Embed Size (px)
Citation preview

Lehigh Valley Health NetworkLVHN Scholarly Works
Department of Emergency Medicine
Subdural Hematoma as a Consequence of EpiduralAnesthesia.Tracy M Bishop DOLehigh Valley Health Network, [email protected]
Kareem S. Elsayed MSUSF MCOM- LVHN Campus, [email protected]
Kathleen E. Kane MDLehigh Valley Health Network, [email protected]
Follow this and additional works at: https://scholarlyworks.lvhn.org/emergency-medicine
Part of the Emergency Medicine Commons
This Article is brought to you for free and open access by LVHN Scholarly Works. It has been accepted for inclusion in LVHN Scholarly Works by anauthorized administrator. For more information, please contact [email protected].
Published In/Presented AtBishop, T. M., Elsayed, K. S., & Kane, K. E. (2015). Subdural Hematoma as a Consequence of Epidural Anesthesia.Case Reports InEmergency Medicine, 2015597942. doi:10.1155/2015/597942

Case ReportSubdural Hematoma as a Consequence of Epidural Anesthesia
Tracy M. Bishop, Kareem S. Elsayed, and Kathleen E. Kane
Department of Emergency Medicine, Lehigh Valley Hospital and Health Network/USF MCOM, CC & I-78, Allentown,PA 18103, USA
Correspondence should be addressed to Kathleen E. Kane; [email protected]
Received 18 October 2015; Revised 17 November 2015; Accepted 24 November 2015
Academic Editor: Aristomenis K. Exadaktylos
Copyright © 2015 Tracy M. Bishop et al.This is an open access article distributed under theCreativeCommonsAttribution License,which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Regional spinal and epidural anesthesia are used commonly in operative procedures. While the most frequent complication,postdural puncture headache (PDPH), is a clinically diagnosed positional headache that is usually self-limited, subduralhemorrhage (SDH) is a potentially fatal complication that cannot be missed. We report a case of an otherwise healthy femalewho presented with persistent positional headache and was ultimately found to have a large subdural hematoma with midline shiftrequiring surgical evacuation.
1. Introduction
Spinal and epidural anesthesia are commonly used in regionalanesthesia and are considered standard of care in obstetricanesthesiology. Complications occur in approximately 0.05%of cases [1]. The most common complication is a postduralpuncture headache (PDPH); this is a clinical diagnosis thattypically begins 24–48 hours following an inadvertent duralpuncture and classically presents as a throbbing positionalheadache [2]. Most PDPH resolve within 5 days withoutintervention [2]. PDPH has been attributed to CSF leakagewith a resultant loss in CSF pressure; subdural hematomaoccurs due to rupture of vascular structures in the subduralspace [2]. There are conflicting reports as to whether a bloodpatch in the setting of a potential dural puncture and clinicallysignificant headache can prevent development of a subduralhemorrhage (SDH) [2, 3].
2. Case Report
A 33-year-old female presented to the Emergency Depart-ment (ED) with a chief complaint of headache.The headachebegan three weeks before, shortly after she completed anormal spontaneous vaginal delivery without complication.During labor, she had one unsuccessful attempt at placingan epidural catheter; the second attempt was successful.She reported that, for the past three weeks, the headachewas constant but varied in intensity. During her pregnancy,
she was diagnosed with gestational diabetes mellitus, whichwas managed conservatively. She denied history of chronicheadaches.
Earlier, she had presented to another ED twice fortreatment of the headache. Her primary care physician haddiagnosed this headache as sinusitis and had prescribed heramoxicillin and pseudoephedrine. Her outpatient physicianordered an MRI to definitively diagnose the sinusitis; aradiologist read theMRI and asked her to go to anEDwithoutdiscussing the results with her.
Upon arrival in the ED, she rated the headache as 9/10.The headache was worsened bymoving her head and relievedwhen lying supine. She described mild photophobia. Shedenied blurred vision, nausea, numbness, weakness, or vom-iting. Her review of systems was negative except for left earpain for aweek. She had sustained a verymild head injury oneweek before when she lost her balance and hit her foreheadon the door of the bathroom while rising from the toilet. Shedenied loss of consciousness and stated that the intensity ofthe headache did not change. She denied smoking, alcohol,drug use, and recent travel. She denied family history ofbleeding disorders. She adamantly denied domestic violence.
On examination, her vital signs were normal. She wasawake, alert, and oriented ×3 with normal mood, affect, andspeech. Her physical exam including a detailed neurologicalexamination was normal.
Her laboratory tests revealed no coagulopathy. Computedtomography (CT) of the head was performed as the MRI
Hindawi Publishing CorporationCase Reports in Emergency MedicineVolume 2015, Article ID 597942, 2 pageshttp://dx.doi.org/10.1155/2015/597942

2 Case Reports in Emergency Medicine
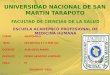
Figure 1
was not immediately available. CT of the head (Figure 1)revealed a 2 cm right hemispheric subdural hematoma whichappeared predominantly chronic but demonstrated super-imposed acute or subacute hemorrhage. There was alsosubfalcine herniation to the left. No acute parenchymalhematoma or depressed skull fracture was identified.
The patient necessitated a neurosurgical consultationgiven the large right subdural hematomawithmass effect andleft midline shift. A burr hole was placed in the operatingroom to drain the subdural hematoma. She also underwenta vertebral and carotid arteriogram that was negative forarteriovenous fistula and aneurysm. She received a bloodpatch andwas discharged homewith no neurological deficits.It is unlikely that the SDH resulted from her minor fallsince her headache had been going on prior to that andwas accompanied with ataxia. Therefore the minor fall wasa sequel of an already existing subdural hematoma.
3. Discussion
Intracranial hemorrhage following spinal or epidural anes-thesia for obstetric or other anesthetic reasons has beenreported with both large and small gauge needles, withpatients ranging from young adult to elderly [4]. In manycases, the SDH was found after the sudden onset of avery severe, debilitating headache, occasionally with rapidneurologic decompensation [5, 6]. However, Nepomucenoand Herd report a 17-year-old primigravida who suffered aninadvertent dural puncture during an attempt at epiduralanesthesia. MRI of the head done four days after the attemptwas normal; however, upon representation four weeks later,repeated MRI demonstrated bilateral subacute subduralhematomas [2].
It is prudent to consider intracranial hemorrhage inthe postpartum patient with headache who underwent anepidural procedure. Many patients with postdural punctureSDH required surgical evacuation and delay in diagnosis maycause significant morbidity and mortality, especially in anoften otherwise healthy population [4].
Conflict of Interests
The authors have no outside support information, conflicts,or financial interest to disclose.
References
[1] D. W. Barbara, B. C. Smith, and K. W. Arendt, “Images inanesthesiology: spinal subdural hematoma after labor epiduralplacement,” Anesthesiology, vol. 117, no. 1, p. 178, 2012.
[2] R. Nepomuceno and A. Herd, “Bilateral subdural hematomaafter inadvertent dural puncture during epidural analgesia,”TheJournal of Emergency Medicine, vol. 44, no. 2, pp. e227–e230,2013.
[3] A. K. Demetriades, M. F. Sheikh, and P. S. Minhas, “Fatal bilat-eral subdural haematoma after epidural anaesthesia for preg-nancy,” Archives of Gynecology and Obstetrics, vol. 284, no. 6,pp. 1597–1598, 2011.
[4] J. A. Amorim, D. S. C. Remigio, O. D. Fiho, M. A. G. deBarros, V. N. Carvalho, and M. M. Valencia, “Intracranialsubdural hematoma post-spinal anesthesia: report of two casesand review of 33 cases in the literature,” Revista Brasileira deAnesesiologia, vol. 60, no. 6, 2010.
[5] V. Schweiger, G. Zanconato, G. Lonati, S. Baggio, L. Gottin, andE. Polati, “Intracranial subdural hematoma after spinal anes-thesia for cesarean section,” Case Reports in Obstetrics andGynecology, vol. 2013, Article ID 253408, 3 pages, 2013.
[6] F. M. B. Bisinotto, R. A. Dezena, D. C. Fabri, T. M. V. Abud, andL.H.Canno, “Intracranial subdural hematoma: a rare complica-tion following spinal anesthesia: case report,” Revista Brasileirade Anestesiologia, vol. 62, no. 1, pp. 88–95, 2012.

Submit your manuscripts athttp://www.hindawi.com
Stem CellsInternational
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Disease Markers
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation http://www.hindawi.com Volume 2014
Immunology ResearchHindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Parkinson’s Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttp://www.hindawi.com