Embed Size (px)
Citation preview
Trichomonas vaginalisTrichomonas vaginalisand other and other
Ameba InfectionsAmeba Infections
Doç.Dr.Hrisi BAHAR
Trichomonas vaginalisTrichomonas vaginalis
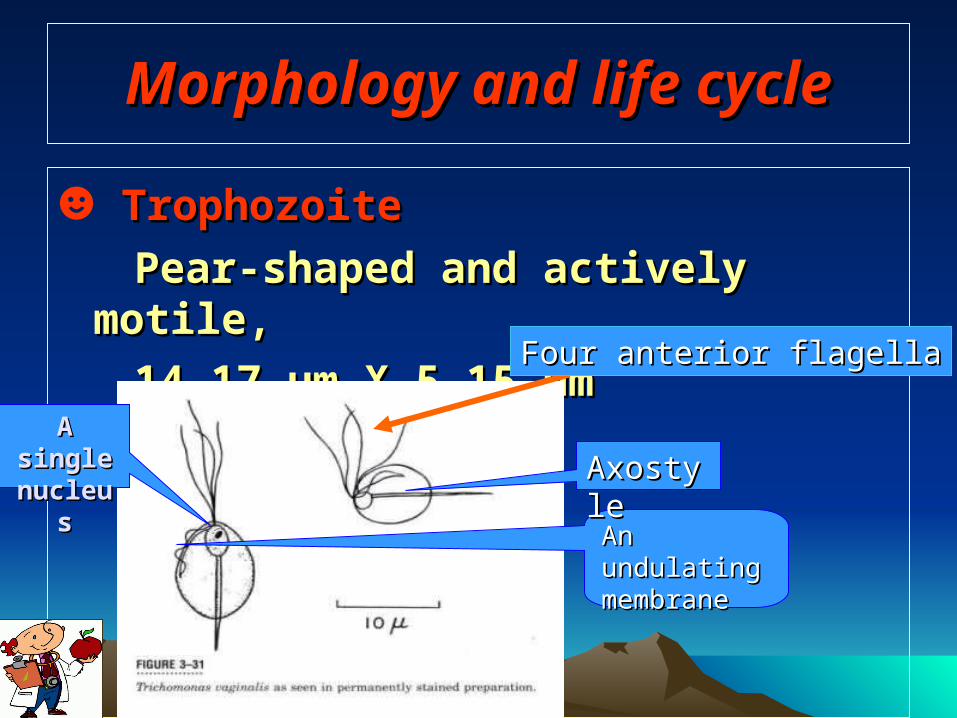
Morphology and life cycleMorphology and life cycle
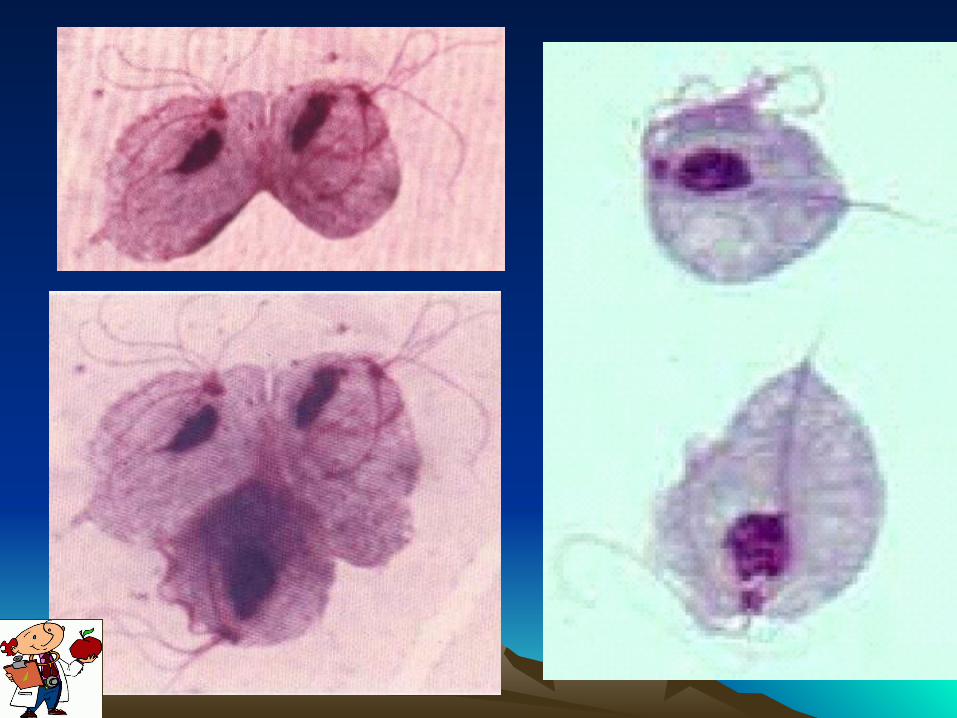
☻ TrophozoiteTrophozoite
Pear-shaped and actively motile, Pear-shaped and actively motile,
14-17 µm X 5-15 µm14-17 µm X 5-15 µm
An An undulating undulating membranemembrane
AxostyleAxostyle
Four anterior flagellaFour anterior flagella
A single A single nucleusnucleus
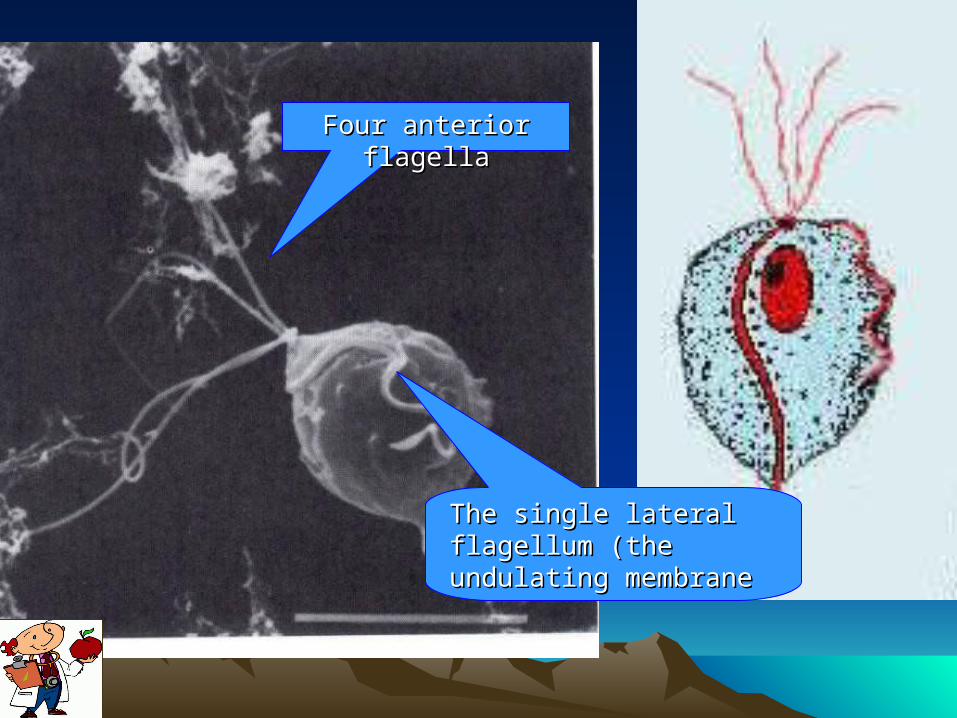
Four anterior Four anterior flagellaflagella
The single lateral The single lateral flagellum (the flagellum (the undulating membraneundulating membrane
Life cycleLife cycle
☻ Life cycleLife cycleThere is oThere is only trophozoite stage in nly trophozoite stage in life cyclelife cycle.. WomenWomen: vagina and urethra: vagina and urethra
TrophozoitesTrophozoites
Men:Men: urethra or prostate, urethra or prostate,
testes, epididymistestes, epididymis
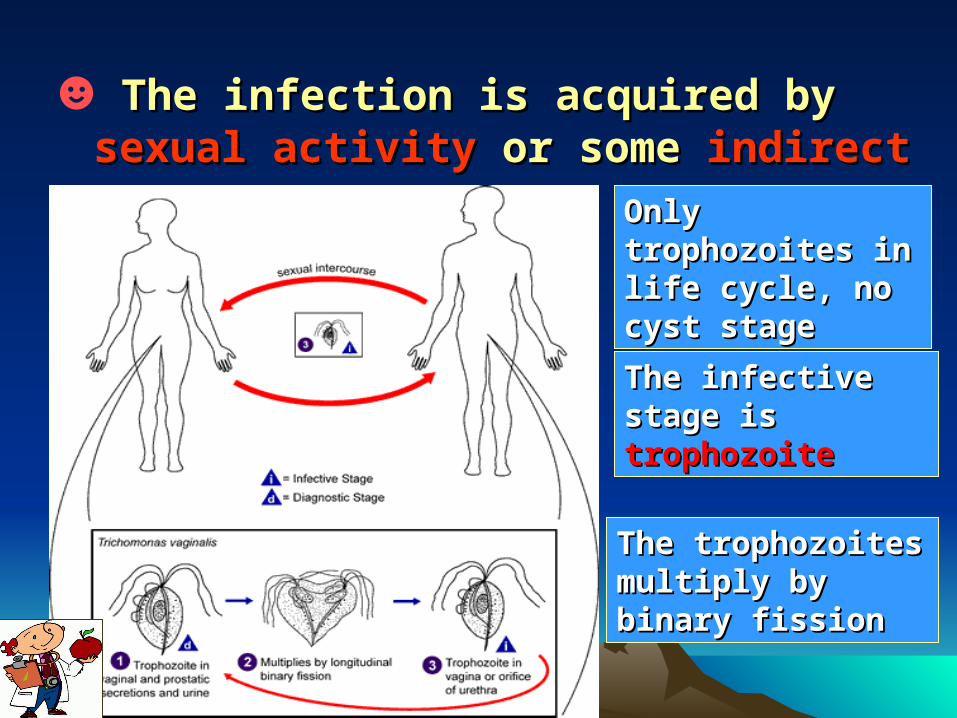
☻ The infection is acquired by The infection is acquired by sexual sexual activityactivity or some or some indirect waysindirect ways
Only Only trophozoites in trophozoites in life cycle, no life cycle, no cyst stagecyst stage
The infective The infective stage isstage is trophozoitetrophozoite
The trophozoites The trophozoites multiply by multiply by binary fissionbinary fission
☻Trichomoniasis is a vaginal infections caused by T. vaginalis.
☻ This infection is among most common conditions in women attending reproductive health care centers.
EpidemiologyEpidemiology
☻ Most prevalent in age group 20-45.
☻Worldwide, over 180 million cases.
☻T. vaginalis accounts for 15-20% of all vaginitis.
EpidemiologyEpidemiology
Trichomonas vaginalisTrichomonas vaginalis
☻ The vagina is the most common site of infection in women, and the urethra (urine canal) is the most common site of infection in men.
☻ Women can acquire the disease from infected men or women, but men usually contract it only from infected women.
Signs and SymptomsSigns and Symptoms
Women:Women:
Signs and symptoms of infection range from having no symptomsno symptoms (asymptomatic) to very symptomaticto very symptomatic. Typical symptoms includeTypical symptoms include :
☻Foul smelling , pale yellow or gray-green discharge from the vagina
☻Vaginal itching or redness.
Signs and SymptomsSigns and Symptoms
Other symptoms can includeOther symptoms can include ☻Lower abdominal discomfort
☻The urge to urinate
☻ The vaginal mucosa often is deeply erythematous.
☻ The cervix is friable and diffusely inflamed, sometimes covered with numerous petechiae ("strawberry cervix").
Signs and SymptomsSigns and Symptoms
Men: ☻Urethritis and, more rarely, epididymitis or
prostatitis can develop in infected males
☻Most are asymptomatic.
☻Reinfection is common.
Trichomonas vaginalis is considered an important cofactor in amplifying human immunodeficiency virus transmission.
DiagnosisDiagnosis
☻ Finding trophozoitesFinding trophozoites
In women:In women: vaginal dischargevaginal discharge
In the male:In the male: urethral discharge , urethral discharge , prostates secretions, centrifuged urine.prostates secretions, centrifuged urine.
Methods:Methods: direct smear or culture direct smear or culture
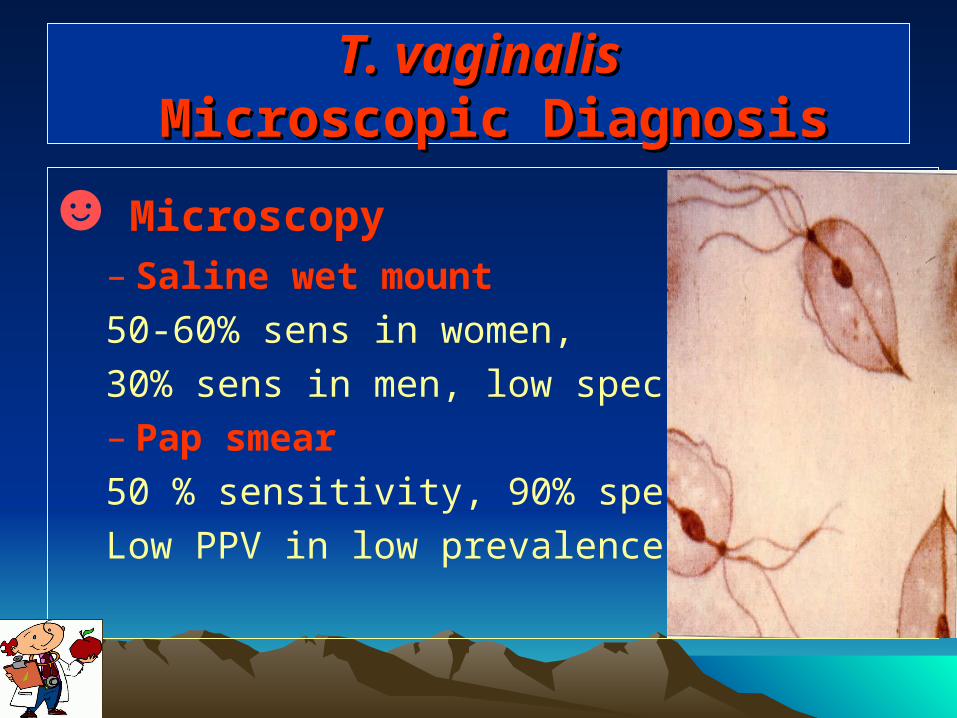
T. T. vvaginalisaginalis Microscopic Diagnosis Microscopic Diagnosis
☻ Microscopy– Saline wet mount
50-60% sens in women,
30% sens in men, low specificity– Pap smear
50 % sensitivity, 90% specificit
Low PPV in low prevalence pop
T.T.vaginalis vaginalis Culture DiagnosisCulture Diagnosis
In-Pouch TVIn-Pouch TV
85-95% sens in women, >95% spec
60 % sens and high specificity in men
TT. vaginalis. vaginalis Antigen Detection Antigen Detection
OSOM Trichomonas Rapid Test (Genzyme Diagnostics, Cambridge, MA) ☻ 10 min point-of-care test
☻ 83.3% sensitive 98.8% specific vs. culture
☻(wet mount 71.4% sensitive)
TT. . vvaginalisaginalis Molecular Methods Molecular Methods
☻ PCR>90% sensitive and >95% specific for females
>90% sensitive and specific for malesCulture 70% sensitive vs. PCR
Recommended Treatment Recommended Treatment by CDCby CDC
☻ Metronidazole 2 g ………orally in a single dose OR
Tinidazole 2 g ……………orally in a single dose
Alternative Regimen
☻ Metronidazole 500 mg......... orally twice a day for 7 days
Patients should be advised to avoid consuming alcohol during treatment with metronidazole or tinidazole. Abstinence from alcohol use should continue for 24 hours after completion of metronidazole or 72 hours after completion of tinidazole.
Free Living AmebasFree Living Amebas
Free Living AmebasFree Living Amebas
Small free-living amebas belonging to the genera :
►► Acanthamoeba
►► Naegleria
occur world-wide .
AcanthamoebaAcanthamoeba spp spp
►► At least 5 species of Acanthamoeba have been identified in human tissues, this is one of the most common amebas in soil and freshwater.
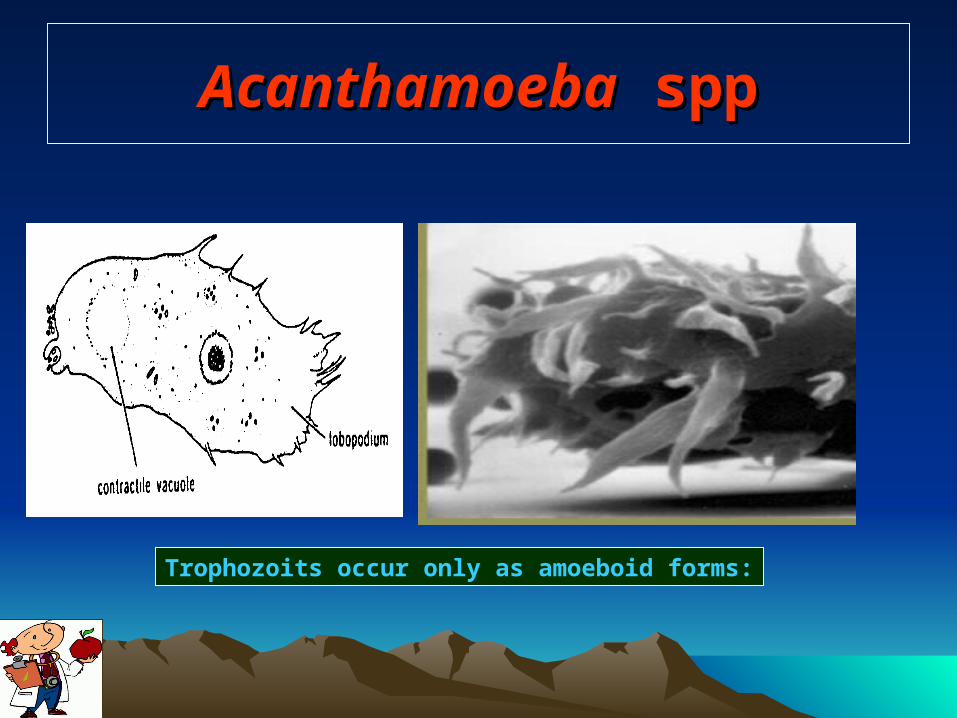
►► Trophozoits occur only as amoeboid forms:
AcanthamoebaAcanthamoeba spp spp
Trophozoits occur only as amoeboid forms:
AcanthamoebaAcanthamoeba spp spp
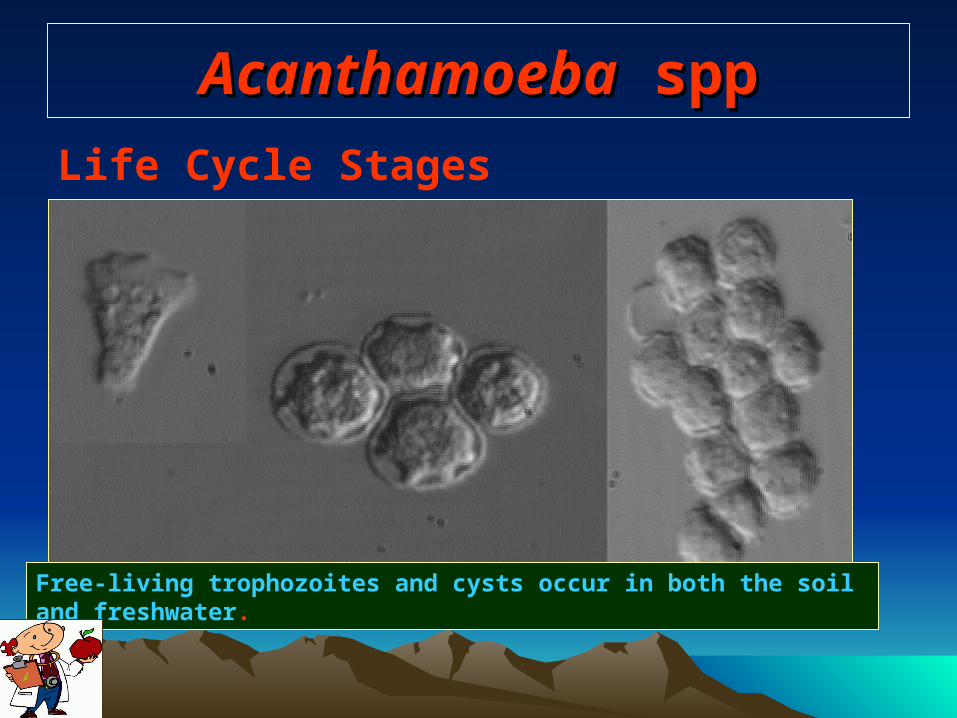
Life Cycle Stages
Free-living trophozoites and cysts occur in both the soil and freshwater.
AcanthamoebaAcanthamoeba spp. spp.
These species cause 2 pathological effects
►► Granulomatous amebic meningoencephalitis.
►► Inflammation and opacity of the cornea.
AcanthamoebaAcanthamoeba spp spp
Symptoms
►► Foreign body sensation, severe ocular pain, photophobia and blurred vision.
►► Often pain is more severe than signs in early course of the disease.
AcanthamoebaAcanthamoeba spp spp
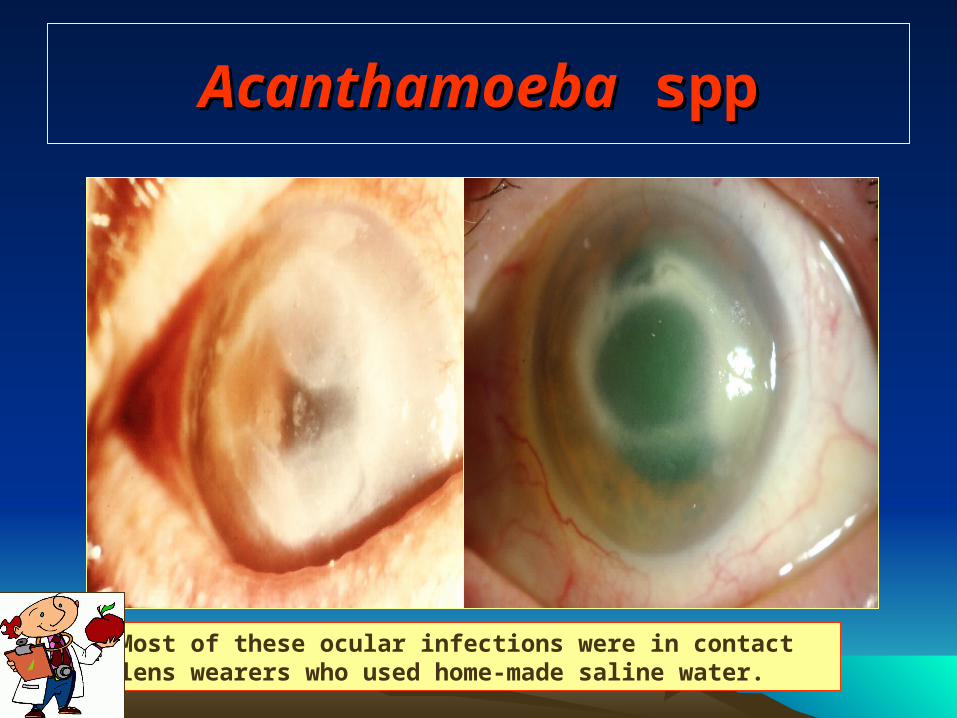
Most of these ocular infections were in contact lens wearers who used home-made saline water.
AcanthamoebaAcanthamoeba spp. spp.
Management
►► Early diagnosis a prognostic factor of
a successful outcome.
►► Topical anti-amoeba agents.
►► Penetrating keratoplasty in a severe
progressive keratitis.
Naegleria sppNaegleria spp
►► Free-living in freshwater and soil including thermal pools
►► They have even been isolated from bottled mineral water in Mexico.
Naegleria sppNaegleria spp
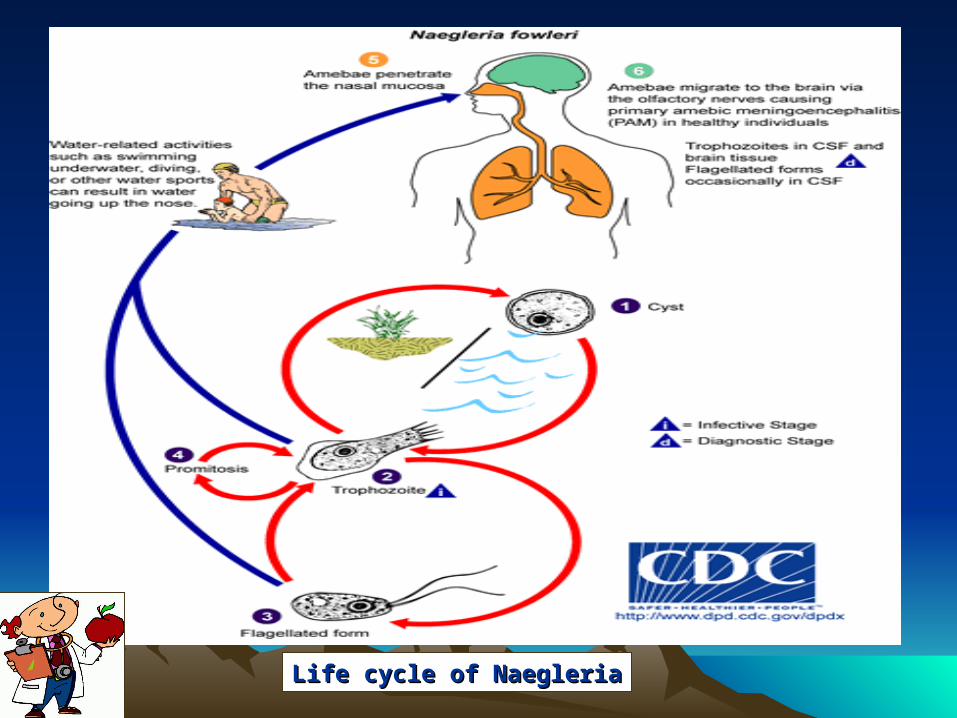
Life cycle of NaegleriaLife cycle of Naegleria
Naegleria sppNaegleria spp
►► N. fowleri is the only species of Naegleria genus that is pathogenic to humans
►► It lives in nature fresh water, lakes and ponds (especially warm water) .
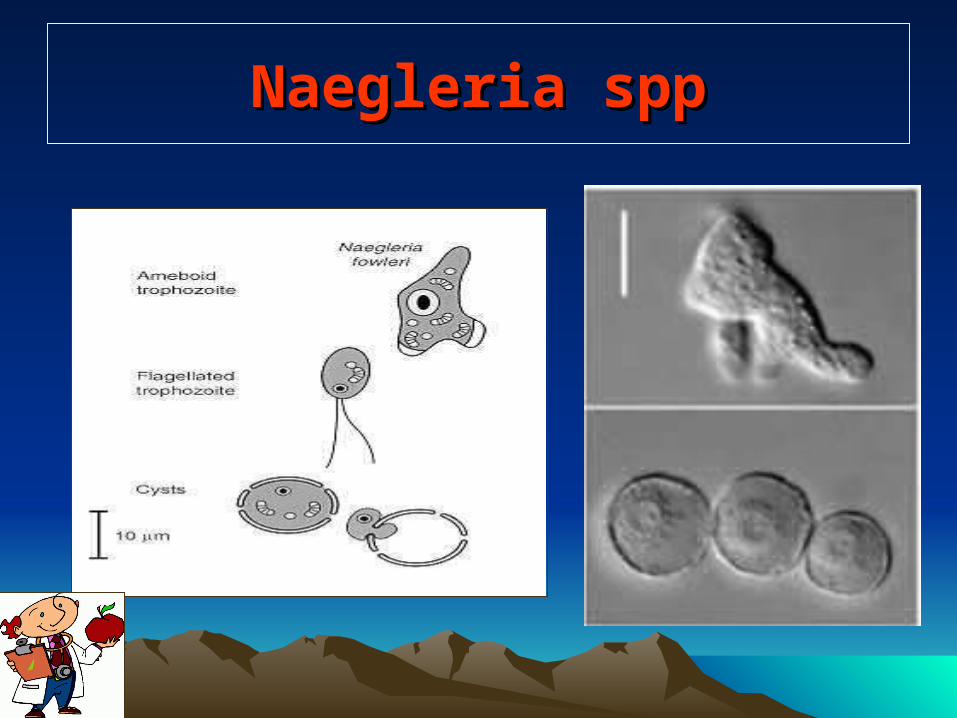
Naegleria sppNaegleria spp
Exists in 3 forms
►► Trophozoite invasive, reproductive form
(7- 20 µ m) which lives in temperatures from
35- 46 .C
►► Flagellate form ,do not divide
►► Resistant cyst form 7 -10 µm in size
Primary Amoebic Meningoencephalitis imary Amoebic Meningoencephalitis (PAM)(PAM)
►► Acute, suppurative infection of the brain and meninges caused by N. fowleri
►► First described in 1965 by R.F. Carter and M. Fowler in Australia
►► Usually affects immunocompetent children and young adults.
Naegleria sppNaegleria spp
Epidemiology
►► N. fowleri has been isolated all over the world
►► As of 1997, approximately 200 cases have been reported worldwide with 81 cases in the US (primarily in central and southeast)
►► Risk factors: jumping/diving, IgA defic
►► Males/females =3/1
►► Mortality rate > 95%
Naegleria sppNaegleria spp
Pathophysiology
►► Trophozoites penetrate the nasal mucosa
and the cribiform plate during inhalation or
aspiration of contaminated dust/water
►► The organisms migrate via the olfactory nerves to invade brain tissue
►► Enzymes are produced resulting in diffuse and
rapid hemorrhage and necrosis of the brain
Naegleria sppNaegleria spp
Clinical manifestation ►► Indistinguishable from acute bacterial meningitis ►► Symptoms begin 2 -14 days from exposure►► Initially may notice change in taste/smell ►► fever, nausea, vomiting.►► Mental status changes seen in 66% ►► Myocarditis has been reported ►► Rapid progression with death occurring in 3-
7days-
Naegleria sppNaegleria spp
Diagnosis
►► Lab studies reveal leukocytosis , hyperglycemia and glycosuria leukocytosis,
►► Molecular studies PCR/DNA probes under research
Naegleria sppNaegleria spp
CT scan of head
►► Not diagnostic for PAM
►► May be normal early in disease
►► Later, may show signs of elevated leptomeningeal enhancement

Naegleria sppNaegleria spp
Important notesImportant notes
►► Consider Naegleria when all studies point to bacterial meningitis but the gram stain is negative
►► Overall mortality is near 95% therefore you need a high index of suspicion
►► Plug your nose or wear nose clips when jumping into fresh water
Naegleria sppNaegleria spp
Treatment
►► Amphotericin B is the mainstay of therapy
►► Successful outcomes are reported with high dose systemic and intrathecal ampho b.
►► Other adjunctive therapy includes miconazole and oral rifampin
►► New studies show that azithromycin may be a useful addition to therapy.