-
8/7/2019 Sentinel Node Biopsy in Melanoma
1/12
Volume 22 Number 1 2008
Sentinel Lymph Node Biopsy inMelanoma in 2008
J. M. Thomas, M.S., F.R.C.P., F.R.C.S., and A. J. Hayes, M.A.,
F.R.C.S., Ph.D.
Intdctin
Sentinel lymph node biopsy (SLNB) in melanoma has been
intensively investigatedand, apart rom the nal results o the
Multicenter Selective Lymphadenectomy Trial
(MSLT-1)1 and a ew other renements, sucient inormation is
available to cometo an initial consensus about the value o this
investigation and its consequences.
Nevertheless, it is dicult to think o a surgical procedure or a
therapy that hasgiven rise to such a wide spectrum o opinion
despite the act that all parties areinterpreting the same data. The
dominant opinion is that SLNB in melanoma shouldbe regarded as
standard o care, which implies that patients not oered the
pro-cedure are being disadvantaged in some way. It has even been
suggested that notoering patients the opportunity or SLNB may have
medicolegal consequences.2Although detractors o the procedure are
in a minority, some have argued thatSLNB is o no benet and should
be abandoned.37
The results o MSLT-1 were rst presented at the meeting in Los
Angeles in Decem-ber o 2004 and were ormally announced at the
American Society o Clinical On-cology (ASCO) in May o 2005,8 but
were not published until September o 2006.1Until these results were
known, it was not unreasonable to regard SLNB as the latestand best
orm o innovative care, especially in view o the prognostic
importance o
sentinel node (SN) status. Furthermore, particularly in the
United States and Austra-lia, the SLNB procedure replaced elective
lymph node dissection (ELND). Results o
CANCERPrinciples & Practice
of Oncology
Vincent T. DeVita, Jr.
Samuel Hellman
Steven A. Rosenberg
7th Edition
Authors:
J. M. Thomas, M.S., F.R.C.P., F.R.C.S., andA. J. Hayes. M.A.,
F.R.C.S., Ph.D., Sarcoma and Melanoma Unit,
Department o Academic Surgery, Royal Marsden Hospital, London,
England.
The opinions and/or clinical experiences outlined herein are
those o the authors and do not necessarily
represent the views o the editors or publisher.
-
8/7/2019 Sentinel Node Biopsy in Melanoma
2/12
Sentinel lymph nodeBiopSyin melanoma Volume, numBer 1
our randomized controlled trials o ELND were showing no
over-
all survival (OS) advantage,912 but o greater concern was thatno
deposits o melanoma were present in approximately 80% othe ELND
specimens, meaning that these patients were undergo-ing excessive
and unnecessary surgery which was associated withsignicant surgical
morbidity, especially chronic lymphedema. Theimmediate attraction o
the SLNB procedure was that it selectedpatients or ELND (or
completion/early/immediate lymphadenec-tomy as it became known)
based on the presence or absence omelanoma deposits in the SN.
Subsequently, the identication otiny deposits o melanoma within the
SN by immunohistochem-istry (IHC)13 that could not be identied by
conventional stainingtechniques ueled urther interest and
ascination in the proce-dure. It is or these perectly logical and
intuitive reasons that theSLNB procedure became standard o care
beore ull evaluationhad been completed.
Over the past decade or so, the SLNB has dominated clinical
practice and research in melanoma. Sucient inormation andoutcome
data are now available to allow a more critical analysiso the
procedure with a view to renement o clinical practice.
A re-evaluation o the procedure is justied i only because
theresults o MSLT-1 do not even show a trend toward an OS
advan-tage. Our responsibility as physicians is to provide patients
withaccurate inormation on which to base their decisions. We
believethat the arguments presented in this review are
evidence-basedand deserve careul consideration.
A Fawk f Assssing th us f SlNb inmana
The theoretical basis underpinning the purported value o SLNBand
subsequent completion lymphadenectomy in SN-positive cas-es can be
summarized by the ollowing three points.
1. Prognostic inormation. Knowing the status o the SN
providesprognostic inormation over and above that which is
providedby the histologic characteristics o the resected primary
tumor.This allows a more accurate stratication o a patients risk
orrelapse at distant sites, or the purposes o adjuvant treatment,or
or entry into trials o adjuvant therapy. I there is no eec-tive
adjuvant treatment, then the only possible benet o theprognostic
inormation is in lessening, but not eradicating, pa-tients
uncertainty as to whether their disease will recur.
2. Therapeutic benet resulting rom surgical resection.
Comple-tion lymphadenectomy in SN-positive patients may have
anintrinsic therapeutic benet by removing LNs containing malig-nant
cells when they are not apparent clinically or by standard
radiologic techniques. Inevitably this will infuence the
patterno disease recurrence, but to achieve a therapeutic
advantage,early lymphadenectomy must be shown to reduce the
inci-dence o systemic spread.
3. Potential detrimental eects o surgery. The two potential
ben-ets o SLNB must be evaluated in the context o
morbiditiesassociated with the procedure. There is a small but
signicantmorbidity o the procedure itsel. O greater concern (see
be-low) is that a proportion o patients will undergo
unnecessary
completion lymphadenectomy as a result o prognostic alse-
positivity within the SN. There is also a lingering concern
thatcompletion lymphadenectomy in SN-positive patients may
in-crease the risk or in-transit recurrence14,1519 despite the
actthat, overall, the incidence o in-transit disease is similar in
botharms o MSLT-1.1
We would have no objection to the SLNB procedure i it wereknown
or were likely that all SN-positive patients would prog-ress to
palpable nodal recurrence. The operations o immediateand delayed
lymphadenectomy are identical, and we know romthe results o MSLT-1
that the morbidity is similar. Our main con-cern relates to
prognostic alse-positivity, meaning that some tinydeposits o
melanoma in the SN are destined or destruction ordormancy rather
than progression. Furthermore, i the evidencesuggests that SLNB
serves only as a prognostic tool or risk strati-cation, then the
question must be asked as to how superior thatprognostic inormation
is over detailed histologic assessment o
the primary tumor and ultrasound o the SN basins. In the
ab-sence o adjuvant treatments, is there any benet to the patientin
having imperect prognostic inormation?
Based on these comments, this review is structured as ollows:
(a)evidence or therapeutic benet or SLNB and immediate
lymph-adenectomy; (b) the role o SLNB as a prognostic tool; (c)
theevidence or prognostic alse-positivity within positive SNs,
and(d) the importance o ultrasound in screening and surveillance
oSN basins.
SlNb as a Thaptic T: mSlT-1
MSLT-1 was designed to compare the survival o SN-positive
pa-tients undergoing immediate lymphadenectomy (the biopsy arm)with
that o patients treated by delayed lymphadenectomy when
metastatic regional nodes became palpable (the observation
arm).
To achieve this primary end point, the trial entered and
random-ized 2001 patients,20 but the published results relating to
survivaldescribed only a subgroup o 1269 patients with tumors o
inter-mediate thickness (1.2 to 3.5 mm).1 No survival inormation or
pri-mary tumor-related details have been published about the 732
pa-tients with tumors thinner than 1.2 mm or thicker than 3.5
mm.
Summary of Trial Design and ResultsForty percent o patients were
randomized to the observation armand, according to the protocol,
were treated by wide local exci-sion (WLE) o the primary tumor and
delayed lymphadenectomywhen the regional LNs became palpable. Sixty
percent o patientswere randomized to the biopsy arm and ater WLE
were investi-gated by SLNB. Immediate lymphadenectomy was perormed
i
any SNs contained metastatic melanoma (SN-positive). The
resultsshowed no dierence in OS (87.1% biopsy arm vs. 86.6%
obser-vation arm) and a 5% dierence at 5 years in disease-ree
survival(DFS) in avor o the biopsy arm (78.3% vs.73.1%). The
abstractconclusion conrmed the prognostic value o SN status. A
post-randomization subgroup analysis claimed a 20% survival
advan-tage when the 122 SN-positive patients in the biopsy arm,
whounderwent immediate lymphadenectomy, were compared to the78
patients in the observation arm, who were treated by
delayedlymphadenectomy1 (Fig. 1).
Published by Wolters Kluwer Health, Inc., 333 Seventh Avenue,
19th Floor, New York, NY 10001. Fax (212) 886-1205. Copyright 2008
Lippincott
Williams & Wilkins. Printed in the U.S.A. All rights
reserved. Reproduction without specifc permission is prohibited.
ISSN 0892-0567.
-
8/7/2019 Sentinel Node Biopsy in Melanoma
3/12
Volume, numBer 1 thomaSand hayeS
Is There a Subgroup Survival Advantage?The claim o a 20%
survival advantage or immediate lymph-adenectomy in the abstract
conclusion1 is based on a subgroupanalysis and is in stark contrast
to the absence o any melanoma-specic survival advantage at the
point o randomization. Becausethe subgroup analysis result is at
such odds with the primary endpoint, this result must be
scrutinized to determine i the compari-son is valid.
Subgroup analyses within a randomized trial are valid only i
thesubgroup is identied beore randomization such that the
char-acteristic that denes the subgroups is randomly
allocated.21These two subgroups were not dened beore the
randomiza-tion. Rather, they are post-randomization selected
subgroups andthe patients in each subgroup were identied by the
procedureunder investigation. Within a randomized controlled trial,
a de-nitive survival comparison between post-randomization
selectedsubgroups is not valid.
The rationale or making the comparison between these
twononrandomized subgroups is based entirely on the assumption
that all patients with positive SNs will inevitably progress to
pal-pable nodal disease and that these two subgroups are
prog-nostically equivalent. As will be shown later, multiple
sources
o indirect and direct evidence now indicate that some
positiveSNs are not destined to progress to palpable nodal
recurrence.Hence the two subgroups are notprognostically
equivalent, andthe 20% survival dierence is not the result o any
therapeuticadvantage rom immediate lymphadenectomy. The reporting
oan invalid subgroup analysis has served only to cloud what is
avery clear conclusion o the primary end point o this large
trial,i.e., that there is at present no evidence that SLNB oers an
OSbenet to patients.
Disease-Free Survival
The 5% advantage in DFS at 5 years means that 100 patientsmust
undergo SLNB or ve patients in the biopsy arm to havea DFS
advantage. In the absence o any dierence in OS, thiscould simply
mean a delay rather than a prevention o recur-rence. In MSLT-1, the
site and timing o rst recurrence were
directly infuenced by the SLNB procedure itsel. In patients
with
melanoma o intermediate thickness, the most likely site o
rst
recurrence is the regional LNs. Patients in the biopsy arm
whowere SN-positive underwent a prophylactic lymphadenectomyat the
time o diagnosis, and thereore these patients will inevi-tably have
ewer regional nodal recurrences. This is conrmedin the results
relating to site o rst recurrence, which show athreeold increase in
nodal recurrence in the observation armand a small increase in
distant recurrence in the biopsy arm(11% vs. 7%). In this cohort o
patients, moreover, regionalnodal recurrences invariably appear
beore distant recurrences.For these reasons, an apparent advantage
in DFS in avor o thebiopsy arm is almost inevitable. To overcome
bias caused by trialdesign, regional nodal recurrences should be
excluded rom thecalculation o DFS. MSLT-1 was unded by the National
CancerInstitute, and an appeal on this matter has now been upheldby
its Clinical Investigations Branch (personal communication toJMT).
In the uture, DFS in MSLT-1/2 will also be calculated onthe
competing incidences o local/in-transit and distant recur-
rences alone.
Differing Practices Among MSLT-1 Centers
Another issue that makes the interpretation o MSLT-1 even
moredicult is diering ollow-up practices among participating
units.In all publications relating to MSLT-1, as well as in the
accom-panying editorial,22 it has been stated or assumed that
delayedlymphadenectomy in the observation arm was perormed
whenmetastatic nodes became palpable. That is not the case.
Almosthal o the patients entered into MSLT-1 (946 o 2001) were
romthe Sydney Melanoma Unit. It now transpires that the 378 orso
patients entered into the observation arm were investigatedby
lymphoscintigraphy at the time o WLE o the primary tumorwhen the
site o the SN was marked by a small permanent tat-too to acilitate
regular interrogation by ultrasound.23 Delayedlymphadenectomy was
perormed not when the regional nodal
metastases became palpable but when nonpalpable metastases
were identied by ultrasound and the diagnosis proven by
ul-trasound-guided cytology. In the same publication, the
authorsconrmed that ultrasound could identiy metastatic deposits
omelanoma in the SN at 4-mm diameter in the groin and neck
and4.5-mm diameter in the axilla. It is not known how many monthsit
would take or such occult deposits to become palpable, butthis
practice directly aected and compromised the primary endpoint o
MSLT-1, i.e., OS dierence rom the point o randomiza-tion. This
inormation was not mentioned in the New EnglandJournal o Medicine
article.1
Unanswered Questions Relating to MSLT-1Several questions
relating to MSLT-1 remain unanswered. Whywere 732 patients omitted
rom the rst publication o the re-
sults, contrary to CONSORT guidelines?I these 732 patients
hadbeen included, how would this have aected the DFS as
calcu-lated? I DFS was recalculated, as is now endorsed by
NationalCancer Institute, would the small DFS advantage in avor o
thebiopsy arm be maintained, lost, or reversed?
Have the results o MSLT-1 been invalidated by the
anomalousmanagement at the Sydney Melanoma Unit? The core
assump-tion that all positive SNs, i not removed, will eventually
progressto palpable nodal recurrence is challenged by the
hypothesis oprognostic alse-positivity. Does this prognostic
dierence not ex-plain the 20% survival advantage in avor o
immediate lymphad-enectomy claimed in the subgroup analysis?
FIG. 1. Trial design and treatment o patients with
intermediate-thickness melanoma. Based on data rom Morton et
al.1
-
8/7/2019 Sentinel Node Biopsy in Melanoma
4/12
Sentinel lymph nodeBiopSyin melanoma Volume, numBer 1
Sntin lyph Nd Stats as a Staging andPgnstic T
Sentinel lymph node (LN) status at the time o diagnosis o
theprimary tumor is the most important single prognostic actor
inmelanoma.2427 It has been shown repeatedly that the
disease-specic survival is signicantly better in SN-negative
patients com-pared to SN-positive patients (approximately 95% vs.
70% at 3
years) and that SN-positivity predicts or distant spread and
death.Unortunately, this prognostic importance does not translate
intoa therapeutic benet because no surgical procedure or
systemictherapy has been shown to improve OS in melanoma.
Algorithmso histologic actors relating to the primary tumor have
beenshown to be almost as prognostically accurate as SN
status.28
It is noteworthy that prognostic tools are still important in
theirown right. There is still no absolute consensus worldwide
thatadjuvant therapy should not be used in melanoma despite thelack
o an OS benet. The Kirkwood adjuvant intereron regi-men suggests a
prolongation o DFS.29 Furthermore, almost allnew adjuvant trials
will wish to include SN-positive patients. The
diculty with this is that prognostically alse-positive patients
willalso be included, and in the uture there may be a consensus
thatonly patients with metastases in the SN greater than a certain
size
should be entered into trials o adjuvant therapy.
How eective is SLNB as a prognostic tool compared to inorma-tion
available rom the primary tumor and noninvasive imaging othe nodal
basins? SLNB was well established beore it was realizedthat
high-resolution ultrasound with Doppler was the best meth-od o
imaging nonpalpable occult metastatic melanoma in theregional
LNs.30 It is known that ultrasound alone can detect occultnodal
metastases in up to one-third o SN-positive
patients.23,31Experienced radiologists can identiy deposits o
melanoma assmall as 3 mm and can conrm the diagnosis by
ultrasound-guid-
ed cytology.32
Occult metastases o this diameter are also easilyidentied by
SLNB, but it has never been shown that SN statusmaintains its
staging and prognostic importance in ultrasound-negative patients.
Ultrasound is a simple noninvasive procedureand ultrasound
screening o the regional node basin(s) at the
time o diagnosis o the primary tumor may provide the
greatestchallenge to SLNB. Those who are skeptical o the importance
oultrasound may say that, like SLNB, ultrasound can only
antecedethe clinical diagnosis o metastatic melanoma. However,
there isone very important dierence. It is likely that all nodal
metasta-ses large enough to be visualized by ultrasound are
destined toprogress to palpable nodal recurrence. On the other
hand, SLNBcan detect most deposits o melanoma likely to progress
but alsoreadily identies some tiny deposits likely to be
prognostically
alse-positive and destined or dormancy or destruction.
Patterns of Melanoma Recurrence in SN-Negative
PatientsUndoubtedly, many patients undergo SLNB hoping or
reassur-ance that their SNs are ree o melanoma. However, being
SN-negative gives no guarantee o remaining recurrence-ree and,
asalways, the incidence o recurrence will increase with
prolonged
ollow-up. With reerence to publications providing a median
ol-low-up o 2 years or more, the recurrence rate at any site is o
theorder o 9.6% to 13.7%.3337 These series agree that the site orst
recurrence in SN-negative patients is distant in approximatelyhal
the patients, that isolated SN basin recurrence is uncommon,and
that the remaining sites o rst recurrence are a combination
o synchronous in-transit and SN basin recurrences. This
inor-
mation conrms that, in a small group o patients,
melanomadisseminates entirely via the bloodstream rather than via
the lym-phatic system.
Pgnstic Fas-Psitivity in th SN in mana
Prognostic (or biological) alse-positivity reers to tiny
deposits omelanoma within the SNs that are destined or dormancy or
de-struction and not or progression to palpable nodal recurrence.
38This hypothesis undamentally challenges the central tenet o
theSLNB procedure, which assumes, without any evidence, that
allpositive SNs (i not removed) will inevitably progress to
palpablenodal recurrence. Prognostic alse-positivity results in
patientsbeing incorrectly up-staged, being given inaccurate
prognosticinormation, undergoing unnecessary completion
lymphadenec-tomy, and possibly unnecessary adjuvant therapy or
entry intosuch trials. A simple mathematical model is presented
below to
estimate the incidence o prognostic alse-positivity together
withother lines o supporting evidence.
Indirect Evidence for Prognostic False-PositivityIndirect
evidence or prognostic alse positivity comes rom oursources. First,
many authors have reported that melanoma mi-crometastases below a
certain size have no adverse prognosticsignicance.35,3943 For
example, Van Akkooi et al.35 state that pa-tients with
micrometastases less than 0.1 mm in the SN shouldbe judged to be
SN-negative. Spanknebel et al.41 conclude thatpatients whose
micrometastases are detectable only by IHC havea prognosis similar
to that o patients with negative SNs. Theseobservations, however,
depend on the SN being removed or his-tologic examination, which
could be construed as contributing tothe therapeutic benet.
Second, there is an unexplained paradox in which younger
patients
with melanoma have a signicantly better prognosis than
olderpatients despite exhibiting a higher incidence o
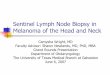
SN-positivity.44,45As shown in Fig. 2, the mortality rom melanoma
rises steeplywith advancing age, whereas the incidence o
SN-positivity re-duces with increasing decades o age. In the
absence o evidencethat melanoma spreads more commonly by the
bloodstream in
FIG. 2. Incidence o SN-positivity with increasing decades o
agecompared with melanoma-specic mortality.44,45
-
8/7/2019 Sentinel Node Biopsy in Melanoma
5/12
Volume, numBer 1 thomaSand hayeS
elderly patients, the most likely explanation is that, in
younger pa-
tients, a more competent host response can eliminate tiny
micro-metastases or induce dormancy. In a study o 3076 patients,
Chaoet al.44 showed that the incidence o SN-positivity was 23.1%
inpatients less than 30 years o age but that the incidence
declinedwith increasing decades o age to 12% in patients between
61and 70 years (P
-
8/7/2019 Sentinel Node Biopsy in Melanoma
6/12
Sentinel lymph nodeBiopSyin melanoma Volume, numBer 1
The incidence o prognostic alse-positivity will decrease as
more
patients in the observation arm develop nodal recurrence.
How-ever, because the median time to nodal recurrence in the
obser-vation arm o MSLT-1 was 16 months and the median ollow-upwas
60 months,1 it is unlikely that nodal recurrence will
increasesuciently to signicantly aect the calculated incidences
oprognostic alse-positivity. Nevertheless, i it is assumed that
nodalrecurrences in the observation arm and among alse-negative
pa-tients in the biopsy arm will increase at the same rate, then a
10%and 20% increase in palpable nodal recurrence among patientswith
intermediate-thickness tumors would reduce the incidenceo
prognostic alse-positivity to 13% and 8.4%, respectively. Itwould
take a 30% increase in nodal recurrence to reduce the inci-dence to
less than 1%. For all strata, a 10% and 20% increase innodal
recurrence would reduce the incidence o prognostic alse-positivity
to 27% and 20%, respectively, and it would take a 50%increase in
nodal recurrence to reduce prognostic alse-positivityto less than
1%.
Does RT-PCR Analysis for Tyrosinase Provide AdditionalPrognostic
Information in SN-Negative Patients?
Detection o tyrosinase mRNA by reverse transcriptase-poly-merase
chain reaction (RT-PCR) in negative SNs was intendedto identiy
SN-negative patients who were destined to recurand in the
expectation that the incidence o SN alse-negativitycould be
reduced. Unlike histology with IHC there was alwaysa risk that
molecular staging would introduce an incidence oalse-positivity
because o the eect o capsular nevus cells.Review o the literature
shows that there is no consensusabout the ability, i any, o RT-PCR
to up-stage negative SNs.Several series, including the Sunbelt
Melanoma Trial with 1446SN-negative patients, report that RT-PCR in
SN-negative pa-tients ailed to detect a subgroup o patients with an
increasedprobability o recurrence.51 At the other extreme, many
authors
report that RT-PCR can upstage 25% to 65% o histologically
negative SNs.5257
Furthermore, some o these series report aDFS dierence in
SN-negative/RT-PCR-negative patients com-pared to
SN-negative/RT-PCR positive patients.53,55,56 However,there is
agreement that SN-negative/RT-PCR-negative patientshave an
extremely low risk or recurrence at any site. Becausepatients
entered into MSLT-2 can be deemed to be SN-positiveon RT-PCR
criteria alone, it is useul to ocus on the experiencerom the John
Wayne Cancer Institute rom which this trial isdirected. Using a
multimarker RT-PCR assay55,57 the researchersdemonstrated that
histologically negative SNs were RT-PCR-positive in up to 40% o
cases. Thereore, using RT-PCR inSN-negative patients in MSLT-2 is
likely to increase prognosticalse-positivity even urther.
utasnd in th Assssnt f SN basin(s) inmana
Ultrasound screening o the SN basin(s) in search o occult
(non-palpable) metastases in melanoma is a neglected technique
and,in general, is poorly understood. Deposits o melanoma as
smallas 34 mm can be identied on the basis o morphologic crite-ria,
and pathologic neovascularization can be identied on powerDoppler
mode. The lesion can then be targeted or cytologicexamination,
which is reported to have a specicity o 100%.Ultrasound is
operator-dependent and considerable expertise
isrequired.30,58,59
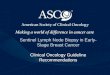
High-resolution ultrasound identies a resting inactive LN as
being
oval in shape with an echo-poor (black) cortical rim o
lymphoidtissue surrounding an echogenic hilus (gray) that
demonstrateslittle or no vascularity (Fig. 4A). This appearance has
been likenedto the pulp around the stone o a cherry. These
appearances maychange in response to inection but are reversible.
Progressivelyin melanoma, the ollowing changes occur in a
metastatic LN.The earliest sign is irregularity o the lymphoid
cortex, which mayprogress to a nodule (Fig. 4B). As the LN becomes
increasinglyinvolved with melanoma, it becomes round rather than
oval, theechogenic hilus is progressively lost, the neovascularity
intensies,and the volume o the LN expands (Fig. 4C).
FIG. 4. High-resolution ultrasound o a normal lymph node (A),o
partial replacement o a lymph node by melanoma (B), ando complete
replacement by melanoma, with and without powerDoppler, which shows
prominent neovascularization (C).
C
B
A
-
8/7/2019 Sentinel Node Biopsy in Melanoma
7/12
Volume, numBer 1 thomaSand hayeS
The American Joint Committee on Cancer (AJCC) staging systemor
melanoma60 does not dene the size o a micrometastasis, buta
metastatic deposit large enough to be identied by ultrasoundmust be
regarded as a macrometastasis or as occult clinical dis-
ease. This entire spectrum o tumor burden is bundled togetherand
classied as N1a or N2a. The crucial importance o tumor bur-den to
prognosis has been discussed above and, or this reason,the next
AJCC classication must dierentiate between micro-metastatic and
nonpalpable, occult macrometastatic deposits omelanoma in the SN.
Similarly, in the context o prognostic alse-positivity,
macrometastases identied by ultrasound will inevitablyprogress to
palpable nodal recurrence, which is why SN basinsshould be screened
by ultrasound beore patients are reerred orSLNB. Ultrasound can
detect occult metastatic melanoma in upto one-third o positive
SNs.23,31 In a recent ASCO presentation,Voit et al.32 showed that,
when the SN is identied by lymphos-cintigraphy, ultrasound can
detect metastatic melanoma in 50%o patients ultimately proven to be
SN-positive.32
At our Unit we do not advise SLNB or patients with primary
mela-
noma. Relevant regional node basin(s) are screened by
ultrasound
at the time o diagnosis. I no suspicious LNs are identied
then,ater wide excision o the primary tumor, patients embark onan
ultrasound surveillance program o the regional LNs with theintent o
perorming delayed lymphadenectomy when nonpal-pable, clinically
occult nodal recurrence is detected sonographi-cally and proven by
ultrasound-guided cytology. Extrapolatingrom the results o MSLT-1,
there is no r isk that patients are beingdisadvantaged by this
method o management. On the contrary,patients whose SNs are
prognostically alse-positive are protectedrom unnecessary
lymphadenectomy because such disease willnot progress to occult or
palpable nodal recurrence. Ultrasounddetection o occult clinical
disease presents a great challenge toSLNB because SN status has
never been shown to have prognosticsignicance in
ultrasound-negative patients.
Cncsins: Th Stats f SlNb in 2008
SLNB does not impart a survival benet to patients with
mela-noma. It is a prognostically imperect tool because it identies
acohort o prognostically alse-positive patients. At present,
thesepatients are wrongly up-staged, are given inaccurate
prognosticinormation, and undergo unnecessary lymphadenectomy
andunnecessary adjuvant therapy or entry into adjuvant trials.
Historically, there has been a trans-Atlantic dierence in
percep-tion o the introduction o SLNB. In Europe, ELND was rarely
per-ormed and thereore SLNB constitutes an increase in the amounto
surgery at the time o diagnosis. However, in the United States
and Australia, because ELND was routinely perormed, the
intro-duction o SLNB meant a reduction in the amount o surgery
atthe time o diagnosis. This dierence in perception is compound-ed
by diering views regarding the ecacy o adjuvant therapy in
melanoma. In some centers in the United States, SN-positive
pa-tients are advised to receive intereron, whereas in other
centersin the United States and mostly elsewhere in the world,
intereronis not advised because any advantage in DFS is not
considered asucient benet to outweigh the morbidity o
treatment.
Notwithstanding these diering perceptions, we argue that it
isnow appropriate or management o the regional LNs in mela-
noma to be rened urther with the replacement o SLNB by
ul-trasound screening and surveillance. MSLT-1 has now shown
thatSLNB does not give the patient a benet in terms o OS, andthe
benet in terms o DFS is unclear. Hence, it is essentially a
prognostic tool. Because, as we have shown, it is an
imperecttool with prognostically alse-positive patients being
over-treated,we argue that SLNB should not be recommended or
routine useoutside o a randomized controlled trial.
rfncs
1. Morton DL, Thompson JF, Cochran AJ, et al. Sentinel-node
biopsy
or nodal observation in melanoma. N Engl J Med2006;355:1307
1317.
2. Thompson JF, Scolyer RA, Keord RF, Uren RF. Melanoma
manage-
ment in 2007.Aust Fam Physician 2007;36:487488; author reply
488489.
3. Medalie N, Ackerman AB. Sentinel node biopsy has no benet
or
patients whose primary cutaneous melanoma has metastasized to
a
lymph node and thereore should be abandoned now. Br J
Dermatol
2004;151:298307.
4. Kanzler MH. The current status o evaluation and treatment o
high-
risk cutaneous melanoma: therapeutic breakthroughs remain
elu-sive.Arch Dermatol2007;143:785787.
5. Gonzalez U. Cloud over sentinel node biopsy: unlikely
survival ben-
et in melanoma.Arch Dermatol2007;143:775776.
6. Thomas JM. Caution with sentinel node biopsy in cutaneous
mela-
noma. Br J Surg 2006;93:129130.
7. Thomas JM. Time to re-evaluate sentinel node biopsy in
melano-
ma post-multicenter selective lymphadenectomy trial. J Clin
Oncol
2005;23:94439444.
8. Morton DL, Thompson JF, Cochran AJ, Essner R, Elasho R.
In-
terim results o the Multicentre Selective Lymphadenectomy
Trial (MSLT-1) in clinical stage I melanoma [Abstract]. J Clin
Oncol
2005;23(16S):7500.
9. Veronesi U, Adamus J, Bandiera DC, et al. Inecacy o
immediate
node dissection in stage 1 melanoma o the limbs. N Engl J
Med
1977;297:627630.10. Sim FH, Taylor WF, Ivins JC, Pritchard DJ,
Soule EH. A prospective ran-
domized study o the ecacy o routine elective lymphadenectomy
in management o malignant melanoma. Preliminary results.
Cancer
1978;41:948956.
11. Hochwald SN, Coit DG. Role o elective lymph node dissection
in
melanoma. Semin Surg Oncol1998;14:276282.
12. Cascinelli N, Morabito A, Santinami M, MacKie RM, Belli F.
Immedi-
ate or delayed dissection o regional nodes in patients with
mela-
noma o the trunk: a randomised trial. WHO Melanoma
Programme.
Lancet1998;351:793796.
13. Cochran AJ, Wen DR, Morton DL. Occult tumor cells in the
lymph
nodes o patients with pathological stage I malignant melanoma.
An
immunohistological study.Am J Surg Pathol1988;12:612618.
14. Thomas JM, Clark MA. Selective lymphadenectomy in sentinel
node-
positive patients may increase the risk o local/in-transit
recurrence inmalignant melanoma. Eur J Surg
Oncol2004;30:686691.
15. Estourgie SH, Nieweg OE, Kroon BB. High incidence o
in-transit me-
tastases ater sentinel node biopsy in patients with melanoma. Br
J
Surg 2004;91:13701371.
16. Kretschmer L, Beckmann I, Thoms KM, Mitteldor C, Bertsch
HP,
Neumann C. Factors predicting the risk o in-transit recurrence
a-
ter sentinel lymphonodectomy in patients with cutaneous
malignant
melanoma.Ann Surg Oncol2006;13:11051112.
17. Dalal KM, Patel A, Brady MS, Jaques DP, Coit DG. Patterns o
rst-re-
currence and post-recurrence survival in patients with primary
cuta-
neous melanoma ater sentinel lymph node biopsy.Ann Surg
Oncol
2007;14:19341942.
-
8/7/2019 Sentinel Node Biopsy in Melanoma
8/12
Sentinel lymph nodeBiopSyin melanoma Volume, numBer 1
18. Borgstein PJ, Meijer S, van Diest PJ. Are locoregional
cutaneous
metastases in melanoma predictable?Ann Surg Oncol1999;6:315
321.
19. de Vries M, Jager PL, Suurmeijer AJ, Plukker JT, van Ginkel
RJ, Hoek-
stra HJ. [Sentinel lymph node biopsy or melanoma: prognostic
value and disadvantages in 300 patients]. Ned Tijdschr
Geneeskd
2005;149:18451851.
20. Morton DL, Cochran AJ, Thompson JF, et al. Sentinel node
biopsy or
early-stage melanoma: accuracy and morbidity in MSLT-I, an
inter-national multicenter trial.Ann Surg 2005;242:302311;
discussion
311313.
21. AHern RP. Sentinel-node biopsy in melanoma. N Engl J Med
2007;356:418; author reply 419421.
22. Balch CM, Cascinelli N. Sentinel-node biopsy in melanoma. N
Engl J
Med2006;355:13701371.
23. Thompson JF, Shaw HM. Benets o sentinel node biopsy or
mela-
noma: a review based on interim results o the rst Multicenter
Se-
lective Lymphadenectomy Trial.ANZ J Surg 2006;76:100103.
24. Morton DL, Thompson JF, Essner R, et al. Validation o the
accuracy
o intraoperative lymphatic mapping and sentinel
lymphadenectomy
or early-stage melanoma: a multicenter trial. Multicenter
Selective
Lymphadenectomy Trial Group.Ann Surg 1999;230:453463.
25. Balch CM, Soong SJ, Gershenwald JE, et al. Prognostic
actors
analysis o 17,600 melanoma patients: validation o the
AmericanJoint Committee on Cancer melanoma staging system. J Clin
Oncol
2001;19:36223634.
26. Gershenwald JE, Thompson W, Manseld PF, et al.
Multi-institutional
melanoma lymphatic mapping experience: the prognostic value
o
sentinel lymph node status in 612 stage I or II melanoma
patients.
J Clin Oncol1999;17:976983.
27. Chao C, Wong SL, Ross MI, et al. Patterns o early recurrence
ater
sentinel lymph node biopsy or melanoma.Am J Surg
2002;184:520
524; discussion 525.
28. Kruper L, Botbyl J, Czerniecki B, et al. Predicting sentinel
lymph node
status in stage I/II melanoma [Abstract].J Clin
Oncol2005;23(16S, pt
l):7501.
29. Kirkwood JM, Manola J, Ibrahim J, Sondak V, Ernsto MS, Rao
U.
A pooled analysis o Eastern Cooperative Oncology Group and
In-
tergroup trials o adjuvant high-dose intereron or melanoma.
ClinCancer Res 2004;10:16701677.
30. Baounta ML, Beauchet A, Chagnon S, Saiag P. Ultrasonography
or
palpation or detection o melanoma nodal invasion: a
meta-analy-
sis. Lancet Oncol2004;5:673680.
31. Rossi CR, Mocellin S, Scagnet B, et al. The role o
preoperative ultra-
sound scan in detecting lymph node metastasis beore sentinel
node
biopsy in melanoma patients.J Surg Oncol2003;83:8084.
32. Voit C, van Akkooi AC, Schaer G, Schoengen A, Sterry W,
Egg-
ermont AM. Role o ultrasound (US) and US-guided ne needle
aspiration cytology (US-FNAC) prior to sentinel lymph node
biopsy
(SLNB) in 500 melanoma patients: reduction o need or SLNB by
high US-FNAC positive identication rate [Abstract]. J Clin
Oncol
2007;25(18S):8512.
33. Berk DR, Johnson DL, Uzieblo A, Kiernan M, Swetter SM.
Sentinel
lymph node biopsy or cutaneous melanoma: the Stanord experi-
ence, 1997-2004.Arch Dermatol2005;141:10161022.
34. Vuylsteke RJ, van Leeuwen PA, Statius Muller MG, Gietema
HA,
Kragt DR, Meijer S. Clinical outcome o stage I/II melanoma
patients
ater selective sentinel lymph node dissection: long-term
ollow-up
results.J Clin Oncol2003;21:10571065.
35. van Akkooi AC, de Wilt JH, Verhoe C, et al. Clinical
relevance o
melanoma micrometastases (
-
8/7/2019 Sentinel Node Biopsy in Melanoma
9/12
Volume, numBer 1 thomaSand hayeS
Some compounds discussed in this publication may be in
investigative stages and not yet approved by the FDA or uses
mentioned. The reader is urgedto check the package insert or each
drug or any change in indications and dosage and or added warnings
and precautions.
58. Voit C, Kron M, Schaer G, et al. Ultrasound-guided ne needle
as-
piration cytology prior to sentinel lymph node biopsy in
melanoma
patients.Ann Surg Oncol2006;13:16821689.
59. Voit C, Mayer T, Kron M, et al. Ecacy o ultrasound B-scan
com-
pared with physical examination in ollow-up o melanoma
patients.
Cancer2001;91:24092416.
60. Balch CM, Buzaid AC, Soong SJ, et al. Final version o the
American
Joint Committee on Cancer staging system or cutaneous
melano-
ma.J Clin Oncol2001;19:36353648.
-
8/7/2019 Sentinel Node Biopsy in Melanoma
10/12
noteS
-
8/7/2019 Sentinel Node Biopsy in Melanoma
11/12
noteS
-
8/7/2019 Sentinel Node Biopsy in Melanoma
12/12
PPO
UPdates
Wolters Kluwer Health-Lippincott Williams & Wilkins
333 Seventh Avenue, 19th Floor, New York, NY 10001
Presorted
standard
U.s. PostaGe PaId
LIPPInCott
WILLIaMs & WILKIns