Embed Size (px)
Citation preview

Review ArticleLoop Myopexy Surgery for Strabismus Associated withHigh Myopia
Yun Su, Qin Shen, and Xianqun Fan
Department of Ophthalmology, Shanghai Ninth People’s Hospital, Shanghai Jiao Tong University, School of Medicine,Shanghai 200011, China
Correspondence should be addressed to Qin Shen; [email protected] and Xianqun Fan; [email protected]
Received 4 February 2016; Accepted 13 April 2016
Academic Editor: Marcel N. Menke
Copyright © 2016 Yun Su et al. This is an open access article distributed under the Creative Commons Attribution License, whichpermits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Strabismus associated with high myopia is a rare abnormality of ocular motility, leading to the impairment of abduction andsupraduction. Loop myopexy of the superior rectus (SR) and lateral rectus (LR) muscles is now the most preferred surgery forrestoring the dislocated eye globe back into the muscle cone. Various procedural modifications have been made based on thisconcept, and satisfactory outcomes have been reached in most cases. In this paper, we review various surgical modificationspublished in the literature that are based on the loop myopexy surgery in patients with high myopic strabismus and summarize theapplicable scope of different surgical procedures for patients with different degrees of strabismus. Three major surgical proceduresare identified and different modifications have been applied based on their concept. Most of these modifications have been provento be safe and effective and result in good ocular alignments. The selection of such modifications is of great importance in differentpatients. Careful evaluation before surgery should bemade not only tomake the correct diagnosis but also to choose an appropriatesurgical procedure and offer individualized modifications in the surgery.
1. Introduction
Strabismus associated with highmyopia is a rare abnormalityof ocular motility characterized by the presence of esotropiaand hypotropia, with restricted abduction and supraduction[1]. In later stages, the affected eye progresses into an extremeesotropic and hypotropic position and the ocular motilityis seriously limited, a condition called “myopic strabismusfixus” [2, 3].
With the evolving understanding of the pathogenesis,consensus has now been reached that strabismus with highmyopia is usually the consequence of the supertemporalprotrusion of the elongated eye globe through the musclecone, leading to an inferior displacement of the lateralrectus muscle and nasal displacement of the superior rectusmuscle [3, 4]. In addition, Rutar and Demer [5] found thatdegeneration in orbital connective tissues, usually the bandbridging the lateral and superior rectus muscles, also enablesa supertemporal shift of the globe through the weak ligament.
Based on the updated pathogenetic mechanism, the tra-ditional recession-resection surgery, which aimed at altering
the forces of the muscles, is no longer popular due to itslimited effects, especially in some severe cases [1, 3]. Manysurgical procedures aim at correcting the muscle paths ofboth the superior and lateral rectus muscles. Loop myopexyof the superior rectus (SR) and lateral rectus (LR) muscles isnow the most preferred surgery for restoring the dislocatedglobe back into the muscle cone [6]. Various modificationshave been made based on this surgical approach, and satis-factory outcomes have been reached in most cases [7–24].
In this paper, we review the various surgical managementtechniques published in the literature that are based onthe procedure of loop myopexy for treating patients withstrabismus associated with high myopia. We also summarizethe applicable scope of surgical procedures for patients withdifferent degrees of strabismus.
2. Advantages of Loop Myopexy Surgery
2.1. Traditional Surgical Management Techniques. Recession-resection surgeries have been traditionally applied to alter theforces of the muscles. Hayashi et al. [1] and Louis et al. [25]
Hindawi Publishing CorporationJournal of OphthalmologyVolume 2016, Article ID 8657036, 7 pageshttp://dx.doi.org/10.1155/2016/8657036

2 Journal of Ophthalmology
performed recession of the medial rectus (MR) muscle andresection of the LR in patients in the early stage of strabismusand obtained good results. However, the correction was notenough for more severe cases. Krzizok et al. [3] claimedthat the recession-resection procedure might aggravate thedeviation because the dislocation of the LR anatomicallywould reduce its abducting force and create depressing forces.They advocated that the most important objective of surgicalmanagement is to normalize the pathological path of theLR instead of reinforcing its forces. They proposed a newsurgical technique that dislocated the LR to the physiologicalmeridian at the equator with a nonabsorbable suture orsilicon loop, combined with a large recession of the MR andLR. However, their procedure was technically difficult andhad a high risk of globe perforation due to the thin sclera inhigh myopia [26].
2.2. Loop Myopexy Surgery. In the past, most attention hasbeen paid to the management of the horizontal musclesbecause some researchers claimed that it was the dislocationof only the LR by the elongated eyeball that caused thecorresponding strabismus [1, 3]. However, this concept wasupdated by Yokoyama’s study [6]. After an evaluation of theanatomic relationships between the muscle cone and globeon magnetic resonance imaging (MRI), they found that theposterior portion of the elongated globe was dislocated fromthe muscle cone supertemporally, leading to an inferior shiftof the LR and nasal shift of the SR. Later, these findingswere further confirmed by Aoki et al. [4] by investigating theextraocular muscle path shift and prolapse of the posterioreyeball from themuscle cone.They also agreed that it was theposterior portion of the globe that stretched and shifted bothof the muscles.
Based on this hypothesis, Yokoyama et al. proposed a loopmyopexy surgery of the muscle bellies of the SR and LR torestore the dislocated globe back into the muscle cone [6].This surgery united these two muscles and reestablished thephysiological muscle plane, thus preventing the globe fromprolapsing through the supertemporal quadrant [6, 17, 20].Various modifications have been suggested on the basis ofuniting these two muscles. Most patients had satisfactoryresults with good ocular alignment.
Yamada’s procedure, a hemitransposition of the SR andLR, cannot be strictly included as a loop myopexy surgerybecause it merely secures the muscle bellies to the sclerawithout actual union of these two muscles [17]. However,its concept was similar to that of a loop myopexy surgeryin that it tried to change the position of the SR and LRand reconstruct the normal anatomic relation of the muscles.Moreover, the application of Yamada’s procedure and itsmodifications showed good postoperative results in patientswith strabismus fixus [17–19]. Therefore, in this review, wealso included it as a special type of loop myopexy surgery.
3. Procedures of Loop Myopexy Surgery
All studies regarding loop myopexy in high myopic strabis-mus in the literature were reviewed and the main surgicalprocedures were determined. Eighteen studies of strabismus
associated with high myopia treated with the procedure ofloop myopexy were eligible for our review. The clinical char-acteristics, surgical management, and outcomes of eighty-nine patients, with ages ranging from 5 to 78 years, aredescribed in Table 1.
Three main surgical management techniques were foundin the literature, namely, Yokoyama’s procedure, Yamada’sprocedure, and the partial Jensen’s procedure. Other studiesfound in the literature were performed based on these threeprocedures, with modifications in various details of thesurgery, such as being with or without medial rectus (MR)muscle recession, scleral fixation, or the use of materials formuscle union. All three surgical procedures were based onthe concept of pathogenesis described by Yokoyama et al. [6].
3.1. Yokoyama’s Procedure. Yokoyama’s procedure, first per-formed in 2000, has drawn wide attention because of itssatisfactory postoperative ocular alignment and the con-cept that there is no abnormality of the muscle forces butabnormality of the muscle paths [6, 10, 26]. In his study, sixpatients with high myopic strabismus were treated with a fullloop myopexy of the SR and LR muscle belly 15mm behindthe insertions using a polyester suture. Postoperatively, theyachieved great improvement in ocular motility and reducedherniation of the globe, as confirmed by MRI [10]. Later, innine studies, a total of 48 patients were treated using thisfull loop myopexy technique with modifications of variousdegrees [7–16].
3.2. Yamada’s Procedure. In 2002, Yamada et al. [17] per-formed a hemitransposition of the SR and LR, combinedwith a large recession of the MR in a patient with bilateralconvergent strabismus fixus. They divided the SR and LRin half 15mm from the insertion, secured the temporal halfof the SR and the superior half of the LR to the sclerabetween the SR and LR at 7mm posterior from the limbus,and performed a recession of the MR by 8mm. Based onthis procedure, Sturm et al. [18] tied the translocated musclehalves together and secured them to the supertemporal scleraat 15mm from the new insertion. Godeiro et al. [19] appliedthe hemitransposition technique, together withMR recessionor Botox injection.
3.3. Partial Jensen’s Procedure. The partial Jensen’s procedurewas first performed by Larsen and Gole in 2004 [20]. Theysplit the SR and LRmuscles in half, from the insertion to pastthe equator, and apposed only the adjacent halves of the LRand SR muscles. After surgery, patients achieved significantimprovement in ocular motility and good cosmetic results. Atotal of 15 patients with high myopic strabismus in four otherstudies received similar surgical treatment [21–24].
4. Modifications of Loop Myopexy Surgery
In other studies, various modifications have been performedbased on the three surgical procedures mentioned above(i.e., Yokoyama’s, Yamada’s, and partial Jensen’s). To eliminatethe risk of scleral perforation, some authors preferred not

Journal of Ophthalmology 3
Table1:Summaryon
literatures
abou
tsurgicaltreatmento
fhighmyopics
trabism
us.
Procedures
Authors
Num
bero
fcases
Preoperativ
estrabism
usSurgicalmanagem
ent
Patie
nts’ou
tcom
eFo
llow-up
(mon
ths)
Yokoyama’s
procedure
Won
getal.,2005
[7]
2
Case1:70Δesotropiaa
nd25Δ
hypo
tropiaw
ithlim
itedocular
movem
ent
Case2:fix
edeyep
osition
inaddu
ctionanddepressio
n
Union
oftheS
RandLR
12mm
behind
thelim
bus
Case1:with
a5-0
Mersilksuture
Case2:with
a240
band
andsilicon
sleeve
Case1:10Δesotropiaw
ithmild
limitatio
nin
abdu
ction
Case2:14Δexotropia,lim
itatio
nin
abdu
ction(−1)in
ther
ight
eye,addu
ction(−2)
intheleft
eye,and
elevation(−1)in
both
eyes
Case1:15
Case2:14
Rowea
ndNoo
nan,
2006
[8]
170Δesotropiaa
nd25Δhypo
tropia
Union
ofthetem
poralh
alfo
fSRandtheu
pper
half
ofLR
,placedpo
sterio
rtothee
quator
by5-0
polybu
tilate-coated
polyestersuture;recessionof
the
MRfor6
mm
20Δhypo
tropia,mild
limitatio
nof
elevationand
abdu
ction
12
Basm
aketal.,2008
[9]
1Fixedeyep
osition
andrestr
icted
ocular
motility
Union
oftheS
RandLR
15mm
behind
their
insertions
with
anon
absorbablepo
lyestersuture;
recessionof
theM
R12mm
from
thelim
bus
Resto
ratio
nof
thed
islocated
eyeballand
improvem
ento
focularm
otility,but
mild
restr
ictio
nin
allgazed
irections
24
Yamaguchi
etal.,2010
[10]
21Ang
leso
fdeviatio
n58.8±36.0∘
Union
oftheS
RandLR
15mm
behind
theinsertio
nswith
apolyeste
rsuture;recessionof
theM
Rfor5
to8m
m
Ang
leso
fdeviatio
nof
0.7±9.0∘degrees,great
improvem
entinabdu
ctionandsursum
duction
48.8
Durnian
etal.,2010
[11]
513Δesotropiaa
nd21.8Δhypo
tropia
Union
ofhalfof
theS
RandLR
14mm
behind
their
insertions
with
5-0no
nabsorbables
uture
Hypotropiad
eviatio
nof
0Δandverticaldeviationof
4.4Δ
6
Shih
etal.,2012
[12]
1Severe
limitatio
nof
ductions
inall
directions
Union
oftheS
RandLR
5to
7mm
poste
riortotheir
insertions
with
apolytetraflu
oroethylene(
Gore-Tex)
Slingand5-0po
lyestersuture;recessionof
theM
Rfor8
mm
andLR
for6
mm
12Δesotropiaw
ithlim
itatio
nin
supraductio
n(−3)
7
Akbarietal.,2013
[13]
1Fixedeyep
osition
inaddu
ctionand
infraductio
nUnion
oftheS
RandLR
with
apolyeste
rsuture;
recessionof
theM
Randresectionof
LRBino
cularly
aligned
12
Akare
tal.,2014
[14]
2058.6±2.5Δ
esotropiaa
nd12.5±
1.3Δhypo
tropia
Union
ofthelateralon
e-qu
artero
fthe
SRandthe
superio
rone-quarter
oftheL
R14
to15mm
poste
rior
totheinsertio
nswith
adou
ble-armed
5-0
polybu
tilate-coated
polyestersuture;recessionof
the
MRfor8
to10mm
6.8±1.4Δesotropia,3.3±1.1Δhypo
tropia,and
significantimprovem
entinabdu
ctionand
supraductio
n48
Acar
andAltintas,2015
[15]
2Ca
se1:65Δesotropia
Case2:85Δesotropia
Union
oftheS
RandLR
with
a5-0
nonabsorbable
polyestersuture;recessionof
theM
Rfor5
.75m
m
Case1:16Δatnear
anddista
nce
Case2:12Δatnear
and14Δatdista
nce,mild
limitatio
nin
abdu
ction(−1)
Case1:36
Case2:25
Shenoy
etal.,2015
[16]
1579.3±32.3Δesotropiaa
nd8.9±
10.1Δ
hypo
tropia
Union
oftheS
RandLR
14to
16mm
from
thelim
bus
throug
ha3
to4leng
thscleraltun
nelw
ith240
silicon
ebandand5-0no
nabsorbablep
olyeste
rsuture;
recessionof
theM
Rfor5
to7.5
mm
16.9±17.4Δ
esotropia,0.6±1.3Δhypo
tropia,and
successrate(
deviation≤20Δ)7
3%7.9±8.5

4 Journal of Ophthalmology
Table1:Con
tinued.
Procedures
Authors
Num
bero
fcases
Preoperativ
estrabism
usSurgicalmanagem
ent
Patie
nts’ou
tcom
eFo
llow-up
(mon
ths)
Yamada’s
procedure
Yamadae
tal.,2002
[17]
1Fixedeyep
osition
inextre
me
addu
ctionandrestr
ictedocular
motility
Hem
itransposition
oftheS
RandLR
with
scleral
fixation7m
mfro
mthelim
bus;recessionof
theM
Rfor8
mm
10Δesotropiaw
ithmild
limitatio
nin
supraductio
nandabdu
ction
12
Sturm
etal.,2008
[18]
1Fixedeyep
osition
inextre
me
addu
ctionanddepressio
n
Hem
itransposition
oftheS
RandLR
with
anew
insertionat7m
mpo
sterio
rfrom
thelim
busa
ndmyopexy
oftranslo
catedmuscle
swith
scleralfi
xatio
nat15mm
from
then
ewinsertion;
recessionof
MRfor
10mm
20∘esotropiaw
ithslightly
limitedocular
motilityin
abdu
ction,
elevation,
andaddu
ction
12
God
eiro
etal.,2009
[19]
2
Case1:50Δesotropiaa
nd12Δ
hypo
tropia
Case2:60Δesotropiaa
nd10Δ
hypo
tropia
4mm
resectionandhemitransposition
oftheS
Rand
LRwith
scleralfi
xatio
nat7m
mfro
mthelim
busb
y6-0mersilene
Case1:5IUbo
tulin
umtoxininjectioninto
theM
R;then
recessionof
theM
Rfor6
mm
Case2:recessionof
theM
Rfor6
mm
Case1:satisfactoryalignm
entw
ithmild
limitatio
nin
abdu
ctionandelevationat8mon
ths
Case2:excellent
ocular
alignm
entw
itham
arked
improvem
entinabdu
ctionandele
vatio
n
Case1:8
Case2:6
PartialJensen’s
procedure
Larsen
andGole,2004
[20]
150Δesotropiaa
nd30Δhypo
tropia
Union
ofthelateralhalfof
theS
Randthes
uperior
halfof
theL
R14mm
from
thelim
busw
ith5-0
Dacronsuture
Sign
ificant
improvem
entinabdu
ctionand
supraductio
n9
Ahadzadeghanetal.,2009
[21]
6≫90Δ
esotropiaa
nd25
to30Δ
hypo
tropia
Union
ofthelateralhalfof
theS
Randthes
uperior
halfof
theL
R16mm
from
thelim
busw
ith5-0
Dacronsuture;recessio
nof
theM
Rfor6
to10mm
5to
20Δesotropiaa
ndmild
limitatio
nin
abdu
ction
andele
vatio
n2
Rajavietal.,2009
[22]
2
Case1:40Δesotropiaa
nd5Δ
hypo
tropia
Case2:50Δesotropiaa
nd2Δ
hypo
tropia
Union
ofthelateralhalfof
theS
Randthes
uperior
halfof
theL
Rpo
sterio
rtothee
quator
with
a5-0
nonabsorbablep
olybutilate-coatedpo
lyestersuture
Case1:10
to12Δesotropiaa
nd3Δ
hypo
tropia,slightly
restr
ictedabdu
ction(−1)
Case2:25Δforfar
and20Δforn
eare
sotro
piaa
nd2Δ
hypo
tropia,mild
restr
ictio
n(−1)in
abdu
ction
Case1:3
Case2:2
Kang
etal.,2011[23]
582.86±37.62Δ
esotropiaa
nd20±
7.91Δ
hypo
tropia
Union
ofthelateralhalfof
theS
Randthes
uperior
halfof
theL
R12
to14mm
from
theinsertio
nswith
a5-0no
nabsorbablep
olyeste
rsuture;recessionof
the
MRfor6
to10mm
Sign
ificant
improvem
entindislo
catio
nof
theg
lobe,
ocular
motility,and
horiz
ontaland
verticaldeviations
5
Hoetal.,2012
[24]
2>90Δesotropiaa
ndmarked
limitatio
non
abdu
ction(−3)
Union
ofthelateralhalfof
theS
Randthes
uperior
halfof
theL
R14mm
from
thelim
busw
itha5
-0Dacronno
nabsorbables
uture;recessionof
theM
Rfor8
to8.5m
m
Case1:greatimprovem
entinocular
motilityand
alignm
entw
ith10Δesotropia
Case2:im
proved
motilitywith
4Δesotropia
Case1:no
tmentio
ned
Case2:10

Journal of Ophthalmology 5
to suture the muscle bellies onto the globe [7–15, 20–24].In some studies, a hang-back technique that did not touchthe sclera was also preferred in the MR recession [18, 24].To minimize the possibility of anterior segment ischemia,some authors advocated a union of parts of the muscle bellybecause the unsecured parts of the SR and LRmuscles wouldcontribute to the circulation of the anterior segment [20–22]. Moreover, given the potential complications of musclecheese-wiring and the disadvantage of the irreversibility ofsuture loop myopexy, different materials, mainly siliconebands, have been applied in the surgery [7, 12, 16]. Shenoy etal. [16] performed a novel modification of loopmyopexy witha silicone band in 15 patients with high myopic strabismus.They believed that there was an increased risk of migration ofthe silicone band, especially in eyes with great axial length, sothey advocated the scleral fixation of the band.This techniquewas proven to be effective and can improve alignmentsignificantly. However, two patients in that study presentedwith complications of foreign body sensation, which requiredremoval of the silicone band.
5. Selection of Surgical Procedure
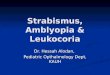
5.1. Selection of a Surgical Procedure Based on Degrees ofStrabismus. The selection of a surgical procedure is basedmainly on the surgeon’s preference and proficiency in acertain technique. All three procedures discussed above havebeen proven to be effective in the treatment of high myopicstrabismus. However, there exist some differences in theapplicable scope of each procedure, which is a considerationthat might be beneficial when planning a surgery. Shenoy etal. found that full loop myopexy of the SR and LR alone cancorrect up to 40Δ of esotropia [16]. After a thorough reviewof the application of Yokoyama-based procedures (i.e., fullloop myopexy), we found it to be more effective in patientswith esotropia of 12 to 85Δ when combined with recessionof the MR muscle [10, 15]. Furthermore, the partial Jensen’sprocedure combined with MR recession has a wider range ofapplication; patients with large esotropia, usually over 90Δ,also have satisfactory outcomes after surgery [21, 24]. Becausethe data in studies related to Yamada’s procedure and thesimple partial Jensen’s procedurewere limited, we are not ableto summarize the applicable scope of these two procedures.Based on the existing findings, we created a diagram forthe applicable scopes of different surgical procedures for thetreatment of high myopic strabismus (Figure 1). However,these scopes were derived mainly from the summary ofour literature review. Further studies of more patients arewarranted to verify the accuracy of these applicable scopes.
5.2. Application of Surgical Procedures to Fixed Eye Position.Myopic strabismus fixus is an extreme condition in whichthe affected eye is fixed inferomedially with restricted ocularmotility. The elongated globe is dislocated from the musclecone, and the posterior portion of the globe is blocked bythe SR and LR, thus leading to restriction in abduction andsursumduction. The main purpose of surgery is to eliminatethe mechanical limitation in ocular motility.
Partial Jensen’s procedure + recession of MR
Yokoyama’s procedure + recession of MR
Yokoyama’s procedure
12011090807060504030200 10 100
(Δ)
Figure 1: Applicable scopes of different surgical procedures for thetreatment of high myopic strabismus. Yokoyama’s procedure alonecan correct up to 40Δ of esotropia. A combination of Yokoyama’sprocedure and recession of the MR muscle is effective in patientswith 12 to 85Δ of esotropia.The partial Jensen’s procedure combinedwith recession of theMRmuscle is able to correct esotropia over 30Δ.
Hayashi et al. classified patients with high myopic stra-bismus into four groups, and the surgical management ofpatients who presented with fixed eye in the extreme positionwas considered a great challenge [1]. Basmak et al. performedYokoyama’s procedure together with recession of the MR in a55-year-old female patient with both eyes fixed in the extremeesotropic and hypotropic position [9]. Postoperatively, goodoutcomes were achieved despite mild restriction in all direc-tions. Yamada’s hemitransposition procedure combined withthe MR recession was performed in a 69-year-old patientwith fixed eye positions and limited ocular motility in botheyes [17]. One year after surgery, the patient’s motility greatlyimproved, although there was mild impairment of abductionand elevation. Ho et al. treated two cases (one bilateral andone unilateral) of severe high myopic strabismus fixus by thepartial Jensen’s procedure combined with MR recession [24].Good ocular alignments were achieved after surgery with lessthan 10Δ esotropia in individual cases.Thus, all three surgicalprocedures mentioned above (i.e., Yokoyama’s, Yamada’s, andpartial Jensen’s) have been proven to be effective in thetreatment of myopic strabismus fixus.
5.3. Role of the Additional MR Recession. The MR recessionis not necessary in all patients. If forced duction test confirmstight muscle or if restricted abduction exists for several years,contracture of the MR muscle is likely to have occurred [27].In these cases, the MR recession is recommended togetherwith the union of the LR and SR [10, 14]. In the study of Akaret al. [14], they performed the MR recession at the same timeas muscle union in 24 eyes of 13 patients whose preoperativeforced duction tests were positive, and all of them hadsignificant improvement in abduction and supraduction.However, if there is no evidence of MR contracture beforesurgery, the MR recession can be applied in a second surgerywhen the union of LR and SR is not sufficient to correctthe abnormal muscle paths. Yamaguchi et al. [10] applied thesame surgical strategy for theMR recession, and four patientsin their study presented without evidence of MR contractureand were successfully cured by only uniting the LR and SRmuscles.
5.4. Surgery of Bilateral High Myopic Strabismus. In patientswith strabismus associated with highmyopia in both eyes, we

6 Journal of Ophthalmology
recommend that bilateral strabismus surgeries be performedsimultaneously to correct the muscle paths, not only toeliminate the disparity between the two eyes but also toavoid the potential risk of having the patient undergo asecond general anesthesia, especially in the elderly. In thosesevere cases, large MR recession is usually needed becausesome residual esotropia will remain after union of the SRand LR bellies. The MR recession will be helpful to furthercorrect the eye position. Morad et al. held a similar opinionthat bilateral myopexy of the SR and LR is the preferredmethod, after comparing the surgical results of patients withhigh myopic strabismus unilaterally and bilaterally [28]. Ifa unilateral myopexy surgery is selected, a procedure thatalso combines ipsilateral MR recession will contribute tosatisfactory outcomes and decrease residual esotropia [29].
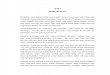
5.5. Process of Selecting a Surgical Procedure. A thorough eyeexamination and imaging of the patient before surgery willbe helpful for the surgical strategy. Patients are suggested tohave an MRI or CT scan of the orbit, which can give a cleardemonstration of the rectus muscle paths, the relationshipbetween the globe and muscle cone, and also the shape ofthe globe to exclude thyroid eye disease [26], severe myopicstaphylomata [29], or sagging eye syndrome [30, 31]. If thereis an absence of alteration in muscle paths, both Yokoyama’sprocedure and traditional recession-resection surgery havebeen recommended in some studies [11, 18]. However, it isstill a controversy in the selection of surgical proceduresin these cases. When the imaging test has confirmed anabnormality in muscle paths, forced duction test can con-tribute to distinguishing contracture of the MR muscle. Ifcontracture of the MR muscle is found, the MR recessionis recommended together with the union of the LR and SR[10, 14]. When performing these two procedures together,there exists the risk of anterior segment ischemia wheninvolving three muscles, so uniting half of the LR and SRmuscles (Yamada’s or Partial Jensen’s procedure) would bepreferred in combination with the MR recession [21, 23, 24].On the other hand, if there is no evidence of MR contracturebefore surgery, the MR recession can be staged in a secondsurgery when the union of LR and SR is not sufficient tocorrect the abnormal muscle paths. Yokoyama’s procedurehas been proven to be effective to correct up to 40Δ ofesotropia [16]. Yamada’s and Partial Jensen’s procedures havebeen performed successfully in patients with around 40Δ to60Δ of esotropia [19, 20, 22]. A flow diagram illustrates the
selecting process of a certain surgical procedure (Figure 2).
6. Summary
Loop myopexy is a safe and effective surgical treatment inpatients with high myopic strabismus. Different modifica-tions of this surgical procedure can be applied based onits concept, most of which have been proven to have goodsurgical outcomes. The selection of such modifications isof great importance in different patients. Careful evaluationbefore surgery should be made not only to make the correct
Patient
Normal musclepaths
Abnormal musclepaths
Orbital MRI or CT
Yokoyama’srecession-resection
Muscle contracture
No Yes
Yokoyama’sYamada’s
partial Jensen’s
Yamada’spartial Jensen’s
+MR recession
Not sufficient
MR recession
Forced duction test
Figure 2: Flow diagram of the selecting process of surgical proce-dure. MRI or CT scan of the orbit before surgery can give a cleardemonstration of the rectus muscle paths. If there is an absenceof alteration in muscle paths, both Yokoyama’s procedure andtraditional recession-resection surgery have been recommendedin some studies. In patients with abnormality in muscle paths,if contracture of the MR muscle is found, the MR recession isrecommended together with the union of the LR and SR. If thereis no evidence of MR contracture, the MR recession can be stagedin a second surgery when the union of LR and SR is not sufficient tocorrect the abnormal muscle paths.
diagnosis but also to choose an appropriate surgical proce-dure and offer individualized modifications in the surgery.
Competing Interests
The authors declare that they have no competing interests.
Acknowledgments
This study was supported by National High Technol-ogy Research and Development Program (863 Program)(2015AA020311) and National Natural Science Foundation ofChina (81320108010, 81470622).
References
[1] T. Hayashi, H. Iwashige, and T. Maruo, “Clinical featuresand surgery for acquired progressive esotropia associated withsevere myopia,” Acta Ophthalmologica Scandinavica, vol. 77, no.1, pp. 66–71, 1999.
[2] A. Bagheri, F. Adhami, and M. X. Repka, “Bilateral recession-resection surgery for convergent strabismus fixus associatedwith high myopia,” Strabismus, vol. 9, no. 4, pp. 225–230, 2002.
[3] T. H. Krzizok, H. Kaufmann, and H. Traupe, “New approachin strabismus surgery in high myopia,” British Journal ofOphthalmology, vol. 81, no. 8, pp. 625–630, 1997.
[4] Y. Aoki, Y. Nishida, O. Hayashi et al., “Magnetic resonanceimaging measurements of extraocular muscle path shift and

Journal of Ophthalmology 7
posterior eyeball prolapse from the muscle cone in acquiredesotropia with high myopia,” American Journal of Ophthalmol-ogy, vol. 136, no. 3, pp. 482–489, 2003.
[5] T. Rutar and J. L. Demer, “‘Heavy Eye’ syndrome in the absenceof high myopia: a connective tissue degeneration in elderlystrabismic patients,” Journal of AAPOS, vol. 13, no. 1, pp. 36–44,2009.
[6] T. Yokoyama, H. Tabuchi, S. Ataka, K. Shiraki, T. Miki, andK. Mochizuki, “The mechanism of development in progressiveesotropia with high myopia,” in Proceedings of the Transactionsof the 26thmeeting of European Strabismological Association, pp.218–221, Swets & Zeitlinger, Barcelona, Spain, September 2000.
[7] I. Wong, S.-W. Leo, and B.-K. Khoo, “Loop myopexy fortreatment of myopic strabismus fixus,” Journal of AAPOS, vol.9, no. 6, pp. 589–591, 2005.
[8] F. J. Rowe and C. P. Noonan, “Surgical treatment for progressiveesotropia in the setting of high-axial myopia,” Journal ofAAPOS, vol. 10, no. 6, pp. 596–597, 2006.
[9] H. Basmak, A. Sahin, and N. Yildirim, “Surgical treatmentof strabismus fixus associated with high myopia,” OphthalmicSurgery Lasers and Imaging, vol. 39, no. 5, pp. 397–398, 2008.
[10] M. Yamaguchi, T. Yokoyama, and K. Shiraki, “Surgical proce-dure for correcting globe dislocation in highly myopic strabis-mus,” American Journal of Ophthalmology, vol. 149, no. 2, pp.341–346, 2010.
[11] J. M. Durnian, S. Maddula, and I. B. Marsh, “Treatment of‘heavy eye syndrome’ using simple loop myopexy,” Journal ofAAPOS, vol. 14, no. 1, pp. 39–41, 2010.
[12] M.-H. Shih, M.-L. Li, and F.-C. Huang, “A preequatorialGore-Tex sling to restore rectus muscle pathways in myopicstrabismus fixus,” Journal of AAPOS, vol. 16, no. 1, pp. 80–82,2012.
[13] M. R. Akbari, L. H. Alhashemi, A. K. Jafari, B. Eshraghi, andG. Fakhraie, “Large angle esotropia with high myopia and alost medial rectus muscle: a case report,” Binocular Vision &Strabology Quarterly, Simms-Romano’s, vol. 28, no. 2, pp. 110–114, 2013.
[14] S. Akar, B. Gokyigit, E. Aribal, A. Demir, Y. S. Goker, and A.Demirok, “Surgical procedure joining the lateral rectus andsuperior rectus muscles with or without medial rectus recessionfor the treatment of strabismus associated with high myopia,”Journal of Pediatric Ophthalmology and Strabismus, vol. 51, no.1, pp. 53–58, 2014.
[15] Z. Acar and O. Altintas, “Pediatric experience in surgicaltreatment of acquired esotropia associated with high myopia,”Journal of Pediatric Ophthalmology and Strabismus, vol. 52, no.3, article 191, 2015.
[16] B. H. Shenoy, V. Sachdeva, and R. Kekunnaya, “Silicone bandloop myopexy in the treatment of myopic strabismus fixus:surgical outcome of a novel modification,” British Journal ofOphthalmology, vol. 99, no. 1, pp. 36–40, 2015.
[17] M. Yamada, S. Taniguchi, T. Muroi, S. Satofuka, and S. Nishina,“Rectus eyemuscle paths after surgical correction of convergentstrabismus fixus,”The American Journal of Ophthalmology, vol.134, no. 4, pp. 630–632, 2002.
[18] V. Sturm,M.N.Menke, K. Chaloupka, andK. Landau, “Surgicaltreatment of myopic strabismus fixus: a graded approach,”Graefe’s Archive for Clinical and Experimental Ophthalmology,vol. 246, no. 9, pp. 1323–1329, 2008.
[19] K. D. Godeiro, D. Kirsch, M. K. Tabuse, and M. Cronemberger,“Yamada’s surgery for treatment of myopic strabismus fixus,”International Ophthalmology, vol. 29, no. 4, pp. 305–308, 2009.
[20] P. C. Larsen and G. A. Gole, “Partial Jensen’s procedure for thetreatment of myopic strabismus fixus,” Journal of AAPOS, vol.8, no. 4, pp. 393–395, 2004.
[21] I. Ahadzadeghan,M. R. Akbari, A. Ameri, F. Anvari, A. K. Jafari,and M. T. Rajabi, “Muscle belly union for treatment of myopicstrabismus fixus,” Strabismus, vol. 17, no. 2, pp. 57–62, 2009.
[22] Z. Rajavi, A.-R. Ramezani, and P. Ashtar-Nakhaee, “Surgicaltreatment of heavy eye syndrome: report of two cases,” Journalof Ophthalmic and Vision Research, vol. 4, no. 4, pp. 256–259,2009.
[23] X.-L. Kang, Y. Wei, K.-X. Zhao et al., “Surgical treatmentof myopic strabismus fixus by modified Yokoyama’s surgery,”Zhonghua Yan Ke Za Zhi, vol. 47, no. 11, pp. 972–977, 2011.
[24] T.-H. Ho, M.-C. Lin, and S.-J. Sheu, “Surgical treatment ofacquired esotropia in patients with high myopia,” Journal of theChinese Medical Association, vol. 75, no. 8, pp. 416–419, 2012.
[25] M. Louis, M. Flanders, J. Chankowsky, S. Lindley, and R. Polo-meno, “Acquired restrictive strabismus and high axial myopia:diagnosis and management,” Canadian Journal of Ophthalmol-ogy, vol. 44, no. 4, pp. 437–440, 2009.
[26] M. P. Ranka and M. A. Steele, “Esotropia associated with highmyopia,” Current Opinion in Ophthalmology, vol. 26, no. 5, pp.362–365, 2015.
[27] P. Aydin, T. Kansu, and A. S. Sanac, “High myopia caus-ing bilateral abduction deficiency,” Journal of Clinical Neuro-Ophthalmology, vol. 12, no. 3, pp. 163–165, 1992.
[28] Y. Morad, E. Pras, Y. Goldich, Y. Barkana, D. Zadok, and M.Hartstein, “Surgical treatment of esotropia associated with highmyopia: unilateral versus bilateral surgery,” European Journal ofOphthalmology, vol. 20, no. 4, pp. 653–658, 2010.
[29] J. L. Demer, “Muscle paths matter in strabismus associated withaxial high myopia,” American Journal of Ophthalmology, vol.149, no. 2, pp. 184–186, 2010.
[30] Z. Chaudhuri and J. L. Demer, “Sagging eye syndrome: con-nective tissue involution as a cause of horizontal and verticalstrabismus in older patients,” JAMAOphthalmology, vol. 131, no.5, pp. 619–625, 2013.
[31] R. J. Tan and J. L. Demer, “Heavy eye syndrome versus saggingeye syndrome in high myopia,” Journal of American Associationfor Pediatric Ophthalmology and Strabismus, vol. 19, no. 6, pp.500–506, 2015.

Submit your manuscripts athttp://www.hindawi.com
Stem CellsInternational
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Disease Markers
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation http://www.hindawi.com Volume 2014
Immunology ResearchHindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Parkinson’s Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttp://www.hindawi.com