Embed Size (px)
Citation preview
Glaucoma Now – Issue No 2, 2011. www.glaucomanow.com 1
i s s u e 2
2 0 11
Main topic:
Trabeculectomy and New Techniques in Glaucoma Surgery
TARGET AUDIENCEThis educational activity is aimed at general ophthalmologists, glaucoma specialists and ophthalmo logy residents.
Glaucoma Now is published and adminis-tered by the editorial board and supported by an unrestricted educational grant from Allergan, inc. Copyright 2010 Editorial Board. All rights reserved. No responsibility as-sumed for injury or damage to persons or property arising from the use of information or ideas contained in this publication.
LEARNING OBJECTIVES• Special Focus: Broad discussion of the advances in trabeculectomy technique. Coverage of the theory behind new technique as well as ongoing trials.
• What’s New: A comprehensive summary of approaches to and development of canal and suprachoroidal surgeries.
• Clinical Issues: use of antifibrotics in trabeculectomy: What options are available? How is quality use best achieved?
• Practical Tips: Conjunctival flap closure. Practical advice on how to best approach secure closure.
Special Focus:
state of the Art Techniques in Glaucoma surgery
PAGe 2
Clinical Issues:
Quality use of Antifibrotics in Trabeculectomy
PAGe 9
What’s New:
Canal & supra- choroidal surgeries
PAGe 6
Practical Tips:
secure Closure of the Conjunctival Flap
PAGe 10
inside this issue:
EDITORIAL BOARDClive Migdal MD, FRCs, FRCOphth Western eye Hospital, London, uK.
Ivan Goldberg MD, FRANZCO, FRACs sydney eye Hospital, sydney, NsW, Australia.
Remo Susanna MD, Professor and Head of Department of Ophthalmology, university of são Paulo, Brazil.
Glaucoma Now is a continuing medical education publication.Distributed worldwide to approximately 40,000 ophthalmologists, our goal is to educate and update general ophthalmologists, glaucoma specialists and ophthalmology residents.
international leaders in the field of glaucoma are invited to contribute to this journal, sharing their most recent insights.
supported by an unrestricted educational grant, the publication is non-promotional and has a fully independent editorial Board.Glaucoma Now is in the process of gaining accreditation for Continuing Medical education (CMe) by the european Accredita-tion Council for Continuing Medical Accreditation.
Executive officer: Patricia Buchholz RPh, PhD Karlsruhe, Germany [email protected] Production by Phosworks www.phosworks.se

2 Glaucoma Now – Issue No 2, 2011. www.glaucomanow.com
special Focus:
state of the Art Techniques in Glaucoma surgeryTony Wells MDeye Clinic, Wellington Hospital, Wellington, New Zealand
Capital eye specialists, Wellington, New Zealand
Core Concepts• Despitedevelopmentofguardedfil-tration surgery (GFs) into modern trab-eculectomy over the last 40 years, cur-rent methods still lack efficiency, high success rates and long-term stability. • Thebestorganisedandwellknownnew approach to trabeculectomy is the Moorfields safe surgery system (Msss). • MitomycinC(MMC)improvespost-trabeculectomy iOP control signifi-cantly, but is also associated with bleb leaks or long-term hypotony. The lat-ter issues may be minimized with ap-propriate surgical technique.• Pre-surgicaltreatmentwithMMCtodecrease ocular surface inflammation may decrease risk of failure by scar-ring. • The Express implant effectivelystents the sclerotomy, but further
studies are needed to demonstrate long-term efficacy and safety.• The3yeardataoftheTubevs.Tra-beculectomy study fulfil expectations, demonstrating a 31% chance of fail-ure in the trabeculectomy group.• Bleb morphology needs to be op-timized, diffuse blebs are desirable. The new Moorfields system is useful for adequately grading blebs.• Non-penetratingglaucomasurgery(NPGs) approaches have decreased complication rates, but also yield less iOP-lowering effects. YAG laser goniopuncture may be needed to cre-ate a sclerostomy.• Inthelast10yearstrabeculectomysuccess and complication rates have improved significantly due to a better understanding of functional compo-nents of the surgery as well as man-agement of wound healing
IntroductionDespite serial improvements over the guarded filtration surgery (GFS) de-scribed by Cairns and Watson1-4 that has evolved into modern trabeculec-tomy, GFS still lacks the efficiency, high success rates, and long term stabil-ity expected from, for example, cataract surgery. Incremental gains particularly in the peri-operative period mean in-creased safety with refinements such as releasable or adjustable sutures, anti-me-tabolites and improved understanding of pre-existing risk factors for failure. Modern trabeculectomy is different enough from Cairns and Watson’s origi-nal description, hence even the name it-self is a misnomer; usually no trabeculum is excised. But the core advance of the Watson and Cairns trabeculectomy, the message of ‘control outflow to improve the safety of the procedure’, became ne-glected frequently enough in later years
to detail and a deep understanding of how components of the procedure inter-act. New approaches to trabeculectomy with close attention to underlying prin-ciples of aqueous dynamics and tissue responses were developed; currently the best organised and well known of these is the Moorfields Safe Surgery System (MSSS), although many individual sur-geons, having grasped the ideas behind MSSS, have developed their own modi-fications.
Technical advances in trabeculectomyAnti-scarring agentsMitomycin C (MMC) in particular im-proves post-trabeculectomy IOP control significantly, but also amplifies imper-fections in surgical technique, increases the risks of complications such as bleb leaks, bleb-related endophthalmitis, and long-term hypotony with secondary con-sequences. While MMC is blamed for these complications, they were common after full-thickness surgery that predated antimetabolites; they may be minimized with appropriate surgical technique. MMC may be safer for operating room staff and patients if it is stained with trypan blue or indocyanine green (Figure 1), with no adverse effects6, 7
Preparation and Conjunctival ApproachWhen MMC became more common in GFS, increased conjunctival wound leaks led to a change from fornix- to limbus-based conjunctival flaps. As better bleb morphology is more likely after a fornix-based approach8, 9 conjunctival incisions are more popular at the limbus. While wound leaks in the early postoperative period are detected more commonly with limbal incisions, small early wound leaks have a minor influence on long term sur-gical outcome10, 11. A fornix-based inci-
as postoperative flat anterior chambers, choroidal detachments, and hypotony maculopathy came to be expected, and many authors published results showing that the control of IOP after surgery was less than ideal. Multiple non-trabeculectomy surgical techniques and variations on these have also been published, usually as case series compared with trabeculectomy, and typ-ically the newer procedure outperformed a fairly lackluster set of trabeculectomy outcomes. So far, few of these alterna-tive approaches have been able to match the efficiency, effectiveness and economy of a well-performed and managed trab-eculectomy. Recently the Tube vs. Trab study5 demonstrated similar short-term efficacy and safety of these two proce-dures, with long term results awaited. While trabeculectomy might be very simple in concept, performing it well and consistently requires fastidious attention

Glaucoma Now – Issue No 2, 2011. www.glaucomanow.com 3
sion with a corneal traction suture12, of-fers better surgical visibility with easier access, hence a more precise scleral flap construction and suture placement. In the early post-surgical period the con-junctiva provides little resistance to flow and even a tight closure of the conjunc-tival wound will not prevent hypotony if the scleral parts of the operation are not well constructed. Pre-surgical treatment to decrease ocular surface inflammation may decrease risk of failure by scarring13. The superior limbus is the preferred site to minimize bleb exposure problems
Scleral flap, Sclerostomy, and SuturesIt is the combination of the scleral flap and sutures, in conjunction with the un-derlying sclerostomy that controls the early postoperative IOP. Simple mea-sures with attention to detail, under-standing scleral flap function, and care-fully using adjustable/releasable sutures, early postoperative hypotony and flow-on complications can be minimized. Major points to consider for scleral flap construction and suture placement14-17 :
Resistance to outflow arises from scler-•al flap apposition over its bed and the sclerostomy edge, not the apposition of the flap edges to the scleral bed. Keep the sides of the scleral flap be-•hind the posterior extent of the scle-rostomy: flow control may be lost if side incisions are too anterior, and it helps to direct aqueous flow posteri-orly.Avoid making the sclerostomy large •relative to the scleral flap, to avoid full-thickness fistulas as the tissue
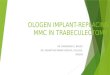
remodels (Figure 2). Punches such as the Kelly or Khaw are best. Flap width should be wider (>0.5mm each side) than the sclerostomy.Using a crescent blade to create the •scleral tunnel may facilitate consistent scleral flaps. Keep the antero-posterior extent of the central trapdoor < 2.5mm to decrease the chance of a flap that is too thin or too thick.Consider a W-shaped or modified •trapezoidal flap (Figure 3). With in-creased resistance to lateral flow, pos-terior flow is maximized, and the short anterior dissection distance minimizes mistakes in scleral flap depth.
Avoid full thickness flow through the •trapdoor: a perforating blood vessel or suture hole in the flap overlying the sclerostomy will compromise scleral flap function.A suture that is both releasable and •adjustable offers maximal control of immediate postoperative flow. (Figure 4). Four throws of 10-0 Ethilon are dependable and robust, and yet remain adjustable.Test scleral flap ability to limit flow •before closing the conjunctiva: repres-surize the anterior chamber to ensure adequate outflow resistance. Aim for day 1 IOP of approximately 20 via appropriate suture tightness and then consider lowering the IOP by adjust-ing the sutures
Figure 1. Indocyanine green (IGC) (or try-pan blue) can be mixed with Mitomycin C to show exactly where the MMC has gone, how large the treatment area is, and the location of any spilt antimetabolite; making the procedure safer for the patient and op-erating theatre staff. Trypan blue stain lasts for several hours, ICG is visible for a day or two after surgery.
Figure 2. Full thickness drainage at the edge of the scleral flap results from the edge of the sclerostomy being too close to the edge of the scleral flap. The appearance of an avascular (‘cystic’) area overlying the full-thickness defect is characteristic, some-times referred to as an ‘aqueous jet’, and was the typical appearance following the full-thickness glaucoma procedures that preceded guarded filtration surgery. Blebs like this typically weep and are associated with late hypotony and bleb-related en-dophthalmitis. To avoid this, ensure that the width of the scleral flap is much greater than that of the sclerostomy.
Figure 3. The W-shaped flap, outlined in orange, is the author’s preferred scleral flap construction. The smallest grey semi-circle represents the sclerostomy made by a 0.5mm Khaw punch, and the blue arrows show the difference in the distances that aqueous has to travel against resistance to reach the subconjunctival space, with the resulting aqueous flow represented by the grey arrows. The orange arrows show the position and force directions of adjust-able sutures; in most cases only two are required.
Figure 4. Adjustable suture placement in W-flap trabeculectomy. Left image: Sutures placed with corneal loops in peripheral corneal grooves allowing complete removal in case adjust-ment fails. Placing loops into corneal grooves ensures they are comfortable, and do not necessarily need to be removed if post-surgical progress is good. Loops above the trapdoor itself are in preparation for tying. Right image: the suture on the right is tight, Note the small loop of suture extending from the 4-throw knot which avoids the loop catching in tenons tissue if removal is desired. The left suture is being tightened. Holding the loop end tying for-ceps along the line of the suture, and holding the free suture end across the line of the suture ensures that if it breaks, it is the free end that breaks first. This patient had Sturge-Weber Syndrome with a large choroidal haemangioma, the AC infusion (Lewicky cannula) ensured that control of the IOP and anterior chamber is not lost during the procedure. IOP on day 1 was 22mmHg, suture adjustment to 14mmHg on day 1 was followed by further adjustment to 12mmHg at week 2.
4 Glaucoma Now – Issue No 2, 2011. www.glaucomanow.com
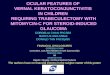
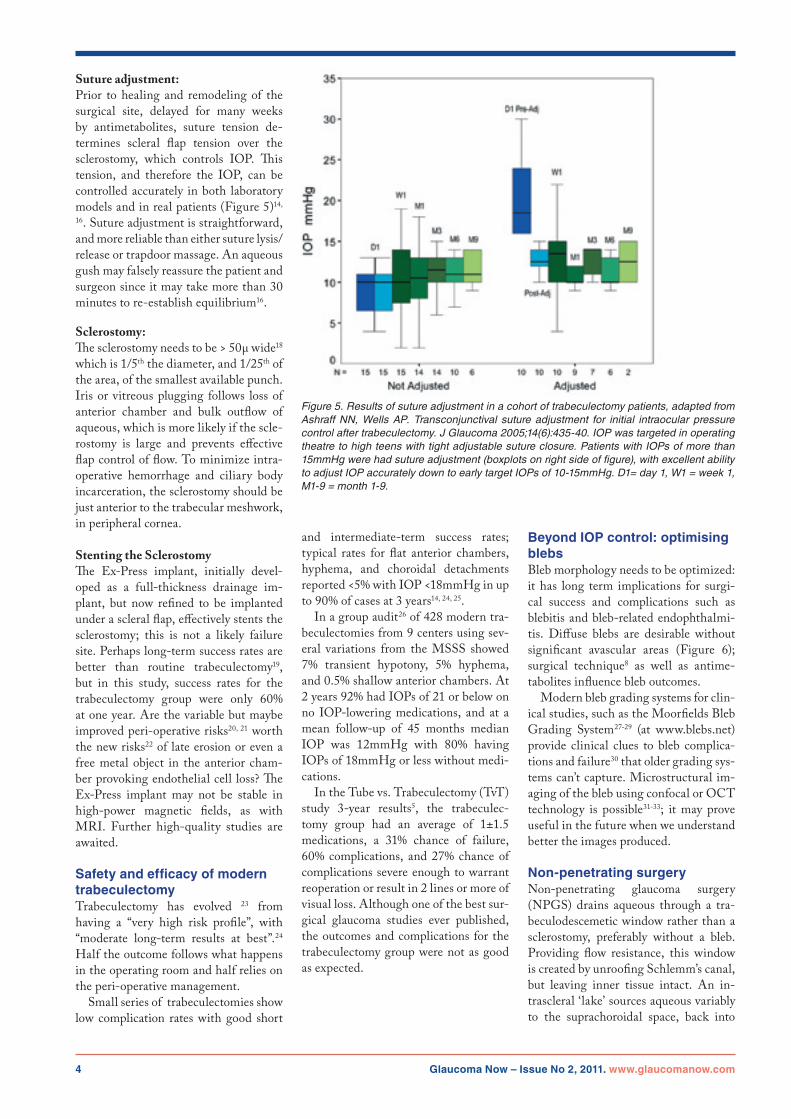
Suture adjustment:Prior to healing and remodeling of the surgical site, delayed for many weeks by antimetabolites, suture tension de-termines scleral flap tension over the sclerostomy, which controls IOP. This tension, and therefore the IOP, can be controlled accurately in both laboratory models and in real patients (Figure 5)14,
16. Suture adjustment is straightforward, and more reliable than either suture lysis/release or trapdoor massage. An aqueous gush may falsely reassure the patient and surgeon since it may take more than 30 minutes to re-establish equilibrium16.
Sclerostomy: The sclerostomy needs to be > 50µ wide18 which is 1/5th the diameter, and 1/25th of the area, of the smallest available punch. Iris or vitreous plugging follows loss of anterior chamber and bulk outflow of aqueous, which is more likely if the scle-rostomy is large and prevents effective flap control of flow. To minimize intra-operative hemorrhage and ciliary body incarceration, the sclerostomy should be just anterior to the trabecular meshwork, in peripheral cornea.
Stenting the SclerostomyThe Ex-Press implant, initially devel-oped as a full-thickness drainage im-plant, but now refined to be implanted under a scleral flap, effectively stents the sclerostomy; this is not a likely failure site. Perhaps long-term success rates are better than routine trabeculectomy19, but in this study, success rates for the trabeculectomy group were only 60% at one year. Are the variable but maybe improved peri-operative risks20, 21 worth the new risks22 of late erosion or even a free metal object in the anterior cham-ber provoking endothelial cell loss? The Ex-Press implant may not be stable in high-power magnetic fields, as with MRI. Further high-quality studies are awaited.
Safety and efficacy of modern trabeculectomyTrabeculectomy has evolved 23 from having a “very high risk profile”, with “moderate long-term results at best”.24 Half the outcome follows what happens in the operating room and half relies on the peri-operative management. Small series of trabeculectomies show low complication rates with good short
and intermediate-term success rates; typical rates for flat anterior chambers, hyphema, and choroidal detachments reported <5% with IOP <18mmHg in up to 90% of cases at 3 years14, 24, 25. In a group audit26 of 428 modern tra-beculectomies from 9 centers using sev-eral variations from the MSSS showed 7% transient hypotony, 5% hyphema, and 0.5% shallow anterior chambers. At 2 years 92% had IOPs of 21 or below on no IOP-lowering medications, and at a mean follow-up of 45 months median IOP was 12mmHg with 80% having IOPs of 18mmHg or less without medi-cations. In the Tube vs. Trabeculectomy (TvT) study 3-year results5, the trabeculec-tomy group had an average of 1±1.5 medications, a 31% chance of failure, 60% complications, and 27% chance of complications severe enough to warrant reoperation or result in 2 lines or more of visual loss. Although one of the best sur-gical glaucoma studies ever published, the outcomes and complications for the trabeculectomy group were not as good as expected.
Beyond IOP control: optimising blebsBleb morphology needs to be optimized: it has long term implications for surgi-cal success and complications such as blebitis and bleb-related endophthalmi-tis. Diffuse blebs are desirable without significant avascular areas (Figure 6); surgical technique8 as well as antime-tabolites influence bleb outcomes. Modern bleb grading systems for clin-ical studies, such as the Moorfields Bleb Grading System27-29 (at www.blebs.net) provide clinical clues to bleb complica-tions and failure30 that older grading sys-tems can’t capture. Microstructural im-aging of the bleb using confocal or OCT technology is possible31-33; it may prove useful in the future when we understand better the images produced.
Non-penetrating surgeryNon-penetrating glaucoma surgery (NPGS) drains aqueous through a tra-beculodescemetic window rather than a sclerostomy, preferably without a bleb. Providing flow resistance, this window is created by unroofing Schlemm’s canal, but leaving inner tissue intact. An in-trascleral ‘lake’ sources aqueous variably to the suprachoroidal space, back into
Figure 5. Results of suture adjustment in a cohort of trabeculectomy patients, adapted from Ashraff NN, Wells AP. Transconjunctival suture adjustment for initial intraocular pressure control after trabeculectomy. J Glaucoma 2005;14(6):435-40. IOP was targeted in operating theatre to high teens with tight adjustable suture closure. Patients with IOPs of more than 15mmHg were had suture adjustment (boxplots on right side of figure), with excellent ability to adjust IOP accurately down to early target IOPs of 10-15mmHg. D1= day 1, W1 = week 1, M1-9 = month 1-9.

Glaucoma Now – Issue No 2, 2011. www.glaucomanow.com 5
the cut ends of Schlemm’s canal, or into intra-scleral lymphatics. There are many variations, sometimes with stents. NPGS may have decreased compli-cation rates, but with diminished IOP-lowering effect compared with trab-eculectomy. YAG laser goniopuncture may be needed to create a sclerostomy. Mitomycin is increasingly used, and blebs are associated with better IOP control35 (while intrascleral lake sizes may not be36). There is a steep learning curve, and low IOPs early after surgery lead to better outcomes37.
ConclusionIn the last ten years trabeculectomy success and complication rates have improved significantly, not as a result of redesigning the procedure but from attention to detail, avoiding hypotony, managing wound healing, and a deeper understanding of the functional compo-nents of this form of glaucoma filtering surgery. Remaining challenges include unpredictable wound healing responses and, despite 5FU and MMC, subop-timal tools for modulating the wound healing response.
References1. Cairns Je. Trabeculectomy. Preliminary report of a new method. Am J Ophthalmol 1968;66(4):673–9.
2. Cairns Je. Trabeculectomy. sub-title: “a sur-gical method of reducing intra-ocular pressure in chronic simple glaucoma without sub-conjunctival drainage of aqueous humour”. Trans Ophthalmol SocUK1969;88:231–3.
3. Cairns JE. Trabeculectomy. Preliminary re-port of a surgical method of reducing intra-ocular pressure in chronic simple glaucoma without sub-conjunctival drainage of aqueous humor. Bibl Ophthalmol1970;81:143–53.
4. Cairns Je. surgical treatment of primary open-angle glaucoma. Trans Ophthalmol soc u K1972;92:745–56.
5. GeddeSJSJ,FeuerWJ,HerndonLW,BrandtJD, Budenz DL, Tube Versus Trabeculectomy study Group. Three-year follow-up of the tube versus trabeculectomy study. Am J Ophthalmol. 2009;148(5):670–84.
6. Reeves G WR, Crowston JG, small KM, Wells AP. The effect of iCG on mitomycin C cytotox-icity in human tenon fibroblasts. J Glaucoma. 2007;16(5):479–82.
7. Healey PR CJ. TrTypan blue identifies anti-metabolite treatment area in trabeculectomy. Br JOphthalmol.2005;89(9):1152–6.
8. Wells AP, Cordeiro MF, Bunce C, Khaw PT. Cystic bleb formation and related complications in limbus- versus fornix-based conjunctival flaps in pediatric and young adult trabeculectomy with mi-tomycinC.Ophthalmology2003;110(11):2192–7.
9. el sayyad F, el-Rashood A, Helal M, et al. Fornix-based versus limbal-based conjunctival flaps in initial trabeculectomy with postopera-tive5-fluorouracil: four-year follow-upfindings.JGlaucoma1999;8(2):124–8.
10. Henderson HW, ezra e, Murdoch ie. early postoperative trabeculectomy leakage: incidence, time course, severity, and impact on surgical out-come.BrJOphthalmol2004;88(5):626–9.
11. Parrish RK, 2nd, schiffman JC, Feuer WJ, Heuer DK. Prognosis and risk factors for early postoperative wound leaks after trabeculectomy withandwithout5-fluorouracil.AmJOphthalmol2001;132(5):633–40.
12. edmunds B BC, Thompson JR, salmon JF, Wormald RP. Factors associated with success in first-time trabeculectomy for patients at low risk of failure with chronic open-angle glaucoma. Oph-thalmology2004;111(1):97–103.
13.Breusegem C SL, Van Ginderdeuren R,Vandewalle e, Renier C, Van de Veire s, Fieuws s, Zeyen T, stalmans i. Preoperative nonsteroidal anti-inflammatory drug or steroid and outcomes after trabeculectomy: a randomized controlled trial.Ophthalmology2010;117(7):1324–30.
14. Ashraff NN, Wells AP. Transconjunctival suture adjustment for initial intraocular pres-sure control after trabeculectomy. J Glaucoma 2005;14(6):435–40.
15.BirchallW,BedggoodA,WellsAP.Doscleralflap dimensions influence reliability of intraocular pressure control in experimental trabeculectomy? eye 2006.
16. Wells AP, Bunce C, Khaw PT. Flap and suture manipulation after trabeculectomy with adjust-able sutures: titration of flow and intraocular pres-sure in guarded filtration surgery. J Glaucoma 2004;13(5):400–6.
17. Birchall W WA. The effect of scleral flap edge apposition on intraocular pressure control in ex-perimental trabeculectomy. Clin experiment Oph-thalmol.2008;34(4):353–7.
18. Team. AP. experimental flow studies in glau-coma drainage device development. Br J Oph-thalmol2001;85:1231–36.
19. LA dJ. The ex-PRess glaucoma shunt ver-sus trabeculectomy in open-angle glaucoma: a prospective randomized study. Adv Ther. 2009;26(3):336–45.
20. Maris PJ Jr iK, Netland PA. Comparison of tra-beculectomy with ex-PRess miniature glaucoma
device implanted under scleral flap. J Glaucoma. 2007;16(1):14–9.
21. De Feo F BA, Bricola G, scotto R, Traverso Ce. efficacy and safety of a steel drainage device implanted under a scleral flap. Can J Ophthalmol. 2009;44(4):457–62.
22. stewart RM DJ, Ashmore eD, Ayyala Rs. Complications following ex-press glaucoma shunt implantation.AmJOphthalmol.2005;140(2):340–1.
23.Gale J WA. Medium-term outcomes of safesurgery system trabeculectomies. Br J Ophthal-mol.2008;92(9):1232–5.
24. Mosaed s MD. Aqueous shunts in the treat-ment of glaucoma. expert Rev Med Devices. 2010;7(5):661–6.
25.StalmansI,GillisA,LafautAS,ZeyenT.Safetrabeculectomy technique: long term outcome. Br JOphthalmol2006;90(1):44–7.
26. JF Kirwan DB, P shah, JDA MacLeod, C Da-vison, P Corridan, A McNaught, A Wells, A King, s Mukherjee, Gs Ang, R Arora, A Lockwood, P Agrawal. ‘Trabeculectomy in the 21st century’: early and intermediate outcomes. uK and eire Glaucoma society. London, 2010.
27. Wells AP, James K, Birchall W, Wong T. in-formation loss in 2 bleb grading systems. J Glau-coma2007;16(2):246–50.
28. Wells AP, Ashraff NN, Hall RC, Purdie G. Comparison of two clinical Bleb grading systems. Ophthalmology2006;113(1):77–83.
29. Crowston JG, Kirwan JF, Wells A, et al. evalu-ating clinical signs in trabeculectomized eyes. Eye2004;18(3):299–303.
30.MarksJRCJ,PetoT,MinassianD,KhawPT.Postoperative increased bleb vascularity persists for over one year and has implications for intraoc-ular pressure control. ARVO. Fort Lauderdale, Florida, 2004.
31.Messmer EM, Zapp DM, Mackert MJ, etal. in vivo confocal microscopy of filtering blebs after trabeculectomy. Arch Ophthalmol 2006;124(8):1095–103.
32.LabbeA,DupasB,HamardP,BaudouinC.Invivo confocal microscopy study of blebs after filter-ingsurgery.Ophthalmology2005;112(11):1979.
33.WellsAPWL,BirchallW.Invivofluorescencemode confocal microscopy of subepithelial tis-sues in glaucoma filtering blebs. Ophthalmic surg LasersImaging.2010;41(1):78–82.
34.Bissig A FM, Mermoud A, Roy S. Deepsclerectomy with the ex-PRess X-200 implant for the surgical treatment of glaucoma. int Oph-thalmol.2010;30(6):661–8.
35.Cabrejas L RG, Muñoz-Negrete FJ, LosadaD. An ultrasound biomicroscopy study of filtering blebs after deep sclerectomy with a new acrylic implant. eur J Ophthalmol. 2010;Oct 22 [epub ahead of print].
36.ChiharaEHK.RelationBetweentheVolumeof the Lake and intraocular Pressure Reduction After Nonfiltering Glaucoma surgery: A spectral-domain Anterior segment Optical Coherence Tomography study. J Glaucoma. 2010 sept 16. [epub ahead of print].
37.Shaarawy T FJ, Smits G, Mermoud A. Lowfirst postoperative day intraocular pressure as a positive prognostic indicator in deep sclerectomy. BrJOphthalmol.2004;88(5):658–61.
Figure 6. An ideal bleb, 3 years after W-flap trabeculectomy with 0.3mg/ml Mitomycin C applied intraoperatively for 3 minutes. Bleb is diffuse and lightly vascular, asymptom-atic, and IOP has ranged between 9 and 12 mmHg between 2 weeks and 3 years follow-up.

6 Glaucoma Now – Issue No 2, 2011. www.glaucomanow.com
What’s New
Canal & supra-choroidal surgeriesNew Glaucoma surgery improving Anterior Aqueous Drainage Robert L. stamper, M.D., Professor of Ophthalmology, university of California, san Francisco, usA
IntroductionAnti-glaucoma medicines, laser surgery and incisional surgery all seek to lower the intraocular pressure (IOP). Inci-sional surgery is indicated when medi-cal treatment and/or laser surgery have failed, are likely to fail or are not avail-able or practical. The most standard surgical procedure is trabeculectomy (or some variation thereof e.g. ExPRESS shunt): aqueous is shunted from the an-terior chamber under Tenon’s capsule and conjunctiva anteriorly. Antimetabo-lites markedly improved the success rate of anterior filtration but brought poten-tial long term problems of late leaking and endophthalmitis. When anterior filtering surgery fails or is likely to fail such as in some secondary glaucomas, tube and plate shunts drain aqueous hu-mor to the equatorial region of the eye
Core Concepts• Both theappearanceof theopticnerve head (ONH) and the retinal nerve fibre layer (RNFL) as well as the visual function maybe influenced by age.• Agealonehasbeendescribedtoaccountforlossofappr.25%ofop-tic nerve fibres during a 70-year life span.• Thereisincreasingevidencethatageing related loss of neuronal structures is not a linear process.• Weincreasinglyrelyontechnologyto diagnose and monitor glaucoma and it is essential that instruments differentiate between pathological changes and age related changes.• Most diagnostic devices do ac-count for the effect, even though normative databases used are fairly limited.• Longitudinal studies and largerage-related normative databases are needed to use current technolo-gies more optimally.
under Tenon’s capsule and conjunctiva. These procedures are time-tested and generally succeed in experienced hands. Hypotony, anterior chamber bleed-ing, suprachoroidal hemorrhage, serous choroidal detachments, late bleb leaks, endophthalmitis, corneal decompensa-tion and bleb scarring occasionally (but too often) bedevil our efforts to prevent vision loss. The last decade or so has seen some interesting efforts to provide an ef-fective and safer alternative. Holmium laser sclerostomy, viscocanalostomy and deep sclerectomy achieved some success but have lost adherents because of inef-fectiveness, complicated surgery or un-anticipated problems. Several new approaches to improve aqueous drainage have have gained some enthusiasts. They can be classified ei-ther by the approach, ab interno vs. ab externo, by the tissue compartment into which the shunted aqueous flows or by the location of the actual surgical site. Some of the more popular of these as well as one that is still in its infancy are described, classified by the approach and the principles, and what is known about results.
Recent approachesThree new ab interno procedures bypass trabecular meshwork by shunting fluid from the anterior chamber either di-rectly into Schlemm’s canal or into the suprachoroidal space.
• TrabectomeAt its distal end, Trabectome® (Neome-dix, Tustin, CA, USA)1 has a ceramic probe that is inserted into Schlemm’s ca-nal under gonioscopic control after be-ing passed across the anterior chamber through a clear corneal limbal incision. Proximal to the ceramic tip, the trabe-cular mesh is ablated by a radiofrequency current across a spacer (Figure 1). About one quarter of the mesh can be ablated through one corneal wound. Presumably this permits aqueous more easily and di-rectly to enter Schlemm’s canal and the collector channels. Advantages are relatively short dura-tion (about 10–15 minutes), IOP drop to the 15–17 mm Hg range in about 65% of eyes with Trabectome alone and 87% in eyes combined with cataract extraction, and a low rate of serious complications.2,3 Good results have been reported out to
Figure 1. Trabectome in action (Courtesy Neomedix, Tustin, CA)
Glaucoma Now – Issue No 2, 2011. www.glaucomanow.com 7
4 years.4 The operation can be combined with cataract extraction especially clear corneal, temporal phacoemulsification.5 Early post-operative complications in-clude an IOP spike, back bleeding from Schlemm’s canal with hyphema, De-scemet’s detachment or damage, and failure to find Schlemm’s canal. In the absence of a leaking wound, hypotony is rare. There are no long-term, pro-spective, controlled studies comparing Trabectome trabeculotomy with other techniques, or comparing combined Trabectome/cataract surgery with cata-ract surgery alone. This is a relatively simple operation that can fit into the glaucoma surgical spectrum between la-ser trabeculoplasty and trabeculectomy or another filtration procedure.
• Glaukos (IStent)The IStent (Glaukos, Laguna Hills, CA, USA) is an L-shaped titanium tube that fits into Schlemm’s canal via an ab in-terno insertion and shunts fluid from the anterior chamber to the collector chan-nels by-passing the mesh and the jux-tacanalicular tissue wherein lies much of the outflow resistance. It is inserted under gonioscopic control via a 2 mm clear corneal, temporal limbal incision (Figure 2). Data is available only for insertion of the IStent combined with cataract surgery. The device increases outflow facility above baseline and even more than cataract surgery alone.6 IOP control is improved compared with cata-ract surgery alone.7 In a multicenter, randomized controlled trial comparing cataract surgery alone with cataract sur-gery and single IStent implantation, at one year, the IStent plus cataract group achieved IOP below 21mmHg without medication more often than the cataract alone group (72% vs. 50%) and, while both groups achieved approximately the same IOP, the IStent plus cataract group accomplished that IOP level with fewer medications.8 In both randomized tri-als, the complications were few and not significantly more frequent than cataract surgery alone. Implantation of two de-vices 180 degrees apart might improve outflow and IOP control over one but little published data is available.9
• Drainage to the Suprachoroidal Some aqueous normally drains into the suprachoroidal space whose pressure is negative compared with the anterior
from the scleral side. The device was de-signed with many of the microchannels unopened. These unopened channels could be opened by a titanium-sapphire laser beam aimed at the device through a gonioprism in the postoperative period to increase aqueous drainage if needed. Results with the first generation device were not bad but a second generation de-vice holds out even more promise.
• CanaloplastyIn canaloplasty, through a novel, flex-ible microcannula (ITrak by IScience, Menlo Park, CA, USA) microamounts of viscoelastic are injected to enlarge Schlemm’s canal via an ab externo deep sclerectomy. Then a circumferential 10/0 polypropylene suture applies traction on the trabecular mesh. The cannula contains a fiberoptic bundle whose tiny light emitting diode at the tip is visible through the sclera; this helps ensure the cannula stays in Schlemm’s canal as it is threaded around the limbus.13 First,
chamber.10 A device using an ab interno approach (CyPass) is under investigation. The Cypass (Transcend, Menlo Park, CA, USA) is a tiny tube-like device made of a highly biocompatible material that is inserted into the suprachoroidal space just above the ciliary face across the anterior chamber under gonioscopic control. (Figure 3) The clear corneal, temporal corneal incision is less than 2 mm. The operation is quick; its ease de-pends on angle landmark identification. Preliminary results have been promising although unpublished. Larger studies are underway.
The following new procedures are in-serted via ab externo techniques:
• SolxThe Solx device is a thin, gold microwa-fer with internal channels that carry aqueous from the anterior chamber to the suprachoroidal space.11,12 (Figure 4) The device is implanted ab externo
Figure 2. IStent in situ (Courtesy Glaukos, Laguna Hills, CA)
Figure 3.Cypass device in situ (Courtesy Transcend, Menlo Park, CA) Figure 4. Drawing of the Solx device.
8 Glaucoma Now – Issue No 2, 2011. www.glaucomanow.com
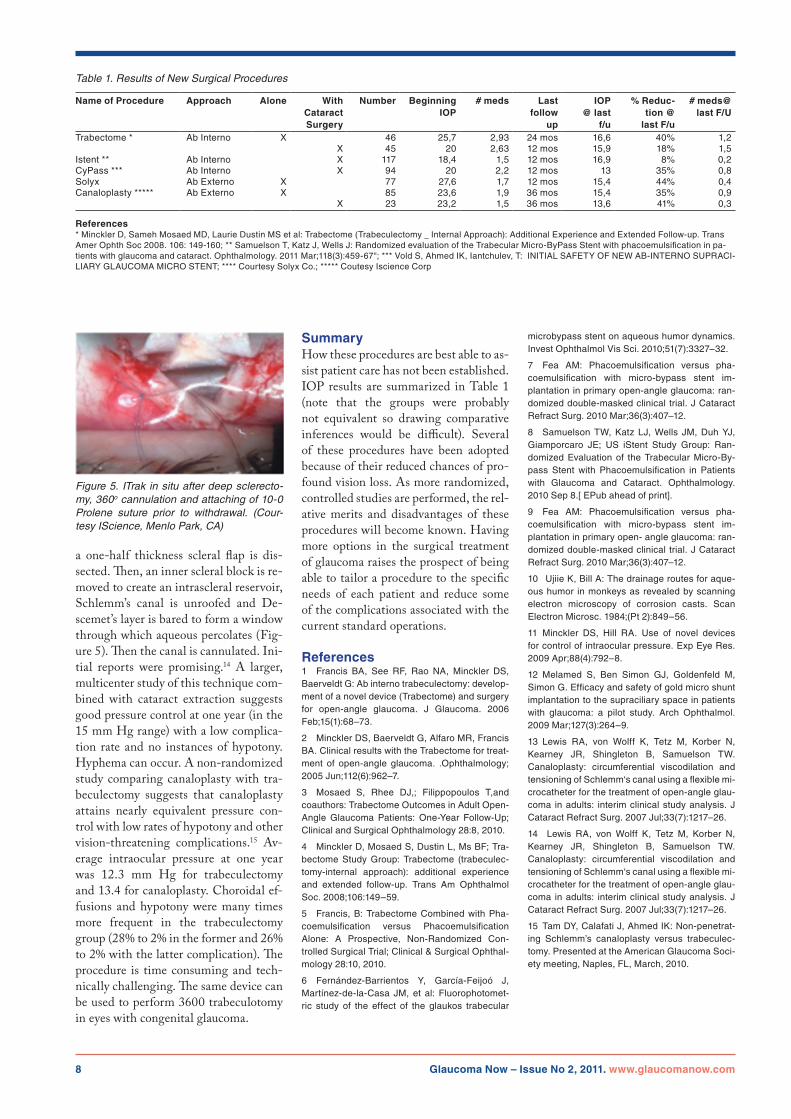
a one-half thickness scleral flap is dis-sected. Then, an inner scleral block is re-moved to create an intrascleral reservoir, Schlemm’s canal is unroofed and De-scemet’s layer is bared to form a window through which aqueous percolates (Fig-ure 5). Then the canal is cannulated. Ini-tial reports were promising.14 A larger, multicenter study of this technique com-bined with cataract extraction suggests good pressure control at one year (in the 15 mm Hg range) with a low complica-tion rate and no instances of hypotony. Hyphema can occur. A non-randomized study comparing canaloplasty with tra-beculectomy suggests that canaloplasty attains nearly equivalent pressure con-trol with low rates of hypotony and other vision-threatening complications.15 Av-erage intraocular pressure at one year was 12.3 mm Hg for trabeculectomy and 13.4 for canaloplasty. Choroidal ef-fusions and hypotony were many times more frequent in the trabeculectomy group (28% to 2% in the former and 26% to 2% with the latter complication). The procedure is time consuming and tech-nically challenging. The same device can be used to perform 3600 trabeculotomy in eyes with congenital glaucoma.
SummaryHow these procedures are best able to as-sist patient care has not been established. IOP results are summarized in Table 1 (note that the groups were probably not equivalent so drawing comparative inferences would be difficult). Several of these procedures have been adopted because of their reduced chances of pro-found vision loss. As more randomized, controlled studies are performed, the rel-ative merits and disadvantages of these procedures will become known. Having more options in the surgical treatment of glaucoma raises the prospect of being able to tailor a procedure to the specific needs of each patient and reduce some of the complications associated with the current standard operations.
References1 Francis BA, see RF, Rao NA, Minckler Ds, Baerveldt G: Ab interno trabeculectomy: develop-ment of a novel device (Trabectome) and surgery for open-angle glaucoma. J Glaucoma. 2006 Feb;15(1):68–73.
2 Minckler Ds, Baerveldt G, Alfaro MR, Francis BA. Clinical results with the Trabectome for treat-ment of open-angle glaucoma. .Ophthalmology; 2005Jun;112(6):962–7.
3 Mosaed S, Rhee DJ,; Filippopoulos T,andcoauthors: Trabectome Outcomes in Adult Open-Angle Glaucoma Patients: One-Year Follow-up; Clinical and surgical Ophthalmology 28:8, 2010.
4 Minckler D, Mosaed s, Dustin L, Ms BF; Tra-bectome study Group: Trabectome (trabeculec-tomy-internal approach): additional experience and extended follow-up. Trans Am Ophthalmol Soc.2008;106:149–59.
5 Francis,B:TrabectomeCombinedwithPha-coemulsification versus Phacoemulsification Alone: A Prospective, Non-Randomized Con-trolled surgical Trial; Clinical & surgical Ophthal-mology 28:10, 2010.
6 Fernández-Barrientos Y, García-Feijoó J, Martínez-de-la-Casa JM, et al: Fluorophotomet-ric study of the effect of the glaukos trabecular
microbypass stent on aqueous humor dynamics. InvestOphthalmolVisSci.2010;51(7):3327–32.
7 Fea AM: Phacoemulsification versus pha-coemulsification with micro-bypass stent im-plantation in primary open-angle glaucoma: ran-domized double-masked clinical trial. J Cataract RefractSurg.2010Mar;36(3):407–12.
8 samuelson TW, Katz LJ, Wells JM, Duh YJ, Giamporcaro Je; us istent study Group: Ran-domized evaluation of the Trabecular Micro-By-pass stent with Phacoemulsification in Patients with Glaucoma and Cataract. Ophthalmology. 2010 sep 8.[ ePub ahead of print].
9 Fea AM: Phacoemulsification versus pha-coemulsification with micro-bypass stent im-plantation in primary open- angle glaucoma: ran-domized double-masked clinical trial. J Cataract RefractSurg.2010Mar;36(3):407–12.
10 ujiie K, Bill A: The drainage routes for aque-ous humor in monkeys as revealed by scanning electron microscopy of corrosion casts. scan ElectronMicrosc.1984;(Pt2):849–56.
11 Minckler Ds, Hill RA. use of novel devices for control of intraocular pressure. exp eye Res. 2009Apr;88(4):792–8.
12 Melamed s, Ben simon GJ, Goldenfeld M, simon G. efficacy and safety of gold micro shunt implantation to the supraciliary space in patients with glaucoma: a pilot study. Arch Ophthalmol. 2009Mar;127(3):264–9.
13 Lewis RA, von Wolff K, Tetz M, Korber N,Kearney JR, shingleton B, samuelson TW. Canaloplasty: circumferential viscodilation and tensioning of schlemm‘s canal using a flexible mi-crocatheter for the treatment of open-angle glau-coma in adults: interim clinical study analysis. J CataractRefractSurg.2007Jul;33(7):1217–26.
14 Lewis RA, von Wolff K, Tetz M, Korber N, Kearney JR, shingleton B, samuelson TW. Canaloplasty: circumferential viscodilation and tensioning of schlemm‘s canal using a flexible mi-crocatheter for the treatment of open-angle glau-coma in adults: interim clinical study analysis. J CataractRefractSurg.2007Jul;33(7):1217–26.
15 TamDY,CalafatiJ,AhmedIK:Non-penetrat-ing schlemm’s canaloplasty versus trabeculec-tomy. Presented at the American Glaucoma soci-ety meeting, Naples, FL, March, 2010.
Figure 5. ITrak in situ after deep sclerecto-my, 360o cannulation and attaching of 10-0 Prolene suture prior to withdrawal. (Cour-tesy IScience, Menlo Park, CA)
Table 1. Results of New Surgical Procedures
Name of Procedure Approach Alone With Cataract Surgery
Number Beginning IOP
# meds Lastfollow
up
IOP @ last
f/u
% Reduc-tion @
last F/u
# meds@ last F/U
Trabectome * Ab interno X 46 25,7 2,93 24 mos 16,6 40% 1,2X 45 20 2,63 12 mos 15,9 18% 1,5
istent ** Ab interno X 117 18,4 1,5 12 mos 16,9 8% 0,2CyPass *** Ab interno X 94 20 2,2 12 mos 13 35% 0,8solyx Ab externo X 77 27,6 1,7 12 mos 15,4 44% 0,4Canaloplasty ***** Ab externo X 85 23,6 1,9 36mos 15,4 35% 0,9
X 23 23,2 1,5 36mos 13,6 41% 0,3
References* Minckler D, sameh Mosaed MD, Laurie Dustin Ms et al: Trabectome (Trabeculectomy _ internal Approach): Additional experience and extended Follow-up. Trans Amer Ophth soc 2008. 106: 149-160; ** samuelson T, Katz J, Wells J: Randomized evaluation of the Trabecular Micro-ByPass stent with phacoemulsification in pa-tientswithglaucomaandcataract.Ophthalmology.2011Mar;118(3):459-67";***VoldS,AhmedIK,Iantchulev,T:INITIALSAFETYOFNEWAB-INTERNOSUPRACI-LiARY GLAuCOMA MiCRO sTeNT; **** Courtesy solyx Co.; ***** Coutesy iscience Corp

Glaucoma Now – Issue No 2, 2011. www.glaucomanow.com 9
Clinical issues:
Quality use of Antifibrotics in TrabeculectomyAshkan Khalili MD, Georgoulas MD PhD Specialist, Peng Tee Khaw PhD FRCS FRCP FRCPath
FSBiol FARVO FMedSci
National institute Health Research Biomedical Research Centre, Moorfields eye Hospital and uCL institute of Ophthalmology, London, uK.
Core Concepts• Wound healing response is themost important determinant of long-term outcome for trabeculectomy• Simple changes in surgical tech-nique can considerably increase safety• Current antifibrotic treatments in-clude steroids and antimetabolites• Antimetabolitessuchas5-FUandMMC are associated with long-term failure and more effective and safer agents are required• Improvementshaveoccurredwithanti-VeGF compounds, steroids or NsAiDs.• Inhibitors of TGF-beta and its in-termediates may be promising• MMPinhibitors improveanti-scar-ring effects
Maximising outcomes with the use of anti-fibrotics in trabeculectomyThe wound healing response to surgery is the most important determinant of the long-term outcome of trabeculectomy. Wound healing is an immensely complex process that includes the activation and silencing of various mechanisms at dif-ferent stages. Based on our recent under-standing of these mechanisms, new anti-scaring approaches have been tried. The current treatments in the clinic include steroids and antimetabolites (5-FU and MMC) to control the scarring. Howev-er, if not used appropriately, these agents have significant risks. Simple changes in surgical technique, such as increasing the surface area of antimetabolite application and methods to control the rate and di-rection of aqueous flow can considerably increase the safety of surgery1 and are summarized in Figure 1.
Many of these measures have now been widely adopted around the world with good results.2 Nonetheless, antimetabo-lites are still associated with long-term failure and better anti-scarring agents with a higher safety profile are required. The anti-VEGF medicines including bevacizumab have shown promise par-ticularly when combined with 5-FU.3 Although the mechanism for this syner-gic effect is not clear, inflammation is one of the major contributors to scarring dur-ing wound healing. Anti-inflammatory drugs, either steroid or NSAID, have offered benefit for the control of scar-ring following surgery. Improvements have also resulted from the optimization of application protocols and new anti-inflammatory drugs. Inhibition of the pro-fibrotic cytok-ines including TGF-beta has been stud-ied extensively but with disappointing results. Different dosing, sustained re-lease formulations, new antibodies and approaches to inhibit the TGF-beta family and its intermediates including CTGF and ALK-5 inhibitor may still be promising4, as may be combinations of therapies. The matrix metalloproteinase (MMP) family plays a key role in many stages of the wound healing from releasing se-questered cytokines in the extra cellular matrix to angiogenesis and scar forma-
tion. As a result the significance of the anti-scarring effects of MMP inhibitors such as Ilomastat to prolong experimen-tal bleb survival has been shown 5,6 to have great promise. In summary, the use of antimetabo-lites has improved the success rate of glaucoma surgery, and with appropriate simple modifications to technique, com-plications can be greatly reduced. Many new therapeutic possibilities promise to improve long term outcomes for glauco-ma surgery combined with entirely new surgical techniques, thereby lowering eye pressure safely to minimize progression for the majority of glaucoma patients.
References1 Khaw PT, Chiang M, shah P. Glaucoma filtra-tion surgery: indications, techniques, and compli-cations.in: Albert & Jakobiec’s Principles & Prac-tice of Ophthalmology. eds: Albert DM, Miller J, AzarDT,BlodiBA:3rded.,2821–2840(Saunders,2008).
2 stalmans, i., Gillis, A., Lafaut, A. s. & Zeyen, T. safe trabeculectomy technique: long term out-come. Br J Ophthalmol90,44–47(2006).
3 How, A. et al. Combined treatment with be-vacizumaband5-fluorouracilattenuatesthepost-operative scarring response after experimental glaucoma filtration surgery. Invest Ophthalmol Vis Sci51,928–932(2010).
4 sapitro, J. et al. suppression of transforming growth factor-ß effects in rabbit subconjunctival fibroblastsbyactivinreceptor-likekinase5inhibi-tor. Mol Vis16,1880–1892(2010).
5 Sherwood,M.B.Asequential,multiple-treat-ment, targeted approach to reduce wound healing and failure of glaucoma filtration surgery in a rab-bit model (an American Ophthalmological society thesis). Transactions of the American Ophthalmo-logical Society104,478–492(2006).
6 Wong, T. T., Mead, A. L. &Khaw, P.T. Matrix Metalloproteinase inhibition Modulates Postop-erative scarring after experimental Glaucoma Filtration surgery. Investigative Ophthalmology & Visual Science44,1097–1103(2003).
Infusion
10 Glaucoma Now – Issue No 2, 2011. www.glaucomanow.com
Practical Tips:
secure Closure of the Conjunctival FlapGarry P. Condon MDAssociate Professor Drexel university College of Medicine, Clinical Assistant Professor university of Pittsburgh, Chairman Department of Ophthal-
mology, Allegheny General Hospital, Pittsburgh Pennsylvania
Core concepts• One of the most critical aspectsin glaucoma filtering surgery is pre-dictable and tight closure of the con-junctival incision.• Fornix based conjunctival flapstend to create a more durable ap-pearing bleb, with limited fibrosis.• TheclosuremethoddescribedbyWisein1993isrecommendable,withslight modifications as described by the author.• It is critical that thewhole flap istightly applied to the cornea-sclera under the anterior conjunctival lip.• Theauthorhasfoundthatthede-scribed technique produces favour-able bleb morphology and reduces bleb migration into the cornea.
One of the most critical aspects in glau-coma filtering surgery is predictable and absolute water tight closure of the con-junctival incision. In the hands of the au-thor, fornix based conjunctival flaps tend to create a more durable appearing dif-fuse posterior bleb with fibrosis limited to the incision site along the limbus. Us-ing a modification of the closure method described by Wise1 with two main dif-
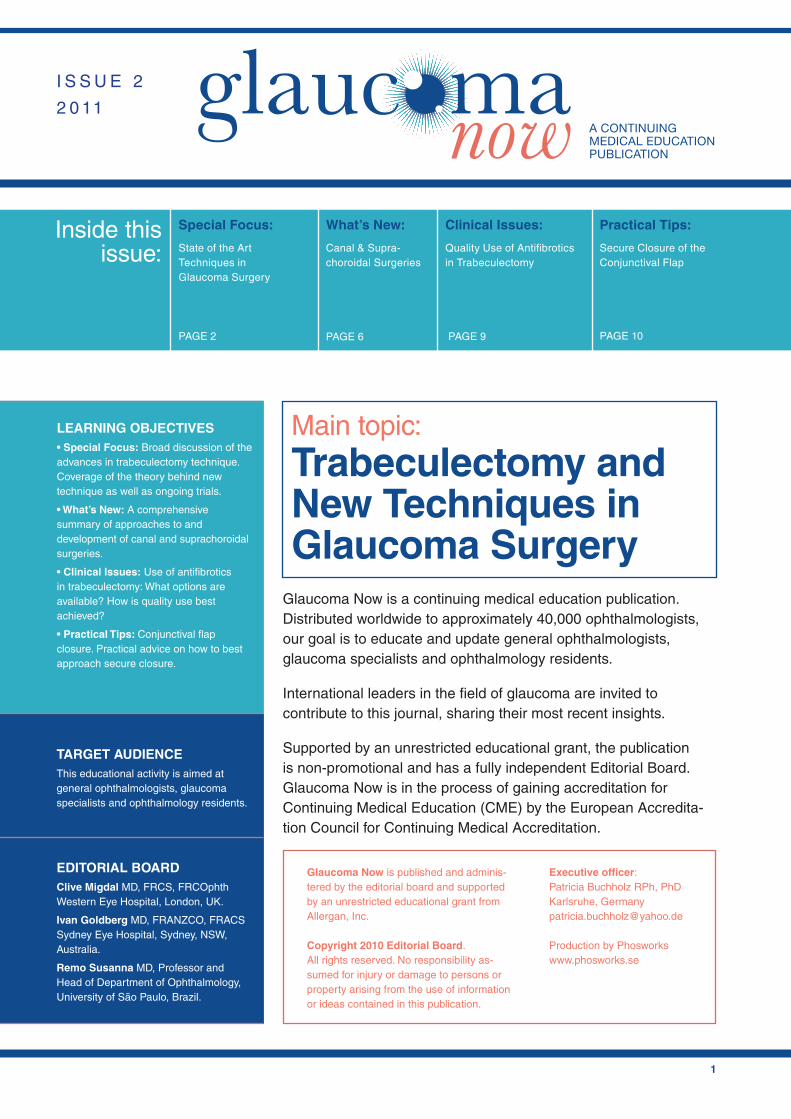
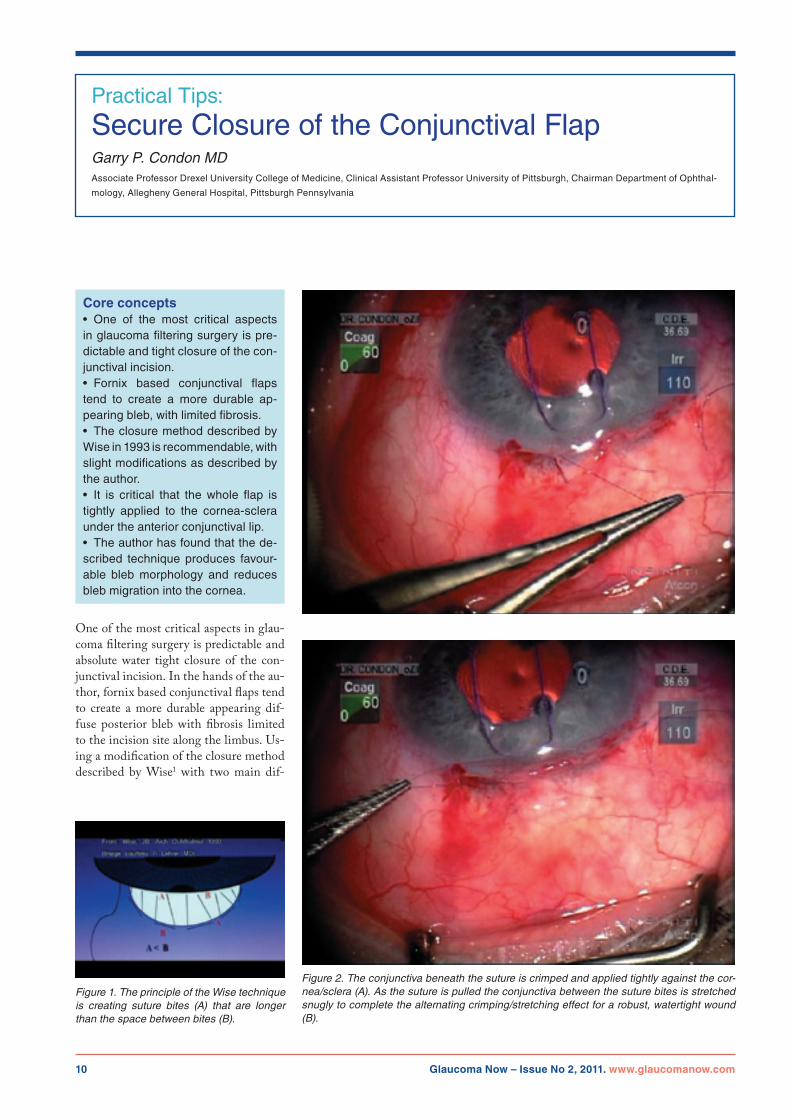
Figure 1. The principle of the Wise technique is creating suture bites (A) that are longer than the space between bites (B).
Figure 2. The conjunctiva beneath the suture is crimped and applied tightly against the cor-nea/sclera (A). As the suture is pulled the conjunctiva between the suture bites is stretched snugly to complete the alternating crimping/stretching effect for a robust, watertight wound (B).
Glaucoma Now – Issue No 2, 2011. www.glaucomanow.com 11
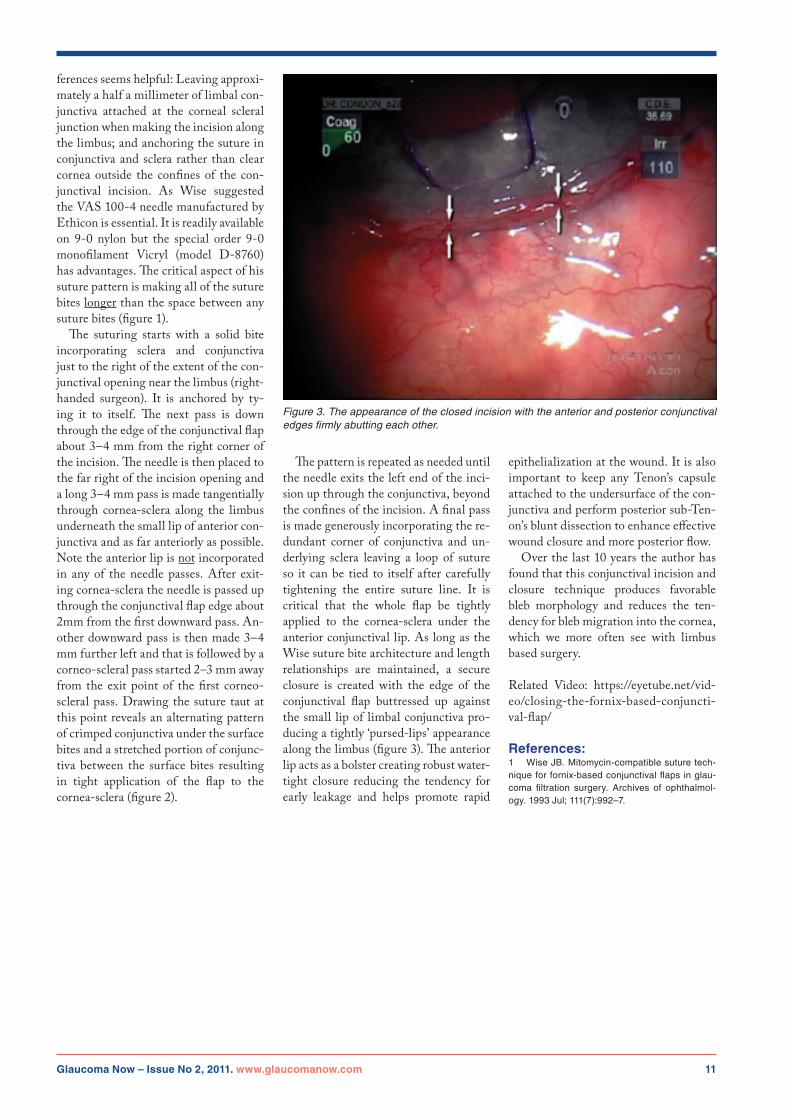
ferences seems helpful: Leaving approxi-mately a half a millimeter of limbal con-junctiva attached at the corneal scleral junction when making the incision along the limbus; and anchoring the suture in conjunctiva and sclera rather than clear cornea outside the confines of the con-junctival incision. As Wise suggested the VAS 100-4 needle manufactured by Ethicon is essential. It is readily available on 9-0 nylon but the special order 9-0 monofilament Vicryl (model D-8760) has advantages. The critical aspect of his suture pattern is making all of the suture bites longer than the space between any suture bites (figure 1). The suturing starts with a solid bite incorporating sclera and conjunctiva just to the right of the extent of the con-junctival opening near the limbus (right-handed surgeon). It is anchored by ty-ing it to itself. The next pass is down through the edge of the conjunctival flap about 3–4 mm from the right corner of the incision. The needle is then placed to the far right of the incision opening and a long 3–4 mm pass is made tangentially through cornea-sclera along the limbus underneath the small lip of anterior con-junctiva and as far anteriorly as possible. Note the anterior lip is not incorporated in any of the needle passes. After exit-ing cornea-sclera the needle is passed up through the conjunctival flap edge about 2mm from the first downward pass. An-other downward pass is then made 3–4 mm further left and that is followed by a corneo-scleral pass started 2–3 mm away from the exit point of the first corneo-scleral pass. Drawing the suture taut at this point reveals an alternating pattern of crimped conjunctiva under the surface bites and a stretched portion of conjunc-tiva between the surface bites resulting in tight application of the flap to the cornea-sclera (figure 2).
Figure 3. The appearance of the closed incision with the anterior and posterior conjunctival edges firmly abutting each other.
The pattern is repeated as needed until the needle exits the left end of the inci-sion up through the conjunctiva, beyond the confines of the incision. A final pass is made generously incorporating the re-dundant corner of conjunctiva and un-derlying sclera leaving a loop of suture so it can be tied to itself after carefully tightening the entire suture line. It is critical that the whole flap be tightly applied to the cornea-sclera under the anterior conjunctival lip. As long as the Wise suture bite architecture and length relationships are maintained, a secure closure is created with the edge of the conjunctival flap buttressed up against the small lip of limbal conjunctiva pro-ducing a tightly ‘pursed-lips’ appearance along the limbus (figure 3). The anterior lip acts as a bolster creating robust water-tight closure reducing the tendency for early leakage and helps promote rapid
epithelialization at the wound. It is also important to keep any Tenon’s capsule attached to the undersurface of the con-junctiva and perform posterior sub-Ten-on’s blunt dissection to enhance effective wound closure and more posterior flow. Over the last 10 years the author has found that this conjunctival incision and closure technique produces favorable bleb morphology and reduces the ten-dency for bleb migration into the cornea, which we more often see with limbus based surgery.
Related Video: https://eyetube.net/vid-eo/closing-the-fornix-based-conjuncti-val-flap/
References:1 Wise JB. Mitomycin-compatible suture tech-nique for fornix-based conjunctival flaps in glau-coma filtration surgery. Archives of ophthalmol-ogy.1993Jul;111(7):992–7.

12 Glaucoma Now – Issue No 2, 2011. www.glaucomanow.com
CME credits can be obtained via the questions on the website very soon.
The process of obtaining CME accreditation for the journal is currently ongoing.
STATEMENT OF NEED AND PROGRAM DESCRIPTIONRecent months and years have seen significant advances in our under-standing of glaucoma. Much has been learned, not only about damage mecha-nisms and pathogenesis, but also about diagnosis and management. Treatment options–bothmedicalandsurgical–continue to expand. This program will review this new knowledge with an em-phasis on incorporating recent insights into day-to-day practice.
DATE OF ORIGINAL RELEASEMarch 2011. Approved for a period of 12 months
DISCLAIMERParticipants have an implied responsibil-ity to use newly acquired information to enhance patient outcomes and profes-sional development. The information presented in this activity is not meant to serve as a guideline for patient care. Any procedures, medications, or other cours-es of diagnosis or treatment discussed
or suggested in this activity should not be used by clinicians without evalua-tion of their patient’s conditions and possible contraindications or dangers in use, applicable manufacturer’s product information, and comparison with recom-mendations of other authorities.
CONTRIBUTORSAnthony Wells,• MD, FRANZCO is ophthal mologist at the eye Clinic of Wellington Hospital in Wellington, New Zealand. He is also a member of Capital eye specialists in Wellington.
Robert Stamper,• MD is Professor of Ophthalmology at the university of California in san Francisco, usA.
Peng Khaw• PhD, FRCs, FRCP, FRCPath, Fs Biol, FARVO, FMedsci, is Professor of Glaucoma and Ocular Healing and Director at uK National institute of Health Research Biomedical Research Centre at Moorfields eye Hospital and uCL institute of Ophthalmology in London, uK.
Stelios Georgoulas• , MD, PhD is his co-worker and a specialist trainee.
Ashkan Khalili,• MD is his co-worker and a PhD student.
Garry P. Condon• , MD is Associate Professor at Drexel university Col-lege of Medicine as well as Clinical Assistant Professor at the university of Pittsburgh and Chairman of the Department of Ophthalmology at Allegheny Hospital in Pittsburgh, Pennsylvania, usA.
DISCLOSURE STATEMENT EDITORIAL BOARDClive Migdal serves on the Faculty and Advisory Boards of the following compa-nies: Alcon, Allergan, Merck, Pfizer and santen.
Ivan Goldberg serves on the Faculty and Advisory Boards of the following com panies: Alcon, Allergan, Merck and Pfizer.
Remo Susanna serves on the Faculty and Advisory Boards of the following companies: Alcon, Allergan, Merck and Pfizer.