Embed Size (px)
Citation preview
LEADING ARTICLE
Drugs 44 (6): 921-927. 199200 12-6667/92/00 12-0921/$03 .50/0© Adis International Limited . All rights reserved .
DRU1217
Role of Helicobacter pylori in Duodenal Ulcer
E.A.J. RauwsDepartment of Gastroenterology and Hepatology, Academic Medical Centre, Meibergdreef,Amsterdam, The Netherlands
Numerous studies have demonstrated the association between antral gastritis and Helicobacterpylori infection (Buck et al. 1986; Marshall & Warren 1984; Warren & Marshall 1983). Humanvolunteer studies (Marshall et al. 1985; Morris &Nicholson 1987) and accidental inoculations (Graham et al. 1988; Langenberg et al. 1990; Wiersinga& Tytgat 1977) with H. pylori have confirmed thepathogenetic role of this microorganism in activechronic gastritis. However, the pathogenetic role ofH. pylori infection in duodenal ulcer disease is lessclear. Duodenal ulcer disease has a multifactorialaetiology and is believed to be the end-point of animbalance between various aggressive and defensive mechanisms. Many aggressive factors havebeen identified, including acid and pepsin, duodenogastric reflux, and recently also H. pylori colonisation. The relative importance of each individual factor is still not clear.
H. pylori is not found in association with intestinal-type epithelium. In the presence of gastricmucin cell metaplasia in the duodenum, considered to be a response to hyperacidity, H. pylori isable to colonise the duodenal mucosa (Wyatt et al.1987, 1990). Subsequently, impairment of the mucosal defence mechanism leads to active duodenitis and renders the mucosa susceptible to ulceration. This sequence of events ultimately leading toduodenal ulceration is not proven , but eradicationof H. pylori with bismuth compounds, with orwithout additional antibiotics, enhances ulcer healing (Graham et al. 1991b) and greatly reduces the
ulcer relapse rate (Borody et al. 1989; Borsch et al.1988; Coghlan et al. 1987; George et al. 1990; Lambert et al. 1987; Marshall et al. 1988;Rauws & Tytgat 1990;Smith et al. 1988), strongly suggestinganimportant aetiological role for H. pylori infectionin duodenal ulcer disease.
1. Epidemiology
In 1983 was suggested that H. pylori is stronglyinvolved in the aetiology of duodenal ulcers (Warren & Marshall 1983). H. pylori is found in almostall patients with endoscopically proven duodenalulcers, but about 50% of patients with nonulcerdyspepsia and about 20% of asymptomatic volunteers are also colonised by H. pylori, but withoutulceration (Rauws et al. 1988).
The peak incidence of duodenal ulcer disease isaround 45 to 55 years of age, but the prevalenceof H. pylori infection increases with age reaching60 to 70%at the age of 70 years (Dooley et al. 1989;Graham et al. 1988).
Remarkably, a relatively isolated group of Australian Aboriginals showed a seroprevalence of H.pylori infection of only 0.7% (Dwyer et al. 1988)and have virtually no peptic ulcer disease (Bateson1976).
20 to 50% of patients with duodenal ulcer havea positive family history, with first-degree relativeshaving a 2- to 3-fold increased risk to develop anulcer (McConnell 1966).
Duodenal ulcers are also more common in

922
patients with bloodgroup 0, nonsecretors and thosewith hyperpepsinogenaemia, all suggesting that inherited factors are also involved in ulcer pathogenesis (Rotter 1980; Samloff et al. 1986).
From these epidemiological data it can be concluded that duodenal ulcer disease is strongly associated with H. pylori infection. H. pylori infection is also a marker for antral gastritis which isknown to be associated with duodenal ulceration,or H. pylori plays a direct role in causing ulceration.
2. Pathogenesis of Duodenal Ulcers
As well as many aggressive factors, defensivemechanisms such as an intact mucus barrier, bicarbonate secretion and mucosal blood flow, alsoplay an important role in the pathogenesis of duodenal ulcers (Peterson 1991; Soli 1990). For example, because only 30 to 40% of patients withduodenal ulcer disease have acid secretion ratesabove the normal range, it had already been previously suggested that other factors apart from acidand pepsin must be important as well. The isolation of H. pylori from the human stomach generated much excitement, especially when it wasshown that this microorganism was the cause ofgastritis and probably played a dominant role inthe pathogenesis of peptic ulcer disease.
H. pylori displays potent urease activity (Eatonet al. 1990; Marshall et al. 1990; Smoot et al. 1990),a property that may have important pathogeneticimplications. Bacterial hydrolysis of urea to ammonium ions may produce an alkaline environment around the microorganisms. In parietal cells,excess ammonia combines with hydrogen ions toform ammonium ions which are secreted in preference to hydrogen ions, probably leading to parietal cell failure and hypo- or even achlorhydria.Hypochlorhydria, usually temporarily, has indeedbeen reported during the initial phase of H. pyloricolonisation (Graham et al. 1988; Morris & Nicholson 1987; Ramsey et al. 1979).
Also as a consequence of generating ammonia,H. pylori may disturb the normal negative feedback of acid to the antral G-cells (granular enter-
Drugs 44 (6) 1992
ochromaffin cells which secrete gastrin) [Levi et al.1989]. This group reported that patients with active duodenal ulcers and H. pylori infection secreted more acid and released more gastrin in response to a test meal than uncolonised patients.The mechanism by which H. pylori infection of thegastric antrum increases basal and meal-stimulatedplasma gastrin levels is unclear. It has been suggested that it might be the result of the ammoniaproduced by the microorganisms raising antral surface pH and thus prevents acid inhibition of thegastrin release by the gastrin-producing G-cells.Other investigators have confirmed this , and alsoshown that the exaggerated gastrin response to ameal is reversed after H. pylori has been eradicated(Graham et al. 1990, 1991a; McColl et al. 1991).
These data strongly support the view thatchronic infection with H. pylori is the cause of thisincreased circulating levels of gastrin . However,eradication of H. pylori and a decrease in gastrinlevels does not change the overall acid output, andcasts some doubt on the importance of the elevatedgastrin levels in the pathogenesis of duodenal ulceration.
In addition, H. pylori produces catalases , lipases, phospholipases, proteolytic enzymes, adhesins and toxins. After attaching to the epithelial cell,these enzymes, metabolic products and toxins mayreach the epithelial cell membrane. Proteases, lipases and phospholipases may reduce the important mucosal defence by degrading the mucous layerand damaging the lipid-containing epithelial cellmembrane.
Figura et al. (1989) demonstrated that cytotoxin-producing strains of H. pylori were isolatedmore frequently from patients with peptic ulcerdisease (66.6%) than from patients with chronicgastritis only (30.1%; p < 0.01).
Finally, H. pylori antigens elicit an immune response. Crabtree et al. (1991) studied mucosal IgAresponse to H. pylori using immunoblotting techniques. Of 19 patients with chronic gastritis whodid not recognise a 120kD protein none had pepticulcers, whereas 25 of 57 with positive recognitionhad peptic ulcers (p < 0.001), suggesting virulencedifferences between the various H. pylori isolates.
Helicobacter pylori in Duodenal Ulcer
3. H. pylori and Gastritis
H. pylori is the most common cause of acuteand chronic gastritis. Most information about acuteH. pylori infection comes from volunteer studies(Marshall et al. 1985; Morris & Nicholson 1987)and accidental inoculation during acid secretionstudies (Gledhill et al. 1985; Graham et al. 1988;Ramsey et al. 1979). In both volunteer studies, thesubjects had normal gastric mucosa before theyswallowed the H. pylori isolate . Repeat endoscopyand biopsy revealed active chronic gastritis, andspiral bacilli were seen adhering to the surface epithelium.
Successful eradication of the organism, especially by an antibiotic with no known intrinsic effect towards the gastric mucosa, leads to normalisation of the gastric mucosa, thus supporting theevidence for the pathogenetic role of H. pylori incausing inflammation.
H. pylori is highly adapted to the mucus thatcovers gastric-type epithelial cells. Patients withduodenal ulceration are known to have chronic antral gastritis characterised by a chronic inflammatory infiltrate associated with lymphoid follicles.The body mucosa is usually normal or shows onlyminimal inflammation. This type of gastritis doesnot progress proximally into the body mucosa(Jonsson et al. 1988; Kekki et al. 1984), so there isno loss of acid secretory capacity.
Grading of gastritis and the extent of its presence (antrum or corpus or both) correlates with thefunction of the gastric mucosa (Sipponen et al.1989). Gastritic and atrophic alterations markedlyaffect the function of gastric mucosa, for instancewith regard to the release of gastrin from the antralglands or the secretion ofacid and pepsin from theoxyntic body mucosa (Siurala et al. 1985; Varis etal. 1979). The classification of atrophy as slight,moderate, or severe (total) , correlates nearly linearly with a decrease in the output of acid, pepsinsand gastrin.
Gastritis may also impair mucosal resistance.Atrophic gastritis affects synthesis, composition,and thickness of the mucous layer at the gastricsurface (Domschke et al. 1981). These effects may
923
influence the physiological homeostasis of thestomach and may also modulate the risk and likelihood of an individual developing a peptic ulcer.
The relative risk of duodenal ulcer is approximately 20-fold in subjects with antral gastritis andnearly normal corpus mucosa, compared with thosewho have an endoscopically and histologically normal antrum (Sipponen et al. 1989).
4. H. pylori and Duodenitis
H. pylori is only found in inflamed duodenalmucosa, and only in association with gastric epithelium (gastric metaplasia) in the duodenum.Gastric metaplasia is common and, as small foci,has been found in 64% of normal subjects (Kreuning et al. 1978). The condition is considered to beeither a defence mechanism or change in responseto damage, i.e. acid entering the duodenum (Rhodes1964).
Wyatt et al. (1987) investigated the strength ofthe association between the presence of H. pylori,gastric metaplasia and duodenitis. In general themore extensive the metaplasia, the more likely therewas to be duodenitis, and active duodenitis wasrarely present if only small foci of gastric metaplasia exist. This study showed that duodenitis is present in those patients with H. pylori-induced gastritis and gastric metaplasia in the duodenum.These results are consistent with the hypothesis thatduodenitis is the result of duodenal colonisation byH. pylori.
Gastric metaplasia is found in the margins ofduodenal ulcers and scars of healed ulcers. Furthermore, if the acid secretion is diminished, forinstance after highly selective vagotomy, then gastric metaplasia is reversed.
5. H. pylori and Duodenal Ulcer
Acid suppressive therapy with H2-receptor antagonists or proton pump inhibitors, which have noeffect on the presence of H. pylori, leads to ulcerhealing. On the other hand, sucralfate and bismuthcompounds, which lack any effect on gastric acidsecretion, also heal ulcers at .the same rate as acid
924
suppressive agents. However, sucralfate and bismuth compounds have many modes of action. Oneof the intriguing effects of tripotassium dicitratobismuthate (colloidal bismuth subcitrate) is its bactericidal effect against H. pylori, an effect absent inall other conventional ulcer healing agents (Marshall et al. 1984, 1987). It has been suggested thatthe lower duodenal ulcer relapse rate after healingwith bismuth compounds might be caused by itsanti-Helicobacter bactericidal effect (Hamilton etal. 1986; Lane & Lee 1988; Lee et al. 1985; Martinet al. 1981). This is, however, difficult to prove,since colloidal bismuth has several effects otherthan its antimicrobial activity (Konturek et al. 1987;Lavy et al. 1976; Lee 1982), including stimulationof prostaglandin E2production with subsequent secretion of alkali into the mucus layer, reduction ofpepsin production, and formation of a glycoprotein-bismuth complex in the gastric mucus layer.
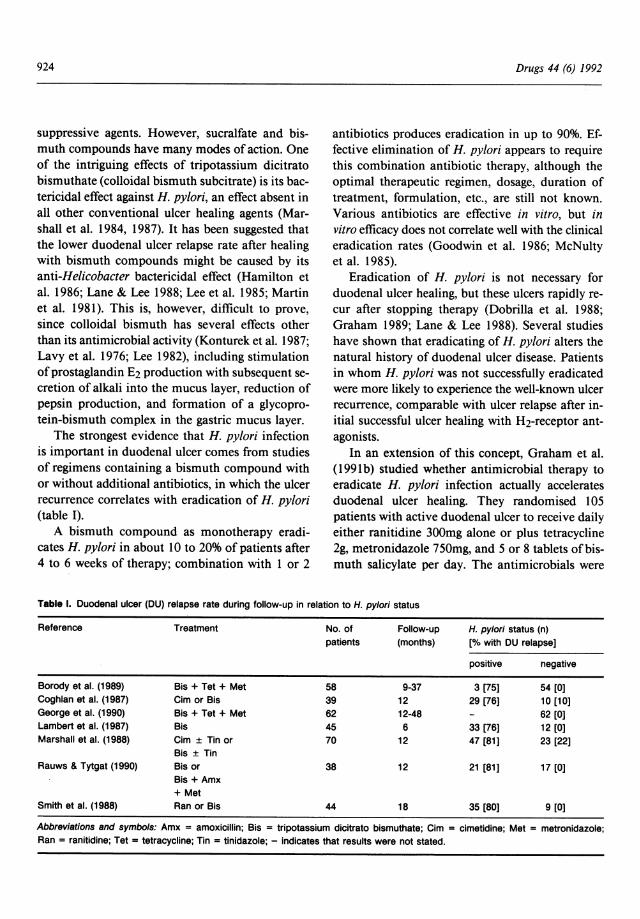
The strongest evidence that H. pylori infectionis important in duodenal ulcer comes from studiesof regimens containing a bismuth compound withor without additional antibiotics, in which the ulcerrecurrence correlates with eradication of H. pylori(table I).
A bismuth compound as monotherapy eradicates H. pylori in about 10 to 20% of patients after4 to 6 weeks of therapy; combination with I or 2
Drugs 44 (6) 1992
antibiotics produces eradication in up to 90%. Effective elimination of H. pylori appears to requirethis combination antibiotic therapy, although theoptimal therapeutic regimen, dosage, duration oftreatment, formulat ion, etc., are still not known.Various antibiotics are effective in vitro, but invitro efficacydoes not correlate well with the clinicaleradication rates (Goodwin et al. 1986; McNultyet al. 1985).
Eradication of H. pylori is not necessary forduodenal ulcer healing, but these ulcers rapidly recur after stopping therapy (Dobrilla et al. 1988;Graham 1989; Lane & Lee 1988). Several studieshave shown that eradicating of H. pylori alters thenatural history of duodenal ulcer disease. Patientsin whom H. pylori was not successfully eradicatedwere more likely to experience the well-known ulcerrecurrence, comparable with ulcer relapse after initial successful ulcer healing with H2-receptor antagonists.
In an extension of this concept, Graham et al.(1991b) studied whether antimicrobial therapy toeradicate H. pylori infection actually acceleratesduodenal ulcer healing. They randomised 105patients with active duodenal ulcer to receive dailyeither ranitidine 300mg alone or plus tetracycline2g, metronidazole 750mg, and 5 or 8 tablets ofbismuth salicylate per day. The antimicrobials were
Table I. Duodenal ulcer (DU) relapse rate during follow-up in relation to H. pylori status
Reference Treatment No. of Follow-up H. pylori status (n)patients (months) [% with DU relapse]
positive negative
Sorody et al. (1989) Sis + Tet + Met 58 9-37 3 [75] 54 [0]Coghlan et al. (1987) Cim or Sis 39 12 29 [76] 10 [10]George et al. (1990) Sis + Tet + Met 62 12-48 62 [0]Lambert et al. (1987) Sis 45 6 33 [76] 12 [0]Marshall et al. (1988) Cim ± Tin or 70 12 47 [81] 23 [22]
Sis ± TInRauws & Tytgat (1990) Sis or 38 12 21 [81] 17 [0]
Sis + Amx+ Met
Smith et al. (1988) Ran or Sis 44 18 35 [80] 9 [0]
Abbreviations and symbols: Amx = amoxicillin; Sis = tripotassium dicitrato bismuthate; Cim = clmetidine; Met = metronidazole;Ran = ranitidine; Tet = tetracycline; Tin = tinidazole; - indicates that results were not stated.
Helicoba cter pylori in Duodenal Ulcer
only given during the first 2 weeks of treatment.Repeat endoscopy was performed after 2, 4, 8, 12and 16 weeks. In this study, combined therapy withantimicrobials and ranitidine resulted in a significantly superior ulcer healing rate compared withranitidine monotherapy. The cumulative percentages of patients with healed ulcers in the group receiving ranitidine plus antibiotics versus ranitidinemonotherapy recipients were 37 vs 18% after 2weeks; 74 vs 53% at week 4;84 vs 68% at week 8;96 vs 80% at week 12; and 98 vs 84% at week 16.These data again indicate that H. pylori infectionis important in duodenal ulcer disease.
6. Conclusion
Duodenal ulceration is a multifactorial disease.Neither gastric acid and pepsin secretion, nor H.pylori infection alone can explain why only somepeople develop ulcers but the majority do not.Other factors must also be involved in the pathogenesis of duodenal ulceration. Most recent datasuggest, however, that although other poorly delineated factors may modify the risk of ulceration, acidand pepsin secretion synergistically with H. pyloriinfection are by far the most important factors inulcer pathogenesis.
Treatment with acid-suppressive therapy or bismuth-antibiotic combinations heals ulcers at anequivalent rate. However, treatment with bismuthcompounds with or without antibiotics leads to remission of the mucosal inflammation and reducesthe duodenal ulcer relapse rate, but only if H. pylori has been successfully eradicated.
The optimal regimen to eradicate H. pylori isnot yet known, but probably in the near future shortcourses of triple therapy or antibiotic combinations with acid-suppressive drugs may prove to beeffective, free from significant side effects, and freefrom inducing microbial resistance. One shouldcarefully assess the possible risks versus potentialbenefits of anti-Helicobacter therapy for the individual patient.
It has been suggested that therapy aimed ateradicating H. pylori should only be considered if
925
duodenal ulcer is a serious management problemrequiring either continuous medication or beforeconsidering surgery, or if complications like bleeding or perforation have occurred (Tytgatet al. 1990).
If anti-H. pylori medication is prescribed, themost effective regimen should be given. Tripletherapy , i.e a combination oftripotassium dicitratobismuthate or bismuth subsalicylate I tablet 4 timesdaily, tetracycline 500mg 4 times daily, and metronidazole 400mg 3 times daily for 2 weeks has beenrecommended.
References
Bateson EM. Duodenal ulcer: does it exist in Australian Aborigines? Australian and New Zealand Journal of Medicine 6: 545547, 1976
Borody T, Noonan S, Cole P, Morgan A, Genne J, et al. Recurrence of duodenal ulcer and Campylobacter pylori infectionafter eradicat ion. Medical Journal of Australia 151: 431-435,1989
Borsch G, Mai U, Opferkuch W. Oral triple therapy may effectively eradicate Campy/obacter pylori in man: a pilot study.Gastroenterology 94: A44, 1988
Buck GE, Gourl y WI(, Lee WI(, Subraman yam K, Latimer JM,et al. Relation of Campy/obacter pylori to gastrit is and pepticulcer. Journal of Infectious Diseases 153: 664-669, 1986
Coghlan JG, Humphries H, Dooley C, Keane C, Gilligan D, etal. Campylobacter pylori and recurrence of duodenal ulcers a 12-month follow-up study. Lancet 2: 1109-1111 , 1987
Crabtree JE, Taylor JD, Wyatt JE, Heatley RV, Shallcross TM,et al. Mucosal IgA recognition of Helicobacter pylori 120 FDAprotein , peptic ulceration and gastric pathology. Lancet 338:332-335, 1991
Dobrilla G, Vallaperta P, Amplatz S. Influence of ulcer healingagents on ulcer relapse after discontinuation of acute treatment: a pooled estimate of controlled clinical trials. Gut 29:181-187, 1988
Domschke W. Norma1e und gestorte Schleimsekretion des Magens - Therapeutische Massnahmen. In Domschke W &Wormsley KG (Eds) Magen und Magenkrankheiten , pp. 162174, Thieme, Stuttgart , 1981
Dooley CP, Cohen H, Fitzgibbons PL, Bauer M, Appleman MD,et al. Prevalence of He/icobacter pylori infection and histologicgastritis in asymptomatic persons. New England Journal ofMedicine 321: 1562-1566, 1989
Dwyer B, Nanxiong S, Kaldor J, Tee W, Lambert J, et al. Antibody response to Campy/obacter pylori in an ethnic grouplacking peptic ulceration. Scandina vian Journal of InfectiousDiseases 20: 63-68, 1988
Eaton KA, Morgan DR, Brooks C, Krakowka S. Essential role ofurease in the pathogenesis of gastritis induced by Helicobacterpylori in gnotobiot ic piglets. Abstract. Gastroenterology 98(Suppl.): A654, 1990
Figura N, Guglielmetti P, Rossolini A, Barberi A, Cusi G, et al.Cytotoxin product ion by Campy/obacter pylori strains isolatedfrom patients with peptic ulcers and from patients with chronicgastrit is only. Journal of Clinical Microbiology 27: 225-226,1989
926
George LL, Borody TJ , Andrews P, Devine M, Moore-Jones D,et al. Cure of duodenal ulcer after eradication of Helieobaeterpylori. Medical Journal of Australia 153: 145-149, 1990
Gledhill T, Leicester RJ, Addis B. Epidemic hypochlorhydria.British Medical Journal 290: 1383-1386, 1985
Goodwin CS, Blake PK, Blincow ED. The minimum inhibitoryand bacterial concentrations of antibiotics and anti-ulcer agentsagainst Campylobaeter pyloridis . Chemotherapy 17: 309-314,1986
Graham DY, Alpert LC, Smith JL, Yoshimura HH . IatrogenicCampylobaeter pylori infection is a cause of epidemic achlorhydria. American Journal of Gastroenterology 83: 974-980,1988
Graham DY. Campylobaeter pylori and peptic ulcer disease.Gastroenterology 96: 615-625, 1989
Graham DY, Klein PD, Opekun AR, Boutton TW. Effect of ageon the frequency of active Campylobaeter pylori infection diagnosed by the [13C) urea breath test in normal subjects andpatients with peptic ulcer disease . Journal of Infectious Diseases 157: 777-780, 1988
Graham DY, Opekun A, Lew GM , Evans DJ, Klein PD, et al.Ablation of exaggerated meal-st imulated gastrin release in duodenal ulcer patients after clearance of Helieobaeter (Campylobaeter) pylori infection. American Journal of Gastroenterology 95: 394-398, 1990
Graham DY, Opekun A, Lew GM, Klein PD, Walsh JH , et al.Helieobaeter pylori-associated exaggerated gastrin release induodenal ulcer patients. Gastroenterology 100: 1571-1575,1991a
Graham DY, Lew GM, Evans 00, Evans J, Klein PD. Effect oftriple therapy (antibiotics plus bismuth) on duodenal ulcerhealing. Annals ofInternal Medicine 115: 266-269, 1991b
Hamilton I, O'Connor HJ, Wood NC, Bradbury I, Axon ATR.Healing and recurrence of duodenal ulcer after treatment withtripotassium dicitrato bismuthate (TBD) tablets or cimetidine.Gut 27: 106-110, 1986
Jonsson KA, Strom M, Bodemar G, Norrby K. Histologicalchanges in the gastroduodenal mucosa after long-term medicaltreatment with cimetidine or parietal cell vagotomy in patientswith juxtapyloric ulcer disease . Scandinavian Journal ofGastroenterology 23: 433-441, 1988
Kekki M, Sipponen P, Siurala M. Progression of antral and bodygastritis in patients with active and healed duodenal ulcer andduodenitis. Scandinavian Journal ofGastroentero!ogy 19: 382388, 1984
Konturek SJ, Radecki T, Piastucki I, Drozdowicz D. Studies onthe gastroprotective and ulcer-healing effects of colloidal bismuth subcitrate. Digestion 37 (Suppl. 2): 8-15, 1987
Kreuning J, Bosman FT, Kuiper G, Wal AM, Lindeman J. Gastric and duodenal mucosa in 'healthy' individuals. Journal ofClinical Pathology 31: 69-77, 1978
Lambert JR , Borromeo M, Korman MG, Hansky J, Eaves ER.Effect of collo idal bismuth (De-Nol) on healing and relapse ofduodenal ulcers - role of Campylobaeter pyloridis . Gastroenterology 92: 1489, 1987
Lane MR, Lee SP. Recurrence of duodenal ulcer after medicaltreatment. Lancet I: 1147-1149, 1988
Langenberg W, Rauws EAJ, Oudbier JH , Tytgat GN . Patient-topatient transmission of Campylobacter pylori infection by fiberoptic gastroduodenoscopy and biopsy . Journal of Infect iousDiseases 161: 507-511,1990
Lavy UI, Koekkoek PH, Jait ly KD. Anti-ulcer activity of colloidal bismuth subcitrate in Shay rats. Archives of InternationalPharmacodynamics and Therapeutics 224: 291-298, 1976
Lee FI, Samloff 1M, Hardman M. Comparison of tripotassiumdicitrato bisrnuthate tablets with ranitidine in healing and relapse of duodenal ulcer. Lancet 1: 1299-1302, 1985
Lee SP. A potential mechanism of action of colloidal bismuthsubcitrate: diffusion barrier to hydrochloric acid. ScandinavianJournal of Gastroenterology 17 (Suppl. 80): 17-21, 1982
Drugs 44 (6) 1992
Levi S, Beardshall K, Haddad G, Playford R, Ghosh P, et al.Campylobaeter pylori and duodenal ulcers, the gastrin link.Lancet I: 1167·1168 , 1989
Marshall 81, Warren JR . Unidentified curved bacilli in the stomach of patients with gastritis and peptic ulceration. Lancet I:1311-1315, 1984
Marshall BJ, Hislop I, Glancy R, Armstrong J. Histological improvement of active chronic gastritis in patients treated with'De-Nol', Australian and New Zealand Journal of Medicine 14(Suppl. 4): 907, 1984
Marshall BJ, Armstrong JA, McGechie DB, Glancy RJ. Attemptto fulfil Koch's postulates for pyloric campylobacter. MedicalJournal of Australia 142: 436-439, 1985
Marshall BJ, Armstrong JA, Francis GJ , Nokes NT, Wee SH.Antibacterial action of bismuth in relat ion to Campylobaeterpyloridis colonization and gastritis . Digestion 37 (Suppl. 2): 1630, 1987
Marshall BJ, Goodwin CS, Warren JR , Murray R, Blincow ED,et al. Prospective double-blind trial of duodenal ulcer relapseafter eradication of Campylobaeter pylori. Lancet 2: 1437-1442,1988
Marshall BJ, Barrett U, Prakash C, McCallum RW, GuerrantRL. Urea protects Helieobaeter (Campylobaeter) pylori fromthe bactericidal effect of acid. Gastroenterology 99: 697-702,1990
Mart in DF, May SJ, Tweedle DEF, Hollanders D, RavenscroftMM, Miller JP . Difference in relapse rates of duodenal ulcerafter healing with cimetidine or tripotasium dicitrate bisrnuthate, Lancet I: 7-10, 1981
McColl KEL, Fullartson GM , Chittajaly R, EI Nujumi AM, Macdonald AMI, et al. Plasma gastrin, daytime intragastric pH andnocturnal acid output before and at I and 7 months after eradication of Helicobacter pylori in duodenal ulcer subjects. Scandinavian Journal of Gastroenterology 26: 339-346, 1991
McConnell RB. In The genetics of gastrointestinal disorders: gastric and duodenal ulcer, pp. 76-101, Oxford University Press,London, 1966
McN ulty CAM, Dent J, Wise R. Susceptibility of clinical isolatesof Campylobaeter pylori to II antimicrobial agents. Agents andChemotherapy 28: 837-838, 1985
Morris A, Nicholson G. Ingestion of Campylobaeter pyloridisCauses gastritis and raised fasting gastric pH. American Journal of Gastroenterology 82: 192-199, 1987
Peterson WL. Helieobaeter pylori and peptic ulcer disease . NewEngland Journal of Medicine 324: 1043-1047, 1991
Ramsey EJ, Carey KY, Peterson WL. Epidemic gastritis withhypochlorhydria. Gastroenterology 76: 1449-1457, 1979
Rauws EAJ, Langenberg W, HouthoffHJ, Zanen HC, Tytgat GNJ.Campylobaeter-pyloridis-associated chronic active antral gastrit is. Gastroenterology 94: 33·40, 1988
Rauws EAJ, Tytgat GNJ . Eradication ofHelieobaeter pylori curesduodenal ulcer. Lancet I: 1233-1235, 1990
Rhodes J. Experimental production of gastric epithelium in theduodenum. Gut 5: 454-458, 1964
Rotter JI. The genetics of peptic ulcer: more than one gene, morethan one disease. In Steinberg AG et al. (Eds) Progress inMedical Genetics 4: I-58, 1980
Samloff 1M, Stemmermann GN, Heilbrun LK, Nomura A. Elevated serum pepsinogen I and II levels differ as risk factorsfor duodenal ulcer and gastric ulcer. Gastroenterology 90: 570576, 1986
Sipponen P, Seppala K, Aarynen M, Helske T, Kettunen P.Chronic gastritis and gastroduodenal ulcer: a case-control studyon risk of coexisting duodenal or gastric ulcer in patients withgastritis. Gut 30: 922.929, 1989
Siurala M, Sipponen P, Kekki M. Chronic gastritis : dynamic andclinical aspects. Scandinavian Journal of Gast roenterology 20(Suppl. 109): 69-79, 1985
Smith AC, Price AB, Borriello P, Levi AJ. A compa rison of ran-

Helicobacter pylori in Duodenal Ulcer
itidine and tripotassium dicitrato-bismuth (TDB) in relapserates of duodenal ulcer. The role of Campylobacter pylori.Gastroenterology 94: A431, 1988
Smoot DT, Mobley HLT. Chippendale GR , Lewison JF , ResauJH . Helicobacter pylori urease activity is toxic in human gastric epithelial cells. Infection and Immunity 58: 1992-1994, 1990
Soli AH. Pathogenesis of peptic ulcer and implications for therapy.New England Journal of Medicine 322: 909-916 , 1990
Tytgat GNJ, Axon ATR, Dixon MF, Graham DY, Lee A, et al.Helicobacter pylori: causal agent in peptic ulcer disease? InWorking Party Reports. World Congresses of Gastroenterology, 26-31 August. 1990, pp. 36-45, Blackwell Scientific , Oxford, 1990
Varis K, Iharnaki T, Harkonen M. SamlofT M. Gastric morphology, function and immunology in first-degree relatives ofprobands with pernicious anaemia and controls. ScandinavianJournal of Gastroenterology 14: 129-139, 1979
927
Warren JR , Marshall BJ. Unidentified curved bacilli in gastricepithelium in active chronic gastritis. Lancet I: 1273-1275, 1983
Wiersinga WM, Tytgat GN . Clinical recovery owing to parietalcell failure in a patient with Zollinger-Ellison syndrome.Gastroenterology 73: 1414-1417, 1977
Wyatt J1, Rathbone BJ, Dixon MF, Heatley RV. Campylobacterpyloridis and acid induced gastric metaplasia in the pathogenesis of duodenitis. Journal of Clinical Pathology 40: 841-848,1987
Wyatt J1, Rathbone BJ, Sobala G, Shallcross T, Heatley RV, etal. The prevalence and distribution of gastric epithelium in theduodenum and its relationship to Helicobacter pylori and inflammation. Journal of Clinical Pathology 43: 981-986, 1990
Correspondence and reprints: Dr E.A.J. Rauws, Department ofGastroenterology and Hepatology, Academic Medical Centre,Meibergdreef9, 1105 AZ Amsterdam, The Netherlands.
Seminar on
Biocompatible SurfacesDesign, Characterisation and Applications
Date: 14-16 April 1993
Venue: San Diego, California, USAFor further information, please contact:
Pharmaceutica l DivisionTechnomic Publishing Co. Inc.
851 New Holland AvenueLancasterPA 17604
USA