Embed Size (px)
Citation preview
Temporary Occlusion of the MiddleCerebral Artery in the Monkey:Clinical and Pathological ObservationsBY ROBERT M. CROWELL, M.D., YNGVE OLSSON, M.D., IGOR KLATZO, M.D.,AND AYUB OMMAYA, F.R.C.S.*
Alntract:TemporaryOcclusion ofthe MiddleCerebral Arteryin the Monkey:Clinical andPathologicalObservations
• The right middle cerebral artery (MCA) was exposed in monkeys via aretro-orbital microsurgical approach. In 43 animals a temporary occlusive clipwas placed on the MCA origin for one to 24 hours. In 20 animals, the origin ofthe MCA was permanently occluded.
Clinical evaluation of the monkeys one to three days postoperativelyshowed that one to two-hour clipping caused no or mild neurological deficits,four-hour clipping caused mild to moderate deficits, six to eight-hour clippingcaused moderate to severe deficits, and 24-hour clipping produced severedeficits or death, a result equivalent to that produced by permanentocclusion. Gross and microscopical evaluation of the brains showed that one totwo-hour clipping usually caused no or mild damage, four-hour clipping causedmild to moderate damage (often with capsular sparing), and six to eight-hourclipping and 24-hour clipping produced severe extensive infarction not differentfrom that caused by permanent occlusion. Six to eight-hour clipping and 24-hour clipping were associated with a high incidence of hemorrhagic infarction,but other clipping times were not. The results suggest that reestablishment offlow by surgical means within a few hours after MCA occlusion in selectedpatients might result in significant restoration of neurological function. If flowrenewal were done within about four hours, an increased incidence ofhemorrhagic infarction might be avoided.
ADDITIONAL KEY WORDSmicrosurgical approach to MCA
focal cerebral ischemia stroke surgerycollateral blood supply
Introduction• Anatomical1-* and physiological15-11 studieshave demonstrated that abundant collateralblood supply exists distal to the circle of Willis.This collateral supply can compensate, at leastin part, for the decrease in blood flow sustainedafter middle cerebral artery (MCA) occlusionin the macaque.8"12 In addition, cerebral tissue
•From the Branch of Surgical Neurology, and theLaboratory of Neuropathology and NeuroanatomicalSciences, National Institute of Neurological Diseasesand Stroke, National Institutes of Health, PublicHealth Service, U. S. Department of Health,Education and Welfare, Bethesda, Maryland, 20014.
Dr. Crowell's present address is: NeurosurgicalService, Massachusetts General Hospital, Boston,Massachusetts.
Stroke, Vol. ], November-December 1970
may be much more resistant to global ischemiathan has previously been recognized.13-18 Suchstudies suggest that early restoration of flowafter MCA occlusion might lead to improve-ment in appropriate stroke patients. This theo-retical possibility has become more attractivesince the development of feasible micro-surgical technique for MCA thromboembolec-tomy17-19 and superficial temporal MCA anas-tomosis.19-21
In evaluating the clinical role of flowrenewal following MCA occlusion, it would behelpful to know how long focal cerebralischemia may be tolerated before irreversiblechange develops. Several studies,22-24 mostnotably the classical work of Harvey andRasmussen, were intended to determine the
439
by guest on June 6, 2018http://stroke.ahajournals.org/
Dow
nloaded from
CROWELL, OLSSON, KLATZO, OMMAYA
maximum tolerable duration of MCA occlu-sion, but this work was done without the aid ofthe dissecting microscope, and surgical trau-ma other than MCA occlusion probably causedsome of the clinical and pathological findings.Recently Sundt and Waltz26 have described amicrosurgical, retro-orbital approach to theMCA origin which avoids retraction of thebrain, wide opening of the dural envelope,damage to the perforating vessels, and excessmanipulation of the MCA. It seems likely thatsuch a technique could provide information onthe effects of temporary MCA occlusionminimally complicated by surgical trauma. Wehave, therefore, applied the method of Sundtand Waltz to produce temporary MCA occlu-sion in macaque monkeys.
The primary objectives of this study were(1) to ascertain the duration of occlusionrequired to produce functional and morpholog-ical changes comparable to those produced bypermanent occlusion, and (2) to determinethe maximal duration of occlusion which failsto produce significant functional and morpho-logical changes.
MethodsSURGICAL PROCEDURE
Sixty-five monkeys {Macaco, mulatto) were usedfor this study. Animals were given phencylidinehydrochloride (Sernylan, 5 mg/kg IM), and smallincrements of sodium pentobarbital (up to 30mg/kg IV or IP) were administered as neededduring surgery. The operative procedures werecarried out by one of us (RMC) under sterile (oroccasionally semisterile) conditions. The Zeissoperating microscope was used to expose theorigin of the right MCA via a retro-orbital
approach.26 After the take-off of the MCA hadbeen gently freed from its arachnoid investment, acontrol or test intervention was carried out: sevenmonkeys underwent division of the MCA betweensilver clips, 13 monkeys had permanent clippingwith a Scoville aneurysm clip, two monkeys hadno clipping whatever, and 43 monkeys hadtemporary clipping for one, two, four, six, eight,ten, or 24 hours (table 1). Occlusion of MCA bythe clip was adjudged satisfactory only when thetip of the Scoville clip could be visualized beyondthe far edge of the vessel and when anatomicalcontinuity of the internal carotid artery (ICA)and anterior cerebral artery (ACA) appearedundisturbed. After clip removal, the dura was leftopen, and the galea and skin were closed with 3-0interrupted silk or stainless steel sutures. In thefirst 20 monkeys, blood pressure was monitoredwith a femoral catheter and a Statham straingauge. Mean pressure remained within the rangeof 95 to llOmmHg.2 6 '2 7
ANGIOGRAPHYEighteen monkeys were studied with right brachi-al retrograde serial angiograms. These studies areto be reported elsewhere.28
CLINICAL EVALUATIONPostoperatively animals were examined in theircages by one of us (RMC). Threat by theexaminer elicited maximal clinical performance.A simple scheme for grading of deficits wasemployed (fig. 1).
ClinicalGrade deficit Criteria
0 None Normal activities includingnormal climbing.
1 Mild Abnormal climbing (slip-ping with contralaterallimbs). Preference for useof ipsilateral hand. Mild
TABLE 1
Clinical Deficii in Relation to Duration of MCA Occlusion
Grod* ofclinicaldeficit
0 (none)1 (mild)2 (moderate)3 (severe)4 (death)
Total
0
200002
1-2
56000
11
Duration4
42400
10
of clipping6-8*
04620
12
(hn)24
01234
10
P
00571
13
d
002327
In this and subsequent tables, "p" indicates permanent MCA occlusion, and "d" meansarterial division.
*One animal in this group was subjected to ten-hour MCA clipping; he sustained a grade2 clinical deficit
440 Strok; Vol. 1, Novamb«r-Dec*mb«r 1970
by guest on June 6, 2018http://stroke.ahajournals.org/
Dow
nloaded from
TEMPORARY OCCLUSION OF THE MIDDLE CEREBRAL ARTERY
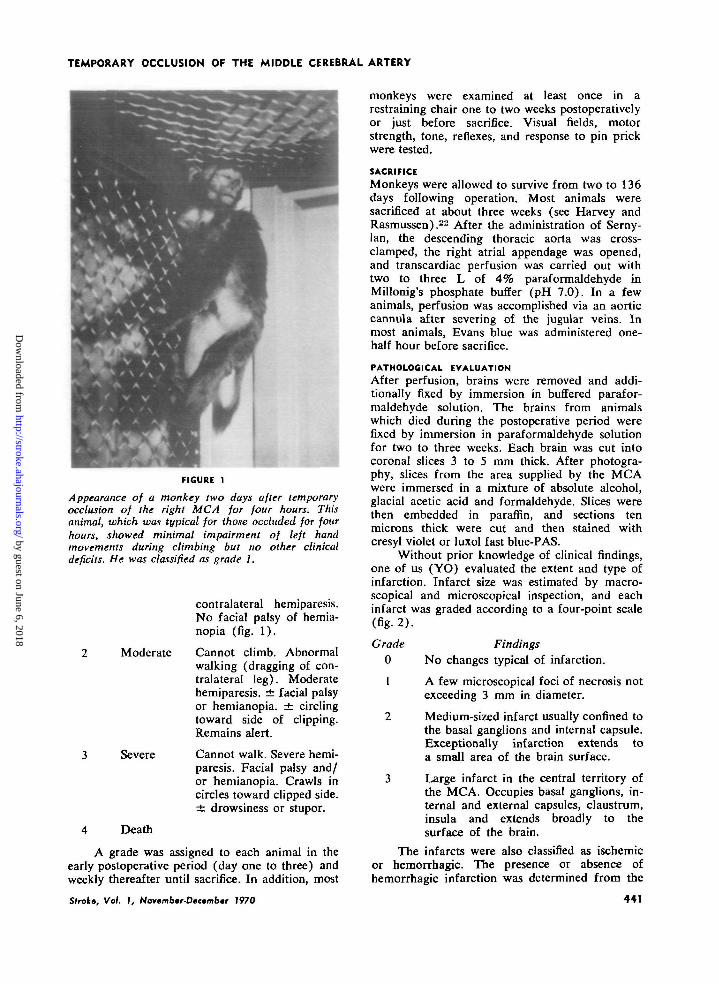
FIGURE 1
Appearance of a monkey two days after temporaryocclusion of the right MCA for four hours. Thisanimal, which was typical for those occluded for fourhours, showed minimal impairment of left handmovements during climbing but no other clinicaldeficits. He was classified as grade 1.
contralateral hemiparesis.No facial palsy of hemia-nopia (fig. 1).
Moderate
Severe
Death
Cannot climb. Abnormalwalking (dragging of con-tralateral leg). Moderatehemiparesis. ± facial palsyor hemianopia. ± circlingtoward side of clipping.Remains alert.
Cannot walk. Severe hemi-paresis. Facial palsy and/or hemianopia. Crawls incircles toward clipped side.± drowsiness or stupor.
A grade was assigned to each animal in theearly postoperative period (day one to three) andweekly thereafter until sacrifice. In addition, most
Stroke, Vol. 1, Norambmr-Dectmbtr 1970
monkeys were examined at least once in arestraining chair one to two weeks postoperativelyor just before sacrifice. Visual fields, motorstrength, tone, reflexes, and response to pin prickwere tested.
SACRIFICEMonkeys were allowed to survive from two to 136days following operation. Most animals weresacrificed at about three weeks (see Harvey andRasmussen).22 After the administration of Serny-lan, the descending thoracic aorta was cross-clamped, the right atrial appendage was opened,and transcardiac perfusion was carried out withtwo to three L of 4% paraformaldehyde inMillonig's phosphate buffer (pH 7.0). In a fewanimals, perfusion was accomplished via an aorticcannula after severing of the jugular veins. Inmost animals, Evans blue was administered one-half hour before sacrifice.
PATHOLOGICAL EVALUATIONAfter perfusion, brains were removed and addi-tionally fixed by immersion in buffered parafor-maldehyde solution. The brains from animalswhich died during the postoperative period werefixed by immersion in paraformaldehyde solutionfor two to three weeks. Each brain was cut intocoronal slices 3 to 5 mm thick. After photogra-phy, slices from the area supplied by the MCAwere immersed in a mixture of absolute alcohol,glacial acetic acid and formaldehyde. Slices werethen embedded in paraffin, and sections tenmicrons thick were cut and then stained withcresyl violet or luxol fast blue-PAS.
Without prior knowledge of clinical findings,one of us (YO) evaluated the extent and type ofinfarction. Infarct size was estimated by macro-scopical and microscopical inspection, and eachinfarct was graded according to a four-point scale(fig. 2).
Grade Findings0 No changes typical of infarction.
1 A few microscopical foci of necrosis notexceeding 3 mm in diameter.
2 Medium-sized infarct usually confined tothe basal ganglions and internal capsule.Exceptionally infarction extends toa small area of the brain surface.
3 Large infarct in the central territory ofthe MCA. Occupies basal ganglions, in-ternal and external capsules, claustrum,insula and extends broadly to thesurface of the brain.
The infarcts were also classified as ischemicor hemorrhagic. The presence or absence ofhemorrhagic infarction was determined from the
441
by guest on June 6, 2018http://stroke.ahajournals.org/
Dow
nloaded from
CROWELL, OLSSON, KLATZO, OMMAYA
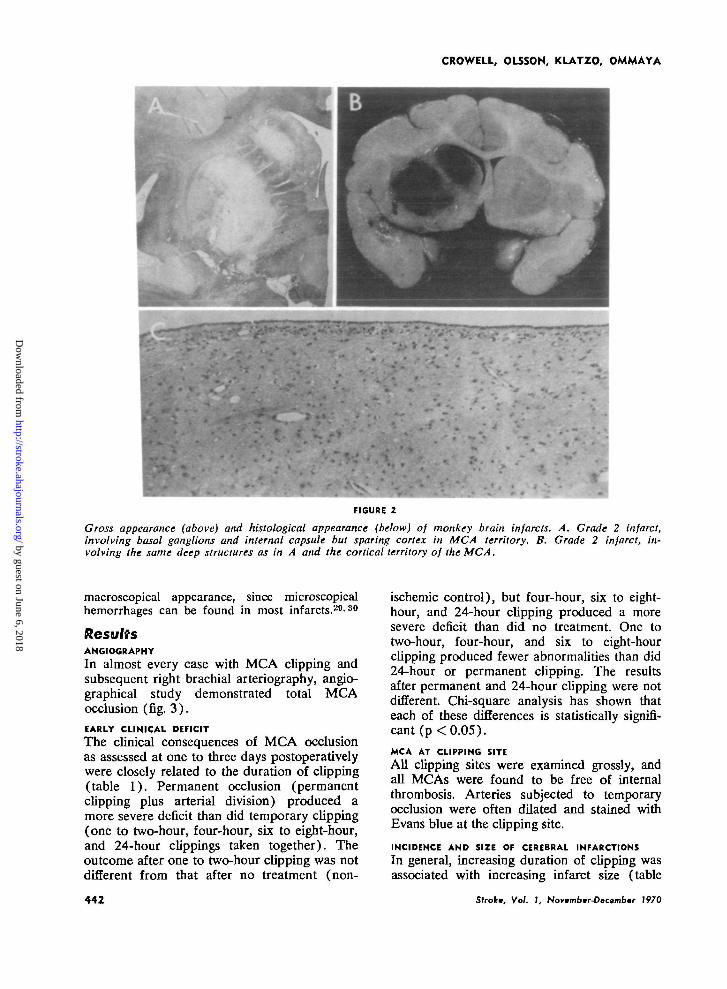
FIGURE 2
Gross appearance (above) and histological appearance (below) of monkey brain infants. A. Grade 2 infarct,involving basal ganglions and internal capsule but sparing cortex in MCA territory. B. Grade 2 infarct, in-volving the same deep structures as in A and the cortical territory of the MCA.
macroscopical appearance, since microscopicalhemorrhages can be found in most infarcts.20'80
ResultsANGIOGRAPHY
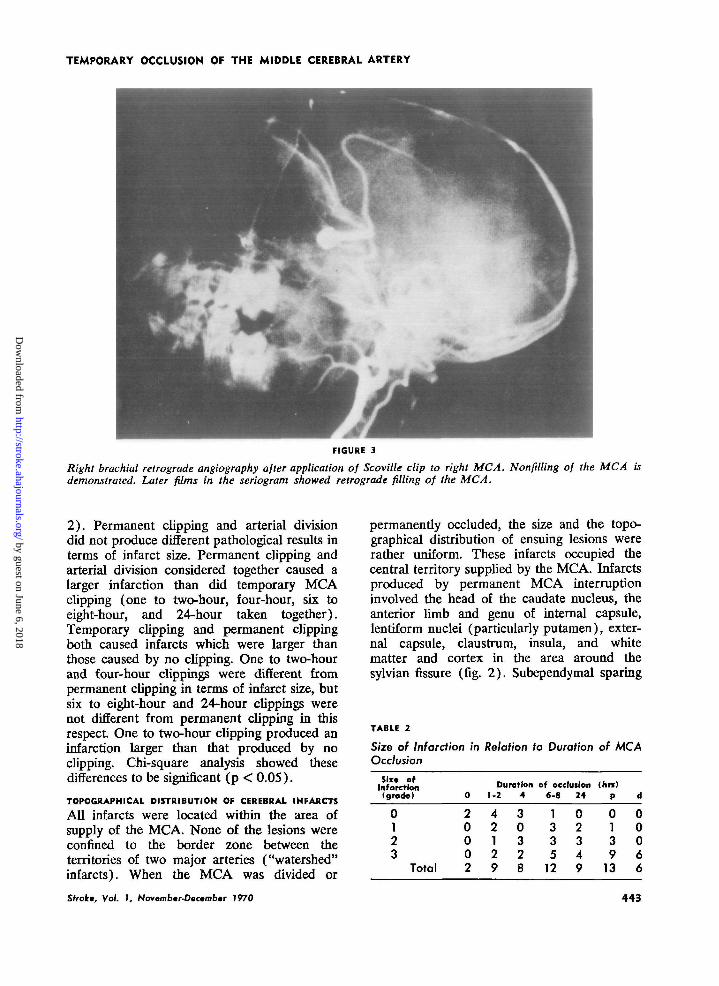
In almost every case with MCA cupping andsubsequent right brachial arteriography, angio-graphical study demonstrated total MCAocclusion (fig. 3).EARLY CLINICAL DEFICITThe clinical consequences of MCA occlusionas assessed at one to three days postoperativelywere closely related to the duration of clipping(table 1). Permanent occlusion (permanentcupping plus arterial division) produced amore severe deficit than did temporary clipping(one to two-hour, four-hour, six to eight-hour,and 24-hour cuppings taken together). Theoutcome after one to two-hour clipping was notdifferent from that after no treatment (non-
ischemic control), but four-hour, six to eight-hour, and 24-hour clipping produced a moresevere deficit than did no treatment. One totwo-hour, four-hour, and six to eight-hourclipping produced fewer abnormalities than did24-hour or permanent clipping. The resultsafter permanent and 24-hour cupping were notdifferent. Chi-square analysis has shown thateach of these differences is statistically signifi-cant (p <0.05).
MCA AT CLIPPING SITE
All clipping sites were examined grossly, andall MCAs were found to be free of internalthrombosis. Arteries subjected to temporaryocclusion were often dilated and stained withEvans blue at the clipping site.
INCIDENCE AND SIZE OF CEREBRAL INFARCTIONS
In general, increasing duration of clipping wasassociated with increasing infarct size (table
442 Slrokt, Vol. 1, Novambtr-Dacambcr 7970
by guest on June 6, 2018http://stroke.ahajournals.org/
Dow
nloaded from
TEMPORARY OCCLUSION OF THE MIDDLE CEREBRAL ARTERY
FIGURE 3
Right brachial retrograde angiography after application of Scoville clip to right MCA. Nonfilling of the MCA isdemonstrated. Later films in the seriogram showed retrograde filling of the MCA.
2). Permanent clipping and arterial divisiondid not produce different pathological results interms of infarct size. Permanent clipping andarterial division considered together caused alarger infarction than did temporary MCAclipping (one to two-hour, four-hour, six toeight-hour, and 24-hour taken together).Temporary clipping and permanent clippingboth caused infarcts which were larger thanthose caused by no clipping. One to two-hourand four-hour cuppings were different frompermanent clipping in terms of infarct size, butsix to eight-hour and 24-hour clippings werenot different from permanent cupping in thisrespect One to two-hour clipping produced aninfarction larger than that produced by nocupping. Chi-square analysis showed thesedifferences to be significant (p < 0.05).
TOPOGRAPHICAL DISTRIBUTION OF CEREBRAL INFARCTS
All infarcts were located within the area ofsupply of the MCA. None of the lesions wereconfined to the border zone between theterritories of two major arteries ("watershed"infarcts). When the MCA was divided or
permanently occluded, the size and the topo-graphical distribution of ensuing lesions wererather uniform. These infarcts occupied thecentral territory supplied by the MCA. Infarctsproduced by permanent MCA interruptioninvolved the head of the caudate nucleus, theanterior limb and genu of internal capsule,lentiform nuclei (particularly putamen), exter-nal capsule, claustrum, insula, and whitematter and cortex in the area around thesylvian fissure (fig. 2). Subependymal sparing
TABLE 2
Size of Infarction in Relation to Duration of MCAOcclusion
Six* ofInfarction(grade)
0123
Total
0
20002
Duration1-2
42129
4
30328
of occlusion6-8
1335
12
24
02349
(hn)P
0139
13
d
00066
Strok; Vol. 1, Noycmbtr-Dactmbtr 7970 441
by guest on June 6, 2018http://stroke.ahajournals.org/
Dow
nloaded from
CROWELL, OLSSON, KLATZO, OMMAYA
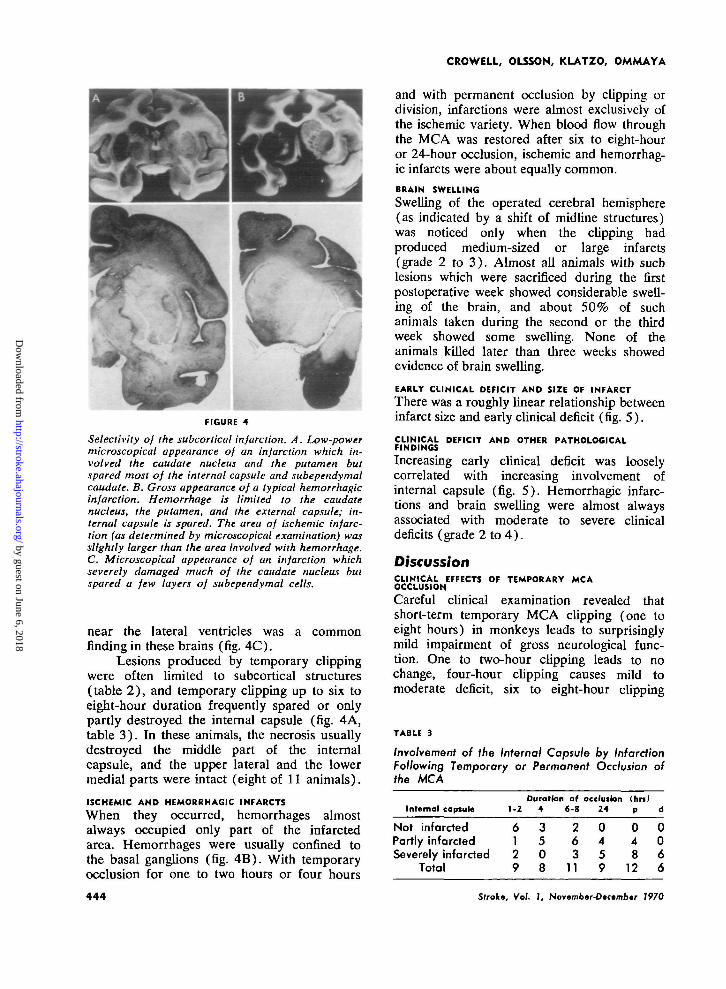
FIGURE 4
Selectivity of the subcortical infarction. A. Low-powermicroscopical appearance of an infarction which in-volved the caudate nucleus and the putamen butspared most of the internal capsule and subependymalcaudate. B. Gross appearance of a typical hemorrhagicinfarction. Hemorrhage is limited to the caudatenucleus, the putamen, and the external capsule; in-ternal capsule is spared. The area of ischemic infarc-tion (as determined by microscopical examination) wasslightly larger than the area involved with hemorrhage.C. Microscopical appearance of an infarction whichseverely damaged much of the caudate nucleus butspared a few layers of subependymal cells.
near the lateral ventricles was a commonfinding in these brains (fig. 4C).
Lesions produced by temporary clippingwere often limited to subcortical structures(table 2 ) , and temporary cupping up to six toeight-hour duration frequently spared or onlypartly destroyed the internal capsule (fig. 4A,table 3) . In these animals, the necrosis usuallydestroyed the middle part of the internalcapsule, and the upper lateral and the lowermedial parts were intact (eight of 11 animals).
ISCHEMIC AND HEMORRHAGIC INFARCTS
When they occurred, hemorrhages almostalways occupied only part of the infarctedarea. Hemorrhages were usually confined tothe basal ganglions (fig. 4B). With temporaryocclusion for one to two hours or four hours
and with permanent occlusion by clipping ordivision, infarctions were almost exclusively ofthe ischemic variety. When blood flow throughthe MCA was restored after six to eight-houror 24-hour occlusion, ischemic and hemorrhag-ic infarcts were about equally common.
BRAIN SWELLING
Swelling of the operated cerebral hemisphere(as indicated by a shift of midline structures)was noticed only when the clipping hadproduced medium-sized or large infarcts(grade 2 to 3 ) . Almost all animals with suchlesions which were sacrificed during the firstpostoperative week showed considerable swell-ing of the brain, and about 50% of suchanimals taken during the second or the thirdweek showed some swelling. None of theanimals killed later than three weeks showedevidence of brain swelling.
EARLY CLINICAL DEFICIT AND SIZE OF INFARCT
There was a roughly linear relationship betweeninfarct size and early clinical deficit (fig. 5) .
CLINICAL DEFICIT AND OTHER PATHOLOGICALFINDINGS
Increasing early clinical deficit was looselycorrelated with increasing involvement ofinternal capsule (fig. 5) . Hemorrhagic infarc-tions and brain swelling were almost alwaysassociated with moderate to severe clinicaldeficits (grade 2 to 4 ) .
DiscussionCLINICAL EFFECTS OF TEMPORARY MCAOCCLUSION
Careful clinical examination revealed thatshort-term temporary MCA clipping (one toeight hours) in monkeys leads to surprisinglymild impairment of gross neurological func-tion. One to two-hour clipping leads to nochange, four-hour cupping causes mild tomoderate deficit, six to eight-hour cupping
TABLE 3
Involvement of the Internal Capsule by InfarctionFollowing Temporary or Permanent Occlusion ofthe MCA
Internal capsuleDuration of occluilon (hn)
1-2 4 6-8 24 p d
Not infarcted 6 3 2 0 0 0Partly infarcted 1 5 6 4 4 0Severely infarcted 2 0 3 5 8 6
Total 9 8 11 9 12 6
444 Stroke, Vol. 1, November-Dccembar 1970
by guest on June 6, 2018http://stroke.ahajournals.org/
Dow
nloaded from
TEMPORARY OCCLUSION OF THE MIDDLE CEREBRAL ARTERY
3 -
Q<cre>
I -
0 -
-
-
-..
M
i
•
••
t.
•
i
•
••
ii
••
it
U
\\
••
•
_
-
-tt
-M
i
t. ||
II !>
tt ••
•
i i
I 2
PATHOLOQCAL GRADE
NO PARTIAL EXTENSIVE
INFARCTION INTERNAL CAPSULE
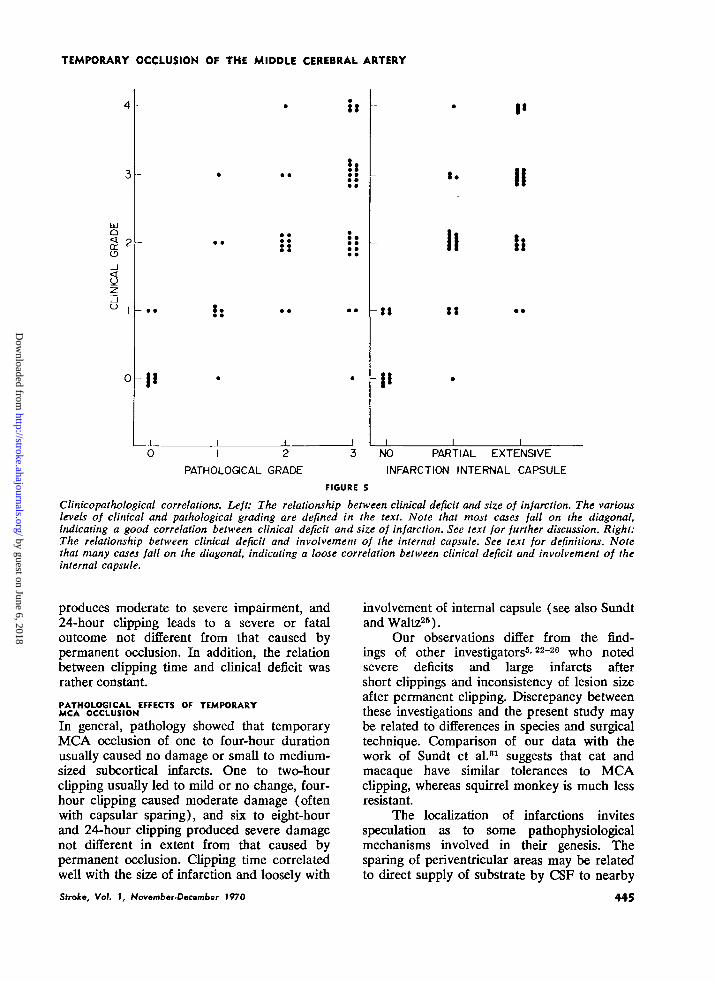
FIGURE 5
Clinicopathological correlations. Left: The relationship between clinical deficit and size of infarction. The variouslevels of clinical and pathological grading are defined in the text. Note that most cases fall on the diagonal,indicating a good correlation between clinical deficit and size of infarction. See text for further discussion. Right:The relationship between clinical deficit and involvement of the internal capsule. See text for definitions. Notethat many cases fall on the diagonal, indicating a loose correlation between clinical deficit and involvement of theinternal capsule.
produces moderate to severe impairment, and24-hour clipping leads to a severe or fataloutcome not different from that caused bypermanent occlusion. In addition, the relationbetween clipping time and clinical deficit wasrather constant
PATHOLOGICAL EFFECTS OF TEMPORARYMCA OCCLUSION
In general, pathology showed that temporaryMCA occlusion of one to four-hour durationusually caused no damage or small to medium-sized subcortical infarcts. One to two-hourclipping usually led to mild or no change, four-hour clipping caused moderate damage (oftenwith capsular sparing), and six to eight-hourand 24-hour clipping produced severe damagenot different in extent from that caused bypermanent occlusion. Clipping time correlatedwell with the size of infarction and loosely with
Stroke, Vol. 1, November-December 1970
involvement of internal capsule (see also Sundtand Waltz26).
Our observations differ from the find-ings of other investigators5'22"20 who notedsevere deficits and large infarcts aftershort clippings and inconsistency of lesion sizeafter permanent clipping. Discrepancy betweenthese investigations and the present study maybe related to differences in species and surgicaltechnique. Comparison of our data with thework of Sundt et al.81 suggests that cat andmacaque have similar tolerances to MCAcupping, whereas squirrel monkey is much lessresistant
The localization of infarctions invitesspeculation as to some pathophysiologicalmechanisms involved in their genesis. Thesparing of periventricular areas may be relatedto direct supply of substrate by CSF to nearby
445
by guest on June 6, 2018http://stroke.ahajournals.org/
Dow
nloaded from
CROWELL, OLSSON, KLATZO, OMMAYA
tissue, or to the extensive anastomoses of theperiventricular arterial system.82'33 The sparingof internal capsule in some cases may berelated to a relative resistance of white matterto ischemic damage. When clipping was ofshort duration (one to four hours), infarctionwas often limited to subcortical structures,suggesting that surface collateral supply issuperior to that for lenticulostriate vessels.82-M
Pathological examination revealed manyhemorrhagic infarctions in animals clipped sixto eight hours and 24 hours but not in thoseclipped one to two hours, four hours, andpermanently. These data suggest that ischemiaof more than four hours' duration may lead tovascular damage and subsequent hemorrhageon restoration of flow. In this connection it isknown that MCA clipping and subsequenthypertension regularly lead to hemorrhagicinfarction,84 and this mechanism cannot beruled out in our studies. In addition, severalclinical studies85'S6 have shown that removal ofICA or common carotid artery (CCA)occlusion in the early postictal period (up totwo weeks) may be associated with a highincidence of hemorrhagic infarction. In theseclinical studies, however, resumption of flowrarely occurred within four hours of the strokeictus. Therefore, the relation between restora-tion of flow and hemorrhagic infarction may besimilar in monkeys and man: restoration offlow by appropriate surgery within the first fourhours might be associated with a low incidenceof hemorrhagic infarction, and revasculariza-tion after greater delay may be associated withincreased risk of hemorrhagic complications.Successful clinical results following very earlyremoval of CCA-ICA"7 s« or MCA17-10 ob-struction are at least compatible with thisconcept. Careful clinicopathological correla-tions, with close attention to the interval torestoration of flow and to arterial bloodpressure will be needed to decide this point inman.
TOLERANCE OF FOCAL CEREBRAL ISCHEMIA
Recent observations have suggested that, underspecial circumstances, even global ischemialasting up to two hours may be borne by thecentral nervous system with relative impuni-ty.1 8 1 4 1 6 This ability to withstand globalischemia may play a role in protecting monkeybrain during MCA occlusion. In addition, thereis abundant anatomical and physiological
evidence that collateral blood supply protectsthe brain after occlusion of a major cerebralartery.1"10 This collateral supply is probablyresponsible, at least in part, for the tolerance ofthe monkey brain to temporary MCA clipping.
Anesthesia probably played a role inprotecting monkeys from cerebral ischemia inthe present study.89'40 Sodium pentobarbitalprobably protected cerebral tissue from ische-mic damage, but this effect was probablyattenuated by the decrease in total cerebralflow induced by the drug.39 Obviously, a studyof the effects of temporary MCA occlusion onmonkey brain unaffected by drugs would bedesirable, but technical problems will makesuch a study difficult.
Leakage of blood past an incompleteocclusion of the MCA might be postulated as afactor which would protect monkey brainduring MCA clipping. Against this possibility,angiographical studies have demonstrated thatScoville clips insure total MCA occlusion whenproperly placed.28
IMPLICATIONS FOR CLINICAL PRACTICE
The experimental data reported here suggestthat removal of MCA occlusion within a fewhours of the stroke ictus might lead to usefulrestoration of function in some clinical caseswith suitable collateral circulation. Limitedneurosurgical experience with prompt MCAthromboembolectomy supports this con-cept.17-19 It may be that angiography and/orregional cerebral blood flow studies11'12'41
could help in selecting cases with suitable focallesions and collateral blood supply for suchsurgical therapy. In addition, the resultssuggest that during neurosurgical procedurestemporary MCA occlusion lasting up to severalhours might be tolerated in patients with goodcollateral supply. In such cases, the protectiveeffect of general anesthesia could also beutilized, and preoperative studies might helpdetermine the adequacy of collateral bloodflow. The neuropathological data suggest that ifrestoration of blood flow is accomplishedwithin about four hours after occlusion, anincreased incidence of hemorrhagic cerebralinfarction might be avoided.
AcknowledgmentWe are grateful to Dr. G. Di Chiro and Mrs. D.Sadowsky for helpful advice and to Mr. W. Parker,Mr. J. Walker, and Mrs. M. Shevitz for technicalassistance.
446 Slrokt, Vol. 7, Novcmbar-Oacember 1970
by guest on June 6, 2018http://stroke.ahajournals.org/
Dow
nloaded from
TEMPORARY OCCLUSION OF THE MIDDLE CEREBRAL ARTERY
References1. Pfeifer RA: Die Angioorchitektonik der Gross-
hirngerinde. Berlin, Julius Springer, 19282. Fay T: Cerebral vasculature: Preliminary
report of study by means of roentgen ray.JAMA 84: 1727-1730, 1925
3. Cobb S: Cerebral circulation. X I I I . Thequestion of "end-arteries" of the brain andthe mechanism of infarction. Arch NeurolPsychiat 25: 273-280, 1931
4. Vander Eecken HM: Anastomoses Between theLeptomeningeal Arteries of the Brain. TheirMorphological, Pathological and Clinical Sig-nificance. Springfield, Illinois, Charles CThomas, 1959
5. Meyer JS, Fang HC, Denny-Brown D: Polaro-graphic study of cerebral collateral circulation.Arch Neurol Psychiat 72: 296-312, 1964
6. Meyer JS, Denny-Brown D: The cerebralcollateral circulation. I. Factors influencingcollateral blood flow. Neurology (Minneap) 7:447-458, 1957
7. Denny-Brown D, Meyer JS: The cerebralcollateral circulation. I I . Production of cere-bral infarction by Ischemlc anoxia and itsreversibility in early stages. Neurology (Min-neap) 7: 567-579, 1957
8. Lascelles RG, Burrows EH: Occlusion of themiddle cerebral artery. Brain 88: 85-96,1965
9. Waltz AG, Sundt TM, Owen CA Jr: Effect ofmiddle cerebral artery occlusion on corticalblood flow in animals. Neurology 16: 1185-1190, 1965
10. Waltz AG, Sundt TM Jr: The mlcrovasculatureand microcirculation of the cerebral cortexafter arterial occlusion. Brain 90: 681-696,1967
11. Baltistini N, Casaechia M, Baestvlini A, et a l :Effects of hyperventilation on focal braindamage following middle cerebral artery oc-clusion. In Brock M, Fieschi C, Ingvar DH, etal (eds) : Cerebral Blood Flow. Berlin, Spring-er Verlag, p 249-253, 1969
12. Paulson OB: Regional cerebral blood flow inapoplexy due to occlusion of the middlecerebral artery. Neurology (Minneap) 20: 63-77, 1970
13. Suda I, Kito K, Adachi C: Viability of longterm frozen cat brain in vitro. Nature 212:268-270, 1966
14. Hossmann K-A, Sato K: Recovery of neuronalfunction after prolonged cerebral ischemia.Science 168: 375-376, 1970
15. Ames A I I I , Wright RL, Kowada M, et a l : .Cerebral ischemia. I I . The M-reflow phenome-non. Amer J Path 52: 437-453, 1968
16. Cantu RC, Ames AA I I I : Experimental preven-
tion of cerebral vasculature obstruction pro-duced by ischemia. J Neurosurg 30: 50-56,1969
17. Jacobson JH I I , Wallman U , Schumacher GH,et a l : Microsurgery as an aid to middlecerebral endarterectomy. J Neurosurg 19:108-115, 1962
18. Lougheed WM, Gunton RW, Bamett HJM:Embolectomy of carotid, middle, and anteriorcerebral arteries. Report of a case. J Neuro-surg 22: 607-609, 1965
19. Yasargil MG: Microsurgery Applied to Neuro-surgery. Stuttgart, Georg Thieme Verlag,1969
20. Yasargil MG: Experimental small vessel surgeryin dog including patching and grafting ofcerebral vessels and the formation of function-al extra-intracranial shunts. In Donaghn RMP,Yasargil MG (eds) : Microvascular Surgery. St.Louis, CV Mosby Company, p 87-126, 1967
21 . Yasargil MG, Krayenbuhl HA, Jacobson JH I I :Microneurosurgical arterial reconstruction.Surgery 67: 221-233, 1970
22. Harvey J, Rasmussen T: Occlusion of themiddle cerebral artery; an experimental study.AMA Arch Neurol & Psychiat 66: 20-29,1951
23. Anthony LU, Goldring S, O'Leary JL, et a l :Experimental cerebrovascular occlusion indog. Arch Neurol 8: 515-527, 1963
24. Heilbrun MP, Goldring S: Steady potential andpathologic correlates of cerebrovascular occlu-sion of dog. Arch Neurol (Chicago) 19: 410-420, 1968
25. Sundt TM Jr, Waltz AG: Experimental cere-bral infarction: Retro-orbital, extra-dural ap-proach for occluding the middle cerebralartery. Proc Staff Meet Mayo Clin 4 1 : 159-168,1966
26. Ralston B, Rasmussen T, Kennedy T: Occlu-sion of the middle cerebral artery undernormotension and anemically induced andchemical induced hypotension. J Neurosurg12:26-33, 1955
27. Cantu R, Ames A I I I , Di Giacinto G, et a l :Hypotension: A major factor limiting recoveryfrom cerebral ischemia. J Surg Res 9: 525-529, 1959
28. Crowell RM, Olsson Y, Ommaya AK: Angio-graphic and microangiographic observationsin experimental cerebral infarction. To bepublished
29. Hain RF, Westharpen PV, Swank RL: Hemor-rhagic cerebral infarction by arterial occlu-sion. An experimental study. J Neuropath &Exp Neurol 11:34-43, 1952
30. Jorgensen L, Torvik A : Ischaemic cerebrovas-cular diseases in an autopsy series. Part 2.
Slrok; Vol. 1, November-December 1970 447
by guest on June 6, 2018http://stroke.ahajournals.org/
Dow
nloaded from
CROWELL, OLSSON, KLATZO, OMMAYA
Prevalence, location, pathogenesis, and clinicalcourse of cerebral infarcts. J Neurol Sci 9:285-320, 1969
3 1 . Sundt TM, Grant WC, Garcia JH: Restorationof middle cerebral artery flow in experimentalinfarction. J Neurosurg 3 1 : 311-322, 1969
32. Van Den Bergh R: The periventricular intra-cerebral blood supply. In Meyer JS, LechnerH, Eichhorn 0 (eds) : Research on theCerebral Circulation. Springfield, Illinois,Charles C Thomas, p 52-65, 1966
33. Vander Eecken H: Arterial topography andarchitecture of the intracerebral demarcationzones of the human adult and foetus. In MeyerJS, Lechner H, Eichhorn O (eds) : Researchon the Cerebral Circulation. Springfield, I l l i -nois, Charles C Thomas, p 42 -51 , 1966
34. Globus JH, Epstein JA, Green MA, et a l : Focalcerebral hemorrhage experimentally pro-duced. J Neuropath & Exp Neurol 8: 113-116,1949
35. Wylie EJ, Hein MF, Adams JE: Intracranialhemorrhage following surgical revasculariza-tion for treatment of acute strokes. J Neuro-surg 2 1 : 212-215, 1964
36. Bruetman ME, Fields WS, Crawford ES, et a l :Cerebral hemorrhage as a complication ofsurgery in carotid artery occlusion. TransAmer Neurol Assoc 88: 52-55, 1963
37. Ojemann R, Austen WG: Surgical treatment ofextracranial occlusive vascular disease. InSmith JL (ed) : Neuroophthalmology. Vol. IV,St. Louis, CV Mosby, p 388-404, 1968
38. Vollmar J, Lanbach K, Gruss JD: Die chirur-gische Behandlung des akuten Arterienver-schlusses. Deutsch Med Wschr 94: 2315-2319,1969
39. Pierce EC, Lambertsen CJ, Deutsch S, et a l :Cerebral circulation and metabolism duringthiopental anesthesia and hyperventilation inman. J Clin Invest 41 : 1664-1671, 1962
40. Wells BA, Keats AS, Cooley DA: Increasedtolerance to cerebral ischemia produced bygeneral anesthesia during temporary carotidocclusion. Surgery 54: 216-223, 1963
4 1 . Cronqvist S, Laroche F: Transitory hyper-anemia in focal cerebral vascular lesionsstudied by angiography and regional cerebralblood flow measurements. Brit J Radiol 40 :270-274, 1967
448 Stroke, Vol. J, Novtmbtr-Dtcimbar 7970
by guest on June 6, 2018http://stroke.ahajournals.org/
Dow
nloaded from
OMMAYAROBERT M. CROWELL, YNGVE OLSSON, IGOR KLATZO and AYUB
Pathological ObservationsTemporary Occlusion of the Middle Cerebral Artery in the Monkey: Clinical and
Print ISSN: 0039-2499. Online ISSN: 1524-4628 Copyright © 1970 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Stroke doi: 10.1161/01.STR.1.6.439
1970;1:439-448Stroke.
http://stroke.ahajournals.org/content/1/6/439located on the World Wide Web at:
The online version of this article, along with updated information and services, is
http://stroke.ahajournals.org//subscriptions/
is online at: Stroke Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. and Answer
Permissions and Rights QuestionServices. Further information about this process is available in therequested is located, click Request Permissions in the middle column of the Web page underthe Editorial Office. Once the online version of the published article for which permission is being
can be obtained via RightsLink, a service of the Copyright Clearance Center, notStrokepublished in Requests for permissions to reproduce figures, tables, or portions of articles originallyPermissions:
by guest on June 6, 2018http://stroke.ahajournals.org/
Dow
nloaded from