-
Christina Adaniel, Komal Jhaveri, Adriana Heguy and Francisco J.
EstevaGenome-Based Risk Prediction for Early Stage Breast
Cancer
doi: 10.1634/theoncologist.2014-0124 originally published online
September 3, 20142014, 19:1019-1027.The Oncologist
http://theoncologist.alphamedpress.org/content/19/10/1019located
on the World Wide Web at:
The online version of this article, along with updated
information and services, is
by Jean Santos on October 19, 2014
http://theoncologist.alphamedpress.org/
Dow
nloaded from
by Jean Santos on October 19, 2014
http://theoncologist.alphamedpress.org/
Dow
nloaded from
-
Breast Cancer
Genome-Based Risk Prediction for Early Stage Breast
CancerCHRISTINA ADANIEL,a KOMAL JHAVERI,a ADRIANA HEGUY,b FRANCISCO
J. ESTEVAaaDivision of Hematology/Oncology, Laura and Isaac
Perlmutter Cancer Center, and bGenome Technology Center, New York
UniversityLangone Medical Center, New York, New York,
USADisclosures of potential conflicts of interest may be found at
the end of this article.
Key Words. Breast cancer x Gene expression x Genomic
profiling
ABSTRACT
Tests to better characterize tumor genomic architecture
arequickly becoming a standard of care in oncology. For
breastcancer,theuseofgeneexpressionassays forearlystagediseaseis
already common practice. These tests have found a place inrisk
stratifying the heterogeneous group of stage III breastcancers for
recurrence, forpredicting chemotherapy response,and for predicting
breast cancer-relatedmortality. In the last 5years, more assays
have become available to the practicing
oncologist.Given the rapiditywithwhich this fieldhasevolved,it
is prudent to review the tests, their indications, and thestudies
from which they have been validated. We presenta comprehensive
review of the available gene expressionassays for early stage
breast cancer. We review data forseveral individual tests and
comparative studies looking atrisk prediction and
cost-effectiveness. The Oncologist 2014;19:10191027
Implications for Practice: Gene expression assays are an
important component in the management of early stage breastcancer.
Understanding their utility as well as their drawbacks is critical
for the practicing oncologist to make informed decisionsregarding
care.
INTRODUCTION
Breast cancer is one of the leading causes of
cancer-relatedmorbidity worldwide [1]. In the U.S., 235,030 new
cases areexpected to be diagnosed in 2014 [2]. Of these,
approximately164,000 cases (70%) will be classified as early stage
(stage III)breast cancer, for which the potential for cure is
excellent.Although surgery is the major curative modality,
adjuvantchemotherapy plays an important role in increasing cure
ratesfor a selected group of patients. Approximately 15%30%
ofpatients with stage I breast cancer and up to 40% of stage
IInode-negative patients will have a recurrence with localtherapy
alone. The disparity in outcomes within groups ofsimilar
histopathologic characteristics speaks to the
incredibleheterogeneity of this disease [3, 4]. How to better
define andidentify these higher risk individuals has been an area
ofintense investigation for more than a decade [5].
This clinical conundrum has resulted in a scientific race
ofsorts to more precisely prognosticate risk of recurrence (ROR)in
early stage breast cancer. The investigation has focusedmainly on
patients with hormone receptor-positive (HR1)HER2-negative (HER22),
and lymph node-negative (LN2)disease, encompassing the majority of
patients with earlystage breast cancer. HER2-positive tumors are
considereda separate group that benefit from adjuvant
HER2-basedchemotherapy [68]. Axillary lymph node involvement
isassociated with poor outcome, and those patients generally
receive adjuvant chemotherapy. However, efforts are ongoingto
identify patients with one to three positive lymph nodes forwhom
chemotherapy is not indicated. This is particularlyimportant
because although the benefits of chemotherapymay be great for a
subset of patients, chemotherapy may alsoconfer significant,
potentially life-long toxicities for others.These include
peripheral neuropathy; premature ovarianfailure; and, rarely,
cardiac dysfunction [9, 10]. Short-termtoxicities are also
substantial. Risk for infection, alopecia, andfatigue, in addition
to the emotional toll that chemotherapycan often take on patients,
are important side effects, and allmay substantially affect quality
of life.These secondary effectsare common to most standard adjuvant
chemotherapyregimens for breast cancer [11].
Focus has been on the larger group of stage III,
node-negative,HR1, HER22breastcancer patients for two reasons:to
better communicatewith patients about true individual riskof
recurrence and to better identify high-risk patients forwhom
adjuvant chemotherapy may be more recommendedand low-risk patients
for whom chemotherapy may offer littlebenefit.
Inorder tohave amoreconcreteunderstandingof the risksand
benefits of adjuvant chemotherapy, several gene
expres-sionassayshavebeendeveloped tobetterstratify this
groupofdiversepatients.Theassaysevaluatevaryingnumbersofgenes
Correspondence: Francisco J. Esteva,M.D., Ph.D., Laura and Isaac
Perlmutter Cancer Center, NewYorkUniversity LangoneMedical Center,
160East 34th Street, New York, New York 10016, USA.Telephone:
212-731-5657; E-Mail: [email protected] ReceivedMarch 25,
2014;accepted for publication July 30, 2014; first published online
in The Oncologist Express on September 3, 2014. AlphaMed Press
1083-7159/2014/$20.00/0
http://dx.doi.org/10.1634/theoncologist.2014-0124
TheOncologist 2014;19:10191027 www.TheOncologist.com AlphaMed
Press 2014
CME
by Jean Santos on October 19, 2014
http://theoncologist.alphamedpress.org/
Dow
nloaded from
-
in the breast tumor, to quantify their expression levels,
andoutput a score that correlates with risk of recurrence.
Thesetests, which are commercially available and in some cases
arecovered by insurance in the U.S., are being used in
clinicalpractice toassistwithprognosticationandoften
toaiddecisionmaking regarding adjuvant chemotherapy.
Since the last time The Oncologist reviewed gene expres-sion
assays for breast cancer, in 2008, more tests have
becomecommercially available, and multiple validation studies
havebeenpublished [12]. Inaddition,onesuchtestwasclearedbytheU.S.
Food and Drug Administration (FDA) in September 2013,and others are
actively seeking approval by regulatory agencies.Given the large
number of options now available to practicingoncologists, it is
pertinent to update this review with acomprehensive analysis of the
available breast cancer geneexpression tests.We aim to provide a
clearer understanding ofthese assays so that providers may make
more informeddecisions in the clinic, avoid unnecessary use of
cytotoxicchemotherapy,andreduce theburdenonthehealthcaresystem.
MATERIALS AND METHODSA comprehensive literature search of all
relevant clinical trials,original research articles, review
articles, and editorials in thePubMed database concerning gene
expression assays in breastcancerwas performed. Original research
publications pertainingto discovery-phase and validation studies
for each of thespecified gene expression assays were reviewed. The
searchtermsgeneexpressionprofiling, geneexpressionassay,
geneexpression, Oncotype DX, MammaPrint, PAM50, BreastCancer Index,
and breast cancer were used. Individual bio-technology company
websites were also reviewed for additionalinformation regarding
tissue requirements, technologyused, andavailability of tests.
Assays based on gene expression profilingwere included. Those based
on immunohistochemistry (IHC)were excluded. Tests that are
clinically available in the U.S. wereincluded (Table 1). Those
available only in Europe, such asMapQuant Dx and EndoPredict, were
excluded.
GENE EXPRESSION ASSAYS
Oncotype DXThis 21-gene assay developed by Genomic Health
(RedwoodCity, CA, http://www.genomichealth.com) is the most
fre-quently used test in clinical practice in the U.S. [13]. Based
onquantitative reverse transcription polymerase chain reaction(PCR)
expression levels of 5 reference genes and 16 selectedgenes related
mostly to the estrogen receptor (ER), HER2,proliferation, and
invasion, the assay determines a recurrencescore (RS) that assigns
patients into a low-, intermediate-, orhigh-risk category.The
original training setwithwhich the assaywas designed used 447
patient specimens from three breastcancer clinical trials (a
variety of patients, some with ER2 andLN1 disease) but was most
heavily weighted toward thetamoxifen-only arm of the National
Surgical Breast and BowelProject-B20 (NSABP-B20) cohort [14]. The
training set included250 candidate genes that were eventually
paired down to 21based on a best-fit model. The assay was validated
in a studypublished by Paik et al. in theNew England Journal of
Medicinein 2004 [14]. The validation cohort included 668 ER1,
LN2patients from the NSABP-B14 study who were all treated with
tamoxifen. The study showed a significant difference in
distantrecurrence at 10 years among the three groups, as defined
bytheRS, and thescoreprovidedpredictivepower independentoftumor
size and age.The distant recurrence rate at 10 years was6.8% for
the low-risk group, 14.3% for the intermediate-riskgroup, and30.5%
for thehigh-risk group.TheRSwas also shownto correlate
independently with overall survival (OS).
The test has since been validated inmultiple other
studies,especially for patients treatedwith endocrine therapy.
Amongthese is another study by Paiket al., from2006,
demonstratingthe use of the Oncotype DX assay not only for
prediction ofrecurrence but also for prediction of chemotherapy
benefit[15]. Again, using the NSABP-B20 cohort, in this study
Paiket al. evaluated 227 patients randomized to treatment
withtamoxifen alone versus 424 patients treated with tamoxifenplus
chemotherapy (cyclophosphamide, methotrexate, and5-fluorouracil
[5-FU] or methotrexate and 5-FU). The RSsignificantly correlated
with benefit from chemotherapy asdetermined by 10-year disease-free
survival (DFS) comparedbetween each RS group in the tamoxifen-only
and tamoxifen-plus-chemotherapy arms. It was estimated that freedom
fromdistant recurrence was increased from 60% to 88% when
che-motherapy was added to tamoxifen in the high-risk RS group.The
benefit of chemotherapy in the intermediate-risk groupwas less
clear. However, it is important to note that, similar toMammaPrint,
this study was not an independent validationbecause therewas
duplication of samples from the training set.Onlyoneof theoriginal
validationstudies
showednoprognosticvalueinpatientswithnode-negativebreastcancerwhoreceivednoadjuvant
systemic therapy [16]. However, the study includedpatients with ER1
and ER2 breast cancer, and the test wasoriginally designed to
assess ER1 tumors. Nevertheless, giventhe aforementioned studies
and similar data from othervalidations, the American Society of
Clinical Oncology (ASCO)and the National Comprehensive Cancer
Network guidelineshave recommended the use of Oncotype DX to
risk-stratifypatients with ER1, HER22, LN2/N1mi (axillary
metastases,2 mm) early stage breast cancer [1720].
PAM50Prosigna (NanoString Technologies Inc., Seattle,WA,
http://www.nanostring.com) is the gene expression profile assaymost
recently cleared by the FDA, gaining approval inSeptember 2013. The
technology, unlike other assays, can beperformed in any
CLIA-certified laboratory with the use ofNanostrings NanoCounter
Analysis System. Briefly, geneexpression is measured in RNA
extracted from formalin-fixedparaffin-embedded tissue using a
novel, digital, color-coded,bar code technology that allows
measurement of multipletranscripts with high sensitivity (less than
one copy per cell). Apanel of 50 classifier genes and 5normal
geneswas selected toclassify breast cancers into an intrinsic
subtype (luminal A,luminal B, HER2-enriched, and basal-like). Using
the intrinsicsubtypedefinedby the50-gene signature, alongwith
standardprognostic parameters, multiple studies have shown
PAM50simproved ability to prognosticate risk of recurrence.
Thetraining set for PAM50 included 29 normal breast samples and189
tumors with approximately 50% LN1 disease and mostlyhigh-grade
tumors [21]. The training set evaluated 1,906genes, and this number
was ultimately reduced to 50 genes
AlphaMed Press 2014TheOncologist
1020 Genome-Based Risk Prediction for Breast Cancer
CME
by Jean Santos on October 19, 2014
http://theoncologist.alphamedpress.org/
Dow
nloaded from
-
of interestwith8 controls.This 50-geneclassifierwas testedon761
samples from patients who had not received adjuvantsystemic therapy
and 133 who had received neoadjuvantchemotherapy (paclitaxel
followed by 5-FU, doxorubicin andcyclophosphamide). In the first
group of no adjuvant therapy,the majority of the samples were
node-negative (710 of 761).The 50-gene classifier showed a clear
difference in recurrence-free survival (RFS) in the 4 identified
intrinsic subtype groups.These intrinsic
subtypesdonotcorrespondcompletelywithERandHER2 statusbasedon IHC
[22], suggesting that the subtypeis not simply a recapitulation of
findings based on routinehistologic examination. The statistically
significant differencein RFS remained after groups were stratified
by ER status.The identified subtypes, however, were less successful
atpredicting outcomes for HER21 tumors. Prediction for riskof
recurrence was significantly improved when the
subtypeclassificationwasadded toknownprognostic clinical
variables.The combination of these parameters was coined ROR-C,
riskof recurrence plus clinical variables. In addition, in the
group ofpatients who received neoadjuvant therapy, risk of
recurrencebased on intrinsic subtypes was able to predict
pathologiccomplete response to chemotherapy with 94% sensitivity
and97%negativepredictivevalue [21].Nielsenetal.validated
thesefindings in an independent cohort of 786 patients with bothLN1
and LN2 disease who were treated with tamoxifen only[23]. The
majority of the tumors were ER1. The intrinsic sub-types and the
ROR scores identified by PAM50 were stronglyprognostic for RFS and
disease-specific survival. An even largervalidation study was
published more recently, in January 2014,lookingat1,478patients
fromtheAustrianBreastandColorectalStudy Group 8 (ABCSG-8) trial
population [24]. This cohortincluded postmenopausal ER1 early stage
breast cancerpatients who received adjuvant hormonal therapy
(tamoxifenalone or tamoxifen followed by aromatase inhibitor)
withoutadjuvant chemotherapy. Again, the PAM50 ROR
significantlypredictedRFS. Inall subgroups,except for
theHER21group,theROR score and ROR risk groups added prognostic
informationto the routinely used clinicopathologic parameters.
Currently,PAM50 is approved for use in postmenopausal women withHR1
tumors with or without lymph node involvement.
MammaPrintMammaPrint (Agendia, Amsterdam, The Netherlands,
http://www.agendia.com) was the first gene expression array for
breast cancer prognosis to be cleared by the FDA, back
inFebruary 2007. MammaPrint is composed of a 70-genemicroarray. The
original training set evaluated 25,000 genesin 78 LN2 sporadic
early breast cancer tumors that were,5 cm in diameter and present
in patients,55 years old [25].The genes were eventually narrowed to
a 70-gene classifierthat showed a difference in expression patterns
betweengood-prognosis and poor-prognosis groups, as defined by
theauthors. However, the groupswere preselected based on
theirclinical outcomes (one group with distant metastases at
5years, the other disease free at 5 years). A subsequentvalidation
study assessed 295 patients with pT1 or pT2 tumorswith pN0 or pN1,
with a median follow-up of 7.8 years [26].Sixty-one of the 295
patients were part of the training set;therefore, this was not a
completely independent validationset, although a separate analysis
was also completed leavingout the repeated tumors. The analysis
showed a significantdifference between OS and metastasis-free
survival in thegood- and poor-prognosis groups. Overall survival
across allpatients. comparing the good-prognosis and
poor-prognosisgroups, was 94% versus 54%, respectively, at 10
years.Whenevaluating the LN1patients alone, theMammaPrint
signaturecontinued to be a significant prognostic marker. This
70-genesignature has since been validated in other studies,
includingpatientswithup49positive lymphnodes [2730]. In
thepast,limitations of the assay included the requirement for
freshfrozen tissue and high-quality cDNA; however, since
2012,Agendiahasmadethetestavailable for
formalin-fixedparaffin-embedded tissue [31].
Breast Cancer IndexThe Breast Cancer Index (BCI)
(bioTheranostics, San Diego, CA,http://www.biotheranostics.com)
incorporates two previ-ously established gene expression assays
into one test. Itevaluates theratioof theexpressionof
twogenes,HOXB13andIL17BR, based on qualitative PCR in combination
with theMolecular Grade Index. The Molecular Grade Index is a
five-gene expression assay looking at genes related to
histologicgrade and tumor progression. In an initial analysis, Ma
et al.demonstrated that in 60 postmenopausal ER1 patientstreated
with 5 years of tamoxifen, the ratio of HOXB13 toIL17BR was an
independent prognostic factor, with higherratios correlating with
poorer outcomes [32]. The study alsoshowed that the ratio was able
to predict for response to
Table 1. Breast cancer gene expression tests clinically
available in the U.S.
Test Company Number of genes Tissue Technology Measure
FDA-cleared
Prosigna Nanostring 501 22 ctla FFPE Digital bar-codedmRNA
analysis
ROR: Low (,10), intermediate(1020), high (.20%) risk
Yes
Oncotype DX Genomic Health 161 5 ctl FFPE qRT-PCR RS: low (,18),
intermediate(18-31), high (.31) risk
No
MammaPrint Agendia 70 Fresh frozen,FFPE
Microarray Good risk and poor risk Yes
Breast CancerIndex
bioTheranostics 51 2 gene ratio FFPE qRT-PCR Low, intermediate,
and high risk No
aProsignameasures the expression levels of 50 genes used in the
PAM50 classification algorithm, 8 housekeeping genes used for
signal normalization, 6positive controls, and 8 negative
controls.Abbreviations: ctl, control/housekeepinggenes;FDA,U.S.
FoodandDrugAdministration; FFPE,
formalin-fixedparaffin-embedded;qRT-PCR,quantitativereverse
transcription-polymerase chain reaction; ROR, risk of recurrence;
RS, recurrence score.
www.TheOncologist.com AlphaMed Press 2014
Adaniel, Jhaveri, Heguy et al. 1021
CME
by Jean Santos on October 19, 2014
http://theoncologist.alphamedpress.org/
Dow
nloaded from
-
tamoxifen therapy. Later, itwas shown that the combinationofthis
two-gene ratio with the Molecular Grade Index providedbetter
predictive value than either alone. This finding wasvalidated in a
cohort of 588 postmenopausal early stage ER1breast cancer patients
from the Stockholm trial of adjuvanttamoxifen versus placebo
[33].This studywas used to developa continuous risk predictor, the
BCI, using a scale of 0 to 10.TheBCI was prognostic in an
independent population of node-negative patients who did not
receive adjuvant therapy, withthe aim of risk stratifying for
breast cancer death [34]. Thepredictive role of the BCI in patients
receiving extended ad-juvant endocrine therapy was tested on tissue
from patientswho participated in theMA.17 trial. In this study,
high BCI wasassociated with a decrease in late recurrence in
patientsreceiving extended letrozole therapy [35].The BCI test may
beconsidered to assess the probability of distant recurrence
inpatients diagnosedwithER1node-negativebreast cancer andto predict
the likelihood of benefit from extended (.5-year)endocrine therapy
in patientswho are recurrence free after aninitial 5 years of
adjuvant endocrine therapy.
COMPARATIVE STUDIESGiven the wealth of data supporting each
individual test, howdoes one choose which to use in clinical
practice? Only ahandful of studies have compared the assays to one
another.One such study evaluated 1,017 ER1 early stage breast
cancerpatients from the Arimidex, Tamoxifen Alone or in
Combina-tion (ATAC) trial [36]. In this study,OncotypeDXwas
comparedwith PAM50 and IHC4 (an integrated score of the
immunohis-tochemical markers Ki-67, ER, PR, and HER2). The
primaryendpoint was distant recurrence after endocrine therapy.The
authors concluded that the PAM50 ROR, compared withthe Oncotype DX
RS, provided more prognostic informationregarding risk of
recurrence and better differentiated theintermediate- and high-risk
groups.
In the sameyear, the Lancetpublishedanarticle comparingthe BCI
with Oncotype DX and IHC4, using the translationalarm of the ATAC
(TransATAC) population. The study looked atboth early (within the
first 5 years) and late (after 510 years)distant recurrence. The
analysis included 665 patients. Theauthors suggestedthat
theBCI,whenusedasa linearmodel,wasmore predictive than Oncotype DX
(hazard ratio: 1.69) and thatonly theBCIwas able topredict for
latedistant recurrence [37].
An interesting study performed years earlier evaluatedthe
concordance between various gene expression arrays. In2006, Fan et
al. compared 5 gene sets, among which were theMammaPrint70-geneset,
theOncotypeDXRS21-geneset, theintrinsic subtypes as defined by
Perou et al., and the ratio ofHOXB13 to IL17BR, which makes up part
of the BCI [38]. Thestudy was based on an independent set of 295
breast cancercases for which gene expressionmicroarrays were
performed.The investigators performed multiple microarrays on
eachsample using the various gene sets mentioned above.Although the
population used was a heterogeneous one,including ER2 cancers and a
variety of adjuvant treatments,Fan and collaborators showed that
for both the compositegroup and theER1patients alone, theRFS
andOSaspredictedby the tests were similar in four of five of the
gene expressionarrays. The two-gene ratio failed to distinguish
outcomesbetween the two high-risk and low-risk groups it had
identified.The studyalso revealed that the70-geneprofile andthe
21-gene RS classify similar groups of patients into riskcategories
(77% concordance for ER1 patients and 81% con-cordance
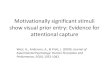
overall).When looking at the intrinsic subtypes, the21-gene RS and
70-gene profile classify all of the basal-likesubtypes into
thehigh-riskcategoryandhave similar trends forthe other subtypes
(Fig. 1). This study suggests that althoughthe actual genes tested
are not the same, similar biologicalcharacteristics are being
tested in the gene expression assaysand generate similar outcomes
in prognostication.
COST-EFFECTIVENESS ANALYSESWith recent cutbacks in health care
expenditure in the U.S.,practitioners are increasingly called on to
make cost-effectivedecisions. This can often be difficult, given
the hefty price tagof genomic testing and insurance restrictions.
Fortunately,several cost-effectiveness analyses have been performed
toassess the available gene expression assays. Adjuvant! Online,a
publicly available online risk predictor, is often used asa
standard with which to compare the cost-effectiveness ofgene
expression assays because it incorporates patient andtumor
characteristics (e.g., age, LN status, tumor size) into
itsprognostication model and is free.
In theU.S., OncotypeDX andMammaPrint have both beenshown
independently to be cost-effective tests in guiding de-cisions
regarding adjuvant therapy [39, 40]. More important,a
cost-effectiveness analysis directly comparing
OncotypeDXwithMammaPrintwas performed in 2012.The analysis
com-pared the cost and quality-adjusted life years (QALYs) of
eachtest. Based on a hypothetical cohort of ER1, LN2 early
stagebreast cancer patients, the study concluded that MammaPrintis
the most cost-effective test based on a willingness-to-paythreshold
of $50,000 per QALY [13].
In the U.K., another cost-effectiveness analysis looked atnine
different gene expression profiles and IHC-based testsincluding
Oncotype DX, MammaPrint, the BCI, and PAM50[41].The study
reviewedprior analyses anddevelopedamodelto evaluate the
cost-effectiveness of adjuvant therapy guidedby the tests as
comparedwith routine care guided by standardclinicopathologic
criteria. Unfortunately, the authors foundthat data were
insufficient to fully compare each of the tests.They suggested that
IHC4 had the most potential to be cost-effective; however, evidence
for its clinical utility equal to orbeyond the genomic-based tests
was lacking.
UNRESOLVED QUESTIONS AND ANTICIPATED STUDIES USINGGENE
EXPRESSION ASSAYSMultigene assays are currently being used in large
part toestimate risk of recurrence in patients with
ER1/HER22tumors; however, the definition of ER positivity is
evolving.Traditionally, tumors were considered ER1 and/or PR1 if
atleast 10%of the cells exhibitedprotein expressionusing IHC.
In2010, a joint committee from ASCO and the American
CollegeofPathology recommendeda1%cutoff for ERandPRpositivity[42].
This recommendation was based on data from a SWOGstudy conducted
decades ago [43], and, consequently, theprognostic and predictive
value of ER and PR between 1%9%remains poorly defined [44].
Given that these assays are already being used in
clinicalpractice, several clinical trials have incorporated them
into
AlphaMed Press 2014TheOncologist
1022 Genome-Based Risk Prediction for Breast Cancer
CME
by Jean Santos on October 19, 2014
http://theoncologist.alphamedpress.org/
Dow
nloaded from
-
their designs to answer further questions about their
utility(Fig.2).TheTAILORxtrial,whichhascompletedaccrual and is
inthe analysis phase, will look at the utility of
chemotherapyspecifically in patients with an intermediate RS
(Oncotype DX)[45]. The results of this trial are highly anticipated
becausethere is no standard of care for these
intermediate-riskpatients, and decisions are largely dependent on
shareddecision making between the provider and the patient.
A similar SWOG trial is ongoing for patients with ER1,HER22
breast cancer and one to three positive nodes. TheRxPONDER trial
randomly assigns patients with an RS#25 toendocrine therapy alone
or to chemotherapy plus endocrinetherapy [46]. This trial is
currently accruing patients, with thegoal of randomizing 4,000
patients, and aims to answer thesamequestionas theTAILORx trialwith
regard to thebenefit ofchemotherapy in patients with low to
intermediate RS butspecifically for node-positive patients.
In line with aims at further personalizing oncologiccare, more
precise prognostication is needed tomeetthe individual needs of
patients. Gene expressionassays have the potential to fill the gap
where clin-icopathologic criteria fall short.
TheMINDACT trial is another large randomizedclinical trialthat
has incorporated MammaPrint into the design. The trialevaluates the
clinical utility of MammaPrint (genomic factors[G]) in
combinationwithclinicopathologic risk factorsassessedby Adjuvant!
Online (clinical factors [C]). The study incorpo-rates early stage
breast cancer cases that are LN2 or thathave one to three positive
lymph nodes. The design is
complex and not only looks at MammaPrint utility but
alsocompares adjuvant chemotherapy and adjuvant endocrineregimens.
In order to evaluate MammaPrint utility, patientswho have
discordant G and C results are randomized toadjuvant chemotherapy
or no chemotherapy. Recently, thepilot phase, which comprised 800
patients, was published.In this first initial cohort of patients,
27% had discordant G andC risks and approximately half received
chemotherapy. Thepilot phase demonstrated that the study is
feasible, and theoutcomes are expected to be quite informative
[47].
Last, the OPTIMA trial is a randomized phase III study thatwill
compare outcomes of test-directed treatment with acontrol arm of
chemotherapy plus endocrine therapy forpN12 or pT3N0 ER1, HER22
breast cancers. In addition toclinical outcomes, the study will
evaluate cost-effectivenessand health resource utilization related
to multigene assays forearly stage breast cancer in the U.K.
[48].
DISCUSSIONAlthough the vast majority of stage III HR1, HER22
patientswill never develop recurrent disease, the fear of
recurrenceoften drives patients and providers to choose
adjuvantchemotherapy. The majority of patients receive no
benefitfrom this treatment; however, this practice continues
becausecurrent prognostic markers fail to identify which
patientswithin this groupareatgreatest risk. In linewithaimsat
furtherpersonalizing oncologic care, more precise prognosticationis
needed to meet the individual needs of patients. Geneexpression
assays have the potential to fill the gap whereclinicopathologic
criteria fall short. Figure 3 shows a proposedalgorithm for
clinical decision making using available multi-gene expression
assays.
Figure 1. Numberof patients per intrinsic subtype and their risk
categories as determinedby the70-geneprofile andRS
(21-geneprofile)derived from microarray data.Within each intrinsic
subtype, risk categories per patient are similar between assays,
although completeconcordance is seen only for the basal-like group.
Adapted from data in Table 2 of Fan et al. [36].
Abbreviation: RS, recurrence score.
www.TheOncologist.com AlphaMed Press 2014
Adaniel, Jhaveri, Heguy et al. 1023
CME
by Jean Santos on October 19, 2014
http://theoncologist.alphamedpress.org/
Dow
nloaded from
-
Figure 2. Overviewof clinical trials that have incorporated
currently available assays into their designs to answer
furtherquestions aboutthe assays utility.
Abbreviations: CT, chemotherapy; HR, hormone receptor; IC,
informed consent; PIS, patient information sheet; R-C,
chemotherapyrandomizationofanthracycline-basedCT
(FECDforN1docetaxel/capecitabine);R-E,endocrine
treatmentrandomization, letrozolevs.tamoxifen followed by
letrozole; R-T, treatment decision randomization based on genomic
vs. clinical prognosis; RS, recurrence score.
AlphaMed Press 2014TheOncologist
1024 Genome-Based Risk Prediction for Breast Cancer
CME
by Jean Santos on October 19, 2014
http://theoncologist.alphamedpress.org/
Dow
nloaded from
-
We have reviewed the four main gene expression assaysused in the
U.S. to evaluate risk of recurrence in early stagebreast cancer
patients with HR1, LN2 disease. The assaysreviewed in this article
each have their own individual ad-vantages. Oncotype DX has perhaps
the strongest clinicalevidence, with 13 retrospective studies,
totaling .4,000patients, suggesting it is clinically useful. The
assay has beenshown to be prognostic, and, to some degree, it may
predictchemotherapy response.
PAM50, thenewcomer to thegroup, hasbeenvalidated inlarge cohorts
(.1,000 patients).The bulk of the data supportits prognostic value
in patients with early stage, ER1/HER22breast cancer. Emerging,
albeit limited, data showed thatPAM50 may also be predictive of
response to neoadjuvantchemotherapy, althoughmore studies are
needed to validateits predictive role in this setting [49]. One of
the potentialadvantages of the PAM50 assay is that it can be
performedand reported by hospital and commercial
laboratories.Although reproducibility and technical expertise
withina laboratory certified under the Clinical Laboratory
Im-provement Amendments of 1988 is necessary, the ability tooffer
testing within ones own institution has multiple benefitsincluding
personalized overview of testing, cost control, likelyfaster
turn-around time, andanopportunity for institutional
datacollection. It should be noted that the FDA cleared only
theProsigna ROR score for clinical use; therefore, reports
fromcommercial laboratories may not include the intrinsic
subtypeinformation.
This skepticism regarding the clinical utility of
molecularsubtypes was reiterated in a publication from the Annals
ofOncology thatevaluated themedical usefulnessof the
intrinsicsubtypes as defined by PAM50 compared with
IHC-classifiedbreast cancer subtypes (HER2 and HR status) [50]. An
expertpanel, the IMPAKT task force, composed of
pathologists,clinicians, biostatisticians, and scientists, reviewed
literatureto determine evidence for the use of PAM50 molecular
subtypes in clinical practice. After a thorough review of
theevidence, the group determined that data were insufficientto
support the clinical validity and utility of PAM50 molecu-lar
subtypes. They recommended against using the intrinsicsubtypes to
guide treatment decisions, in part because theremay be some
discrepancy between intrinsic subtypes definedby PAM50 compared
with IHC-defined classes, which wereconsidered to be more strongly
validated tests. These rec-ommendations fall in line with the FDA
recommendations foruse of this assay. However, the IMPAKT task
force did notaddress the utility of the PAM50 ROR score, which
shouldbe considered separately and which we feel has been
wellestablished based on the available data.
Looking at all four of the assays reviewed in this paper,we
return to the study by Fan et al., which was the only oneto
evaluate all of these assays together in a single investiga-tion
[39]. Fan et al. used the gene sets from each assay(MammaPrint,
Oncotype DX, PAM50, and the two-gene ratiofrom the BCI) to compare
predicted outcomes for an inde-pendent set of breast cancers. It is
important to note thatthe gene set for the PAM50 ROR was not
compared with theotherassays in this studybut rather the intrinsic
subtypes fromPAM50 were used. The study concluded that the gene
sets asa whole identified similar groups of high-risk and
low-riskcancers, although100%concordancewasnot seen.The
largestdiscrepancy was within the luminal A group, in which
somecases identified as low risk by the MammaPrint, or
70-gene,assay were classified as intermediate risk by the
OncotypeDX, or 21-gene, assay. The purpose of this study was not
todetermine which assay was most predictive of outcomes butrather
to evaluate the inherent concordance between genesets. Although
interesting in terms of biological principles,underscoring the
concept that the assays are ultimatelymeasuring the same tumor
properties, the study does notdistinguish one assay from another in
terms of usefulness forclinical practice.
Perhaps themostuseful study fordirecting clinical
decisionmaking, in our opinion, was the head-to-head comparison
ofPAM50 and Oncotype DX [36]. In this investigation,
PAM50providedmore prognostic information thanOncotypeDXwithregard
to likelihood ratios and distant recurrence rates
overamedianof10yearsof follow-up.Comparison indices revealedthat
the PAM50 ROR outperformed the Oncotype DX RS forevery
tumorsubtype. Inaddition,hazard ratios for the low-andhigh-risk
groups categorizedbyRORwere improved comparedwith the low- and
high-risk groups identified by the RS. Al-though this is only a
single study, it provides high-quality datawith which to compare
the two tests.
That being said, a major drawback of all of the gene ex-pression
assays reviewed is that HER21 and LN1 patientswere included in the
testcohorts. By including thesehigher riskindividuals, the
recurrence scores may have less inherentclinical utility because
they are currently only being applied toHR1, HER22, LN2 disease.
Including HER21 and LN1 high-risk patients in the test cohort may
bias the analysis andcompromise the ability to determinewhether the
assays havejust as strong predictive potential in a population with
lowerrisk overall. A study that excludes such patients wouldprovide
more clinically relevant information. These studiesare
upcoming.
Figure 3. Suggested schema for clinical decision making.
www.TheOncologist.com AlphaMed Press 2014
Adaniel, Jhaveri, Heguy et al. 1025
CME
by Jean Santos on October 19, 2014
http://theoncologist.alphamedpress.org/
Dow
nloaded from
-
Including HER21 and LN1 high-risk patients in thetest cohortmay
bias the analysis and compromise theability to determine whether
the assays have just asstrong predictive potential in a
populationwith lowerrisk overall.
The prohibitive cost of genomic studies is another
obstacleassociated with these tests. Although clearly dependent
onthe health care system of the country and on individual
healthcare plans, the valueofgene expression assays is still
controlled,for the most part, by individual biotechnology
companies.Because the tests are not considered entirely routine, as
ofyet, there is an additional price tag beyond standard
tumorprocessing. We hope that, given the abundance of
availabletests, competition will eventually drive down the cost of
ge-nomic testing.
We still have room to improve on our prognosticationefforts.
With recent studies revealing the utility of immune-related
biomarkers for breast cancer, perhaps, in the nearfuture, levels of
tumor-infiltrating lymphocytes or interleukinexpression will be
incorporated into standard prognostictesting [51]. For now, the
currently available assays provide at
least more information than that provided by traditional
IHC.They have been shown to provide reproducible results
usingroutinely stored tumor specimens. More important,
exploita-tion of the tumor genetic milieu has proven to be an
essentialtool for better understanding of tumor biology. As
such,the assays enhance our ability to study the nature of
eachindividual tumor; given this information, they serve as a
guidefor physicians caring for intermediate-risk early stage
breastcancer patients. The practice of medicine is both science
andart, and ultimately decisions regarding adjuvant
chemother-apywill involve amyriad of factors including but not
limited togenomic assays.
AUTHOR CONTRIBUTIONSConception/Design: Christina Adaniel,
Francisco J. EstevaProvision of study material or patients: Adriana
HeguyCollection and/or assembly of data: Christina Adaniel, Komal
JhaveriData analysis and interpretation: Adriana Heguy, Francisco
J. EstevaManuscriptwriting:ChristinaAdaniel, Komal Jhaveri,
AdrianaHeguy, Francisco
J. EstevaFinal approval ofmanuscript: Christina Adaniel, Komal
Jhaveri, Adriana Heguy,
Francisco J. Esteva
DISCLOSURESThe authors indicated no financial relationships.
REFERENCES
1. Goss PE. Planning cancer control in LatinAmerica and the
Caribbean. In: Lee BL, Badovinac-Crnjevic T et al. Planning cancer
control in LatinAmerica and the Caribbean. Lancet Oncol
2013;14:391436.
2. Siegel R,Ma J, ZouZetal. Cancer statistics, 2014.CA Cancer J
Clin 2014;64:929.
3. CancerGenomeAtlasNetwork. Comprehensivemolecular portraits of
human breast tumours.Nature 2012;490:6170.
4. Liu JC,Voisin V, Bader GD et al. Seventeen-genesignature from
enriched Her2/neu mammarytumor-initiating cells predicts clinical
outcome forhuman HER21:ERa- breast cancer. Proc Natl AcadSci USA
2012;109:58325837.
5. Esteva FJ, Sahin AA, Cristofanilli M et al.Molecular
prognostic factors for breast cancermetastasis and survival. Semin
Radiat Oncol 2002;12:319328.
6. Esteva FJ. Monoclonal antibodies, small mole-cules, and
vaccines in the treatment of breastcancer. The Oncologist
2004;9(suppl 3):49.
7.Morrow PK, Zambrana F, Esteva FJ. Recentadvances in systemic
therapy: Advances in systemictherapy for HER2-positive metastatic
breast cancer.Breast Cancer Res 2009;11:207.
8. Fornier M, Esteva FJ, Seidman AD.Trastuzumabin combination
with chemotherapy for the treat-ment of metastatic breast cancer.
Semin Oncol2000;27(suppl 11):3845; discussion 92100.
9.Martn M, Esteva FJ, Alba E et al. Minimizingcardiotoxicity
while optimizing treatment efficacywith trastuzumab: Review and
expert recommen-dations. The Oncologist 2009;14:111.
10. Lenihan DJ, Esteva FJ. Multidisciplinary strat-egy
formanaging cardiovascular riskswhen treatingpatients with early
breast cancer. The Oncologist2008;13:12241234.
11. Dean-ColombW, Esteva FJ. Emerging agents inthe treatment of
anthracycline- and taxane-refractory metastatic breast cancer.
Semin Oncol2008;35:S31S38; quiz S40.
12. Ross JS, Hatzis C, SymmansWF et al. Commer-cializedmultigene
predictors of clinical outcome forbreast cancer. The Oncologist
2008;13:477493.
13.YangM, Rajan S, Issa AM. Cost effectiveness ofgene expression
profiling for early stage breastcancer: A decision-analytic model.
Cancer 2012;118:51635170.
14. Paik S, ShakS,TangGetal.Amultigeneassay topredict recurrence
of tamoxifen-treated, node-negative breast cancer. N Engl J Med
2004;351:28172826.
15. Paik S, Tang G, Shak S et al. Gene expressionand benefit of
chemotherapy in women with node-negative, estrogen
receptor-positivebreastcancer. JClin Oncol 2006;24:37263734.
16. Esteva FJ, Sahin AA, Cristofanilli M et al.Prognostic role
of a multigene reverse transcriptase-PCR assay in patients with
node-negative breastcancer not receiving adjuvant systemic therapy.
ClinCancer Res 2005;11:33153319.
17. Harris L, Fritsche H, Mennel R et al. AmericanSociety of
Clinical Oncology 2007 update ofrecommendations for the use of
tumor markers inbreast cancer. J Clin Oncol 2007;25:52875312.
18. DowsettM, Cuzick J,Wale C et al. Prediction ofrisk of
distant recurrence using the 21-gene re-currence score in
node-negative and node-positivepostmenopausal patients with breast
cancer treatedwith anastrozole or tamoxifen: A TransATAC study.J
Clin Oncol 2010;28:18291834.
19. Habel LA, ShakS, JacobsMKetal.Apopulation-based study of
tumor gene expression and risk ofbreast cancer death among lymph
node-negativepatients. Breast Cancer Res 2006;8:R25.
20. Chang JC, Makris A, Gutierrez MC et al. Geneexpression
patterns in formalin-fixed, paraffin-
embedded core biopsies predict docetaxel chemo-sensitivity in
breast cancer patients. Breast CancerRes Treat 2008;108:233240.
21. Parker JS, Mullins M, Cheang MC et al. Super-vised
riskpredictorofbreast cancerbasedon intrinsicsubtypes. J Clin Oncol
2009;27:11601167.
22. Esteva FJ, Hortobagyi GN, Sahin AA et al.Expression of
erbB/HER receptors, heregulin andP38 in primary breast cancer using
quantitativeimmunohistochemistry. Pathol Oncol Res
2001;7:171177.
23. Nielsen TO, Parker JS, Leung S et al. Acomparison of PAM50
intrinsic subtyping withimmunohistochemistry and clinical
prognosticfactors in tamoxifen-treated estrogen receptor-positive
breast cancer. Clin Cancer Res 2010;16:52225232.
24. Gnant M, Filipits M, Greil R et al. Predictingdistant
recurrence in receptor-positive breast can-cer patients with
limited clinicopathological risk:Using the PAM50 risk of recurrence
score in 1478postmenopausal patients of the ABCSG-8 trialtreated
with adjuvant endocrine therapy alone.Ann Oncol 2014;25:339345.
25. van tVeerLJ,DaiH,vandeVijverMJetal.Geneexpression profiling
predicts clinical outcome ofbreast cancer. Nature
2002;415:530536.
26. van de Vijver MJ, He YD, vant Veer LJ et al.A
gene-expression signature as a predictor ofsurvival in breast
cancer. N Engl J Med 2002;347:19992009.
27. Bueno-de-Mesquita JM, LinnSC, Keijzer Retal.Validation of
70-gene prognosis signature in node-negative breast cancer. Breast
Cancer Res Treat2009;117:483495.
28. BuyseM,Loi S, vantVeer Letal.Validation andclinical utility
of a 70-gene prognostic signature forwomen with node-negative
breast cancer. J NatlCancer Inst 2006;98:11831192.
AlphaMed Press 2014TheOncologist
1026 Genome-Based Risk Prediction for Breast Cancer
CME
by Jean Santos on October 19, 2014
http://theoncologist.alphamedpress.org/
Dow
nloaded from
-
29.Wittner BS, Sgroi DC, Ryan PD et al. Analysis ofthe
MammaPrint breast cancer assay in a predom-inantly postmenopausal
cohort. Clin Cancer Res2008;14:29882993.
30. Saghatchian M, Mook S, Pruneri G et al. Addi-tional
prognostic value of the 70-gene signature(MammaPrint() among breast
cancer patients with4-9 positive lymph nodes. Breast
2013;22:682690.
31. SapinoA,RoepmanP,LinnSCetal.MammaPrintmolecular diagnostics
on formalin-fixed, paraffin-embedded tissue. J Mol Diagn
2014;16:190197.
32.Ma XJ, Salunga R, Dahiya S et al. A five-genemolecular grade
index and HOXB13:IL17BR arecomplementary prognostic factors in
early stagebreast cancer. Clin Cancer Res 2008;14:26012608.
33. Jerevall PL,MaXJ, LiHetal. PrognosticutilityofHOXB13:IL17BR
andmolecular grade index in early-stage breast cancer patients from
the Stockholmtrial. Br J Cancer 2011;104:17621769.
34. Habel LA, Sakoda LC, Achacoso N et al.HOXB13:IL17BR and
molecular grade index andrisk of breast cancer death among patients
withlymph node-negative invasive disease. BreastCancer Res
2013;15:R24.
35. SgroiDC,CarneyE, ZarrellaEetal. Predictionoflate disease
recurrence and extended adjuvantletrozole benefit by the
HOXB13/IL17BR biomarker.J Natl Cancer Inst 2013;105:10361042.
36. Dowsett M, Sestak I, Lopez-Knowles E et al.Comparison of
PAM50 risk of recurrence score withoncotype DX and IHC4 for
predicting risk of distantrecurrence after endocrine therapy. J
Clin Oncol2013;31:27832790.
37. Sgroi DC, Sestak I, Cuzick J et al. Prediction oflate
distant recurrence in patients with oestrogen-
receptor-positive breast cancer: A prospective com-parisonof
thebreast-cancer index (BCI) assay,21-generecurrence score, and
IHC4 in the TransATAC studypopulation. Lancet Oncol
2013;14:10671076.
38. Fan C, Oh DS, Wessels L et al. Concordanceamong
gene-expression-based predictors for breastcancer. N Engl J Med
2006;355:560569.
39. Rete`l VP, Joore MA, Drukker CA et al. Pro-spective
cost-effectiveness analysis of genomicprofiling in breast cancer.
Eur J Cancer 2013;49:37733779.
40. Lamond NW, Skedgel C, Rayson D et al. Cost-utility of the
21-gene recurrence score assay innode-negative and node-positive
breast cancer.Breast Cancer Res Treat 2012;133:11151123.
41.Ward S, ScopeA, Rafia R et al. Gene expressionprofiling and
expanded immunohistochemistrytests to guide the use of adjuvant
chemotherapy inbreast cancer management: A systematic reviewand
cost-effectiveness analysis. Health TechnolAssess 2013;17:1302.
42. Hammond ME, Hayes DF, Dowsett M et al.American Society of
Clinical Oncology/College OfAmerican Pathologists guideline
recommendationsfor immunohistochemical testing of estrogen
andprogesterone receptors inbreast cancer. J
ClinOncol2010;28:27842795.
43. Harvey JM, Clark GM, Osborne CK et al.Estrogen receptor
status by immunohistochemistryis superior to the ligand-binding
assay for predictingresponse to adjuvant endocrine therapy in
breastcancer. J Clin Oncol 1999;17:14741481.
44. Iwamoto T, Booser D, Valero V et al. Estrogenreceptor
(ER)mRNAandER-relatedgeneexpressionin breast cancers that are 1% to
10% ER-positive
by immunohistochemistry. J Clin Oncol 2012;30:729734.
45. Sparano JA. TAILORx: Trial assigning individu-alized options
for treatment (Rx). Clin Breast Cancer2006;7:347350.
46. Albain KS, Barlow WE, Ravdin PM et al.Adjuvant chemotherapy
and timing of tamoxifenin postmenopausal patients with
endocrine-responsive, node-positive breast cancer: A phase3,
open-label, randomised controlled trial.
Lancet2009;374:20552063.
47. Rutgers E, Piccart-GebhartMJ, Bogaerts J et al.The EORTC
10041/BIG 03-04 MINDACT trial isfeasible: Results of the pilot
phase. Eur J Cancer2011;47:27422749.
48. Bartlett J, Canney P, Campbell A et al. Selectingbreast
cancer patients for chemotherapy: Theopening of the UK OPTIMA
trial. Clin Oncol (R CollRadiol) 2013;25:109116.
49. Prat A, Bianchini G, Thomas M et al.Research-based PAM50
subtype predictor iden-tifies higher responses and improved
sur-vival outcomes in HER2-positive breast cancerin the NOAH study.
Clin Cancer Res 2014;20:511521.
50. Guiu S, Michiels S, Andre F et al. Molecularsubclasses of
breast cancer: How do we definethem?The
IMPAKT2012WorkingGroupStatement.Ann Oncol 2012;23:29973006.
51. Sota Y, Naoi Y,Tsunashima R et al. Constructionof novel
immune-related signature for prediction ofpathological complete
response to neoadjuvantchemotherapy in human breast cancer. Ann
Oncol2014;25:100106.
CME This article is available for continuing medical education
credit at CME.TheOncologist.com.
www.TheOncologist.com AlphaMed Press 2014
Adaniel, Jhaveri, Heguy et al. 1027
CME
by Jean Santos on October 19, 2014
http://theoncologist.alphamedpress.org/
Dow
nloaded from
-
References
http://theoncologist.alphamedpress.org/content/19/10/1019.full.html#ref-list-1
This article cites 51 articles, 23 of which you can access for
free at: by Jean Santos on O
ctober 19, 2014http://theoncologist.alpham
edpress.org/D
ownloaded from