Embed Size (px)
Citation preview

The Management of Giant Retinal Tears Using Perfluoroperhydrophenanthrene A Multicenter Case Series
Peter J. Kertes, MD, Hussein Wafapoor, MD, Gholam A. Peyman, MD, Nassim Calixto, Jr, MD, Hilary Thompson, PhD, Vitreon Collaborative Study Group
Objective: The purpose of the study was to determine the predictors of success and evaluate the use of perfluoroperhydrophenanthrene as an intraoperative and postoperative tool in the management of giant retinal tears in a multicentered collaborative study.
Design: Multicentered prospective case series. Participants: Twenty-three centers consecutively enrolled 162 eyes of 161 patients
with retinal tears 900 or greater in circumferential extent. Intervention: Perfluoroperhydrophenanthrene was used as an intraoperative surgi
cal adjunct in all cases and left after surgery in 16 eyes (9.9%). Main Outcome Measures: Retinal reattachment and visual acuity. Results: Intraoperative reattachment was achieved in 158 eyes (97.5%); 147 eyes
(90.7%) remained attached at their most recent follow-up. Seventy-nine eyes (48.8%) experienced an improvement in their visual acuity, 26 eyes (16.0%) remained unchanged, and 57 (35.2%) worsened. Recurrent retinal detachment occurred in 80 patients (49.4%). Other significant postoperative complications included cataract formation in 20 (39.2%) of 51 eyes, macular pucker in 12 (7.4%), corneal decompensation in 10 (6.2%), and hypotony (intraocular pressure equal to or less than 5 mmHg) in 9 (5.6%). A chi-square analysis of preoperative characteristics showed that hypotony (P = 0.007), macular detachment (P = 0.020), a history of cataract extraction (P = 0.003), poor visual acuity (P = 0.000), giant tear extent greater than 1800 (P = 0.004), and higher grade proliferative vitreoretinopathy (P = 0.000) all predicted a poor visual outcome. Vitreon (Vitro phage , Inc., Lyons, IL) was left in 16 eyes (9.9%) for an extended postoperative retinal tamponade for between 3 and 1034 days (mean, 87.2 days). The Vitreon was well tolerated, and these eyes experienced a similar outcome and rate of retinal reattachment to the rest of the group.
Conclusions: Vitreon is a safe and useful adjunct to pars plana vitrectomy in the management of giant retinal tears and may, additionally, be the perfluorocarbon liquid that can be used most safely as a temporary postoperative tool for extended retinal tamponade, reinforcing its role as a useful adjunct in the management of these complex retinal detachments. Ophthalmology 1997; 104: 1159-1165
Originally received: August 27, 1996. Revision accepted: March 5, 1997.
From the LSU Eye Center. Louisiana State University Medical Center School of Medicine, New Orleans, Louisiana.
EY02377 from the National Eye Institute, National Institutes of Health, Bethesda, Maryland, and by an unrestricted departmental grant from Research to Prevent Blindness, New York, New York.
Presented at the Annual Meeting of the Association for Research in Vision and Ophthalmology, Fort Lauderdale, Florida, April 26, 1996.
Supported in part by U.S. Public Health Service grants EY07541 and
Members of the Vitreon Study Group participating in this study of giant retinal tears are listed in the Appendix at the end of this article. Dr. Peyman has a financial interest in Vitreon. Reprint requests to Gholam A. Peyman, MD, LSU Eye Center, 2020 Gravier St, Suite B, New Orleans, LA 70112.
1159

Ophthalmology Volume 104, Number 7, July 1997
Giant retinal tears are retinal breaks that extend 90° or more in circumference. They tend to occur more commonly in males and often are associated with high myopia and trauma. High-grade proliferative vitreoretinopathy (PVR) develops in 40% to 50% of patients and complicates their treatment. I
-4 Over the years, many innovative
techniques have been devised to manage these complex retinal detachments and have included such maneuvers as rapid head movements to unfold the flap of retina5 and air-fluid exchange with the patient in the prone position and the operating surgeon underneath him in a supine position.6- 10 Methods to fixate the retinal flap intraoperatively with retinal microincarceration, 11,12 adhesives,13 retinal tacks,14-16 screws/ and sutures l7
-19 generally have
proved unsatisfactory and have been fraught with complications.
The perfluorocarbon liquids have been a great boon to giant tear surgery.20-25 These low-viscosity, heavier-thanwater liquids are inert, optically clear, and immiscible with blood and water. These properties allow the perfluorocarbons to be used for relatively atraumatic hydraulic manipulation of the retina. Their high specific gravity unrolls the retinal flap and completely displaces subretinal fluid in a posterior-to-anterior direction, which allows surgery to be performed with the patient in the usual supine position. Their low viscosity permits easy intraocular injection through a small gauge needle and easy removal by passive egress through a flute needle during air-liquid exchange. Their high surface tension closes retinal breaks internally and prevents these heavy liquids from flowing into the subretinal space.26- 30
This report presents the Vitreon Collaborative Study Group's experience with the intraoperative and, in 16 cases (9.9%), the adjunctive postoperative use of perfluoroperhydrophenanthrene (Vitreon) in the management of giant retinal tears. This large consecutive series of 162 eyes from 23 participating centers has moreover permitted meaningful statistical evaluation of characteristics that are predictive of outcome.
Patients and Methods
One hundred sixty-two eyes of 161 patients with retinal detachments secondary to retinal tears extending 90° or more in circumference were entered consecutively into the study, underwent surgery between January 1, 1989, and July 31, 1994, and were observed for a minimum of 6 months. Informed patient consent was obtained under an investigational protocol approved by the institutional review board at each of the participating centers. One hundred twenty-three patients (76.5%) were male and 38 (23.5%) were female. Ages ranged from 4 to 83 years with a mean of 41.9 years. Most eyes had no condition predisposing them to the development of a giant tear, although 41 patients (25.3%) had a history of trauma and 20 eyes (12.3%) were highly myopic. Of the 80 (49.4%) that had undergone previous cataract extraction, 40 (24.7%) were aphakic and 40 were pseudophakic (anterior chamber intraocular lens in 11, posterior chamber intraocular lens in 29). Preoperative Snellen acuity ranged from
1160
20/20 to light perception. One hundred sixteen eyes (75.3%) had giant tears that extended between 90° and 180°, and 38 eyes (24.7%) had tears greater than 180° in circumferential extent. Nine eyes (5.8%) had 360° retinal tears. The macula was detached or partially detached in 118 eyes (72.8%), and 2 eyes had a macular hole that was recognized before surgery. Sixty-six eyes (40.7%) had some PVR at the time of their surgery with 52 (32.1 %) of these being grade CorD (Table 1)?1
Vitreon was provided to the investigators by Vitrophage, Inc (Lyons, IL), under the auspices of an ongoing Phase III Food and Drug Administration study of Vitreon.
With the participation of so many centers and surgeons, there obviously were some variations in the surgical technique, although it followed a general scheme that has been described elsewhere.27.32.33 Briefly, the surgery included a complete three-port pars plana vitrectomy followed, as needed, by membrane dissection or a relaxing retinotomy (necessary in 14 eyes or 8.6% of cases) or both. Perfluoroperhydrophenanthrene then was injected through a small gauge needle or cannula over the optic nerve to flatten the retina. Subretinal fluid was pushed in an anterior-toposterior direction and out the giant tear. Any traction that remained could be better visualized and managed at this stage. The perfluorocarbon liquid helped to open retinal folds and expose tissue planes and facilitated membrane dissection by stabilizing and providing countertraction of the posterior retina. When the retina was flat and apposed to the underlying retinal pigment epithelium, endophotocoagulation or cryopexy or both were performed to manage the edge of the flap.
The perfluoroperhydrophenanthrene then was removed from the eye via a flute needle during a slow and deliberate, complete air-Vitreon exchange. The eye then could be flushed with either a long-acting gas or filled with silicone oil, depending on the case and the surgeon's choice. An encircling scleral buckle then could be placed, and this was done in 100 eyes (62.5%) in this series. Of the 82 patients that were phakic at the time of their surgery, a lensectomy was deemed necessary in 31 (37.8%) to achieve adequate dissection of the vitreous base (Table 2).
Vitreon was left in 16 (9.9%) of eyes to provide extended retinal tamponade. In the remaining 146 eyes in which Vitreon was removed intraoperatively, 79 (48.8%) were filled with a long-acting gas mixture, 57 (35.2%) with silicone oil, and 10 (6.2%) with air or infusion fluid (Table 2).
After surgery, patients were examined at 1 day, 1 week, 1 month, 3 months, and 6 months, and thereafter at the discretion ofthe operating surgeon. Snellen visual acuity, slit-lamp examination, intraocular pressure, gas bubble size, and dilated funduscopic findings were recorded at each visit. A minimum follow-up of 6 months was obtained for all patients with a mean of 13.7 months and a range of 6 to 48 months. Eighty-six eyes (53.1 %) were observed for 12 months or more, and 25 eyes had 2 or more years of follow-up.
Statistical Analysis The chi-square analysis of the relation between preoperative characteristics (such as hypotony, macular detach-

Kertes et al . Vitreon in the Management of Giant Retinal Tears
Table 1. Preoperative Patient Characteristics
Number of Eyes Preoperative Findings (total = 162)
Eye OD 84 OS 78
Sex Male 124 Female 38
Predisposing conditions High myopia 20 Boxer 3 Marfan syndrome 2 Stickler syndrome 2 Choroidal hemorrhage 2 PDR 1 ROP 1
Trauma Blunt 24 Penetrating 16 IOFB 1
PYR grade None 93 A 1 B 13 CI-3 21 01-3 31
Extent of giant tear 900 34 >90-1800 82 >180-2700 27 >2700 11
lens status Phakic 82 Pseudophakic
ACIOl 11 PCIOl 29
Aphakic 39 Dislocated 1
Previous surgery PPY 28 Scleral buckle 21
Hypotony (lOP :s; 5 mmHg) 22 Status of macula
Detached 106 Partially detached 12 Macular hole 2 Flat 38
%
51.9 48.1
76.5 23.5
12.3 1.9 1.2 1.2 1.2 0.6 0.6
14.8 9.9 0.6
57.4 0.6 8.0
13.0 19.1
22.1 53.2 17.6
7.1
50.6
6.8 17.9 24.1 0.6
17.3 13.1 16.8
65.4 7.4 1.2
23.5
00 = right eye; OS = left eye; POR = proliferative diabetic retinopathy; ROP = retinopathy of prematurity; 10FB = intraocular foreign body; PVR = proliferative vitreoretinopathy; AClOL = anterior chamber intraocular lens; PClOL = posterior chamber intraocular lens; PPV = pars plana vitrectomy; lOP = intraocular pressure.
ment, history of previous cataract extraction, visual acuity, giant tear extent, and PVR grade) and outcome visual acuity was conducted as two-tailed tests at an alpha level of 0.05. The stepwise multivariate discriminant analysis was performed to determine the relative importance of each of the predictors when compared to one another.
For the stepwise analysis, the PVR was classified as grade A, B, C, D, absent, or "unknown," and these
classes were represented as the numbers 1, 2, 3, 4, and 0, respectively. The history of lens extraction in the eye undergoing the procedure was encoded as "phakic," "pseudophakic," or "aphakic" and represented by the numbers 0, 1, and 2, respectively. The preoperative visual acuity was divided into a class distribution with the following classes: greater than or equal to 20/40, less than 20/40 to 20/80, less than 20/100 to 20/200, less than 20/ 200 to 20/800, less than 20/800 to light perception, and no light perception but were coded numerically by their log of the minimum angle of resolution (logMar) equivalent for the discriminant analysis. These classes were all derived from the frequency distributions of observed outcomes. All statistical analyses were performed using programs and procedures from the Statistical Analysis System (SAS Institute, Cary, NC).
Results
Four eyes (2.5%) were deemed irreparable at the time of initial surgery. Retinal reattachment was achieved intraoperatively in the remaining 158 eyes (97.5%). At their most recent follow-up, 147 eyes (90.7%) remain attached. The most common postoperative complications were recurrent retinal detachments, which occurred in 80 patients (49.4%), and cataract formation over the follow-up period in 20 (39.2%) of the 51 eyes that were left phakic. Other complications included significant macular pucker in 12 eyes (7.4%), corneal decompensation in 10 eyes (6.2%), and hypotony in 9 eyes (5.6%). Ninety-five eyes (58.6%) required at least a second procedure (Table 3). Additional surgery ran the gamut from simple additional laser retinopexy or silicone oil or Vitreon removal to complex retinal detachment-PVR surgery.
Visual Acuity
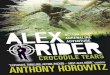
The distribution of preoperative and postoperative visual acuities can be seen in Figure 1. After surgery, visual acuities ranged from 20/20 to no light perception. Overall,
Table 2. Variations in Operative Procedure
Number of Eyes Operative Procedure (total = 162) %
Scleral buckle 84 51.9 lensectomy 31/82 37.8 Relaxing retinotomy 14 8.6 Postoperative tamponade
BSS/air 10 6.2 long-acting gas (79) (48.8)
C2F6 2 1.2 SF6 14 8.6 C3FS 63 38.9
Silicone oil (1000-12,000 cs) 57 35.2
Yitreon 16 9.9
BSS = balanced salt solution; cs = centistokes.
1161

Ophthalmology Volume 104, Number 7, luly 1997
Table 3. Complications
Complication
Operative complications Irreparable Slippage Vitreous hemorrhage Retinal f olds Rolled edge
Postoperative complications Recurrent detachment Cataract Macular pucker Hypotony (lOP :5 5 mmHg) Corneal decompensation Vitreous hemorrhage Hyphema Phthisis
lOP = intraocular pressure.
Number of Eyes (total = 162)
4 8 4 2 1
80 20/51
12 12 10 5 3 3
%
2.5 4.9 2.5 1.2 0.6
49.4 39.2
7.4 7.4 6.2 3.1 1.9 1.9
of those patients in whom a Snellen acuity could be obtained, 79 (48.8%) improved at least 1 Snellen line, 26 (16.0%) remained unchanged, and 57 (35.2%) experienced a worsening of their vision. A total of 10 eyes (6.2%) lost the ability to perceive light over the followup period, and 2 eyes (1.2%) became blind and painful and subsequently were enucleated.
The large size of this series permitted meaningful statistical evaluation of factors that were predictive of outcome. And, given the fact that perftuoroperhydrophenanthrene was being evaluated for toxicity and as a new surgical adjunct, the authors wanted to ensure that no new or unexpected preoperative characteristics emerged as being predictive of a poor outcome. A chi-square analysis of preoperative characteristics showed that the frequency of hypotony (P = 0.007), macular detachment (P =
80
70 D Preop
III 60 -Final -r:: Q)
50 :;:::; co
Figure 1. Ranges of preopera-a.. - 40
tive and final Snellen visual 0 .... acuities in patients with giant Q) 30 .0 retinal tears treated with ad- E junctive p erfluoroperhydro- :J 20 phenanthrene. Z
10
0 20120- 20/50-20/40 20180
1162
0.020), a history of cataract extraction (P = 0.003), poor visual acuity (P = O.OOO), giant tear extent greater than 1800 (P = 0.oo4), and higher grade PVR (P = O.OOO) all were associated with poor visual outcomes. Operative factors that were associated with poor final visual acuity were the need for a relaxing retinotomy (P = 0.024) and silicone oil fill (P = 0.018). Although when preoperative PVR grade, visual acuity, and giant tear extent were corrected for as covariants, neither a relaxing retinotomy (P = 0.7631) nor silicone oil fill (P = 0.5268) retained statistical significance. And, not surprisingly, postoperative persistent retinal detachment (P = O.ool) and hypotony (P = 0.041) were significantly associated with poor visual outcomes.
A stepwise discriminant analysis also was carried out to determine the relative importance of these predictors of poor postoperative visual acuity in combination. We found that poor preoperative visual acuity was the most important variable (P = 0.0001), followed by a history of lens extraction (P = 0.0168) and then PVR grade (P = 0.02oo).
Retinal Redetachment
A similar univariate and multivariate analysis was performed for all the preoperative, intraoperative, and postoperative factors for which we had data, and none proved to significantly predict the occurrence of recurrent retinal detachment.
Postoperative Vitreon Tamponade
Sixteen patients (9.9%) had Vitreon left in their eyes to provide an extended postoperative retinal tamponade. This was done at 10 of the Collaborative Study's 23 participating centers and was done at the discretion of the operating surgeon in cases in which it was thought that the retina could not otherwise be attached safely and reli-
20/100-201200
<201200 ·20/800
Visual Acuity
<201800 NLP

Kertes et al . Vitreon in the Management of Giant Retinal Tears
ably. One center contributed five (31.2%) of these eyes, and no other institution left Vitreon after surgery in more than two of their enrolled giant tear cases. Seven (43.8%) of these 16 cases had had a traumatic injury that was thought to contribute to the formation of their giant tear. One patient had Stickler's syndrome and another was a habitual head banger.
The Vitreon was left for a period ranging from 3 to 1034 days (mean, 87.2 days). There was no clinical evidence of excessive postoperative inflammation or other complications that could be attributed to this extended tamponade. However, no consistent electrophysiologic testing was done on this small subgroup of patients, so nothing definitive can be said about the presence or absence of more subtle retinal toxicity. In the one eye in which Vitreon was left for 1034 days, emulsification and opacification of the heavy liquid-fluid interface were noted, and emulsified Vitreon was present in the anterior chamber, which resulted ultimately in corneal decompensation. The retina in that eye remained attached at most recent follow-up, 35 months after the original surgery. Two additional eyes had Vitreon in the anterior chamber during the period that the heavy liquid was left as a tamponade and neither suffered any observable anterior segment sequelae. The other postoperative complications that this group suffered were not significantly different from the group as a whole (Table 3). A visually significant cataract developed in four (44.4%) of nine eyes over the period of observation. Three eyes (18.8%) had a significant intraocular pressure spike in the early postoperative period. For each patient, the pressure was controlled with a short course of medications, and none was thought to have suffered glaucomatous optic atrophy.
This group had a similar visual outcome (range, 20/ 20-no light perception) and rate of retinal redetachment (6 of 16, or 37.5%). The redetachments occurred from 29 to 425 days after the original surgery (mean, 184 days) and occurred, in all cases, after removal of the Vitreon. All 16 patients had at least 1 additional procedure (11 patients), and some had as many as 3 additional procedures (3 patients).
Discussion
The adjunctive use of perfluorocarbon liquids such as Vitreon in the management of giant retinal tears offers considerable advantages over techniques described previously.I-19 Most notably, it permits surgery to be done with the patient in the supine position, it largely prevents the otherwise vexing problem of posterior slippage of the retinal flap, and it obviates the need for mechanical fixation of the flap. These factors make the surgery technically easier to perform and increase its anatomic and functional success. In this series, our intraoperative retinal reattachment rate of97.5% (158 of 162 eyes) and overall reattachment rate of 90.7% (147 of 162 eyes) at last follow-up represent a considerable improvement over such methods as prone air-fluid exchange or intemal manipulation under silicone oil, which report rates of reattachment as low as 39%.4.7,9,10,34,35
These rates of attachment, redetachment, and visual results compare favorably to those of other series in which perfluorocarbon liquids were used in the management of giant retinal tears.20-25 The other reports largely have been retrospective reviews of various subpopulations of patients with giant tears, which makes comparison to our general population difficult. However, as expected, our outcomes lie somewhere in between the more favorable results found in patients presenting with uncomplicated giant tears25 and the more discouraging outcomes realized in the population with more complicated associated disease.22,23 It probably is fair to say that the prospective and multicenter nature of this series reflects what the average success rate might be for patients with giant retinal tears treated with a perfluorocarbon liquid.
Much controversy exists as to the need, impact, and importance of scleral buckling22 and lensectomy22,26 in giant tear surgery. The reports debating these issues, however, tend to be small series that look at select subsets of patients with giant tears and make recommendations that may not be generalizable. This series, which is the largest of its kind, enrolled patients with giant tears consecutively as they presented to the various participating centers, allows for a somewhat broader perspective, and gives insight into what reasonably can be expected for the average patient presenting with a giant tear. It also elucidates which of the preoperative, intraoperative, and postoperative variables importantly impact outcome. Our analysis of the data showed that patients who underwent scleral buckling or lensectomy or both had a distribution of final visual acuities and rate of redetachment no different from patients who did not have these interventions. The variables that were associated with a poor final visual acuity can be grouped into three categories according to their timing relative to the surgery. The preoperative factors that were associated individually with a poor visual result included macular detachment, hypotony, pseudoaphakia or aphakia, poor visual acuity at presentation, higher grade PVR, and giant tears greater than 1800 in extent. Operatively, only the need for a relaxing retinotomy and a silicone oil tamponade predicted a worse final acuity. These operative variables lost their statistical significance, however, when preoperative PVR grade, visual acuity, and giant tear extent were corrected for as covariants. And finally, patients with postoperative hypotony or persistent retinal detachments were less likely to see well.
It is curious that when a similar analysis was carried out on these same data to see which of these many variables were predictive of recurrent retinal detachment (which occurred in 80 [49.4%] of 162 eyes) in this series, no statistically significant relation could be found. This underscores the importance of careful follow-up in these patients and the need to stress to them that despite modern surgical advances and a potentially positive visual outlook, redetachment occurs commonly and a second operation often will be required.
Although Vitreon was removed intraoperatively in the majority of cases (90.1%), 16 eyes (9.9%), under the auspices of the investigational protocol, had Vitreon left for a prolonged postoperative retinal tamponade. The decision to do this was made at the surgeon's discretion and
1163

Ophthalmology Volume 104, Number 7, July 1997
was influenced by the anatomy of the detachment and giant tear, the degree of inferior retinal stiffness, and the inability of some patients to maintain the prone position for an extended period if a long-acting gas or silicone oil were chosen for the extended tamponade, Because PVR occurs preferentially in dependent portions of the retina, 36 eyes with inferior retinal disease probably benefit most from an extended postoperative Vitreon tamponade. This is supported by the findings of the Vitreon Collaborative Study Group.24.32
Although the number of patients in this subgroup was small and no special or consistent testing was done to evaluate long-term retinal toxicity, the Vitreon appeared to be clinically well tolerated in all cases. It is perhaps this long-term safety that sets Vitreon apart from the other perfluorocarbon liquids used in vitreous surgery. In animal studies, Vitreon was shown to be nontoxic when left for up to 6 weeks in rabbits and 22 weeks in monkeys.37 This is in contrast to perfluoro-octane, which has caused significant retinal toxicity after as little as 48 hours.38 Subretinal perfluorocarbon liquids, conversely, are toxic to the photoreceptors and the retina and should be removed. No patients in the current study were found to have subretinal Vitreon in the postoperative period. It has been the experience of the Vitreon Collaborative Group that this complication occurs less frequently with Vitreon than with the other perfluorocarbon liquids. This may relate to the somewhat higher viscosity (8.03 centristrokes) and surface tension (16 dynes/cm) of Vitreon compared with those of perfluoro-octane.
The favorable anatomic and visual results of this series confirm the use of Vitreon as a safe adjunct to pars plana vitrectomy in the management of giant retinal tears. The length of follow-up and size of the current study give it the statistical power to comment on the relative significance of a number of preoperative, intraoperative, and postoperative variables as predictors of final visual acuity and recurrent retinal detachment. Although further study is needed, Vitreon additionally may be the perfluorocarbon liquid that can be used most safely as a temporary postoperative tool for extended retinal tamponade, reinforcing its role as a useful adjunct in the management of these complex retinal detachments.
Appendix
The Vitreon Study Group List of Participants
Gholam A. Peyman, MD, George A. Williams, MD, Jane C. Werner, MD, R. Joseph Olk, MD, Harry W. Flynn Jr, MD, Hamid Mani, MD, Ralph Paylor, MD, Peter Campochiaro, MD, Thomas O. Bennett, MD, Joel A. Schulman, MD, Kevin J. Blinder, MD, Robert Wendel, MD, Rickey Medlock, MD, Bert M. Glaser, MD, James G. Randall, MD, Ching J. Chen, MD, Jay L. Federman, MD, William Tasman, MD, Nalin J. Mehta, MD, Nicholas Z. Zakov, MD, George E. Sanborn, MD, Neil Brourman, MD, Michael J. Elman, MD
1164
References
1. Freeman HM. Current management of giant retinal breaks and fellow eyes. In: Ryan SJ, ed. Retina, 2nd ed. St. Louis: Mosby, 1994, v. 3, 2313-28.
2. Glaser BM. Treatment of giant tears combined with proliferative vitreoretinopathy. In: Ryan SJ, ed. Retina, 2nd ed. St. Louis: Mosby, 1994, v. 3, 2329-33.
3. Freeman HM, Johnson MR. Giant retinal breaks. In: Spaeth GL, Katz LJ, Parker KW, eds. Current Therapy in Ophthalmic Surgery. Toronto: BC Decker Inc, 1989;256-64.
4. Glaser BM. Treatment of giant retinal tears combined with proliferative vitreoretinopathy. Ophthalmology 1986; 93: 1193-7.
5. Freeman HM. Current management of giant retinal breaks with an inverted retinal flap. In: Kanski JJ, Morse PH, eds. Disorders of the Vitreous, Retina and Choroid. London: Butterworths, 1983;210-27.
6. Norton EWD, Aaberg T, Fung W, Curtin VT. Giant retinal tears. I. Clinical management with intravitreal air. Am J Ophthalmol 1969; 68: 10 11-21.
7. Machemer R, Allen A W. Retinal tears 1800 and greater: management with vitrectomy and intravitreal gas. Arch Ophthalmol 1976; 94: 1340-6.
8. Lincoff H. A small bubble technique for manipulating giant retinal tears. Ann OphthalmoI1981;13:241-3.
9. Freeman HM, Castillejos ME. Current management of giant retinal breaks: results with vitrectomy and total air fluid exchange in 95 cases. Trans Am Ophthalmol Soc 1981;79: 89-102.
10. Vidaurri-Leal J, de Bustros S, Michels RG. Surgical treatment of giant retinal tears with inverted posterior retinal flaps. Am J Ophthalmol 1984;98:463-6.
11. Schepens CL, Freeman HM. Current management of giant retinal breaks. Trans Am Acad Ophthalmol Otolaryngol 1967;71:474-87.
12. Peyman GA, Rednam KRV, Seetner AA. Retinal microincarceration with penetrating diathermy in the management of giant retinal tears. Arch Ophthalmol 1984; 102:562-5.
13. Faulbom J. Treatment of giant retinal tears after perforating injuries with vitrectomy and a cyanoacrylate tissue adhesive. Adv Ophthalmol 1976;33:204-7.
14. Ando F, Kondo J. A plastic tack for the treatment of retinal detachment with giant tear. Am J Ophthalmol 1983;95: 260-1.
15. de Juan E Jr, McCuen BW II, Machemer R. The use of retinal tacks in the repair of complicated retinal detachments. Am J Ophthalmol 1986; 102:20-4.
16. Abrams GW, Williams GA, Neuwirth J, McDonald HR. Clinical results of titanium retinal tacks with pneumatic insertion. Am J Ophthalmol 1986; 102:13-9.
17. Usui M, Hamazaki S, Takano S, Matsuo H. A new surgical technique for the treatment of giant retinal tear: transvitreoretinal fixation. Jpn J Ophthalmol 1979;23:206-15.
18. Hirose T, Schepens CL, Lopansri C. Subtotal open-sky vitrectomy for severe retinal detachment occurring as a late complication of ocular trauma. Ophthalmology 1981;88:1-9.
19. Federman JL, Shakin JL, Lanning RC. The microsurgical management of giant retinal tears with trans-scleral retinal sutures. Ophthalmology 1982; 89:832-9.
20. Chang S, Lincoff H, Zimmerman NJ, Fuchs W. Giant retinal tears: surgical techniques and results using perfluorocarbon liquids. Arch Ophthalmol 1989; 107:761-6.
21. Mathis A, Pagot V, Gazagne C, Malecaze F. Giant retinal tears: surgical techniques and results using perfluorodecalin

Kertes et al . Vitreon in the Management of Giant Retinal Tears
and silicone oil tamponade. Retina 1992; 12(Suppl 3):S7-SlO.
22. Kreiger AE, Lewis H. Management of giant retinal tears without scleral buckling: use of radical dissection of the vitreous base and perfluoro-octane and intraocular tamponade. Ophthalmology 1992;99:491-7.
23. Glaser BM, Carter JB, Kuppermann BD, Michels RG. Perfluoro-octane in the treatment of giant retinal tears with proliferative vitreoretinopathy. Ophthalmology 1991; 98: 1613-21.
24. Millsap CM, Peyman GA, Mehta NJ, et al. Perfluoroperhydrophenanthrene (Vitreon) in the management of giant retinal tears: results of a collaborative study. Ophthalmic Surg 1993;24:759-63.
25. Ie D, Glaser BM, Sjaarda RN, et al. The use of perfluorooctane in the management of giant retinal tears without proliferative vitreoretinopathy. Retina 1994; 14:323-8.
26. Verstraeten T,Williams GA, Chang S, et al. Lens-sparing vitrectomy with perfluorocarbon liquid for the primary treatment of giant retinal tears. Ophthalmology 1995; 102: 17-20.
27. Blinder KJ, Peyman GA, Paris CL, et al. Vitreon, a new perfluorocarbon. Br J Ophthalmol 1991;75:240-4.
28. Chang S. Low viscosity liquid fluorochemicals in vitreous surgery. Am J Ophthalmol 1987; 103:38-43.
29. Peyman GA, Schulman JA. Vitreous Substitutes. Norwalk, CT: Appleton & Lange, 1995; 133-6, 155-61.
30. Peyman GA, Schulman JA, Sullivan B. Perfluorocarbon liquids in ophthalmology. Surv Ophthalmol 1995;39:375-95.
31. The Retina Society Terminology Committee. The classification of retinal detachment with proliferative vitreoretinopathy. Ophthalmology 1983;90:121-5.
32. Blinder KJ, Peyman GA, Desai UR, et al. Vitreon, a shortterm vitreoretinal tamponade. Br J Ophthalmol 1992;76: 525-8.
33. Peyman GA, Schulman JA. Intravitreal Surgery: Principles and Practice, 2nd ed. Norwalk, CT: Appleton & Lange, 1994;576-9.
34. Leaver· PK, Lean JS. Management of giant retinal tears using vitrectomy and silicone oilJ fluid exchange: a preliminary report. Trans Ophthalmol Soc U K 1981; 101:189-91.
35. Leaver PK, Cooling RJ, Feretis EB, et al. Vitrectomy and fluid/silicone-oil exchange for giant retinal tears: results at six months. Br J Ophthalmol 1984;68:432-8.
36. Michels RG, Wilkinson CP, Rice TA. Retinal Detachment. St. Louis: CV Mosby Co, 1990;672:858-8.
37. Peyman GA, Conway MD, Soike KF, Clark LC Jr. Longterm vitreous replacement in primates with intravitreal Vitreon or Vitreon plus silicone. Ophthalmic Surg 1991;22: 657-64.
38. Chang S, Sparrow JR, Iwamoto T, et al. Experimental studies of tolerance to intravitreal perfluoro-n-octane liquid. Retina 1991;11:367-74.
1165










![$PQZSJHIU …ousar.lib.okayama-u.ac.jp/files/public/5/56175/...rhages, retinal pigment epithelial tears, and/or chorio-capillaris atrophy [9-11]. The risk of serious complica-tions](https://img.pdfslide.net/doc/110x75/5e274ba9c8f801547e287b2d/pqzsjhiu-ousarlibokayama-uacjpfilespublic556175-rhages-retinal-pigment.jpg)





![Blood, Sweat & Tears - [Book] the Best of Blood, Sweat & Tears](https://img.pdfslide.net/doc/110x75/577c780e1a28abe0548e8be9/blood-sweat-tears-book-the-best-of-blood-sweat-tears.jpg)









