Embed Size (px)
DESCRIPTION
Scleral Diseases
Citation preview
CONJUNCTIVA AND SCLERAL DISEASES
BAGIAN ILMU PENYAKIT MATA
FAKULTAS KEDOKTERAN
UNIVERSITAS HASANUDDIN
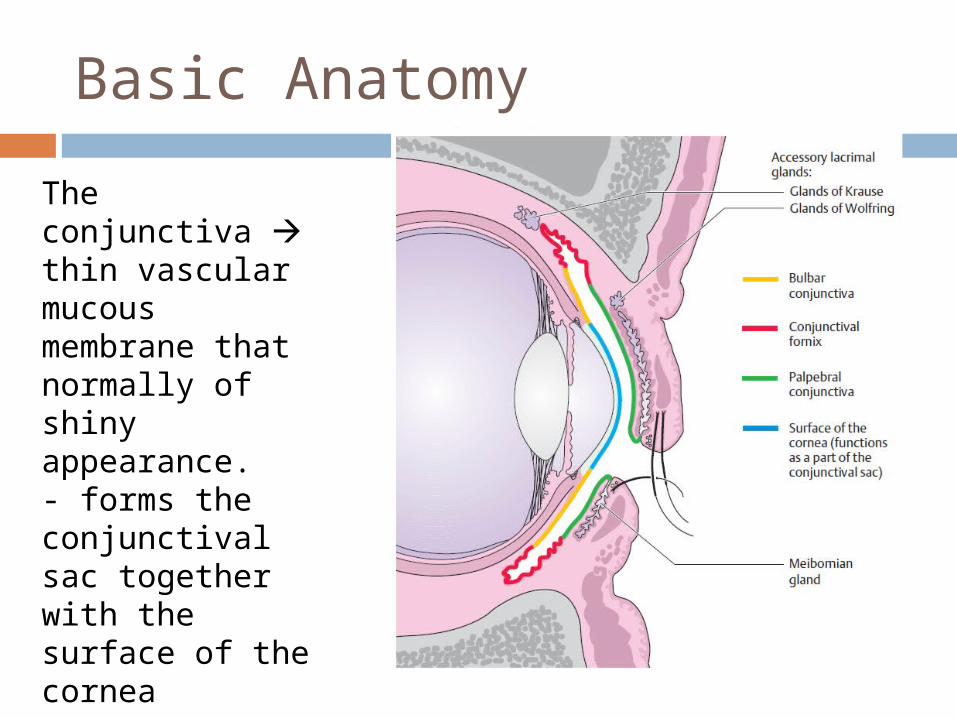
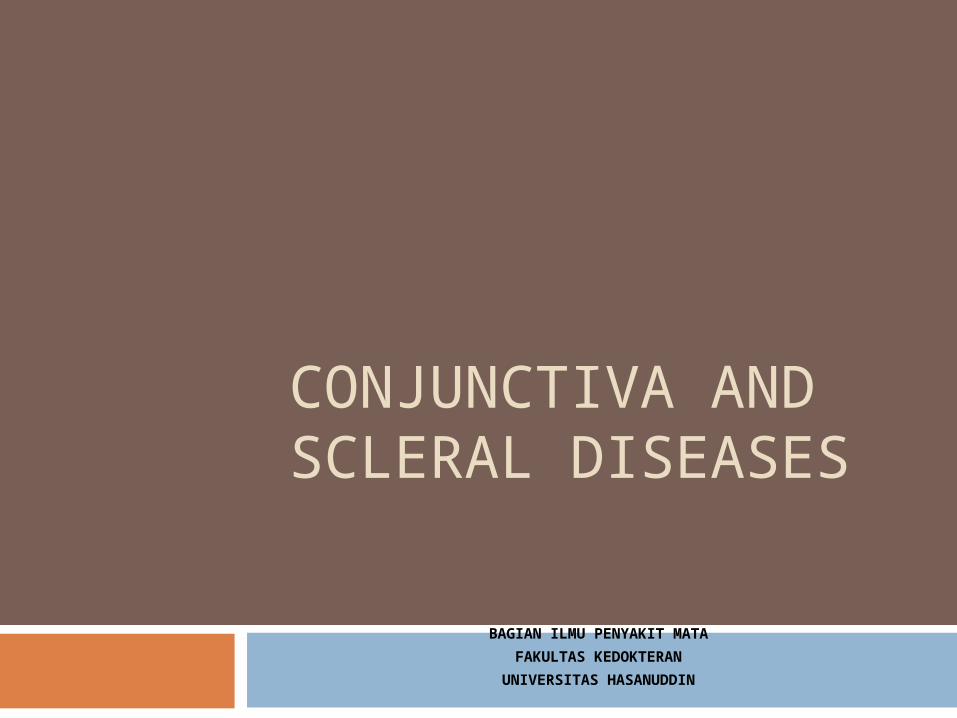
Basic Anatomy
The conjunctiva thin vascularmucous membrane that normally of shiny appearance.- forms the conjunctivalsac together with the surface of the cornea
Function
Motility of the eyeball. The loose connection between the bulbar conjunctiva
Articulating layer Protective function
CONJUNCTIVITIS
DefinitionAny form of inflammation of the conjunctiva, marked by vascular dilatation, cellular infiltration and exudation
ClassificationBased On :
a. Causes
b. Age of onset
c. Type of exudates
d. Progressivity
1
Based on the Causes
Bacterial conjunctivitis Most common causesStaph, Strep,
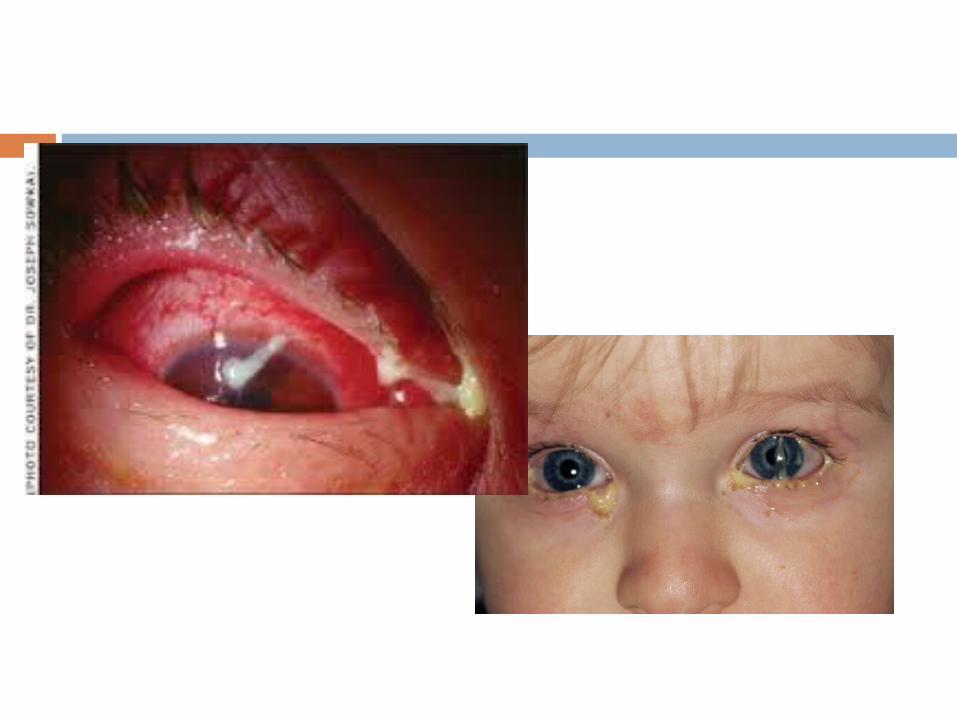
Pneumococcus Acute phase :sign and symptom : vasodilatation
( conjuctival injection) mucopurulen discharge, accompanied by irritation, sticky and foreign body sensation
Chronic phase : slow onset, slowly progress Vision does not affected
Diagnosis
Sign and symptom most reliable Laboratory finding swab culture ( only
if standard treatment tend to fail)
Treatment Bacterial conjunctivitis responds very well to
antibiotic (gentamicin, tobramycin, Aureomycin, chloramphenicol, neomycin, polymyxin B in combination with bacitracin and neomycin , Terramycin,kanamycin, fusidic acid, ofloxacin, and acidamphenicol)
Ointments (longer acting) and eyedrops 1 See Appendix for side effects of medications
Preparations that combine an antibiotic and cortisone can more rapidly alleviate subjective symptoms
Treatment …
Personal hygiene : hold transmission
Prognosis Good, if had sufficient theraphy
Viral Conjunctivitis
Epidemic conjunctivitis, pharyngoconjunctivitis fever, acute haemorrhagik conjuctivitis
highly contagious caused by type 18 or19 adenovirus spread by direct contact
Sign and symptoms
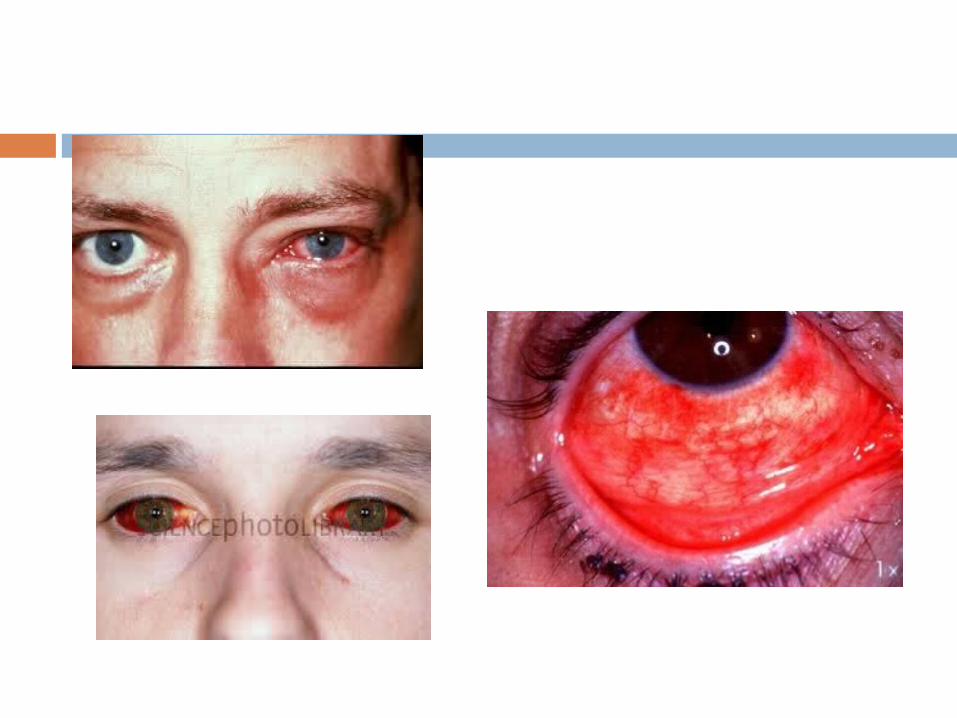
Usually unilateral. Severe lacrimation and itching mucoid discharge Subconj. Bleeding : acute hemorrhagic often also have a moderate influenza
infection Diagnostic considerations: Characteristic
findings include reddening and swelling of the plica semilunaris
Various types
1. PHARINGOCONJUNCTIVA FEVER Marked by pharingitis, fever and follicular conjunctivitis highly contagius phase (10-12 days) Self healing 5-14 days Type 3 adenovirus Identification with netralization test No specific R
2. EPIDEMIC KERATOKONJUNCTIVITIS No systemic symptopms 7-14 days Sometimes accompanied by epithelial keratitis with normal
corneal sensation
3. Acute Haemorrhagic conjunctivitis
conjunctivitis Apollo XI (1969). Caused by enterovirus tipe 70. Short incubation period (8-48
jam) Short lasting (5-7 days) Self limited in 5-7 days
Allergic/ Immunologic Conjunctivitis Hay fever seasonal Vernal conjunctivitis Giant papillary conjunctivitis Phlyctenular conjunctivitis Oculomucocutaneus syndromes ( SSJ,
Lyell’s Syndrome)
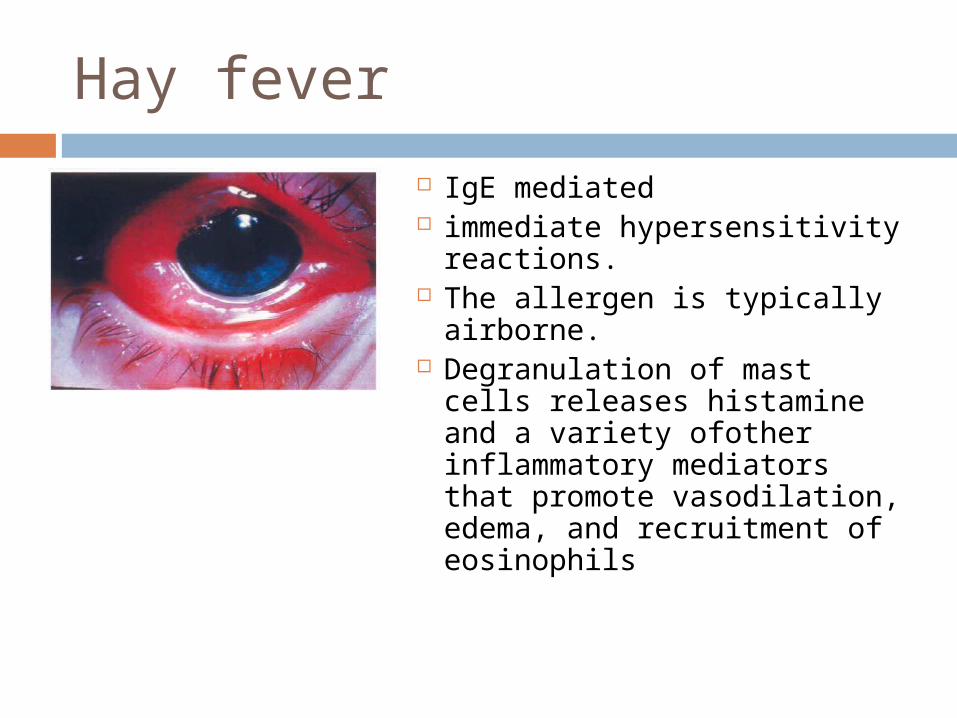
Hay fever
IgE mediated immediate hypersensitivity
reactions. The allergen is typically
airborne. Degranulation of mast
cells releases histamine and a variety ofother inflammatory mediators that promote vasodilation, edema, and recruitment of eosinophils
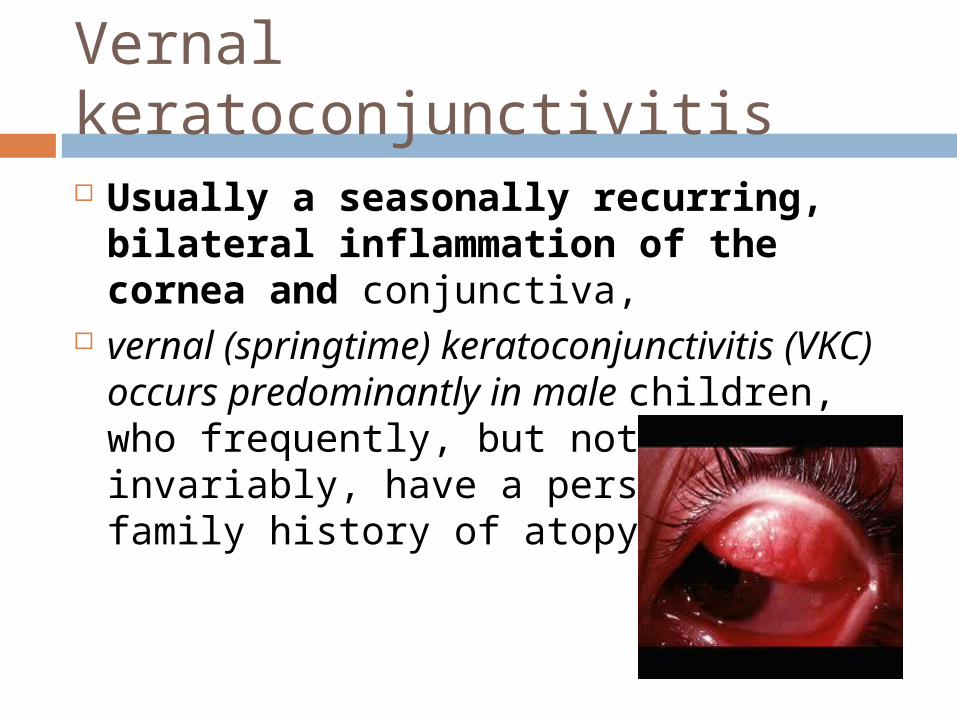
Vernal keratoconjunctivitis
Usually a seasonally recurring, bilateral inflammation of the cornea and conjunctiva,
vernal (springtime) keratoconjunctivitis (VKC) occurs predominantly in male children, who frequently, but not invariably, have a personal or family history of atopy
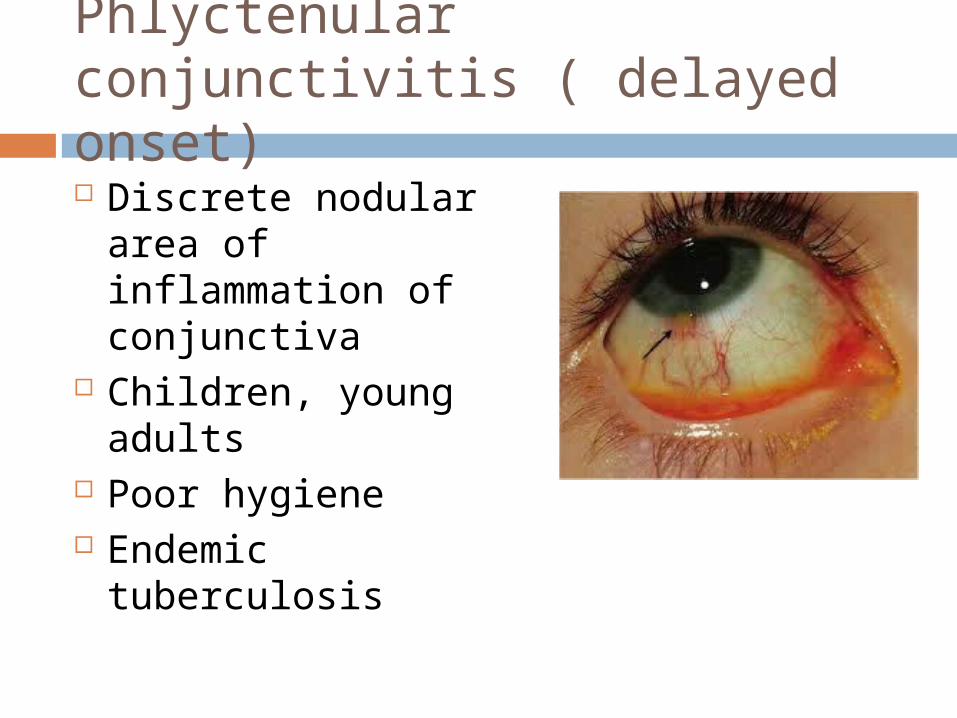
Phlyctenular conjunctivitis ( delayed onset) Discrete nodular area
of inflammation of conjunctiva
Children, young adults
Poor hygiene Endemic tuberculosis
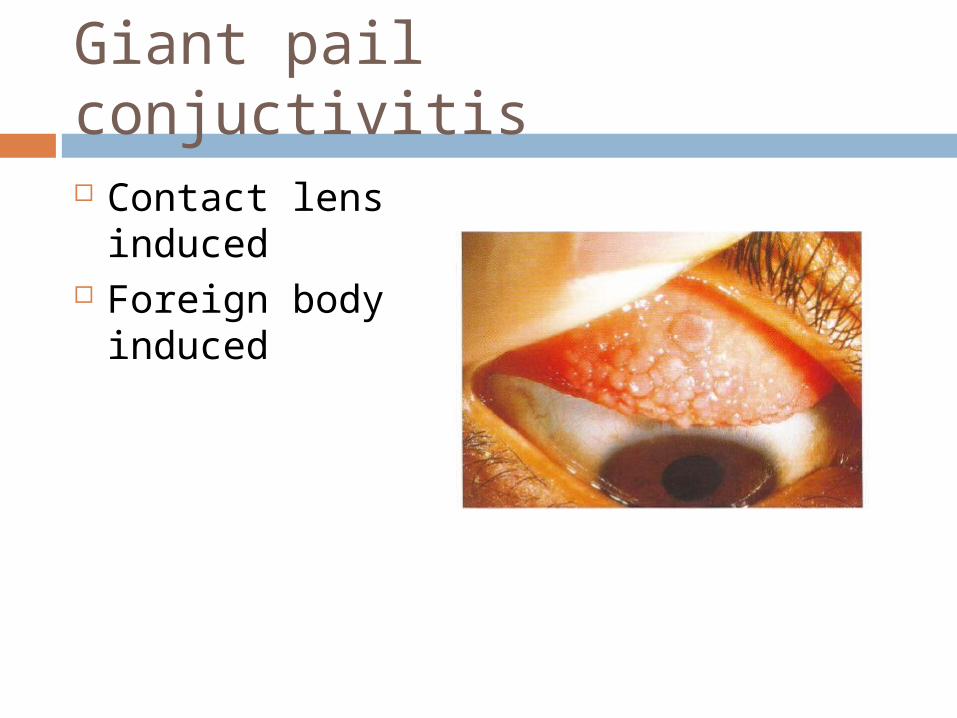
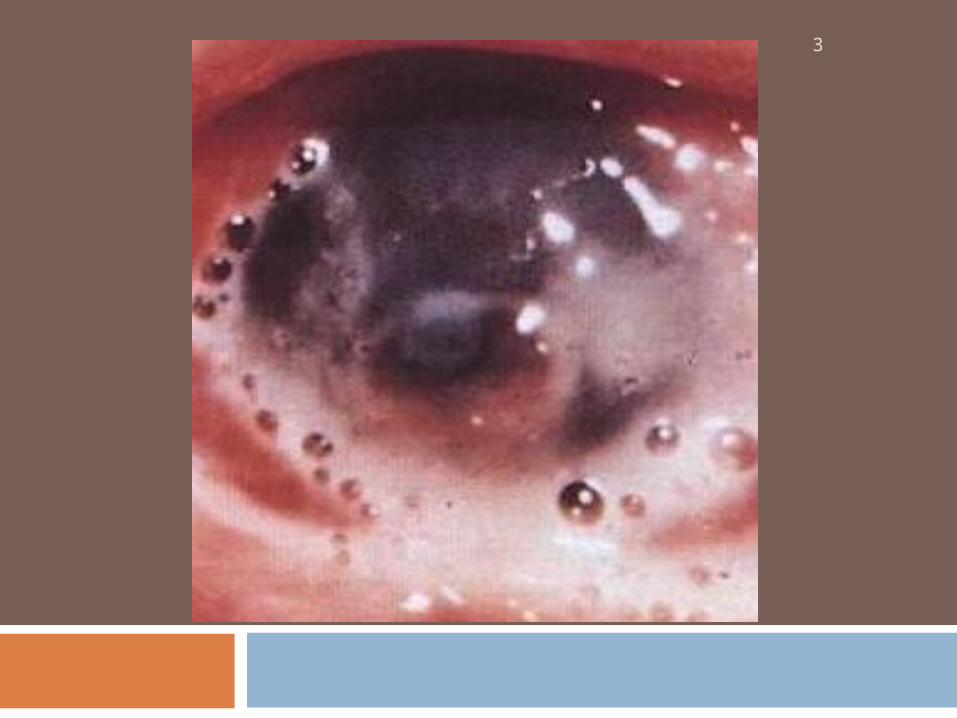
Giant pail conjuctivitis
Contact lens induced
Foreign body induced
3
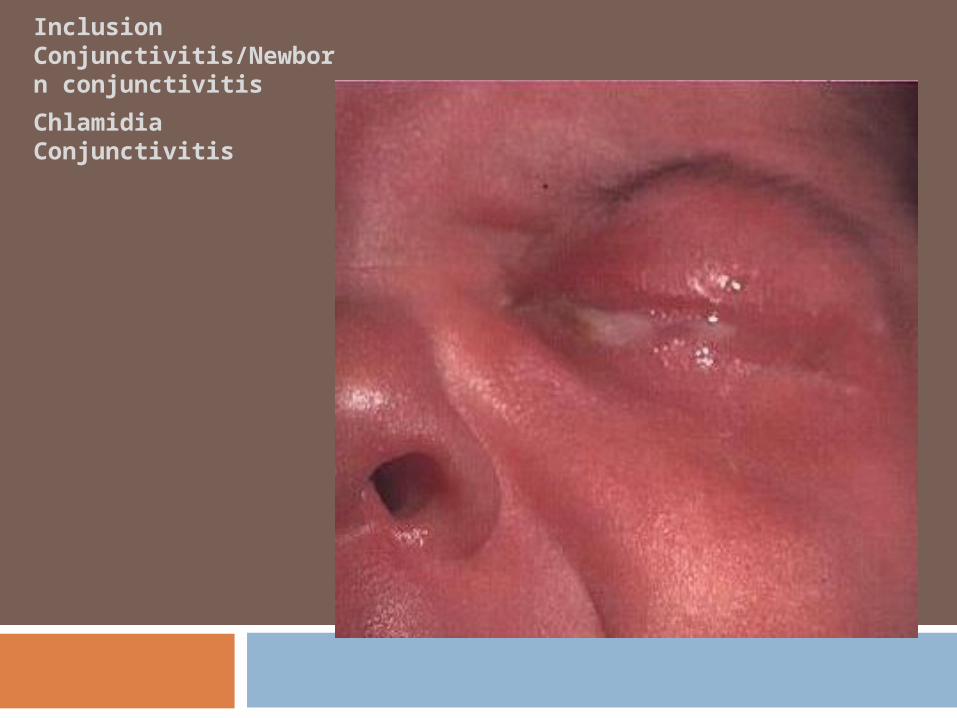
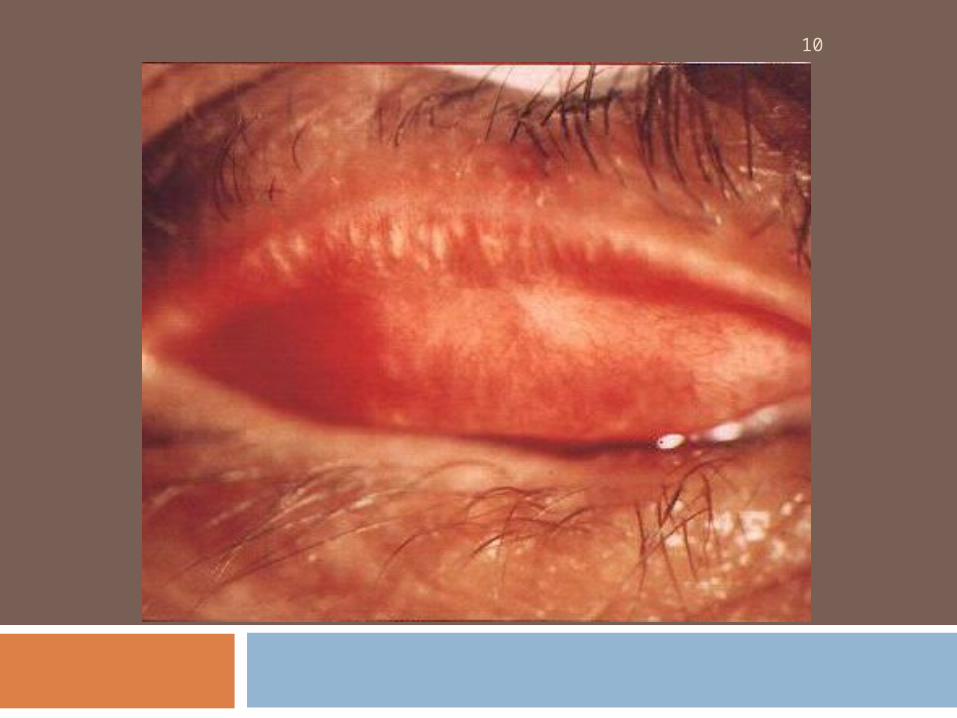
Inclusion Conjunctivitis/Newborn conjunctivitis
Chlamidia Conjunctivitis
10
Treatment oral: Tetrasiklin / doksisiklin /
eritromisin Eyedrops / Ointment : Sulfonamid /
tetrasiklin / eritromisin / ripampisin.
Prognosis: Depends on efficiency, adequacy,
immediate theraphy good prognosis
DEGENERATIVE DISEASES OF CONJUNCTIVA
PINGECUELA Harmless grayish yellow thickening of the
conjunctival epithelium in the palpebral fissure.
The harmless thickening of the conjunctiva is due to hyaline degeneration of the subepithelial collagen tissue.
Advanced age and exposure to sun, wind, and dust foster the occurrence of the disorder.
Treatment: No treatment is necessary.
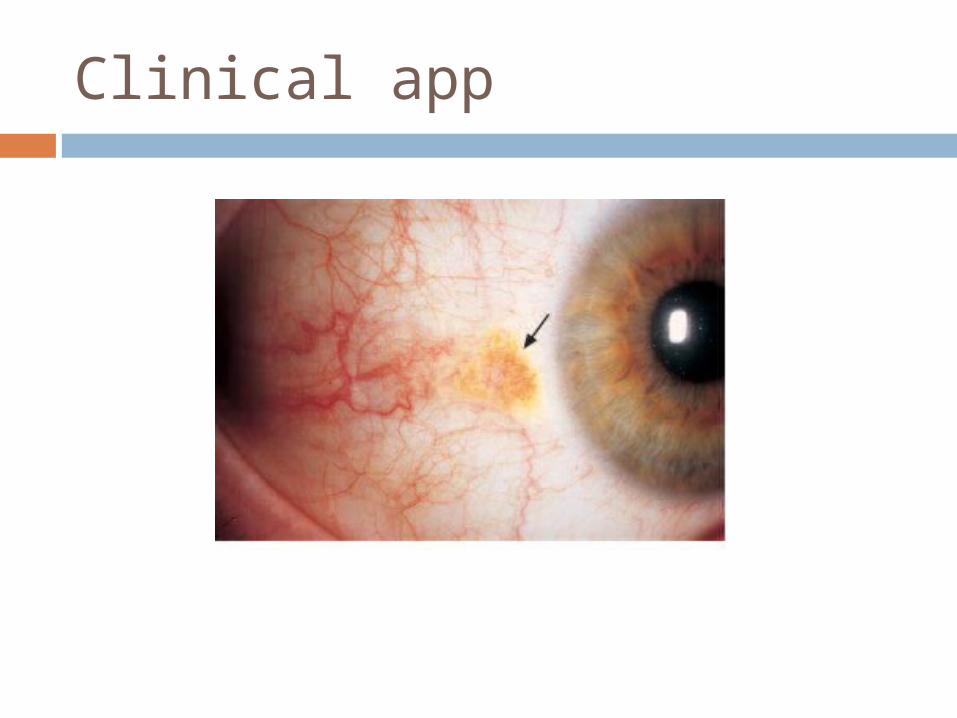
Clinical app
PTERYGIUM Triangular fold of conjunctiva that
usually grows from the medial portion of the palpebral fissure toward the cornea.
Epidemiology: Pterygium is especially prevalent in southern countries due to increased exposure to intense sunlight.
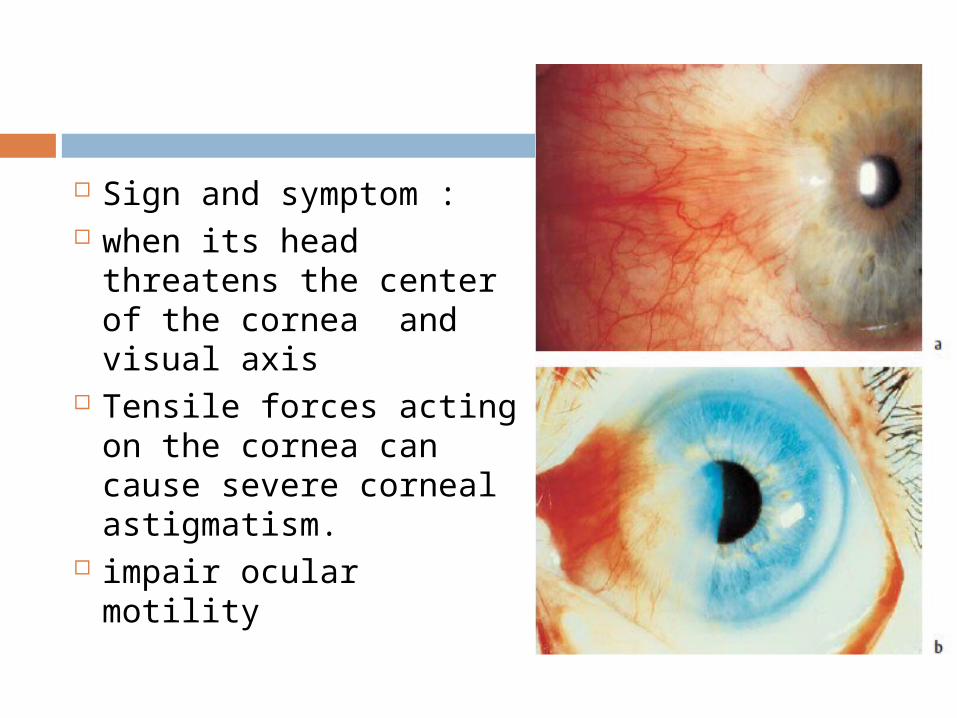
Sign and symptom : when its head
threatens the center of the cornea and visual axis
Tensile forces acting on the cornea can cause severe corneal astigmatism.
impair ocular motility
Treatment : Surgical exision
SCLERITIS
Diffuse or localized inflammation of the sclera
Classification :
According to location:
Anterior (inflammation anterior to the equator of the globe).
Posterior (inflammation posterior to the equator of the globe).
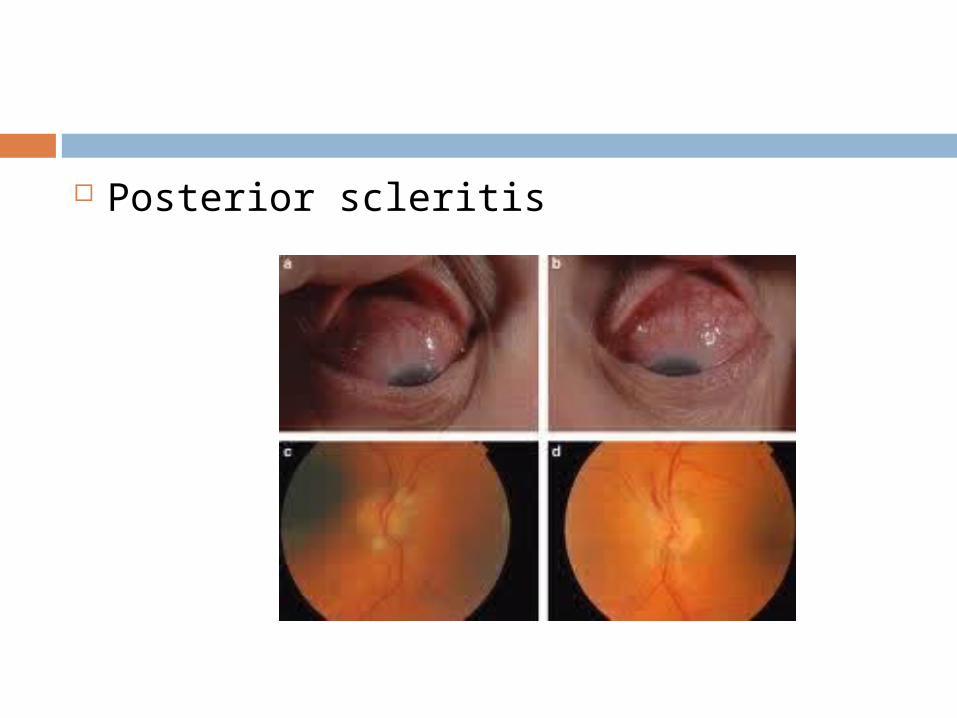
Posterior scleritis
Anterior scleritis classified according to its nature:
Non-necrotizing anterior scleritis (nodular or diffuse).
Necrotizing anterior scleritis (with or without inflammation).
Etiology: Approximately 50% of scleritis cases (which tend to have severe clinical courses) are attributable to systemic autoimmune or rheumatic disease
Sign and symptoms
Unilateral or bilateral reddening Focal/diffuse redness Slight tenderness on palpation, pain on
eye movement (esp. episcleritis) Severe pain on Scleritis (except
scleromalacia perforans)

Diffuse non necrotizing scleritis
Marked thickening andedema of thesclera and deep,diffuse reddening of sclera
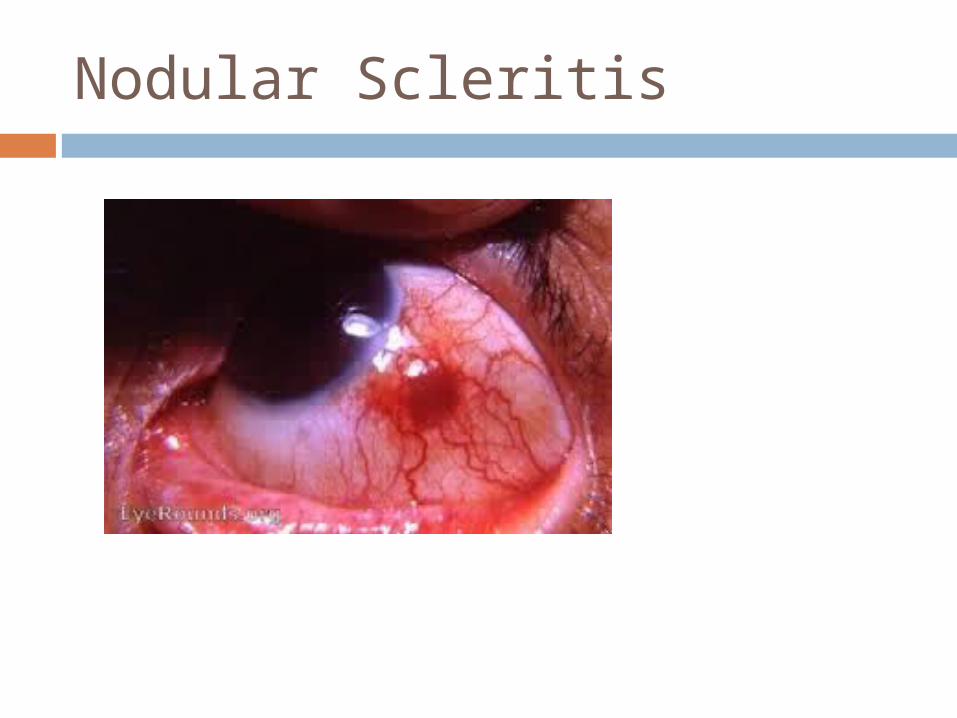
Nodular Scleritis
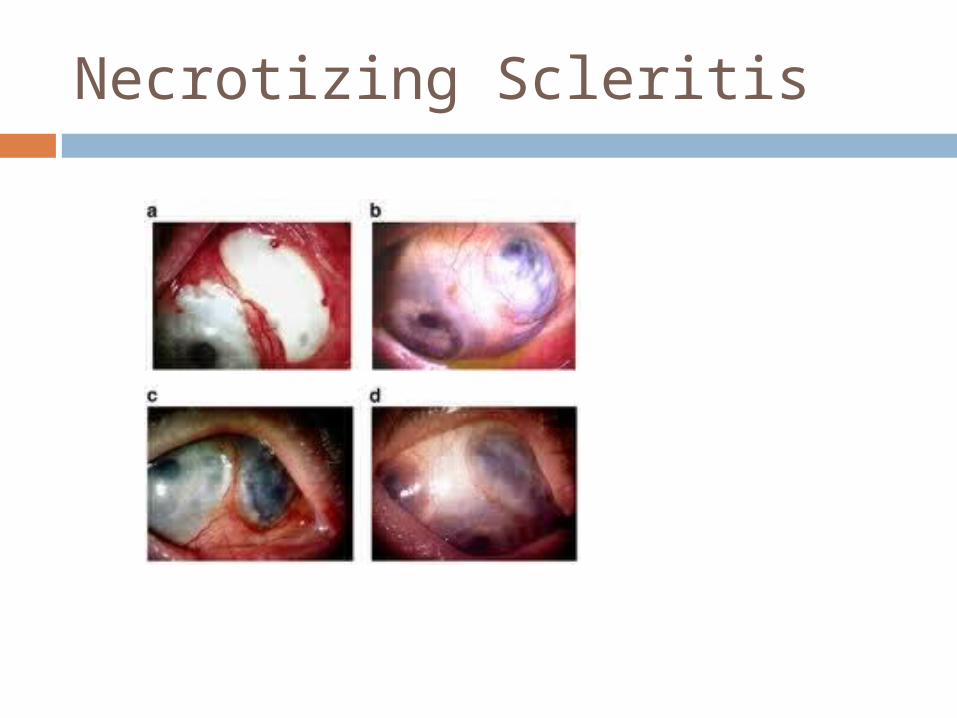
Necrotizing Scleritis
Episcleritis Circumscribed, usually segmental, and
generally nodular inflammation of the episclera (connective tissue between sclera and conjunctiva).
Epidemiology: Episcleritis is the most commonform of scleral inflammation.
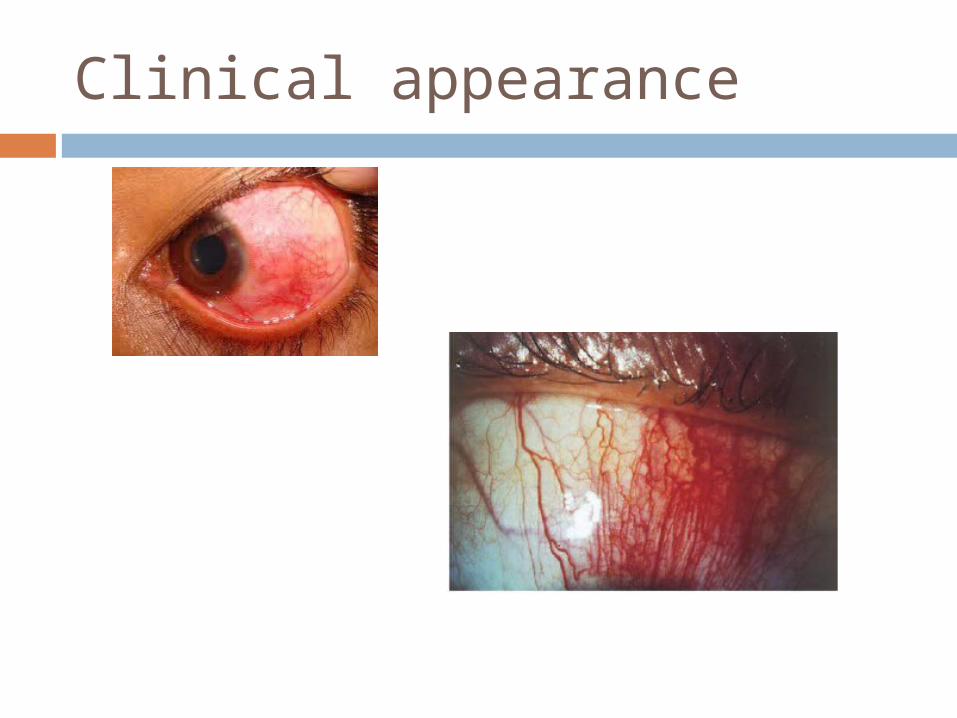
Clinical appearance
Treatment : Topical NSAID Systemic NSAID to control pain Graft/ patch for threatening perforation
Prognosis : Episcleritis Self limiting, recurrent Scleritis recurrence high, perforation
Terima Kasih