing retinal detachment. Approximately 80% of patients with BRVO without RRD were reported to achieve a visual acuity of better than 201200 after at least I year of follow-up.I,2 Our results are somewhat better than those for other retinal vascular disorders complicated by RRD, For example, Rice and associates l7 reported that of 107 eyes that underwent vitrectomy for rhegmatogenous diabetic retinal detachment, 64% attained macular reattachment and 36% achieved a visual acuity of 201200 or better.
Some authors have successfully treated RRD after BRVO with scleral buckling,8,l3-15 and we believe that scleral buckling may be preferred over vitrectomy in selected cases, The disadvantages of scleral buckling for posterior retinal breaks is the need to deform the posterior pole and the technical difficulty of placing a buckle beneath a posterior retinal break. However, one of the disadvantages of vitrectomy is the risk of an intraoperative iatrogenic retinal tear, Therefore, if retinal breaks are located anteriorly, scleral buckling should be considered.
Postoperative proliferative vitreoretinopathy appears to be more common in eyes with RRD after BRVO than in
(%) No. (%) p*
(loa) 10 (77) (0) 3 (23) NS
(loa) 8 (62) (0) 5 (38) O.0391t
those with conventional RRD, Proliferative vitreoretinopathy developed in six of eight eyes (75%) in our series that failed primary vitrectomy, A recent study revealed that breakdown of the blood-retinal barrier occurs in patients with BRVO,18 and retinal neovascularization has been shown to cause breakdown ofthe blood-retinal barrier in rabbits,19 Breakdown of the blood-retinal barrier is suggested to be an important initiating event in proliferative vitreoretinopathy,20 Thus, RRD after BRVO is likely to lead to proliferative vitreoretinopathy if initial surgery fails,
We found that the two types of retinal breaks that can precipitate RRD after BRVO have a different prognosis, Significantly more eyes with retinal tears than eyes with retinal holes had a final visual acuity of 201200 or worse (P = 0,0391), Two major factors are believed to explain this difference, One is macular damage caused by preoperative macular detachment. The rate of preoperative macular detachment was higher in patients with retinal tears than in those with retinal holes (P = 0.0112). It is known that retinal detachment caused by a tractional retinal tear is rapidly progressive, which may increase the risk of macular involvement. In patients with BRVO, macular involvement by the vasoocclusive process in the acute phase, subretinal macular scarring, or macular cystoid changes also can influence macular function,I,2 but these changes would be expected to affect both groups of patients, In eyes in which the macula had already detached, we were unable to precisely evaluate the preoperative status of the macula with fluorescein angiography.
The other factor associated with a poor visual outcome was a higher rate of recurrent retinal detachment in patients with retinal tears (P = 0,0302). Patients with retinal tears had a higher incidence of preretinal neovascular membranes (P = 0.0112). The greater degree of vitreoretinal adhesion present in these patients mandates more extensive surgical dissection. Histological study revealed inner retinal atrophy in patients with BRVO,21 Atrophic weakening of the neural retina increases the risk of an iatrogenic retinal break during separation of neovascular
31

Ophthalmology Volume 104, Number 1, January 1997
membranes or vitreous cortex from the retina, consequently worsening the prognosis for complete retinal reattachment. In contrast, eyes with retinal holes rarely had neovascular membranes and often the posterior vitreous had detached from the inner retinal surface around the retinal break. The low rate of iatrogenic retinal breaks (8%) in eyes with retinal holes compared with eyes with retinal tears (46%) supports this hypothesis.
Current opinion is that in cases of RRD after BRVO, there is minimal vitreoretinal adhesion. 16 This hypothesis is supported by a significant increase in the incidence of partial posterior detachment in patients with BRVO compared with controls.22 However, many eyes with traction retinal tears in this study showed extensive vitreoretinal adhesion, which is reflected in the fact that the rate of iatrogenic retinal breaks occurring in patients with traction retinal tears (46%) was at the same level as in eyes undergoing vitrectomy for diabetic RRD (55%).17 The reason for extensive vitreoretinal adhesion in our cases is not clear. Preoperative photocoagulation treatment is believed to be one factor that contributes to this status because histopathologic study has revealed that photocoagulation induces vitreoretinal adhesion at the site of coagulation in the dog eye.23 However, in the study by Russell et al,16 none of the four patients who had BRVOrelated retinal traction tears and consequent RRD had received laser treatment to midperipheral retina preoperatively. Photocoagulation does not explain the vitreoretinal adhesion seen in this study either because only 5 of the 25 eyes (20%) had received photocoagulation therapy preoperatively. We believe that some other factors contribute to this condition, which appears to have a strong influence on final visual outcome. Future investigation may further reveal the characteristics of the vitreoretinal relationship in patients with RRD after BRVO.
References
1. Michels RG, Gass JDM. The natural course of retinal vein obstruction. Trans Am Acad Ophthalmol Otolaryngol 1974;78:166-77.
2. Gutman FA, Zegarra H. The natural course of temporal retinal branch vein occlusion. Trans Am Acad Ophthalmol Otolaryngol1974;78:178-92.
3. Schatz H, Yannuzzi L, Stransky TJ. Retinal detachment secondary to branch vein occlusion: part I. Ann Ophtha1mol 1976;8:1437-52.
4. Schatz H, Yannuzzi L, Stransky TJ. Retinal detachment secondary to branch vein occlusion: part II. Ann Ophthalmol 1976;8:1461-71.
32
5. Murakami K, Ho PC, Trempe CL, Pruett Re. Tractional detachment of the macula following branch retinal vein occlusion. Ann Ophthalmol 1983; 15:760-5.
6. Branch Vein Occlusion Study Group. Argon laser photocoagulation for prevention of neovascularization and vitreous hemorrhage in branch vein occlusion: a randomized clinical trial. Arch Ophthalmol 1986; 104:34-41.
7. Smiddy WE, Isemhagen RD, Michels RG, et al. Vitrectomy for nondiabetic vitreous hemorrhage: retinal and choroidal vascular disorders. Retina 1988;8:88-95.
8. Zauberman H. Retinopathy of retinal detachment after major vascular occlusions. Br J Ophthalmol1968;52:117-21.
9. Regenbogen L, Godel V, Feiler-Ofry V, et al. Retinal breaks secondary to vascular accidents. Am J Ophthalmol 1977; 84: 187 -96.
10. Joondeph HC, Goldberg MF. Rhegmatogenous retinal detachment after tributary retinal vein occlusion. Am J Ophthalmol 1975; 80:253-7.
11. Joondeph HC, Joondeph Be. Posterior tractional retinal breaks complicating branch retinal vein occlusion. Retina 1988; 8: 136-40.
12. Ramos-Umpierre A, Berrocal JA. Retinal detachment following branch vein occlusion: case report. Ann Ophthalmol 1977; 9:339-40.
13. Gutman FA, Zegarra H. Retinal detachment secondary to retinal branch vein occlusions. Trans Am Acad Ophthalmol OtolaryngoI1976;81:491-6.
14. Cohen G. Rhegmatogenous retinal detachment secondary to branch retinal vein occlusion: a case report. Retina 1981;1:186-9.
15. Chess J, Eichen AL. Rhegmatogenous retinal detachment associated with branch vein occlusion. Ann Ophthalmol 1989;21:309-11.
16. Russell SR, Blodi CF, Folk Je. Vitrectomy for complicated retinal detachments secondary to branch retinal vein occlusions. Am J Ophthalmol 1989; 108:6-9.
17. Rice TA, Michels RG, Rice EF. Vitrectomy for diabetic rhegmatogenous retinal detachment. Am J Ophthalmol 1983; 95:34-44.
18. MiyakeK, Miyake T, Kayazawa F. Blood-aqueous barrier in eyes with retinal vein occlusion. Ophthalmology 1992; 99:906-10.
19. de Juan E Jr, Wilson D, Hatchell D. Breakdown of the blood-retinal barrier in a model of retinal neovascularization. Invest Ophthalmol Vis Sci 1987;28:1108-15.
20. Campochiaro PA, Bryan JA III, Conway BP, Jaccoma EH. Intravitreal chemotactic and mitogenic activity: Implication of blood-retinal barrier break down. Arch Ophthalmol 1986; 104: 1685-7.
21. Frangieh GT, Green WR, Barraquer-Somers E, Finkelstein D. Histopathologic study of nine branch retinal vein occlusions. Arch Ophthalmol 1982; 100: 1132-40.
22. Trempe CL, Takahashi M, Topilow HW. Vitreous changes in retinal branch vein occlusion. Ophthalmology 1981; 88:681-7.
23. Okun E, Collins EM. Histopathology of experimental photocoagulation in the dog eye. Am J Ophthalmol1962;54:3-16.