Embed Size (px)
Citation preview

Journal of Neurology, Neurosurgery, and Psychiatry 1986;49:524-528
Thalamic tumours invading the brain stem producecrossed cerebellar diaschisis demonstrated by PETHIDENAO FUKUYAMA, MASAKUNI KAMEYAMA, KIYOSHI HARADA,NAOKI FUJIMOTO, AKIRA KOBAYASHI,* WARO TAKI,* TSUNEMASAISHIKAWA,* HAJIME HANDA,* SHUJI TANADA,t KANJI TORIZUKAt
From the Department of Neurology, Neurosurgery,* and Nuclear Medicine,j Kyoto University School of
Medicine, Kyoto, Japan
SUMMARY Two cases of thalamic tumour, spreading through the midbrain into the pons ventro-laterally, showed suppression of cerebellar blood flow on the opposite side to the tumour, and alsoshowed reduction of blood flow in the pons on the side of the tumour in positron emissiontomographic studies. The pathophysiological mechanism ofcrossed cerebellar diaschisis may be dueto functional suppression of the pontine nuclei by destruction of descending fibres from the cerebralcortex.
The purpose of this study was to elucidate the mech-anism of crossed cerebellar diaschisis based on posi-tron emission tomographic (PET) findings in threecases of deeply seated brain tumours. It has beenreported that crossed cerebellar diaschisis has beenobserved in cases of frontal or parietal lobelesions.1`6 We have studied two cases of thalamictumour involving the brain stem in which crossedcerebellar diaschisis was observed, while a third caseof thalamic tumour expanding upward toward thelateral ventricle showed no reduction of contralateralcerebellar blood flow. The three cases were examinedwith oxygen-15 PET; we discuss the patho-physio-logical mechanism of crossed cerebellar diaschisis,based on the PET findings.
Patients and methods
Three cases of brain tumour were identified on X-ray CTscans, which were performed a day before PET study. Theorbitomeatal line was marked on the CT scan and referencedto the PET study. Eighteen normal volunteers (age 32 + 7 8),were also examined, and the normal range on cerebellarhemispheric cerebral blood flow (CBF), cerebral metabolicrate of oxygen (CMR02) and oxygen extraction fraction(OEF) were determined.
Address for reprint requests: Dr H Fukuyama, Department of Neu-rology, Kyoto University School of Medicine, 54 Shogoin, Sakyo-ku,Kyoto, 606, Japan.
Received 2 July 1985 and in revised form 4 September 1985.Accepted 10 September 1985
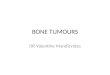
Case IA 63-year-old female was admitted because of right hemi-paresis, which began with right leg weakness about one weekbefore admission. Neurological examination on admissionrevealed a mildly decreased level of consciousness, and righthemiplegia including the face. The tongue was deviated tothe right, and pupils were anisocoric (right 3 mm, left25 mm), but reactive to light. Deep tendon reflexes wereexaggerated on the right side, combined with Babinski's sign.Extraocular movements were not limited, and she had nosensory deficits in all modalities. A CT scan showed a tha-lamic tumour on the left side extending through the midbraininto the pons ventrolaterally (fig 1).
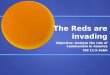
Case 2A 26-year-old male began to have occipital headache 2 yearsbefore admission, and gradually developed right arm weak-ness and unsteadiness of gait 1 year before admission, witha tendency to fall towards the right side when walking. InJune, 1983, hydrocephalus was found by CT and he wastreated with bilateral ventricular drainage, but neurologicaldeterioration continued. Dysarthric speech, dysphagia andfinally a locked-in syndrome developed. Communicationwas then possible only by eye movement. A CT scan showeda left sided brain stem tumour extending from the thalamus,locating mainly on the left side of the midbrain and the pons(fig 2).
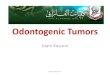
Case 3On 7 June, 1984, a 50-year-old female suddenly lost con-sciousness on a bus, followed by convulsive movements fora few minutes. No paresis was observed after the convulsion.She had also suffered from a similar episode 7 months earlier.Neurological examination revealed no abnormalities,although EEG showed sharp waves bilaterally, most promi-nent on the right frontal leads. A large tumour in the right
524
Protected by copyright.
on February 18, 2021 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.49.5.524 on 1 May 1986. D
ownloaded from

Thalamic tumours invading the brain stem produce crossed cerebellar diaschisis demonstrated by PET 525
Fig 1 Case 1. 63-year-oldfemale, sufferedfrom left Fig 2 Case 2. 26-year-old male with brain stem tumourthalamic tumour extending downwardly into the pons. Note involving the thalamus. Note also crossed cerebellarthat the right cerebellum and the left outer part of the pons diaschisis and contralateral brain stem suppression of CBFshow reduction of CBF and CMRO2 (arrow). Decreased CBF in the left temporal lobe Was dueto lower, CBF CMR02, OEF and CTscan. R in CTscan to partial volume effect originated from asymmetricalindicates right side of the brain and L left side. middle cerebralfossa. OEF image of the pons showed
remarkable bilateral reduction of OEF.tnalamus, extenumng upwara to tne corona raulaLa, wasshown by CT (fig 3).
Details of our PET scanner were reported elsewhere.' Inbrief, it has four rings of 192 bismuth germanate detectors,providing seven slices at one scan process. The best spatialresolution is 7 6 mm in full width halfmaximum at the centreof the scan field, and the axial resolution at the centre is12 mm. Blood sampling was performed two or three times ina scan process from the cannulation of the cubital artery, andoxygen- 15 activity in the whole blood and plasma, as well asarterial blood gases were determined. Prior to the study, a
transmission scan using 68Ge - 68Ga was performed for 20minutes for attenuation correction. Calibration factorsbetween PET scanner and well counter as well as that of crossplanes of PET scanner were obtained in every study. Cere-bral blood flow was measured by inhaling oxygen- 15 labelledcarbon dioxide 10-15 mCi per minute continuously throughthe mask, and CMRO2 and OEF of the brain by the con-tinuous inhalation of oxygen-15 labelled oxygen 20-30rmCiper minute. Scan data were collected for 5 to 7 minutes. Asingle breath of oxygen- 15 labelled carbon monoxide 80 mCi
Protected by copyright.
on February 18, 2021 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.49.5.524 on 1 May 1986. D
ownloaded from

526 Fukuyama, Kameyama, Harada, Fujimoto, Kobayashi, Taki, Ishikawa, Handa, Tanada, Torizuka
..~~~ ~ ~ ~ ~ ~ ~ h-7 R
Fig 3 Case 3. 50-year-old,female with minimalneurological complications. The tumour in the thalamuswithout contrast enhancement expands upwardly. Note no
crossed cerebellar diaschisis.
was used to measure cerebral blood volume (CBV). Calcu-lation of CBF, CMR02, and OEF was based on the steadystate method,8'- ' and CMR02 and OEF were corrected byCBV value." 12
Image data were processed with a Hitachi image pro-
cessing computer using system subroutines, in order toreconstruct functional images constituting 128 x 128 pixelsand calculate mean CBF, CMR02 and OEF of eachcerebellar hemisphere. The region of interest was determinedusing light pen on both cerebellar hemisphere excludingvermis, so as to cover about 100-150 pixels.
Results
The normal value of CBF in both cerebellar hemi-spheres from 18 normal volunteers was 39 5 + 9-6(mean + standard deviation) ml/lOOml/min, that ofCMR02 2-72 + 049 ml/100 mi/min and that of OEF0 377 + 0-079.
In case 1, cerebellar hemispheric CBF on thecontralateral side to the tumour was 28-5 + 4-2, whilethat on the ipsilateral side was 38 1 + 4 9. CMR02showed the same tendency; CMR02 on the con-tralateral side was 2-07 + 0-38 and on the ipsilateralside 2 59 +046, while ipsilateral OEF was0 43 + 0.057 and contralateral was 0 40 + 0-054 (fig1). Case 2 revealed that CBF on the contralateral sideto the tumour was 16-0+ 3-7 and on the ipsilateral side23-2 + 2 5, CMR02 was 1-07 + 0 42 and 1 44 + 0-28and OEF was 0-326 + 010 and 0-352 + 0-06respectively (fig 2). Those two cases had invasion ofthe tumour into the midbrain and the pons. In case 2,CBF and CMR02 decreased remarkably in both cere-bellar hemispheres compared with normal values, butmore marked reduction was noticed on the side con-tralateral to the tumour. On the other hand, case 3,which showed no tumour invasion into the brain stem,had a normal range of CBF and CMR02, that is47-9 + 9-9 in the right cerebellar hemispheric CBFand 48-0 + 13 2 in the left, 2-85 + 0-63 in the rightCMR02 and 2-79 + 0 79 in the left and 0-378 + 0 034in the right OEF and 0-368 + 0-031 in the left.
Cases 1 and 2 also seemed to show a moderatedegree of reduction in blood flow and oxygen con-sumption within the pons ipsilateral side of thetumour, but these findings were not convincingbecause of the poor spatial resolution of the PETscanner. The decreased area of CBF in the ponsobserved by PET, however, coincided with thetumour density of the CT scan, while CMR02 in thepons of both cases, was reduced to remarkably lowlevels compared to CBF: laterality was less con-spicuous, which could be ascribed to a remarkablereduction ofOEF in the pons especially in case 2. Onthe other hand, case 3 without crossed cerebellardiaschisis exhibited symmetrical CBF, CMR02 andOEF patterns of the pons.
Clinical records showed that case I and 2 withcrossed cerebellar diaschisis showed definite hemi-plegia or quadriplegia, in contrast to case 3 who hadno remarkable neurological deficits.
Discussion
Diaschisis was first reported by Von Monakowaround the turn of this century.'3 He reported thatstructures remote from a primary lesion in the centralnervous system was functionally suppressed by some
Protected by copyright.
on February 18, 2021 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.49.5.524 on 1 May 1986. D
ownloaded from

Thalamic tumours invading the brain stem produce crossed cerebellar diaschisis demonstrated by PET 527
neuronal mechanisms. Crossed cerebellar diaschisishas been defined as cerebellar suppression of the CBFon the side contralateral to a supratentorial lesion.Supratentorial lesions, due to cerebrovascular disor-ders or cerebral tumours have been investigated byPET scan, as first reported by Baron et al.' 2 CBF,CMR02 and metabolic rate of glucose of cerebellarhemisphere were reduced on the side contralateral tothe supratentorial lesion, mainly located in the frontalor parietal lobes.4'5 These reports favoured thehypothesis that crossed cerebellar diaschisis might becaused by the damage of the descending fibres fromthe cerebral cortex to the pontine nuclei, but no directevidence was presented. In another report, deeplyseated brain tumours did not show crossed cerebellardiaschisis, but the authors stressed the importance ofdescending fibre systems from the cerebral cortex.6
Afferent fibres to the cerebellum, mainly from thefrontal and parietal cortex, descend with pyramidalfibres and end on the ipsilateral pontine nuclei; somepart of these fibres descend further onto the inferiorolivary nuclei. These nuclei project their fibres trans-versely to the contralateral cerebellar hemisphere. Onthe other hand, efferent fibres from the cerebellumoriginate from the dentate nucleus, crossing the mid-line in the superior cerebellar peduncle. Some of thefibres terminate in the contralateral red nucleus. Theremaining fibres end in the ventrolateral nucleus ofthethalamus, which projects diffusely to the cerebral cor-tex as the thalamic radiations.14 On the basis of thesefibre connections, we can say that fibres and nuclei inthe pons relate only to descending fibres from thecerebral cortex. Therefore, the asymmetricaldifference of CBF found in the pons supports thehypothesis that abnormal function of descendingtracts produces crossed cerebellar diaschisis.No asymmetry was found on OEF of the cerebellar
hemisphere in any cases, which suggests that CBF andCMR02 were not decreased by ischaemia producedby the pressure of the tumour. The remarkable bilat-eral reduction of OEF in the pons in case 2 maysuggest either mass effect of the tumour or directinvasion into the contralateral side, which coincidedwith the clinical finding of a locked-in syndrome.Therefore, in this case, bilateral reduced cerebellarhemispheric CBF and CMR02 compared withnormal values, but more pronounced on the side con-tralateral to the tumour, were partly due to increasedintracranial pressure in the posterior fossa and partlydue to bilateral fibre disconnection between cerebellarand cerebral cortex.
In single photon emission CT by the Xe-133inhalation method, it has been reported that manycases of putaminal haemorrhage show more frequentsuppression of contralateral cerebellar blood flowthan cases of thalamic haemorrhage.l5 This result is
supportive evidence that crossed cerebellar diaschisismight be caused by the damage of descending fibresfrom the cerebral cortex to the cerebellum.
Cases 1 and 2 with crossed cerebellar diaschisispresented the definite motor palsy, in contrast to case3 without crossed cerebellar diaschisis who showedminimal neurological deficits. Considering theintimate relationship of corticopontine fibres withcorticospinal and corticobulbar fibres, these clinicalfindings also suggest that crossed cerebellar diaschisiscan result from damage of the descending fibres fromthe cerebral cortex. This accords with Patronas' clin-ical observation.6Our results, along with the anatomical consid-
erations, suggest that descending fibres from the cere-bral cortex, invaded or destroyed at the brain stemlevel, suppressed the pontine nuclei which theninfluenced the function of the contralateral side of thecerebellar hemispheres. Therefore, it can be inferredthat the descending fibres play a more important rolein producing crossed cerebellar diaschisis than theascending fibres from the cerebellum.
References
Baron JC, Bousser MG, Comar D, Castaigne P. "Crossedcerebellar diaschisis" in human supratentorial braininfarction. Ann Neurol 1980;8:128.
2 Baron JC, Bousser MG, Comar D, Castaigne P. "Crossedcerebellar diaschisis" in human supratentorial braininfarction. Trans Am Neurol Assoc 1980;105:459-61.
3Lenzi G-L, Frackowiak RSJ, Jones T. Cerebral oxygenmetabolism and blood flow in human cerebral ischemicinfarction. J Cerebr Blood Flow Metab 1982;2:321-35.
'Martin WRW, Raichle ME. Cerebellar blood flow andmetabolism in cerebral hemisphere infarction. AnnNeurol 1983;14:168-76.
' Kushner M, Alavi A, Reivich M, et al. Contralateralcerebellar hypometabolism following cerebral insult: Apositron emission tomographic study. Ann Neurol1984; 15:425-34.
6Patronas NJ, Di Chiro G, Smith BH, et al. Depressedcerebellar glucose metabolism in supratentorialtumours. Brain Res 1984;291:93-101.
7Senda M, Tamaki N, Yonekura Y, et al. Performancecharacteristics of Positologica III: a whole bodypositron emission tomograph. Stroke 1985;9:940-6.
'Jones T, Chesler DA, Ter-Pogossian MM. The continuousinhalation of oxygen-15 for assessing regional oxygenextraction in the brain of man. Br J Radiol1976;49:339-43.
9 Frackowiak RSJ, Lenzi G-L, Jones T, Heather JD. Quan-titative measurement of regional cerebral blood flowand oxygen metabolism in man using 1"O and positronemission tomography: Theory, procedure, and normalvalues. J Comput Assist Tomogr 1980;4:727-36.
0 Lammertsma AA, Jones T, Frackowiak RSJ, Lenzi G-L.
Protected by copyright.
on February 18, 2021 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.49.5.524 on 1 May 1986. D
ownloaded from

528 Fukuyama, Kameyama, Harada, Fujimoto, Kobayashi, Taki, Ishikawa, Handa, Tanada, Torizuka
A theoretical study of the steady-state model for mea-suring regional cerebral blood flow and oxygen util-isation using oxygen-15. J Comput Assist Tomogr1981;5:544-50.
l Lammertsma AA, Jones T. Correction for the presence ofintravascular oxygen- 15 in the steady-state techniquefor measuring regional oxygen extraction ratio in thebrain: 1. Description of the method. J Cereb Blood FlowMetab 1983;3:416-24.
12Lammertsma AA, Wise RJ, Heather JD, et al. Correctionfor the presence of intravascular oxygen-15 in thesteady-state technique for measuring regional oxygen
extraction ratio in the brain: 2. Results in normal sub-jects and brain tumour and stroke patients. J CerebBlood Flow Metab 1983;3:425-31.
13von Monakow C. Die Lokalisation im Grosshirn und derAbbau der Funktion durch kortikale Herde. Wiesbaden,Bergmann, 1914.
"Brodal A. Neurological Anatomy in Relation to ClinicalMedicine. 3rd ed. New York: Oxford University Press,1981:294-393.
Kanaya H, Endo H, Sugiyama T, Kuroda K. "Crossedcerebellar diaschisis" in patients with putaminal hemor-rhage. J Cereb Blood Flow Metab 1983;3(suppl 1):S27-8.
Protected by copyright.
on February 18, 2021 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.49.5.524 on 1 May 1986. D
ownloaded from