Embed Size (px)
Citation preview

3/25/2021
1
Cervical Ripening
Section II
Topics to be covered
•Definition of Cervical Ripening
•Review the pharmacological properties of prostaglandins
•Compare/contrast methods used for cervical ripening
•Explain the procedures for administration of prostaglandins
•Describe nursing role assessments and interventions with cervical ripening/prostaglandins
1
2

3/25/2021
2
Process of affecting physical softening, thinning and dilating of the cervix in
preparation for labor and birth
Indications for Prostaglandins
• Ripening an unfavorable cervix
• Has been used for induction
• IUFD
• Will not be covered in this class
• Treatment of postpartum hemorrhage
3
4

3/25/2021
3
• Score of 6 or less
• Unfavorable cervix
• Score over 8
• Favorable cervix, Induction likely to be successful
• Approaches success rate of spontaneous labor
5
6
3/25/2021
4
Cervical Ripening Agents
Mechanical and Other
Methods of Ripening
• Membrane Stripping
• Amniotomy
• Transcervical Balloon Catheters
• Hygroscopic/Osmotic Dilators
• Laminaria (seaweed)
• Lamicel and Dilapan
• Nipple Stimulation
• Sexual Intercourse
7
8
3/25/2021
5
Let’s review handout:Mechanical methods and other methodsof Ripening andLabor induction
Demonstration on inserting Ripening balloon catheter
9
10

3/25/2021
6
11
12

3/25/2021
7
13
14
3/25/2021
8
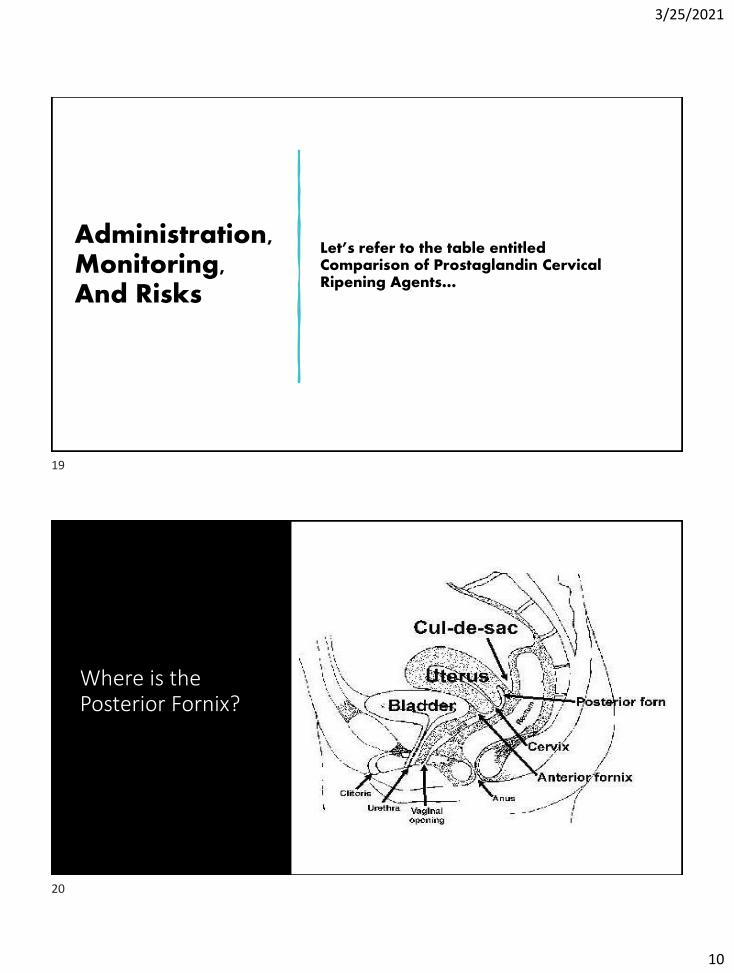
•PGE1 (misoprostol) Cytotec
Prostaglandin Cervical Ripening Agents
PGE2 (Dinoprostone)
Cervidil (insert) FDA approved
15
16

3/25/2021
9
How Do Prostaglandins
Work?
•Soften the cervix and relax cervical smooth muscle
•May also produce uterine contractions• Increase Inflammatory mediators in the cervix
•Remodel the cervical extracellular matrix through a decrease in collagen and cervical glycosaminoglycans
Chiossi et al (2012)
Misoprostol
• Routes of administration
• Oral Is starting to be used more for cervical ripening/induction
• Sublingual
• Buccal
• Intravaginal
• Currently being used for cervical ripening/induction
• Rectal
• Currently being used to treat postpartum hemorrhage
• 800-1000mcg
17
18
3/25/2021
10
Administration, Monitoring, And Risks
Let’s refer to the table entitled Comparison of Prostaglandin Cervical Ripening Agents…
Where is the Posterior Fornix?
19
20

3/25/2021
11
Misoprostol: Oral Versus Intravaginal
Route Onset Peak Half-Life Duration
Oral 8 to 11 minutes 30 minutes 90 minutes 2 hours
Intravaginal 20 minutes 1 to 2 hours 4 hours; 4 to 6 hours in some women
Simpson, K. R. (2020)
•Misoprostol should not be used for cervical ripening or labor induction in patients at term who have had a cesarean delivery or major uterine surgery.
•ACOG, 2019
•Contraindication
ACOG, 2019
21
22

3/25/2021
12
Prostaglandin Ripening:
Nursing Care*
• Monitor for Maternal/Fetal response
• Fetal Heart Rate
• Maternal comfort/discomfort
• Monitor for Contraction Activity
• Main side effect is tachysystole with or without fetal heart rate changes
• Monitor for Labor Progress
Contraction Activity
• In addition to contraction frequency, don’t forget
• Duration
• Intensity
• Resting tone
• Relaxation time
23
24

3/25/2021
13
AWHONN Staffing Recommendations
• Women receiving pharmacologic agents for cervical ripening such as Cervidil or Cytotec require continuous electronic fetal monitoring and a minimum of 1 nurse to 2 women with assessment of maternal-fetal status at least every 30 minutes
AWHONN (2010, p.18); Simpson (2020, p.s8)
Nursing Care: Fetal Response
• Assess fetal heart rate using continuous electronic fetal monitoring
• Observe for evolving patterns over time
• FHR Patterns Associated With Acidemia
• Be on the watch for these patterns
• Absent variability with recurrent late decelerations
• Absent variability with recurrent variable decelerations
• Absent variability with fetal bradycardia
25
26
3/25/2021
14
Interventions for Uterine
Tachysystole and/or Fetal
Heart Rate Concerns
Related to Prostaglandins
•Reposition
•Assess hydration status and consider IV fluid bolus
•Consider Terbutaline (Brethine) based on fetal response
• 0.25 mg SQ
• If cervidil is in place, remove it
•Notify provider based upon maternal/fetal response
Oxygen for Intrauterine
Resuscitation????
27
28
3/25/2021
15
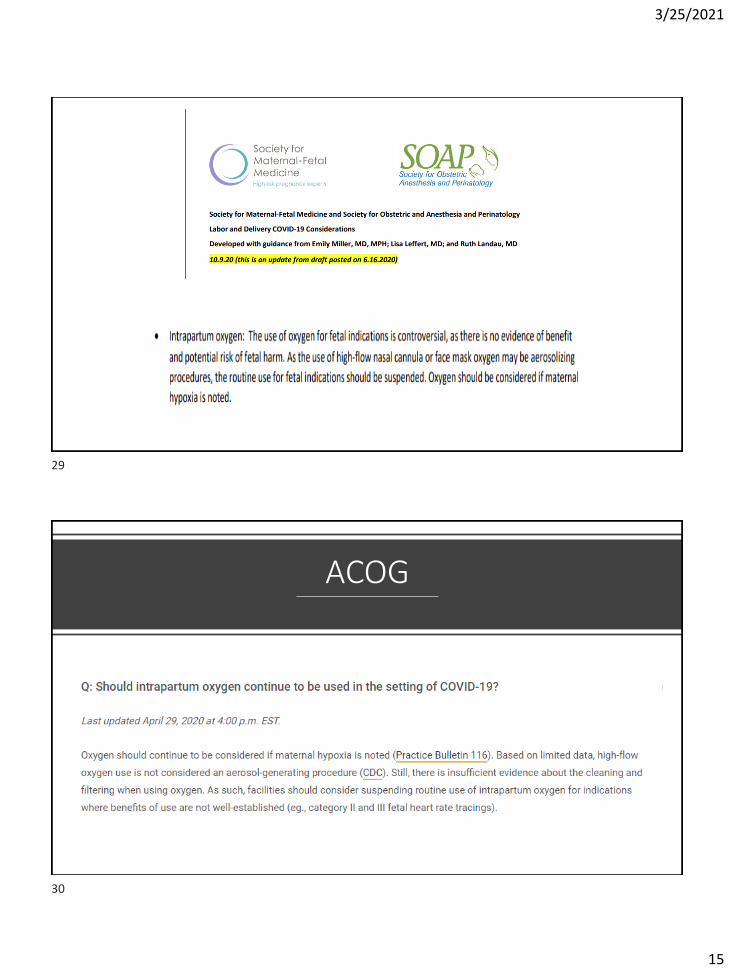
ACOG
29
30
3/25/2021
16
ARRIVE Trial
• Multicenter unmasked trial
• Randomly assigned low-risk nulliparous women who were at 38 weeks 0 days to 38 weeks 6 days of gestation to either
• Labor induction at 39 0/7 weeks to 39 4/7 weeks, or to
• Expectant management
• Women were asked to fore go elective delivery before 40 weeks 5 days and to have delivery initiated no later than
42 2/7 weeks
Arrive Trial
• Primary outcome
• Perinatal death or severe neonatal complications
• Secondary outcome
• Cesarean delivery
31
32

3/25/2021
17
Arrive Trial Conclusions
• Compared to expectant management, induction of labor at 39 weeks in low-risk nulliparous women
• Did NOT result in a significantly lower frequency of composite adverse perinatal outcomes
• It DID result in a significantly lower frequency of cesarean delivery
Society for Maternal Fetal MedicineSMFM
33
34
3/25/2021
18
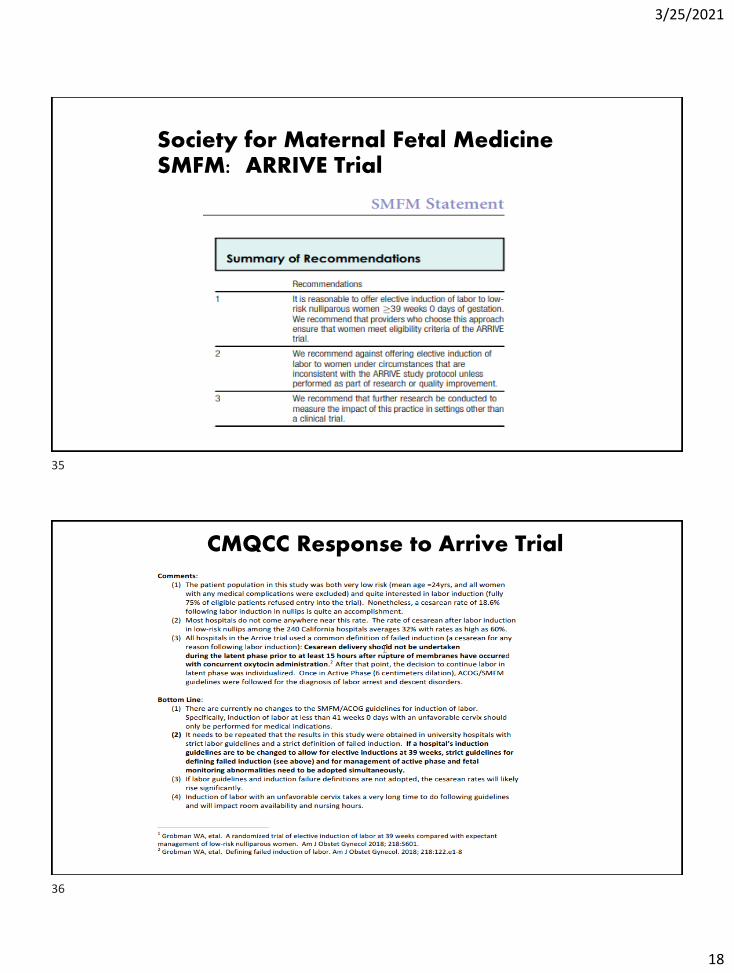
Society for Maternal Fetal MedicineSMFM: ARRIVE Trial
CMQCC Response to Arrive Trial
35
36

3/25/2021
19
Questions?
Case Study
37
38

3/25/2021
20
References
• Abrão, K. C., Francisco, R. P. V., Miyadahira, S., Cicarelli, D. D., & Zugaib, M. (2009). Elevation of uterine basal tone and fetal heart rate abnormalities after labor analgesia: A randomized controlled trial. Obstetrics & Gynecology, 113(1), 41-47.
• American Academy of Pediatrics & American College of Obstetricians and Gynecologists (2017). Guidelines for Perinatal Care, 8th edition. Elk Grove, IL: American Academy of Pediatrics.
• American College of Obstetricians and Gynecologists (2019). Medically indicated late-preterm and early-term deliveries. ACOG Committee Opinion Number 764, January 24, 2019. Washington, DC: ACOG.
• American College of Obstetricians and Gynecologists (2019). Avoidance of nonmedically indicated early-term deliveries and associated neonatal morbidities. ACOG Committee Opinion Number 765, January 24, 2019. Washington, DC: ACOG
• American College of Obstetricians and Gynecologists (2019). Vaginal birth after cesarean delivery. ACOG Practice Bulletin Number 205. Washington, DC: ACO
• American College of Obstetricians and Gynecologists (2013a; reaffirmed 2019). Definition of Term Pregnancy. ACOG Committee Opinion Number 579. November 2013.
39
40

3/25/2021
21
ACOG & SMFM Consensus Statement
• http://www.acog.org/Resources_And_Publications/Obstetric_Care_Consensus_Series/Safe_Prevention_of_the_Primary_Cesarean_Delivery
• American College of Obstetricians and Gynecologists & Society for Maternal-Fetal Medicine (2014; reaffirmed 2016). Obstetric Care Consensus Safe Prevention of the Primary Cesarean Delivery. Number 1. March 2014.
References
• American College of Obstetricians and Gynecologists (2014). revitalize: Obstetric data definitions (version 1.0). Retrieved from https://www.acog.org/-/media/project/acog/acogorg/files/pdfs/publications/revitalize-ob.pdf?la=en&hash=D9ECE1577C2A0B535F42C1B8DC492070
41
42
3/25/2021
22
• American College of Obstetricians and Gynecologists (2009; reaffirmed 2019). Induction of labor. ACOG Practice Bulletin Number 107. Washington, DC: ACOG.
• American College of Obstetricians and Gynecologists (2009; reaffirmed 2019). Intrapartum fetal heart rate monitoring: Nomenclature, interpretation, and general management principles. ACOG Practice Bulletin Number 106, Washington, DC: ACOG.
• Association of Women’s Health, Obstetric and Neonatal Nurses (2019). Position Statement: Elective Induction of Labor. Washington, DC: AWHONN.
• Association of Women’s Health, Obstetric and Neonatal Nurses (2018). Fetal heart monitoring. Washington, DC: AWHONN.
• Association of Women’s Health, Obstetric and Neonatal Nurses (2015). Fetal Heart Monitoring Principles and Practices, 5th ed. Washington, DC: AWHONN
43
44

3/25/2021
23
• Association of Women’s Health, Obstetric and Neonatal Nurses (2010). Guidelines for Professional Registered Nurse Staffing for Perinatal Units. Washington, DC: AWHONN.
• Caldeyro-Barcia, & Poseiro, J. J. (1960). Physiology of the uterine contraction. Clinic Obstetr Gynecology, 3: 386-408.
• Chiossi, G., Costantine, M. M., Bytautiene, E., Kechichian, T., Hankins, G. D. V. et al. (2012). The effects of prostaglandin E1 and Prostaglandin E2 on in vitro myometrial contractility and uterine structure. American Journal of Perinatology, 29, 615-622
• Clark, S., Belfort, M., Saade, G., Hankins, G., Miller, D., & Frye, D. (2007). Implementation of a conservative oxytocin-based protocol for oxytocin administration: maternal and newborn outcomes. American Journal of Obstetrics & Gynecology, 197: 480.e1-480.e5.
• Clark, S. L., Simpson, K. R., Knox, E., & Garite, T. J. (2009). Oxytocin: new perspectives on an old drug. American Journal of Obstetrics & Gynecology, 200: 35.e1-35.e6.
45
46
3/25/2021
24
• Dudley, D. J. (1997). Oxytocin: Use and abuse, science and art. Clinical Obstetrics and Gynecology, 40(3), 516-524.
• Freeman, R. K., Garite, T. J., Nageotte, M. P., & Miller, L. A. (2012). Fetal Heart Rate Monitoring, 4th edition. Philadelphia: Wolters Kluwer/Lippincott Williams & Wilkins.
• Gard, J. W., Alexander, J. M., Bawdon, R. E., & Albrect, J. T. (2002). Oxytocin preparation stability in several common obstetric intravenous solutions. American Journal of Obstetrics & Gynecology, 186, 496-498.
• Garite, T. J., & Simpson, K. R. (2011). Intrauterine resuscitation. Clinical Obstetrics and Gynecology, 54(1), 28-39.
• Grobman, W. A., et al (2018). Defining failed induction of labor, American Journal of Obstetrics & Gynecology, 218(1), 122e1-122e8.
• Grobman, W. A., et al (2018). Labor induction compared with expectant management of low-risk nulliparous women. The New England Journal of Medicine, 379(6), pp. 513-523.
• Harper, L. M., Caughey, A. B., Odibo, A. O., Roehl, K. A., Zhao, Q., & Cahill, A. G. (2012). Normal progress of induced labor. Obstetrics & Gynecology, 119(6), 1113-1118.
47
48

3/25/2021
25
• Institute for Safe Medication Practices. https://www.ismp.org/recommendations/high-alert-medications-acute-list.
• Miller, L. A., & Miller, D. A., & Cypher, R. L. (2017). Fetal Monitoring A Multidisciplinary Approach, 8th ed. St. Louis: Elsevier/Mosby.
• Robinson, C., Schumann, R., Zhang, P., & Young, R. C. (2003). Oxytocin-induced desensitization of the oxytocin receptor. American Journal of Obstetrics & Gynecology, 188, 497-502.
• Society of Maternal-Fetal (SMFM) Publications Committee (2019). SMFM statement on elective induction of labor in low-risk nulliparous women at term: the ARRIVE trial. www.smfm.org
• Society for Maternal-Fetal Medicine; Bernstein, P. S., Combs, C. A., Shields, L. E., Clark, S. L., Eppes, C. S.; and the SMFM Patient Safety and Quality Committee (2017). The development and implementation of checklists in obstetrics. www.smfm.org
• Simpson, K. R. (2020). Cervical ripening and labor induction and augmentation, 5th edition. Washington, D.C.: AWHONN.
49
50

3/25/2021
26
• Spong, C. Y, (2013). Defining “Term” Pregnancy: Recommendations From the Defining “Term” Pregnancy Workgroup. JAMA 309(23), 2445-2446.
• Wen, T., Beceiro, A., Conway, D., & Piper, J. (2001). Is there a maximum effective dose of pitocin? American Journal of Obstetrics & Gynecology, 185(6), Supplement December, page S212.
51