Embed Size (px)
Citation preview

Research www.AJOG.org
OBSTETRICS
The incidence of preeclampsia and eclampsia and associatedmaternal mortality in Australia from population-linkeddatasets: 2000-2008Charlene Thornton, PhD; Hannah Dahlen, PhD; Andrew Korda, FRANZCOG; Annemarie Hennessy, PhD
OBJECTIVE: To determine the incidence of preeclampsia and 2008 was 1.9 (95% confidence interval, 1.28e2.92) when compared
eclampsia and associated mortality in Australia between 2000 and2008.STUDY DESIGN: Analysis of statutorily collected datasets of singletonbirths in New South Wales using International Classification of Diseasecoding. Analyzed using cross tabulation, logistic regression, andmeans testing, where appropriate.
RESULTS: The overall incidence of preeclampsia was 3.3% with adecrease from 4.6% to 2.3%. The overall rate of eclampsia was 8.6/10,000 births or 2.6% of preeclampsia cases, with an increase from2.3% to 4.2%. The relative risk of eclampsia in preeclamptic women in
From the, School of Medicine (Drs Thornton,Korda, and Hennessy), and the School ofNursing and Midwifery (Dr Dahlen), University ofWestern Sydney, Sydney, NSW, Australia.
Received Nov. 12, 2012; revised Jan. 5, 2013;accepted Feb. 25, 2013.
The authors report no conflict of interest.
Reprints: Charlene Thornton, PhD, University ofWestern Sydney, School of Medicine, LockedBag 1797, Penrith South DC NSW,Australia 1797. [email protected].
0002-9378/$36.00ª 2013 Mosby, Inc. All rights reserved.http://dx.doi.org/10.1016/j.ajog.2013.02.042
476.e1 American Journal of Obstetrics & Gynecology JUNE 2013
with the year 2000. The relative risk of a woman with preeclampsia/eclampsia dying in the first 12 months following birth compared withnormotensive women is 5.1 (95% confidence interval, 3.07e8.60).
CONCLUSION: Falling rates of preeclampsia have not equated to adecline in the incidence of eclampsia. An accurate rate of both pre-eclampsia and eclampsia is vital considering the considerablecontribution that these diseases make to maternal mortality. Theidentification and treatment of eclampsia should remain a priority inthe clinical setting.
Key words: eclampsia, incidence, maternal mortality, preeclampsia
Cite this article as: Thornton C, Dahlen H, Korda A, et al. The incidence of preeclampsia and eclampsia and associated maternal mortality in Australia frompopulation-linked datasets: 2000-2008. Am J Obstet Gynecol 2013;208:476.e1-5.
eported rates of preeclampsia and
R eclampsia in developed countriesvary significantly. The preeclampsia rateis commonly quoted in the literature asbeing anywhere between 5% and 8% ofall pregnancies worldwide, althoughmore recently lower rates of 2-8% arebeing cited.1,2 Geographic variation,varying definitions of the disease and thesize of data sources used largely accountfor these variations3 although seasonalvariation at birth and time of conceptionhave also been postulated as explana-tions of rate variations.4Eclampsia rates also vary significantlyin the literature. In Europe rates of 2-3cases per 10,000 births are quoted5,6
although rates in developing countriesare between 16-69 per 10,000 births.7
Knight3 quotes 2.7/10,000 births in a12-month surveillance of all maternityunits in the United Kingdom in2005/2006, although an earlier surveil-lance study in the Unitd Kingdom in19928 resulted in a rate of 4.9/10,000.Worldwide, 12% of maternal deaths areattributed to eclampsia9 with a casefatality rate of 3-5% in developingcountries.10 The Australasian MaternityOutcomes Surveillance System (AMOSS)is currently conducting a surveillance ofeclampsia in Australia in 2011, althoughreporting of cases to AMOSS is voluntaryand results are to date, not available.Effective detection and treatment of
preeclampsia and eclampsia within anycountry or health region should at leastbe influenced by clinician’s knowledgeof the incidence of the disease withintheir area of practice. The aim of thisstudy was to determine the incidenceof both preeclampsia and eclampsia inthe largest populated area of Australia
(which contributes to be over one thirdof all Australian births), the variationsover time periods and maternal mortal-ity subsequent to diagnosis within a12-month period following birth.
MATERIALS AND METHODS
Data sourcesBirth data includingmaternal age, parity,delivery type, smoking status, andneonatal outcomes for the period July 1,2000, till June 30, 2008, of all singletonbirths was provided by New South Wales(NSW), Australia, Department of Healthas recorded in the NSW MidwivesData Collection (MDC). This popula-tion based surveillance system containsmaternal and infant data on all birthsof greater than 400 g birthweight or20 weeks’ gestation and covers over one-third of births that occur in Australia.1
The NSW MDC contains statistics on33% of births that occur in Australiaannually. This dataset (NSW MDC)was linked to the Admitted PatientData Collection (APDC) and the NSWRegistry of Births, Deaths and Marriages(BDM). The APDC records all admittedpatient services provided by NSW Public

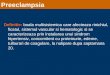
FIGURE 1Cases of preeclampsia expressed as a percent of all births and eclampsiaexpressed as a percent of all preeclampsia cases
Thornton. Incidence of preeclampsia and eclampsia in Australia 2000-2008. Am J Obstet Gynecol 2013.
www.AJOG.org Obstetrics Research
Hospitals, Public Psychiatric Hospitals,Public Multi-Purpose Services, PrivateHospitals, and Private Day ProceduresCentres. The BDM is a record of allbirths, deaths and marriages that occurin NSW. The incidence of preeclampsiaand the incidence and timing of event inrelation to birth of eclampsia was pro-vided by the APDC using the Interna-tional Classification of Diseases Coding(ICD-10-Australian Modification) thathas been in use in the Australian settingsince 1998. The codes O14.0, O14.1,O14.2, and O14.9 were used to identifythe cases of preeclampsia and are thosethat refer to new onset proteinurichypertension. The codes O15.0, O15.1,O15.2, and O15.9 were used to identifythe cases of eclampsia and the timingof the seizure in relation to the deliveryof the infant. Cause of death was ob-tained from ICD-10 codes as recordedon the death certificate and located in theBDM registry. Linkage of the datasetswas conducted by the New South WalesCentre for Health Record Linkage(CHeReL). Probabilistic data linkagetechniques were used for these purposesand deidentified datasets were providedfor analysis. Probabilistic record linkagesoftware works by assigning a “linkageweight” to pairs of records. For example,records that match perfectly or nearlyperfectly on first name, surname, date ofbirth, and address have a high linkageweight, and records that match only ondate of birth have a low linkage weight. Ifthe linkage weight is high it is likely thatthe records truly match, and if the link-age weight is low it is likely that therecords are not truly a match. Thistechnique has been shown to have a falsepositive rate of 0.3% of records.11 Ethicalapproval was obtained from the NSWPopulation and Health Services ResearchEthics Committee, protocol no. 2010/12/291.
SubjectsThe MDC dataset for this period con-tains the antenatal, birth, and postnataldetails on 691,738 births during thisperiod. The APDC contains >1.7million admissions for the same womenoccurring after the index pregnancy. TheBDM registry contains death data on 97
women who died within 12 monthsfollowing delivery.
Data analysisIncidence and demographic data wascalculated. Contingency table analyses,Student t tests and analyses of variance(ANOVA) were used to examine differ-ences between the pregnancies coded aspreeclamptic/eclamptic and those not.Binary logistic regression modellingwas also undertaken. Significance wasdetermined <0.05 level. All analyseswere conducted using IBM SPSS v.20(IBM, Armonk, NY).
RESULTS
There was an overall preeclampsia rate of3.3% of singleton births (22,827 casesfrom 691 738 births) (Figure 1 for ratevariations between year 2000 and 2008).There has been a decrease in the inci-dence of preeclampsia in this setting of50% over this period, with a continuoustrend of decline occurring (c2, P<.001).In total there were 597 episodes ofseizure in 529 pregnancies. Fifty-fivewomen experienced >1 seizure in the 1pregnancy and 4 women experienced aseizure in 2 pregnancies. This equates toan overall seizure event rate of 8.6/10,000births. Between the years 2000 and
JUNE 2013 Ameri
2008, there has been no change in theincidence of eclampsia (0.1% of allbirths in 2000 and 2008) (Figure 1). Theoverall eclampsia rate in women withpreeclampsia was 2.6% or 237/10,000births effected by preeclampsia, with anincrease from 2.3% in the year 2000 to4.2% in 2008 (c2, P¼ .007). The relativerisk of eclampsia in women with pre-eclampsia in 2008 was 1.9 (95% confi-dence interval [CI], 1.28e2.92) whencompared with the year 2000. Seventy-three percent of seizures occurred inprimiparous women (c2, P< .0001) andwhen an examination of parity and therelationship to seizure occurrence wasundertaken (following logistic regres-sion adjustment for age and smokingstatus) the odds ratio (OR) of a pri-miparous woman experiencing a seizurewhen compared with a multiparouswomanwas 4.5 (95%CI, 3.55e5.63). Ananalysis of the risk of seizure in 2008compared with 2000 for all womenwhenadjusted formaternal age, gestational ageat birth, smoking, and parity did notshow a significant increase in risk overthe period of the study (OR, 1.86; 95%CI, 0.52e6.72).
Table 1 displays the time when theevent occurred, with the majority ofseizures occurring during labor (44.1%).
can Journal of Obstetrics & Gynecology 476.e2

TABLE 1Occurrence of seizureWhen seizureoccurred
Percent ofall episodes
Antenatally 25.1%
During labor 44.1%
Postnatally 26.3%
Not specified to venue 4.5%
Thornton. Incidence of preeclampsia and eclampsiain Australia 2000-2008. Am J Obstet Gynecol 2013.
Research Obstetrics www.AJOG.org
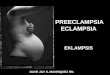
The unadjusted RR of a seizure occur-ring in all women postnatally following abirth via caesarean section comparedwith a vaginal birth was 2.9 (95% CI,2.14e3.99. An analysis of the time frombirth to seizure was undertaken anddisplayed in Figure 2. The majority ofwomen experienced eclampsia on theday of birth (53%). Median time foreclampsia was zero days (day of birth),range, 0e55 days. When the cases thatoccurred following the day of birth were
FIGURE 2Time between birth and occurrence ocases occurring during delivery or po
Thornton. Incidence of preeclampsia and eclampsia in Australia
476.e3 American Journal of Obstetrics & Gynecol
examined, the median day of postnatalseizure occurrence was day 4 (range,1e55).Maternal characteristics and neonatal
outcomes are described in Table 2. Thistable demonstrates that women witheclampsia were younger, more likely tobe primiparous, delivered at earlier ges-tations, and their infants suffered higherneonatal mortality.The seasonal variation of eclampsia
was explored and when examined inrelationship to the number of births thatoccurred within each season, there wasno statistical difference in the incidenceof eclampsia based on season of seizureoccurrence (c2, P ¼ .35).Of all cause maternal deaths that
occurred within the 12-month periodfollowing delivery (n ¼ 97), 18% (n ¼17) had experienced preeclampsia. Ofthe 30 early deaths (within 42 days ofbirth) attributed to medical causes(nonviolent deaths), 17% (n ¼ 5) hadexperienced preeclampsia. The recordedreason (with n ¼ 1 for each cause):
f eclampsia as a percentage of allstnatally
2000-2008. Am J Obstet Gynecol 2013.
ogy JUNE 2013
surgical misadventure, multiorgan fail-ure, intracranial hemorrhage, ruptureduterus, and aortic dissection. Thisequates to a RR for women with pre-eclampsia/eclampsia dying in the first12 months following birth when com-pared with normotensive women of5.1 (95% CI, 3.07e8.60). The NeonatalMortality Rate for infants of womenwith eclampsia was 22.3/1000 and 10.7/1000 for infants of women with pre-eclampsia compared with 7.9/1000 forthe normotensive cohort.
COMMENT
This paper reports a mean preeclampsiarate of 3.3% of all singleton pregnanciesover an 8-year period and eclampsia inthis setting has an incidence of 8.6/10,000 births. These figures are similar tothe world pooled estimate of 3.4%10 andcomparable with that seen in Norway.12
The discrepancy in rates of pre-eclampsia between developed and devel-oping countries and between developingcountries is because of a number of fac-tors including the significant variation inthe quality and accessibility of care andthe variations in reporting methods andstandards. The size of the dataset fromwhich rates are calculated greatly influ-ence the reliability of the data and forthis reason, population-based datasetssuch as this which rely on standardizedcoding and are validated for reliabilityare optimal for calculating disease inci-dence. The issue around consensus ofdiagnostic features is also contentiouswhen defining preeclampsia. This paperused the “research definition” as estab-lished by Redman and Jefferies13 ofpregnancy onset proteinuric hyperten-sion in comparison to the definitionsfound within the SOMANZ guidelines14
that include nonproteinuric variationsof preeclampsia, although it has beenreported that in 77% of cases, womenwith preeclampsia diagnosed undermoreinclusive definitions do have proteinuriaas a diagnostic factor.15
The declining rate of preeclampsiaover the study period (4.6% to 2.4% ofall births) is of great interest. Potentialreasons for this could be an improve-ment in the early identification ofcases over time with the initiation of

TABLE 2Details of women with and without eclampsia
VariableEclampsian [ 529
Preeclampsiawithout eclampsian [ 22,298
Nonhypertensiven [ 668,911 P value
Agea 28.7 (6.31) 29.5 (5.86) 30.2 (5.58) < .001
Primiparousb 73.2% 45.0% 41.6% < .001
Smoked during pregnancyb 13.9% 8.2% 14.8% < .001
Gestation at deliverya 37.6 (3.27) 37.9 (2.84) 39.1 (2.06) < .01
Vaginal birthb 49.8% 40.5% 73.8% < .001
Neonatal mortality rateb 22.3/1000 10.7/1000 7.9/1000 < .001a Mean, standard deviation, and ANOVA; b c2 analysis.
Thornton. Incidence of preeclampsia and eclampsia in Australia 2000-2008. Am J Obstet Gynecol 2013.
www.AJOG.org Obstetrics Research
medication at earlier gestations tomaintain blood pressure control atacceptable limits or the shift away fromblood pressure management from theinpatient to the outpatient setting witha subsequent decrease in the likelihoodof a preeclampsia diagnosis beingrecorded on the birth admission. It couldalso be postulated that women withmilder forms of disease are now lessprevalent or are being omitted from thecoding systems because of an increase inmore women with more severe diseasemanifestations. Earlier treatments couldalso have resulted in more womenreceiving a diagnosis of gestationalhypertension rather than preeclampsia.It could also be postulated that in-creasing rates of induced labors andelective caesarean sections, and associ-ated birth at earlier mean gestations,16
are resulting in a fall in preeclampsiacases because of a reduction in theperiod required for women to developand display disease manifestations, prac-tices that effectively reduce the occur-rence of cases that would have presentedin postdate pregnancies.
The 4.2% eclampsia rate (expressed asa percentage of preeclampsia cases) atthe end of the study period was higherthan that reported in the greater major-ity of developed countries10 with therelative risk for women with pre-eclampsia suffering an eclamptic seizurealmost doubling between the years 2000to 2008. This increase reflects globaltrends reported by the World HealthOrganization, with an increase from0.1% to 0.8% of live births affected byeclampsia in developing countries over a10-year reporting period.10 In our study,this equated to an overall eclampsia rateover the 8-year period of 8.6/10,000births with no change between 2000and 2008. This finding is in contrastwith falling eclampsia rates reportedin both Canada (12.4 to 5.9/10,000births between 2003 and 2009)17 and theUnited States (6.34 to 4.80/10,000delivery hospitalizations between 1998and 2008).18 The latter study did reportan increase in postpartum eclampsiafrom 1.76 to 2.8 cases/10,000 deliveryhospitalization during the same period.These results would also support the
argument that the incidence of pre-eclampsia and eclampsia are not posi-tively correlated and that identificationof impending eclampsia and treatmentvariations differ significantly betweenobstetric units and countries.Vigilance and the use of magnesium
sulphate (MgSO4) have well been iden-tified as the most effective tools toprevent eclampsia,19 although the useof MgSO4 has come under considerablecriticism because of a perceived toxicityassociated with its use.20-22 In Australiathere has not been any adverse drugreactions from MgSO4 reported tothe Australian Government TherapeuticGoods Administration.23 In contrast, theInstitute of Safe Medication Practices22
in the US maintains a database ofincidents relating to MgSO4 of whichthere are more than 50 cases, some ofwhich resulted in maternal death orpersistent vegetative state involving theuse of MgSO4 diluted in intravenousfluids.There are both short- and potential
long-term sequelae of having experi-enced an eclamptic seizure. A study thatfollowed women 6-24 months afterthey experienced an eclamptic seizure24
reported that 10% of women reportedpersistent amnesia, 22% reported loss ofmemory, 11% experienced visual dis-turbances, and 10% had ongoing head-aches. Long-term consequences mayinclude structural changes to the whitematter of the brain, with lesions seenin 40% of women and loss of cerebraltissue in 25% of women 6 weeks
JUNE 2013 Ameri
postpartum.25-27 So although there wasno mortality associated with eclampsiaduring this study, eclampsia does causesignificant long-term morbidity. Mag-nesium sulphate usage differed signifi-cantly between obstetric units in NewSouth Wales15 from 2.4%-18.0% of allwomen with preeclampsia. Worldwidethe use of MgSO4 also varies greatly.
Seasonal variation found in this studywas in contrast with those found inearlier work where the incidence ofeclampsia is greatest when in seasonswhen the temperature is lowest.4,5
There could be a number of reasons forthis including the statistical power ob-tained from a dataset of this size or therelative narrow range of temperatureexperienced within the state of NSWover a 12-month period (32�F variationbetween mean winter and summertemperatures).
In this study, almost 17% (n ¼ 5) ofdirect maternal deaths were in womenwho had preeclampsia. This figurereflects what occurs worldwide, with10-15% of direct maternal deaths attri-buted to preeclampsia in both developedand developing countries.2,28 Neonatalmortality rates of 22.3/1000 for infantsborn to mothers with eclampsia in thisstudy compares favorably with rates of60/1000 in other developed countries.6
This study used ICD-10-AM codingwith a narrow definition of preeclampsiaand a collection period encompassing691,738 births providing robust dataconcerning the epidemiology of pre-eclampsia in Australia. Themethodology
can Journal of Obstetrics & Gynecology 476.e4

Research Obstetrics www.AJOG.org
used in the work is of course only asreliable as the datasets sourced. The useof data linkage methodology has beenvalidated previously with a false-positiverate of 0.03% of cases.11 Data linkage hasimproved the ascertainment of cases inother studies concerning maternal mor-tality, with reports of up to 55% in-creases in case identification using thismethodology.29 The risk with all largeroutinely collected datasets is thatmore complex medical complications ofpregnancy are more likely to be incor-rectly coded, as supported by validationstudies undertaken30-32 but previouswork using population datasets to iden-tify preeclampsia cases reported speci-ficities >99%.33 This has to be balancedin comparison to smaller datasets, whichalthough may have greater accuracy ofdiagnosis, are more likely to reportType II errors and are less likely to actu-ally represent what is occurring on apopulation level. This study also does notinclude data on multiple pregnancies,which are affected more frequently bypreeclampsia and may increase overallrates of disease.
The incidence of preeclampsia hasaltered over the past 2 decades and cur-rent disease rates need to be used in anyfuture discussion. Comparison of data-sets such as these on an internationalstage would provide a statistical basis,enabling a robust disease profile to beestablished. Considering the role playedby eclampsia in maternal and infantmorbidity and mortality increasing ratesshould be of concern to all clinicians, asvigilance and prophylaxis are the onlytools to prevent eclampsia. It wouldappear that more efficient surveillanceof women with preeclampsia is urgentlyrequired as this will influence treat-ments, including the timely use ofMgSO4 where required. -
REFERENCES
1. Australian Bureau of Statistics. Births 2010.ABS, Canberra, Australia.2. World Health Organization InternationalCollaborative Study of Hypertensive Disordersof Pregnancy. Geographic variation in the
476.e5 American Journal of Obstetrics & Gynecol
incidence of hypertension in pregnancy. Am JObstet Gynecol 1988;158:80-3.3. Knight M. Eclampsia in the United Kingdom.BJOG 2005;114:1072-8.4. Rylander A, Lindqvist P. Eclampsia is moreprevalent during the winter season in Sweden.Acta Obstet Gynecol Scand 2011;1:114-7.5. Subramaniam V. Seasonal variation in theincidence of preeclampsia and eclampsia intropical climatic conditions. BMC Women’sHealth 2007;7:18.6. Kullberg G, Lindeberg S, Hanson U.Eclampsia in Sweden. Hypertens Pregnancy2002;21:13-21.7. Altman D, Carroli G, Duley L, Magpie TrialCollaboration Group. Do women with pre-eclampsia, and their babies, benefit frommagnesium sulphate? The Magpie Trial: arandomised placebo-controlled trial. Lancet2002;359:1877-90.8. Douglas KA, Redman CWG. Eclampsia in theUnited Kingdom. BMJ 1994;309:1395-9.9. World Health Organisation. The World HealthReport 2005: Make every mother and childcount. Geneva: World Health Organization;2005.10. Dolea C, AbouZahr C. Global burden ofhypertensive disorders of pregnancy in the year2000.Geneva:WorldHealthOrganisation; 2003.11. Centre for Health Record Linkage. Qua-lity assurance report. [Internet] 2012. Avail-able at: http://www.cherel.org.au/media/24160/qa_report_2012.pdf. Accessed Oct. 22, 2012.12. Klungsoyr K, Morken NH, Irgens L,Vollset SE, Skjaerven R. Secular trends in theepidemiology of pre-eclampsia throughout 40years in Norway: prevalence, risk factors andperinatal survival. Paed Perinat Epi 2012;26:190-8.13. Redman CWG, Jefferies M. Revised defini-tionofpre-eclampsia.Lancet1988;8589:809-15.14. Lowe SA, Brown MA, Dekker G, et al.Guidelines for the management of hypertensivedisorders of pregnancy [Internet] 2008. Avail-able at: http://www.somanz.org/pdfs/somanz_guidelines_2008.pdf. Accessed June 26, 2012.15. Thornton C. Benchmarking the hyper-tensive disorders of pregnancy [PhD thesis].Sydney, NSW: University of Western Sydney;2011.16. Mealing NM, Roberts CL, Ford JB,Simpson JM, Morris JM. Trends in induction oflabour, 1998-2007: a population-based study.ANZ J Obstet Gynaecol 2009;49:599-605.17. Liu S, Joseph KS, Liston RM. Incidence,risk factors, and associated complications ofeclampsia. Obstet Gynecol 2011;118:987-94.18. Callaghan William M, Creanga Andreea A,Kuklina Elena V. Severe maternal morbidityamong delivery and postpartum hospitalizationsin the United States. Obstet Gynecol 2012;120:1029-36.19. Duley L, Gulmezoglu AM, Henderson-Smart DJ, Chou D. Magnesium sulphate
ogy JUNE 2013
and other anticonvulsants for women withpre-eclampsia. Cochrane Database SystemRev [Internet] 2005. Available at: http://www.mrw.interscience.wiley.com.cochrane/clsysrev/articles/CD000025/frame.html. Accessed June26, 2012.20. Yeast JD, Halberstadt C, Meyer BA,Cohen GR, Thorp JA. The risk of pulmonaryoedema and colloids osmotic pressure changesduring magnesium sulfate infusion. Am J ObstetGynecol 1993;169:1566-71.21. Benedetti T, Kates R, Williams V. Hemody-namic observations in severe preeclampsiacomplicated by pulmonary oedema. Am JObstet Gynecol 1985;152:330-4.22. Rice SK. Minimizing risk of magnesiumsulfate overdose in obstetrics. Am J MaternChild Health 2006;31:340.23. Australian Government Department ofHealth and Aging. Therapeutic goods adminis-tration Australia [Internet] 2008. Available at:http://www.tga.gov.au. Accessed June 26,2012.24. Andersgaard A, Herbst A, Johansen M,Borgstrom A, Bille A, Oian P. Follow-upinterviews after eclampsia. Gynecol ObstetInvestig 2009;67:49-52.25. Loureiro R, Leite CC, Kahhale S. Diffusionimaging may predict reversible brain lesionsin eclampsia and severe preeclampsia: initialexperience. Am J Obstet Gynecol 2003;189:1350-5.26. Demirtas O, Gelal F, Vidinli BD. Cranial MRimaging with clinical correlation in preeclampsiaand eclampsia. Diagn Interv Radiol 2005;11:189-94.27. Zeeman G. Neurologic Complications ofpre-eclampsia. Semin Perinat 2009;33:166-72.28. KhanKS,Wojdyla D, Say L.WHOanalysis ofcauses of maternal death: a systematic review.Lancet 2006;367:1066-74.29. Cliffe S, Black D, Bryant J, Sullivan E.Maternal deaths in New South Wales, Australia:a data linkage project. ANZ J Obstet Gynaecol2008;48:255-60.30. Roberts CL, Bell JC, Ford JB, Hadfield RM,Algert CS, Morris JM. The accuracy of reportingof the hypertensive disorders of pregnancy inpopulation health data. Hypertens Pregnancy2008;27:285-97.31. PymM, Taylor L. Validation study of the NewSouth Wales midwives data collection 1990.Public Health Bull Suppl 1993;5-8:1-6.32. Thornton C, Makris A, Ogle R, Hennessy A.Generic obstetric database systems are unreli-able for reporting the hypertensive disorders ofpregnancy. ANZ J Obstet Gynaecol 2004;44:505-9.33. Chen JS, Roberts CL, Simpson JM,Ford JB. Prevalence of pre-eclampsia, preg-nancy hypertension and gestational diabetesin population-based data: impact of differentascertainment methods on outcomes. ANZ JObstet Gynaecol 2012;52:91-5.